
Abstract
Long-acting injectable (LAI) drug suspensions consist of drug nano-/microcrystals suspended in an aqueous vehicle and enable prolonged therapeutic drug exposure up to several months. The examination of injection site reactions (ISRs) to the intramuscular (IM) injection of LAI suspensions is relevant not only from a safety perspective but also for the understanding of the pharmacokinetics. The aim of this study was to perform a multilevel temporal characterization of the local and lymphatic histopathological/immunological alterations triggered by the IM injection of an LAI paliperidone palmitate suspension and an analog polystyrene suspension in rats and identify critical time points and parameters with regard to the host response. The ISRs showed a moderate to marked chronic granulomatous inflammation, which was mediated by multiple cyto-/chemokines, including interleukin-1β, monocyte Chemoattractant Protein-1, and vascular endothelial growth factor. Lymphatic uptake and lymph node retention of nano-/microparticles were observed, but the contribution to the drug absorption was negligible. A simple image analysis procedure and empirical model were proposed for the accurate evaluation of the depot geometry, cell infiltration, and vascularization. This study was designed as a reference for the evaluation and comparison of future LAIs and to support the mechanistic modeling of the formulation–physiology interplay regulating the drug absorption from LAIs.
Keywords
Introduction
Long-acting intramuscular (IM) or subcutaneous (SC) injectable (LAI) drug nano-/microsuspensions constitute a relatively new class of formulations that enable prolonged and stable therapeutic drug exposure from 2 weeks to several months (Remenar 2014). They consist of pure drug nanocrystals and/or microcrystals (i.e., size range typically 100 nm–10 µm), which are dispersed in a buffered aqueous vehicle containing small amounts of stabilizing excipients (e.g., hydrophilic polymers and/or surfactants) to avoid particle agglomeration (Rabinow 2004). Since these formulations do not rely on the use of a drug carrier, very high drug loads (≥30% w/v) can be achieved. This facilitates the administration of large doses required for a monthly dosing scheme via a single injection of relatively small volumes. LAI suspensions are free of organic solvent, sterile, and adhere to strict limits for endotoxin levels. The principles dictating the nano-/microsuspension formulation development and determining the drug dissolution rate have been extensively reviewed elsewhere (Shegokar and Müller 2010; Möschwitzer 2013). This attractive formulation strategy has so far resulted in the successful marketing of 3 once-monthly IM injectable nano-/microsuspensions, and several promising candidates are currently being tested in clinical trials (Samtani, Vermeulen, and Stuyckens 2009; Lindenmayer 2010; Gopalakrishna, Aggarwal, and Lauriello 2013; Spreen, Margolis, and Pottage 2013; Remenar 2014).
The drug absorption from LAI suspensions of practically water-insoluble drugs is generally considered to be dissolution rate limited and, therefore, driven by the physical properties of the nano-/microparticles and the depot being formed upon IM or SC injection (Zuidema et al. 1994; Samtani, Vermeulen, and Stuyckens 2009). Nevertheless, the drug release and absorption might be influenced by several other factors such as the agglomeration or the local spreading of the drug particulates, the particle size, and surface properties (e.g., the host protein adsorption) that dictate the phagocytosis efficiency, the susceptibility to the local enzymatic (pro)drug degradation, and lymphatic uptake, all of which can be modulated by the local inflammatory response (Zuidema et al. 1994; Medlicott, Waldron, and Foster 2004; McLennan, Porter, and Charman 2005). Hence, some challenges associated with the parenteral administration of LAIs, especially related to the complex in vivo disposition and pharmacokinetics, remain to be elucidated and are currently the subject of investigations (Darville et al. 2014).
Although all LAI nano-/microsuspension constituents are generally well tolerated and biodegradable, the particles are recognized as nonself, leading to local inflammatory reactions (J. M. Anderson, Rodriguez, and Chang 2008). Hence, it is imperative to carefully assess their local tolerability and disposition. Time-dependent macroscopic observation and histopathological evaluation of the administration/implantation sites are an integral part of the preclinical assessment for the evaluation of the biocompatibility of materials (U.S. Pharmacopeia 2000; International Organization for Standardization 2007). However, there are no specific sampling time points recommended for the implantation sites, since this is highly depending on the intended implantation duration. Evaluation of implantation sites is most commonly performed at the so-called steady state (i.e., late phase tissue response). To assess the IM toxicity of new drugs, several criteria, including the histopathological evaluation of administration sites at 3, 7, and 21 days after injection, were recommended (Grim, Rerábková, and Carlson 1988). More recently, Thuilliez and coworkers evaluated the IM injection sites of control rats in 7 studies and reported lesions secondary to the administration procedure of saline (damage by the needle and volume). The data were used to generate standardized terminology for IM injection sites (Thuilliez et al. 2009).
Most literature on biocompatibility assessment relates to solid implantable biomaterials or polymeric materials, rather than aqueous suspensions of pure drugs. For example, the biocompatibility of SC naltrexone sustained-release polymeric microspheres in rats and rabbits has been investigated after 3, 7, 14, 21, and 28 days using standard histopathological procedures (Yamaguchi and Anderson 1992). However, such studies most often focus on the subacute or long-term tolerability and the reversibility of the lesions but omit the acute phase reaction (Turner, Lawrence, and Autian 1973; Grim, Rerábková, and Carlson 1988). Also, the findings of SC implant studies cannot be readily extrapolated to IM LAIs, as the host reaction is determined not only by the administration route but also by the size, shape, and chemistry of the material as well as the animal species (Yamaguchi and Anderson 1993; Brodbeck et al. 2003; Engelhardt 2008).
The paucity of literature on the nature and dynamics of the tissue response to IM/SC LAI nano-/microsuspensions can be attributed to the relatively recent introduction of this formulation approach but also to the proprietary nature of the formulations currently in development. Only a few relevant publications are available to date. A preclinical pharmacokinetic and tolerability study following a single SC or IM injection of a 200 nm LAI nanosuspension of the anti-HIV drug rilpivirine in rats and dogs has demonstrated that the LAI was well tolerated but generated a transient local injection site reaction (ISR) that possibly led to the formation of secondary formulation depots in draining lymph nodes (van’t Klooster et al. 2010). However, no histopathological data were disclosed.
Paquette and coworkers evaluated the host reaction to SC injected LAI suspensions of the antipsychotics aripiprazole monohydrate (DV ,50 = 5 µm) and olanzapine pamoate monohydrate (DV ,50 = 7.4 µm) in support of clinical studies (Paquette et al. 2014). The cellular dynamics of the tissue response were evaluated by means of histopathology of the IM injection sites in monkeys 30 and 50 days after injection as well as by a time-course assessment of the SC injection site histology and cytokine concentrations (in injection site fluid) on day 1, 3, 7, 10, 14, and 21 in rats. Localized and drug-dependent reactions were accompanied by increased levels of proinflammatory cytokines that mediated an acute inflammatory reaction with subsequent giant cell-free chronic inflammation. In spite of the value of the pioneering work, the discrepancy in administration route and absence of (semi-)quantitative histological data made an accurate evaluation of the regulation and progression of the ISR difficult.
Finally, our group recently illustrated by means of a pharmacokinetic study in the rat, supported by qualitative histopathology, that the local tissue response resulting from the IM administration of a commercially available paliperidone palmitate (PP) LAI is modulating the prodrug (PP) dissolution and subsequent drug (paliperidone [PAL]) systemic absorption (Darville et al. 2014). Both the cell infiltration and the neovascularization of the formulation depot have been identified as potential rate-limiting processes for the drug absorption. The meticulous examination of the LAI injection sites is therefore relevant not only from a safety perspective but also for the mechanistic understanding of the drug release mechanisms.
In this study we continued our previous research on the IM PP-LAI nano-/microsuspension disposition by looking at the local host response from a histopathological perspective, rather than focusing on the pharmacokinetics (Darville et al. 2014). The aim was to perform a temporally resolved, multilevel characterization of the local histopathological and immunological alterations triggered by the IM injection of PP-LAI and polystyrene (PS) nano-/microsuspensions in the rat in order to (1) elucidate the nature and dynamics of the ISR, (2) identify the critical time points and parameters of interest with regard to the host response, hence, supporting recommendations for future study designs, (3) quantitatively evaluate the predictive value of inert spherical PS microspheres as model particles, (4) evaluate the contribution of lymphatic drug absorption and PP-LAI retention, and (5) investigate the formulation depot geometries as well as the rate and extent of the local inflammatory cell infiltration by quantitative image analysis and modeling. The obtained results provide a sound basis of comparison for the tolerability study of new LAI nano-/microsuspensions. Additionally, the data might support future mechanistic modeling of the interplay between formulation characteristics and physiological processes, and the effects on drug release and absorption.
Materials and Methods
Model Nano-/Microsuspensions
The Xeplion® IM LAI PP nano-/microsuspension (PP-LAI) was provided by Janssen Pharmaceutica NV (Beerse, Belgium). It consisted of pure PP nano-/microcrystals suspended at 156 mg/ml in an aqueous buffer solution (pH 7.1) containing 12 mg/ml polysorbate 20 and 30 mg/ml polyethylene glycol 4000. The volume-weighted median equivalent sphere diameter (DV ,50) of the PP-LAI nano-/microcrystals, as previously determined by laser diffractometry, was 1.08 ± 0.03 µm (Darville et al. 2014). The formulation was sterile and contained no more than 2.33 I.U./mg endotoxin (i.e., human endotoxin limit calculated as described in the European Pharmacopoeia, §2.6.14. Bacterial Endotoxins). Fluorescent nonfunctionalized PS microspheres (Fluoresbrite® 1 µm; Polysciences Europe GmbH, Eppelheim, Germany) were used to evaluate whether such particles could function as model formulation for LAIs and to facilitate the tracking of the particles following administration. The monodisperse spherical PS particles had average dimensions of 1.06 ± 0.03 µm and were suspended at 156 mg/ml in quantitatively identical sterile vehicle.
IM Administration in the Rat
All animal experiments were approved by the KU Leuven Institutional Ethical Committee for Animal Experimentation and were conducted according to European Commission directive 2010/63/EU. The rodents were housed with environmental enrichment and a 12-h light/dark cycle at 20°C to 22°C. Free access to rodent food and water was given at all times and the animals were allowed to acclimatize for 1 week before assignment to a study group.
Male Wistar rats, aged 8 to 9 weeks and weighing 350 ± 30 g, received a single IM bolus injection of 200 µl/kg body weight of either PP-LAI or PS in the left hind leg (musculus biceps femoris) after skin disinfection. Sterile, particle-free vehicle was injected in the contralateral hind limb. Naive animals were additionally included for histology and received IM injections of equal volumes of sterile phosphate-buffered saline pH 7.4. Needles of 27 G were used to reduce needle track trauma. An overview of the study design, including the number of rats per allocation, the dosing conditions, and the sampling time points, is presented in Table 1.
Overview of the Study Arms, Dosing Schemes, and Sampling Intervals.
Note: CYTOK = quantification of cytokines in injection site exudate; HISTO = qualitative and quantitative histopathology of the IM injection sites and the ipsilateral iliac and popliteal lymph nodes; IM = intramuscular; LN = ipsilateral iliac and popliteal lymph node bioanalysis for the quantification of paliperidone palmitate (PP) and paliperidone concentrations; NA = not applicable; PP-LAI = PP long-acting injectable; PBS = phosphate-buffered saline.
aPP-LAI of 200 µl per kilogram body weight corresponds to 20 mg of PAL equivalent per kilogram body weight.
bInsufficient injection site exudate volume for cytokine quantification.
Tissue Sampling
The animals were sacrificed by exsanguination under isoflurane/oxygen anesthesia prior to gross examination. For histopathology (n = 3 per time point and per test article), the IM administration sites as well as the ipsilateral (cf. IM injection site) medial iliac lymph node (ILN) and regional popliteal lymph node (PLN) were collected and fixed in 10% v/v neutral-buffered formalin. For the PP and PAL concentration determination in the primary draining lymph nodes of rats, the ipsilateral ILN and PLN were isolated and the surrounding adipose tissue was carefully removed as much as possible. The lymph nodes were weighed and stored at −20°C prior to bioanalysis. For the cytokine concentration determination, the PP-LAI IM administration sites containing the remaining formulation depot were isolated from the hind leg and any excess muscle and adipose tissue was trimmed off. The administration site was chopped using a straight blade on an RNase-decontaminated cutting surface before being transferred into a filtration–centrifugation tube (Corning Costar® Spin-X®, 0.22 µm cellulose acetate membrane filter; Corning Life Sciences, Tewksbury, MA). Samples were kept on melting ice and protected from light until filtration–centrifugation at 16,000 × g for 20 min at 4°C. A second identical filtration–centrifugation cycle was performed after redispersion of the sample to maximize fluid yield. The undiluted injection site fluid filtrates (ISFs) were stored at −80°C until cytokine analysis. Analog samples of hind leg skeletal muscle from naive animals were collected and processed in a similar way.
Cytokine Analysis
The cytokine concentrations (n = 6–8 per time point) were measured in ISFs using a custom magnetic bead–based multiplex rat cytokine immunoassay for the following targets: tumor necrosis factor (TNF)-α, interferon (IFN)-γ, interleukin (IL)-1α, IL-1β, IL-2, IL-6, IL-12p70, regulated on activation and normal T cell expressed and secreted protein (RANTES), monocyte chemoattractant protein (MCP)-1, macrophage inflammatory protein (MIP)-2, MIP-3α and the vascular endothelial growth factor (VEGF; Bio-Plex Pro® Rat Cytokine Assay; Bio-Rad Laboratories Inc., Hercules, CA). The ISF samples were thawed at room temperature and diluted 3-fold in the kit’s sample diluent prior to analysis. The assay was further performed in accordance with the manufacturer’s assay protocol using a MAGPIX® instrument (Luminex Corporation, Austin, TX). The raw data were processed with the Bio-Plex Manager v6.1 (Bio-Rad Laboratories Inc.) software and Excel® 2010 (Microsoft Corporation, Redmond, WN). For each of the cytokines, the lowest acceptable standard concentration (i.e., coefficient of variation [CV] % ≤ 25% and mean accuracy within 70–130% of nominal value) was used as the lower limit of quantification (LLOQ).
Quantification of PP and PAL in Draining Lymph Nodes
The frozen lymph nodes (n = 6–9 per time point) were thawed at ambient temperature prior to homogenization and quantification of PP and PAL in the supernatant by means of qualified reverse-phase high-performance liquid chromatography methods with tandem mass spectrometric detection. The chromatographic and mass spectrometric conditions for the quantification of PAL and its internal standard JNJ-17340362 were identical to those reported previously (Darville et al. 2014). Those for the quantification of PP and its internal standard JNJ-3905343 are provided in Supplemental Material. Calibration curves for PP and PAL were obtained by least squares linear regression of the log-transformed peak area ratios of PP: JNJ-3905343 and PAL: JNJ-17340362, respectively, against the log-transformed PP or PAL standard concentrations. The LLOQ (signal: noise ratio ≥5 with %CV ≤20% and mean accuracy within 80–120% of nominal value) for PP and PAL were 4.00 and 5.00 ng/g lymph node, respectively.
Histotechnology and Immunohistochemistry
The IM administration sites were defined as the residual formulation (i.e., PP-LAI or PS) depots, including the surrounding (peri-)muscular tissue. Sagittal cross sections of the excised and formalin-fixed administration sites and lymph nodes were sampled for routine paraffin embedding, staining with H&E and mounting on standard glass slides. Serial sections were stained immunohistochemically for the detection of CD3-∊, CD31, CD68, CD79b, and CD163 markers, using an avidin–biotin–peroxidase complex method with biotinylated secondary antibodies and 3,3′-diaminobenzidine as chromogenic substrate, according to established protocols (Darville et al. 2014). Additionally, frozen sections of adjacent slices of selected administration sites and lymph nodes were prepared for polarized light microscopy and stained with 0.3% w/v oil red O (ORO) in 60% v/v 2-propanol and Gill’s hematoxylin followed by aqueous mounting.
Qualitative and Semiquantitative Histopathology
Following histoprocessing, the administration sites and lymph nodes were subjected to qualitative and semiquantitative bright field microscopic histopathological evaluation. The formulation depots were classified into three categories based on their location: truly IM depots, partial IM depots (i.e., formulation present between muscle fibers (endomysium), and in loose interstitium (peri- or epimysium)) and interfascial depots (i.e., exclusively present in larger peri- or epimysial interstitium). The histological evaluation of the IM injection sites included the type and extent of the local tissue response, the amount of edema, the cellularity of the formulation depots with regard to granulocytes, macrophages, multinucleated giant cells (MNGC), T lymphocytes and B lymphocytes, the size of the phagocytic macrophages, skeletal muscle de-/regeneration and necrosis, the angiogenesis within the depots, as well as the formation of granulation tissue and encapsulation. These parameters were semiquantitatively evaluated by scoring from 0 to 5 (0 = none, 1 = minimal, 2 = slight, 3 = moderate, 4 = marked, and 5 = severe). The parameters of interest, together with the applied definitions and some explanatory comments are listed in Table S1 (Supplemental Material). All samples were evaluated by two scientists (N. D. and M. v. H. [board-certified veterinary pathologist]). The results are presented as mean scores ± SD (n = 3 per group and per time point).
Quantitative Evaluation of the Depot Geometry and Cellularization
All available H&E-stained (n = 3 for all time points, except for PS 168 hr where n = 2) and adjacent CD31 immunohistochemical sections were digitalized at 20× magnification using a NanoZoomer 2.0-HT digital slide scanner (Hamamatsu Photonics K.K., Hamamatsu City, Shizuoka Pref., Japan) to enable the quantification of the cellular infiltration into the depots as well as the extent of the angiogenesis, respectively. The following image analysis procedures were manually applied to each micrograph separately using ImageJ v1.47 (National Institutes of Health, Bethesda, MD, http://imagej.nih.gov/ij/).
The H&E micrographs (red-green-blue [RGB] images) were loaded in ImageJ and the scale was calibrated, allowing metric dimensions to be obtained. The contour of the PP-LAI or PS depots were accurately defined using the polygonal selection tool and the total absolute depot cross-sectional area (Sdepot ) was measured (Figure 1A). The circularity (C) of the polygonal selection was measured as an indication of the depot geometry (cf. Supplemental Material).
Schematic representation of the quantitative image analysis of intramuscular (IM) administration site micrographs for the determination of depot geometry descriptors and the measurement of (fractional) cross-sectional areas and derived depot volumes that are infiltrated by cells. (A) Representative H&E-stained cross section of an administration site 72 hr after IM PS administration in the rat. The uninfiltrated formulation depot is indicated with (*); the portion of the depot infiltrated by inflammatory cells is indicated with an arrow. The black contour line is manually defined and accurately delineates the depot, allowing the measurement of the absolute total cross-sectional depot area. (B) Color, brightness, and/or contrast thresholding is applied on the selection to quantitatively determine the fraction and absolute cross-sectional area of the depot that has been infiltrated (red). (C) The cross-sectional depot contour is fitted with an ellipse having an identical area, orientation, and centroid as the selection to provide geometry descriptors for statistical analysis and calculations of equivalent volumes. a is half of the major axis and b is half of the minor axis. (D) Three-dimensional representation of the average (n = 3) equivalent total depot volume (dark) and residual, uninfiltrated depot volume (light) assuming symmetry along the major axis of the best fit ellipse (i.e., prolate spheroid). Scale bars represent 1 mm.
The absolute area infiltrated by cells (Sinfiltr. ) was obtained through color, brightness, and/or contrast thresholding (Figure 1B). The residual, un-infiltrated cross-sectional area of the depot (Sresid. ) was subsequently calculated by subtraction. Sresid. was additionally determined through the inverse process of thresholding, that is, as an individual measurement of the area clear of cellular infiltration, as a way to validate the thresholding procedure. Sdepot recovery values of 100.0% ± 5% were deemed acceptable.
The region of interest representing the depot was fitted with an ellipse possessing an identical area (Sdepot ), orientation, and centroid as the original polygonal selection and characterized by the dimensions of the major axis (A = 2a) and minor axis (B = 2b; Figure 1C). Assuming that the major axis of the best fit ellipse is also the symmetry axis of the 3-dimensional volume that would represent the entirety of the depot (Figure 1D), the volume of the corresponding solid of revolution along the major axis (i.e., the total absolute depot volume, Vdepot ) could be calculated with the formula for a prolate spheroid volume (cf. Supplemental Material). Similarly, the residual, un-infiltrated volume of the depot (Vresid. ) was calculated from the measured, absolute Sresid . The volume of the depot infiltrated by cells (Vinfiltr. ) is then equal to the volume of the shell between the two prolates (Figure 1D) and was calculated as the difference between Vdepot and Vresid .
Volumetric fractions infiltrated by cells (FV,infiltr. ) were directly calculated from the fraction of the area that had been infiltrated (FS,infiltr. ; i.e., the ratio of Sinfiltr. over Sdepot ; equation 1).

The step-by-step derivation of the above equation is provided in Supplemental Material. All measurements and derived calculations were normalized for an average body weight of 0.350 kg and are reported as mean values ± SD (n =3).
Modeling the Depot Infiltration
The dynamic courses of cellular infiltration within the depots were parameterized to compare the rate and extent of the host response to the PP-LAI and PS formulations and obtain representative, usable parameters for future modeling efforts. The cumulative 3-parameter Weibull distribution function (equation 2) was fitted to the data by means of nonlinear regression using GraphPad Prism® v5.00 (GraphPad Software Inc., La Jolla, CA; Costa and Sousa Lobo 2001). F represents the cumulative fraction of the depot that has been infiltrated by cells (FSA,infiltr. or FV,infiltr. ) and is expressed as percentage. T 0 is the location parameter and represents the lag time, in hours, preceding the initiation of the infiltration, β (≥0) is the dimensionless shape factor, and α (>0) is the scale factor expressed in days. The time (T), expressed in days, is the independent variable. A maximum attainable infiltration of 100% was assumed.

The goodness of fit was reported through the coefficient of determination (R 2). All model parameters, primary and secondary, are reported as best fit mean values ± SE with 95% confidence intervals.
Statistical Analysis
The lymph node weights at the different time points were compared by one-way ANOVA with Tukey’s multiple comparison test. The 2-tailed unpaired Student’s t-test was used for the comparison of the geometry descriptors as well as the singular primary and secondary nonlinear regression parameters for the PP-LAI and PS groups. The overall nonlinear regression fits, independent of the specific model parameters, were compared using the F-test. The robust regression and outlier removal (ROUT) method (Q = 1%) was applied during nonlinear regression to identify and exclude possible outliers. The suitability of the best fit curve to describe the data was verified using the replicates’ lack-of-fit test and the normality of the data point scatter around the best fit curve was evaluated with the D’Agostino-Pearson test. All statistical analyses were performed using Prism® v5.00. Statistical significance was considered for p values less than .05.
Results
Temporal Evolution of the Local Inflammatory Response
The temporal sequence of the main histopathological events after IM administration of PP-LAI or PS in the rat is qualitatively described in the following sections. Larger analog overview images to those presented in the H&E insets in the figures below are available elsewhere (Darville et al. 2014). No relevant qualitative differences between the local tissue response to PP-LAI and PS were observed unless stated otherwise. Severity adjectives are used in accordance with the semiquantitative grading system previously defined.
Acute inflammatory response (4, 8, and 24 hr)
The IM injection of PP-LAI or PS resulted in the local injury of the host tissues and triggered a mild to moderate acute inflammatory response with edema (Figure 2A–B). Slight to moderate hemorrhages caused by the needle tract trauma were occasionally observed. Minimal to moderate muscle fiber degeneration, evidenced by the loss of fiber striation and the occurrence of vacuolated, and sometimes fragmented, myofibers were seen surrounding the formulations (Figure 3A and Supplementary Figure S3a). The extent of the muscle damage appeared to be slightly higher when formulation depots were located in the endomysium as opposed to depots present in looser perimysium. In most cases, compression and separation of bordering myofibers by the injected volumes of the test article (i.e., resulting in an increased initial hydrostatic pressure and volume displacement) were observed. An eosinophilic (protein-rich) exudate was most notable after 24 hr and was accompanied by dilated blood or lymphatic vessels (Supplementary Figure S2b).
Temporal evolution of key histopathological parameters following a single intramuscular injection of paliperidone palmitate long-acting injectable (•) or polystyrene (□) in the rat. Criteria for scoring are provided in the text. All parameters are expressed as mean scores on a semiquantitative scale (0–5) ± SD (n = 3).
Characteristic histopathological features of the acute inflammatory response (≤24 hr) initiated by a single intramuscular (IM) injection of paliperidone palmitate long-acting injectable (PP-LAI) or polystyrene (PS) in the rat hind limb. (A) Skeletal muscle fiber degeneration with (B) leukocytostasis and extravasation (PP-LAI, 4 hr). (C) Migration of blood-derived CD68+ macrophages from nearby and distant blood vessels toward the administration site (indicated by the white arrows) (PP-LAI, 24 hr). (D) Onset of depot infiltration by granulocytes and CD68+ macrophages (PP-LAI, 4 hr) and first evidence of phagocytosis of (E) PP-LAI and (F) PS by granulocytes after 4 hr. Low-magnification H&E overviews of the respective IM administration sites containing the depots formed by the PP-LAI or PS nano-/microparticles (indicated with *) are presented as insets. Portions of the depots, as seen at higher magnification, are indicated with (*) as well in panel A, C, D and F. The findings are representative of 3 animals per time point.
Degranulating perivascular mast cells were observed 4 hr after administration of the test articles (Supplementary Figure S2a). Leukocytostasis with margination and extravasation of white blood cells, mainly neutrophils and, to a lesser extent, CD68+ monocytes/macrophages, was observed in the proximity of the depots from 4 hr onward (Figure 3B). Initially, the leukocytes emigrated from postcapillary venules adjacent to the formulation depots. However, from 8 hr onward, extravasation from distant blood vessels and subsequent migration through the interstitial tissues (endo- and perimysium) became prominent (Figure 3C). Chemotaxis of neutrophils and macrophages led to their accumulation in the connective tissue surrounding the depots with focal accumulations at the interface with the injected test articles (Figures 3D and 2C).
As the recruitment of inflammatory cells persisted, the formulation depots became increasingly circumscribed by an expanding rim of infiltrating granulocytes (i.e., still the predominant cell type at 8 hr) and CD68+ monocyte-derived macrophages (Figure 2C–D). The first evidence of phagocytosis by the infiltrating neutrophils was already observed after 4 and 8 hr, for PS and PP-LAI, respectively (Figure 3E–F). After 24 hr, the phagocytosis was still limited and only neutrophils and macrophages (8–10 µm in size) lining the depots contained multiple solid spherical particles (PS) or slightly eosinophilic material (PP-LAI) within their cytoplasm (Figure 3E–F). The identity of the intracellular foreign content had previously been confirmed by means of fluorescence microscopy (PS) and polarized light microscopy (PP-LAI) on frozen sections as well as by transmission electron microscopy on paraformaldehyde/glutaraldehyde-fixed, epoxy resin-embedded, and uranyl acetate/lead-(II)-citrate stained ultrathin sections (Darville et al. 2014).
Initiation of tissue repair (24–48 hr)
The first indications of wound healing were observed after 24 hr. Regeneration of damaged myofibers was characterized by an increased number of nuclei from satellite cells and CD68+ macrophages, as well as the formation of myotubes. The activation of endothelial cells (i.e., hypertrophic cells) with budding and sprouting of capillaries from preexisting vessels started after 24 hr (Supplementary Figure S2c). However, capillary sprouts only started to infiltrate the formulation depots after 72 hr (Figures 2F and 4A). From 48 hr onward, the edema was rapidly substituted by loose interstitial fibrin (Supplementary Figure S2d). Spindle-shaped cells (fibroblasts and endothelial cells) were proliferating in the surrounding interstitium (Figure 4A) and indicated the formation of granulation tissue.
Characteristic histopathological features of the chronic inflammatory response (>24 hr) initiated by a single intramuscular (IM) injection of paliperidone palmitate long-acting injectable (PP-LAI) or polystyrene (PS) in the rat hind limb. (A) Spindle-shaped fibroblasts and activated endothelial cells with capillary sprouting (arrows) and microhemorrhages (PP-LAI, 72 hr). (B) Deep infiltrating phagocytic granulocytes (PS, 72 hr). (C) Large CD68+ macrophages containing numerous nano-/microparticles (PP-LAI, 14 days). (D) Near-total depot infiltration with decreased CD68+ macrophage cellularity in the outer portions of the granuloma (PP-LAI, 21 days). (E) Perivascular CD79b+ B cells (PP-LAI, 28 days). Low-magnification H&E overviews of the respective IM administration sites containing the depots formed by the PP-LAI or PS nano-/microparticles (indicated with *) are presented as insets. (F) Loaded macrophages in blood or lymphatic vessels adjacent to the formulation depots (PP-LAI, 72 hr). The findings are representative of 3 animals per time point.
Chronic inflammation (24 hr–14 days)
The host response to the tissue injury and persistent foreign material gradually evolved into a moderate to marked granulomatous chronic inflammatory reaction with a more heterogeneous histological presentation (Figure 2B). The moderate to marked infiltration of mononuclear cells, mainly activated macrophages, was the dominant feature of the chronic inflammatory reaction to both test articles (Figure 2D–E). After 48 hr, CD68+ macrophages and granulocytes formed radial migration tracks within the formulation depots, indicating a relatively dense nano-/microcrystal agglomerate that formed upon efflux of the vehicle. In PP-LAI depots, the number of granulocytes rapidly decreased, only for the macrophages to become the predominant cell type from 48 to 72 hr onward (Figure 2C–D). After PS injection, the presence of granulocytes was noted up to at least 7 days (Figure 2C). These granulocytes were consequently able to infiltrate PS much deeper toward the center, suggesting a looser structure of the PS depots (Figure 4B). The neutrophils showed eccentric, multilobulated nuclei and were slightly swollen due to the presence of numerous phagocytosed PS microspheres. The macrophages in the inflammatory rim were exclusively CD68+ and CD163−. A few lymphocytes were seen scattered throughout the interstitium adjacent to the depots from 24 hr onward. CD3-∊+ T cells were dispersed in gradually increasing numbers throughout the expanding inflammatory rim after 48–72 hr (Figure 2E). Moderate T-cell infiltrations were noted after 7 days, gradually declining for PS. In contrast, a sustained slight to moderate presence of T cells was observed in response to IM PP-LAI.
After 48 hr, the lesions were classified as foreign body granulomas, displaying a central, almost cell-free depot, which was entirely surrounded by a dense inflammatory rim (on average 340 µm, 48 hr after injection of PP-LAI). The capsule mainly consisted of epithelioid macrophages and included some T cells, young fibroblasts, vascular endothelial cells (cf. angiogenesis), and few granulocytes (Figure 2C–E). The ability of the macrophages to proliferate (cf. scattered mitotic figures) and the persistent recruitment of blood-derived macrophages led to rapid expansion of the inflammatory rim with a deep infiltration of the formulation depot after 7 days (Figure 2D). The infiltrated macrophages were enlarged due to the extensive phagocytosis of PP-LAI and PS particles, with dimensions reaching 14 and 18 µm after 48 to 72 hr and 7 to 14 days, respectively (Figure 4C). However, no MNGCs were noted in either type of formulation depot at the examined time points. The deep infiltration and marked prevalence of macrophages containing PP-LAI or PS particles within the heterogeneous inflammatory rim implied that an important fraction of the injected particles was present intracellularly in macrophages (Supplementary Figure S3d–e).
After 7 days, a minimal deposition of delicate collagen strands was observed in the outer portion of the inflammatory capsule (Supplementary Figure S2f). The superficial angiogenesis seen after 48 hr turned into a moderate to marked radial vascularization of the granuloma after 7 days (Figures 2F and Supplementary Figure S2e).
Foreign material resorption and wound healing (14–28 days)
After 14 days, the cellular infiltration of the remaining depots was near complete (Figures 2D and 4C–D). The depots were completely substituted by infiltrated cells from 21 days onward in all animals except 1, in which a surprisingly low cellular infiltration was observed (similar to the extent observed after 72 hr–7 days). The relative contribution of the macrophages to the total formulation cellularity appeared to gradually decline as the prevalence of T cells and, to a lesser extent, of fibroblasts in the outer layers continued to increase (Figures 2E and 4D; Supplementary Figure S3c–d). Few perivascular CD79b+ plasma cells were found from 14 and 7 days onward in some PP-LAI and PS depots, respectively (Figure 4E and Supplementary Figure S3b). The prominent vascularization of the granulomas remained stable from 14 days onward, indicating a sufficient irrigation for the sustainment of the healing response (Figure 2F). Muscle damage or signs of active regeneration were no longer observed from 21 days onward (Supplementary Figure S3a). After 28 days, the resorption was incomplete for both test articles. The general size of the inflammatory lesions clearly diminished for PP-LAI, while persistent granulomas were seen for the nondegradable PS microspheres (Supplementary Figure S3d–e).
Evaluation of the Draining ILNs
The ILNs of some animals were slightly swollen and moderately hemorrhagic during the first 48 to 72 hr, independent of the test article. A marked yellow discoloration, with increasing intensity over time, was noted from 72 hr onward in all subjects having received PS (Figure 5A).
Lymph node accumulation and retention of intramuscular (IM) paliperidone palmitate long-acting injectable (PP-LAI) and polystyrene (PS). (A) Yellow discoloration of the draining iliac lymph node (ILN) 7 days after IM PS administration. (B) Intracellular fluorescent PS microspheres in macrophages in the transverse sinuses near the capsule. Inset: macrophage containing intracellular PS. (C) Sinus histiocytosis in ILN 72 hr after IM administration of PP-LAI. (D) Polarized light micrograph showing birefringent particles (PP-LAI nano-/microcrystals) in the medullary sinuses after 72 hr. Inset: cluster of PP-LAI nano-/microcrystals in the lymph node cortex 7 days after IM PP-LAI administration.
At histology, an increase in macrophages was observed in the transverse sinuses near the capsule at 48 hr, this progressed to sinus histiocytosis in the majority of the ILNs from the 72 hr time point onward (Figure 5C). The severity of the sinus histiocytosis declined after 3 weeks. However, sinus histiocytosis was still noted in one ILN at the 4-week time point.
From 48 hr onward, multifocal ORO-positive staining of micron-sized lipid droplets, mainly located in clustered macrophages in the transverse sinuses near the capsule, was observed. Birefringent particles (PP-LAI nano-/microcrystals) were detected mainly within the medullary sinuses (Figure 5D) and occasionally as clustered particles in the ILN cortex (Figure 5D, inset) 48 and 72 hr and 7 days after PP-LAI administration.
Under fluorescence microscopy, multiple individual PS microspheres were seen in macrophages in the transverse sinuses from 24 hr onward (Figure 5B). The extent of lymphatic accumulation rapidly increased with considerable amounts of PS having been relocated to the ILN after 7 days. An ORO-positive cortical staining similar to that observed with PP-LAI was seen in some animals. The mechanisms of lymph node accumulation were not explored in this study. However, evidence of macrophages loaded with intracytoplasmic particles within blood or lymphatic vessels was found on H&E, CD68, and CD31 sections of the PP-LAI IM administration sites after 48–72 hr (Figure 4F). In addition, lymphatic absorption and subsequent lymph node retention of PP-LAI were demonstrated by bioanalysis of the draining lymph nodes (cf. infra).
Lymph Node Retention of PP-LAI
The wet weights of the draining/regional lymph nodes as a function of time after IM injection of PP-LAI in rats are presented in Figure 6. A transient increase in ILN and PLN weights on day 1 after PP-LAI administration was observed, presumably due to the increased lymphatic drainage that was induced by the injected fluid volume and the edema which accompanied the acute inflammation of the injection site. The ILN weights were significantly increased by day 7, with a 127.4% increase in weight observed by day 14 (Figure 6a), which correlated histologically with sinus histiocytosis. The qualitative features of the ILN weight evolution resembled those of the PP concentration–time profiles in the ILNs (cf. infra). The PLN weight gain was more gradual but statistically significant (even when normalized for the increasing total body weight). Maximal weights (i.e., 76.9% increase as compared to day 0) were observed on day 28 (Figure 6b).
Weights of the primary draining/regional lymph nodes in rats as a function of time after intramuscular administration of paliperidone palmitate long-acting injectable. (a) Draining medial iliac lymph node weights. (b) Ipsilateral popliteal lymph node weights. Data represent individual and mean ± SE (n ≥ 6) wet weights immediately after necropsy. Statistically significant differences between the two groups are indicated with **p < .01 and ***p < .001.
The PP and PAL concentrations measured in the primary draining/regional lymph nodes (i.e., ILN and PLN) of rats having received a single IM injection of PP-LAI are depicted in Figure 7. High PP and PAL concentrations were detected in ILN and PLN from day 1 onward (Figure 7a), indicating lymphatic accumulation of PP and, to a lesser extent, of PAL.
Lymph node retention of paliperidone palmitate (PP) and paliperidone (PAL). (a) Apparent PP (red) and PAL (blue) concentrations in the draining iliac lymph node (ILN; full lines) and popliteal lymph node (PLN; dashed lines), expressed in nanogram, PP/PAL per gram lymph node. (b) Recovery of PP/PAL per gram primary draining lymph node (i.e., ILN + PLN) expressed as percentage of the total PAL equivalent dose. All data represent mean values ± SE (n ≥ 6).
Following IM injection of PP-LAI, a rapid and extensive PP and PAL accumulation occurred during the first 24 hr. The highest concentrations were observed on day 7 for both PP and PAL, irrespective of the lymph node. The concentrations in the lymph nodes steeply declined after 14 days to reach low but still measurable concentrations by day 28. Generally, the PP concentrations were approximately 2–3 orders of magnitude higher than the corresponding PAL concentrations and lymph node retention of both compounds was greater (approximately 1 order of magnitude) in the draining ILN than in the regional PLN (Figure 7a).
Remarkably, the lymph node concentration–time profiles displayed qualitative features very similar to those of the PAL plasma concentration–time profiles reported in a previous pharmacokinetic study in rats with IM PP-LAI (Darville et al. 2014). PAL concentrations (expressed as ng/g lymph node) were generally higher (approximately 1 order of magnitude) than the PAL plasma concentrations observed under identical dosing conditions. Since systemic concentrations of PP following IM injection of PP-LAI are generally much lower than the corresponding PAL concentrations due to the rapid ester hydrolysis, and because the aqueous solubility of PP is lower than the reported quantification limit, the very high local concentrations of PP strongly indicate that most of the measured PP accumulates as solid PP-LAI nano-/microparticles. The latter was confirmed by the extensive retention of birefringent micron-sized particles in the medullary sinuses of the draining lymph nodes from 72 hr onward, as observed under polarized light micrograph (Figure 5D).
However, the proportion of the administered PP-LAI dose retained in the primary draining lymph nodes (i.e., the combined net amount of PP and PAL in ILN and PLN, for a given time point) did not exceed 0.98% ± 0.478% (on day 7) of the administered PP-LAI dose (Figure 7b). The cumulative combined lymph node retention amounted to 1.97% ± 0.66% of the administered PP-LAI dose. Although the lymph node retention might have been underestimated due to the simultaneous elimination of PP and PAL from the lymph nodes (i.e., dissolution and efferent lymphatic transport with systemic absorption), these observations strongly indicate a negligible net contribution of the lymph node retention to the PAL systemic absorption and the previously reported multiphasic pharmacokinetics.
Changes in Cytokine Levels in ISF in Response to PP-LAI Injection
ISF sample volumes did not allow cytokine analysis on days 14, 21, and 28. In addition, only 1 individual control sample yielded sufficient ISF for cytokine analysis, while the remaining control samples needed to be pooled. The time courses of selected cytokines involved in the acute and chronic host response are presented in Figures 8 and 9, respectively.
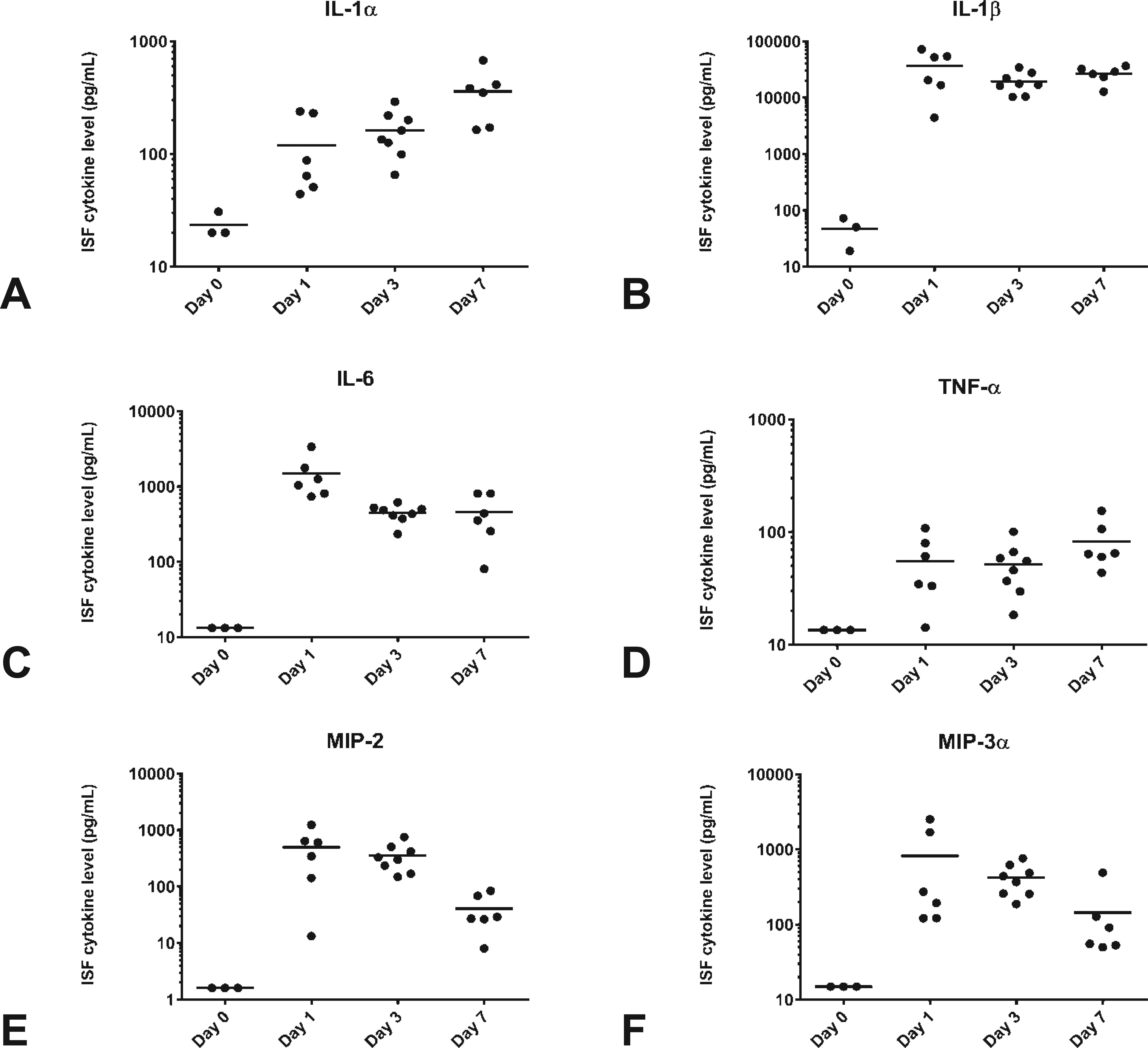
Changes in early phase cytokine concentrations (A–F) in injection site fluid filtrate prior to (day 0) and 1, 3, and 7 days after a single intramuscular injection of paliperidone palmitate long-acting injectable in the rat. The horizontal bars represent the means of the respective individual cytokine/growth factor concentrations (data points).
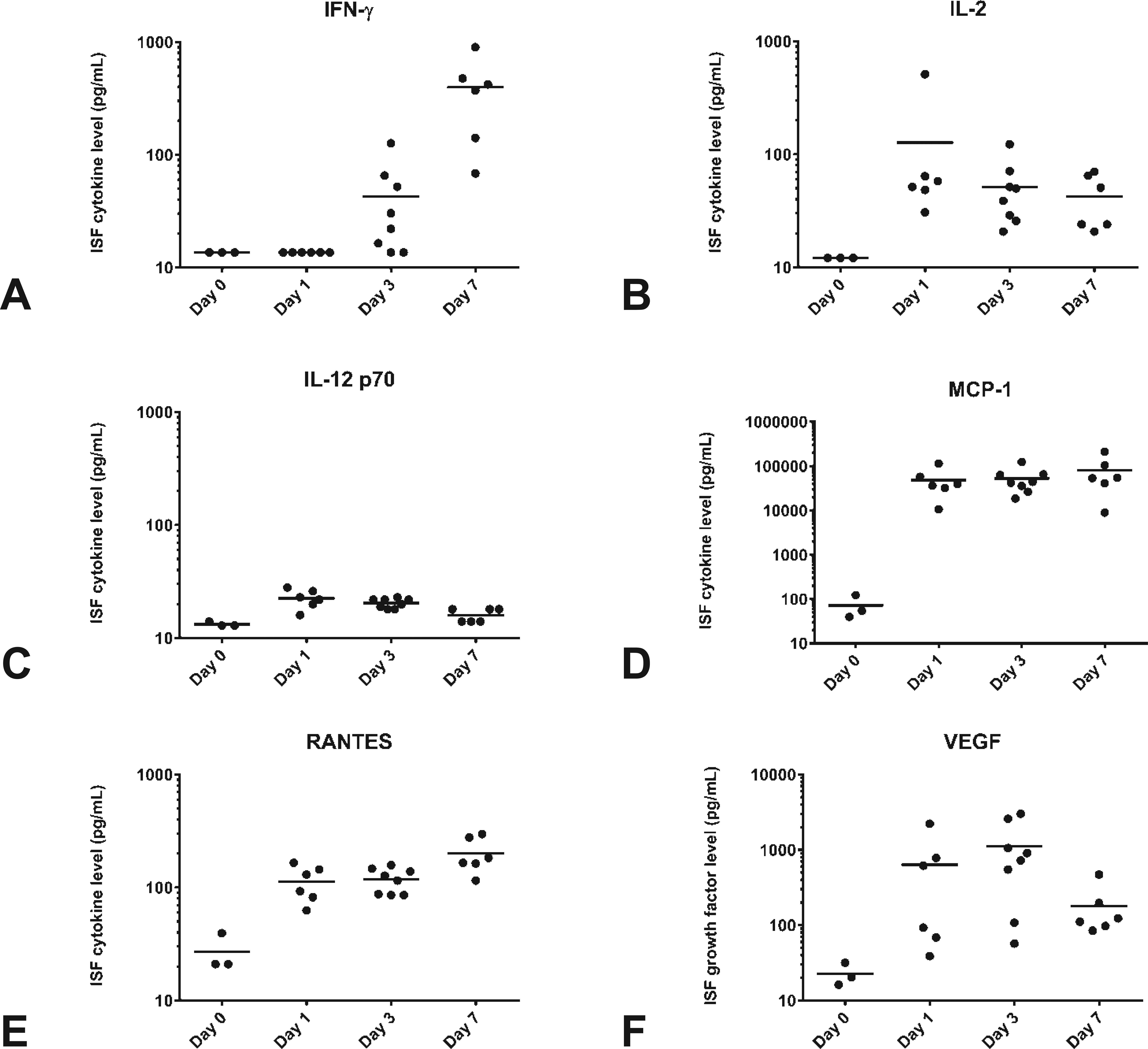
Changes in late phase cytokine (A–E) and (F) vascular endothelial growth factor concentrations in injection site fluid filtrate prior to (day 0) and 1, 3, and 7 days after a single intramuscular injection of paliperidone palmitate long-acting injectable in the rat. The horizontal bars represent the means of the respective individual cytokine/growth factor concentrations (data points).
The most pronounced increases compared to the control group were observed for IL-1β and MCP-1, but also IFN-γ, IL-1α, IL-6, MIP-2, MIP-3α, RANTES, and VEGF showed strong increases. For most cytokines, a high interanimal variation was observed. In addition, moderate elevations in IL-2 and TNF-α were found, while IL-12p70 only showed a marginal increase with concentrations only just above the limit of quantification.
The highest IL-1β, IL-6, MIP-2, MIP-3α, and VEGF levels were found on days 1 to 3, but concentrations were still elevated compared to the control group on day 7. Increases in IL-2, MCP1, and TNF-α were comparable on days 1 to 7. IL-1α and RANTES concentrations increased from day 1 onward, reaching the highest levels on day 7, while IFN-γ only increased from day 3 onward, peaking after 7 days. IL-12p70 only showed a marginal increase compared to the control group.
Quantitative Evaluation and Modeling of the Depot Infiltration
Depot geometry
The depot location frequencies and geometry descriptors for both test articles are summarized in Table 2. The majority of the IM injections resulted in a single, well-defined depot being located in the peri- or epimysium. In about 10% of the animals, the formulation was mainly present in endomysial tissue (i.e., true IM depot). A limited number of injections resulted in the combined presence of formulation in interfascial and deep IM connective tissue. No correlations were found between the depot location and the time elapsed after injection. These findings highlight the low probability of achieving deep IM injections in rodent animal models. As previously suggested, the location of the formulation might influence the dynamics of the inflammatory response as well as the pharmacokinetics (Darville et al. 2014).
Descriptive Statistics of PP-LAI and PS Depot Parameters.
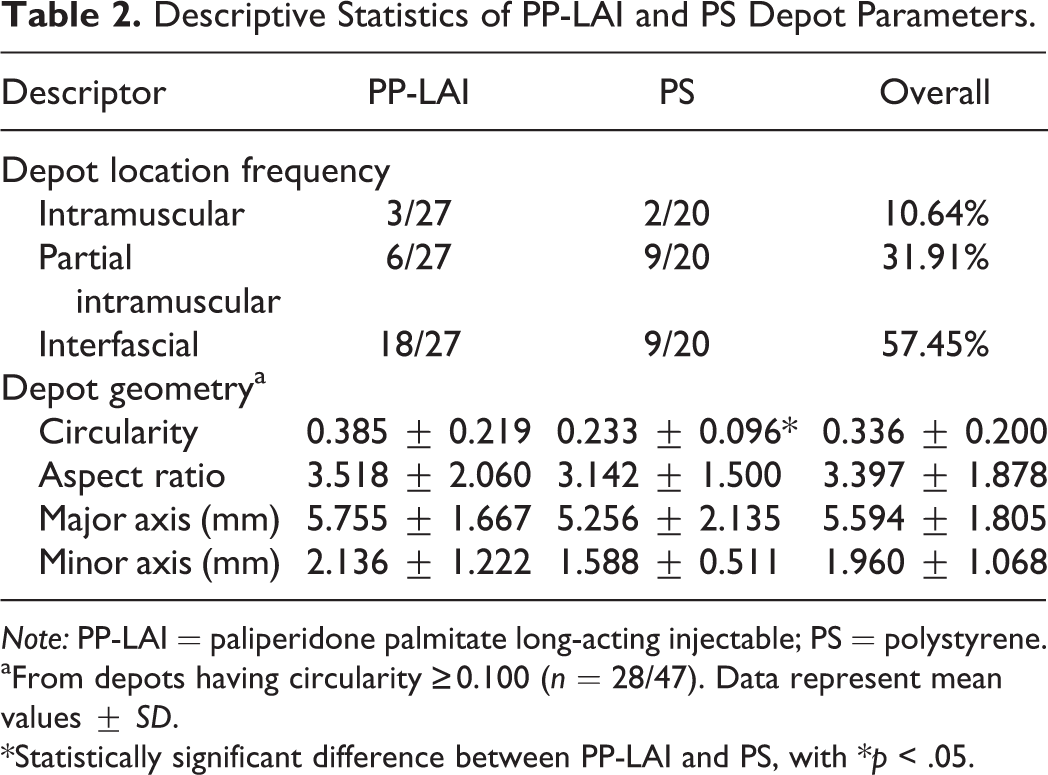
Note: PP-LAI = paliperidone palmitate long-acting injectable; PS = polystyrene.
aFrom depots having circularity ≥0.100 (n = 28/47). Data represent mean values ± SD.
*Statistically significant difference between PP-LAI and PS, with *p < .05.
The observed depot geometry was greatly influenced by the location of the formulation within the skeletal muscle tissue. Depots present in the interfascial spaces were characterized by symmetry along the 2 cross-sectional axes and high cross-sectional area to perimeter ratios. Twenty-six of 27 interfascial depots had C ≥ 0.1, a threshold selected post factum based on the apparent depot location and appearance (see H&E insets in Figures 3 and 4). The shape of the majority of the depot cross sections could thus be approximated by an ellipse. Fitting the depot demarcations with an ellipse that has an identical area, orientation, and centroid yielded dimensions and geometry descriptors that could be used for the subsequent estimation of prolate (infiltrated) depot volumes (Figure 1 and Table 2). In general, PP-LAI and PS formulation depots showed comparable average geometries, except for the circularity, which was slightly lower in case of PS, presumably due to the higher prevalence (not statistically significant) of (partial) IM injections in this group. The approximation of the 3-dimensional shape of formulation depots with C ≥ 0.1 by a prolate spheroid was supported by the transversal symmetry observed in sequential sections of the administration sites. Since all cross sections used for extrapolation were taken at or near the center of the depot and represented the maximal cross-sectional area of the depot, the proposed prolate geometry assumption was justified. For the depots whose cross sections strongly deviated from an ellipsoid shape (i.e., C < 0.1), absolute volume calculations were made using the respective measured areas, in conjunction with the average aspect ratio obtained from ellipsoid depots (C ≥ 0.1).
Depot cellularization
The primary parameter for all subsequent calculations, which was directly obtained from quantitative image analysis, was the total cross-sectional area of the formulation depots (i.e., including cellular infiltration; Sdepot ). Since the depot integrity was preserved, and clear depot demarcations were identifiable at all times, the integration of polygonal selections that were representative of a median cross section was possible (cf. Figure 1). The individual and average PP-LAI and PS depot areas, irrespective of the geometry, are presented in Figure 10A–B. It follows from the assumption of prolate geometry with symmetry along the longest axis that the total depot volumes were characterized by qualitatively similar profiles (data not shown). Hence, both parameters are descriptors of the “size” of the depots and are used interchangeably in this context.
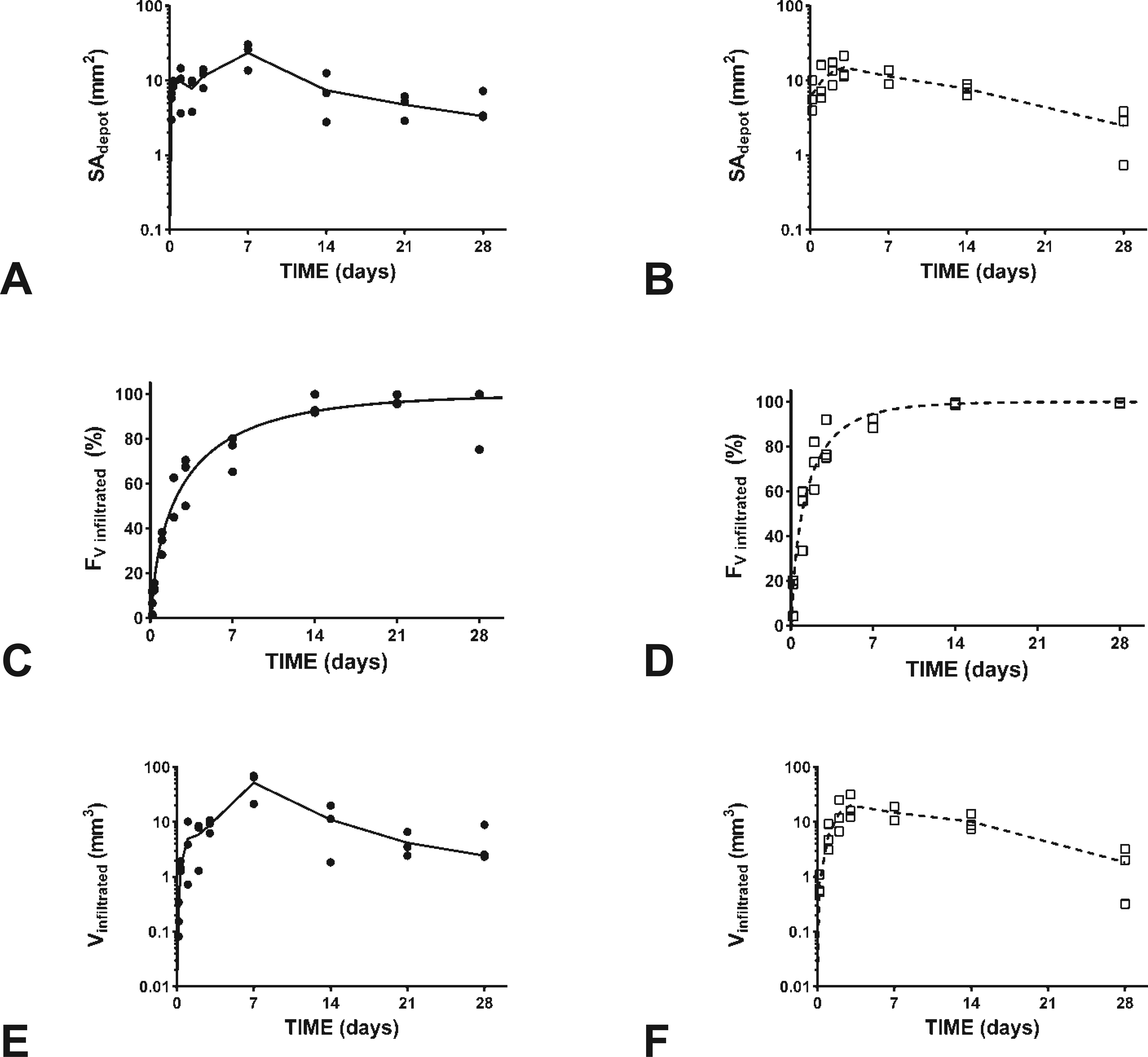
Quantitative characterization of the paliperidone palmitate long-acting injectable (•) and polystyrene (□) depot dimensions and cellularization as a function of time after a single intramuscular administration in the rat. (A) and (B) Measured individual (data points) and mean (lines) absolute formulation depot cross-sectional areas. (C) and (D) Calculated volume fractions of the formulation depots being infiltrated by inflammatory cells (data points) and best fits of the 3-parameter cumulative Weibull distribution (lines). (E) and (F) Calculated individual (data points) and mean (lines) absolute formulation depot volumes infiltrated by inflammatory cells.
The calculated depot volumes at 4 hr after PP-LAI or PS injection (5.65 mm3 on average) were significantly smaller than the injection volumes (i.e., 200 µl/kg body weight) and approximated the volume of solid (i.e., 156 mg/ml formulation) that had been administered. Only a slight increase in depot dimensions was seen during the first 48 hr, while the initial depot geometries and well-defined boundaries remained preserved over time (Figure 10A–B). The depots reached maximal dimensions 7 and 3 days after PP-LAI and PS injection, respectively (Figure 10C–D). The apparent size of the granulomas was gradually decreasing from 7 days onward and was in line with the histopathological findings.
The volume fraction of the formulation depot that was infiltrated (FV,infiltr. ) could directly be calculated from measured fraction of the cross-sectional infiltrated area (FS,infiltr. ; see Figure S4c–d and derivation in Supplemental Material). The corresponding FV,infiltr. data are presented in Figure 10C–D, and the nonlinear regression parameters are summarized in Table 3. The 3-parameter Weibull distribution could adequately describe both data sets (R 2 > 0.94). The identified outlier resulted from the 1 animal that showed an unusually low infiltration (cf. supra) and was therefore excluded for fitting and subsequent volume calculations. The calculated gradual infiltration correlated well with the semiquantitative findings on macrophages and T cells.
Determination Coefficients and Model Parameters of the Modified Cumulative 3-parameter Weibull Distribution Model Obtained through Nonlinear Regression for the Fraction of Depot Volume (FV,infiltr. ) Infiltrated.a,b
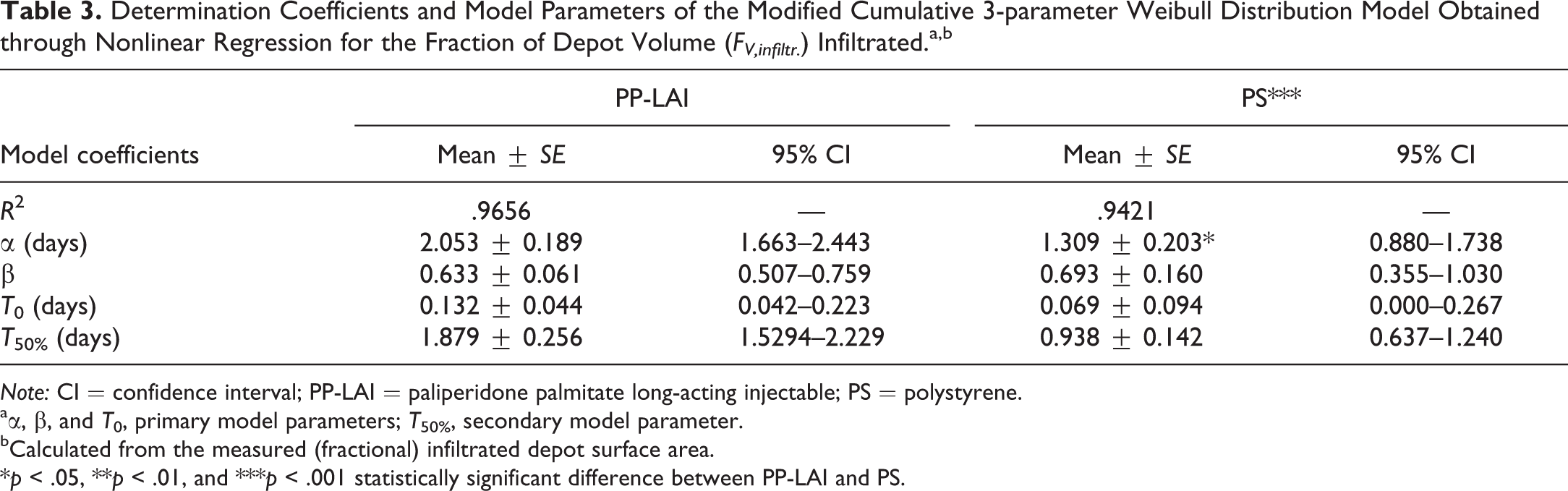
Note: CI = confidence interval; PP-LAI = paliperidone palmitate long-acting injectable; PS = polystyrene.
aα, β, and T 0, primary model parameters; T 50%, secondary model parameter.
bCalculated from the measured (fractional) infiltrated depot surface area.
*p < .05, **p < .01, and ***p < .001 statistically significant difference between PP-LAI and PS.
The calculated net volumes of the PP-LAI and PS formulation depots that were infiltrated by inflammatory cells (Vinfiltr. ) are presented in Figure 10E–F and were similar. The temporal evolution of Vinfiltr. was analogous to that of Sdepot (Figure 10A–B) and qualitatively resembled the shape of the PAL plasma concentration–time profiles observed in rats upon IM administration of an identical dose of PP-LAI (Darville et al. 2014).
The time to onset of depot infiltration (T 0 = 3.2 ± 1 hr for PP-LAI) and the slightly but significantly faster infiltration of the PS depots (α = 31 hr) in comparison to PP-LAI (α = 49 hr) were in line with the histopathological observations (Figure 2C–E and Table 3). T 50% values of approximately 2 and 1 day(s) after IM injection of identical doses of PP-LAI and PS, respectively, might have been underestimated (cf. limited macrophage recruitment and infiltration at these time points). Nevertheless, they provide an estimate for the fast and pronounced depot infiltration, which could easily be underrated based on 2-dimensional histological sections only.
Depot vascularization
The dynamics of the depot vascularization (CD31+) were in accordance with the semiquantitative histopathological data (Figure S4e–f, Supplemental Material). The observed angiogenic area appeared to be maximal after 7 days and gradually decreased at a similar rate as Vinfiltr.. The data scatter in the PP-LAI group could partly be explained by interindividual variability in the extent of angiogenesis but might also have been the consequence of the inability to accurately estimate the angiogenic area based on the image analysis of a single depot cross section (cf. transverse vs. longitudinal sections of CD31+ vessels).
Discussion
With the present study, we aimed to expand our previous work, in which we explored the complex local disposition of a commercially available LAI nano-/microsuspension of the antipsychotic prodrug PP in the rat and investigated the concurrent pharmacokinetics (Darville et al. 2014). Our aim was to further elucidate the nature and dynamics of the ISR to LAIs, to identify critical time points and parameters for the evaluation of the IM administration sites, to include quantitative image analysis and modeling to investigate the formulation depot geometry and cellularization, and to evaluate the utility of inert spherical PS microspheres as model particles. In addition, we wanted to gain insight in the contribution of lymphatic drug absorption and lymph node retention of LAI nano-/microparticles.
The biocompatibility of SC and, to a lesser extent, IM implantable biodegradable polymeric materials (e.g., poly lactic-co-glycolic acid (PLGA) microspheres, polyethylene terephthalate fabrics, etc.) and lipid-based solid implants have been investigated thoroughly in the past (F. D. Anderson et al. 1993; Hagerty et al. 2000; Marchant, Anderson, and Dillingham 1986; Muhamed et al. 2013; van Bilsen et al. 2004; Yamaguchi and Anderson 1992, 1993). Also, an increasing number of studies have reported on the surface chemistry–dependent foreign body reaction to synthetic biomaterials by quantifying the cytokine (mRNA or protein) levels in exudate surrounding the implants (Brodbeck et al. 2003; Luttikhuizen et al. 2007; Rodriguez, Meyerson, and Anderson 2009; Schutte et al. 2009). In contrast, only a few case reports on the local response to the SC or IM injection of aqueous LAI suspensions of pure drug nano-/microcrystals are available to date.
After a single IM bolus injection of PP-LAI in rats, the nature, extent, and time course of the ISR were compared to those seen after IM injection of equal volumes of an analog suspension containing nonfunctionalized insoluble PS microspheres of approximately the same size (1.0 µm). The IM injection of PP-LAI or PS in the rat induced a moderate to marked, localized ISR during the observation period of 28 days. Overall, the 2 test formulations appeared to be well tolerated in the rat, which was in accordance with the tolerability profile (i.e., clinical observations only) of PP-LAI in humans (Hough et al. 2009). The used volume of 200 µl/kg body weight in the musculus biceps femoris was in line with the 0.1 ml proposed by Grim and coworkers as an optimal volume (1988). This was supported by the injection of identical volumes of vehicle, which only resulted in a short-lived mild acute inflammation similar to that induced by the injection of sterile saline (Darville et al. 2014; Thuilliez et al. 2009). Conversely, the sustained response to the persisting presence of foreign PP-LAI or PS microparticles could be described as a multimodal process (J. M. Anderson and McNally 2011). A short trauma-induced acute inflammation was rapidly followed by the formation of granulation tissue and evolved into a chronic inflammatory reaction with slow resolution of the IM formulation depot and tissue lesions. The progression of the general inflammation was similar to that reported upon SC injection of naltrexone-loaded PLGA microspheres (25–150 µm) in the rat (Yamaguchi and Anderson 1992). The type of inflammatory response resembled the one encountered after SC injection of an LAI olanzapine microsuspension in the rat, except for the depot cellularization, which was less pronounced in that study (Paquette et al. 2014).
Immediately after injection of PP-LAI or PS (i.e., >4 hr), the typical signs of a mild to moderate acute inflammation were observed. During the acute phase of the inflammatory reaction, nonspecific adsorption of host proteins to the injected nano-/microparticles might influence the host response, in particular the particle phagocytosis, and thereby the rate of drug release/absorption (Wilson et al. 2005). In line with the early development of edema, nonspecific adsorption of plasma-derived proteins was likely to be immediate (Fogh-Andersen et al. 1995). Hemorrhages caused by the injection procedure might facilitate the protein adsorption. In addition, degranulation of mast cells, which was also noted during the acute phase, plays an important role in the protein adsorption. Also, some common suspension stabilizers, for example, polysorbate 20 (Tween® 20), have been shown to activate the release of complement C3a. C3a is a potent leukocyte chemoattractant that is capable of inducing mast cell degranulation (Weiszhár et al. 2012). The histamine released during degranulation presumably contributed to the increased vascular permeability and, hence, the rapid formation of a moderate protein-rich edema.
The complex protein adsorption pattern (i.e., type, extent, and conformation) plays a major role in the regulation of the host response and can affect phagocytosis, as inflammatory cells interact with the adsorbed protein layer (e.g., through integrin receptors) rather than directly with the biomaterial surface (Thiele et al. 2003; Wilson et al. 2005; J. M. Anderson, Rodriguez, and Chang 2008). Conversely, the adsorbed protein layer is a reflection of the material’s surface properties and is generally known to be greatly influenced thereby (Müller et al. 2003). Hence, the nano-/microparticle surface properties likely modulate the progress of the overall host response. Proteins that typically adsorb following tissue trauma and have the ability to facilitate recognition, cell adhesion, recruitment, and/or activation include fibrinogen, fibronectin, vitronectin, IgG, and complement proteins (Jenney and Anderson 2000; Brodbeck et al. 2003). Based on the semiquantitative assessments and quantitative measurements, no major differences were noted in the phagocytic response for PP-LAI and PS; both showed early recruitment of phagocytes and similar onset and degree of depot infiltration. These findings suggested a similar protein adsorption onto both types of microparticles in spite of the presence of polyethoxylated suspension stabilizers (i.e., Tween® 20 and polyethylene glycol 4000), which adsorb onto the hydrophobic PP-LAI and PS surfaces and are known to reduce opsonization by steric hindrance (Owens and Peppas 2006; Torchilin 2012).
The local injuries to vascular, connective, and muscular tissues caused by the injection procedure and the concomitant tissue perturbation led to the above activation of the host defense mechanisms. This was characterized by the extravasation and recruitment of cells of the myeloid lineage, predominantly neutrophils as well as blood-derived monocytes/macrophages. In addition, the concentrations of multiple (sub-)acute and chronic inflammatory cytokines and chemokines were elevated in inflammatory exudates (ISF) from day 1 onward, indicating a considerable inflammatory response. In general, the cytokine profile observed after an IM injection of PP-LAI was in line with the findings by Paquette and coworkers who recently highlighted the compound-specific nature of the profile after SC injection of 2 other LAI microsuspensions of atypical antipsychotics (Paquette et al. 2014). Particularly, the strong increase in IL-1β and MCP-1 stood out in the current study. Also, IL-1α and TNF-α, which are strongly involved in innate immunity, were elevated. These cytokines are secreted by mast cells, endothelial cells, and activated macrophages in response to tissue damage and induce the endothelial chemokine production and the local expression of endothelial adhesion molecules, hence promoting the extravasation of immunocompetent neutrophils and macrophages to the injured extravascular spaces (Dinarello 2009; Rider et al. 2011). Furthermore, increases in IL-6, MIP-2, and MIP-3α were consistent with the IL-1β increase, which is a known inducer of these cytokines/chemokines. All these observations are in good agreement with the qualitative and semiquantitative histopathology data and support a critical role for IL-1β during the early inflammatory response.
In the present study, the evaluation of immune activation outside the injection site was limited to morphological evaluation of the draining lymph nodes, which showed no indications for immunostimulation. This was in good agreement with the findings reported by Paquette et al. (2014), which indicated that the IM injection of LAI drug microsuspensions typically has no impact on the general immune state of injected animals.
The first indications of wound healing that comprised a mixed population of macrophages and proliferating fibroblasts at the depot interface, as well as the neovascularization of the inflammatory rim, were perceived 24 to 48 hr after IM injection of PP-LAI or PS. The formation of granulation tissue, which consisted of a clear demarcation of the formulation depot by a thin layer of macrophages, fibroblasts, endothelial cells, and fibrin, was the hallmark of the tissue repair. This process was independent of the test article but seemed to be more apparent in case the formulation depots were located in perimysial interstitium. This was attributed to the easier access of the infiltrating cells from all directions through the looser connective tissue, as compared to the focal and sometimes distant extravasation and migration locations in deep IM endomysium.
An important component of the cellularization of the formulation depots and, hence, of the removal of particulate material and tissue repair, is the angiogenesis. Macrophages, IL-1β, and chemoattractants (e.g., MIP-2) greatly contribute to the release of proangiogenic factors, such as VEGF and TNF-α (Brodbeck et al. 2003; Xia and Triffitt 2006; Luttikhuizen, Harmsen, and van Luyn 2006; Dinarello 2009). Expected low oxygen levels within the formulation depots (cf. oxygen diffusivity in tissue ∼1.5 ×10−5 cm2/s) provided an additional stimulant for the macrophage infiltration, followed by their immobilization in hypoxic areas (or upon recognition of foreign particles, hence the concentric cellularization process; Lewis et al. 1999). Upon injection of PP-LAI and PS, the highest concentrations of VEGF were seen on days 1–3, which coincided with the onset of the depot vascularization (capillary sprout formation). As the radial vascularization increased, less VEGF was required for the formation of new capillaries. Therefore, the lower VEGF levels measured after 7 days were expected to further decrease with time, as was also reported by Paquette and colleagues (2014).
Although not specifically evaluated in this study (cf. CD31 is marker for blood vascular and lymphatic endothelium), lymphangiogenesis is known to occur in areas that require greater removal of excess fluid or cellular debris and often accompanies angiogenesis to alleviate the increased interstitial pressure resulting from the leakiness of the nascent blood capillaries (cf. efflux of leukocytes, macromolecules, and plasma filtrate; Cromer et al. 2014; Alitalo and Carmeliet 2002). As is the case with blood vascular endothelial cells, it has been described that several of the inflammatory cytokines elevated in the current study (e.g., IL-1β, IL-6, and TNF-α) can increase lymphatic endothelial cell permeability in vitro (Cromer et al. 2014).
Lymphatic capillaries have an incomplete or absent basement membrane and the overlapping “cleft-like” intercellular junctions between overlapping adjacent endothelial cells, which vary from 15 nm to several microns, are known to open and close in response to variations in interstitial volume and pressure (McLennan, Porter, and Charman 2005). Submicron particulates could be transported via lymph and accumulate in draining lymph nodes or enter the systemic blood circulation through the thoracic duct (Ikomi et al. 1996; Swartz 2001). Although larger particles are more effectively retained in lymph nodes by filtration or phagocytosis in the medullary sinuses, their passive lymphatic uptake decreases with increasing particle size (Oussoren et al. 1997a). Lymphatic uptake has been demonstrated for PS nanospheres up to 260 nm in size following SC administration (Hawley, Davis, and Illum 1995). Also, van’t Klooster and colleagues hypothesized, based on the high local rilpivirine concentrations and the concurrent absence of lymph node toxicity after IM injection of a 200 nm LAI nanosuspension in dogs, that rilpivirine nanocrystals entered the lymphatics to form secondary drug reservoirs in the draining lymph nodes (van’t Klooster et al. 2010). Therefore, it is clear that special attention should be given to the assessment of lymph nodes that are associated with the route of administration of a test article (Elmore 2006). The knowledge of the physicochemical properties of the administered test article may support the unambiguous identification of phagocytosed material. For example, in the present case, practically insoluble crystalline PP-LAI particles could be seen as intracytoplasmic birefringent particles under polarized light microscopy, demonstrating the lymphatic transport and subsequent lymph node retention of PP-LAI from 24 to 48 hr onward.
Since excess fluid can cause an increase in interstitial pressure and facilitate lymph formation and transport, the site of injection and the injection procedure itself may be important determinants of the efficiency of the lymphatic drainage. Oussoren et al. reported higher lymphatic absorption of liposomes after injection in the tight and adipose-free SC tissue of the footpad of rats, as opposed to the loose and fatty SC tissue of the abdominal flank (1997b). The differences in lymphatic uptake were attributed to dissimilarities in the structural organization of the SC administration sites, with a lesser spreading, and thus higher interstitial pressure expected in the dense structure of the footpad subcutis. Similarly, the injection of PP-LAI or PS in the tight skeletal muscle matrix might have generated a (temporary) high interstitial pressure that promoted lymphatic uptake of solid particulates. Furthermore, muscle activity promotes lymph formation and unidirectional propulsion (Swartz 2001). The PP-LAI and PS particles may also have been transported from the IM injection site to the lymph node by phagocytic macrophages. Ikomi et al. have reported that leukocytes (∼6 µm in diameter) can enter the lymphatic system via the intercellular lymphatic junctions (1996). In the present study, CD68+ macrophages that were apparently loaded with particulate material were observed within CD31+ vessels, indicating a possible active migration of macrophages through the (newly formed) lymphatics toward the draining lymph nodes. Nevertheless, the precise mechanisms of the lymph node retention or relocation of drug nano-/microcrystals remain unknown to date. It is important to stress, however, that despite the high concentrations of PP and PAL measured in the draining lymph nodes, the net amount of lymphatic PP/PAL only amounted for a minor fraction of the administered PP-LAI dose. Hence, the contribution of lymphatic absorption to the previously reported systemic PAL plasma exposure was most likely negligible (Darville et al. 2014).
In general, an identical progression of the host response was perceived for PP-LAI and PS until 48 hr, after which the inflammatory response to the latter was slightly more pronounced. The nature of the ISR remained remarkably similar, with the exception of the stronger and longer residence of granulocytes upon PS injection and the more sustained maximal macrophage infiltration. The macrophages in the inflammatory rim delineating and infiltrating both test-article depots were exclusively CD68+ and CD163−. McLennans (1993) demonstrated that the phagocytosing macrophages in degenerating rat skeletal muscle fibers were all ED1+ and ED2−. He described that ED1+ monocytes/macrophages were attracted to the damaged fibers from adjacent arterioles, which is in line with the extravasation from distant blood vessels and migration toward the depot, as we noted. This was supported by the expression of the rat CD68/ED1-antigen on the membranes of cytoplasmic granules, like phagolysosomes, as well as on the cell surface of monocytes and inflammatory macrophages. The amount of ED1 expression in a single cell can be correlated to its phagocytic activity, explaining the strong expression we noted in the inflammatory rim (Damoiseaux et al. 1994). The CD163/ED2-antigen is constitutively expressed on most subpopulations of mature tissue macrophages in rats, and a link between CD163 and a proinflammatory macrophage phenotype was proposed (Polfliet et al. 2006). Since PS microspheres are insoluble in aqueous media, the chronic inflammation was the result of the persistence of solid micron-sized particles, rather than of chemical irritation. Based on the analogy in ISR presentation, the same was assumed for PP-LAI. The analogous histology profiles and proficient phagocytosis in both cases suggested that both types of particles, although chemically distinct, might have induced similar cytokine profiles and displayed comparable surface characteristics (cf. protein coat) in vivo. However, cytokine data for PS were not available for comparison. Nonetheless, a similar apparent lack of effect of the material surface chemistry on the types and sequence of infiltrating cells has been observed by Schutte et al., following SC injection of 3 different nondegradable polymers. Although a few cytokines were differently expressed, the cumulative concentrations of the cytokines, when classified based on their inflammatory versus wound healing roles, were not significantly affected by the surface properties of these materials (Schutte et al. 2009; Brodbeck et al. 2003).
In the present study, special attention was given to the assessment of the early response to IM injection of LAIs by including multiple time points (i.e., 4, 8, 24, and 48 hr). Indeed, for products that intentionally degrade, it is important to include interim assessments and evaluate the host response prior to significant degradation of the implanted materials. This is most relevant for slowly dissolving drug LAI nano-/microsuspensions, since the local tissue response to IM injections of such formulations is a possible determinant of the drug dissolution and pharmacokinetics (van’t Klooster et al. 2010). For example, the granuloma formation, the extensive intracellular accumulation of formulation by phagocytosis, and the depot vascularization are thought to regulate the drug absorption after IM injection of PP-LAI in the rat (Darville et al. 2014). Similarly, the formation of a dense fibrous capsule around bioerodible norethindrone/cholesterol SC implants, and the active processing thereof by inflammatory components, have been hypothesized to be drug absorption rate limiting (F. D. Anderson et al. 1993). Finally, the physical behavior of the formulation (e.g., the formulation spreading within the connective tissues, particle agglomeration, etc.) also plays an important role in the in vivo drug release and absorption (Zuidema et al. 1994). Since all the above processes can directly or indirectly be influenced by the acute inflammatory components, as they modulate the inflammatory cascade, it is important to consider early time points (e.g., 24 and 48 hr) for the examination of the LAI nano-/microsuspension injection sites and adapt the study design to the expected duration of the host–formulation interactions.
The inclusion of acute time points in this study additionally provided the necessary temporal resolution for the modeling of the depot cellularization based on quantitative measurements. A simple image analysis procedure using standard H&E slides was proposed to quantify the depot geometries and dimensions. Fitting the 3-parameter Weibull model to the derived data for the fraction of the formulation that had been infiltrated by cells enabled statistical comparison between PP-LAI and PS. The significantly lower scale factor (α) for PS compared to PP-LAI reflected the slightly faster and deeper infiltration of the PS depots. This was presumably facilitated by the monodispersity and spherical shape of the PS microspheres, and hence the larger interparticle spaces, as opposed to the PP-LAI nano-/microcrystals that formed an agglomerate with limited porosity (Yamaguchi and Anderson 1993). The other quantitative descriptors did not differ significantly, and the results were in line with the qualitative and semiquantitative histopathological findings. The data indicated the appropriateness of the applied methodology. Nevertheless, the suitability of unmodified PS nano-/microspheres as a model for LAI drug nano-/microcrystals is difficult to establish based on this sole report.
The depot volumes at 4 hr after IM injection of PP-LAI or PS were comparable to the volume of solid that had been administered. This showed an almost total and immediate effusion and/or absorption of the aqueous vehicle after IM injection of both test articles. The only slight increase in depot dimensions seen during the first 48 hr, suggested a minimal dilution of the formulation by edematous fluid. Moreover, the preservation of the initial depot geometries and well-defined boundaries over time demonstrated that the observed size increase was not a consequence of the (mechanical or convectional) spreading of the particulate formulation. The negligible spreading of the formulation was most likely a consequence of the rapid vehicle disappearance and the size-exclusion properties of the ground substance (i.e., fibrous network of collagen and immobilized macromolecules; Levick 1987; Hawley, Davis, and Illum 1995). The knowledge of the limited spreadability and the temporal evolution of the depot dimensions is useful, since the formulation spreading has been shown to influence the drug absorption rate after IM injection (Bjerregaard et al. 2001). The gradual depot expansion until day 7 and 3 after PP-LAI and PS injection, respectively, was therefore caused by the cellular infiltration and the resulting increased depot porosity. The extensive granulation tissue and deep infiltration indicate the relatively loose structure of the particle aggregates. The gradually decreasing PP-LAI depot dimensions from 7 days onward was attributed to the slow resorption (i.e., dissolution) of PP-LAI particles, since the fraction of the PP-LAI dose retrieved in the draining lymph nodes was minor.
Remarkably, the evolution of the infiltrated depot volume (Vinfiltr. ) qualitatively resembled the shape of the PAL plasma concentration–time profiles that were seen after PP-LAI injection in the rat (Darville et al. 2014). Since the granulation tissue mainly consisted of macrophages loaded with PP-LAI nano-/microcrystals, it is possible that the macrophage infiltration and subsequent phagocytosis are determinant factors for the PAL (i.e., the active moiety of PP) absorption. This could be explained by phagocytosis-related differences in PP dissolution or hydrolysis rate. Indeed, IM PP shows flip-flop pharmacokinetics (i.e., PAL absorption rate constant ka < elimination rate constant k), whereby the apparent half-life reflects the slow dissolution rate-limited absorption (Samtani, Vermeulen, and Stuyckens 2009). Hence, the terminal (>14 days) rate of decrease in the (infiltrated) depot volume may provide an estimation of the PP dissolution and PAL absorption rate. Although this was not investigated in this study, and the rate-limiting steps in the multiphasic pharmacokinetics in animals and humans remain to be identified, these findings are in line with our previous report. Also, the outcome of this work could serve as a basis for future in silico model-based explorations by providing physiological data on the time course of the inflammatory response to a reference LAI suspension.
In summary, this study presents a detailed chronological characterization of the nature and dynamics of the host responses elicited by the IM injection of a clinically relevant aqueous LAI PP nano-/microsuspension and an analog PS microsphere model suspension in the rat. Standard histopathology, semiquantitative assessment of critical inflammation/healing parameters, and the evaluation of proinflammatory cytokine concentrations in local inflammatory exudates were combined in an integrated approach. The ISR to both suspensions were moderate to marked but remained necrosis free and localized. Early time points (4, 8, 24, and 48 hr) were included, since several events that direct the progression of the tissue reaction and potentially influence the drug absorption rate in vivo occurred within this time frame. These events include the edema formation and vehicle effusion (i.e., influencing the degree of agglomeration and, hence, potentially the (pro)drug dissolution and absorption rate) and the recruitment of phagocytic cells with the surrounding of the formulation depot (i.e., influencing the effective dissolution surface area, prodrug hydrolysis rate and possibly the passive drug absorption rate; Darville et al. 2014). The acute inflammation with IL-1/TNF-α-mediated recruitment and activation of myeloid cells was followed by elevated VEGF concentrations and the formation of granulation tissue. This led to an increase in multiple cytokines/chemokines and resulted in a chronic active inflammation that was dominated by proinflammatory macrophages and was accompanied by T-cell recruitment at later stages. Contrary to foreign body reactions observed after SC implantation of many biodegradable biomaterials, no MNGCs and very little fibrosis were observed in this study throughout the observation period of 4 weeks. Lymphatic uptake and lymph node retention of PP-LAI nano-/microparticles were observed, but the net contribution to the previously reported PAL systemic exposure was deemed negligible. The overall nature of the inflammatory response was similar to that previously observed following SC injection of LAI microsuspensions of 2 other drugs from the same class, but relevant differences in the dynamics and histology were reported here. However, direct comparison was hindered by differences in administration route, injection volumes, and drug particle sizes. A simple image analysis procedure was proposed for the accurate and sensitive evaluation of the formulation depot geometry, cell infiltration, and vascularization. The empirical modeling of the quantitative depot cellularization data enabled the statistical comparison between PP-LAI and PS. In this study, the reactions to both test articles were surprisingly similar, although slightly faster infiltration kinetics were observed with PS.
LAI nano-/microsuspensions of poorly water-soluble drugs represent a relatively recent formulation strategy and the current availability of commercial formulation and production platforms is facilitating the market entry of several other LAIs in the future. Hence, it is imperative to elucidate the nature and dynamics of the host response to this class of formulations. Only a few reports on the local host response to these emerging formulations have been published to date. As such, this work might provide a framework for further research and serve as reference for formulations to come. Future mechanistic in vivo studies, supported by in silico simulations are necessary to elucidate the impact of the complex tissue dynamics on the formulation behavior and drug release/absorption and vice versa.
Supplemental Material
Supplemental Material, DS1_TPX_10.1177_0192623315618291 - Modeling the Time Course of the Tissue Responses to Intramuscular Long-acting Paliperidone Palmitate Nano-/Microcrystals and Polystyrene Microspheres in the Rat
Supplemental Material, DS1_TPX_10.1177_0192623315618291 for Modeling the Time Course of the Tissue Responses to Intramuscular Long-acting Paliperidone Palmitate Nano-/Microcrystals and Polystyrene Microspheres in the Rat by Nicolas Darville, Marjolein van Heerden, Tim Erkens, Sandra De Jonghe, An Vynckier, Marc De Meulder, An Vermeulen, Patrick Sterkens, Pieter Annaert and Guy Van den Mooter in Toxicologic Pathology
Footnotes
Acknowledgments
The authors wish to thank the necropsy and histology team in Beerse, in particular Kristel Buyens and Loes Versmissen for all the histological/immunohistochemical stains and Ann Kegels to run the multiplex cytokine assay.
Author Contributions
Authors contributed to conception or design (ND, MV, AVe, PS, PA, GV); data acquisition, analysis, or interpretation (ND, MV, TE, SD, AVy, MD); drafting the manuscript (ND, MV, TE, SD, AVy, MD, AVe, PS, PA, GV); and critically revising the manuscript (SD, PA). All authors gave final approval, and agreed to be accountable for all aspects of work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Both ND and MvH contributed equally to this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. Financial support was provided by the Agency for Innovation by Science and Technology in Flanders, Belgium (IWT Vlaanderen, Grant No. 100682).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.