
Abstract
Evidence-based strategies to decrease fall rates are well established. However, little is understood about how older people engage in fall prevention strategies. Motivational Interviewing (MI) sessions aimed to facilitate individuals’ engagement in fall prevention can be analyzed to learn what it means for older people to engage in fall prevention. Thus, the purpose of this study was to explore how older people describe their engagement in fall prevention. Participants in our parent project, MI for Fall Prevention (MI-FP), who received MI sessions were purposively selected for maximum variation in age, sex, fall risks, and MI specialist assigned. The first (of 8) MI sessions from 16 participants were recorded, transcribed, and analyzed using qualitative content analysis. Three researchers first deductively analyzed fall prevention strategies that participants described using an evidence-based fall prevention guideline as a reference. Then, we inductively analyzed the characteristics of these strategies and how participants engaged in them. Finally, we used the Capability, Opportunity, Motivation, Behavior (COM-B) model to organize our results about factors influencing engagement. We found (1) older adults engage in unique combinations of fall prevention strategies and (2) decisions about engagement in fall prevention strategies were influenced by multiple factors that were personal (e.g., who I am, capability, motivation, and opportunities). This study highlighted how fall prevention can be a life-long lifestyle decision for older people. Understanding older people’s perspectives about engaging in fall prevention is essential to develop interventions to promote evidence-based fall prevention strategies in real-world settings.
One in 4 older people aged 65 and older fall each year in the United States. 1 Many accidental falls can be prevented by using evidence-based strategies, such as balance-focused exercises, to address the unique fall risks of individuals.2-4 Yet, prior research examining the extent to which a person’s fall prevention behaviors are consistent with health care recommendations (e.g., adherence) shows that only half of the participants in fall prevention trials enacted the recommended interventions. 5 One gap in the research examining the uptake of fall prevention behaviors is limited evidence regarding older people’s engagement. According to Higgins et al, 6 engagement represents more than adherence and includes internal and external influences on adherence, such as one’s desire and capability to actively choose to participate in recommended fall prevention behaviors in ways uniquely appropriate to oneself.
Gaps in Older Peoples’ Engagement in Fall Prevention
Prior quantitative and qualitative research suggests older people’s engagement in evidence-based fall prevention strategies is essential to reduce their risks of falling 7 and begins to elucidate that engagement in fall prevention behaviors is a dynamic process.8-11 For example, one recent study examined the extent to which older people engaged in fall prevention efforts using 3 indicators of patient engagement: (1) Consultation (receiving information), (2) Involvement (prioritizing risks), and (3) Partnership (identifying prevention actions) guided by Patient and Family Continuum of Engagement framework. 12 Participants engaged in a multifactorial assessment conducted by a registered nurse trained in fall prevention and motivational interviewing (MI) and discussed risks they prioritized. They also co-created fall prevention care plans, yet less than half reported behavior changes that were part of their fall prevention care plans. 13 Other research provides descriptions of complex barriers to older people’s engagement, ranging from the influence of individual beliefs and attitudes, social issues, and inadequate access to resources,14-16 as well as enablers such as patient-centered approaches that promote self-efficacy.10,17,18 These findings raise basic questions about how older people engage in fall prevention. Exploring older people’s perspectives about the dynamics involved in real-life decisions and the influences on engagement in fall prevention is essential to develop interventions to promote evidence-based fall prevention strategies.
Purpose
The purpose of this study was to describe older people’s engagement in fall prevention strategies and behaviors recommended by their primary-care providers. We approached this question using data from MI sessions focused on fall prevention. Motivational interviewing is a behavior change communication approach designed to elicit individuals’ own descriptions on their experience with a health topic. The MI sessions offer an ideal foundation for qualitative exploration to gain deeper understanding of older people’s engagement in fall prevention. Thus, the specific aims were to understand: (1) what fall prevention strategies older people used to engage in fall prevention and (2) how older people engaged in those fall prevention strategies. This study is part of a larger randomized trial called “Using Motivational Interviewing to Engage Older People in Fall Prevention” (Motivational Interviewing for Fall Prevention [MI-FP study]) in which we tested the feasibility, acceptability, and initial impact of MI to engage community-dwelling older people to reduce fall risks and prevent falls. We analyzed the first of 8 MI sessions from the MI-FP study to understand what it means for older people to engage in fall prevention before further MI sessions were provided. The Consolidated Criteria for Reporting Qualitative Research (COREQ) criteria 19 were used to guide this report of qualitative findings.
Methods
Design and Setting
In this qualitative study, we analyzed the first of 8 MI session transcripts and audio-recordings of participants in the MI-FP study (manuscript in review). The MI-FP study enrolled participants who were assessed for fall risks from April 2019 through July 2022 from an internal medicine primary-care clinic at an academic medical center in the northwest United States. Inclusion criteria for participation were: age ≥ 65 years; high fall risk using Centers for Disease Control and Prevention [CDC] Stopping Elderly Accidents Deaths and Injuries [STEADI] fall risk score ≥ 4; and receipt of fall prevention recommendations from their primary-care provider. Participants provided verbal consent to participate in the study, as approved by our Institutional Review Board (IRB). This study was approved by the Oregon Health and Science University Institutional Review Board (#8993) and registered as Clinical Trial # NCT04612842.
Overview of MI Sessions
Motivational interviewing sessions were 1:1 telephone discussions that were 15 to 30 minutes long. The MI-FP study ensured fidelity of the MI sessions through MI specialists’ proficiency levels and adherence to the protocol. Motivational interviewing sessions were facilitated by 6 MI specialists who already had basic MI training and experience in using MI. Motivational interviewing specialists were assigned participants after completing 6 hours of study-specific training (e.g., study protocol, fall prevention, providing MI to older people, using telephone and video calls to provide MI).
The proficiency of the interventionists lends support for these data to be an ideal source for examining older adults’ perspectives on engagement in fall prevention. Motivational interviewing proficiency was confirmed using the Motivational Interviewing Treatment Integrity Coding Manual (MITI 4.2) coding scheme. 20 We determined proficiency as scoring at least 3 (1-5 possible rating) for the relational and technical global scores of the MITI 4.2. In addition, our goal for MI Behavioral Skills included a ratio higher than 2:1 for reflection statements to questions.20,21 Throughout the MI-FP study, MI specialists participated in monthly advanced MI training sessions. Fidelity of MI sessions were maintained by monthly self- and group-coding of MI sessions using the MITI 4.2 coding scheme. Randomly selected MI sessions were assessed quarterly by a qualified external MITI coding team. Details of implementing MI sessions to address fall prevention are described elsewhere. 22 All initial sessions began with these semistructured questions: “People are not necessarily happy to talk about fall prevention. How do you feel about talking about fall prevention today?” “What comes to your mind when you think about fall prevention?” and “What do you currently do to keep yourself safe, grounded, and active?”
Participant Selection
Participants were purposively sampled from the MI-FP study from a pool of 83 participants who had completed their first MI session. Interviews with poor audio quality were not considered. To maximize the variation of perspectives related to engagement in fall prevention, we selected female and male participants to represent the 65 to 74, 75 to 84, and ≥85 years age groups and a range of fall risk scores (4-14 range; 14 indicates highest fall risk using STEADI fall prevention guideline). 23 In addition, we sampled MI sessions conducted by 6 different MI specialists to account for any variance on participants’ responses to different MI styles. Finally, new participants were added to the study until no new findings arose.
Data Collection
The initial MI sessions were conducted between September 2020 and September 2021. Participants’ baseline characteristics were collected through chart review for date of birth, sex (female, male, and other), and STEADI fall risk scores. Participants’ MI session data were collected by the MI specialists in audio recordings that were transcribed verbatim, de-identified, stored, and analyzed using Atlas.ti (ATLAS.ti Scientific Software Development GmbH, Berlin, Germany).
Analysis
Using a constructivist paradigm 24 suited to understand the meaning of phenomena, we used a content analysis approach with deductive and inductive coding, to understand what it means for older people to engage in fall prevention. The codes for fall prevention strategies that participants may use to describe their engagement with fall prevention were developed deductively. The codes to describe evidence-based fall prevention strategies were developed based on CDC’s STEADI fall prevention guideline, which had been incorporated into electronic health records at the study hospital. The STEADI fall prevention guideline was chosen because it directly addresses fall prevention in primary care and represents a synthesis of recommendations and guidelines from the United States Preventative Services Task Force, 4 American Geriatric Society, 25 and a Cochrane Review. 2 Fall prevention strategies in STEADI may include one or more of the following according to results of multifactorial fall risk assessments: refer to physical therapy, refer to evidence-based exercise or fall prevention program (e.g., Tai Chi), optimize medication regimen, refer to occupational therapist to evaluate or improve home safety, address orthostatic hypotension with pharmacologic and nonpharmacologic approaches, refer to ophthalmologist, provide education on good footwear, refer to podiatrist, and optimize treatment of long-term health conditions.
General evidence-based actions that are not included in the STEADI guideline were also coded, such as walking and use of walking aids. While general endurance physical activity such as walking is recommended for all older people, including those with frailty and multiple long-term conditions,26-28 it alone is not thought to be fall-preventative and thus is not included in the STEADI guideline. General physical activity guidelines all suggest aerobic physical activity be pursued in accordance with one’s abilities and conditions.26-28 Similarly, although use of assistive devices for walking and transferring are considered standard practice across settings,29-31 they are not explicitly included in the STEADI guideline.
The other codes and findings we developed throughout the study were inductively derived. Text and audio data were analyzed by 3 researchers who first read and listened to the data beginning in July 2022 during online meetings to become familiar with the flow of the MI sessions and to build a coding structure with definitions. Later, coding continued asynchronously and was reviewed and discussed by the research team to resolve discrepancies and to organize findings. To organize our findings, we used Michie et al’s 32 Capability, Opportunity, Motivation for Behavior (COM-B) model. This model provides a framework to understand factors that contribute to engagement in fall prevention. Matrices were developed to examine similarities and differences of codes across participants and to determine when we reached saturation of data.
Results
We analyzed 16 initial MI sessions from 16 participants (mean age of 79.31; 53% female; and low to moderately high fall risk [mean STEADI fall risk score: 7.56]; and all identified themselves as White race). Overall, MI-FP sessions met proficient levels, thus ensuring the quality of MI sessions analyzed. While MI specialists had their own styles of delivering MI, information that was shared about fall prevention were similar across the interventionists. We identified 2 main findings. The first was that older people engaged in unique combinations of fall prevention strategies. The second was that participants’ decisions about what and how they engaged in fall prevention were influenced by multiple factors. We present exemplar quotes as well as a summary of participants’ descriptions to present our results.
Older People Engaged in Unique Combinations of Fall Prevention Strategies
Two broad categorizations of fall prevention strategies were identified. Participants reported engaging in fall prevention strategies that aligned and did not align with STEADI fall prevention guidelines. Their selection of fall prevention strategies and the intensities with which they engaged in them were unique. This is illustrated by the story of one participant, Leigh (age 96, female; fictitious names are used here and afterwards for participant quotations). She described that she knows that that Birkenstock sandals could increase her risk of falls, but because she loved their comfort, she was unwilling to stop wearing them. Thus, she was aware that a good footwear is key to fall prevention (endorsed in STEADI), but it was not something that she was going to change. She also described her desire to resume a group-based fall-risk reducing exercise class that she had enjoyed which had been disrupted due to the COVID-19 pandemic. She was also aware that balance-challenging exercises can decrease fall risks (endorsed in STEADI) but was unable to restart them because she did not have access to the class that she enjoyed. The fall prevention strategies that she was actively engaging in were daily walks, which she believed helped prevent falls and her use of a cane when walking outside. While walking is beneficial to overall health and use of mobility aids may prevent falls, they are not explicitly endorsed by STEADI guidelines.
Table 1 captures and organizes participants’ engagement with fall prevention strategies that align with STEADI guidelines and other (non-STEADI) strategies individuals reported as useful in reducing or preventing falls. Commonly mentioned STEADI fall prevention strategies were balance exercises (e.g., Tai Chi, physical therapy sessions to improve balance control), home safety, feet/footwear, vision, management of hypotension, avoidance of high fall risk medications, and treatment of underlying illnesses or symptoms that contribute to fall risk (e.g., vertigo). 23
Fall Prevention Strategies That Participants Described in Motivational Interviewing Sessions About Fall Prevention.
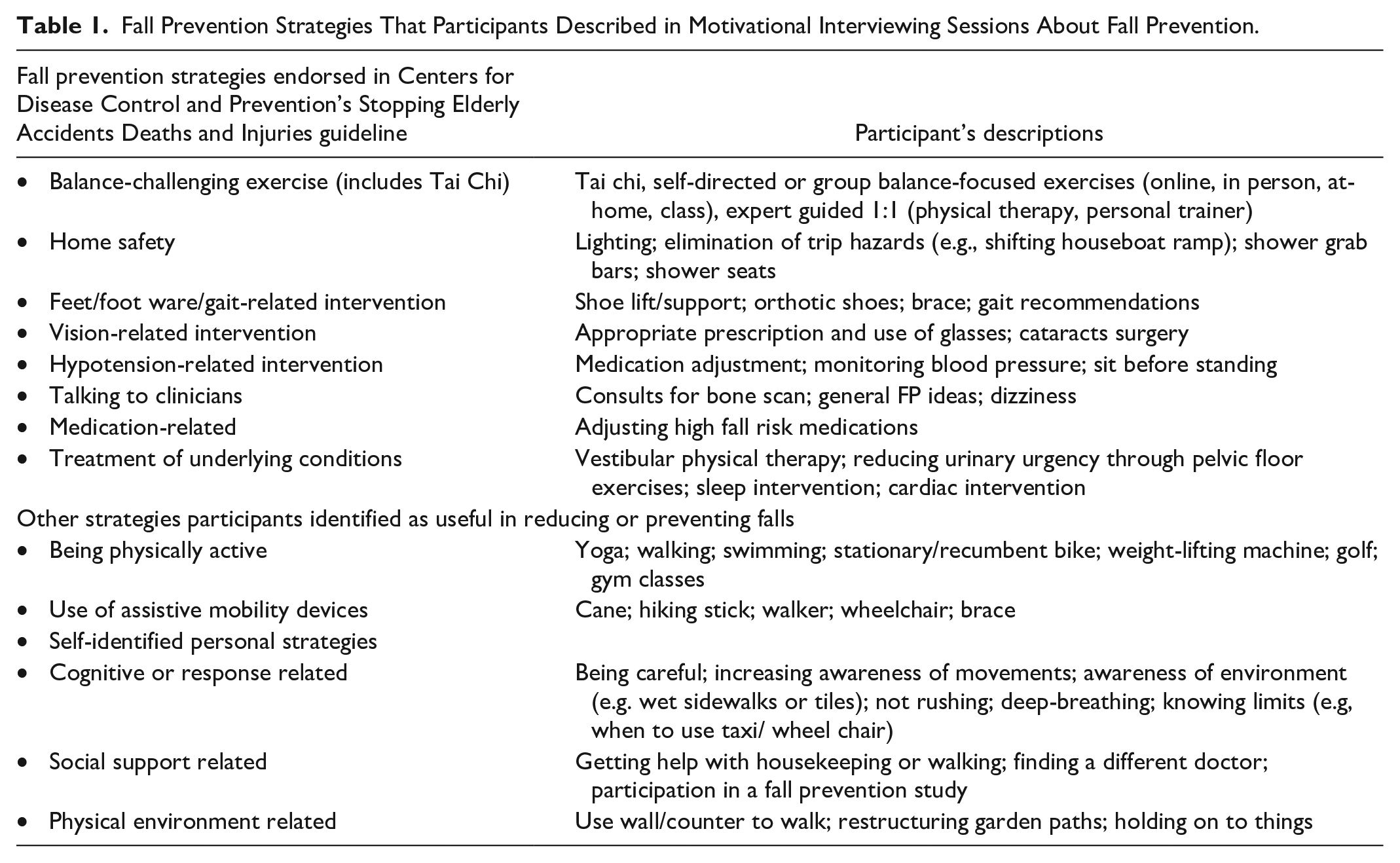
There were a wide variety of fall prevention strategies that participants engaged in that were not explicitly included in STEADI fall prevention guidelines such as selected use of assistive devices, walking, and being careful. How participants used assistive devices varied according to the individual’s physical and social environment, the purpose of device use, and their preference. For example, participants described how they used assistive devices such as canes and walkers mostly indoors (or outdoors), mostly for long distances, only at some times of the day (e.g., in the morning or at night), when expecting crowds of people, or only when feeling dizzy. Walking sticks were preferred by individuals who saw themselves as physically active.
Walking at a comfortable pace and being careful were 2 commonly described fall prevention strategies that were not explicitly part of STEADI guidelines but part of general physical activity recommendations for older people and standard practice among participants. Many participants described walking, often daily, as a way to engage in fall prevention based on their strong desires to be physically active. They noted that staying physically active was essential to being healthy and being healthy meant fewer falls. Finally, several participants described being careful and thoughtful, through actions such as holding on to other people or furniture and practicing mindfulness to stay calm and focused. Many participants described being careful—a general way of being that encompassed maintaining attention to potential fall risk and taking actions to avoid falls. Participants’ engagement in their personal, nonevidence-based strategies are reflected in a quotation below: I take extreme measures to prevent falling, let’s put it that way. I had two serious falls that injured me. I think both of them were more than a year ago now. [I’ve] not had any falls of any sort since, because I take such care to not fall. I mean, I hold on to stuff. I have a stick. I look where I’m going, I walk slowly, and [I’m] just a typical little old lady. . .because both times I fell was because I was hurrying, and I wasn’t paying attention to where my feet were. (Natalie, age 83, female)
Decisions About Engagement in Fall Prevention Strategies Were Influenced by Multiple Factors
Participants were impacted by a range of factors such as their capabilities, opportunities available to them, and their motivation to determine what and how they engaged in fall prevention. Table 2 describes these factors and how they apply to fall prevention with examples of participants’ quotes. How these factors impacted participants varied by the individual based on their values, beliefs, and preferences. Thus, fall prevention looked different for each individual.
Factors Influencing Participants’ Engagement in Fall Prevention.
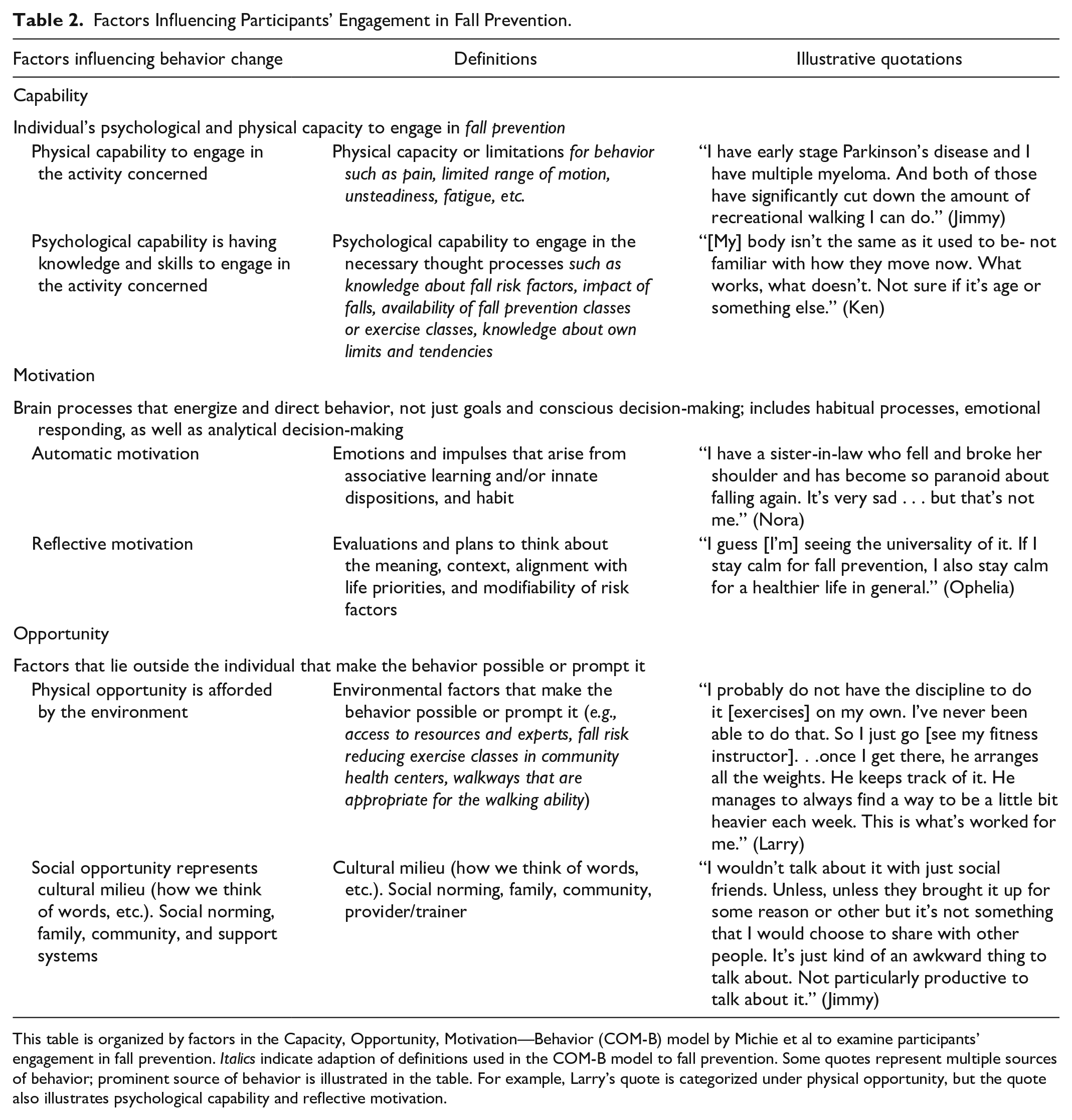
This table is organized by factors in the Capacity, Opportunity, Motivation—Behavior (COM-B) model by Michie et al to examine participants’ engagement in fall prevention. Italics indicate adaption of definitions used in the COM-B model to fall prevention. Some quotes represent multiple sources of behavior; prominent source of behavior is illustrated in the table. For example, Larry’s quote is categorized under physical opportunity, but the quote also illustrates psychological capability and reflective motivation.
Casey’s situation (age 73, female) illustrated how capabilities, opportunities, and motivation factors impacted choices that she made. This case also illustrates that capability and motivation factors are closely tied to the sense of who I am. She described herself as a very active person who is on the board of performance arts and enjoys international travel and aqua aerobics. She also acknowledged that she is a person who falls often. She described how she has accepted this risk in the past but now feels more concerned about it because of the significant harm that she will incur from a future fall: “I’m just klutzy. I’ve accepted it. I’ve embraced it. So, falling has always been a part of my life, but now that I’m older, I realize it can be really dangerous.” She realizes that her physical capability will worsen with age, and the same type of fall she had in the past may cause more harm now that she is older. Since she was motivated to stay active because that’s who she identifies herself as, she was interested in using hiking sticks as her fall prevention strategy. This creates a new opportunity for her to continue activities she enjoys doing as a solution to address her current fall risks.
Capabilities were also reflected in many participant statements of who they are, or self-perception of themselves, as a whole person in the MI sessions. For example, participants described their age; health status; personality; social relationships; things that they enjoy or are important to them; their preferences, values, and goals; and who they were in the past. Participants’ ages and how they are living with the uncertainties of aging were often mentioned across all age groups in our sample. Two quotations illustrate age-related perceptions about their capabilities about fall prevention. The first is about transitioning to being older. In this statement, she describes the liminal state that she’s in because of changes in her physical capability.
When you get old, you have to pay attention to all those things so much more. And your mind catching up with what your body is doing. You have to say, my god, I’m old. You know? And your body just doesn’t do what it’s supposed to be doing. And it’s going slower and it’s wobbly. (Ophelia, age 78, female)
The second quotation is regarding thoughts about one’s future, older self, in which he sees himself to be more at risk for falling, and he expects his perception and engagement will change for fall prevention. In this statement, he describes how his psychological capability to engage in fall prevention is expected to shift as he prioritizes his needs over what others think or how he judges himself: I guess I’m at the stage where I am more embarrassed about falling than worrying about it, because I haven’t completely reached the age where I don’t care what other people are thinking about me or being ashamed at the situation. (Ken, age 81, male)
Participants also described how who they are, as a whole person, influenced their motivation for fall prevention. Each participant had unique motivations for engaging in fall prevention. Self-identify and things that matter were the drivers to engage in fall prevention. Radica (age 70, female) stated “I had a couple of major falls, and I certainly don’t want them to happen again.” She considers herself to be “pretty healthy and strong” and was strongly committed to not falling again. She mentioned changing her health-care provider to someone who was supportive of this goal and sought care from a cardiologist, podiatrist, and ophthalmologist. For Jack (age 84, male), maintaining his ability to support his wife, who is sick, was the motivator to engage in fall prevention. Thus, he was determined to walk every day despite pain and awkward gait.
Opportunity that participants described related to fall prevention varied by the individual. Descriptions of participants’ access to programs influenced how they engaged in fall prevention. For Larry (age 79, male), having a fitness trainer that knew and challenged him was critical to continue with the exercises. Conversely, lack of access limited opportunities for some to engage in balance exercises. Martha (age 79, female) explained how she tried to register for balance-focused exercise classes, only to find that the classes were no longer offered. Thus, she had to come up with alternative ways to improve her balance. In some cases, the impacts of COVID-19 pandemic were specifically mentioned as limiting access to opportunities. Leo (age 71, male) described how COVID-19 disrupted his exercise routine and was unable to find a good enough alternative.
Discussion
Overall, our findings highlight that engagement in fall prevention involves varying degrees of reflective cognitive processes of participants to determine meaningful fall prevention strategies that may have life-long implications. Fall prevention is personal because it is influenced by who they are, an individual’s capabilities, access to opportunities, and motivation that vary between people and across time. This aligns with prior studies that older people prefer individualized fall prevention interventions and need supportive environments to manage their fall risks.10,18,33,34 Participants engaged in personalized combinations of fall prevention strategies; including those that were endorsed in STEADI guidelines (e.g., balance-challenging exercises) and those that were not explicitly endorsed but are considered standard practice (e.g., use of walking aids), as well as those that were potentially but not empirically known to be preventative for falls (e.g., walking, being careful). Participants engaged with these strategies in a way that worked for them, and scientific evidence for strategies was not explicitly considered for fall prevention. This aligns with what Worum et al 35 found: Research evidence about fall prevention provided assurance for older people supporting their choices on what fall prevention strategies to engage in. However, the uptake of fall prevention strategies was the result of figuring out what would make them safer in real-world contexts. The diversity of self-identified personal fall prevention strategies that participants described in MI sessions were impressive, and illustrated careful observation and reflective thinking about health needs, preferences, and values by older people.
We found that participants’ engagement in fall prevention strategies was affected by multiple factors that were unique to the individual such as their capability, opportunity, and motivation. In this study, the COM-B model 32 was used as a supportive framework to organize factors influencing engagement in fall prevention because of its natural fit with participants’ statements. Participants often described their capability—physical and psychological—to describe their sense of who I am impacting how they engage in fall prevention now and in the future. This aligns with a prior study in which self-identify was critical to determine older people’s responses to fall risks and fall prevention strategies.5,36 While categorical organization of factors did not fully capture factors or conditions that overlap, interrelate, or shift, this model helps to characterize fall prevention efforts. We were not able to evaluate participants’ engagement with fall prevention based on their fall risks given the scope of this study. The quantitative analysis of the randomized controlled trial (RCT) explores how fall risks impact participants’ fall prevention behaviors. Future work to integrate findings about fall risks and individuals’ engagement in fall prevention will be valuable.
Our findings about how older people engage in fall prevention supports Higgins et al’s definition of patient engagement. 6 They defined patient engagement as an “individual’s desire and capability to actively choose to participate in care in a way uniquely appropriate to the individual, in cooperation with a healthcare provider or institution, for the purpose of maximizing outcomes or improving experiences of care.” 6 This definition and our research results highlight how individuals actively make personal choices about their engagement in health. For fall prevention, it meant that older people in our study were actively engaged in or preparing to engage in multiple fall prevention strategies at the intensities that worked for them. Furthermore, the choices they made about fall prevention seem to have life-long life-style implications as they expected fall risks to increase as they age, and strategies to prevent falling involved making choices for day-to-day activities.
Our findings provide a new perspective from which to examine current fall prevention practices in primary care. Current practices are limited in that they often occur as part of brief clinical encounters where the emphasis is on informing older people about their fall risks, providing evidence-based strategies (e.g., balance exercises), and connecting them to resources to address their fall risks (e.g., physical therapy).37-39 Our findings suggest that it is important to combine clinical recommendations for fall prevention along with providing a safe space for older people to explore and identify what they are capable of and how they could engage in fall prevention. Various clinician team members can facilitate engagement in fall prevention through supportive conversations. In these conversations, re-framing the language of fall prevention is important because older people do not always perceive themselves to be at risk. 34 Furthermore, efforts to understand older people’s perspectives about engaging in fall prevention are essential.
Practice Implications
Our findings inform how best to frame fall prevention conversations and provide individualized support for fall prevention. Because we found that participants’ engagement in fall prevention was influenced by who they are and their capabilities, opportunities, and motivation, we have 2 suggestions for clinical practice. First, we propose that fall prevention assessment should include assessment of the affective domain (e.g., concern about falling, motivation to engage in fall prevention) and cognitive domain (e.g., knowledge about potential fall risks and prevention options) in addition to standardized fall risk assessments (e.g., STEADI fall risk assessment, 4-stage balance test). Assessment of the affective domain, specifically concern about falling, has been strongly recommended by World Guidelines for Fall Prevention and Management for Older Adults. 3 This will help clinicians to understand older people’s baseline readiness to engage in fall prevention and lead to productive conversations around meaningful choices for fall prevention. Second, evoking older adults’ goals for their health and their confidence to reach them is essential for shared decision-making and alignment of care. 40 Therefore, we encourage integrating elements of MI during any conversation about fall prevention to support older people to find meaningful fall prevention strategies in a nonjudgmental and nonthreatening environment. 22 Motivational interviewing skills, such as open-ended questions, reflections on the older adult’s responses, and affirming their abilities, encourage clinical team members to explore older people’s experiences and perspectives about fall prevention to develop therapeutic relationships. 22 For example, the clinician can ask “what being careful means” for fall prevention, as many older people use being careful as their primary strategy to not fall. For those who are highly ambivalent about aging and fall prevention strategies, exploring how they are feeling about changes to their physical capability is a start. It is important that clinical teams ask these questions with genuine curiosity grounded with the knowledge that how a person engages in fall prevention is unique to who they are. Then, with information about what is important for the patient, their goals related to fall prevention can be identified. Finally, further research is needed to explore how MI can be best integrated into clinical workflow to consistently provide individualized support for fall prevention.
Limitations
This study has 3 important limitations. First, this study is an analysis of MI sessions that were provided with a goal to facilitate behavior change and not to answer specific qualitative research questions. Thus, research interview guides were not used and the nature of MI sessions may have shaped how participants described their engagement in fall prevention. The benefit of using this approach was that we gained insight into older people’s engagement in fall prevention in a “natural way” as conversationally skillful clinicians may hear it. We selected initial MI sessions because MI specialists are developing therapeutic relationships and actively exploring participants’ values and perspectives that undergird their engagement in fall prevention. Second, participants in this study were White urban-dwelling older people who chose an academic medical center for their care. Thus, study findings are not generalizable to older people in general. Instead, they provide in-depth descriptions about engagement in fall prevention as a basis for conducting quantitative research in the future that is generalizable. Third, the timing of this study coincided with the COVID-19 pandemic. We captured some examples of how the pandemic impacted opportunities for fall prevention, but it is unclear how the pandemic may have affected participants’ engagement in fall prevention.
Conclusion
We found that participants engaged in fall prevention as a unique combination of fall prevention strategies influenced by their personal view of who I am. Furthermore, each individual had their own story about factors related to their capabilities, opportunities, and motivations that influenced their decisions about whether and how much to engage in fall prevention. Engagement in fall prevention was personalized among participants. This underscores the need for researchers and clinical teams to explore and implement strategies such as MI that can support the uptake of evidence-based fall prevention strategies in a way that aligns with older persons’ priorities, preferences, and beliefs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Institute of Nursing Research and National Institute of Health Office of Directors (grant no. 1K23NR018672-01A1 Award) and Oregon Health & Science University Faculty Initiative Pool Award.