
Abstract
We have previously indicated that the ideal animal tumor model should mimic the human disease. This means that the investigator should be able to ascertain the influence of host factors on the initiation of tumorigenesis, mimic the susceptibility of tumor response based on age and reproductive history, and determine the response of the tumors induced to chemotherapy. The utilization of experimental models of mammary carcinogenesis in risk assessment requires that the influence of ovarian, pituitary, and placental hormones, among others, as well as overall reproductive events are taken into consideration, since they are important modifiers of the susceptibility of the organ to neoplastic development. Several species, such as rodents, dogs, cats, and monkeys, have been evaluated for these purposes; however, none of them fulfills all the criteria specified previously. Rodents, however, are the most widely used models; therefore, this work will concentrate on discussing the rat rodent model of mammary carcinogenesis.
General Concepts
Spontaneous mammary tumors are frequently observed in long-term rodent studies. In mice, the development of “spontaneous” mammary tumors is linked to the infection of female mice with either an exogenous mouse mammary tumor virus (MMTV) or a less virulent endogenous provirus and has been discussed in a previous publication (Russo and Russo 1996). In the rat, the majority of spontaneously developed tumors, with the exception of leukemia, are neoplasms of endocrine organs or of organs under endocrine control. Spontaneous mammary tumors develop in females of various strains of rats, such as August, Albany-Hooded, Copenhagen, Fisher, Lewis, Osborne-Mendel, Sprague-Dawley (SD), Wistar, and Wistar/Furth (Russo and Russo 1996). Spontaneous mammary tumors are third in incidence among spontaneous tumors found in the Fisher 344 rat used in the National Cancer Institute/National Toxicology Program (NCI/NTP) carcinogenicity bioassays (Russo and Russo 1996). They are predominantly benign tumors, that is, fibroadenomas (FA), fibromas, and more rarely adenomas. Malignant tumors such as adenocarcinomas are rare, although they are the most frequent tumors induced by chemical carcinogens (Russo and Russo 1996). The development of spontaneous tumors varies as a function of strain, age, and endocrine influences. Hormone withdrawal inhibits tumor development, and hormone supplementation, such as chronic administration of estrogens, increases the incidence of adenocarcinomas, whereas chronic administration of prolactin (PRL) or of growth hormone stimulates benign tumor growth (Russo and Russo 1996). The long latency period for spontaneous tumor development, up to 2 years in susceptible strains to develop a 50 to 70% tumor incidence, limits the usefulness of this model for experimental studies.
Comparative Aspects of Mammary Gland Development in the Human and in the Rat
The mammary gland differs from almost all other organs and glandular elements. During the process of development, they are composed of an immature mammary parenchyma surrounded by mature stromal tissue. In other glands, on the other hand, both parenchyma and stroma develop harmoniously at the same time and in definitive space. In the mammary gland, the glandular parenchyma penetration into the surrounding tissue occurs during the prepubertal period rather slowly. By this time, the tissue surrounding the epithelium is fat, connective tissue, and blood vessels that have become completely mature, whereas the gland itself remains in an embryonal state. It is during pubertal growth in both the rat and the human that the epithelial component begins to be stimulated by hormonal impulses to penetrate into the mature surrounding tissue. The postnatal development of the rat mammary gland has been thoroughly studied in the SD strain of rats (Russo and Russo 1996). However, it is not known whether differences in susceptibility to carcinogenesis exhibited by other strains of rats are related to variations in the pattern of gland development and branching or in relation with variations in the physiology of the animals. In the human female, the developmental pattern of the mammary gland is fragmentary known, and no comparative studies among women of different races, genetic backgrounds, or environments are available (Russo and Russo 1987a; Russo, Tay, and Russo 1982).
There are basic differences between the developmental pattern of the human and rat mammary glands. For example, in the human, the ductal structures grow along connective tissue septa, and rarely do the lobular structures grow into fat tissue. In the rat, instead, there is a constant growth of ductal and lobular structures into the adjacent fat tissue. This difference must be considered when the influence of the parenchyma on the stroma is studied in one species or the other. Another difference that might be of importance is that in the rat there is a gradient in development from the nipple to the distal portion, which is the last to differentiate; in the human, the growth or the development is more labryinthic and a different degree of development in different portions of the breast is observed (Russo and Russo 1987; Russo, Tay, and Russo 1982).
Pathogenesis
Pathogenesis of Rat Mammary Tumors
Mammary gland tumors induced in rats by a single dose of 7,12-dimethylbenz (a) anthracene (DMBA), N-methyl-N-nitrosourea (NMU), or irradiation comprise a spectrum of morphology from benign, typical FAs and adenomas to papillomas with hyperplastic, atypical, and dysplastic epithelium and significant stromal and myoepithelial components, to tumors that are architecturally and cytologically malignant and invade adjacent normal tissue. Metastases from even the most anaplastic tumors are low in frequency less than 10% (van Zwieten 1984). Carcinogenic initiation occurs primarily in the epithelium of terminal end buds (TEBs; Figure 1) while they are developing into alveolar buds (ABs) and terminal ducts (TDs); these structures are considered to be equivalent to the terminal ductal lobular unit (TDLU) described in the human breast (Russo and Russo 1996; Wellings, Jensen, and Marcum 1975).
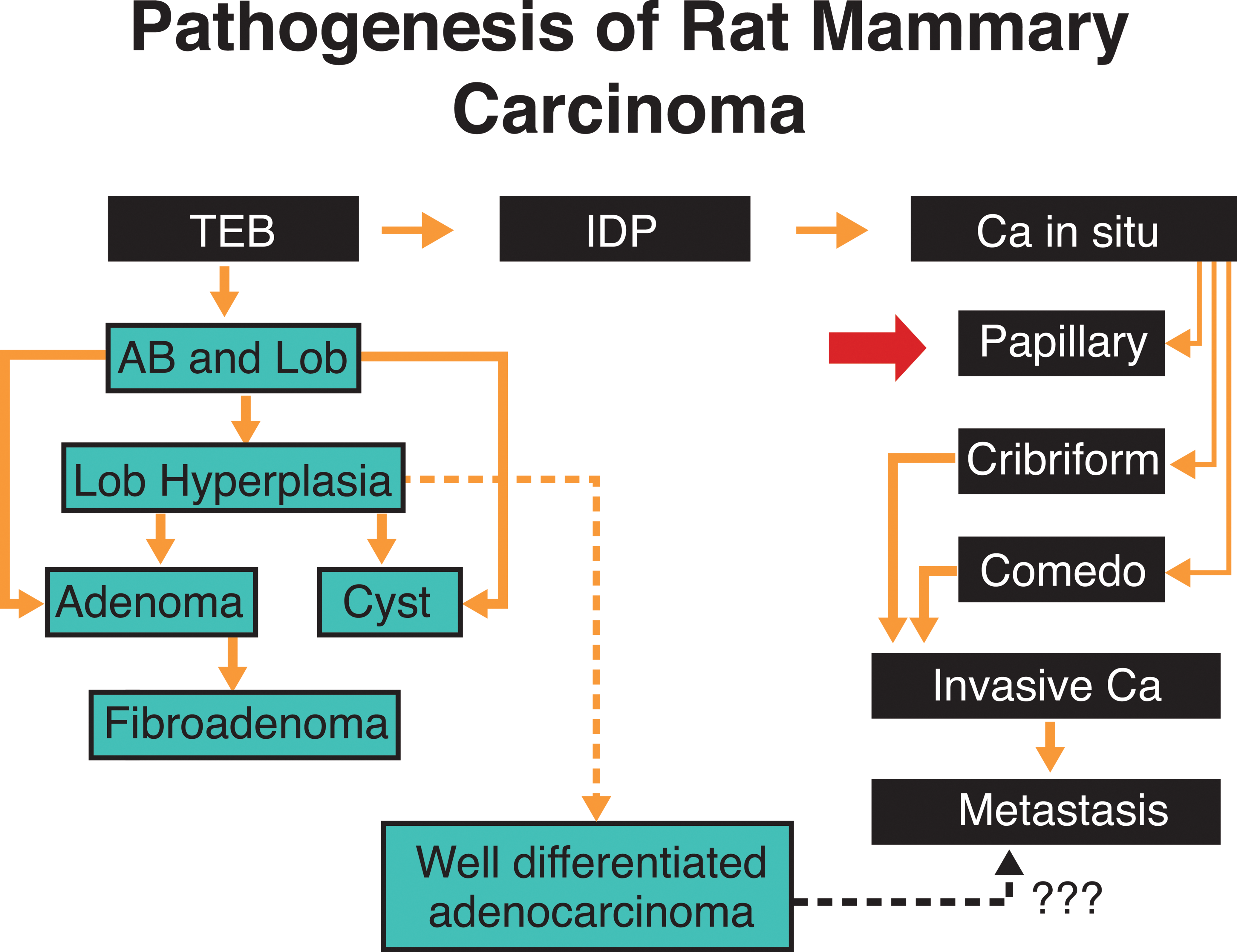
Pathogenesis of chemically induced rat mammary tumors. The undifferentiated terminal end bud (TEB) affected by the carcinogen progresses to IDP, and in situ ductal carcinoma (Ca in Situ) that exhibit various histopathological types. Further tumor growth and coalescence of neighboring lesions originate invasive carcinomas (Invasive Ca), which might become metastatic. When the carcinogen affects more differentiated structures, such as alveolar buds (AB) and lobules (Lob), the lesions developed are more benign in nature and appear later than the ductal carcinomas. Alveolar bud hyperplasia (AB Hyperplasia; adapted from Russo and Russo 1994 with permission).
Excessive epithelial proliferation and development of progressive cytologic abnormalities result from carcinogen exposure and ultimately produce tumors (Russo et al. 1977; Russo and Russo 1987). This process can be initiated with the administration of DMBA to virgin rats (Russo et al. 1977). The administration of DMBA when the animals are between the ages of 45 and 55 days induces the largest number of transformed TEBs. Affected TEBs, instead of differentiating into ABs, become larger, and they are called intraductal proliferations (IDPs). IDPs become progressively larger and their confluence leads to the formation of carcinomas (Russo and Russo 1987; Russo et al. 1977).
Tumor development does not occur as a random event in all six pairs of mammary glands. Virgin animals treated with the carcinogen develop a greater number of tumors in those glands located in the thoracic region than in glands located in the abdomino-inguinal area. These topographic differences in tumor incidence appear to be due to the asynchronous development of the thoracic mammary glands, which retain the undifferentiated TEBs for a longer period of time than mammary glands located in different topographic areas (Russo and Russo 1996, 1987)
However, a trend in a different direction has been observed in irradiated animals (van Zwieten 1984). Those TEBs that were already differentiated into ABs before DMBA administration do not develop carcinomas but remain unmodified, undergo dilation, give rise to hyperplastic lobules (Figure 1), exhibit epithelial proliferation forming tubular adenomas, or give rise to cystic dilations. Hyperplastic lobules and cysts appear later than IDPs, the first ones being observed at 5 to 6 weeks after DMBA administration (Russo and Russo 1987; Russo et al. 1977; Russo, Tait, and Russo 1983; Russo, Tay, and Russo 1982).
The observation that mammary carcinomas arise from undifferentiated structures of the gland, namely TEBs, whereas benign lesions, such as adenomas, cysts, and FAs, arise from structures that were more differentiated at the time of carcinogen administration, indicates that the carcinogen requires an adequate structural target and the type of lesion induced is dependent upon the area of the mammary gland that the carcinogen affects. Thus, the more differentiated the structure at the time of carcinogen administration, the more benign and organized is the lesion which develops (Russo and Russo 1996).
The high susceptibility of the TEB to neoplastic transformation is attributed to the presence of stem cells and the cell kinetic properties of its lining epithelium, whose rate of cell proliferation and of DNA synthetic activity (DNA-LI) are maximal at the tip and decrease toward the ductal or proximal portion of the gland. The TEB is also characterized by having the highest growth fraction, which progressively diminishes in the more differentiated ABs and lobules (Russo and Russo 1980). The high rate of cell proliferation is associated with the short length of the cell cycle (Tc), which in TEBs of young virgin rats has an average length of 11 hr, lengthening to 21 and 28 hr in TDs and ABs, respectively. Using these cell kinetic parameters, we have calculated the rate of cell loss in each one of the compartments of the mammary tree. Interestingly, the TEB is the structure with the highest proliferative ratio and the lowest percentage of cell loss. DMBA is metabolized by mammary epithelial cells to polar metabolites, including epoxides (Russo, Tait, and Russo 1983; Tay and Russo 1981a, 1981b) that may be responsible for causing DNA damage.
When dissociated breast epithelial cells of TEBs obtained from virgin animals and lobular cells obtained from parous animals are grown in vitro, they exhibit different rates of formation of polar metabolites. Cells of TEBs produce more polar and less phenolic metabolites than do lobular cells, indicating that the former, in addition to their higher proliferative activity, produce more epoxides, with a greater binding of DMBA to DNA (Russo and Russo 1987; Russo, Tay, and Russo 1982; Tay and Russo 1981a, 1981b). Autoradiographic studies show that the greatest uptake of [3H]DMBA occurs in the nucleus of the epithelial cells of TEBs, and the lowest uptake is observed in ABs and lobules, indicating that the highest DMBA–DNA binding is associated with the structure of the gland with the highest replicative properties (Russo, Tay, and Russo 1982). The ability of the cells to remove DMBA adducts from the DNA, an indication of their capability to repair the damage, is less in TEB cells than in lobular cells. This is attributed to the shorter Go and Tc and not to lack of reparative enzymes (Russo and Russo 1987; Tay and Russo 1981a, 1981b).
Pathogenesis Human Breast Tumors
The nature and site of origin of neoplastic growth in human breast has been the subject of numerous studies based on examination of surgical and autopsy tissues (Black 1969; Cheatle 1926, 1931; Dawson 1962, 1934; Gallagher 1969; Geschickter 1945; Karpas et al. 1965; Kern and Brooks 1969; Kiaer 1954; Levin et al. 1964; Parks 1959; Russo and Russo 1987b; Ryan and Coady 1962; Cheatle 1926; Sandison 1962; Vorherr 1974).
The TD or terminal duct is best regarded as having two parts. The first part is closest to the nipple and is called extralobular or entering TD. The second part of the TD is referred to as the intralobular or axial TD. The ductules, together with the intralobular or axial TD and the distinctive loose intralobular connective tissue, are the three recognized constituents of the lobule. The lobule type 1 (Figure 2), essentially synonymous with the TDLU, is the basic morphologic and functional microstructure of the mammary gland (Alpers and Wellings 1985; Russo and Russo 1996; Wellings 1980; Wellings, Jensen, and Marcum 1975). The preponderance of evidence indicates that most mammary carcinomas arise from lobules type 1 (TDLU) or their precursors (Figure 2). Lesions originated in lobules type 1 include at least carcinoma in situ, the common infiltrating duct carcinomas, and perhaps some other kinds of infiltrating carcinomas. In contrast, it is thought that classical lobular carcinoma in situ (LCIS) may arise from the more differentiated lobules type 2 (Figure 2).
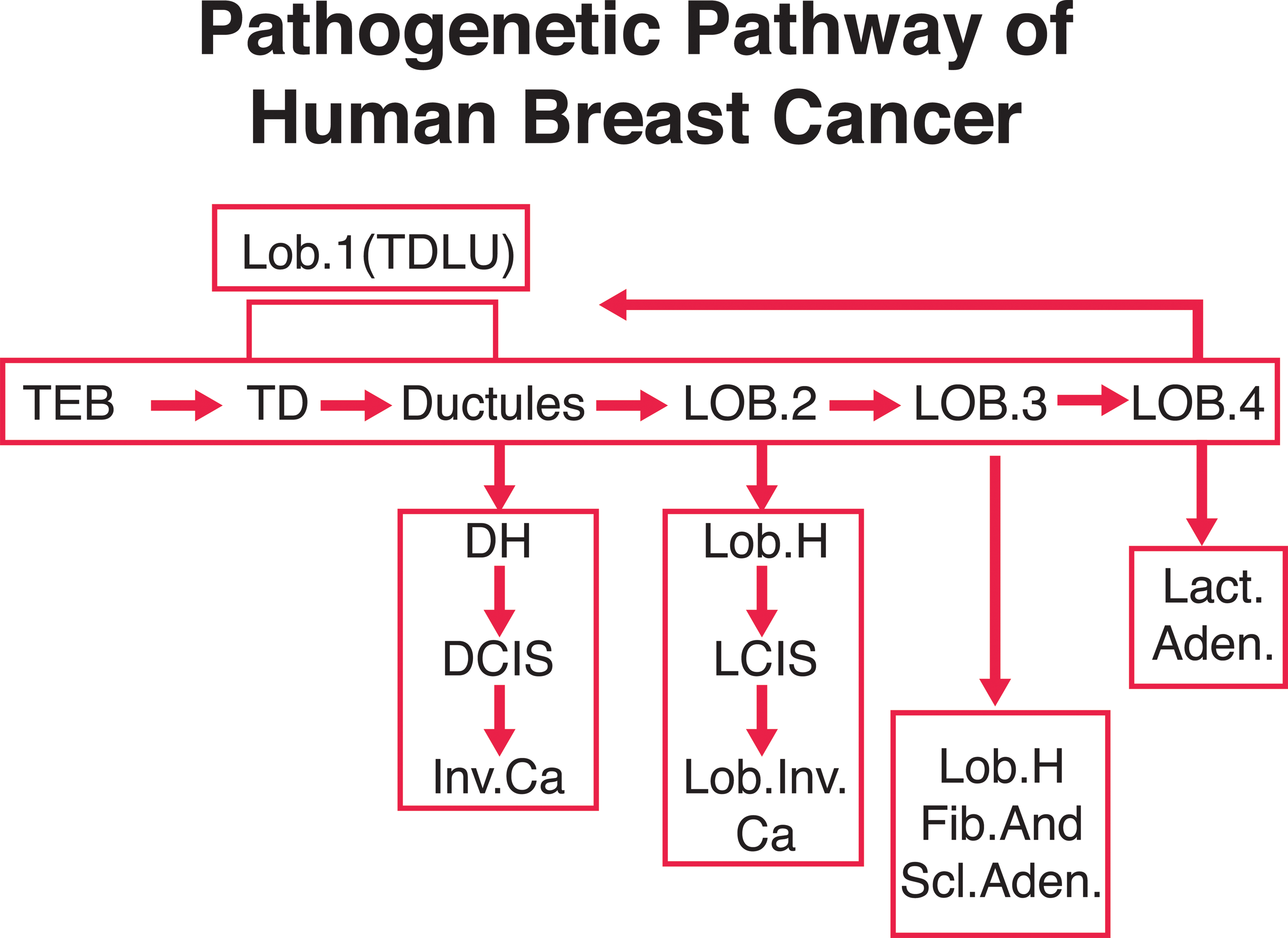
Chart representing the pathogenetic pathway of human breast cancer lesions (adapted from Russo and Russo 1994 with permission).
Comparative Aspects of Pathogenesis
The TEB in the human female is a prepubertal structure and the biology and the differentiation of the structure from the prepubertal to the pubertal age needs to be studied. Most of the data collected for the study of mammary carcinogenesis are derived from observations of postpubertal breasts. In the postpubertal breast, most of the structures of the gland are mainly composed of TDs and ductules forming lobules type 1, which are the basic TDLU. The terminal ductal structures of the TDLU originate preneoplastic lesions that evolve to ductal carcinoma in situ (DCIS), progressing to invasive carcinoma and finally metastasize. The differentiation of lobules type 1 to type 2 is also important since morphologic observations suggest that lobules type 2 could be involved in the development of atypical lobules that originate LCIS (Figure 2) and its invasive form.
Lobules type 3 present in the human breast seem to give origin to hyperplastic or hypersecretory lobules, FAs, sclerosing adenosis (Figure 2), and apocrine cysts, whereas lactating adenomas seem to originate from lobules type 4 (Figure 2). In the rat, these more benign lesions originate from virginal and mature lobules.
An important difference between the pathogenic pathway in the rat and human is at the level of the TDLU. The TEB in the rat would be equivalent to the intralobular TD in the human, the area that is most susceptible to neoplastic growth. However, an important gap in our knowledge is the lack of observations of early carcinomas in the human breast in order to determine whether they originate from more undifferentiated TEBs before the lobular elements have formed. Another possibility is that in humans, carcinogenesis takes place in more differentiated structures, or TDLU. The presence of lobules type 1 in the postmenopausal woman may explain the rising incidence of neoplasia in older women; however, this does not rule out the possibility that malignant transformation had occurred much earlier in life. Chemically induced mammary carcinogenesis requires active cell replication that is maximal in the TEB. In the human breast, the highest peak of cell replication occurs in the TD during early adulthood, decreasing considerably with age (Russo and Russo 1996; Russo, Tay, and Russo 1982). This observation indicates that during early adulthood, when cell turnover is more rapid, more chances exist for a neoplastic process to be initiated. Epidemiologic findings reveal that the young woman’s breast is more susceptible to ionizing radiation. This could be explained as a consequence of incomplete differentiation of the gland, meaning one having TDs with high replicative properties (Calaf et al. 1982a, 1982b; Russo 1978). These observations are supported by experimental data showing that the TDLU or lobule type 1 of the human female has the highest in vitro binding of carcinogen to DNA. When these structures are cultured and treated in vitro with carcinogens, they express phenotypical changes of transformation that are not expressed by lobules type 2 and 3 (Russo et al. 1988).
It has been shown that in human the usual ductal hyperplasia has few similarities to atypical ductal hyperplasia (ADH), DCIS, or invasive cancer. ADH has many similarities to low-grade DCIS (Burstein et al. 2004; Schnitt and Collins 2009; Simpson et al. 2005). In contrast, low-grade DCIS appears to be genetically distinct from high-grade DCIS (Burstein et al. 2004; Simpson et al. 2005). It seems that different forms of invasive breast cancer that develop mostly from different types of DCIS lesions, with low-grade DCIS lesions giving rise to low-grade invasive breast carcinomas, and high-grade DCIS lesions giving rise to high-grade invasive breast carcinomas (Burstein et al. 2004; Lopez-Garcia et al. 2010; Schnitt and Collins 2009; Simpson et al. 2005).
Comparative Histopathological Classification of Mammary Tumors between Human and Rat
The validity of rat mammary carcinogenesis for the study and understanding of the biology of human mammary carcinogenesis and for validating the development of strategies for breast cancer prevention and cure requires that in these two models, in addition to similarities in the basic pathogenesis and developmental concepts, that (a) the histotype of the tumors is similar; (b) the cell types present in the rat react with similar immunocytochemical markers as do the human ones, and (c) the biologic behavior of tumors is comparable in the 2 species. Rat mammary tumors have been classified by several authors (Greaves and Faccini 1984; Russo and Russo 1996; Russo et al. 1989b; Russo et al. 1990; van Zwieten 1984). There is agreement that tumors appearing histologically malignant in the rat have features in common with the intraductal and infiltrating ductal carcinomas in humans, but few spontaneously metastasize. Similarly, benign FAs and adenomas that occur in rats closely resemble the human benign tumors.
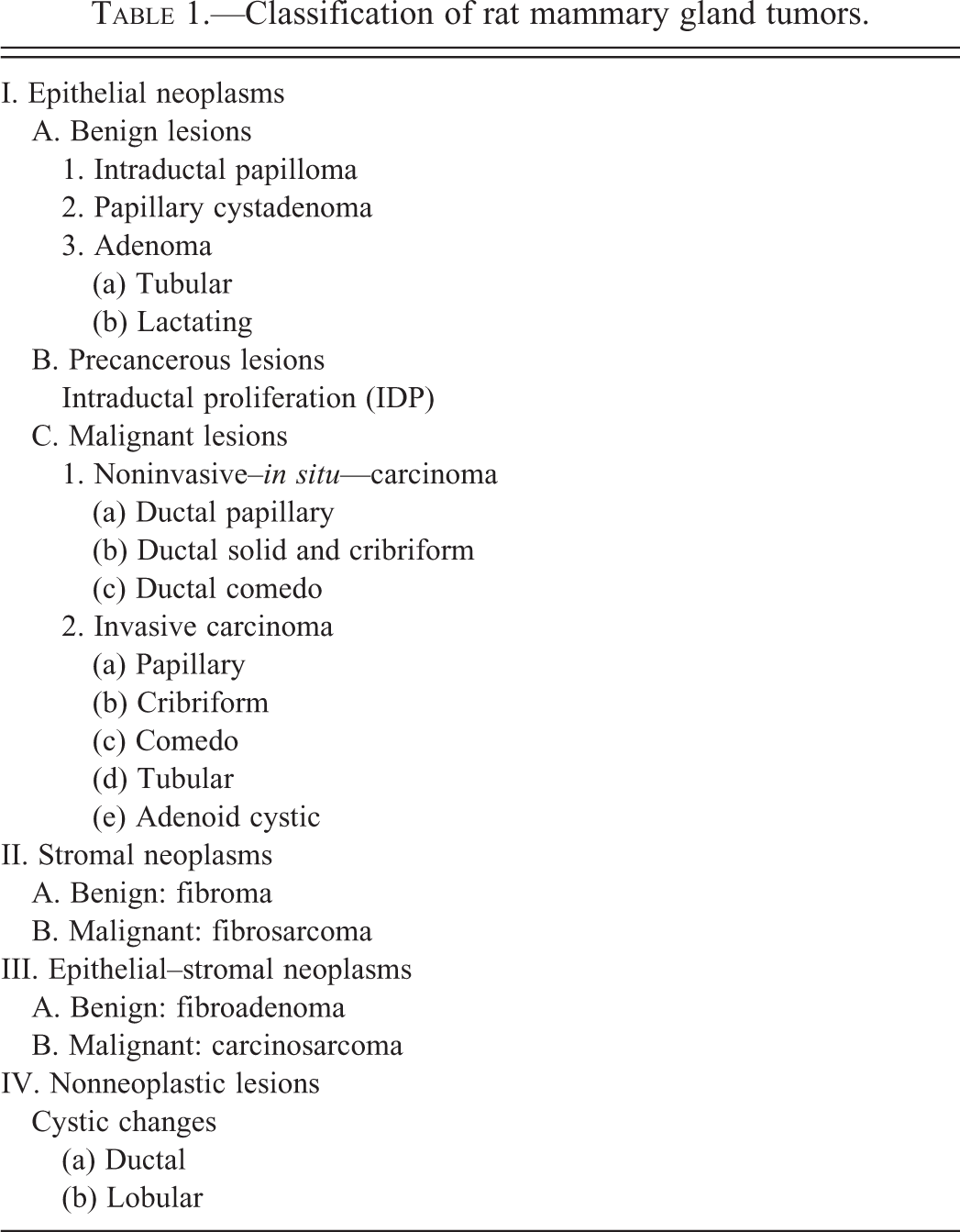
The majority of induced tumors are papillomatous with hyperplastic epithelium containing both epithelial and myoepithelial cells, and appear cytologically benign, or they may be composed of epithelial cells with varying degrees of cytologic atypia, growing in solid, papillary adenomatous patterns. In most tumors, the abnormal epithelium tends to remain rigidly confined by the adjacent stroma and shows no clear evidence of invasion. All of these features contribute to the difficulty of making clear distinctions between benign and malignant lesions. The main histological types of mammary tumors found in the rat are shown in Table 1. It is clear that most of the lesions found in the rat mammary glands have their counterpart in human pathology. However, there are specific lesions in humans, such as Paget's disease of the nipple and infiltrating ductal carcinoma, scirrhous, and medullary type that have not been reported in the rat mammary gland. Lobular carcinoma, in situ or invasive, has not been reported in the rat (Russo et al. 1989b).
Classification of rat mammary gland tumors.
The role of Aging and Parity in the Rat as Determinants of a Lower Susceptibility to Cancer and Benign Lesions
The susceptibility of the mammary gland to carcinogenesis decreases significantly with age. This has been explained as a consequence of a decrease in the number of undifferentiated structures. It has been reported that mammary tumorigenesis by a carcinogen is inhibited in rats in which mammary growth has been prestimulated by hypothalamic lesions (Clemens, Welsch, and Meites 1968) or pituitary grafting (Welsch, Clemens, and Meites 1968), or when carcinogen is administered to lactating rats (Dao, Bock, and Greiner 1960; Huggins, Grand, and Brillantes 1959). Decreased tumor incidence has also been observed when mice and rats (Russo and Russo 1978a; Russo 1978; Russo and Russo 1978b) are inoculated with chemical carcinogens after pregnancy and lactation. In the rat (Russo and Russo 1978a), it has been demonstrated that the protective effect seen during pregnancy and lactation extends to the postweaning period. Thus, administration of a single dose of DMBA to parous rats when the glands have regressed to a resting stage induces a much lower incidence of mammary carcinomas. This indicates that it is not the hormonal status of pregnancy and lactation by itself that protects the gland, but the permanent changes induced in the gland structure and in the biological properties of the gland epithelium which are independent of the hormonal status of the host (Ciocca and Russo 1980). The degree of differentiation of the mammary gland can be described at a given time in the life span of the rat according to the number of TEB, TD, AB, and lobules, and their level of DNA synthesis and proliferative activity (Russo and Russo 1996). A decrease in the density of TEB is observed with aging, and in the glands of multiparous rats, TEB are undetectable. TD are the last generation of ducts which result from the lack of differentiation of TEB → AB → lobules. These TD share some features of the TEB, such as a high DNA labeling index. Pregnancy and lactation induce further differentiation of TD to AB and lobules, and as a consequence, TDs are rarely observed in the mammary gland of resting multiparous rats (Russo and Russo 1987, 1996; Russo, Tewari, and Russo 1989a).
The highest incidence of tumors is observed in YV rats, and the lowest in multiparous rats. Histological evaluation of the tumors reveals that 100% of the tumors developed in YV rats are adenocarcinomas. In multiparous rats, only 21% of tumors are carcinomas. In OV rats, 63% of the tumors are carcinomas. Numerous lesions induced by DMBA are of a benign nature. Thus, FAs are twice as frequent in multiparous rats as in age-matched OV rats (Russo and Russo 1987, 1996). However, YV and OV rats develop a higher incidence of HAN than multiparous rats. In addition, the incidence of adenomas and cysts is similar among YV and OV rats, but the incidence is much lower in the mammary gland of multiparous rats. In conclusion, the lower incidence of carcinomas in the gland of multiparous rats is related to the absence of TEB and to the lower number of TDs with low DNA-LI.
The refractoriness of parous rats to carcinogenesis can, therefore, be explained as a consequence of a higher degree of differentiation of the gland after pregnancy and lactation. On the other hand, the higher susceptibility of the mammary gland of virgin rats is explained by the presence of TEB and TD with very high DNA-LI. However, OV rats have more tumors than multiparous rats, demonstrating that the lower susceptibility observed in multiparous rats is not due to age alone but to the higher degree of differentiation that pregnancy and lactation induces in the mammary gland (Russo and Russo 1987, 1996; Schmitt-Ney et al. 1992).
Differential Response of the Rat and Human Mammary Gland to Prolactin
Prolactin Effect on the Stem Cells of the Rat Mammary Gland
Transgenic and gene disruption techniques have shown that complete PRL deficiency results in the arrest of mammary organogenesis at an immature pubertal state. In this arrested developmental state, the epithelial component of the gland consists of a basic ductal system and TEB, but none of the lobuloalveolar system. PRL induces the differentiation and growth of alveolar progenitor cells from the ductal epithelium (Chepko and Smith 1997; Smith 1996). This development of alveoli from precursor cells in the ductal epithelium may involve both clonal growth from committed precursors and induction of phenotypic changes in cells that are near specialized “organizer” cells. In addition, PRL is an essential survival factor for lobuloalveolar cells during both pregnancy and lactation (Bailey et al. 2004; Capuco et al. 2002; Humphreys and Hennighausen 1999; Travers et al. 1996). Therefore, local or systemic increase of PRL will maintain the lobular structures. The mammary gland is an important site of PRL synthesis and secretion. PRL is present in significant concentrations in milk (Ben-Jonathan et al. 1996; Kacsoh et al. 1993). It has been suggested that locally synthesized PRL in the mammary gland might act as a growth factor for both normal breast epithelium and breast cancer cells (Clevenger et al. 2003) and as a consequence the maintenance of the epithelial cell proliferation.
Prolactin Effects in Human Mammary Gland Are Restricted to the Lobule 4 and Development toward Lactation
During pregnancy, the lobuloalveolar epithelium undergoes extensive proliferation under the influence of PRL, placental lactogens (PLs), progesterone, and local growth factors such as RANK-ligand and insulin-like growth factor-2 (IGF-2; Brisken et al. 2002; Hovey et al. 2003; Srivastava et al. 2003). PLs are synthesized during pregnancy in most mammals. The major stimulus to mammary gland development during pregnancy is presumably PLs, rather than pituitary PRL (Handwerger 1991). Loss of PLs and placental steroids at parturition is accompanied by elevation of pituitary PRL secretion, and a corresponding shift to pituitary-dominated regulation of mammary gland function during lactation. The importance of this shift is that pituitary PRL is strongly regulated by a suckling-induced neuroendocrine reflex, which allows nursing activity to determine directly the lactational stimulus to the mammary glands. During and after parturition, progesterone, estrogen, and PL fall precipitously, and PRL rises. The lobuloalveolar epithelium in the lobules type 3 and 4 are converted to a secretory phenotype. At the end of lactation, involution of the lobuloalveolar system occurs in response to milk stasis and falling systemic lactogens (Santagata et al. 2014).
Therefore, PRL and PLs, each of which binds to the PRL-R, act during 3 stages of mammary gland development: lobule budding during organogenesis, lobuloalveolar expansion during pregnancy, and lactational differentiation after parturition.
FAs in the Human Breast and in the Rat Mammary Gland
FAs in the Human Breast
FA is the most common benign tumor of the breast in young women in the childbearing period. Gradual enlargement over a period of months or years is the rule in early adolescence and in pregnancy. Married and unmarried women were affected in approximately equal numbers. Among the married women, those with children predominated in a ratio of 2:1.
FA is a benign, confined tumor of the breast that has a mixture of glandular and mesenchymal elements. FAs that are allowed to grow after initial detection usually cease to grow when they reach 2 to 3 cm in diameter (Haagensen 1986). Blacks more commonly develop FAs compared with whites and at a younger age as well. FAs in blacks are also more likely to recur. Infarcts of the breast may occur during pregnancy or lactation with a resultant discrete mass. FA is the most common benign tumor of the breast in young women in the childbearing period; however, more rapid growth may occur during menopause. The gross appearance of FAs is usually characteristic and often diagnostic by its sharp circumscription and smooth boundary with surrounding breast tissue. The cut surface is white, and the epithelial elements are light brown areas. The FA is usually a solitary lesion, but in few cases multiple tumors are present and the interval between the excision of a previous tumor and the second mass vary from 2 to 25 years. The tumor occurs most often in the outer and upper quadrant. The upper half of the breast is more frequently affected than the lower and the outer more often than the inner portion. The sizes vary but more often is between 2 and 5 cm in diameter (Haagensen 1986).
Cysts from 1 to several mm in diameter may be found in older growths containing also hard, hyalinized fibrous tissue with occasional areas of calcification. In the majority of FAs, the number and the size of the ducts are increased. Approximately 1 of 200 FAs show infarction (Wilkinson and Green 1964).
Microscopically, fibrous tissue composes most of the FA; either the stroma may surround and easily definable duct-like epithelial structures pattern known as pericanalicular or the epithelium may be stretched into curvilinear arrangements known as intracanalicular. Smooth muscle is an extremely rare component of FAs (Goodman and Taxy 1981). The epithelium within an FA may have the same appearance as elsewhere in the breast, including apocrine metaplasia (Azzopardi 1979). Rarely, squamous metaplasia is present (Salm 1957).
The epithelia form tubules that are composed of cuboidal or low columnar cells with round uniform nuclei resting on a myoepithelial cell layer. The stroma is made up of loose connective tissue rich in acid mucopolysaccharides, but it may be partially or totally composed of a dense fibrous type. The spindle cells are predominantly CD34-positive fibroblasts, admixed with scattered Factor XIIIa–positive cells (Moore and Lee 2001; Silverman and Tamsen 1996). The cellularity of the stroma varies from case to case and the alternative diagnosis of phylloides tumor should be considered.
FAs often resemble the normal mammary tissue of adolescence. The hypertrophy of duct epithelium, scarcity of mammary lobules, and the increase in pale-staining periductal connective tissue found in adolescence are also characteristics of these new growths. The ordinary FA may be looked upon as an exaggerated form of puberty hypertrophy affecting an isolated portion of the breast. The accuracy of this interpretation can be proved experimentally. Typical benign FA occurs in the breast of rats and rabbits that have been continuously stimulated with increased amounts of estrogenic hormone.
Ultrastructurally, the most interesting feature of FAs is the constant presence of a multilayered basal lamina around the epithelial and endothelial cells (Carstens 1974). The stromal cells have features of fibroblasts (Reddick et al. 1987). FAs contain progesterone receptors almost universally and estrogen receptors in approximately one-fourth of the cases (Umekita and Yoshida 1998). Approximately 20% of FAs have been found to have clonal chromosome aberrations, suggesting that FA is a benign neoplasm of the specialized stroma of the breast with an accompanying epithelial component (Fletcher et al. 1991).
According to Rosai (2004), the morphologic variations in FA are plentiful, and among them are hyalinization, calcification, and/or ossification of the stroma. Presence in the stroma of multinucleated giant cells of reactive nature can also be found (Berean et al. 1986). Presence in the stroma of mature adipose tissue, smooth muscle, or metaplastic cartilage has been reported (Arrigoni, Dockerty, and Judd 1971; Goodman and Taxy 1981; Metcalf and Ellis 1985; Oberman, Nosanchuk, and Finger 1969; Petrik 1987; Shimizu et al. 1996) as well as prominent myxoid changes (Carney and Toorkey 1991). Sclerosing adenosis occurs in less than 10% of cases (Azzopardi 1979). Lactational changes are manifested by an increase in the amount of cytoplasm in the epithelial cells, which appear vacuolated, and by dilatation of the glandular lumina by secretion.
There is a distinct type of FA that tends to occur in adolescents (often in blacks and sometimes involving both breasts), reach a large size (over 10 cm), and show hypercellularity of glands and/or stroma (Dehner, Hill, and Deschryver 1999; Eusebi and Azzopardi 1980; Fekete et al. 1987; Mies and Rosen 1987; Pike and Oberman 1985). No differences have been found in FAs removed from patients taking oral contraceptives and those in control cases, except for the occasional formation of acini in the former (Fechner 1970).
A variant of FA is the tubular adenoma (Hertel, Zaloudek, and Kempson 1976). Grossly tubular adenomas have a fine nodularity and the tubular structures are seen but no lobular configuration is evident. Tubular adenomas may have evidence of secretory activity, but when not occurring in association with pregnancy or lactation should not be termed “lactating adenomas.” Lactating adenomas are certainly analogous in some ways to tubular adenomas and may represent a physiologic response of the tubular adenoma to pregnancy. In addition to showing lactational changes, the adenomas presenting in pregnancy have a more evident lobular anatomy than that seen in most tubular adenomas.
Traditionally, the risk for subsequent carcinoma in patients with typical FA has not been considered to be higher than for the general population (Fondo et al. 1979; Pick and Iossifides 1984). Malignant changes in FAs are found in only 0.1% of cases (Goldman and Friedman 1969; McDivitt, Farrow, and Stewart 1967; Pick and Iossifides 1984). They usually involve the epithelial component, and the large majority are in situ lesions (Diaz, Palmer, and McDivitt 1991; Fondo et al. 1979; Pick and Iossifides 1984). As well described by Rosai (2004), “in some cases the malignant tumor is entirely within the confines of the FA, but in others it involves the surrounding breast as well.” The latter may simply represent extension into the FA by a carcinoma originating elsewhere in the breast. In a series of 105 FAs containing carcinoma, 95% of the cases were in situ lesions, and lobular and ductal types occurred with equal frequency. Nine of the 10 FAs harboring an invasive carcinoma also contained carcinoma in situ (CIS), supporting the origin of the invasive component in the FA. CIS within the FA was associated with CIS in the surrounding breast in 21% of the cases (Fondo et al. 1979). A large-scale epidemiologic study reported by Dupont et al. (1994) concluded that FA represents a low long-term risk for breast carcinomas and that this risk is increased in women with complex FAs, ductal hyperplasias, or a family history of breast carcinoma. This risk is not further increased if the FA contains foci of atypical epithelial hyperplasia (Carter et al. 2001). Sarcomatous transformation of the stroma of an FA is an even rarer phenomenon (Curran and Dodge 1962).
FAs in the Rat Mammary Gland
The incidence of spontaneous mammary tumors in several different strains and stocks of female rats has been published (van Zwieten 1984) ranging in duration from 18 months to the natural life span of the rats (Tables 2 and 3). In general, the mean incidence of FA in females of most rat strains varies from approximately 20 to 40%. On average, FAs occur more commonly in SD rats than in other strains with values as high as 68% (van Zwieten 1984) instead of in the ACI/N rats with the lowest incidence (4.8%; Maekawa and Odashima, 1975).
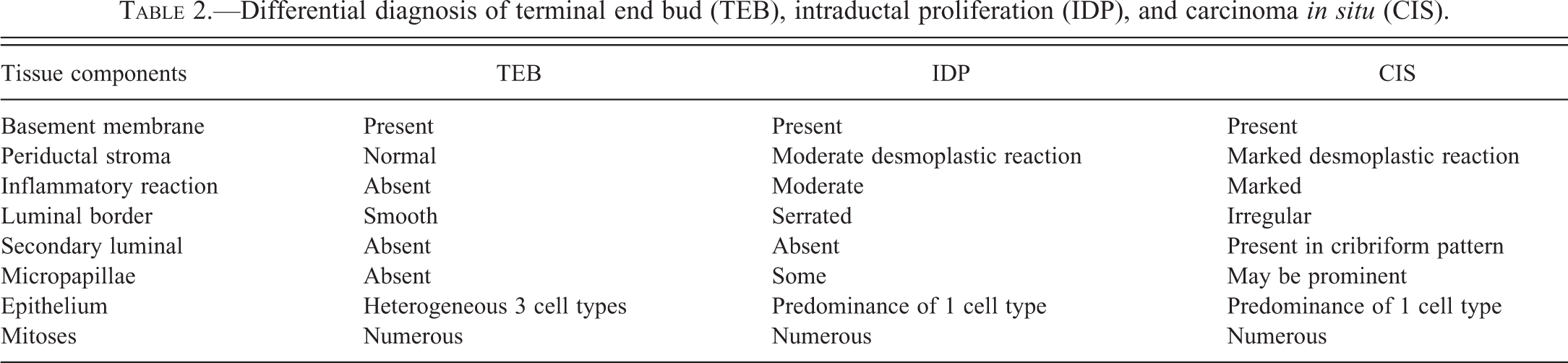
Differential diagnosis of terminal end bud (TEB), intraductal proliferation (IDP), and carcinoma in situ (CIS).
Incidence of invasive rat mammary cancer induced by DMBA.
Note: DMBA = 7,12-dimethylbenz (a) anthracene.
As in humans, spontaneous mammary tumors in rats occur far more commonly in females than in males. Mammary tumors have been observed in virtually every strain, although none were observed in males of some strains of rats (Burek 1978). FAs are found in approximately 1 to 2% of male rats, regardless of strain, although incidences as high as 11% have been reported in SD (Anver et al. 1982) and Wistar (Kroes et al. 1981) rats. In a full life-span study in F344 rats, 13.4% of the males had either an FA or an adenoma (Solleveld et al. 1984).
Mammary tumors, like most other neoplasms in the rat, occur with increasing frequency as the animal ages (Burek 1978; Solleveld et al. 1984). The prevalence of mammary tumors, regardless of type, is essentially 100% in female F344 rats older than 137 weeks (Solleveld et al. 1984) and in female SD rats between 118 and 130 weeks of age (van Zwieten 1984). Although the age-specific prevalence rates of FAs and adenocarcinomas in these 2 strains continued to increase with increasing age, Burek (1978) found that in WAG/Rij and BN/BiRij rats only adenocarcinomas continued to increase in each age group. FAs, however, had a peak risk period between 31 and 36 months of age, and their incidence decreased in older rats. The age-specific prevalence rate of both FAs and adenocarcinomas decreased slightly during an earlier age period in both F344 (85–97 weeks) and SD (53–65 weeks) rats (Solleveld et al. 1984).
As in the human, the FA in the rat mammary gland is a benign tumor composed of both well-differentiated epithelial and fibrous connective tissue (Figure 3). FAs may range in size from a few millimeters to 8 cm or more in diameter. As described by van Zwieten (1984), these tumors are spherical or discoid, smooth or slightly bosselated masses that are freely movable in the subcutis. Their consistency can be firm and tough or soft and rubbery, and the cut surface is generally white or pink and has a distinctive lobulated pattern. The histological appearance of FAs can vary depending on the relative proportions of epithelium and fibrous connective tissue (cf. Figure 3A and B with Figure 4A–B). Thus, FAs can range from those composed predominantly of epithelial tissue to those composed predominantly of connective tissue. The alveolar structures in some FAs may be widely distended with secretion (Figure 4A–B). Some FAs contain multiple foci of epithelium, showing unusual growth patterns with cellular pleomorphism and atypia. These foci can range from small papillary projections within the ductules in some tumors to solid, cribriform, or papillary epithelial formations within clusters or distended ductules in others. Occasionally, adenocarcinomas arise within FAs, suggesting that the smaller foci of cellular atypia may represent an early premalignant change (van Zwieten 1984).
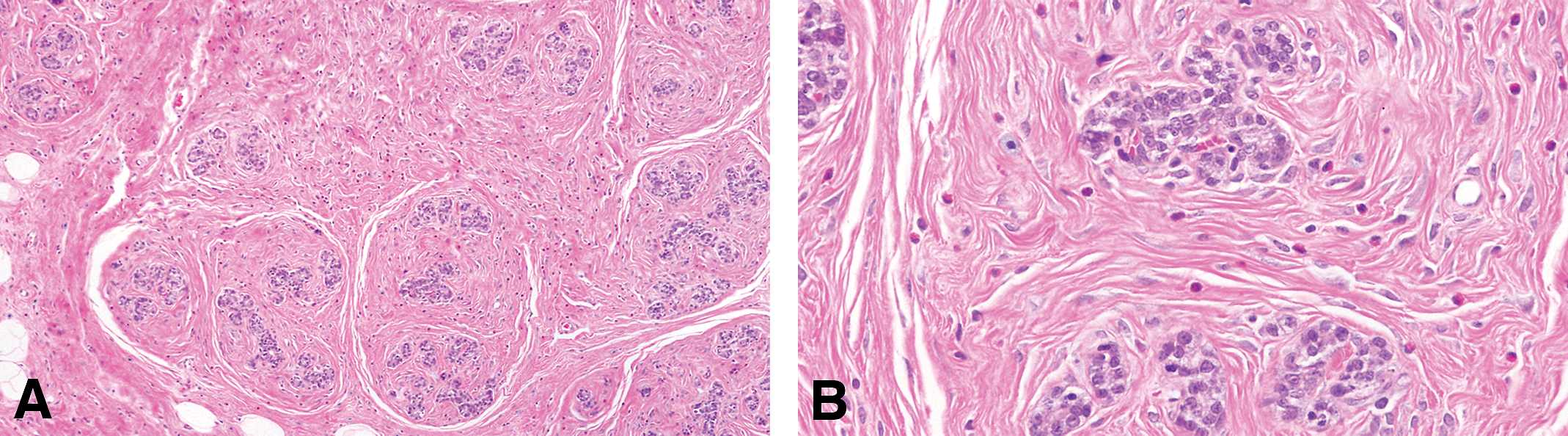
(A) The fibroadenoma is a benign tumor composed of both well-differentiated epithelial and fibrous connective tissue. (B) Glandular epithelial cells surrounded by dense connective tissue. Stained with H&E, 4× and 40×, respectively.
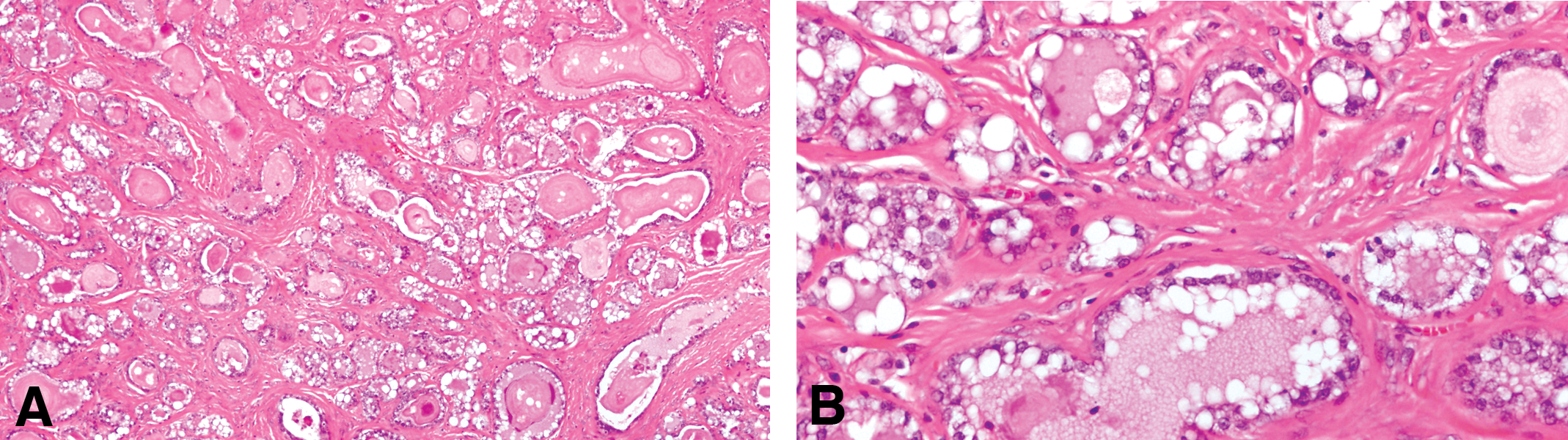
(A) Fibroadenoma composed predominantly of alveolar structures distended with secretion. (B) The epithelial cells are secreting lipids and proteinaceous material. Stained with H&E, 4× and 40×, respectively.
Experimental Induction of FAs Using Hormones
The rapid growth of a preexisting FA during pregnancy indicates a special responsiveness to estrogen. The increase in the number of ducts in their lining cells and in the amount of periductal fibrous tissue found in growing fibroadenomas duplicates the histologic pattern of rapid mammary growth in normal adolescence and in early pregnancy. This pattern is repeated when the mammary gland of the rat or monkey or human is stimulated with high doses of estrogen (Geschickter et al. 1934). Estrogen in combination with gonadotropic hormone increased the number of successfully transplanted FAs in rats and stimulated hyperplasia in these growths (Heiman and Krehbiel 1936). Geschickter (1945) produced FAs in the mammary glands of rats by implanting pellets of estrone under the skin to provide a constant, intense estrogenic stimulation. He also found that a constant absorption for many months of excessive amounts of estrogen leads to the formation of FAs; however, fluctuations of the concentration of estrogen induced large cysts but no FAs. This corroborates the clinical observation that FAs have a tendency to form during adolescence, pregnancy, and the menopause when a relatively constant estrogenic stimulation is maintained, rather than in cyclic women where there is a repeated rise and fall in the level of the hormone (Geschickter 1941).
Experimental Induction of FAs Using Chemical Carcinogens
The 2 most widely used experimental systems for the study of mammary tumorigenesis are the models in which tumors are induced in the SD rat by DMBA or in the SD or Fischer 344 rat by NMU. DMBA, given by gavage in a single dose of 2.5 to 20 mg, induces tumors with latencies that generally range between 8 and 21 weeks with and final tumor incidences close to 100% if sufficient time elapses before necropsy (Russo et al. 1990). NMU administered by intravenous or subcutaneous injection in a single dose of 25- or 50-mg/kg body weight yields tumors with similar latency and incidence (Russo et al. 1990).
Tumor latency is, in general, inversely related to carcinogen dose, whereas both tumor incidence and number are directly related, if relatively early end points are used. For the study of modulating factors, tumor latency is often the most sensitive end point. Tumor histology is influenced by carcinogen dose. In SD rats given a single NMU dose of 10-mg/kg body weight, 42% of tumors were malignant, whereas 86 to 94% were malignant at doses from 35 to 50 mg/kg (McCormick et al. 1981). Tumor incidence, number of malignant tumors per rat, and latency all showed a dose response, but number of benign tumors per rat did not (McCormick et al. 1981).
The susceptibility of the mammary gland to DMBA or NMU-induced carcinogenesis is strongly age-dependent and is maximal when the carcinogens are administered to animals between the ages of approximately 45 and 60 days, that is the age of sexual maturity. Active organogenesis and high rate of proliferation of the glandular epithelium are characteristics of that period (Grubbs et al. 1986; McCormick et al. 1982; Rose et al. 1980; Russo and Russo 1978b, 1980). DMBA activation in the gland is also high, but it may not be a significant factor, since NMU, which is similarly most effective at that age, does not require activation. The age-related changes in susceptibility are independent of dietary fat content; increased tumorigenesis occurs in rats fed high-fat diet at all ages tested. In virgin rats treated with DMBA, tumors that develop are largely carcinomas, although the proportion can be altered by carcinogen dose and dietary fat. The administration of DMBA to virgin rats of different ages induces tumors with an incidence that is directly proportional to the density of highly proliferating TEBs (Russo and Russo 1978b). A 100% incidence of carcinomas is obtained when DMBA is administered to rats aged 30 to 55 days, but the highest number of tumors/animal is observed when the carcinogen is given to animals when they are 40 to 46 days of age, a period when TEBs are most actively differentiating into ABs. The sharp decrease in the number of TEBs observed in animals older than 55 days is also accompanied by a lower incidence of tumors as well as a lower number of tumors/animal (Russo and Russo, 1978b, 1980, 1987; Russo, Tay, and Russo 1982).
Genetic Influences in Rat Mammary Tumorigenesis
Genetic factors control the susceptibility of different rat strains to DMBA or NMU mammary tumorigenesis. Of the commonly used strains, SD and Wistar-Furth are the most susceptible; Fischer 344 and ACI rats show intermediate susceptibility, and Copenhagen rats are essentially completely resistant even to direct application of DMBA to the gland (Isaacs 1986). Copenhagen rats did develop fibrosarcomas in response to parenteral DMBA. In contrast, tumor induction by diethylstilbestrol (DES) is demonstrable in the ACI but not in the SD strain of rats, although a co-carcinogenic effect of DES with DMBA can be shown in SD rats (Boylan and Calhoon 1983; Rothschild et al. 1987). Both malignant and benign tumors are increased by the combined treatment, but there is a relatively greater increase in benign tumors. In extensive analyses comparing DMBA tumorigenesis, mammary gland growth rate, serum hormone levels, and DMBA:toxicokinetics in female rats of several strains and F1 hybrids between the strains, Isaacs (Isaacs 1986, 1988; van Zwieten 1984) found no major difference that correlated with susceptibility to tumorigenesis. Transplantation studies demonstrated that inherent characteristics of the gland and not of the host animal determine response to DMBA. Glands from rats from a resistant or a susceptible strain were transplanted into F1 hybrids between the 2 strains and directly exposed to DMBA. While similar percentages of glands from the 2 strains developed malignant changes (60% in resistant and 80% in susceptible), macroscopically detectable tumors developed in 70% of susceptible and only in 10% of resistant glands. The result clearly suggests that genetic factors govern the progression from microscopic to macroscopic tumor rather than from normal to histologically malignant epithelium (Isaacs 1988).
Relevance of DCIS in the Rat to Human DCIS
Morphological Features of DCIS in the Rat
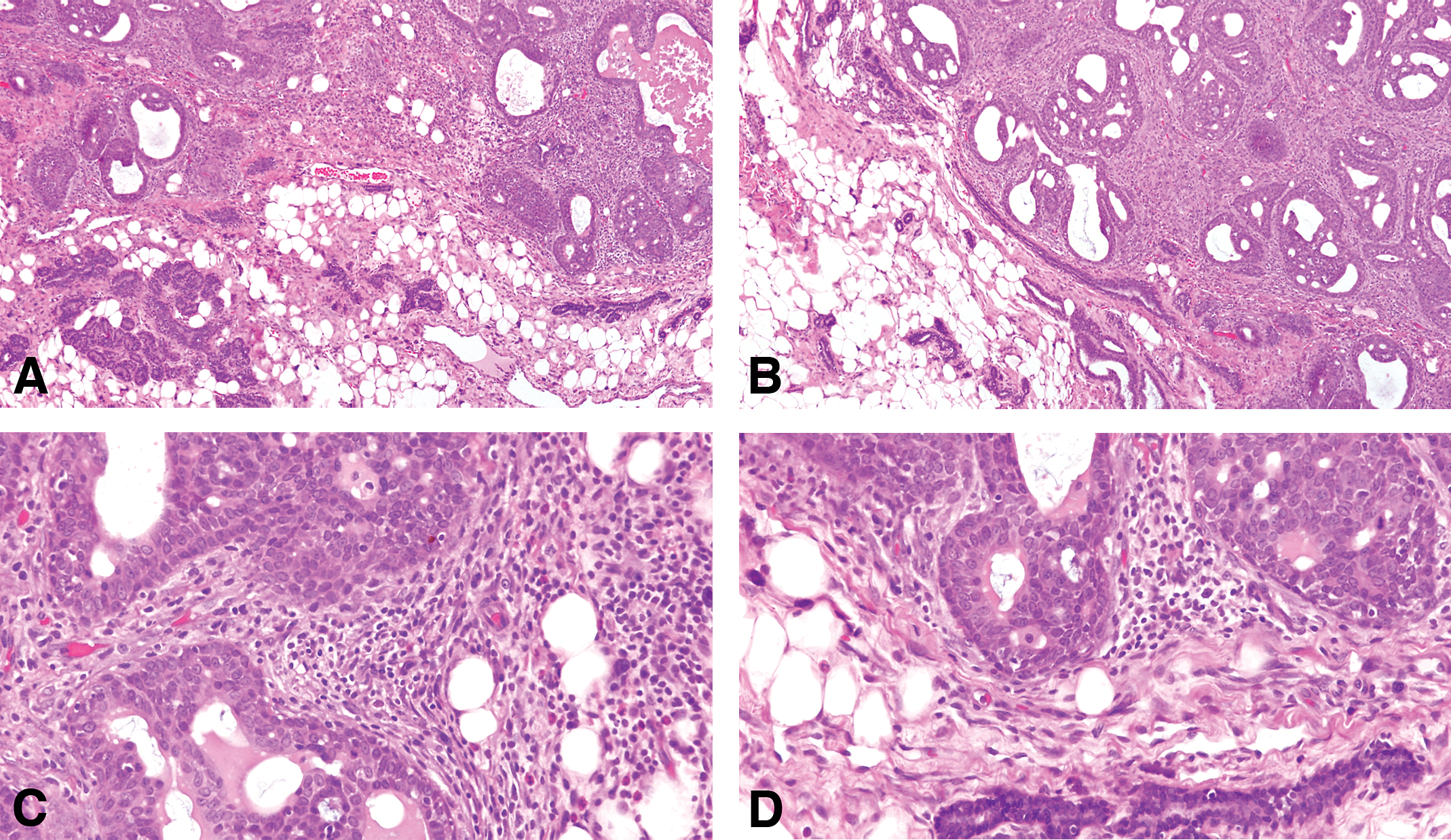
The earliest change observed in the mammary parenchyma after carcinogen treatment of virgin rats is the dilation of terminal ductal structures, namely the TEBs. They exhibit thickening of the epithelial lining, which may be up to 6 layers thick. These cells have a large, round nucleus, prominent nucleolus, and coarse chromatin along the inner leaflet of the nuclear membrane. These early lesions called IDPs; (Russo and Russo 1996; Russo et al. 1977; Figures 5 and 6) represent the transition between the normal TEB (Russo, Tewari, and Russo 1989a, Russo et al. 1990, 1977; Russo, Tay, and Russo 1982; Russo, Wilgus, and Russo 1979) and carcinoma in situ; the criteria for identifying these 3 types of structures are outlined in Table 2 (Russo et al. 1977, 1990; Russo, Tewari, and Russo 1989a; Russo, Wilgus, and Russo 1979; Russo, Tay, and Russo 1982). IDPs appear to evolve into carcinoma in situ through the development of (a) micropapillae, which might be the only pattern present or combined with cribriform pattern; (b) pseudolumina, forming a cribriform pattern; or (c) a comedo pattern. A progressively increasing desmoplastic reaction in the stroma surrounding the transformed ductal structures is a hallmark of neoplastic progression.
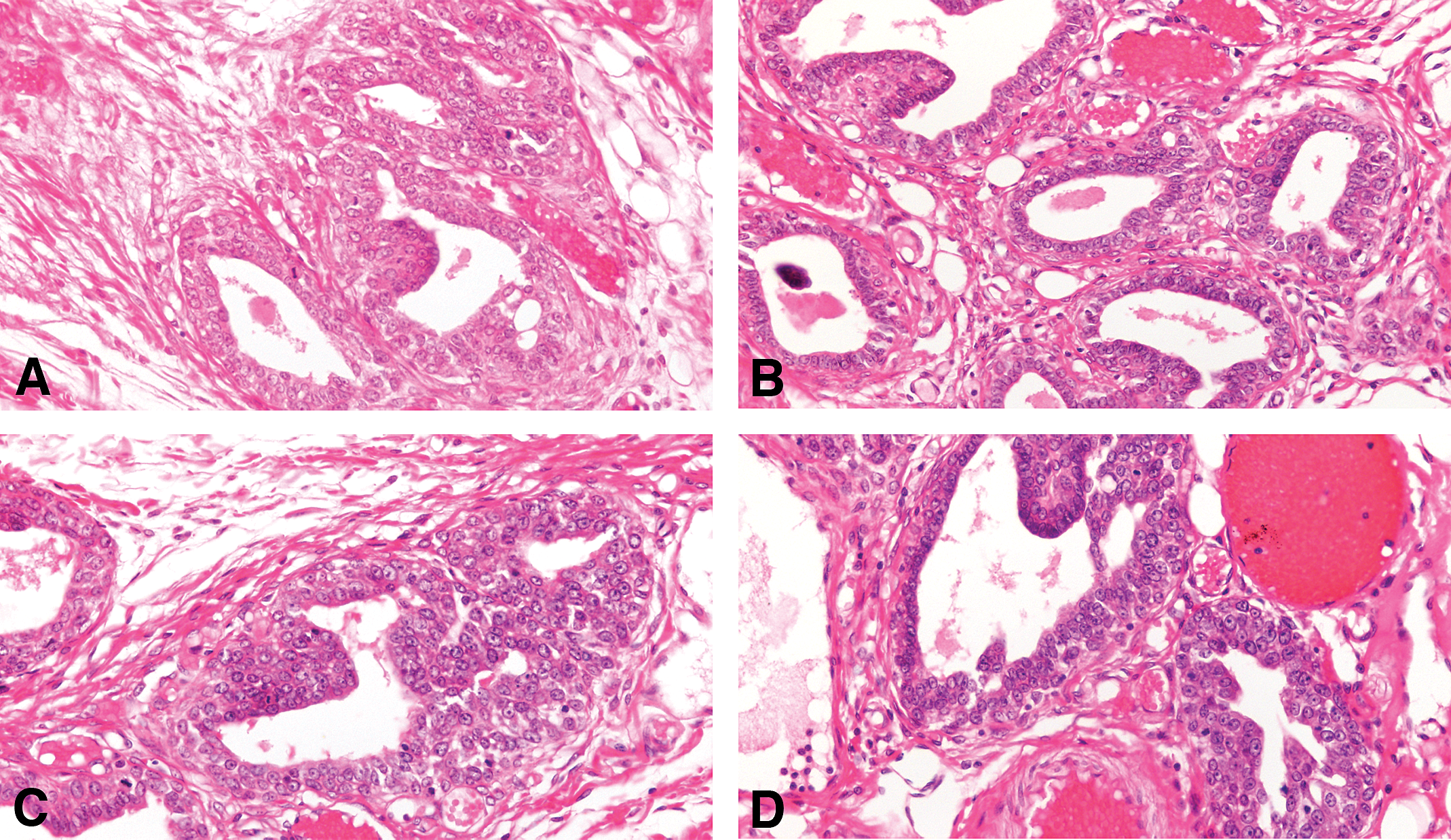
The earliest change observed in the mammary parenchyma after carcinogen treatment of virgin rats is the dilation of terminal ductal structures, namely the TEBs forming the IDP (A, B, C, and D): They exhibit thickening of the epithelial lining, which may be up to 6 layers thick. These cells have a large, round nucleus, prominent nucleolus, and coarse chromatin along the inner leaflet of the nuclear membrane (B, C, and D): Stained with H&E, 20×.
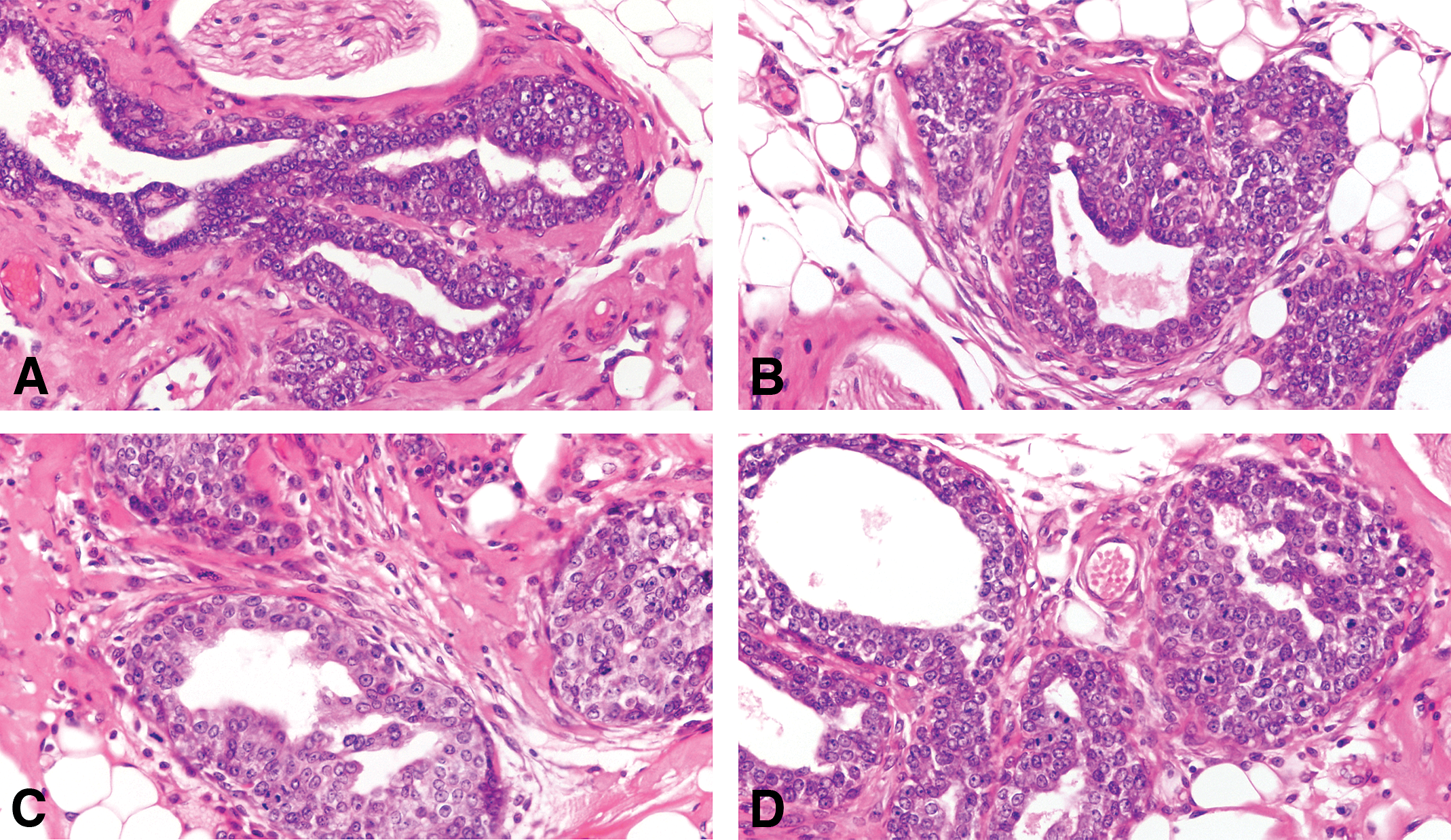
(A and B) The IDPs are early lesions that represent the transition between the normal TEB and carcinoma in situ. (C and D) IDPs appear to evolve into carcinoma in situ through the development of: (a) micropapillae, which might be the only pattern present or combined with cribriform pattern, (b) pseudolumina, forming a cribriform pattern, or (c) a comedo pattern. A progressively increasing desmoplastic reaction in the stroma surrounding the transformed ductal structures is a hallmark of neoplastic progression. Stained with H&E, 20×. IDP = intraductal proliferations.
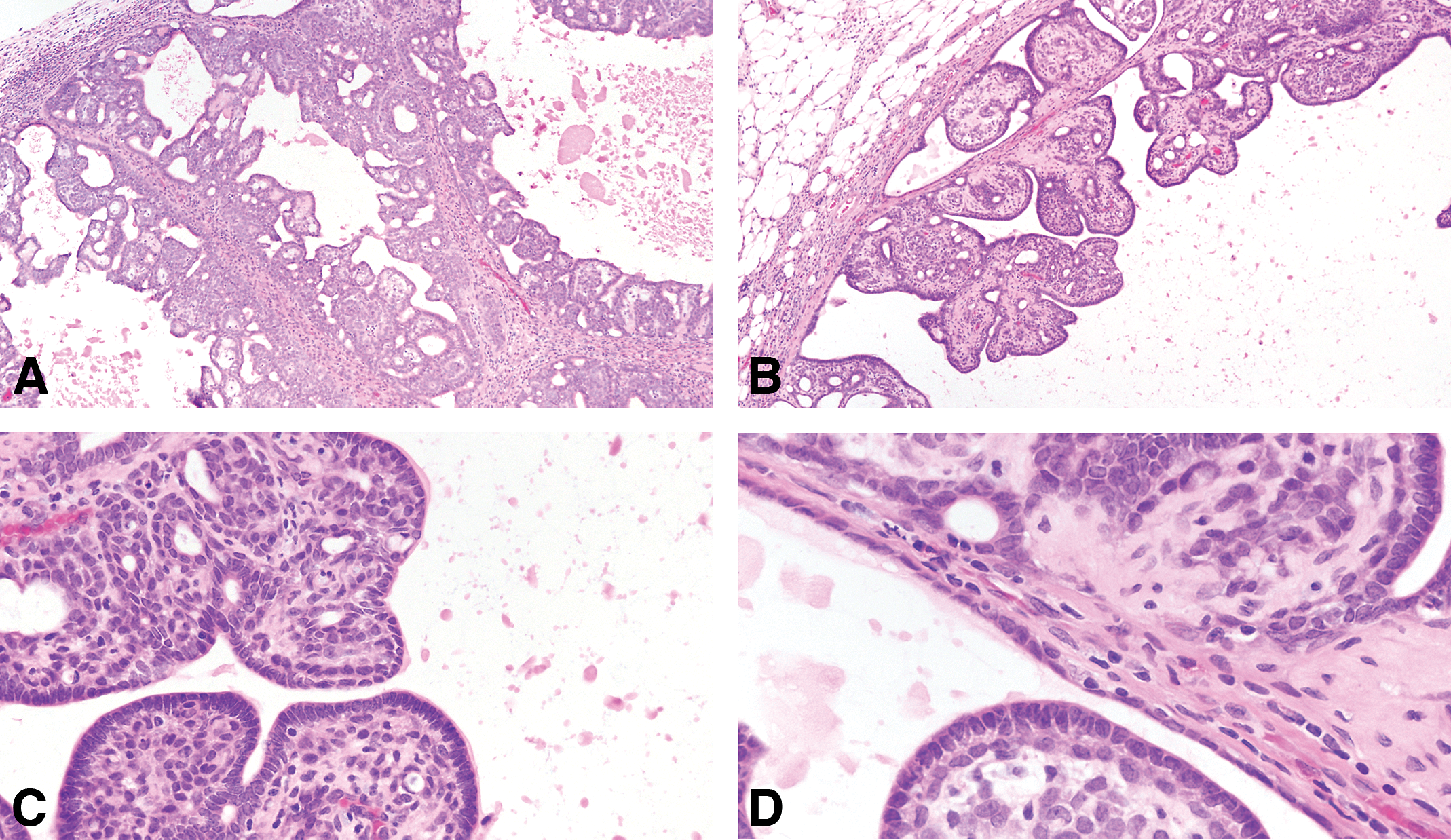
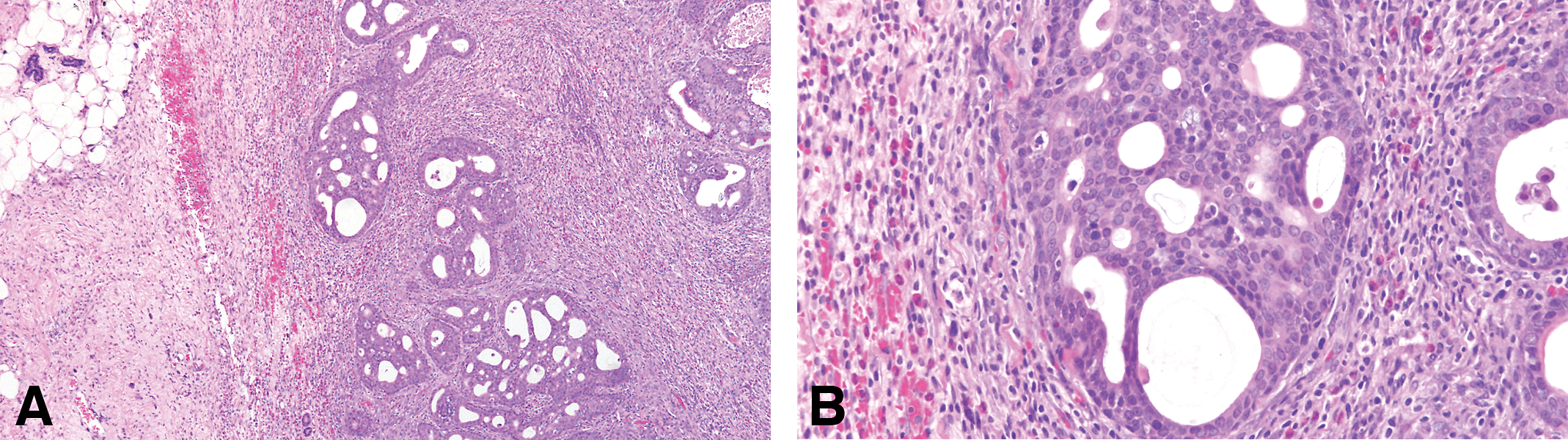
In the intraductal papillary carcinoma (Figure 7A and B), the ductal structures are dilated, and the lining epithelium grows inward, forming epithelial papillae devoid of fibrovascular core. Most of the epithelial cell population is uniform in size and shape. Mitotic figures are often found. The stroma, which is separated from the epithelium by a well-defined basement membrane, exhibits a slight to marked desmoplastic reaction, with replacement of fat by fibroblasts, and infiltration by lymphocytes and mast cells.
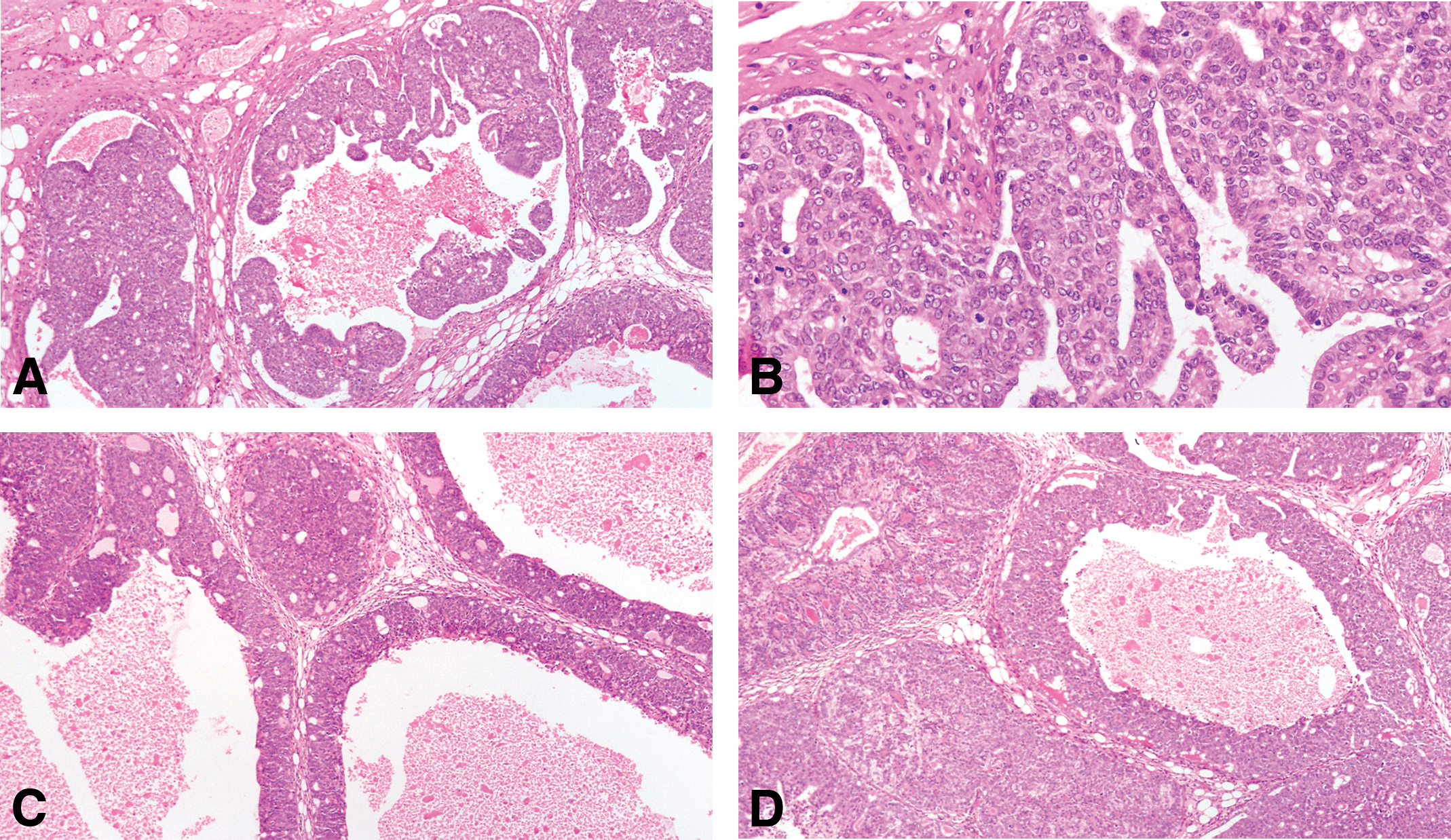
(A and B) In the intraductal papillary carcinoma, the ductal structures are dilated, and the lining epithelium grows inward, forming epithelial papillae devoid of fibrovascular core. Most of the epithelial cell population is uniform in size and shape. Mitotic figures are often found. The stroma, which is separated from the epithelium by a well-defined basement membrane, exhibits a slight to marked desmoplastic reaction, with replacement of fat by fibroblasts, and infiltration by lymphocytes and mast cells. (C and D) The intraductal cribriform carcinoma is the result of epithelial cell proliferation in a solid pattern with formation of’ secondary lumina. The tumors are cytologically similar to papillary carcinomas, and like them, they elicit a stromal reaction and lymphocytic infiltration. Stained with H&E, 20×.
The intraductal cribriform carcinoma is the result of epithelial cell proliferation in a solid pattern with formation of’ secondary lumina (Figure 7C and D). The tumors are cytologically similar to papillary carcinomas and like them; they elicit a stromal reaction and lymphocytic infiltration.
The intraductal ductal comedocarcinoma is characterized by intraductal growth of epithelium and accumulation of necrotic cellular debris in the lumen. This necrotic material is similar to the one observed in the invasive comedocarcinoma (Figure 8). The surrounding stroma may exhibit a marked desmoplastic reaction. Comedo and cribriform patterns may be present simultaneously in the same tumor. Less frequently, a papillary component is present as well.
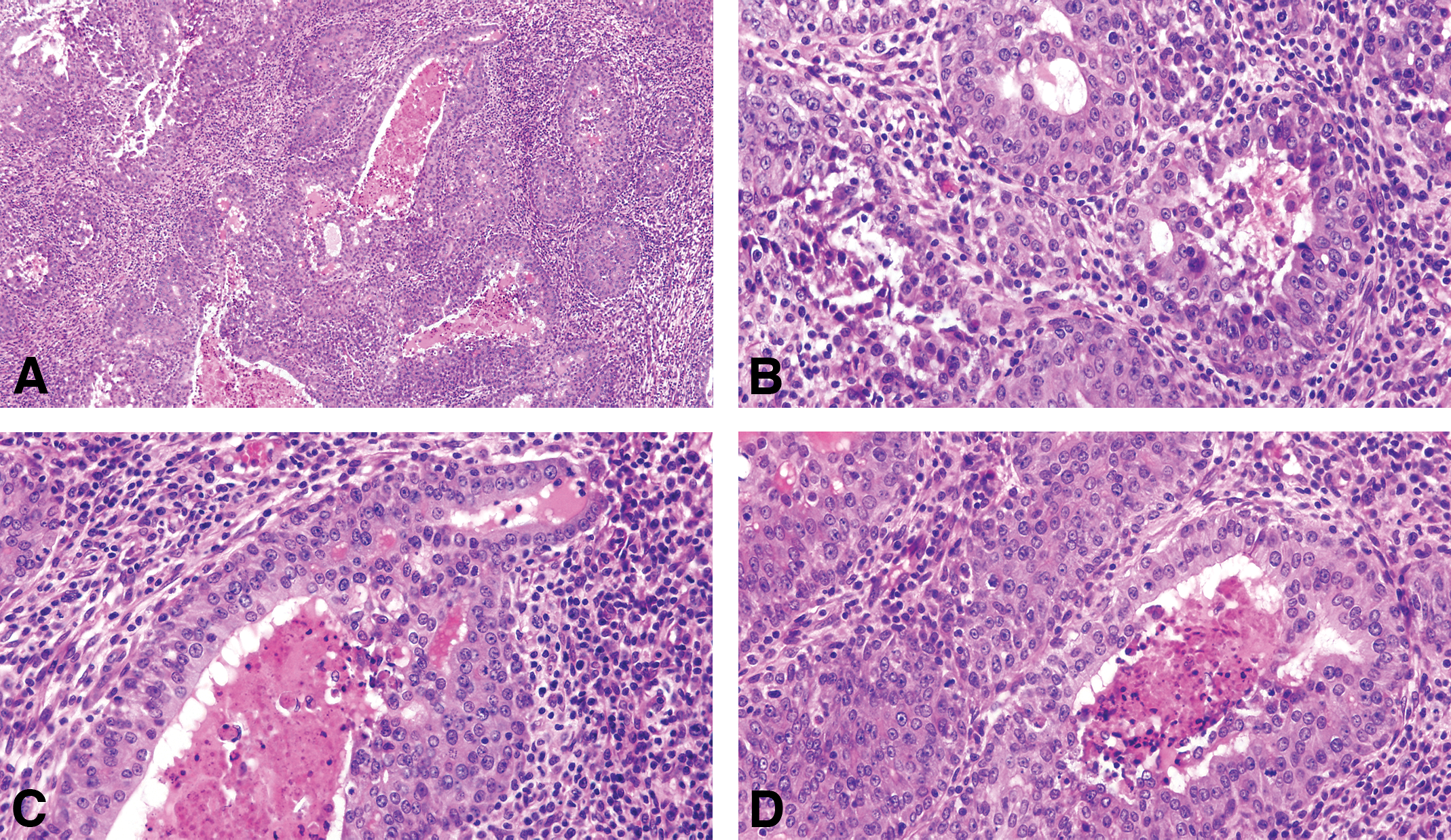
(A) The invasive comedocarcinoma is characterized by intraductal growth of epithelium and accumulation of necrotic cellular debris in the lumen stained with H&E, 4×, (B, C, and D) invasive comedo carcinoma containing the necrotic material similar to the one observed in the non-invasive comedocarcinoma. The surrounding stroma may exhibit a marked desmoplastic reaction as seen in B, C, and D. The invasive comedo carcinomas appear as distended ductal structures lined by a multilayered epithelium surrounding necrotic debris. Invasion occurs as an extension of duct-like structures or sheets of epithelial cells arranged in a serpiginous pattern into a stroma in which desmoplastic reaction and inflammatory cell infiltration may occur. Individual neoplastic cells are pleomorphic. Some of these tumors resemble the comedo carcinoma of the human breast. Stained with H&E, 40×.
Human DCIS or DCIS
DCIS constitutes 30 to 40% of the breast cancer cases diagnosed mammographically, with one case of DCIS detected in every 1,300 screening mammograms (Siziopikou 2013). The architectural subtypes of DCIS are very similar to those described for the rat. However, for clinical purposes, they have been divided into noncomedo and comedo subtypes; noncomedo subtypes were further subdivided into cribriform, micropapillary, solid, and papillary, while the comedo subtype was defined by high-grade cells, prominent central necrosis, and associated pleomorphic microcalcifications (Fitzgibbons, Henson, and Hutter 1998; The Consensus Conference Committee 1997). Additional classification systems have been proposed (European Commission Working Group on Breast Screening Pathology on Breast Screening Pathology et al. 1998; Holland et al. 1994; Scott et al. 1997) accounting the degree of atypia of the nuclei that correlates with clinical outcomes (European Commission Working Group on Breast Screening Pathology et al. 1998; Holland et al. 1994). In this system, the nuclear grade of the DCIS lesions is defined as low grade (grade 1), intermediate grade (grade 2), and high grade (grade 3; Lester et al. 2009). In rats, most of the nuclei are grade 1 or 2, and grade 3 nuclei are rarely observed. Other features like the size (Lester et al. 2009) and the margins (Harris et al. 2004; Schnitt and Collins 2009; Stomper and Margolin 1994) that are important prognostic parameters in human are not relevant in the rat mammary pathology.
Differential Diagnosis
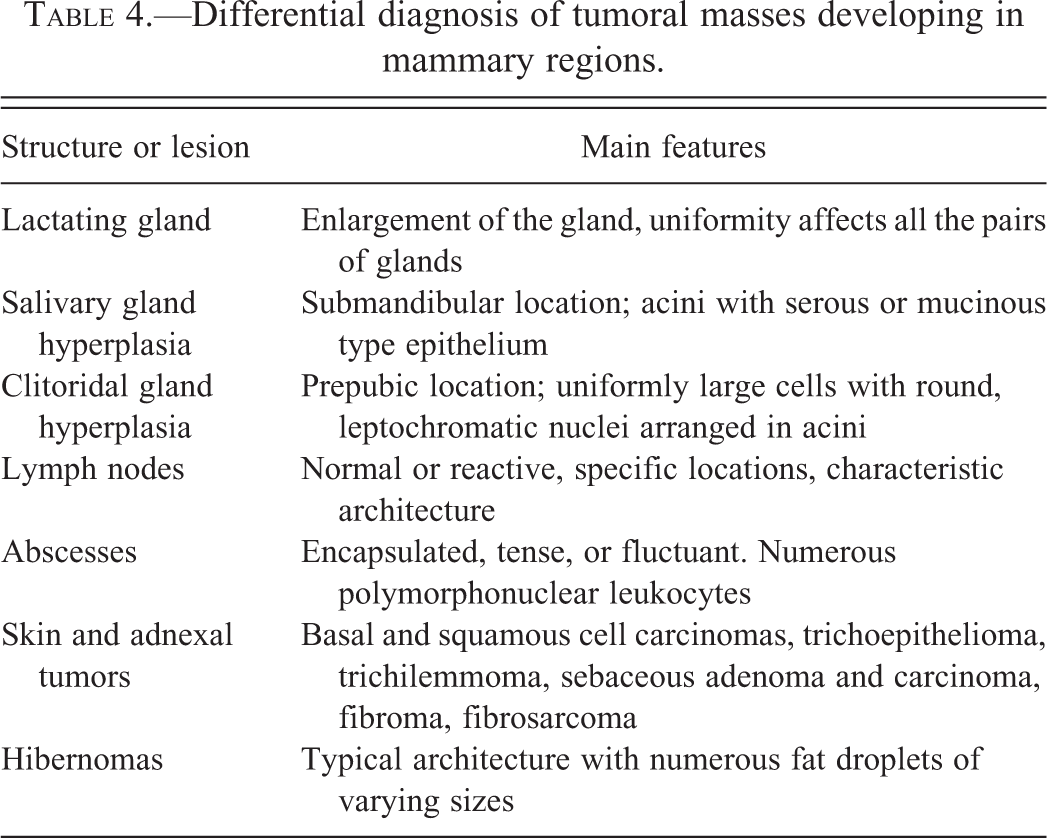
In the human as well as in the rat, the lesions that need to be differentiated with DCIS is the ADH (Page and Anderson 1987; Page et al. 1985; Schnitt and Collins 2009) and occasionally must be differentiated from invasive carcinomas; a frequent such mimicker is invasive cribriform carcinoma that needs to be distinguished mostly from cribriform DCIS (Fisher et al. 1975; Maluf 2004; Yaziji, Gown, and Sneige 2000). The criteria listed in Table 4 can be used in the rat and to a certain extent in the human lesions. An elegant review of DCIS in human has been published (Siziopikou 2013), indicating the most important concerns in the differential diagnosis of DCIS in the human breast are microinvasion around DCIS lesions, extension of a DCIS lesion into adjacent benign structures or foci of sclerosing adenosis, the presence of foci of lymphatic/vascular invasion mimic DCIS lesions, and the comedo-type DCIS lesions often need to be distinguished from the pleomorphic subtype of LCIS lesions (Fulford, Reis-Filho, and Lakhani 2004; Jacobs 2003; Sneige et al. 2002).
Differential diagnosis of tumoral masses developing in mammary regions.
Invasive Carcinoma in the Rat versus the Human
Histopathology of Invasive Carcinoma in the Rat Mammary Gland
The diagnosis of invasive carcinomas is based upon the presence of unequivocal growth of malignant epithelial cells into the adjacent stroma. The presence of invasion can be difficult to judge because under normal conditions the mammary gland ducts grow diffusely into the fat pad, adjacent muscle, and subcutaneous tissue of the skin. The subtypes of invasive lesions found in the rat mammary gland are depicted in Table 1. The histological type more frequently found in a large series of 584 tumors induced by DMBA in the rat mammary gland in our laboratory at the FCCC is provided in Table 3.
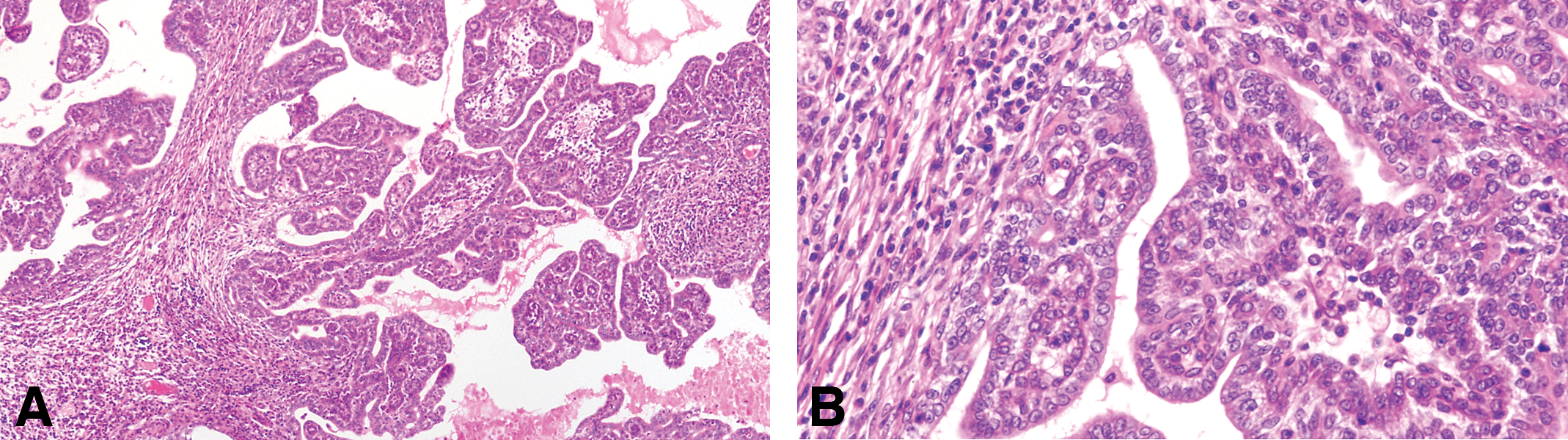
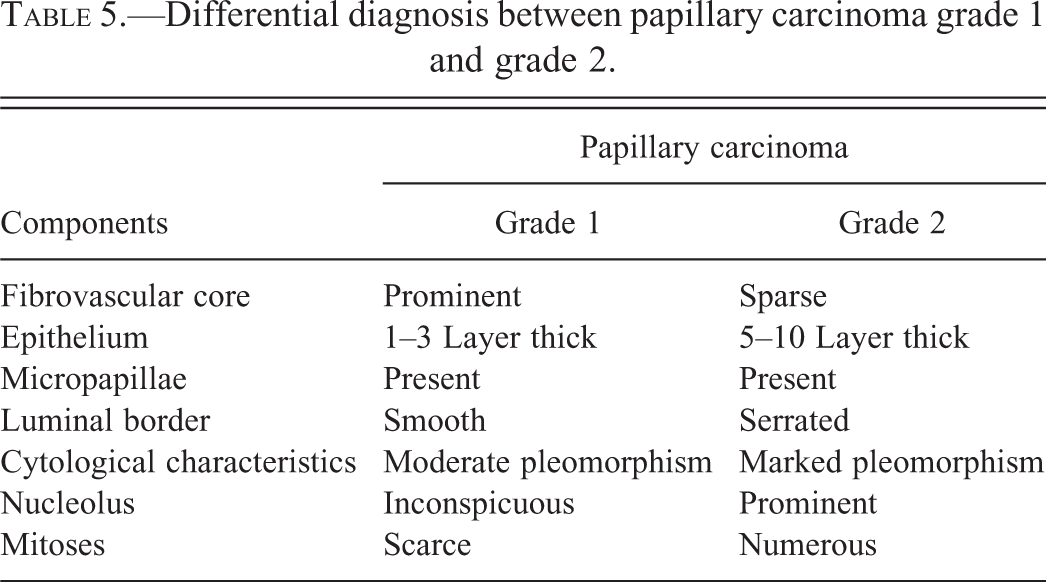
The invasive papillary carcinomas are the most typical and frequent of the DMBA- and NMU-induced tumors in the rat (Russo and Russo 1996; Table 3). Most of the tumors are detectable by palpation; they efface the normal architecture of the gland, invading surrounding structures. When they invade the skin, they ulcerate and undergo local necrosis. Papillary carcinomas contain delicate fibrovascular cores, often heavily infiltrated by lymphocytes and mast cells. The fibrovascular cores are considerably thinner than those seen in intraductal papillomas. On top of the fibrovascular core grows the epithelium, which depending upon its thickness and cytologic characteristics allows one to classify these lesions into grade 1 or grade 2 (Table 5). Papillary carcinomas grade 1 are composed of 1 to 2 layers of epithelial cells, which in turn emit short epithelial papillae devoid of fibrovascular cores (Figures 9 and 10). This type of tumors comprises 5.91% of all the invasive cancers (Table 3). The papillary carcinoma grade 2 is also formed by papillary projections; however, the cores of connective tissue are sparser than those observed in the papillary carcinoma grade 1, and the secondary projections (papillae) of epithelium are solid clusters of cells (Figure 11). The luminal borders of these cell projections are in some occasion serrated, whereas those present in papillary carcinomas grade 1 are smooth (Table 5). The epithelial cells in this tumor type are slightly more pleomorphic than those of the papillary carcinoma grade 1. The basic histological and cytological differences between these tumor subtypes are depicted in Table 5. Occasionally, in papillary carcinomas grade 2, the luminal spaces may become dilated or cystic; these lesions are called cystic papillary carcinomas. They may well represent a further evolution of a papillary or cribriform type. The papillary carcinoma type 2 represents 26.05% of the invasive carcinoma and 23.10% are mixed with papillary carcinoma type 1 (Table 3).
(A) Invasive papillary carcinomas type 1 contain delicate fibrovascular cores, often heavily infiltrated by lymphocytes and mast cells. Stained with H&E, 4×. (B) The fibrovascular cores are considerably thinner than those seen in intraductal papillomas. Stained with H&E, 10×. (C and D) On top of the fibrovascular core grows, the epithelium, which are composed of 1 to 2 layers of epithelial cells, which in turn emit short epithelial papillae devoid of fibrovascular cores. Stained with H&E, 40×.
(A and B) The luminal borders of these cell present in papillary carcinomas grade 1 are smooth. The epithelial cells in this tumor type are less pleomorphic than those of the papillary carcinoma grade 2. Stained with H&E, 4× and 40×, respectively.
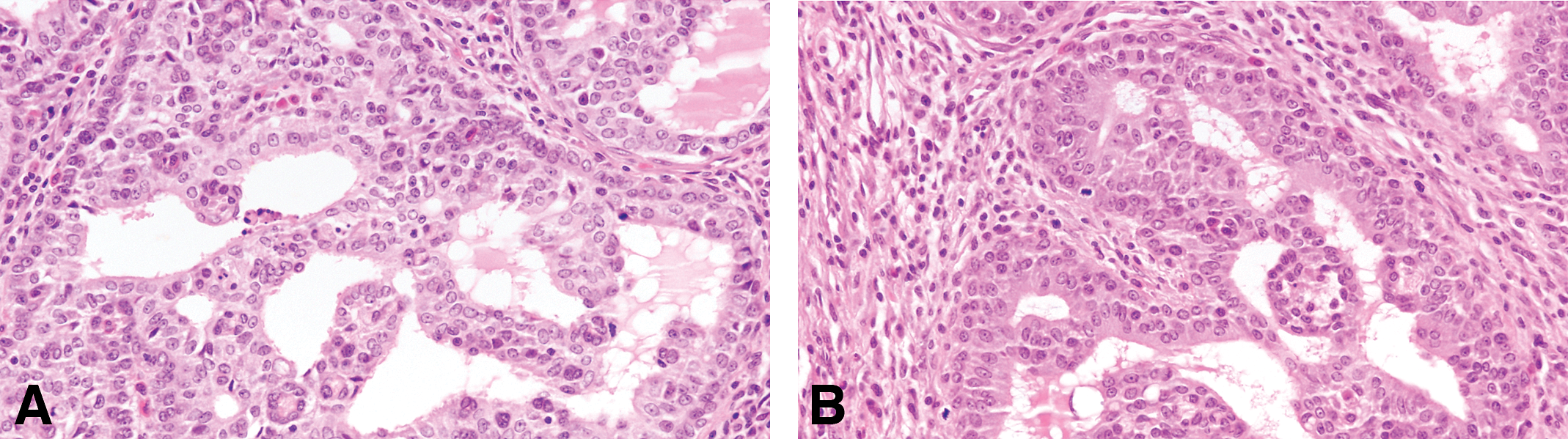
(A and B) Papillary carcinoma grade 2 is formed by papillary projections; however, the cores of connective tissue are more sparse than those observed in the papillary carcinoma grade 1, and the secondary projections (papillae) of epithelium are solid clusters of cells. The luminal borders of these cell projections are in some occasion serrated. The epithelial cells in this tumor type are pleomorphic, Stained with H&E, 40×.
Differential diagnosis between papillary carcinoma grade 1 and grade 2.
The invasive cribriform carcinoma (Figures 12 –16) exhibits the same cellular arrangement as the in situ lesions in which the solid sheets of neoplastic epithelial cells are interrupted by round or irregularly shaped secondary lumina of variable size. Invasion is characterized by penetration of haphazardly arranged, finger-like projections of epithelium into the surrounding stroma (Figures 15 and 16). The cribriform pattern may be maintained even in small clusters of cells infiltrating the dermis, skeletal muscle, and connective tissue, as well as in metastatic lesions (Figure 16A and B). Individual neoplastic cells are moderately to markedly pleomorphic. The degree of pleomorphism varies from tumor to tumor and even in different areas of the same tumor. Interestingly enough, even in the most pleomorphic tumors the glandular pattern is still present, with secretory material within the newly formed lumina (Figure 14). The infiltrating neoplastic cells are in general surrounded by a connective tissue that exhibits a marked desmoplastic reaction, with heavy lymphocytic and mast cell infiltrations (Figures 12 and 13). The cribriform type of tumor appears in general as a uniform pattern, but it may be associated with papillary or comedo patterns in the same tumor. The invasive cribriform carcinomas represent 27.05% of the mammary cancers in the rat (Table 3).
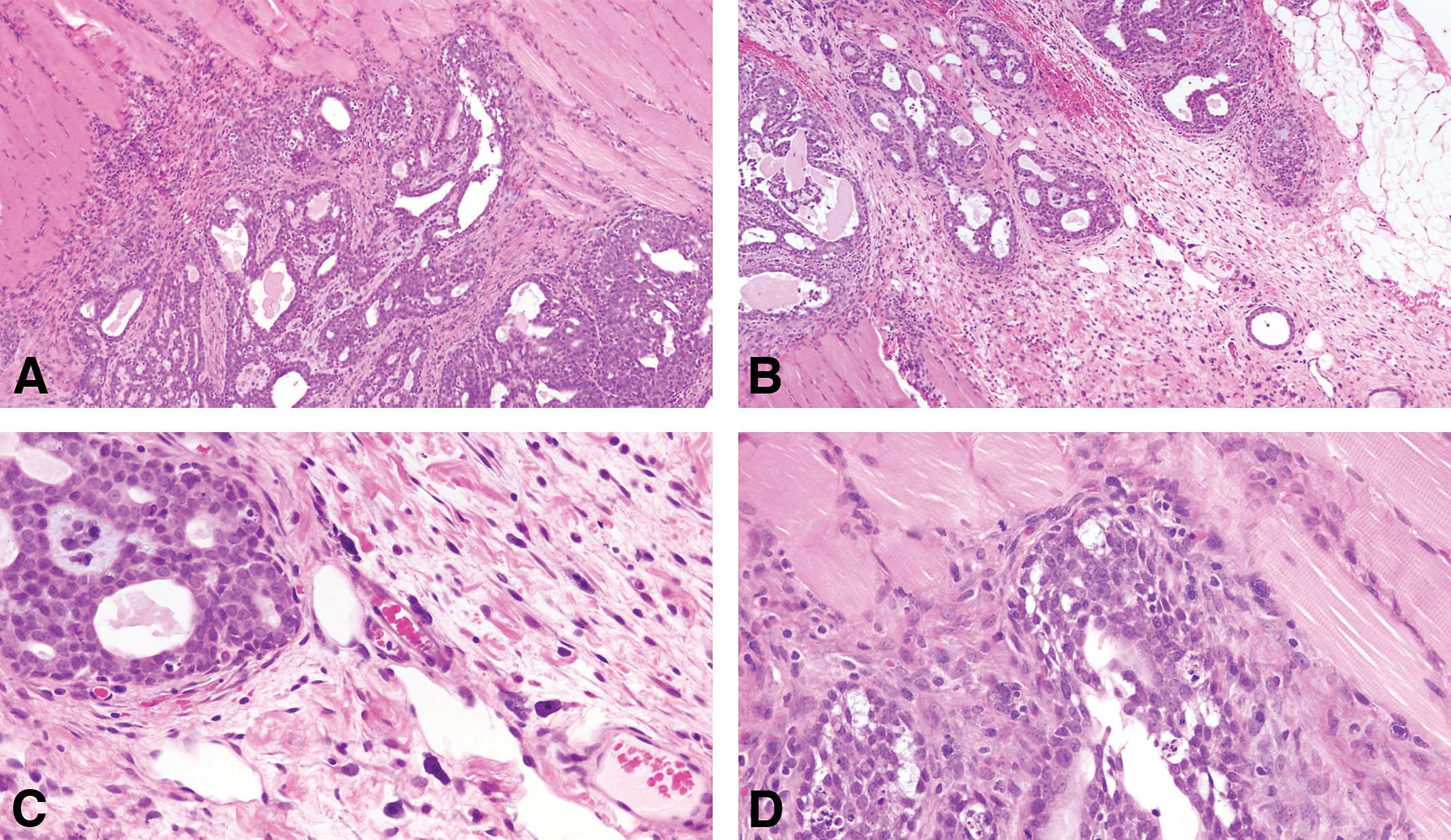
(A and B) The invasive cribriform carcinoma exhibits the same cellular arrangement as the in situ lesions in which the solid sheets of neoplastic epithelial cells are interrupted by round or irregularly shaped secondary lumina of variable size. Stained with H&E, 4×. (C and D) The cluster of neoplastic cells invading the stroma are surrounded by a profuse inflammatory response. Stained with H&E, 20×.
(A and B) In the invasive cribriform, the invasion is characterized by penetration of haphazardly arranged, finger-like projections of epithelium into the surrounding stroma. (B) The cribriform pattern may be maintained even in small clusters of cells infiltrating the dermis, skeletal muscle, and connective tissue, as well as in metastatic lesions. Stained with H&E, 4× and 40×, respectively.
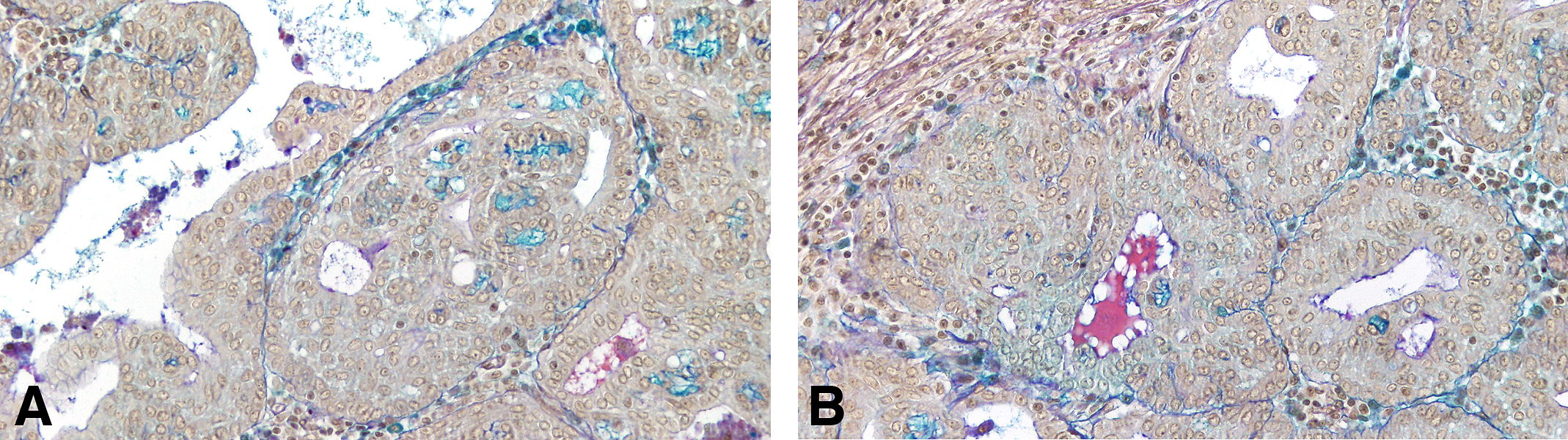
(A and B) In the invasive cribriform carcinoma even in the most pleomorphic tumors, the glandular pattern is still present, with secretory material within the newly formed lumina. Formation of intercellular spaces shows Alcian blue and PAS positive reaction identified as proteoglycans. Deposition of proteoglycans around a carcinoma in situ, and around mast cells is also observed. Stained with Alcian blue and PAS, 10×. PAS = periodic acid–Schiff stain.
(A and B) Cribriform carcinoma invading the muscle wall. Stained with H&E, 4×. (C and D) Neoplastic cells are moderately to markedly pleomorphic. The degree of pleomorphism varies from tumor to tumor and even in different areas of the same tumor. Stained with H&E, 40×.
(A and B) The infiltrating neoplastic cells are, in general, surrounded by a connective tissue that exhibits a marked desmoplastic reaction, with heavy lymphocytic and mast cell infiltrations. The cribriform type of tumor appears, in general, as a uniform pattern, but it may be associated with papillary or comedo patterns in the same tumor. Stained with H&E, 40× and 4×. (C and D) The tumor cells are surrounded by lymphocytes in the invasive areas to the muscle wall. Stained with H&E, 40×.
The invasive comedo carcinomas (Figure 8) represents only 0.95% of the invasive cancer and are more frequently found in animals that have been treated with chemical carcinogens at a young age. The lesions appear as distended ductal structures lined by a multilayered epithelium surrounding necrotic debris. Invasion occurs as an extension of duct-like structures or sheets of epithelial cells arranged in a serpiginous pattern into a stroma in which desmoplastic reaction and inflammatory cell infiltration may occur. Individual neoplastic cells are pleomorphic. Some of these tumors resemble the comedo carcinoma of the human breast (Figure 8B–D; Fisher et al. 1975).
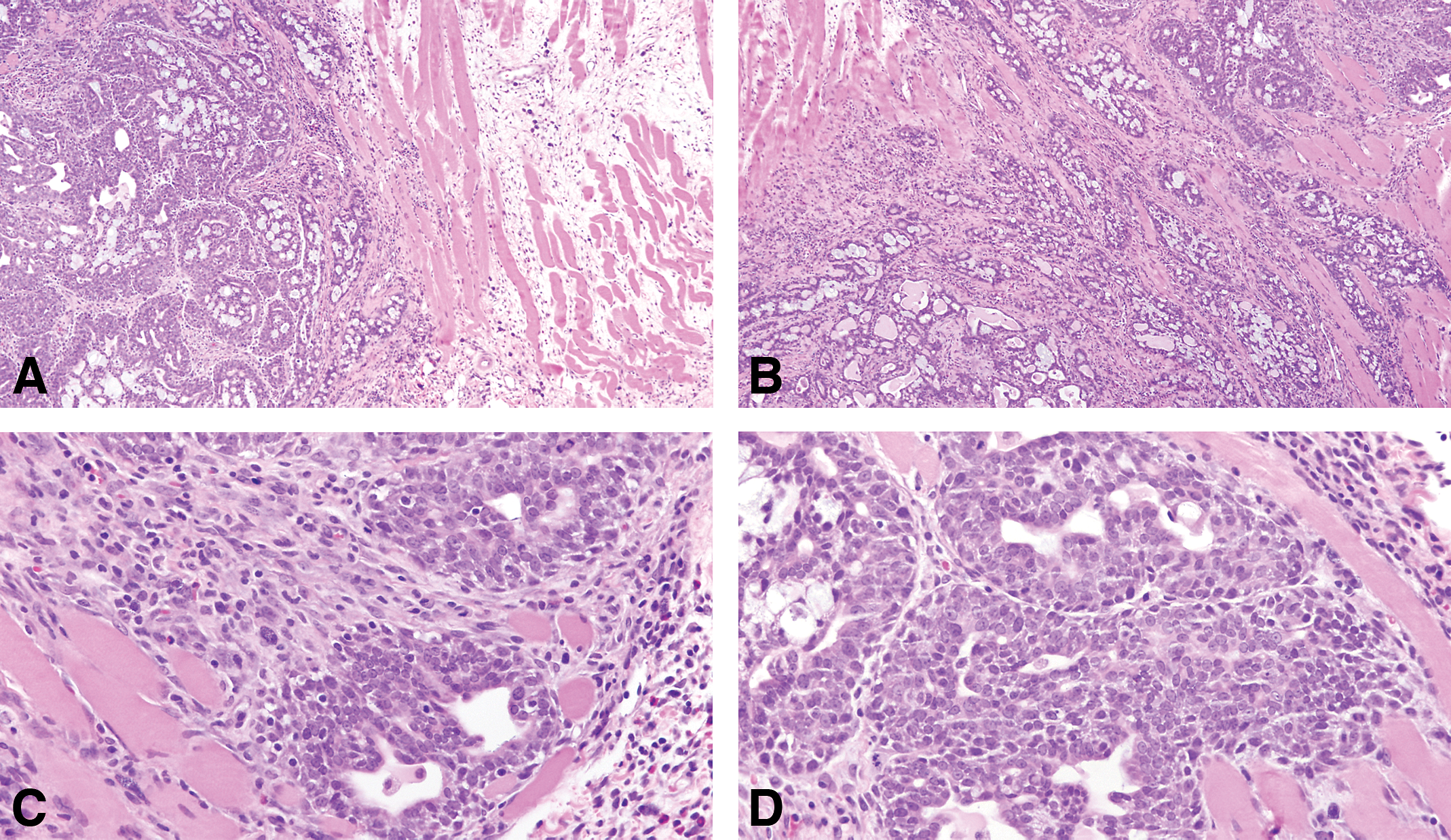
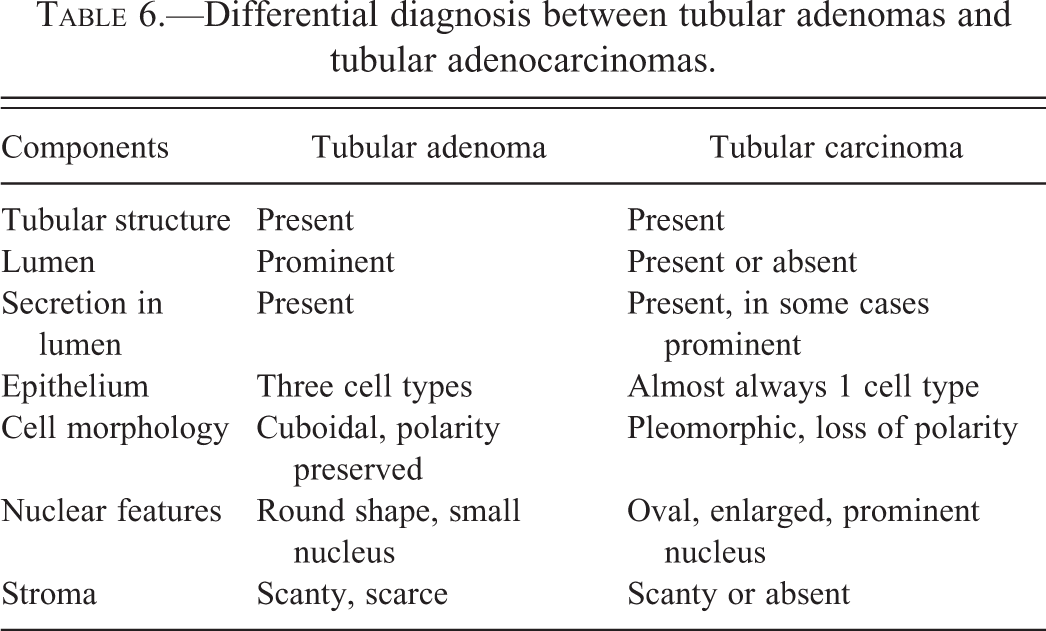
The invasive tubular carcinomas are composed of tubular or alveolar structures but are more irregular in the invasive areas forming distorted glandular structures in the areas of invasion surrounded by desmoplastic reaction (Figure 17). Some of them present scanty secretory material. These lesions could be derived from adenomas. Several transitional steps between adenomas and fully manifest carcinomas are found, which in some cases makes it difficult to differentiate one from the other. Tubular carcinomas, however, differ cytologically enough from tubular adenomas to allow their identification (Table 6). The epithelial cells composing the tubular carcinoma have increased nuclear size, and the nuclei contain prominent nucleoli; tubular adenomas (Figure 17), on the other hand, have cells with smaller nuclei, and nucleoli are absent or inconspicuous. Tubular carcinomas represent 6.67% of the invasive lesions in the rat mammary gland (Table 3).
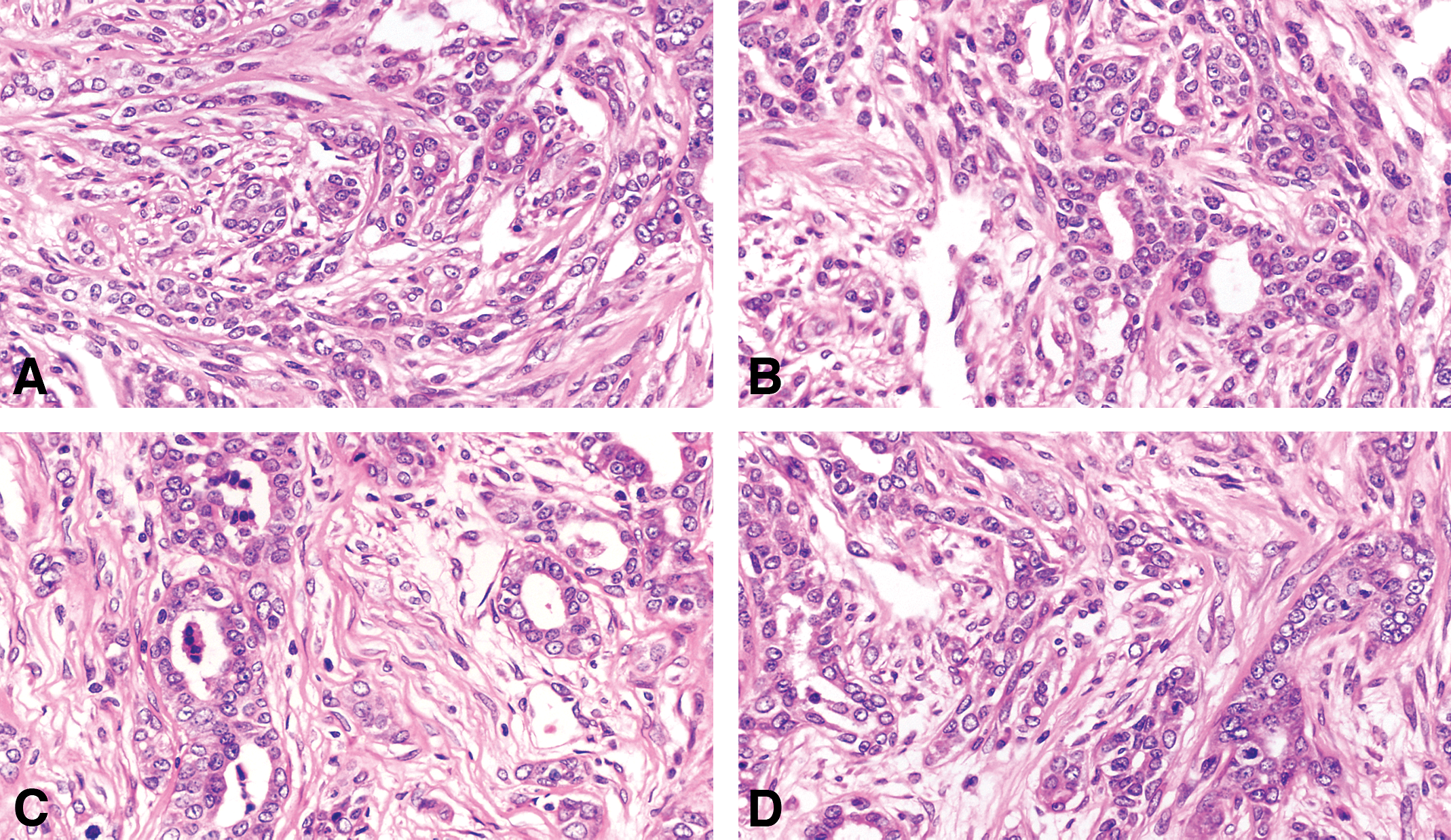
(A, B, C, and D) The invasive tubular carcinomas are composed of tubular or alveolar structures but are more irregular in the invasive areas forming distorted glandular structures in the areas of invasion surrounded by desmoplastic reaction. The epithelial cells composing the tubular carcinoma have increased nuclear size, and the nuclei contain prominent nucleoli. Stained with H&E, 40×.
Differential diagnosis between tubular adenomas and tubular adenocarcinomas.
Ten percent of the invasive cancers in the rat mammary glands are the adenoid cystic type that (Figure 18), is characterized by a biphasic cellular pattern of myoepithelial and epithelial cells surrounded by a lightly eosinophilic stroma. In the human is a rare basal-like breast cancer (Kreike et al. 2007; Marchio, Weigelt, and Reis-Filho 2010; Weigelt et al. 2008). In the rat, this tumor has the same markers as the luminal type.
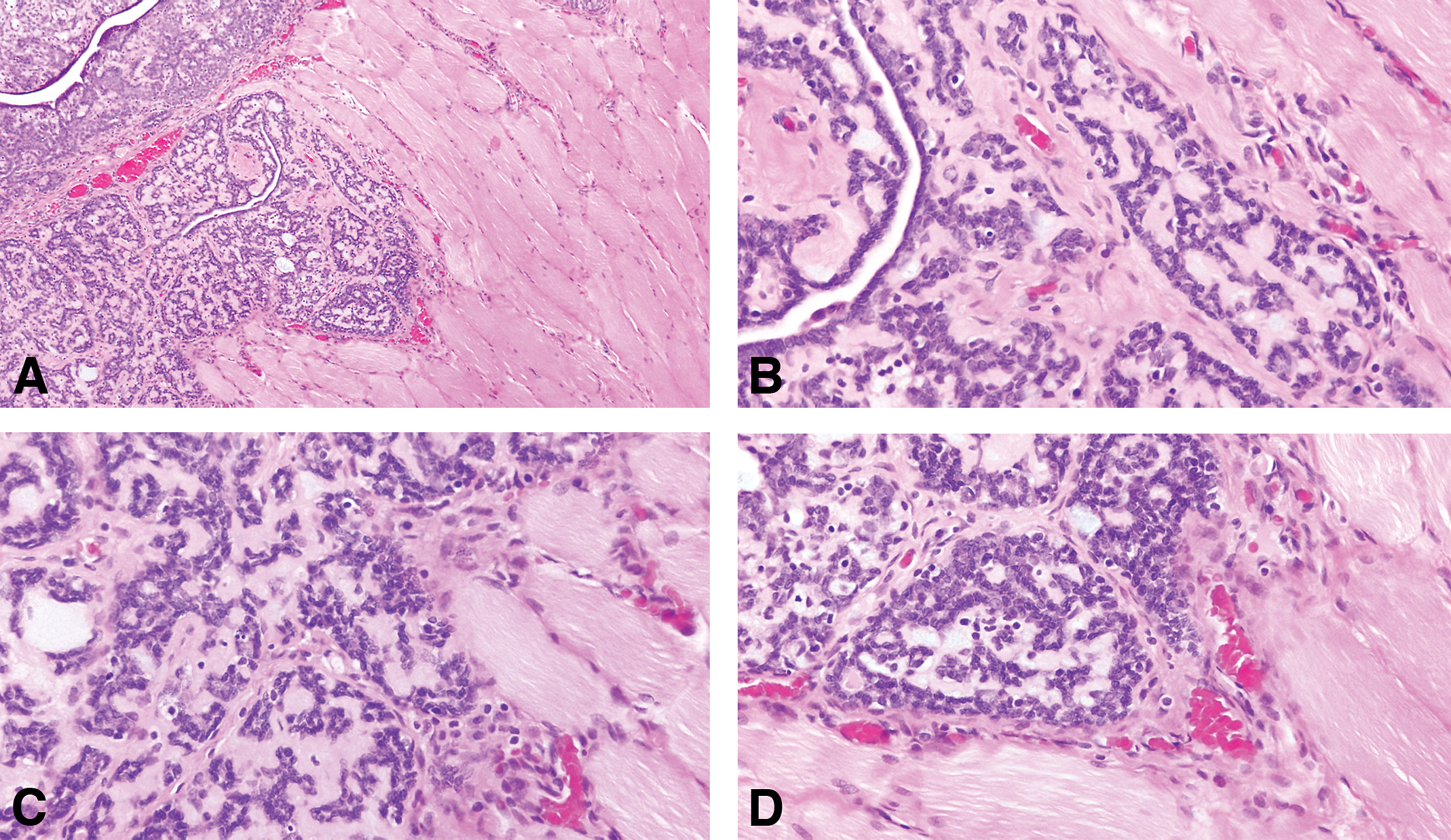
(A) Invasive adenoid cystic type stained with H&E, 4×. (B, C, and D) The tumor is characterized by a biphasic cellular pattern of myoepithelial and epithelial cells surrounded by a lightly eosinophilic stroma. Stained with H&E, 40×.
Stromal Neoplasms
The stromal tumors in the rat are very similar to those described in human (Table 1), among them are fibromas well-circumscribed and nonencapsulated tumors composed of proliferating fibroblasts arranged in interlacing bundles and embedded in variable amounts of collagen fibers. In some tumors, there are isolated remnants of glandular epithelium, which suggests that they originate from FAs (Figure 19). The malignant counterpart is the fibrosarcoma composed of malignant fibroblasts exhibiting the expected anaplastic characteristics and increased number of mitoses are the essential components of fibrosarcomas.
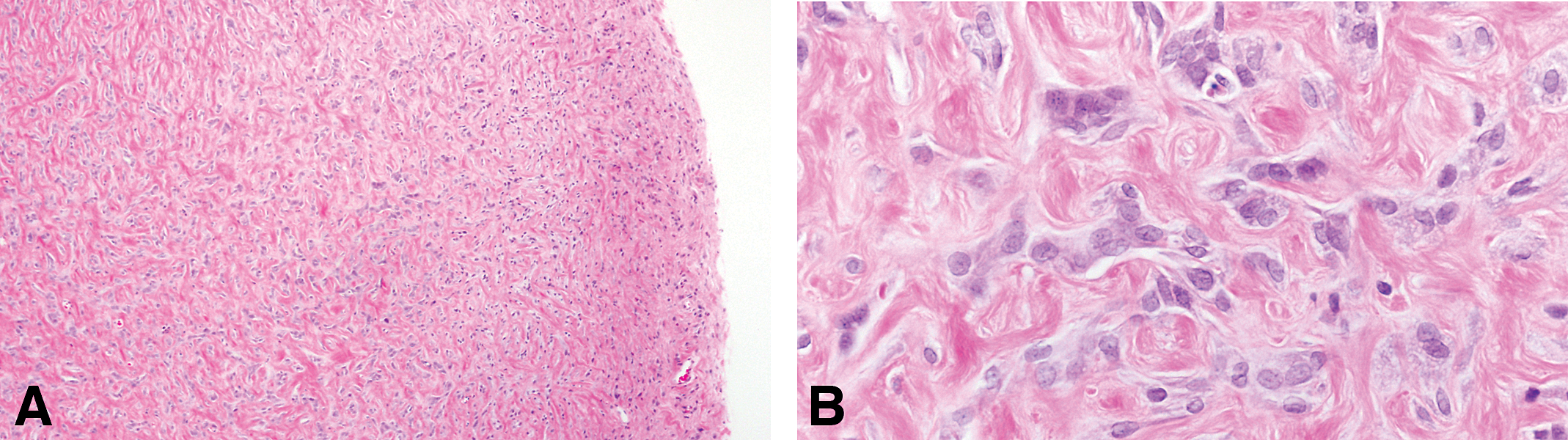
(A) Fibromas well-circumscribed and nonencapsulated tumors composed of proliferating fibroblasts arranged in interlacing bundles and embedded in variable amounts of collagen fibers. (B) In some tumors, there are isolated remnants of glandular epithelium, which suggests that they originate from fibroadenomas. Stained with H&E, 4× and 40×, respectively.
A combination of epithelial and stromal components are often found in the rat, mainly FAs that were described more in detail in a previous section due to their predominance in the rat pathology. The carcinosarcomas is a rare entity, with malignant characteristics in both the epithelium and the stroma. The epithelial component varies from well-differentiated tubular structures to poorly demarcated and elongated cells, which are difficult to differentiate from neoplastic stromal cells. The specific markers keratin, myoglobin, desmin, and vimentin are useful for separating spindle-shaped epithelial cells from the stromal component. Nuclei vary in size and shape, and giant, multinucleated cells may be found. Mitoses are common in both the epithelium and the stroma.
Nonneoplastic Lesions
Among the nonneoplastic lesions in the mammary gland, cystic changes are the ones most frequently found. Cysts can originate from either ductal or lobular elements. Those derived from ducts exhibit a 10- to 100-fold increase in the normal diameter of the duct. They are lined by flat, cuboidal epithelial cells, and have myoepithelial cells that are compressed against the basement membrane. Duct ectasia or galactocele are characterized by the accumulation within the lumen of eosinophilic granular material composed of lipids and protein secretion. Crystals similar to cholesterol and focal calcifications are common.
Lobular cysts are characterized by a grape-like configuration. The small cystic dilatations can be confluent, forming 1 large cyst lined by low cuboidal epithelial cells, although some may contain cells with large vacuoles and decapitation of the apical portion of the cytoplasm. The nuclei are, in general, round or oval and are compressed against the basement membrane.
Differential Diagnosis of Mammary Tumors
Although a common practice for evaluating the tumorigenic response of the rat mammary gland to carcinogens is the quantization of palpable tumors, it is important to keep in mind that palpable lesions are lumps or swellings whose nature can be determined only through histologic examination. Normal organs, nonneoplastic lesions, and tumors of nonmammary origin that under gross examination can be confused with mammary tumors are listed in Table 4. Whether spontaneous or carcinogen-induced rat mammary tumors are benign or malignant can be determined by criteria derived from gross examination (macroscopic criteria), histopathologic examination, and analysis of the biological behavior of the tumor (Table 7).
Criteria of malignancy in mammary tumors.
The 2 major criteria to be taken into consideration upon gross examination of a tumor are its rate of growth and macroscopic appearance (Table 7). Generally, malignant tumors tend to grow faster; however, some exceptions to this rule are observed. We have also found that tumors in the mammary glands located in the thoracic region grow faster than those arising in glands located in the abdominal region (Russo and Russo 1996). The gross appearance of carcinomas is generally soft and fleshy. They are well vascularized and contain areas of necrosis and hemorrhage. Some tumors have cysts containing blood and necrotic material. FAs, on the other hand, are white, with a rubbery and firm consistency, and they shell out from their capsule when they are sectioned. Carcinomas can be firm if they have elicited an intense desmoplastic response.
Among the criteria of malignancy, the most important one is the loss of the tubular–alveolar pattern of the normal mammary gland, a pattern maintained in the adenomas and FAs (Table 7). Cytologically, malignant cells are larger than their normal counterparts and have an increased nucleocytoplasmic ratio. The enlarged nuclei contain coarse chromatin and more prominent nucleoli. The epithelial heterogeneity expressed by the normal gland, or even by benign lesions, in which at least myoepithelial, dark, and intermediate or clear cell types are identified, is rarely observed in malignant lesions (Russo and Russo 1996). The predominant cell in malignancy is the intermediate type, dark cells are rarely observed, and very few myoepithelial cells remain, especially in the invasive lesions. The number or mitoses is generally higher in malignant lesions than in benign ones. Finally, the invasion of the stroma and neighboring tissues, such as muscle and dermis, is a hallmark of malignant tumors. The stromal response to invasion, as demonstrated by fibrosis and inflammatory infiltration, is generally more prominent in the malignant lesions than in the noninvasive or benign ones.
The most reliable criterion of malignancy is the ability of a tumor to metastasize to distant organs, such as lymph nodes or lungs. Very few authors report the finding of metastases from either spontaneous or experimentally induced rat mammary tumors. This lack of metastasizing ability of rat tumors could be attributed to the short period of time that treated animals have been followed in most studies, since only when the study is prolonged for 2 or 3 years, essentially the whole life span of the animal, do metastases become evident. The histopathologic type of a tumor does not seem to affect its metastasizing ability, since it has been found that cribriform, comedo, or papillary carcinomas produce metastases with similar frequency (Russo and Russo 1996). Transplantability is considered another reliable criterion of malignancy in the mammary gland tumors of the rat. The ability of neoplastic lesions to elicit angiogenesis has been postulated to be a biological marker of malignancy, but it has not been extensively used (Brem, Jensen, and Gullino 1978; Maiorana and Gullino 1978; Russo et al. 1990).
Biological Importance of the Chemical Carcinogen-induced Rat Mammary Tumor Model
The DMBA rat mammary model has been able to demonstrate that the carcinogen acts on the intermediate cell of the TEB and that this structure is the one that evolves to IDP and carcinoma in situ. There are several factors that regulate the susceptibility of the TEB; some of them are (a) topographic location of the mammary gland, (b) age of the animal, and (c) reproductive history. The high proliferative activity of the TEB is associated with higher binding of the carcinogen, and its short Tc makes them less likely to repair the DNA damaged by the carcinogen. Even though most of the TEBs are transformed to IDPS, not all of them evolve to carcinomas. The regulatory mechanism of this process is more complex due to intrinsic properties of the TEB. We have observed that IDPs progressing to carcinomas, secrete proteoglycans, and attract lymphocytes and mast cells, emphasizing the importance of the interaction of the initiated cells with the host as a mechanism in the progression of the disease. It is clear that the understanding of the mechanisms that modulate the progression of an IDP to a carcinoma will not only further our knowledge and understanding of carcinogenesis, but will also provide the tools for the prevention of the disease, as a result of the development of strategies for stopping the progression of initiated cells to fully manifested malignancy (Russo and Russo 1996).
Molecular Classification of Human Breast Cancer and Its Counterpart in the Rat
The use of gene expression microarray technology has introduced a new classification based on molecular signatures (Perou et al. 2000; Sorlie et al. 2003; van ’t Veer et al. 2003; West et al. 2001) and allowed for the identification of 4 groups with distinct molecular features of mammary cells (estrogen receptor positive/luminal like, basal-like, HER2/neu positive, and normal breast; Table 8). The tumors were classified into basal-like, HER2/neu overexpressing, luminal-like types, and normal breast tissue–like subgroup. The normal breast tissue–like subtype originally proposed has since been recognized as probably arising from normal-tissue contamination (Perou et al. 2000; Sorlie et al. 2003; van ’t Veer et al. 2003; West et al. 2001). The most well-characterized and widely accepted molecular subtypes are the luminal A, luminal B, HER2/neu, and basal-like types. The basal-like subtype commonly displays a triple-negative phenotype often defined by a lack of estrogen receptor and progesterone receptor protein expression, with an absence of HER2/neu overexpression (Diaz et al. 2007; Foulkes et al. 2003; Livasy et al. 2006; Luck et al. 2008; Millikan et al. 2008; Peppercorn, Perou, and Carey 2008; Rakha and Reis-Filho 2009; Rakha, Reis-Filho, and Ellis 2008; Rakha et al. 2009; Turner and Reis-Filho 2006; Turner et al. 2007). Similarly, luminal A, luminal B, basal-like, and HER2/neu subtypes of DCIS were described (Bryan, Schnitt, and Collins 2006; Livasy et al. 2007).
Molecular subtypes of breast cancer.

Adapted from Gruver, Portier, and Tubbs (2011).
Using 3 markers, ER, PgR, and HER2/neu (Table 9; Figures 20 and 21), we have reclassified the mammary tumors in the rat. The ER and PgR were evaluated according to the Allred’s criteria (Allred et al. 2002). The expression of HER2 was evaluated by manual tracing of the tumor areas and run by Aperio Image Membrane Algorithm. They were evaluated as negative (−) weakly positive (+), moderate positive (++) when some spots were reacted in the cell membrane, and 3+ was defined as a circumferential membrane staining that is complete, intense, and within >10% of tumor cells. These kinds of tumors were defined as HER2 positive (Wolff et al. 2013).
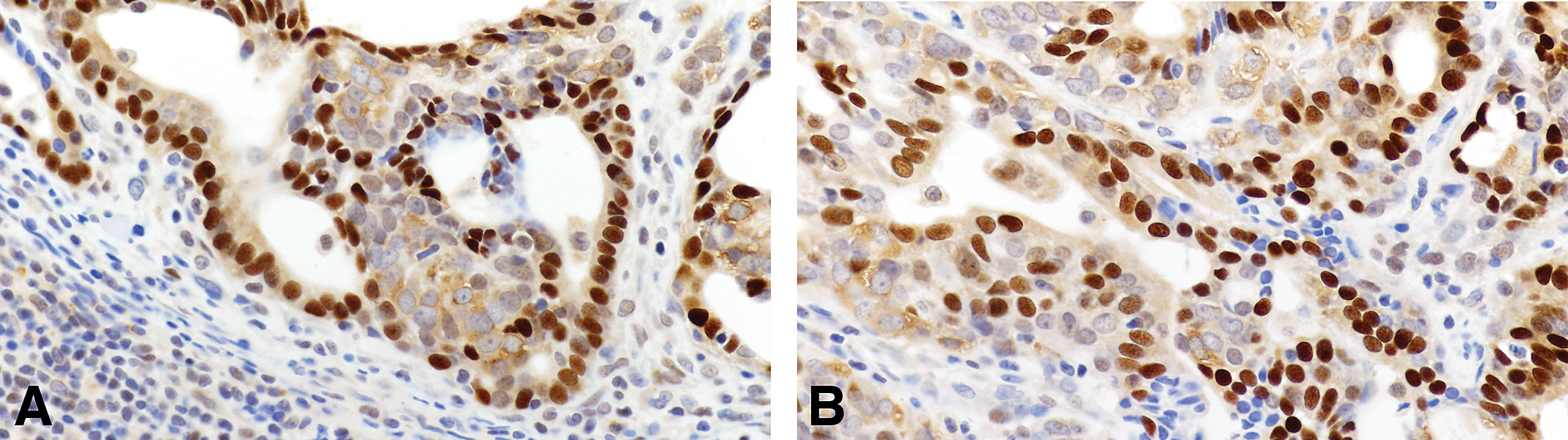
Invasive carcinoma of luminal type A containing positive cells for ER(A) and Pg R(B) 40×.
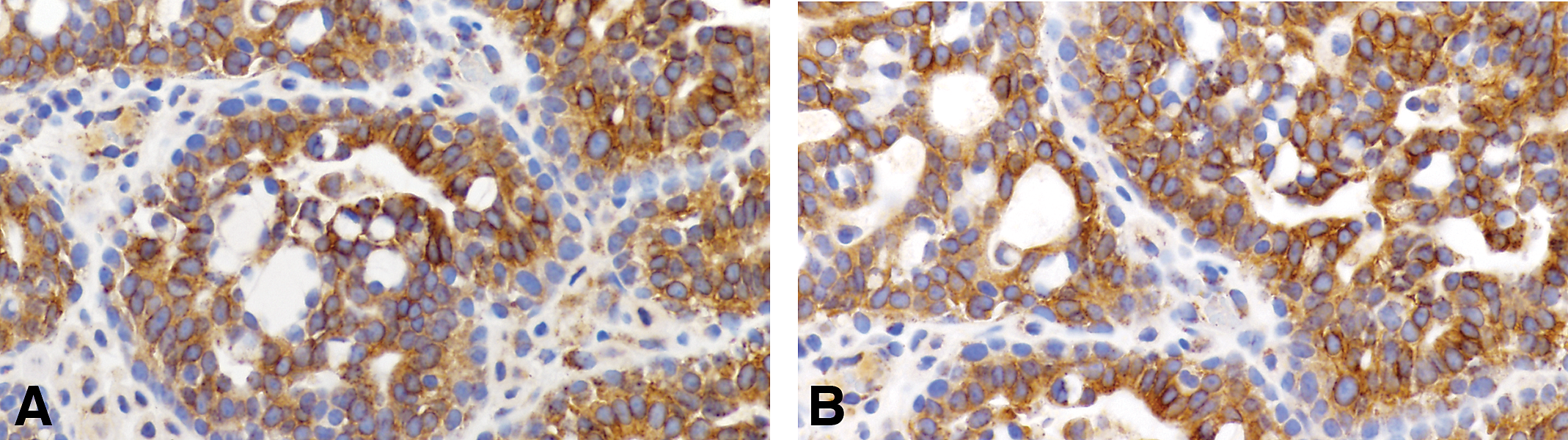
Invasive carcinoma of luminal type A containing positive cells for HER2/neu (A) and (B) 40×.
Immunocytochemical evaluation of rat mammary tumors.

The mammary tumors (59 rats) listed in Table 10 and histologically classified as invasive papillary, cribriform, comedo, tubular type, and adenoid cystic reacted with antibodies detecting ER alpha, PgR, and HER2/neu positive. The proportion of ER alpha positive cells varies from 15.1 to 57.5%. The proportion of PgR-positive cells varied from 11.1 to 61.1%. The HER2/neu was found only positive in a fraction of the tumors that were ER and PgR positive and classified as luminal A, comprising 76.2%, whereas the other fraction of the tumors were HER2/neu negative and considered luminal type B, comprising only 23.8% of the tumors.
Invasive rat mammary cancer induced by DMBA classified using the histological criteria and immunophenotype.
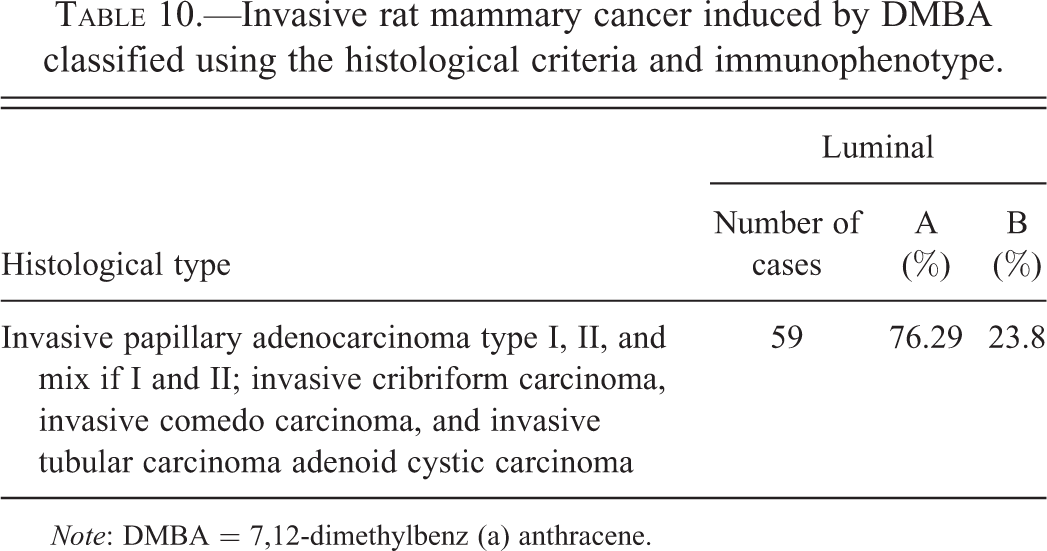
Note: DMBA = 7,12-dimethylbenz (a) anthracene.
At the time of the publication of this work, the authoritative work of Santagata et al. (2014) was published showing that the use of other immunocytochemical markers like Vitamin D and androgen receptors in addition to HER2/neu and estrogen receptor may allow to better differentiate cancer subtypes in the human. Therefore, the study in the rat model using new immuno-cytochemical markers as well as the comparison with the same makers in preneoplastic lesions and the final comparison with the human lesions warrants a new series of studies besides the one described in the present work.
Final Considerations
The rat mammary tumor model is well suited for studying in situ and invasive lesions. However, unless the animals are kept for longer periods of time and the methodology for detecting early metastatic events improves, the rat model is not a good model for studying the metastatic process. The classification of the tumors matches well with the criteria used in the human pathology and provides an adequate model for understanding these phases of the human disease. The role of immunosurveillance is an area that should be better studied and could potentially provide new insight into the inflammatory processes involved in the initiation and progression of mammary neoplasia. In turn, it could provide an adequate model for testing vaccines and other tools using cytokines inhibitors.
The use of immunocytochemical markers allows us to differentiate 2 cell subtypes, luminal A and B. We have not detected any of the tumors studied as positive only for HER2/neu or as triple negative. An important consideration is that the presence of histochemical markers does not indicate that the tumors in the rat will behave exactly as they do in the human disease but will provide an initial point of comparison and more studies on this subject could be extremely beneficial.
Footnotes
Acknowledgments
A special acknowledgment goes out to Ms. Rose Sonlin for verifying the accuracy of the references and for her help with preparation of the manuscript; and to Ms. Patricia A. Russo for her editorial suggestions. I also acknowledge the work of Dr. Yanrong Su in performing the immunocytochemical studies in the rat mammary tumors. This work was supported by NIH core grant CA06927 to Fox Chase Cancer Center.
Author’s Note
We dedicate this work to the memory of Irma H Russo, MD who passed away on June 25, 2013. For the past 22 years, Irma has worked at Fox Chase; first as director of surgical and clinical pathology and then as director of the molecular endocrinology section of the Breast Cancer Research Laboratory, which she founded in 1973 with her husband, Jose. Irma was a pioneer in classifying the rat mammary tumors and their correlation with the human pathology in addition to identifying the mechanisms of breast cancer prevention as mediated by pregnancy. The collaboration between Jose and Irma was so deep it was, at times, impossible to determine where one ended and the other began. Thanks to her innate sense of scientific collaboration and creativity, together they published 6 books and over 200 research. Irma had a very distinguished career in research and remained devoted till the end to the mission of understanding the cellular and molecular basis of breast cancer. She will be remembered not only by her many friends, colleagues, and the more than 50 MDs and PhDs she trained and mentored over the years, but also by every human being who was touched by her good nature.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by NIH core grant CA06927 to Fox Chase Cancer Center and by an appropriation from the Commonwealth of Pennsylvania.