
Abstract
Recombinant interleukin-2 (rIL-2) administration in oncology indications is hampered by vascular toxicity, which presents as a vascular leak syndrome. We used this aspect of the toxicity of rIL-2 to evaluate candidate biomarkers of drug-induced vascular injury (DIVI) in rats given 0.36 mg/kg rIL-2 daily. Groups of rats were given either 2 or 5 doses of rIL-2 or 5 doses of rIL-2 followed by a 7-day recovery. The histomorphologic lexicon and grading scheme developed by the Vascular Injury Working Group of the Predictive Safety Testing Consortium of the Critical Path Institute were utilized to enable semiquantitative integration with circulating biomarker levels. The administration of rIL-2 was associated with time-dependent endothelial cell hyperplasia and hypertrophy and perivascular inflammation that correlated with increases in circulating angiopoietin-2, lipocalin-2, monocyte chemotactic protein-1, tissue inhibitor of metalloproteinase-1, vascular endothelial growth factor A, E-selectin, and chemokine (C-X-C motif) ligand-1, and the microRNAs miR-21, miR-132, and miR-155. The dose groups were differentially identified by panels comprising novel candidate biomarkers and traditional hematologic parameters. These results identify biomarkers of the early stages of DIVI prior to the onset of vascular smooth muscle necrosis.
Introduction
Drug-induced vascular injury (DIVI) hampers drug development due to the lack of reliable noninvasive biomarkers that can be monitored in nonclinical animal studies or human clinical trials. Also, clinical drug–induced vasculitis (CDIV) may occur with drugs that did not demonstrate DIVI in nonclinical studies (Kerns et al. 2005). As a result, drug candidates may progress into the clinic before the vascular risks are appreciated, or alternatively, DIVI in animal studies may impede the further development of a compound that is actually safe and efficacious in humans.
The discovery and characterization of circulating biomarkers that are differentially diagnostic for DIVI in animal studies and predictive of translational risk are needed to monitor CDIV in clinical trials. Despite different inciting causes and outcomes, vasculitides share multiple common features, including activation and damage to endothelial cells (ECs) and inflammation. Thus, the Vascular Injury Working Group (VIWG) of the Predictive Safety Testing Consortium of the Critical Path Institute (PSTC) is assessing candidate biomarkers of DIVI in research animals (Mikaelian et al. 2014), while the “Safer and Faster Evidence–based Translation” program of the innovative medicine initiative is doing the same in humans (Bendjama et al. 2014; Bendjama et al. 2013).
Interleukin-2 (IL-2) is a cytokine central to the proliferation and function of T cells and natural killer (NK) cells. Recombinant IL-2 (rIL-2) administration for the treatment of malignancies results in a dose-limiting vascular leak syndrome at subtherapeutic doses (Anderson et al. 1993). Vascular leak syndrome is characterized by an increase in vascular permeability leading to fluid and protein extravasation, hypoalbuminemia, and interstitial edema and may progress to organ failure. This vascular toxicity may be related to the direct toxicity of rIL-2 to ECs (Baluna et al. 1999) or may be the result of the trafficking and activation of inflammatory cells. The toxicity of rIL-2 is recapitulated in animals where it is characterized by massive multi-tissue perivascular infiltration by lymphocytes, eosinophils, macrophages and NK cells, and EC hypertrophy/hyperplasia (H/H). Here, we evaluated the blood circulating profile of a panel of potential biomarkers in the rIL-2 rat model of vascular injury. Most of the candidate biomarkers evaluated were chosen based on the efforts of the VIWG of PSTC (Thomas et al. 2012; Mikaelian et al. 2014), including angiopoietin-2, E-selectin, chemokine (C-X-C motif) ligand-1, lipocalin-2, monocyte chemotactic protein-1, tissue inhibitor of metalloproteinase-1, vascular endothelial growth factor A, α-1-acid glycoprotein (orosomucoid), endothelin-1, total nitrite, and thrombospondin-1. A set of plasma microRNA (miRNAs) was selected based upon the literature of the most frequently dysregulated miRNAs in DIVI and CDIV (Thomas et al. 2012; Carlsen et al. 2013; Kurz et al. 2013; Shimizu et al. 2013). These miRNAs were miR-10a, miR-21, miR-126, miR-132, miR-134, miR-145, miR-155, miR-223, miR-379, miR-409-3p, and miR-511.
Materials and Methods
Animals
Male Han Wistar rats (Crl:Wi[Han]) aged 8 weeks were purchased from Charles River Laboratories (Raleigh, NC) and were acclimated 2 weeks before dosing. Animals were randomized by weight and assigned to either vehicle or rIL-2 (Proleukin®; Sigma-Aldrich, St. Louis, MO) groups and single housed in polycarbonate solid-bottom cages. Upon study initiation, the rats were 305 ± 13 g (mean ± standard deviation). Animal identification and conditions of housing, acclimatization, environment, diet, and water were in accordance with facility standard operating procedures. All animal procedures were conducted in an Association for Assessment and Accreditation of Laboratory Animal Care accredited facility under an Institutional Animal Care and Use Committee approval protocol.
Treatment and Sampling
Rats were subcutaneously administered 0.36 mg/kg rIL-2 q.d. in sterile water (n = 6 rats/group/time point, 3 time points; Proleukin, Novartis, Dorval, Quebec, Canada) or sterile water alone (n = 12, 4 rats/group/time point) as vehicle control. Necropsies were carried out 3 hr post-dose after 2 or 5 doses, with a recovery group necropsied 7 days after 5 days of dosing with either rIL-2 or the vehicle. At necropsy, the rats were anesthetized with isoflurane/O2 anesthesia; blood was collected from the abdominal aorta for clinical chemistry (serum), coagulation (sodium citrate), hematology (ethylenediaminetetraacetic acid [EDTA]), and miRNA (EDTA) evaluations.
Clinical Pathology
Standard hematology and clinical chemistry panels were evaluated at all time points using the Abbott Cell-Dyn 3500 (Abbott Park, IL) and the Roche/Hitachi Modular Analytics system (Roche Diagnostics, Indianapolis, IN), respectively. The measured clinical chemistry parameters were alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, γ-glutamyl transpeptidase, bilirubin, blood urea nitrogen, plasma creatinine, glucose, cholesterol, triglycerides, total proteins, albumin, globulin, albumin–globulin ratio, calcium, phosphorus, sodium, potassium, chloride, and glutamate dehydrogenase. Coagulation and hematology parameters were prothrombin time, activated partial thromboplastin time, fibrinogen concentration, mean corpuscular volume, mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration, red blood cell distribution, percentage reticulocytes, total white blood cell and platelet counts, and absolute counts of reticulocytes, neutrophils, lymphocytes, monocytes, eosinophils, and basophils.
Novel candidate DIVI biomarkers (angiopoietin-2, E-selectin, chemokine [C-X-C motif] ligand-1, lipocalin-2, monocyte chemotactic protein-1, tissue inhibitor of metalloproteinase-1, vascular endothelial growth factor A, α-1-acid glycoprotein [orosomucoid], endothelin-1, total nitrite, and thrombospondin-1) were measured using previously described methods (Mikaelian et al. 2014). The novel candidate biomarker data of 1 rat in the recovery group were excluded from the analysis because they did not fall in the range for the measured analytes, thereby suggesting sample degradation.
miRNAs real-time polymerase chain reaction
Total RNA was extracted from 200 μl plasma using the miRNeasy kit (Qiagen, Valencia, CA) according to the manufacturer’s instructions. The samples were reverse transcribed using the TaqMan MicroRNA Reverse Transcription kit (Applied Biosystems, Carlsbad, CA) and miRNA-specific primers provided by the manufacturer; qPCR amplification was performed using TaqMan miRNA-specific assays (Applied Biosystems) in a 7900HT Thermocycler (Applied Biosystems). The SDS 2.4.1 files were loaded into the RQ Manager software and the raw C t values were calculated using automatic baseline and threshold values. miRNAs with C t values above 35 were considered not expressed. Fold changes in miRNA expression were calculated according to the ΔΔC t -method, using spiked-in ath-miR-159, and endogenous miR-16 and U6snRNA for normalization (Livak and Schmittgen 2001).
Histology
Tissues for histomorphologic evaluation were selected based on the list established by the VIWG of PSTC extended to a few additional tissues based on in-house experience with the toxicity of rIL-2. These tissues were the eyes, heart, injection site, kidneys, liver, lung, mesentery, pancreas, skeletal muscles, spleen, ureters, urinary bladder, epididymis, and testis (including the pampiniform plexus). The tissues were fixed in 10% neutral-buffered formalin for 24 hr and subsequently processed, embedded in paraffin, sectioned at 4 μm, mounted on glass slides, deparaffinized, and stained with hematoxylin and eosin. Assessment and grading for endothelial, medial, and adventitial changes were defined by the VIWG lexicon of PSTC (Mikaelian et al. 2014); the grades were 0 = normal, 1 = minimal, 2 = mild, 3 = moderate, and 4 = marked/severe for each tissue/organ. The findings graded in this study consisted of endothelial H/H and perivascular inflammation; a cumulative score was derived consisting of the sum of the scores of each finding for all 14 tissues/organs. The rationale for using a cumulative score was that the administration of rIL-2 causes systemic vascular injury, which would best be captured as a disease process by adding up the histologic score of all available tissues.
Immunohistochemistry (IHC)
Anti-rat smooth muscle actin antibody (clone 1A4, 1:100 dilution) and anti-CD31 antibody (clone JC70A, 1:200 dilution), as well as antibody diluent, were from DAKO Corporation (Carpinteria, CA). All buffers, reagents, and autostainers were from Ventana Medical Systems (Roche Diagnostics, Tucson, AZ; Supplemental Material 1). IHC was performed on all rats. CD31 was assessed in the liver, lungs, and spleen, and smooth muscle actin was assessed in the liver and the spleen. CD31 immunolabeling was graded as follows: rats given the vehicle were given grade 0, which corresponded to moderate immunolabeling essentially restricted to the ECs of the portal vessels, with occasional weak immunolabeling of a few sinusoidal ECs. Grade 1 corresponded to stronger immunolabeling of the ECs of the portal vessels, with a small to moderate number of moderately labeled ECs in the sinusoids. Grade 2 corresponded to extension of the immunolabeling to the ECs of the centrilobular vein, an increase in the number of CD31-immunolabeled sinusoidal ECs, including around the centrilobular vein and the presence of CD31+ neocapillaries in the portal spaces.
In Situ Hybridization (ISH)
The ISH procedure followed previously described methods (Jorgensen et al. 2010; Supplemental Material 1) with anti-digoxin rabbit antiserum from Sigma-Aldrich and was performed on the Discovery Ultra Ventana™ autostainer (Roche Diagnostics, Tucson, AZ). ISH was performed on all rats given rIL-2 and in 4 rats given the vehicle. miR-126 levels were assessed in the liver, lung, mesentery, pampiniform plexus, and spleen and were semiquantitatively graded in all tissues as normal with moderate and well-defined labeling (grade 0), slightly increased labeling (grade 1), or decreased labeling (grades −1, −2, or −3), with a −3 grade indicating almost complete loss of miR-126 tissue expression.
Statistical Analysis
For continuous variables, Kruskall–Wallis with Dunn’s posttest (GraphPad Prism® 5.04 2010; GraphPad Software, San Diego, CA) was used to compare the differences between treatment groups. TIBCO Spotfire® 3.3.1 (2011; TIBCO Spotfire, Boston, MA) was used to determine the correlation between histomorphologic endpoints and candidate biomarkers. Multiple regression with stepwise selection (R 3.1.1 2014; R Foundation for Statistical Computing, Vienna, Austria) was used to identify the best combination of biomarkers to produce scores that correlate with the histomorphologic endpoints, and the combinations of biomarkers that best differentiate the 4 treatment groups (Venables and Ripley 2002). This combination of biomarkers was obtained by the stepwise linear regression method where biomarkers were selected based on their correlation to the histopathologic score and added into the composite score one by one until there was no substantial improvement in the correlation between the composite score and the total histologic score.
Results
Histologic Evaluation
The administration of rIL-2 was associated with time-dependent changes that included minimal to mild EC H/H and perivascular inflammation that were most prominent after 5 doses of rIL-2, with partial recovery after 7 days (Figure 1 and Table 1); the inflammation was comprised predominantly of mononuclear cells and eosinophils and was accompanied by perivascular edema. These changes are consistent with the vascular injury typically reported for rIL-2 (Anderson et al. 1993; Wolfgang, McCabe, and Johnson 1998). Other changes included minimal to mild myocardial necrosis and macrophage infiltration of the spleen (not shown).
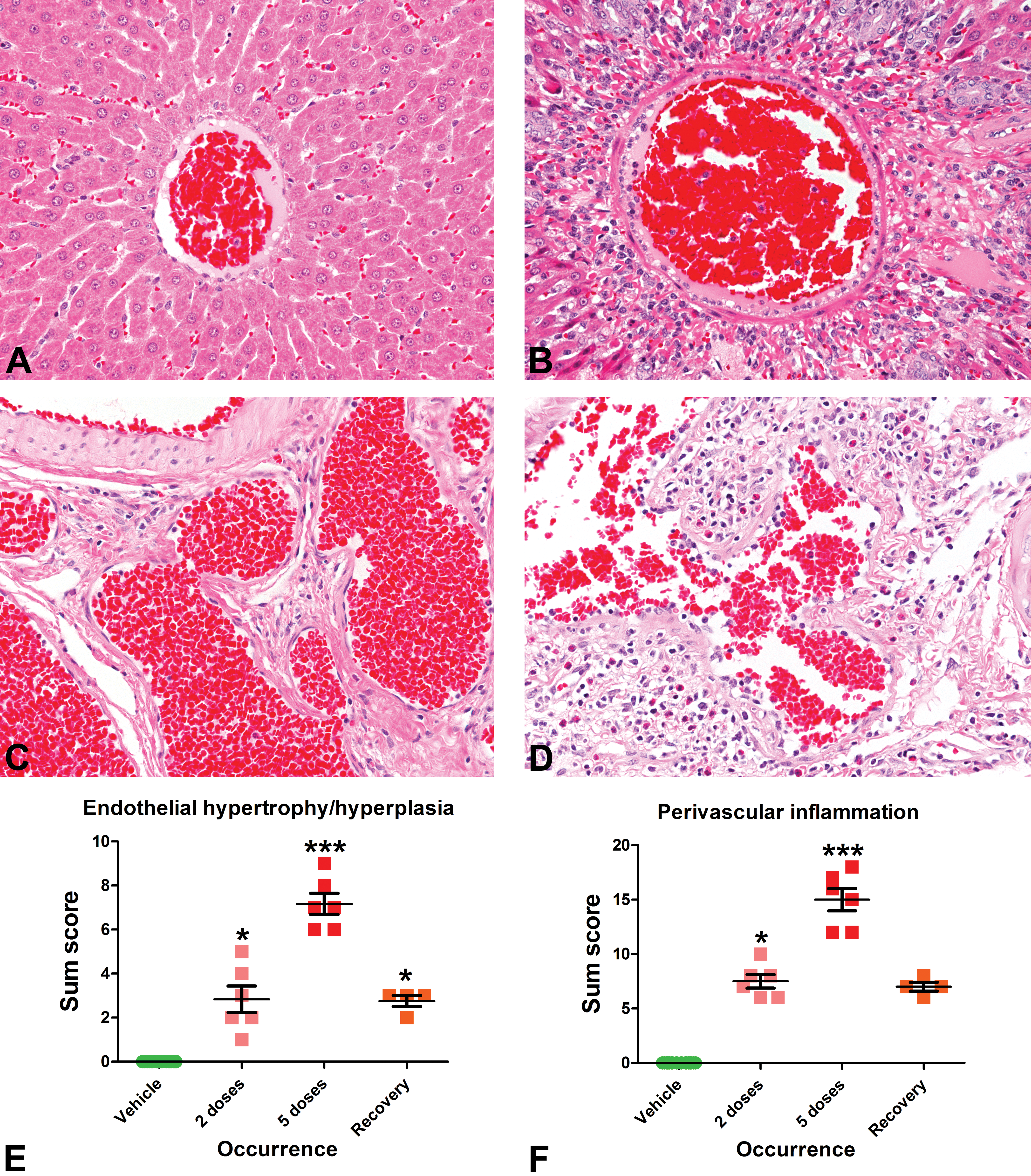
The administration of recombinant interleukin-2 (rIL-2) was associated with time-dependent histologic vascular changes, which were most prominent in the liver (A, B) and in the pampiniform plexus (C, D). These changes, compared to vehicle-dosed rats (A, C), included minimal to mild endothelial hypertrophy/hyperplasia (H/H) and perivascular inflammation, which were maximal after 5 doses (B, D–F). Endothelial H/H (E) and perivascular inflammation (F) captured as a sum score in the organs examined were present after 2 doses of rIL-2, progressed after 5 doses of rIL-2, and had a trend toward recovery after 7 days. Kruskall–Wallis with Dunn’s post-test, *p < .05; ***p < .001.
Temporal changes in histomorphologic endpoints, clinical pathology, candidate biomarkers, and plasma miRNAs in rats administered 2 or 5 doses of recombinant interleukin-2 with a 7-day recovery period.
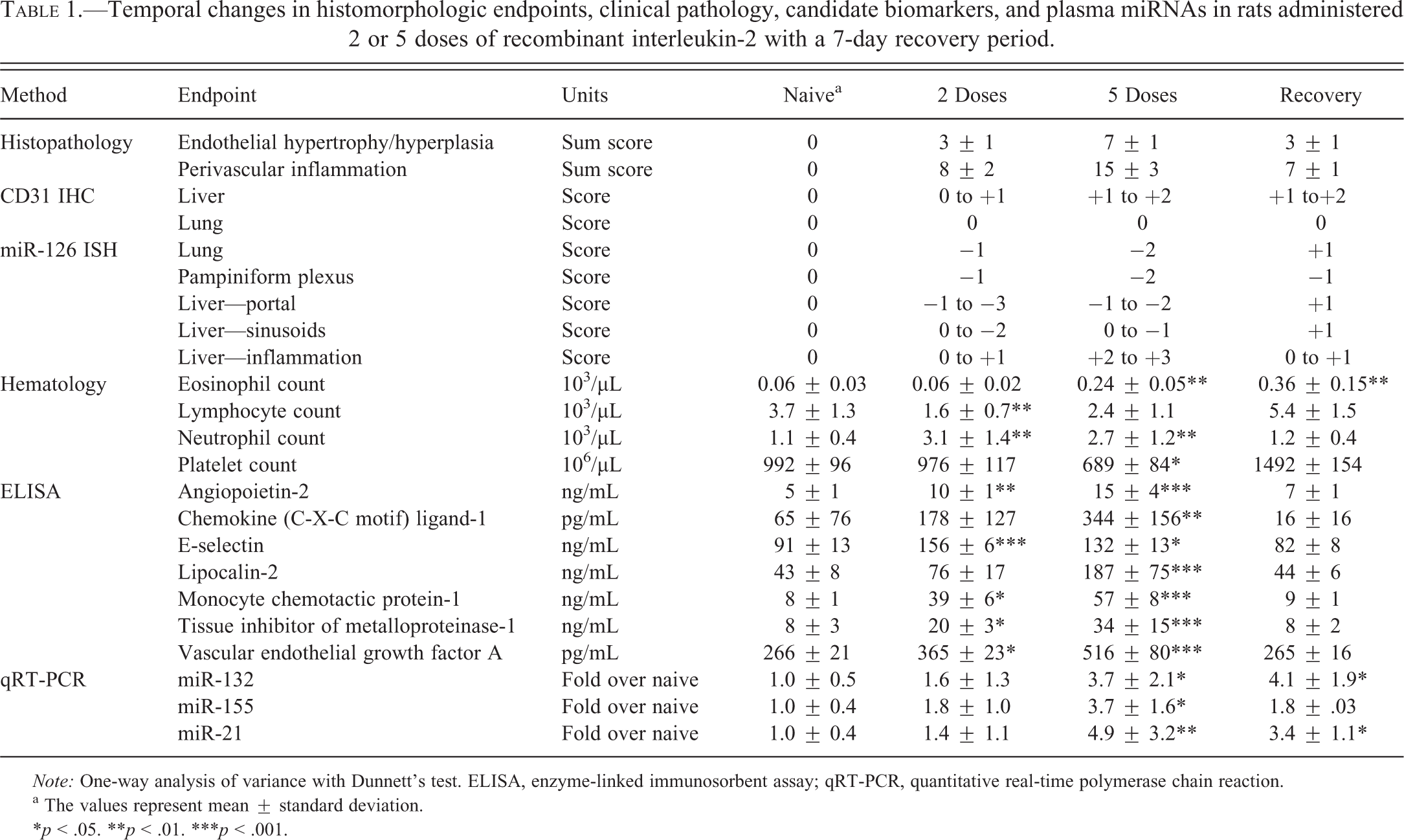
Note: One-way analysis of variance with Dunnett’s test. ELISA, enzyme-linked immunosorbent assay; qRT-PCR, quantitative real-time polymerase chain reaction.
a The values represent mean ± standard deviation.
*p < .05. **p < .01. ***p < .001.
IHC
Immunolabeling for CD31 showed time-dependent increases (Figure 2) in the ECs of the larger vessels (arteries and veins of the portal spaces, centrilobular veins) with minimal increases after 2 doses and mild increases after 5 doses. Concurrently, there was de novo CD31 expression in ECs lining the hepatic sinusoids. The expression of CD31 in the liver had not returned to baseline levels at the recovery time point (Table 1). The expression of CD31 remained unchanged across the study in the lungs and spleen, indicating a different response to rIL-2 of the ECs of the liver compared to the ECs of the lung and the spleen. There were no changes in smooth muscle actin immunolabeling, which confirmed the absence of vascular smooth muscle cell (VSMC) necrosis.
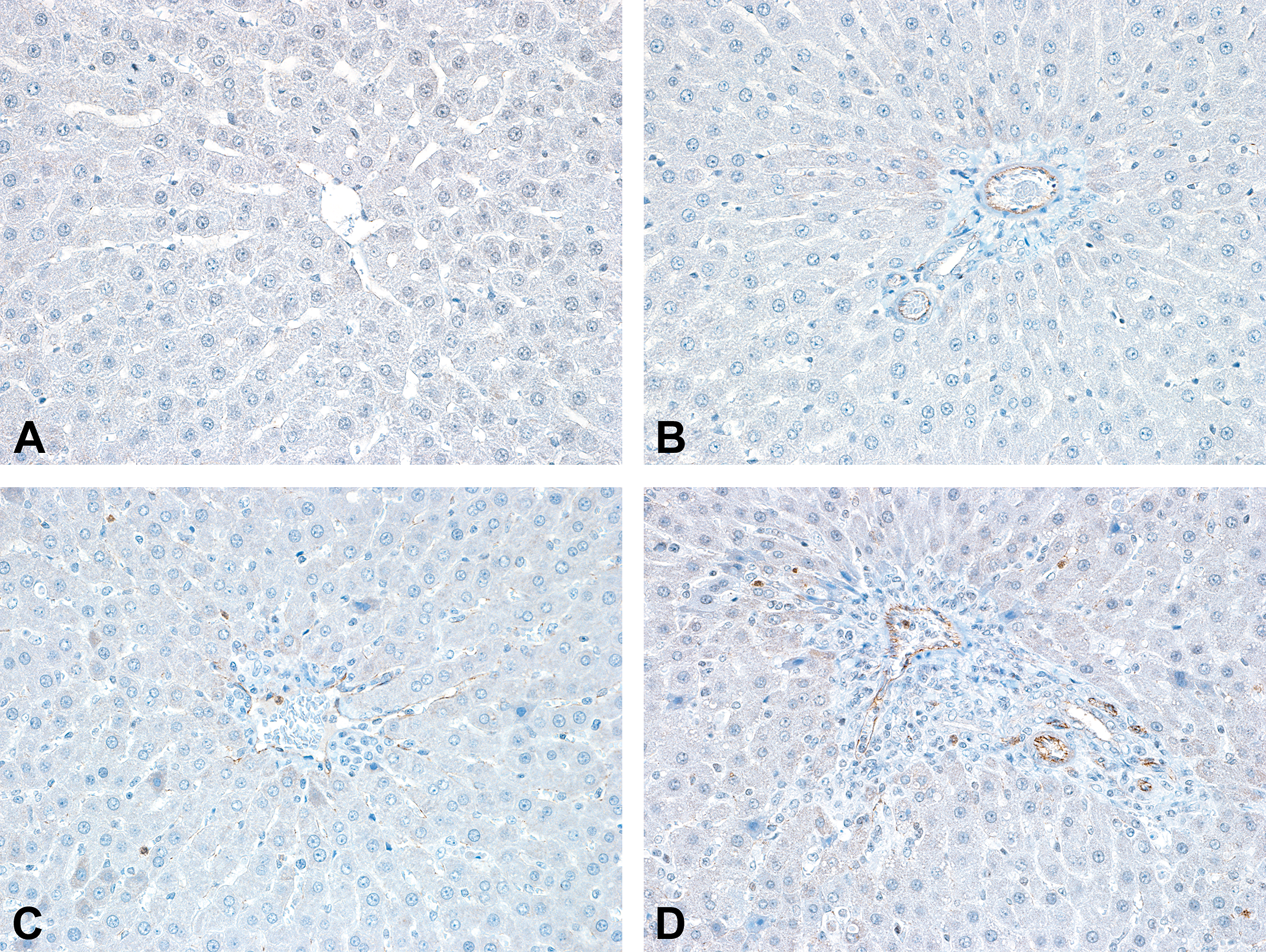
Compared to the rats administered the vehicle (A, B), the expression of CD31 was increased in the portal vessels and in the sinusoids of the liver in rats administered 5 doses of recombinant interleukin-2, especially in the portal arteries (D), and also in the centrilobular veins (C).
ISH
The expression of miR-126 in rats administered the vehicle was restricted to the vascular ECs (arteries, veins, and lymphatics). At a cellular level, miR-126 expression was predominantly nuclear with weaker cytoplasmic expression in ECs from rats administered the vehicle. The administration of rIL-2 resulted in time-dependent decreases in the expression of miR-126 in the liver (Figure 3), the pampiniform plexus, and the lungs (Supplemental Figure S2) but not in the spleen, the mesenteric lymph nodes, or arteries, indicating a different response of ECs to rIL-2 depending on the organ. During the dosing phase, miR-126 expression shifted from a predominantly strong nuclear pattern to a weaker and predominantly cytoplasmic pattern. At recovery, the nuclear labeling was regained and was stronger than in rats administered the vehicle.
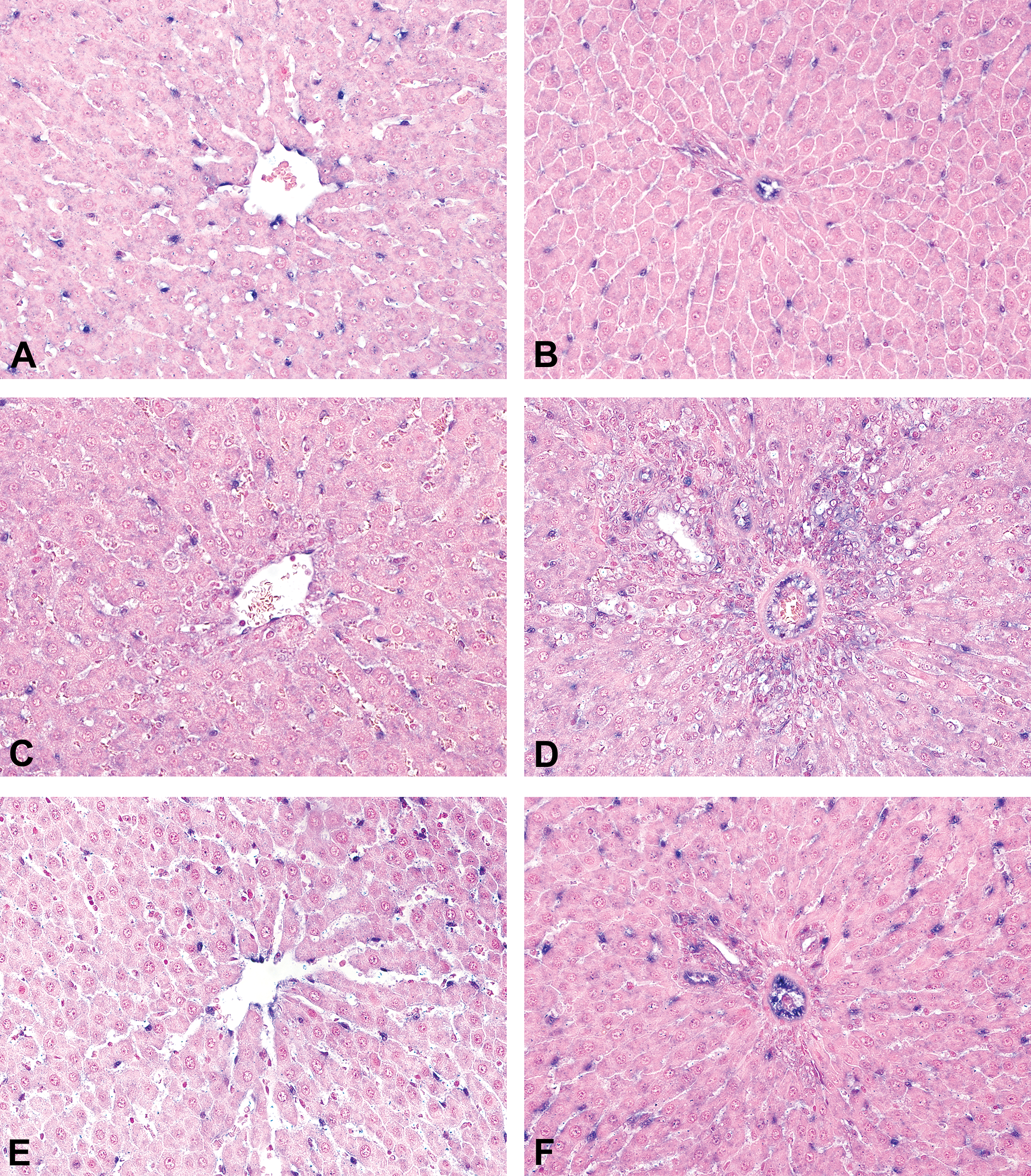
Compared to the rats administered the vehicle (A, B), the expression and/or intensity of miR-126 in the liver decreased after 5 doses of recombinant interleukin-2 in the centrilobular (C) and portal areas (D), with a concurrent weak diffuse hybridization for miR-126 in the inflammatory infiltrates of the portal spaces (D). At recovery, the level of expression of miR-126 in the endothelial cells (ECs) was similar to that of the controls in the sinusoidal and centrilobular vein ECs (E). However, compared to the vehicle-dosed rats, the expression of miR-126 was higher at the recovery time point in ECs of the portal areas (F).
In the liver, after a gradual decrease in all vessels during the dosing phase of the study (Figure 3C and D), the expression of miR-126 returned to the baseline or slightly above the baseline at recovery in the sinusoids and centrilobular veins and was higher than at baseline in the portal vessels (Figure 3E and F). Concurrent to the decrease of miR-126 expression in ECs during the dosing phase, perivascular inflammatory infiltrates became weakly positive for miR-126 (Figure 3D).
In the lungs, the changes in miR-126 expression were most prominent in the respiratory capillaries and in the midsized/small parenchymal pulmonary arteries (Supplemental Figure S2). In these vessels, miR-126 expression decreased during the dosing phase of the study and was increased compared to vehicle-dosed rats at recovery. In the pampiniform plexus, miR-126 expression decreased in vessels of all size during the dosing phase and at recovery was still lower compared to baseline (not shown).
Clinical Pathology
Clinical chemistry findings associated with the administration of rIL-2 were time dependent and consisted of reversible increases in the activity of alanine aminotransferase, aspartate aminotransferase, γ-glutamyl transpeptidase, and glutamate dehydrogenase, along with a decrease in the concentration of albumin. These findings replicate earlier reports from our laboratory and were attributed to liver injury and to the vascular leak syndrome (Table 1, Supplemental Figure S1; Hack et al. 1991; Anderson et al. 1993; Wolfgang, McCabe, and Johnson 1998). The hematology findings were consistent with the reported pharmacologic effects of rIL-2 and consisted of decreases in lymphocyte and platelet counts and increases in eosinophil and neutrophil counts; most of these findings had normalized after a 7-day recovery period except for the eosinophil count.
Novel Candidate Biomarkers
There were time-dependent increases in the serum concentrations of angiopoietin-2, chemokine (C-X-C motif) ligand-1, lipocalin-2, monocyte chemotactic protein-1, E-selectin, tissue inhibitor of metalloproteinase-1, and vascular endothelial growth factor A (Table 1, Supplemental Figure S1). All these candidate biomarkers peaked after 5 doses, except for E-selectin which peaked after 2 doses. All candidate biomarkers had returned to baseline values at the recovery time point.
Circulating miRNAs
There were time-dependent increases in the plasma concentrations of miR-21, miR-132, and miR-155; of note, miR-21 and miR132 remained elevated at the recovery time point (Table 1, Supplemental Figure S1). The increased plasma miR-126 and miR-145 were not statistically significant, although the expression of tissue miR-126 changed over time as assessed by ISH (see above).
Correlations between Histomorphology and the Candidate Biomarkers
Correlations between the histomorphologic endpoints and the candidate biomarkers were made during the induction of the disease (after 2 or 5 doses); the data from the recovery group were excluded from the correlation analysis because this time point corresponds to a resolution stage of vascular injury rather than an ongoing DIVI.
There were strong positive correlation scores (Spearman’s ρ in the 0.8–0.9 range) between multiple candidate biomarkers and EC H/H and perivascular inflammation after 2 or 5 doses of rIL-2 (data not shown). The highest correlations were obtained for tissue inhibitor of metalloproteinase-1, monocyte chemotactic protein-1, vascular endothelial growth factor A, angiopoietin-2, and lipocalin-2. Pairs of biomarkers, which also included traditional hematology markers, achieved higher correlations than individual biomarkers. In particular, the composite score for the biomarker pair monocyte chemotactic protein-1/eosinophil count was strongly positively correlated with endothelial H/H and perivascular inflammation (Figure 4), and multiple biomarker pairs adequately differentiated the 4 treatment groups in this study (Figure 5).
The composite score for the biomarker pair monocyte chemotactic protein-1 (MCP1)/eosinophil count (AEOS) was strongly positively correlated with endothelial hypertrophy/hyperplasia (A) and perivascular inflammation (B). The histomorphologic scores are cumulative scores consisting of the sum of the scores of each finding for all 14 tissues/organs. The stepwise linear regression method was used to create a composite biomarker score for the pair of MCP1 and AEOS, specifically the composite score = 1.85 log(MCP1) + 10.8 log(AEOS) – 2.3.
Pairs of circulating markers identified the 4 dose groups in rats administered the vehicle or recombinant interleukin-2 as 2 doses, 5 doses, or 5 doses + 7-day recovery. These pairs were monocyte chemotactic protein-1 (MCP1) and the platelet count (PLAT), vascular endothelial growth factor A (VEGF) and PLAT, MCP1 and hemoglobin concentration (HGB), and VEGF and α-1-acid glycoprotein-1 (AGPa1, orosomucoid).
Discussion
Using the rIL-2 rat model of DIVI, here we demonstrate that multiple novel candidate biomarkers correlate with endothelial H/H and perivascular inflammation. Also, pairs of circulating markers identified the dose group, which bodes well for the ability to differentiate both ongoing and resolving DIVI in the rat. The validation of these candidate biomarkers is a work in progress through the efforts of the VIWG of PSTC and requires the assessment of animal models with multiple mechanisms of DIVI and of models of tissue-specific toxicity with no or with minimal vascular involvement. This study supports (1) the further investigation of angiopoietin-2, chemokine (C-X-C motif) ligand-1, lipocalin-2, monocyte chemotactic protein-1, E-selectin, tissue inhibitor of metalloproteinase-1, and vascular endothelial growth factor A as candidate biomarkers of DIVI; (2) the use of a sum histomorphologic score and of panels of biomarkers to identify and quantify DIVI; and (3) expanding the candidate biomarkers of DIVI to circulating miR-21, miR-132, and miR-155.
Individual Candidate Biomarker Analysis
Most candidate biomarkers showing significant differences between treated and control animals in this study were selected based on the efforts of the VIWG of PSTC with the exception of the eosinophil count, the platelet count, and the miRNAs (Thomas et al. 2012; Mikaelian et al. 2014). Many of the selected candidate biomarkers examined in this study are associated with inflammation, including tissue inhibitor of metalloproteinase-1, monocyte chemotactic protein-1, lipocalin-2, chemokine (C-X-C motif) ligand-1, and E-selectin, while others are associated with endothelial damage or activation, including angiopoietin-2 and vascular endothelial growth factor A. Each of these groups of markers is unlikely to be DIVI specific because inflammation and endothelial response are common consequences of tissue damage. However, if these results are confirmed in subsequent studies, these candidate biomarkers may enable the ranking of compounds with respect to their DIVI toxicity because of the satisfactory correlation between their circulating levels and the histomorphologic endpoints.
The evaluation of the individual biomarkers provides information as to their possible value beyond monitoring rIL-2-mediated vascular injury. For example, circulating E-selectin was higher after 2 doses of rIL-2 than after 5 doses. This observation is consistent with the biology of E-selectin as assessed in vitro, with maximum upregulation in human umbilical vein ECs 6 to 12 hr after activation and return to baseline at 24 hr (Leeuwenberg et al. 1992). Similarly, circulating E-selectin also peaks in patients in acute vasculitis and decreases thereafter (Takeshita et al. 1997). However, circulating E-selectin is decreased in models of DIVI using fenoldopam and CI-1044 in rats (Cameron et al. 2013). These contrasting observations in rats suggest that the direction and magnitude of E-selectin changes may depend on the underlying pathophysiologic mechanisms of DIVI.
There were time-dependent changes in lymphocyte, eosinophil, neutrophil, and platelet counts following rIL-2 administration. These parameters are unlikely candidate biomarkers of DIVI because they are directly related to the mechanistic effects of rIL-2 (Hack et al. 1991; Anderson et al. 1993; Wolfgang, McCabe, and Johnson 1998) and are not observed with compounds causing archetypal DIVI. However, some of these candidates may have value in the context of a fit for purpose validation. In particular, the decrease in platelet count may reflect, in part, endothelial damage and ensuing platelet consumption, and the lymphocyte, eosinophil, and neutrophil counts may be useful in the context of the development of next-generation rIL-2 compounds. Finally, the observed decrease in albumin concentration, which may be the result of vascular leakage, likely was also impacted by the liver toxicity, the acute phase response, and decreased food intake caused by the administration of rIL-2. Therefore, albumin is unlikely to become a biomarker of DIVI.
Correlation of Biomarker Dysregulation and Histomorphometry
A sum histomorphologic score was used to score DIVI severity because the effects of rIL-2 are systemic, and therefore the effects on circulating biomarker levels were anticipated to be the result of the additive changes in each of the affected organs/tissues. Quantification of endothelial damage is difficult because these cells have a small amount of cytoplasm and their expression of terminal differentiation markers depends on the vascular bed and is altered during activation (Pusztaszeri, Seelentag, and Bosman 2006). This study identified differences in the IHC and ISH phenotype of ECs among vascular beds and their sensitivity to rIL-2.
Although single biomarkers in several cases could differentiate between rIL-2-treated animals and controls, several pairs of biomarkers more accurately differentiated between rIL-2 treatment groups. Specifically, the pairs monocyte chemotactic protein-1/platelet count, vascular endothelial growth factor A/platelet count, hemoglobin concentration/monocyte chemotactic protein-1, and vascular endothelial growth factor A/α-1-acid glycoprotein-1 adequately identified the 4 dose groups (2 doses, 5 doses, 5 doses + recovery, and vehicle). Of note, although the platelet count, hemoglobin concentration, and α-1-acid glycoprotein-1 did not directly correlate with the histomorphologic endpoints, they were useful to identify the dose group. This observation argues for expanding the identification of candidate biomarkers of DIVI to clinical pathology endpoints even when they do not individually correlate to the histomorphologic endpoints. Future studies will determine whether these observations are rIL-2 specific or can be expanded to DIVI caused by other mechanisms.
Comparison of Biomarkers in the Rat rIL-2 Model with Human DIVI
In humans, a multivariate analysis was used by Safer and Faster Evidence–based Translation to identify a panel of circulating biomarkers that separates healthy volunteers, patients with acute vasculitis, and patients in remission (Bendjama et al. 2014; Bendjama et al. 2013). The original panel was comprised of 24 circulating proteins (Supplemental Table S1). The current panel, which is in the process of being validated, is comprised of 10 parameters: macrophage inhibitory protein-1, serum amyloid A, tumor necrosis factor receptor superfamily member-1A, tissue inhibitor of metalloproteinase-1, P-selectin, vascular cell adhesion molecule-1, intercellular adhesion molecule-1, thrombomodulin, age, and sex. The absence of a complete overlap between the nonclinical and the clinical panels of vascular injury may represent a hurdle to their acceptance by regulatory authorities and clinicians. However, the Safer and Faster Evidence–based Translation and PSTC panels share similarities when assessed in ingenuity pathway analysis (Supplemental Table S1). These similarities support the translational relevance of this model and indicate that these panels detect similar underlying processes such as inflammation and the fibroblastic response to inflammation that occurs during DIVI. As novel assays become available, the overlap between the clinical and nonclinical biomarkers will likely increase.
miRNAs as Circulating and Tissue Biomarkers
The miRNAs selected here evaluate the processes of inflammation as well as endothelial and vascular smooth muscle differentiation. The 3 circulating miRNAs upregulated in this study, miR-21, miR-132, and miR-155, are generally associated with inflammation but also have roles in angiogenesis (Anand and Cheresh 2011; Urbich, Kuehbacher, and Dimmeler 2008). Importantly, miR-21 and miR-132 were still higher at recovery where they correlated with resolving histomorphologic changes, while all the protein biomarkers had normalized by this point. Therefore, miR-21 and miR-132 may identify resolving vascular injury, a process which was not adequately captured by the protein biomarkers evaluated in this study.
The absence of a robust relationship between plasma and tissue miR-126 is a common occurrence in the assessment of miRNAs as biomarkers (Xu et al. 2014; Waters et al. 2012). The nonsignificant trend toward an increase in miR-126 and miR-145, the archetypal miRNAs of ECs, and VSMCs, respectively, warrants their further evaluation in other models of DIVI. The changes in tissue distribution of miR-126 with disease and recovery support a role of miR-126 in EC maturation (Harris et al. 2008; Wang et al. 2008; van Solingen et al. 2009; Wu, Yang, and Li 2009; Zhang, Kandic, and Kutryk 2011; Asgeirsdottir et al. 2012). As the number of miR-126-positive ECs decreased, weak staining for miR-126 was detected in perivascular cells interpreted as inflammatory cells. The biologic significance of detecting miR-126 in inflammatory cells is not known: it may correspond to de novo expression of miR-126 or to transfer of miR-126 from ECs to inflammatory cells.
Conclusions
The correlation between the sum histomorphologic score and the candidate biomarkers is a first step toward the validation of the lexicon of the VIWG of PSTC and of its candidate biomarkers. Future studies will require the use of compounds that cause VSMC necrosis, which is the archetypal change of nonclinical DIVI, although it is not a central feature of CDIV. All candidate biomarkers had returned to baseline after a 7-day recovery period with the exception of miR-21 and miR-132 that correlated with residual histomorphologic changes. This observation warrants the investigation of miR-21 and miR-132 as indicators of residual vascular injury in the context of normalization of the other candidate biomarkers.
Footnotes
Supplemental Material
Supplemental Material 1. The IHC and ISH procedures were performed on a Ventana platform.
Supplemental Figure S1. Graphical representation of the clinical pathology, novel candidate biomarkers, circulating miRNAs, and histomorphologic endpoints showing time-dependent changes in rats administered rIL-2.
Supplemental Figure S2. Compared to vehicle-dosed rats, miR-126 expression in the lung (a) was decreased after 5 doses of rIL-2 (b) and was increased at recovery (c).
Supplemental Table S1. The candidate biomarkers of DIVI of PSTC and Safer and Faster Evidence–based Translation overlapped, including the pathways they encompassed. The cells highlighted in yellow are shared between the rat panel and the human panel. The comparison was limited to the 10 most significant categories for “ingenuity canonical pathways,” “upstream regulator,” “top diseases and functions,” and “ingenuity toxicity list.”
Authors’ Contribution
Authors contributed to conception or design (NK, BD, DK, MA, and IM); data acquisition, analysis, or interpretation (NK, CB, DK, MA, VH, FH, AR, TM, and IM); and drafting the manuscript (NK, FH, and IM). All authors critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.