
Abstract
Sex, the states of being female or male, potentially interacts with all xenobiotic exposures, both inadvertent and deliberate, and influences their toxicokinetics (TK), toxicodynamics, and outcomes. Sex differences occur in behavior, exposure, anatomy, physiology, biochemistry, and genetics, accounting for female–male differences in responses to environmental chemicals, diet, and pharmaceuticals, including adverse drug reactions (ADRs). Often viewed as an annoying confounder, researchers have studied only one sex, adjusted for sex, or ignored it. Occupational epidemiology, the basis for understanding many toxic effects in humans, usually excluded women. Likewise, Food and Drug Administration rules excluded women of childbearing age from drug studies for many years. Aside from sex-specific organs, sex differences and sex × age interactions occur for a wide range of disease states as well as hormone-influenced conditions and drug distribution. Women have more ADRs than men; the classic sex hormone paradigm (gonadectomy and replacement) reveals significant interaction of sex and TK including absorption, distribution, metabolisms, and elimination. Studies should be designed to detect sex differences, describe the mechanisms, and interpret these in a broad social, clinical, and evolutionary context with phenomena that do not differ. Sex matters, but how much of a difference is needed to matter remains challenging.
Sex differences in behavior, exposure, anatomy, physiology, biochemistry, and genetics influence toxicokinetics (TK) and toxicodynamics from the molecular to whole animal level, accounting for female–male differences in responses to xenobiotics in humans and other animals. The Institute of Medicine (IOM; Wizemann and Pardue 2001, 2) concluded that “sex matters” and exhorted: “Being male or female is an important fundamental variable that should be considered when designing and analyzing basic and clinical research.” Aside from obvious differences related to sex-specific organs and reproductive events, xenobiotics can interact differently with the male and female sex hormones and their receptors. There remain many gaps in understanding sex differences in toxicology. Much of our understanding of toxic effects on humans stems from industrial toxicology and epidemiologic studies of workforces exposed to high levels of one or more chemicals. In addition to limitations from inexact exposure information, the traditional industrial workforces were almost exclusively male, and females were often absent or in such small numbers that they were ignored by epidemiologists (Zahm and Fraumeni 1995; Craft 2003; Kogevinas and Zahm 2003).
Even when a study comprises both sexes, the analysis might ignore sex differences (Wallace and Gill 1982; Shalat et al. 2003) or adjust for them or may lack gender-specific exposure (Greenberg and Dement 1994). The concurrence of globalization with the widespread entry of women into factories in developing countries offers the opportunity for new wave occupational epidemiology studies, which have the potential to fill the gaps in knowledge about exposure of both women and men to old and new industrial chemicals and particles (Gochfeld 2005).
Until the early 1990s, the U.S. Food and Drug Administration (FDA 1977) recommended against testing drugs on women, particularly women of childbearing age. In 1992, under encouragement from women’s health advocates, the National Institutes of Health and the IOM reported that women were being denied evidence uniquely beneficial to their gender and that legal and ethical issues needed to be overcome (Mastroianni, Faden, and Federman 1994). In response to the growing disquiet and the impending IOM report, the FDA (1993) reversed its position and recommended inclusion of women in drug trials. However, researchers proved reluctant to countenance such a dramatic shift in paradigm, and women continued to be underrepresented. In many cases, female participants were required to certify or even prove that they were taking contraceptives, for fear of liability in the event of pregnancy. Ironically, this imposed a potent biologic influence on the very outcomes of interest (Holdcroft 2007). Contraceptives affect many clinical chemistry and physiology variables as well as DNA methylation, endothelial function, macrophage function, and immune responses, thereby compromising the drug studies supposed to represent all women (Campesi et al. 2012). I calculated that if 40% of U.S. females are of childbearing age (15–44 years, U.S. Census), and 62% of women of childbearing age use contraception (Jones, Mosher, and Daniels 2012) and 68% of these use oral hormones (Guttmacher Institute 2015), then about 16% of females are represented by women in studies requiring hormonal contraception. In other cases, the warnings or releases required by institutional review boards would scare away most women from volunteering, even for low-risk trials.
Some studies that observe male–female differences have determined that they are all due to the average body size differences (Schwartz 2003) without leading to mechanistic investigation. In other cases, statistical adjustment obscured differences. Laboratory research continued to focus on male animals or male cells, perhaps because of a mistaken belief that female development and physiology are intrinsically more variable than males (Itoh and Arnold 2015). The National Institute of Health has tried to engage scientists and expand the use of female animals, tissues, and cells (McCullough et al. 2014); indeed, this has become a controversial requirement for grant funding (Mazure 2016).
Background
This review began with participation in two conferences in 2002 and 2003, and the literature was reviewed in 2005 (Gochfeld 2007) and again in 2015 to 2016 for the presentation at the Society of Toxicologic Pathology. Literature was obtained primarily through the PUBMED access to the National Library of Medicine via the Rutgers University library portal. This was not intended as a comprehensive review but to illustrate the areas in which sex differences had been identified.
In response to the IOM report (Wizemann and Pardue 2001), the Scientific Committee on Problems of the Environment (SCOPE) teamed with the International Union for Pure and Applied Chemistry to sponsor a weeklong symposium on endocrine disruptors (Miyamoto and Burger 2003). The Scientific Group on Methodologies for the Safety Evaluation of Chemicals, an organ of SCOPE, conducted a weeklong workshop on “gender and toxicology” (Klein, Gochfeld, and Davis 2007). The resulting Framework for Gender Differences in Human and Animal Toxicology (Gochfeld 2007) emphasized that sex was not adequately accounted for or analyzed in toxicology, epidemiology, and even in drug development studies. Many studies used only 1 sex, or if both were used, observed sex differences were unexplored (Gochfeld 2007). Toxicokinetic studies focused on metabolism, with absorption differences ignored. Physiologists and ethologists had a well-established sex hormone paradigm involving gonadectomy with and without same- or opposite-sex hormone replacement to demonstrate the primary regulatory role of the sex hormones. Toxicologists were just beginning to use this powerful approach. Other sex differences such as a direct role of genes on the X or Y chromosome were underappreciated. By 2010, there had been little improvement in attention to sex and gender in drug research and clinical practice (Arnold, Chen, and Itoh 2014; Nieuwenhoven and Klinge 2010) or in pharmacology and toxicology research (Gochfeld 2010). Toxicology fared somewhat better than drug development, but under the key words “gender” or “sex,” male–female differences receive scant attention in toxicology texts. For example, Klaassen (2013) has a 1-page entry under gender, none under sex. In an otherwise excellent chapter on solvents, Bruckner, Anand, and Warren (2013) cite our paper (Vahter et al. 2007) and only one 2008 paper in the section on gender.
The Framework was organized around exposure, TK, toxicodynamics, and modulating influences (Figure 1; Gochfeld 2007; Vahter et al. 2007). The present article focuses on TK. Toxicodynamics will require a separate paper.
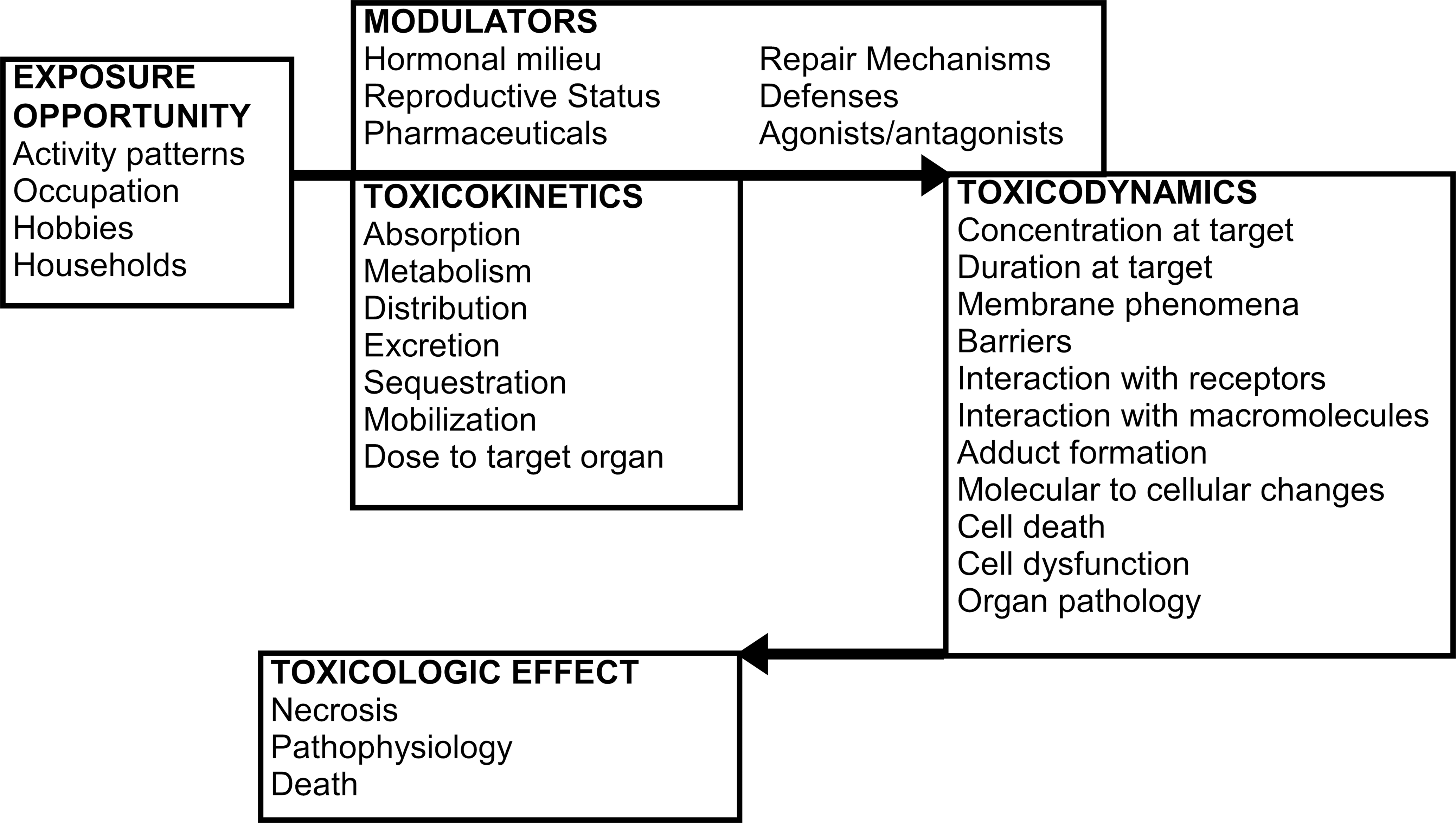
Framework for sex differences in toxicology linking exposure, toxicokinetics, and toxicodynamics (after Gochfeld 2007).
TK encompasses absorption, distribution, metabolism, and elimination (ADME).
Toxicodynamics includes the interaction of a chemical or its metabolites with targets at the molecular, subcellular, and cellular level, resulting in a pathophysiologic effect or organ toxicity (Johnson et al. 1997). Both toxicokinetic and toxicodynamic actions are subject to modification, particularly by the gonadal steroids and growth hormone, by various agonists and antagonists, and by coexposures.
Semantics
Sometime in the 1980s, toxicologists began publishing on “gender differences” rather than “sex differences,” the terminology used in the 1960s (Dubois and Puchala 1961; Munoz et al. 1961). Perhaps it was considered impolite to talk about sex in public. However, sex referring to the genetic/gonadal/hormonal condition of an individual as male or female is different from gender, a state of self-identifying as masculine or feminine—a distinction made painfully clear even to the lay public in 2016 by controversy over bathroom use by transgender individuals. This article uses the term sex, and the author acknowledges having capitulated to the gender movement in the 2007 paper. However, animals do have gender reflected in varying manifestations of aggressive or maternal traits. Franconi and Campesi (2014) compromise using the term “sex-gender differences.” This article uses the term sex to refer to male and female animals and to men and women.
Another semantic issue is the use of “fold differences” in lieu of percentage differences. Thus, a 50% difference would be reported as a 1.5-fold difference. This is often clearer when talking about 10-fold or 100-fold differences in some measure. A 10-fold difference is sometimes represented as a 10× difference or 1,000% difference in the literature.
Sex differences
Sex differences in responses to chemical, physical, biological, or psychosocial stressors are readily apparent, and dramatic differences in how males and females respond to exposures remain challenging. Of particular interest is why some chemicals produce cancer or disease in one sex but not another. Is this grounds for dismissing it or for understanding it (see Cancer section)? Such differences in humans are not unique nor unexpected. Males and female humans have different lifestyles, experiences, and exposures (gender differences), many of which are not technically or ethically amenable to controlled trials. Animal studies, however, offer the opportunity to bypass these differences and focus on sex differences in anatomy, physiology, biochemistry, molecular biology, and behavior. In addition to sex-specific organs and sexually distinctive hormonal axes, males and females may show differences in anatomy, physiology, and biochemistry of the organ systems they have in common. The classical sex hormone paradigm of agonists–antagonists–gonadectomy replacement is increasingly exploited and has been supplemented in the past decade by a variety of knockout mice (Carey et al. 2007) as well as by high-throughput genetic sequencing facilitating advances in various -omics.
Differences between sexes can be broken down as (1) sociocultural, (2) exposure, (3) body size and composition, (4) genetic–molecular–biochemical, and (5) hormonal and reproductive, including pregnancy. This review focuses on the adult male and female (nonpregnant), with the recognition that differences may be altered during development, during estrous or menstrual cycles, or by pregnancy. Some of the sex differences in anatomy, physiology, and pharmacology arise from the larger average size and mass of males in various species, and therefore the average larger volume and mass of male organs compared with females. In many papers, physiologic variables are “standardized” for body mass or surface area that partially corrects for the body size differences (Nair and Jacob 2016). But it is too easy to “blame” observed differences on biometrics alone, while ignoring biology.
ADRs
Much of our knowledge of ADRs comes from spontaneous reports by patients or doctors to various pharmacovigilance systems in different countries (Ryu et al. 2015). These suffer from selection bias with more severe ADRs more likely to be reported. Across nations (Ryu et al. 2015; Patel and Patel 2016), women report more ADRs than men, partly reflecting a machismo attitude among males and partly reflecting actual susceptibilities. A Dutch study reported that women were more likely than men to volunteer for a web-based pharmacovigilance survey program for altruistic reasons (Härmark et al. 2013). Rademaker (2001) estimated a 50% increased risk of ADR for women, while Nakagawa and Kajiwara (2015) estimated a 2-fold increased risk across “all drug classes,” and women had more severe ADRs more likely to require hospitalization. This ADR sex difference is not apparent in childhood (Damien et al. 2016).
The heightened response of female rats to anesthesia has been known for almost a century (Nicholas and Barron 1932). Women may require higher doses of some drugs, while being more sensitive to respiratory depression and waking sooner. ADRs can be related to overdose and toxicity of the desired pharmacologic effect or to side effects unrelated to the primary mode of action. The former are dose dependent, the latter more likely to be idiosyncratic and possibly dose independent. ADRs frequently arise from drug interactions, so simply taking more medications creates both an arithmetic risk increase (more drugs leads to more risk) and a multiplicative risk (interaction). Both TK and toxicodynamics play roles in ADRs.
Calabrese (1985) published a list of pharmaceuticals already known to affect males and females differently. Compared with men, women respond well at lower doses of psychoactive drugs (Seeman 2004; Maron et al. 2004). At the same dosage regimen of fluoxetine (Prozac), women showed a greater cortisol reduction than men (Bano, Akhter, and Afridi 2004). This could be due to a higher concentration of the drug at the target (toxicokinetic) or altered metabolic profile. The difference in rates of ADR probably has multiple causes, both pharmacokinetic and pharmacodynamics (Miller 2001; Anderson 2008). Most of the FDA drug bans are based on toxic effects in women (Heinrich 2001). These effects might have been recognized earlier if women had been represented in the drug development trials.
Is the ADR risk because women take relatively higher doses? Are the relatively higher doses a function of inadequately studied pharmacokinetics or pharmacodynamics. Do women take more medications in general, thus increasing their risk arithmetically, or is it “simply” that women are more likely to report perhaps more mild events. All of these probably contribute (Anderson 2008). Paradoxically, one study found that the ADR reports by women are more serious and more likely to result in hospitalization (Miller 2001), for example, sodium phosphate induced nephropathy (Ehrenpreis et al. 2011). But a U.S. study of 2,341 fatal ADRs found males overrepresented (Shepherd et al. 2012). Females also experience more allergic and hepatotoxic effects from a variety of drugs (Anderson 2008).
Using the Dutch National Medical Registry, Rodenburg, Stricker, and Visser (2012) found about 1/3 of ADRs requiring hospital admissions were attributable to cardiovascular drugs, with women only slightly overrepresented (55%). Women were significantly more likely to suffer from diuretics and cardiac glycosides and less prone to ADR from coronary vasodilators. In Korea, women were overrepresented in ADRs due to drugs but not due to contrast media ADRs (Ryu et al. 2015).
Among the most serious ADRs are cardiac arrhythmias, which can be caused by cardiovascular drugs or noncardiovascular drugs (Frommeyer and Eckardt 2016). Noncardiac medications may cause Brugada syndrome (males at greater risk) or long QT interval (females at greater risk), both of which may lead to fatal arrhythmias (Konigstein et al. 2016). The commonly used opiate pain medication, tramadol, has primarily nervous system toxicity but also affects the electrophysiology of the heart. Among 1,400 tramadol poisoning cases, electrocardiogram abnormalities were identified in a third, with males significantly overrepresented among the tachycardia and S-wave abnormalities (p < .0001) and females significantly overrepresented among long QT interval and right bundle branch block (Ghamsari, Dadpour, and Najari 2016).
Anatomy, body and organ size, composition and physiology
Across human societies, males average taller and heavier than females with relatively more muscle mass and lower body fat. These anatomical differences have received more attention than physiologic differences. The body weight difference is used to correct organ weights and physiologic metrics or to scale therapeutic doses for females (Nair and Jacob 2016). The International Commission on Radiological Protection (ICRP) developed its “reference man” to assist in calculating radiation doses to organs. ICRP 89 (Valentin 2001) provided mean values for percentage body composition for adult males and females (Table 1). The data were not intended for physiologically based pharmacokinetic modeling and were therefore limited by the lack of distribution parameters (Gochfeld 2007). Some of the key variables such as renal clearance (Cl) are not provided.
Absolute and Relative Body Composition for Adult Caucasian Men and Women Extracted from “Reference Man Table” 2.8 in the International Commission on Radiological Protection (ICRP Publication 89, Valentin 2001).
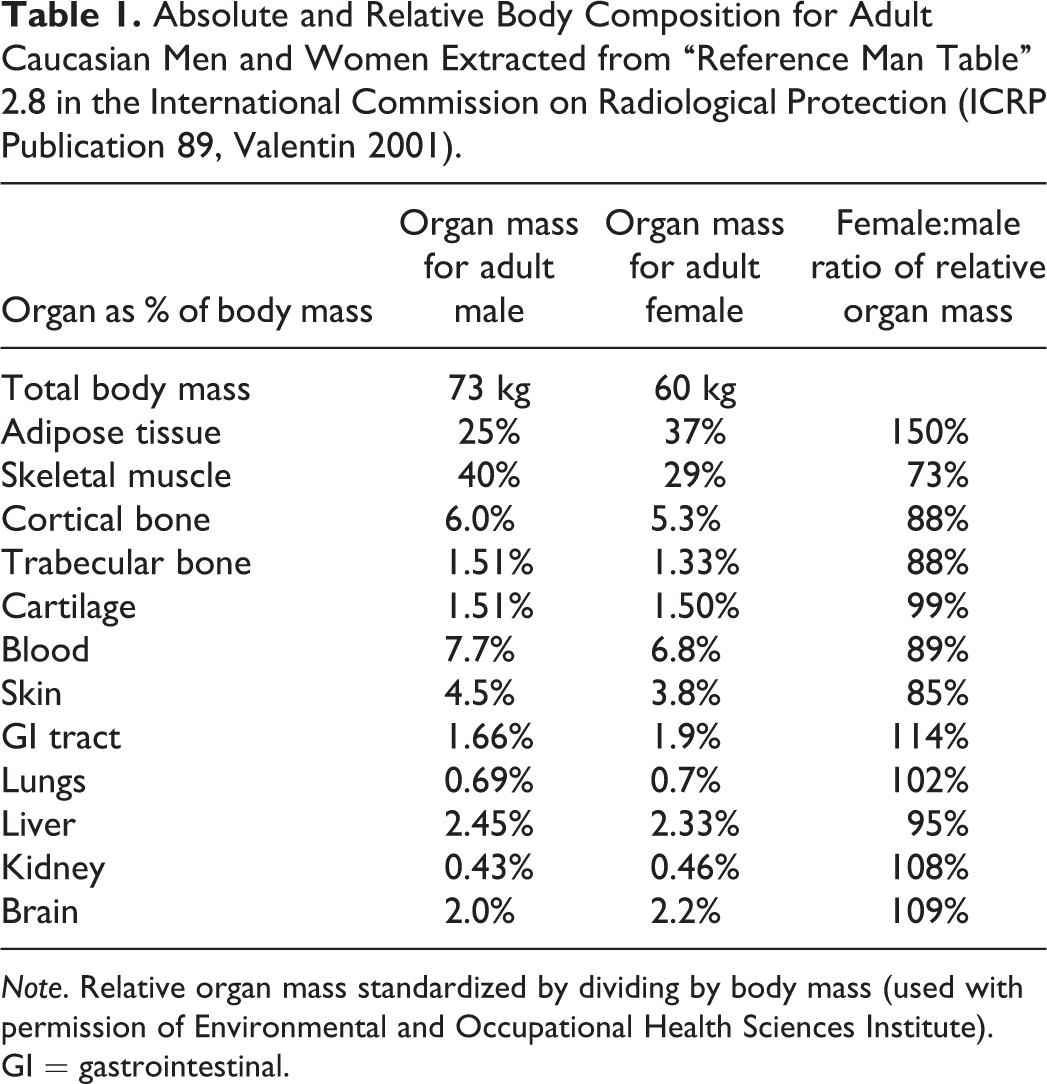
Note. Relative organ mass standardized by dividing by body mass (used with permission of Environmental and Occupational Health Sciences Institute). GI = gastrointestinal.
To standardize the morphological differences, the ICRP data were converted to percentages of organ weight divided by body weight (given as 73 kg for adult males and 60 kg for adult females), and I examined the ratio of these relative organ weights for females versus males (Table 1). For most organs, there is less than a 10% difference in the weight-corrected values; however, the ratio for adipose tissue was 50% higher in females. Females also had relatively heavier pituitaries (21%), adrenals (13%), and gastrointestinal (GI) tract (14%), while males had higher total lung capacity and vital capacity (13%), blood (11%), bone (12%), skin (15%), and particularly skeletal muscle (27%; Valentin 2001). There was only a slight difference (6%) in the body mass to surface area, 38.4 kg/m2 for males versus 36.1 kg/m2 for females. Thus, substantial differences persist even after scaling for body weight.
Male and female adult mice are generally very similar in body weight. B6C3F1 average 46.2 g (males) and 46.4 g (females), with males weighing more in youth and females more at 18 months in some strains (Rao 1999). Males tend to grow fast and are then slightly surpassed in weight by adult females. Rats, on the other hand, show much greater sex dimorphism. Pooling control rats from 26 studies, Bailey, Zidell, and Perry (2004) found quite different organ/body weight regressions between females and males for liver and kidney with greater similarity with brain weight as the denominator.
Related to anatomic size differences are average physiologic differences between men and women. The differences in forced vital capacity are documented in reference standards for spirometry, but there are inconsistencies: with heavy exercise, women have higher maximum ventilation rate (from table 2.32 in Valentin 2001). Relative cardiac output is higher in women (1.1-fold), while men have higher blood volume (1.2-fold: Valentin 2001). The basal metabolic rate (BMR) of women is given as 52 kcal/hr compared with 68 for men; thus, standardized for body mass, the female BMR is 93% compared with men, while weight standardized total energy expenditure is 78% of male (i.e., 22% or 1.3-fold lower energy intake per day), reflected in average calories consumed. Risk assessors use a default value of 2 L/day for adult drinking water intake, which is a good approximation of the 1,960 ml/day for females, but underestimates the 2,600 ml/day for males (from table 2.30 in Valentin 2001).
Sex hormones and the sex hormone paradigm
Mammals have heterogametic sex determined in the embryo by whether it is XX (female) or XY (male). The Y chromosome carries the sry gene that directs the sex differentiation, formation of the fetal testis, and whether the fetus will be bathed in testosterone and develop into a male. Genes on the sex chromosomes directly influence brain development as well as determine the hormones which indirectly exert many effects. In both sexes, androgens influence brain function (National Research Council [NRC] 2005). Steroids can modify gene expression, even stimulating neurons to generate new or discard old synapses (Kawata, Yuri, and Morimoto 1994).
The estrogenic and androgenic hormones and their receptors vary throughout the life cycle. The estrous/menstrual cycle in females superimposes a dramatic short-term cycle as well. Since the mid-1900s, physiologists and ethologists (Fraps 1955; Murton, Thearle, and Lofts 1969) and more recently toxicologists have explored the influence of estrogenic and androgenic hormone systems on a wide variety of behavioral and physiologic phenomena. A typical experimental sequence would include (1) observing sex differences, (2) gonadectomy, (3) replacement with same-sex hormone, and (4) replacement with opposite sex hormone. Later modifications included (5) experiments with agonists and antagonists, (6) studies with genetically modified animals (knockouts), and finally (7) separation of genetic sex from gonadal sex by manipulating the sry testis-determining gene (Arnold and Burgoyne 2004). See Arnold, Chen, and Itoh (2014) for recent summary.
Some of the genes that have very great fold differences are located on the Y and X chromosomes (Yang et al. 2012). To what extent do these impact development separately from determining the sex hormone environment. This required the separation of genetic and hormonal sex. Arnold and Burgoyne (2004) relocated the testis-determining sry gene from the Y chromosome to an autosome by transgenic insertion. Upon successful breeding, this produced XX as well as XY males and XY as well as XX females. They found fewer than 10 genes differentially expressed in XX versus XY males and XX versus XY females, indicating few genes are regulated directly in the absence of sex hormones (Van Nas et al. 2009; Arnold, Chen, and Itoh 2014).
Organisms, such as almost all vertebrates, that have separate sexes, manifest dimorphic behavior, particularly with regard to reproduction, controlled by sex-specific brain centers that may add new neurons or contract under hormonal control. These are linked to various cycles including annual photoperiod. Significant sex differences occur in centers corresponding to touch and olfaction in nocturnal mammals and to vision and hearing in birds (Nottebohm and Arnold 1976).
An attractive feature of the sex hormone paradigm is its elegant logic. However, it sometimes raises more questions than it answers—not just is some variable influenced by hormones, but how, when, and even why? In some cases, there are disconnects, when gonadectomy reduces a behavior, but replacement does not restore it. For example, in male animals, estrogen does not always have the same effect as castration. Two examples of the “classic sex hormone paradigm” are shown in Table 2.
Application of the Classic Sex Hormone Paradigm to Examine Sex Differences in Elimination of Perfluorooctanoic Acid and in the Expression of CYP2J5 in Mouse Kidney.
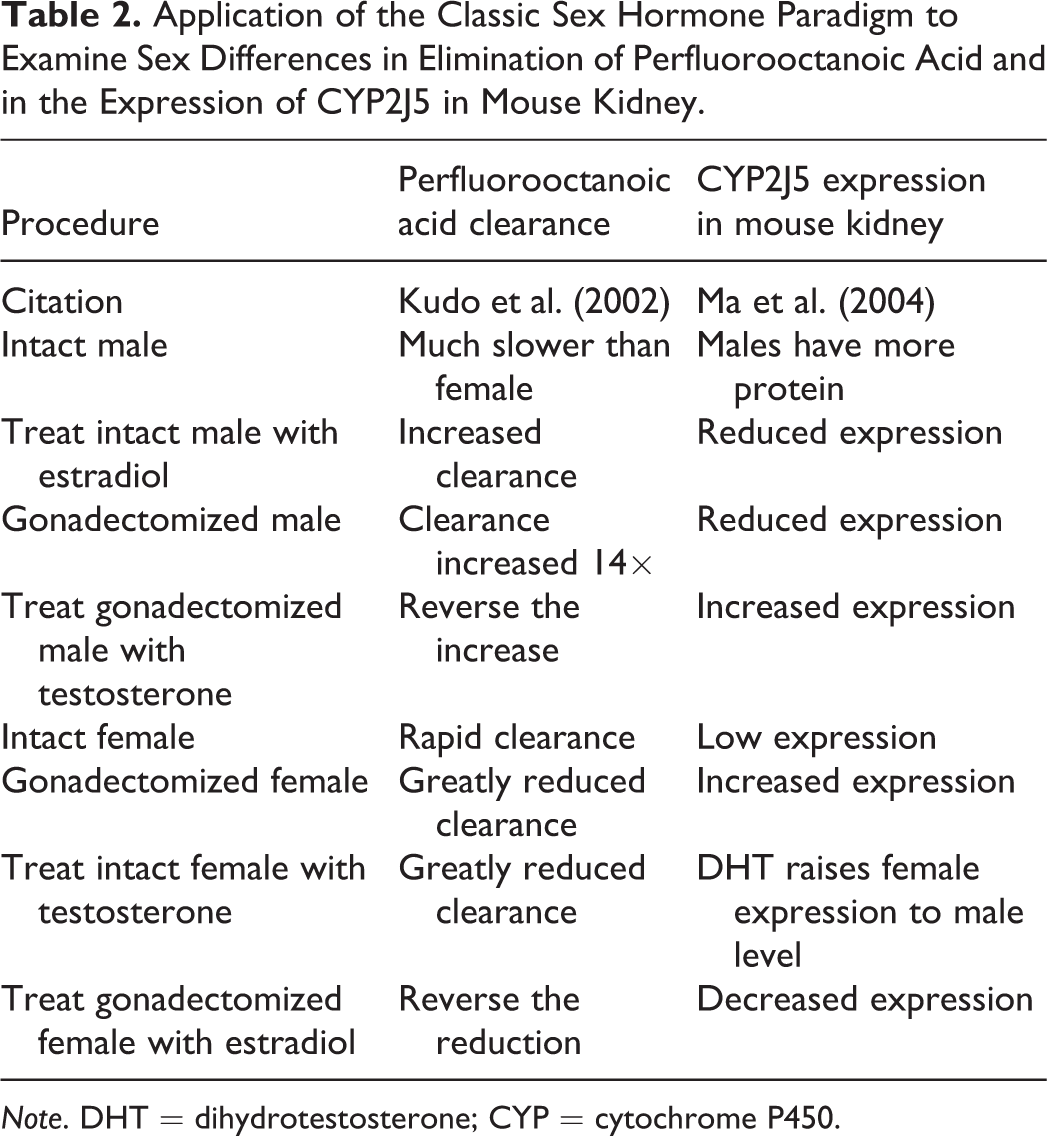
Note. DHT = dihydrotestosterone; CYP = cytochrome P450.
Some examples of renal Cl fit the classic sex hormone paradigm. Perfluorooctanoic acid (PFOA) has attracted increasing attention because detectable residues of this persistent organic pollutant are almost universal in human and animal tissue. PFOA is eliminated via an organic anion transporter (OAT) in the renal tubule, but the half-life is 70 times longer in male than female rats (Worley and Fisher 2015). Estradiol treatment or castration speed elimination in males, while subsequent testosterone treatment lengthens it. Ovariectomy slowed Cl in females and estradiol restored it (Worley and Fisher 2015).
Intrauterine position: Rodents have gender
Nature conducts its own sex hormone intervention in animals that have litters and perhaps in humans. In boy–girl (MF) twin gestations, there is inconsistent evidence regarding possible masculinization of the female sib, exposed to her brother’s androgens through twin testosterone transfer (TTT). For example, cognitive effects have been reported, such as greater mathematics aptitude, reviewed skeptically by Ahrenfeldt et al. (2015). Also females from MF twins had larger tooth dimensions than those from girl-girl (FF) twins (Ribeiro et al. 2013). The evidence is sufficient to warrant further investigation in humans (Tapp, Maybery, and Whitehouse 2011); however, Ahrenfeld et al.’s (2015) study of 9th graders found no difference in school performance on either visuospatial or language skills between girls from FF or MF twins. Since twin studies are popular, the paucity of evidence indicative of TTT in human twins suggests that it is minor and/or rare.
In animals, however, testosterone transfer is well established in mice and gerbils that have large litters (vom Saal and Bronson 1980). Female embryos lying between 2 males (2 M females) later exhibit more male-typical behavior than 0M or 1M females, including mounting receptive females. Similarly, 2F males have different behavior and lower reproductive success than 2M males. The intrauterine hormonal environment affects anatomy (anogenital distance), maturation (vaginal opening), sexual maturity, aggressive behavior, hormone production, mating and fertilization, and fecundity (Clark, Vonk, and Galef, Jr. 1998). These gender differences are a significant potential source of individual variability with impacts particularly on behavioral and reproductive toxicology. Having a contiguous male fetus increased masculine behavior of male rats, decreased female behavior in female, and increased weights at gestation day 21 of both sexes, without affecting anogenital distance (Hernández-Tristan, Arevalo, and Canals 1999).
Growth hormone
Growth hormone plays multiple roles in regulation of sex-dependent gene expression (Waxman and O’Connor 2006). Many of the cyp450 genes are upregulated by growth hormone. In rats and mice, the male–female differences in cytochrome P450 (CYP) expression may exceed 500 fold, such that some isoforms appear sex-specific. Similar but smaller differences are seen in humans. The transcription factor and signal transduction cascade were worked out by Waxman and O’Connor (2006). The schedule of growth hormone release differs. In human females, growth hormone is released at a relatively continuous level, which increases CYP3A4 expression in the liver in response to dexamethasone, while pulsatile releases characteristic of males suppress it (Dhir et al. 2006). This effect is less marked in humans than in rats. Similarly, CYP2C11 expression is regulated by growth hormone in the spleen and thymus (Thangavel et al. 2007).
Exposure
The 2007 Framework addressed sex differences in exposure opportunity and contact related to behavior and occupation in the home, community, and workplace environment (Gochfeld 2007). The present article assumes many actual or potential sex and gender differences in exposure. Behavioral differences subsumed under “lifestyle” directly affect contact and intake. For examples, smoking is damaging to both sexes, but males and females smoked differently, with males inhaling more per cigarette, while women held cigarettes close to their face and experienced greater sidestream smoke (Burger and Gochfeld 1990). Beyond humans, male and female mammals and birds exhibit different individual and social behavior that influences consumption of nutrients and toxicants (Burger 2005). Sexual dimorphism, dominance, and social groupings are important in the wild and intrude on laboratory studies as well. Males and females differ in locomotor and exploratory activities and energy intake related to dominance, mating, and reproduction. Assuring equal dietary intake usually requires paired gavage feeding, bypassing important parts of the upper GI tract.
Endocrine disruption
There are major sex differences in targets of endocrine disruption. Peakall, Miller, and Kinter (1975) presented mechanisms by which chlorinated hydrocarbon pesticides induced hormones that degraded estrogen, interfering with egg production in birds such as pelicans, eagles, and falcons, resulting in extinction of some bird populations within a 20-year period. Publication of “Our Stolen Future” (Colburn, Dumanski, and Myers 1996) revived and focused interest in endocrine active substances in the environment affecting humans, resulting in substantial research (see papers in Miyamoto and Burger 2003) on sex differences including, for example, synthesis and release of proteins and hormones, up- or downregulation of receptors, nonsteroidal agonists (activation binding), nonactivating receptor binding (competitive inhibition), nonhormonal mimics or antagonists (receptor or nonreceptor mediated), altered metabolism (increased or decreased breakdown), and altered transport quantity or free: bound ratios.
This rapidly expanding field of inquiry intersects TK and toxicodynamics and is beyond the scope of the present article.
Toxicokinetics
TK is divided into 4 processes: absorption, distribution, metabolism, and elimination. These can be viewed as taking over where exposure ends. TK determines the amount of an active agent circulating in the blood and delivered to a target organ, where many other factors combine to determine whether there is a toxic effect such as an ADR (Leming and Baitang 2012). Xenobiotics can be inhaled from air, ingested from food or water, absorbed through skin, or injected. Absorption through the alveolar–capillary membrane (lung), the GI mucosa, or the skin depends on a variety of chemical, medium, and intrinsic biologic factors. Substances may differ in their bioaccessibility (ease of release from the environmental media, diet, or tablet) or in the absorptive capacity of the organ–blood interface (Burger et al. 2003). Absorption may be passive (diffusion) or active, facilitated by transporters. Together these phenomena influence the circulating concentration of the xenobiotic, its peak concentration (C max) available to reach target organs (their biologically effective dose), and the duration of effect measured by the area under the curve (AUC), which can be terminated at any time or carried out to infinity. The total volume in which a substance might be distributed at any time, the volume of distribution, is designated V d. It comprises the blood, extracellular and intracellular fluid, and body fat. The time from dosing to reach C max is designated T max. The phenomenologic approach to TK can be seen in reports of blood or plasma concentrations, AUC or half-lives (T 1/2) of chemicals, particularly pharmaceuticals. Sex differences in these metrics may arise due to differences in any of the stages of TK.
Xenobiotic concentrations in blood depend on the volume of distribution and rates of Cl from the blood. Even corrected for body weight, males have higher blood volume and females have higher body fat content (Anderson 2008). Females have somewhat lower average renal Cl (lower glomerular filtration rate [GFR]). Xenobiotics are eliminated from the body (or in some cases deposited in repository organs), and the elimination or Cl curves have been quantified for many substances, each with its own half-life (T 1/2) in the body as a whole and in different compartments.
Many of the toxicokinetic studies of xenobiotics focus on the blood level of the drug (or active metabolite) without being able to or even trying to define how such differences arise or persist—the black box approach. Greater body mass and blood and fluid volume and lower body fat explain only part of the difference (Schwartz 2003).
Fletcher, Acosta, and Strykowski (1994) identified 30 studies from 1980 to 1993, reporting sex differences in TK for nutrients, ethanol, and pharmaceuticals. Cl was one of the common measures with males exceeding females in 17 of the 29 cases, a few by a large margin. Clewell et al. (2002) reviewed toxicokinetic data to identify age-specific or sex-specific vulnerabilities for risk assessment and found many age differences but not many sex differences (designated M = F in Table 3 adapted from Clewell et al. 2002). For most toxicokinetic functions, the data were deemed insufficient. Most differences identified were subtle.
Clewell et al. (2002) Reviewed the Literature on Toxicokinetics with Regard to Male/Female Similarities or Differences.
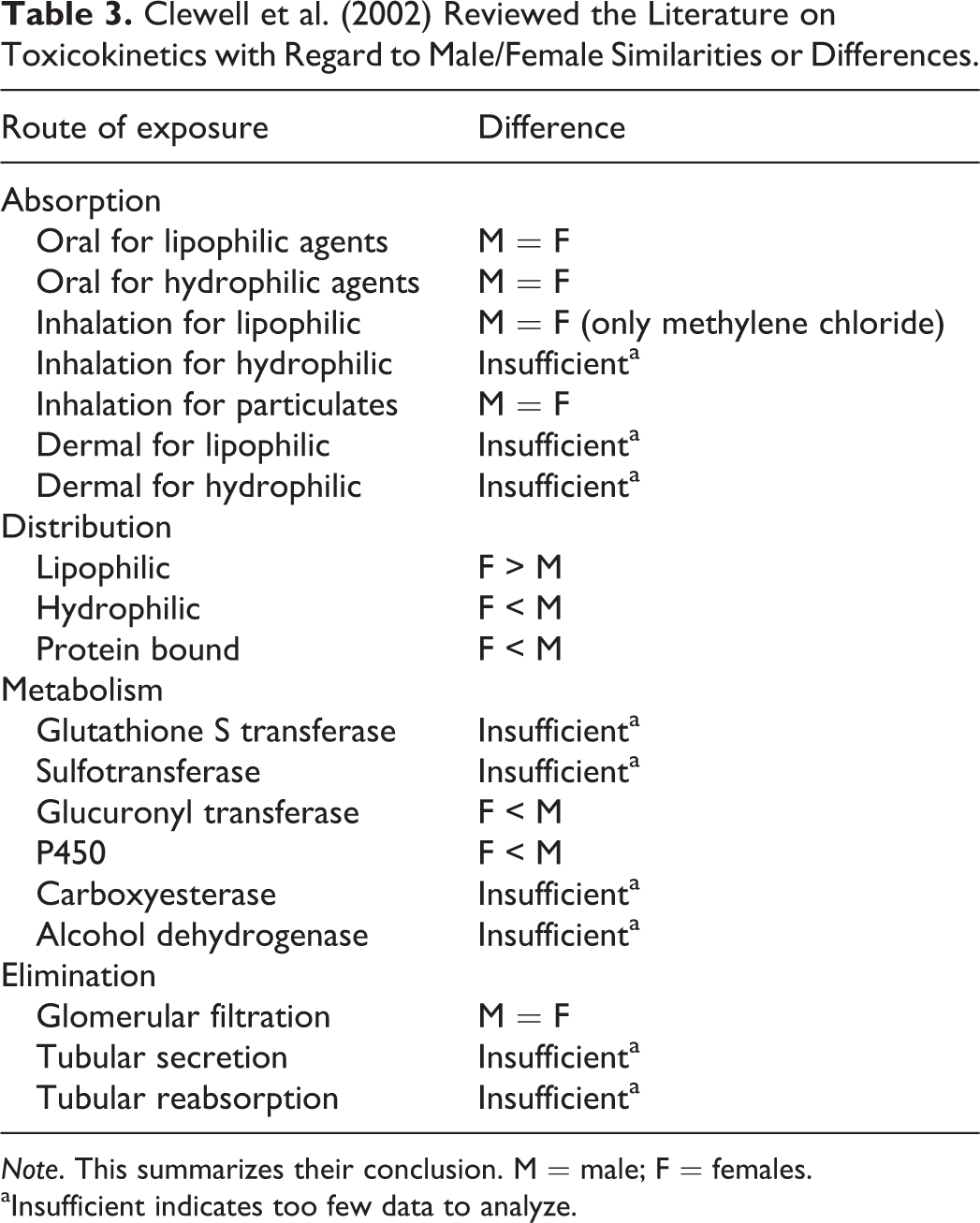
Note. This summarizes their conclusion. M = male; F = females.
aInsufficient indicates too few data to analyze.
Absorption
Absorption or permeability refers to the ease with which a substance that is bioavailable can be transferred into the blood either through passive diffusion or active transport. The intravenous route for a dissolved substance results in 100% transfer to the blood stream. Comparison of the blood level achieved by other routes is considered a measure of bioavailability. Absorption can occur through the lung, GI tract, or skin.
Although bioavailability has been studied extensively, absorption has proven less tractable. Studies of sex differences in GI absorption have been sparse (Walsh 1997; Clewell et al. 2002). Schwartz (2003) believed that absorption was generally less efficient in females for a variety of substances. Sex differences in the metabolic enzyme expression or activity in the gut wall could modify absorption (Beierle, Meibohm, and Derendorf 1999).
Once a substance contacts the alveolar–capillary membrane, the GI mucosa, or the skin, there is an opportunity for passage into the blood stream and thence throughout the body. The substance may undergo metabolism by the microbiota or by the enzymes in the respiratory or intestinal tracts. Toxicologists often choose a parenteral dosing route specifically to avoid the vagaries of intake and absorption. Hydrophilic and lipophilic substances have different absorption properties. This spectrum of properties is often described by the octanol: water partition coefficient between 2 phases or media. Transport across the mucosal surface may be by passive diffusion (lipophilic xenobiotics) or by carrier-mediated facilitated transport. Energy-dependent active transport results in absorption against a concentration gradient. Nonpolar solvents are generally efficiently absorbed (the usual assumption is 100%), so there is little room for male–female differences in absorption for this class of compounds. Many risk assessments simply assumed 100% absorption, essentially ignoring that important phenomenon (Burger et al. 2003).
Strongly hydrophilic substances are poorly absorbed. Vesicle packets involved in endocytosis and exocytosis are important for certain large molecules, such as the absorption of vitamin B12. Beierle, Meibohm, and Derendorf (1999) did not find support for consistent sex differences in GI absorption prompting Clewell et al. (2002) to list M = F for both lipophilic and hydrophilic substances.
GI tract
In the GI tract, absorption is influenced by pH, gastric emptying time, and intestinal transit (Fletcher, Acosta, and Strykowski 1994), and by surface area of the organ, as well as the presence of transporters, concurrent intake, and the microbiome (Dietert and Silbergeld 2015). Women secrete less gastric acid and have slower gastric emptying (Clewell et al. 2002), and this difference is heightened in pregnancy (Fletcher, Acosta, and Strykowski 1994).
Absorption can be passive or active (Rozman and Klaassen 2001), and great advances have been made in characterizing transporters and identifying their ligands as well as the underlying control of expression. It has long been known that children absorb a much higher percentage of ingested lead (ca. 50%) than do adults (ca. 10%; Agency for Toxic Substances and Disease Registry 1999). It is likely that this reflects upregulation of divalent cation transport in order to maximize the absorption of calcium needed for the growing skeleton—lead just comes along for the ride (Vahter et al. 2007). Women are much more likely than men to have depleted iron stores, and they have significantly greater absorption of cadmium from the diet than men or than women with normal iron stores (Vahter et al. 2002; Berglund et al. 1994). Acetaminophen was administered to rats, and intestinal absorption was quicker and greater in females (Raheja, Linscheer, and Cho 1983).
Several sugars characterized by absorption in different parts of the intestinal tract are used clinically to determine permeability of the GI tract. A study of age × sex interaction found that permeability for lactulose and sucralose declined with age in females but not in males (McOmber, Ching-Nan, and Shulman 2010). The authors could only speculate that this is “hormonal,” perhaps related to glucocorticoids which alter permeability in rats as well as human.
Respiratory tract
In humans, airflow through the pulmonary tree may differ due to geometry, resulting in different flow rates, impaction, and turbulence (Valentin 2001). Male mice are slightly larger than females and have higher tidal volume, flow rates, and ventilation rates (L/min). The higher tidal volume in male mice is not solely anatomical, since Estrogen Receptor (ER)-alpha knockout mice show a reversed pattern (higher tidal volume in females; Card et al. 2006).
There are few sex differences in absorption of airborne substances, either volatile or particulate from lung; based on a small sample of 8 men and 9 women (Ernstgård et al. 2003), Clewell et al. (2002) found data only for methylene chloride and for particulates also with no male–female difference. In rats, males absorb more manganese from a manganese sulfate aerosol than females (Dorman et al. 2004). Conversely, exposure to inhaled lead acetate resulted in higher lead concentration in the lung of females, but greater cytotoxicity in males (Fortoul et al. 2005).
Dermal absorption
Area of contact, skin thickness, intactness, keratinization, and blood flow influence uptake through the skin. Sex was not addressed in their review of dermal absorption (Wester and Maibach 1997; Bronaugh and Maibach 1999). The ICRP reference reports no difference in epidermal thickness by sex (Valentin 2001). Bronaugh, Stewart, and Congdon (1983) documented some differences in rat skin permeability. A human study showed that men had slightly but significantly higher transepidermal water loss than women (Chilcott and Farrar 2000).
Dermal absorption of bis(2-chloroethoxy)methane was compared in male and female rats and mice. Absorption was more rapid and higher in rats than mice, and females of both species had higher absorption reflected in higher C max and AUC (Waidyanatha et al. 2011). Bathwater exposure to chloroform resulted in equal uptake (measured by exhaled breath) in men and women at 40°C, while men absorbed about 50% more at 30°C (Corley, Gordon, and Wallace 2000).
Trichloroethylene (TCE) is absorbed through the skin more by females than males. In rats, dermal penetration was 2-fold greater in females than males. Gonadectomy of males increased TCE uptake in a rat skin preparation, reflected in the AUC. Testosterone decreased dermal penetration in skin from females (McCormick and Abdel-Rahman 1991).
Distribution
Transport
Once absorbed, a xenobiotic distributes itself in the blood, and lipophilic substances quickly move into fat, such that fat becomes part of the volume of distribution. For a lipophilic drug, women had a 28% greater V d, while for water-soluble drugs, the V d was 36% lower in females (Wilson 1984). The transport and distribution of lipophilic and hydrophilic substances was one of the few areas of sex difference reported by Clewell et al. (2002), and for some chemicals normalizing for lean body mass, erased much of the sex difference (Beierle, Meibohm, and Derendorf 1999). The xenobiotics and their metabolites are transported in the blood either “free”: dissolved or in ionic form, or “bound to protein. Albumin is the major transport protein for the many chemicals and their metabolites. Nutritional factors influence the availability of protein for binding, but this is probably not a limiting factor. Metallothioneins (MTs) are low molecular weight proteins rich in sulfhydryl groups that bind cations. The physiologic role is to transport zinc, but other metals have a high affinity for MT, which can transfer the metal to the kidney for elimination. After a cadmium injection, male mice (9 weeks old) had greater MT-mRNA than females, but this was not apparent at 4 weeks or 46 weeks. Ovariectomy resulted in a 1.25-fold increase in MT-mRNA that was reversed by estradiol, and conversely MT-mRNA was reduced in males receiving estradiol (Sogawa et al. 2001). Females average more body fat and greater storage of lipophilic contaminants (Valentin 2001).
The free:bound ratio influences the bioavailability of the substance, changes the chemical properties, influencing how transport occurs between the capillary and interstitial space (O’Flaherty 1997).
Transporters into cells
The endothelial wall and adjacent cell membrane poses a potential barrier to substances in the blood stream. Lipophilic substances readily pass from blood to extracellular fluid and into cells. Males and females may differ in the expression or function of transporters. Female mice retain more ascorbate than males, attributed to a difference in the ascorbate transporter (Kuo et al. 2004). The world of transporters has grown dramatically in the past decade. Rapid progress means simultaneous discoveries and variable nomenclature. The ABCG2 efflux transporter, also known as the breast cancer resistant protein from its role in resistance to chemotherapeutic drugs, shows different expression patterns in rats and mice and humans. Male rats and mice had higher expression than females. Sex hormone manipulation revealed that the expression in male rat kidney was due to suppressive effect of estradiol, while in mouse liver, it was induced by testosterone (Tanaka et al. 2004).
One group of transporters attracting attention are the multidrug and toxin extrusion transporters, moving organic molecules (including anticancer drugs) into and out of cells, which are expressed differently in males and females (Lickteig et al. 2008).
Metabolism
Metabolism offers a rich literature on sex differences, particularly for organic, xenobiotics, and phase I metabolism. There is great variability among species, strains, developmental stages and sexes, as well as among organs and chemical substrates. Gene expression differences can be reflected in measurements of specific mRNA, protein, or in enzyme activity. There may be sex differences in constitutive levels as well as in inducibility by different substrates (Iba et al. 1999). The well-established sensitivity of female rats to barbiturates attributed to hepatic metabolism is an example of different amounts or activities of phase I enzymes (Czerniak 2001).
In our laboratory at Rutgers University, we developed an ecotoxicology model based on the ubiquitous, native, long-lived, white-footed mouse (Peromyscus leucopus). We analyzed a wide variety of phase I and phase II enzymes in both sexes at different ages from 6 months to 48 months (Guo et al. 1993) and showed that males had significantly higher microsomal P450 content as well as NADPH-CYP oxidoreductase activity at all ages, and many of the P-450 enzyme activities were higher in males. Females showed age-dependent decreases for several enzymes between 6 months and 24 months of age, which was less apparent in males.
Phase I and CYPs
Phase I metabolism involves a variety of reactions including oxidation, hydroxylation, and epoxide formation which occur in many organs, predominantly in the liver. Metabolism changes the chemistry, distribution properties, and toxicity of the original xenobiotic, detoxifying some chemicals and activating others. Metrics include concentration of the xenobiotic or metabolite in blood or their ratio, measures of enzyme amount or activity, and measures of gene-specific mRNA.
Attention has focused particularly on the CYP families (Parkinson 2001), with measurement of the specific mRNA expression, or the amount of enzyme protein, and/or the enzyme activity (ratio of parent to metabolite). In the 1980s, when researchers worked with microsomal fractions and P450s were lumped together as “mixed function oxidases” (MFOs), before the classification of families and isoforms, sex differences were already apparent. Raheja, Linscheer, and Cho (1983) recognized that females were less susceptible to substances “metabolized by the P-450 MFO system.” They dosed rats with acetaminophen and documented that liver damage appeared earlier and progressed to greater severity in male rats. By 6 hr, females had eliminated 24% of the dose compared with 17% for males (about 1.4-fold difference). Females also showed greater depletion of glutathione. Sex differences for several of the CYP isoforms for several studies are summarized in Table 4.
Male–Female Expression and/or Activity Comparisons for Selected CYP enzymes.
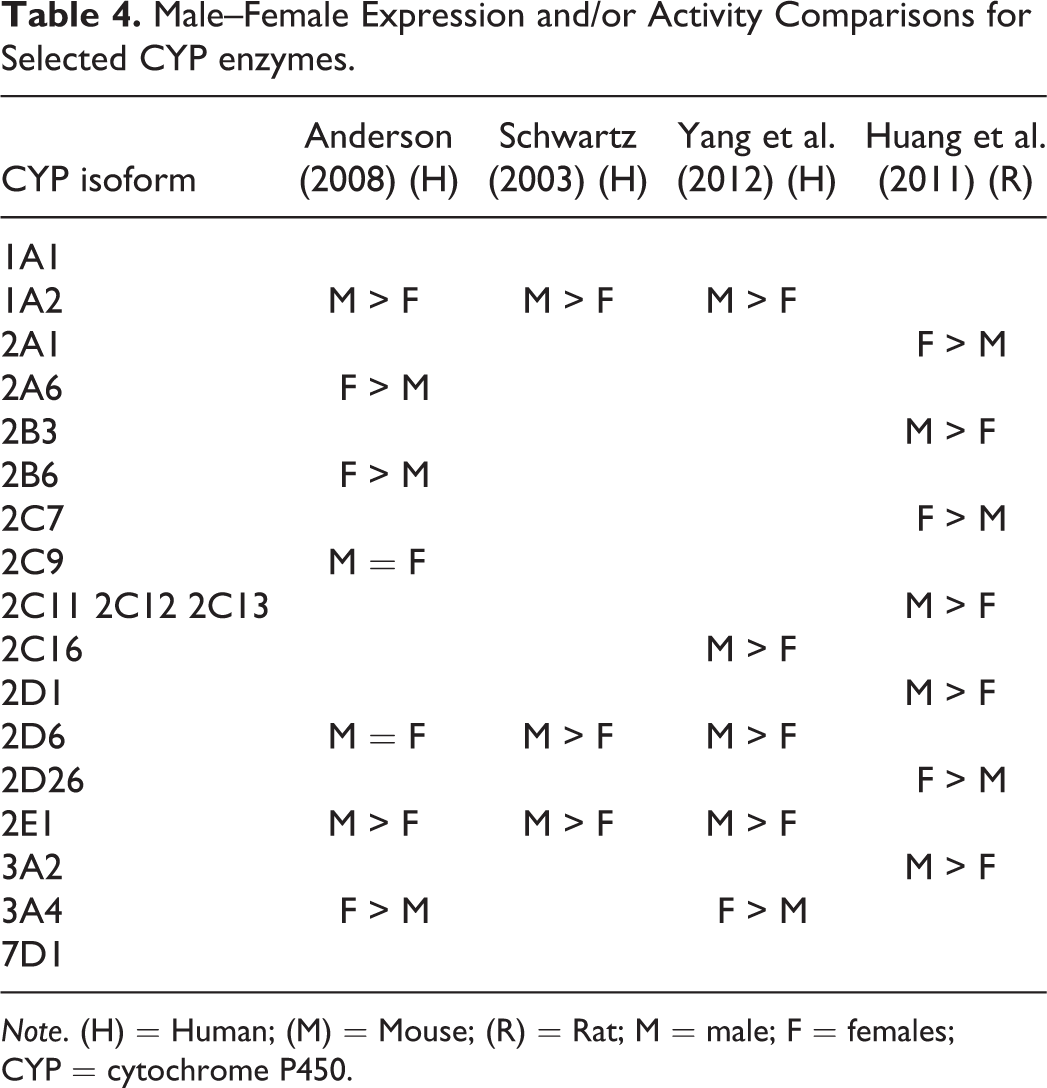
Note. (H) = Human; (M) = Mouse; (R) = Rat; M = male; F = females; CYP = cytochrome P450.
In their review, Clewell et al. (2002) found evidence of higher activity of CYP1A2, CYP3A4, CYP2D6, and CYP2E1 in males. In humans, Mahgoub et al. (1977) found a bimodal distribution in the debrisoquine/4-OH debrisoquine ratio, attributable to a single autosomal gene mutation and Kahn et al. (1985) found slower hydroxylation in female mice of several strains. “Poor” versus “extensive” metabolism of this antihypertensive drug is now known to be related partly to polymorphisms in CYP2D6, one of the main drug-metabolizing enzymes.
In some cases, the sex difference is greater than 10-fold. For example, male rats treated with monochloroacetate had a 45× increase in liver injury enzymes after exposure to chloroform, reflecting a sex difference susceptibility (Davis and Berndt 1992). Sex differences in CYP1A1 and CYP1A2 are well documented. In untreated rats, CYP1A1 protein and mRNA were detected in kidney and lung of female rats but not males (Iba et al. 1998). CYP1A2 was detected in liver of both sexes. In untreated rats, CYP1A1 activity was significantly higher in females than males in liver (1.8×) and kidney (16×) but not in lung (Iba et al. 1998). Pyridine induction increases CYP1A1 mRNA and protein in liver, kidney, and lung in females. Pyridine upregulated CYP1A1 mRNA without a concomitant increase in protein, in liver and lung of male rats. Nicotine-induced CYP1A1 in rat lung tissue, males > females (Iba et al. 1998). The response of CYP1A2 to pyridine was different. Both mRNA and protein increased in liver of female rats, while in males the protein (but not the mRNA) was increased.
Rodents have some sex-related P450s, such as CYP2C11 and 3A2 in male rats and CYP2C12 in females. Schwartz (2003) reported that CYP2C9 and CYP2C19 levels are similar between males and females, but treatment with estradiol and progesterone reduced CYP2C19 activity (Palovaara, Typbring, and Laine 2003). Sexual and developmental differences expression in the CYP3A enzyme family have been demonstrated in rodent (Jan et al. 2006). CYP3A1 is virtually absent in adult male rats but is highly inducible while 3A2 protein is present constitutively. CYP3A9 is a female predominant enzyme while CYP3A18 occurs in males (Mahnke et al. 1997). CYP3A18 and CYP3A23 proteins were present before and after puberty, about 1.2-fold higher in male rats than females. CYP3A9 was detected only in adult rats, about 2× higher in females, while CYP3A2 was detected only in male rats (Mahnke et al. 1997).
Jan et al. (2006) detected CYP3A2, CYP3A18, CYP3A9, and CYP3A1 constitutively in males rats, while females had very low levels of all 4 proteins, although all (particularly CYP3A2) proved inducible by pregnenolone 16α-carbonitrile in both sexes.
Differences in P450 expression or activity can be due to genetics, sex hormones, body weight and fat, or to enzyme inducers in the diet. CYP1A2 is involved in metabolism of polyaromatic hydrocarbons and various amines. It is expressed mainly in the liver with higher activity in males (Beierle, Meibohm, and Derendorf 1999) and has been implicated in the activation of xenobiotics. A wide range of substances can induce CYP1A2, and variation in this enzyme level contributes to variable risk of amine related cancers (Clewell et al. 2002). More than half of drugs studied are metabolized by CYP3A4 (Tanaka 1999), which occurs in the GI tract and liver. In humans, men have somewhat higher CYP1A2 and CYP2E1 while women “appear” to have greater CYP3A activity (Scandlyn, Stuart, and Rosengren 2008). One study showed a 1.4-fold higher level in young women reflecting induction by progesterone. Other studies have found higher CYP3A4 levels in males, which would result in faster metabolism of drugs. CYP2C19 showed higher activity in males in 1 study and females in another (Clewell et al. 2002). Males tend to have higher alcohol hydrogenase activity, while females achieve higher blood alcohol levels for the same intake, again influenced by body composition.
Penaloza et al. (2014) were able to demonstrate that methylation altered production of CYP450 and other proteins were influenced by stress or estradiol and that different gene methylation patterns “partially explain the sex-based differences in expression” (Penaloza et al. 2014, 966).
Cells isolated from male and female mice younger than 10 days, presex hormone production, showed sex differences in enzyme profiles with females having 2 to > 300× higher methylation of X-ist (a gene involved in inactivating 1 X chromosome in females), as well as CYP1A1 and other P450s (Penaloza et al. 2014). The authors concluded that different methylation rates explained some of the sex differences in CYP expression, resulting in different metabolic profiles even at birth.
Enzyme inducibility can differ between males and females. St. John’s wort increased CYP3A4 levels by 50% in 8 men versus 90% in 8 women while CYP1A2 increased 20% in women but not at all in men (Wenk, Todesco, and Krahenbuhl 2004). Pretreatment with rifampin induced CYP3A in the intestine (male > female), with faster oral Cl for the drug midazolam. However, after intravenous midazolam, there was greater CYP3A induction in females (Gorski et al. 2003). Male mice treated with acrylonitrile developed higher blood cyanide levels, attributable to differential action of CYP2E1. Expression of cyp2e1 was higher in male kidney than in female, with no sex difference in the liver (Chanas, Wang, and Ghanayem 2003). Iba et al. (1998) showed that whereas pyridine induction of CYP1A2 was greater in females than males, the reverse was true for induction by beta-naphthoflavone.
An example of a classically direct sex hormone effect on P450 is CYP2J5 in the mouse kidney, which is upregulated by testosterone and downregulated by estrogen (see Table 2).
This is one of the P450s which convert arachidonic acid to epoxyeicosatrienoic acid. Males have higher CYP2J5 protein than females, and castration decreases expression. Dihydrotestosterone (DHT) administered to females or castrated males increased the protein to almost normal male levels (Ma et al. 2004). Treatment of ovariectomized females or castrated males with estradiol reduces CYP2J5. Mice with reduced androgen receptor have lower levels of CYP2J5 and do not respond to DHT. The androgen receptor antagonist, flutamide, likewise lowers CYP2J5 levels (Ma et al. 2004).
CYP1A1 (formerly known as the aryl hydrocarbon hydroxylase) is inducible by a variety of polycyclic aromatic carcinogens that bind to the aromatic hydrocarbon receptor (AhR; Harper et al. 1991). It is involved in metabolic activation of carcinogens in tobacco smoke. Levels of CYP1A1 differ between males and females. Benzo[a]pyrene induced greater CYP1A1 in male rats than in females, while fluroanthene induction did not produce a sex difference (Ramesh et al. 2000). A dose of tetrachlorodibenzodioxin (TCDD) that was lethal to wild-type male mice was not lethal to wild-type females or to CYP1A1 null males (Uno et al. 2004).
Researchers are now examining networks of coexpressed genes, for example, the relationship between CYP3A4, glutathione-s-transferase (GST) genes, and other drug metabolizing enzymes and transporter genes (DMETs). Yang et al. (2012) identified 80 genes (out of 19,541) differentially expressed in male and female liver samples, including 7 genes on the X and 12 on the Y chromosomes. Ten of the DMET genes had more than a 1.5-fold difference including SLC3A1, CYP7A1, ACSL4, CYP3A7, GSTA1, CYP3A4, GSTA2, UGT2B17, SLC13A1, and ADH1A, and they have a wide variety of actions. Huang et al. (2011) characterized many proteins using what they characterize as “Quantitative shot-gun proteomics,” identifying many sex-biased CYP enzymes. CYP2D1 metabolism in females was 70% that of males, corresponding to the amount of protein, rather than a difference in activity.
Phase II—conjugation
Many drugs and their metabolites are not water soluble, and they are eliminated via the bile and feces. Phase II metabolism typically involves conjugation to an organic moiety, which renders the substance water soluble for excretion in the urine. Phase II reactions include glucuronidation, acetylation, methylation, sulfation, or conjugation with glutathione. Clewell et al. (2002, 329) found “no evident differences” between sexes, and some reactions involving acetyltransferase show no sex difference (Schwartz 2003), particularly when corrected for body weight. Phase II is essential for renal Cl of many xenobiotics, and it is generally faster in men (Schwartz 2003). Rats administered acetaminophen excreted it quickly in the urine. The glucuronide conjugate was significantly greater in females, while the sulfate conjugate was higher in males (Raheja, Linscheer, and Cho 1983). In our studies of the white-footed mouse, we found that at all ages up to 48 months, males had about 3× higher phase II metabolizing UDP-glucuronosyltransferase than females (Figure 2; Guo et al. 1993).
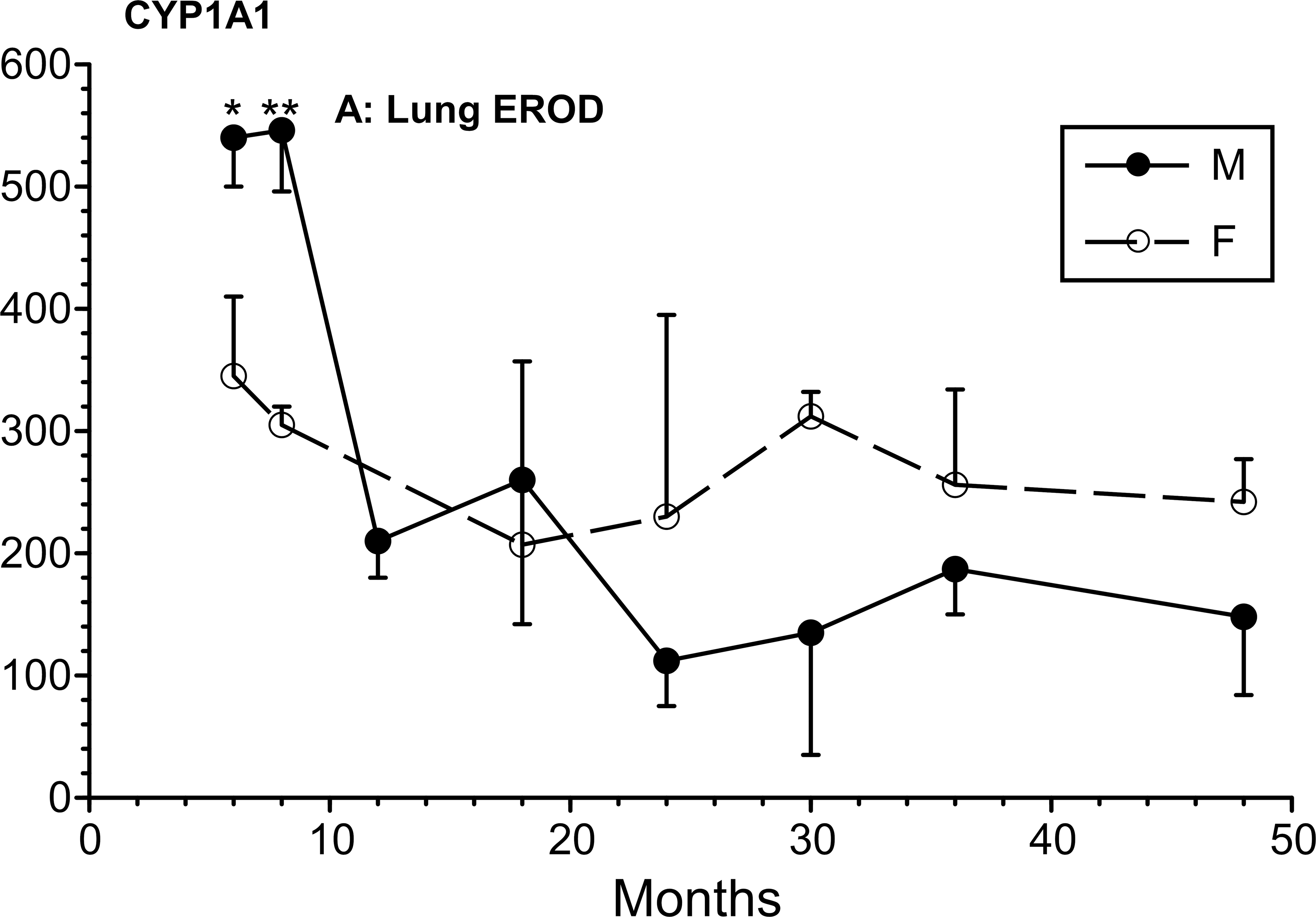
Sex differences in cytochrome P450 1A1 across the life cycle in a laboratory population of the white-footed mouse (Peromyscus leucopus; Guo et al. 1993). Nonoverlapping error bars indicate significant difference (p < .05).
Change during the estrous cycle can be dramatic. Estradiol level affected UDP-glucuronyltransferase and NADPH-cytochrome c reductase (Watanabe et al. 1997). Glucuronidation rate was higher in liver of male rats compared with females, while the reverse was true in kidney. Castration increased urinary excretion of a glucuronide by males almost to the female level, which was suppressed by testosterone treatment. Conversely, glucuronide excretion by females was reduced by ovariectomy or testosterone (Palylyk-Colwell and Jamali 2004). Male rats had lower UDP-glucuronosyltransferase activity than females. Gonadectomy increased activity in males and decreased it in females. Females had higher biliary excretory rates for bilirubin (Muraca, De Groote, and Fevery 1983).
Elimination
Xenobiotics or their metabolites are excreted primarily through the urine and through the bile into feces but also through the lungs, skin, sweat, saliva, and milk. For urinary excretion, the compound must be delivered to the kidney or converted there to a water-soluble form usually by phase II metabolism. Renal excretion can be viewed as 3 phases: glomerular filtration sensitive to blood flow and hydrostatic pressure, tubular reabsorption, and tubular secretion. At the glomerulus, most of the fluid, electrolytes, small molecules, and even small proteins are filtered. Many of these are too precious to waste and must be retrieved quickly from the tubule into the capillaries wrapped around them. Reabsorption removes 90% plus of the water, all of the sugar and amino acids, most of the electrolytes—basically reabsorbing anything the body doesn’t want to waste from the tubular contents. As urine formation continues, tubular secretion eliminates substances that aren’t completely filtered including creatinine and some drugs, as well as H+ and NH4 + to maintain blood pH. Renal Cl, particularly GFR, is a critical variable that is typically higher in men than women (Kadiri and Ajayi 2000), allowing women to retain more contaminant, even after conjugation. Female rats also have lower GFR associated with lower renal blood flow (Cerrutti, Quaglia, and Torres 2001).
Clewell et al. (2002) reported generally higher (but inconsistent) GFR in males and found no information on sex differences in tubular secretion. Tubular secretion typically involves transporters moving substances into the urine, against the reabsorption of water. Kidney transporters of the ABC family (efflux transporters) and of the solute carrier (SLC family of uptake transporters) play a role in drug disposition and elimination. Substantial differences between men and women influence the movement of compounds into and out of renal tubular cells (Yang et al. 2012).
OATs are active in the renal tubule, and their expression is modified in complex ways by sex hormones (Kudo et al. 2002). As an example, PFOA, a ubiquitous environmental contaminant, is persistent in the environment and is not metabolized in animals, but is eliminated mainly in urine. PFOA shows sex differences in renal elimination, related to sex-specific expression of OATs in proximal renal tubule cells, accounting for much higher and faster excretion in female versus male rats (Worley and Fisher 2015). Similar sex difference occurs in Fathead Minnow (Pimephales promelas), and androgen treatment slows the elimination in females, but estrogen did not accelerate elimination by males (Lee and Schultz 2010). Thus, this appears to be a widespread phenomenon but may have different adaptive significance in terrestrial and aquatic organisms.
Joseph et al. (2015) analyzed expression of 30 ABC efflux transporters and solute carrier transporters (SLC) uptake transporters in kidneys of 61 men and 34 women and reported no differences across 24 genes. Theirs is a good example of the misleading use of Bonferroni corrections for multiple comparisons, which is prone to type II errors, especially when there are many independent variables. This led Joseph et al. (2015) to report no significant differences by sex. However, from their data-rich graph, I calculated individual t scores, finding that at least SLC31A1 (p < .001) was significantly lower in females (Figure 3). ATP2B2 and ABC5 appear statistically lower in females (p = .05), while ATP7B is statistically higher in females (p < .02). Overcorrecting obscures differences that deserve investigation. Of the 22 transporters that showed an apparent sex difference, 21 had higher expression in males (binomial test p < .0001). Even if all 8 transporters with no apparent difference were female biased, the male predominance (21 of the 30) would still be significant (binomial test p = .02).
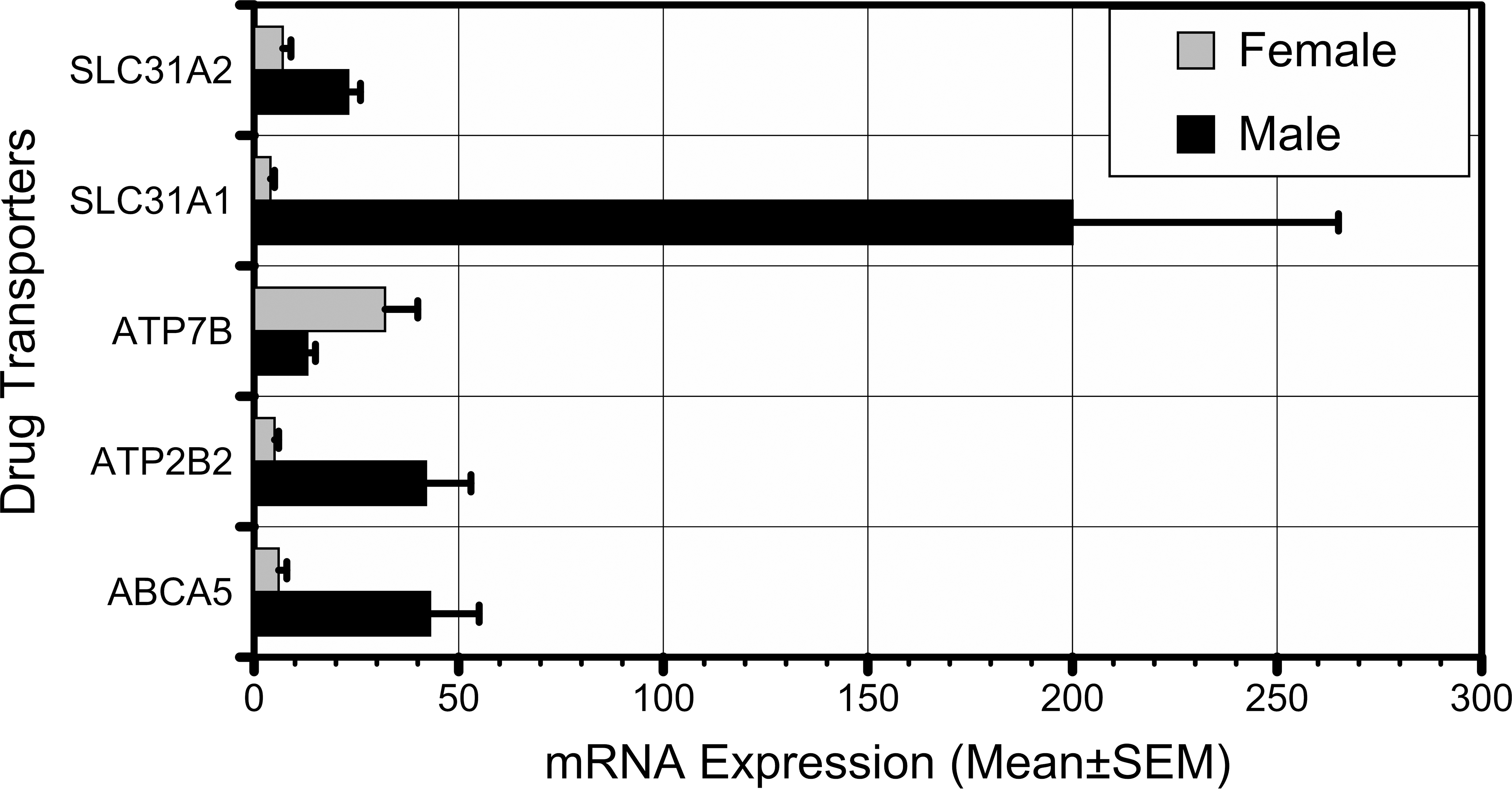
Of the 24 genes examined by Joseph et al. (2015), 5 appear to show significant sex differences. Most of the genes showed higher expression in males.
SLC31A1, a member of the solute carrier family 31, is a high-affinity copper transporter in cell membrane. ATP7B (Wilson disease protein), the significantly female biased transporter, is active in liver and brain, eliminating excess copper into the bile and plasma. ATP2B2 is a calcium ion efflux transporter maintaining intracellular homeostasis. It is not obvious why these primary functions should be sex biased, and it is likely that additional functions will be identified for these transporters. It is also possible that some of these differences will prove unstable if they are replicated or tested in other systems.
The uptake, distribution, and elimination of metals can also vary by sex. A single dose of methylmercury was followed by higher urinary elimination of mercury in males versus females with a concomitant reduction in brain and blood but not kidney mercury concentrations (Hirayama and Yasutake 1986).
Dose to organs
The toxicokinetic processes influence the blood level at any point in time. Absorption increases the blood level, while distribution to a target organ and elimination result in clearing the substance from the blood. At any time point, the blood level determines the amount available for transfer into organs: target organs, storage depots, or elimination.
Liver
Of the studies reviewed for this article, there were differences in gene expression, protein product, and enzyme activity, with varying substrates and varying induction, without producing a clear and consistent pattern across species and studies.
Many of the toxicokinetic differences occur in the liver and have been studied both in vivo and in vitro. The liver is the first pass recipient of nutrients and toxicants directly from the intestine through the portal circulation. The branches of the portal vein and hepatic artery run parallel through the liver to the lobules. As blood moves through liver lobule from the portal vein to the hepatic vein, its contents are subjected to the body’s most active metabolic tissue as well as to a decrease in oxygen tension, as it moves away from proximity to the hepatic artery. Here is a key intersection between TK (delivery) and toxicodynamics (response).
Women are less tolerant to both acute central nervous system (CNS) and hepatotoxic effects of ethanol than males. They experience higher blood alcohol levels for the same intake, and women develop liver damage sooner (Ashley et al. 1977) attributed to TK and toxicodynamics (Ronis et al. 2004). In rats, transporters of the multidrug resistance-associated protein (Mrp2 and Mrp3) were higher in females than males, while members of the OAT family were either equal or higher in males. Androgen treatment increased Mrp3 in females only (Rost et al. 2005).
Brain
Imaging reveals a complex pattern of sexual dimorphism in the adult human brain (Goldstein et al. 2001). This sexual dimorphism in size and organization begins early in life. The X and Y chromosomes have a relatively large number of genes related to brain structure, influenced directly before gonadal hormones are available (Arnold and Burgoyne 2004). In early embryonic life, genes on the Y chromosome begin to exert an effect on brain development. As the embryo develops its own hormonal capability, the sex steroids can modify brain development (Kawata, Yuri, and Morimoto 1994). The hormones may exert their effect at critical periods in development and throughout life (NRC 2005).
The blood–brain barrier (BBB) keeps substances circulating in the blood stream from entering the brain circulation. The barrier is comprised of astrocytes and endothelial cells with tight junctions that allow passage only of small, lipophilic substances. Pakulski, Drobnik, and Millo (2000) made measurements during neurosurgery and reported slightly lower, but not significant albumin permeability in females compared with males. Saija et al. (1990) measured the blood-to-brain transfer in rats of aminoisobutyric acid, finding higher permeability at estrus compared with proestrus, and there was a “marked increase” in permeability after ovariectomy.
After pretreatment with lipopolysaccharide, mice injected with sodium selenite showed greater brain accumulation in females than in males (Minami et al. 2002). Conversely, dietary selenite protected the BBB, resulting in lower permeability during chemically induced convulsions in female rats, while male rats experienced higher permeability related to convulsions (Seker, Akgul, and Oztas 2008). However, the combination of selenium and vitamin E reduced permeability during hyperthermic convulsions in both sexes (Oztas, Akgul, and Seker 2007).
Carcinogens and cancer
Apart from cancers of the respective male and female sex organs, there are sex differences in cancer risks and rates that involve both TK and toxicodynamics (Crump, Krewski, and Van Landingham 1999). Cancer depends in part on how efficiently a xenobiotic is metabolized and whether the metabolite is itself active (Zang and Wynder 1996). For the same lifetime smoking, women have up to a 70% higher lung cancer risk than men (Zang and Wynder 1996). Observational studies of smoking behavior indicate that women have higher sidestream smoke than men (Burger and Gochfeld 1990), but it may also reflect respiratory physiology, metabolism, or other susceptibility factors.
It is perplexing when a particular cancer is increased in one sex and not the other, given similar or even controlled “identical” exposures. The dioxin release in Seveso, Italy, in 1976, was followed by a 5× increase in lymphoreticulosarcoma in men, and a similar increase in myeloid leukemia and multiple myeloma in women (Bertazzi et al. 1993). Gallo et al. (1986) had identified TCDD binding to the Ah receptor downregulating the estrogen receptor and had predicted a possible protective effect against breast and endometrial cancer, which was borne out by the Bertazzi et al. (1993) cancer data on the dioxin-exposed population around Seveso.
Chemicals such as TCE and perchlorethylene (PERC) increase kidney tumor rates in male rats but not in female rats or male or female mice. Green, Odum, and Nash (1990) suggested that this related to a unique alpha-2 globulin present in the male rat kidney tubule where it undergoes hydrolysis, which contributes to cell necrosis, proliferation, and malignancy (Bruckner, Anand, and Warren 2013). Thus, the cancer in male rats is often considered inapplicable to human risk assessment. However, reports suggest that both TCE and PERC have also been implicated in increased rates of kidney cancer in humans, leading to a National Academy of Science (NAS; 2009, 9) conclusion of “limited/suggestive evidence of an association” for PERC as a human renal carcinogen.
The National Toxicology Program’s (NTP) cancer bioassays are a rich resource for comparing cancer incidence rates among male and female control rats and mice. Moore et al. (2013) reviewed 180 studies of B6C3F1 with both sexes, for the incidence of primary pulmonary neoplasms. The median incidence for alveolar bronchiolar adenomas and carcinomas was 16% and 8% in males compared with 5% and 2% in females.
This article has identified examples of differences in TK, some at the gene expression or transporter level. If metabolism or elimination is slowed, prolonged exposure may occur. For drugs with narrow therapeutic windows, even modest differences may result in ADRs based on toxicity or on therapeutic failure. The arylamine N-acetyl transferase gene has common single nucleotide polymorphisms that determine slow, intermediate, or rapid acetylation in phase II metabolism. These differences have been implicated as a cancer risk, although a recent meta-analysis did not find breast cancer differences related to this common polymorphism (Wang and Marei 2016). Modest differences in DMET expression, for example, in CYP3A4 and or GSTA1 might increase cancer risk, without causing any clinically apparent “disease” (Yang et al. 2012).
Of the 278 carcinogens reviewed, 201 (72%) had significant sex differences (p ≤ .05) in at least 1 nonreproductive organ; 130 showed male bias and 59 female bias (Kadekar et al. 2012). Using only substances with strong evidence in the NTP bioassay database, 68 carcinogens increased cancer in males versus only 19 in females (Kadekar et al. 2012). Of these 201 chemicals, 130 induced gender-specific tumors in male rats and 59 in female rats. Male-specific tumors included pancreatic and skin tumors, and female-specific tumors included lung tumors. For some tumor sites, these differences in gender susceptibility can be associated with literature data on sex hormone receptor expression. In conclusion, gender-specific tumors were common. The male dominance is in line with recent human data, and the male susceptibility to carcinogens should be further studied.
Microbiome
Animals and humans have microbiome ecosystems on skin, in axillae, inguinal region, in the respiratory tract, and at various points in the GI tract. These organisms and their interactions play active roles in metabolism, influencing the metabolites produced and their bioaccessibility. Recently, the microbiome has been recognized for its important role in TK (metabolism) and as a target “organ” as well (Dietert and Silbergeld 2015). The microbiome is examined in detail by Silbergeld in this issue.
Discussion
The measurable concentration of any agent in the blood at any time is a dynamic result of the four toxicokinetic processes: absorption, distribution (including Cl), metabolism, and elimination.
This review has provided examples of many areas where sex differences exist, without accounting for the areas where they don’t exist. There are two caveats before proceeding with discussion: (1) many studies have been one of a kind and have not been replicated, and (2) there is no consistent criterion for how much of a fold difference is “important” either clinically or evolutionarily. What fold difference in what enzyme system would encourage or require the Environmental Protection Agency to take action on an environmental contaminant, FDA to take action on a drug, or a clinician or patient to adjust a dose.
Clinical evidence is mostly phenomenologic and not linked with toxicokinetic estimates. Meibohm, Beierle, and Derendorf (2002, 529) concluded that sex differences in drug responses, including the roles of physiology and metabolism, were “generally only subtle”, but they singled out drugs effecting the QT interval and some CNS responses. Women were more responsive than men to opioids (Craft 2003), while the converse is true in studies of female rodents, and Craft (2003) was cautious about attributing differences to TK or toxicodynamics. Many of the reported sex differences in response to drugs are probably primarily toxicokinetic influencing the C max and AUC. For example, women had a 20% to 30% greater response to muscle relaxants, while males were up to 40% more responsive to the sedative effects of propofol (Pleym et al. 2003).
Data Limitations
This article has focused on studies that report some differences between males and females. Many of the reports are one of a kind and may not be replicated, so it becomes important to search for patterns that explain the observations. Small fold differences may be due to error and should not be overinterpreted. For a comprehensive picture, however, the reported sex difference need to be juxtaposed to studies or phenomena that looked for sex differences with adequate power and found them absent. These may be buried among studies that didn’t even look for sex differences and studies that lacked power. Unfortunately, it is more difficult to search for “non-sex difference” than for sex difference.
Although granting agencies usually require power calculations, the majority of papers reviewed make no mention of their power. Moreover, there is always a suspicion that studies that are “negative” because of lack of power never get published (“negative publication bias”). Epidemiology research is intrinsically conservative, biased toward avoiding type I errors, even at the risk of type II errors (Gochfeld 2003). Many human studies of TK have fewer than 10 males and 10 females, and many animal studies include 6 or fewer animals in each dosage group. Such small samples compromise the ability to detect and publish small differences, and conversely, when differences are detected, one wonders how much credence to place in the result.
A reasonable guidance is to scrutinize positive reports of sex difference to rule out possible confounders such as a difference in age, while negative reports of no sex difference should be examined to ascertain that there was adequate power to detect a difference, let’s say a 1.5-fold or 50% difference (Gochfeld 2007). In this review, my access to literature benefited from the essentially free access accorded by the Rutgers University library system. Although my primary references were through PUBMED, I encountered many citations to new, online open access journals that are not themselves indexed on PUBMED. Whereas I previously cautioned against “Abstract based science” (Gochfeld 2007), I now worry about the proliferation of hundreds of for-profit journals offering rapid online publication, with claimed but unproven peer review practices. Caveat emptor.
Does Sex Matter?
Our attention to sex differences was focused by the IOM’s conclusion (Wizemann and Pardue 2001) that sex matters. The current review as well as the previous review (Gochfeld 2007) estimated that many toxicokinetic differences are on the order of about 1.2-fold (20%) uncorrect for body size, although some enzyme expression ratios are many fold, resulting in higher susceptibility of females to some xenobiotics and a higher risk of ADR. There is generally little quantification of the impact of such differences, and although drug development studies now include females, it is not apparent that differences discovered can or should influence prescribing practices (Schwartz 2003). Numeracy, the ability to interpret numbers such as percentages, is a challenge for both patients (Schapira et al. 2008) and clinicians (Taylor and Byrne-Davis 2016) and are context dependent. A 20% increase in cancer risk might influence behavior. How can a patient or physician interpret or respond to a 20% increase in the C max of a drug or its duration of effect?
Managing prescriptions in an era of polypharmacy is challenging enough, particularly if patients are exhorted to “ask your doctor” or “be sure to tell your doctor.” Doctors can’t always welcome and process such information in a brief clinical encounter. Using sex difference information in TK to fine-tune doses should, in principle, reduce the number of ADRs. In the foreseeable future, however, patients are likely to bear the burden of recognizing when a side effect becomes enough of an ADR to warrant discontinuance and reporting. It is quite clear that sex matters both with regard to differential responses to xenobiotics and willingness to report. It is not clear whether the medical profession and society are prepared to make use of the information.
Conclusion
Between exposure and toxicodynamics, TK determines how much of a pharmacologic or toxicologic dose reaches target organs. Studies of sex differences in ADME can identify magnitudes of difference (fold differences), for those substances being measured. What fold difference corresponds to increase susceptibility or risk, varies greatly and risk itself, whether environmental cancer or ADR, is continuous rather than categorical.
The academic’s mantra that “more research is needed” remains true. Descriptions of sex differences and the mechanisms underlying or modifying them apply broadly to environmental chemicals and pharmaceuticals. Extrapolating from inbred rodents to outbred humans has always been challenging.
But there is a final consideration. No human studies select participants at random from the demographic they are hopefully representing. It is understood that any metric will show variability, a composite of individual variation, analytic variation, and what statisticians call “error.” Statisticians accommodate this variation with a standard deviation or confidence limits, without having to acknowledge that the sample actually comprises heterogeneous individuals some of which, particularly the outliers, may not be at all representative, with regard to some toxicokinetic process, for example, proximal tubular reabsorption or renin secretion (Schnermann 2015). Toxicology has the luxury of replicates, seldom available in human studies, but it is sobering that even inbred mice may manifest consistent interindividual variability, for example, in arterial blood pressure (Schnermann 2015), variability that we pay good money to erase when we buy inbred strains.
Postscript
I came away from this review with innumerable questions about whether particular findings were species-specific, substrate-specific, and generalizable versus idiosyncratic. I wonder “why” such differences exist, what adaptive value they may have for different sexes. How many differences are artifacts of particular methodologies, or of inbred laboratory animals, and why some differences seem tightly controlled and others not. I think that any generalizations about toxicokinetic differences must be viewed through an evolutionary framework which interprets the sex differences as adaptations to the somewhat different lives experienced by males and females (Hrdy 1981).
Footnotes
Acknowledgments
I would like to thank Justin Vidal and Dinesh Stanislaus for the invitation to participate in the symposium on the Influence of Age, Hormones, and the Microbiome on Variation in Toxicologic Responses at the 35th annual meeting of the Society of Toxicologic Pathology (San Diego, June 2016). I would also like to thank all of my coparticipants in the 2003 SGOMSEC workshop on gender, particularly our host Erminio Marafante, as well as Werner Klein, Bernard Goldstein, Deborah Cory-Slechta, and cochairs Joanna Burger and Marie Vahter. Thirty years of interactions with colleagues at the Environmental and Occupational Health Sciences Institute and Rutgers University, particularly Joanns Burger, Michael Gallo, Howard Kipen, Jeffrey Laskin, Robert Laumbach, Michael Pratt, Ken Reuhl, and Iris Udasin, have been particularly valuable. My research in environmental toxicology has been supported by many agencies including the National Institute for Environmental Health Sciences (ESO 5022) and the Department of Energy through the Consortium for Risk Evaluation with Stakeholder Participation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.