
Abstract
While the study pathologist (SP) signs the pathology report and is ultimately accountable for the data, the sponsor peer review pathologist (SPRP) generally signs a peer review (PR) statement indicating agreement with the overall pathology data and the associated interpretations. Additionally, the SPRP is often the initial contact to field internal and regulatory pathology data queries. Therefore, the SPRP should conduct as comprehensive a pathology PR as necessary to have complete confidence in the data and interpretations. Ideally, the SPRP should be involved at study design, as the study evolves, through completion of the overall study report. The SPRP should prepare as much as possible before the actual PR start date to include a review of all available data that may impact the PR. This review should focus on identifying findings not already identified in the draft pathology report that may need further interrogation. While all discrepancies between the SPRP and SP may be discussed for mutual learning, the emphasis should be on resolving issues that impact study interpretation. The final pathology report should reflect the consensus between the SP and SPRP and appropriately communicate the study findings. This article provides further background and example scenarios to illustrate these PR perspectives.
Introduction
The history, purpose, requirements and/or regulatory considerations, and recommendations for peer review (PR) are addressed in a number of excellent publications (some recent—Morton et al. 2010; Mann and Hardisty 2013). Although not generally required, PR is “endorsed” by regulatory bodies and is best practice standard in the pharmaceutical industry. Several Societies of Toxicologic Pathology, including the Society of Toxicologic Pathology (STP), have endorsed (Boorman et al. 2010) the recommended guidelines of Morton et al. 2010. Mann and Hardisty (2013) suggest slightly more rigorous guidelines for PR, and each pharmaceutical company will likely have specific internal guidelines (standard operating procedure [SOP]).
Both the SP and the SPRP offer unique expertise, and both often learn from the PR. The SP often has vast experience in toxicologic pathology and comprehensive knowledge of the study at hand. The SPRP also generally has extensive experience, and often has knowledge of target biology, pharmacology and pharmacokinetic data, mechanism of target-mediated and off-target toxicity, findings in previous studies and class effects, etc. (Morton et al. 2010). While the study pathologist (SP) signs the pathology report and is ultimately accountable, the final pathology data should reflect a consensus between the SP and SPRP. Most PR statements signed by the SPRP contain language indicating agreement with the overall pathology data and/or the associated interpretations. Additionally, the SPRP is often asked to explain or defend pathology data by internal line management, drug development teams, safety review boards, and will likely be the initial pathology contact from external (e.g., Food and Drug Administration [FDA]) queries. Therefore, while SOP requirements must be met, it is prudent to conduct as comprehensive a PR as necessary to give the SPRP complete confidence in all aspects of the data including interpretation and reporting. A number of factors including experience as a toxicologic pathologist and as an SPRP will impact the approach, and the SPRP should conduct a PR in a manner that works best for them.
This article reflects personal experience from the perspective of a sponsor PR of studies conducted in accordance with Good Laboratory Practices (GLPs) at contract research organizations (CROs). While following the published recommended guidelines will ensure the highest quality pathology data, additional information included here may be useful in preparation for and conduct of a PR, particularly for pathologists with less experience conducting PR. A checklist is included in Table 1.
Peer review pathologist checklist.
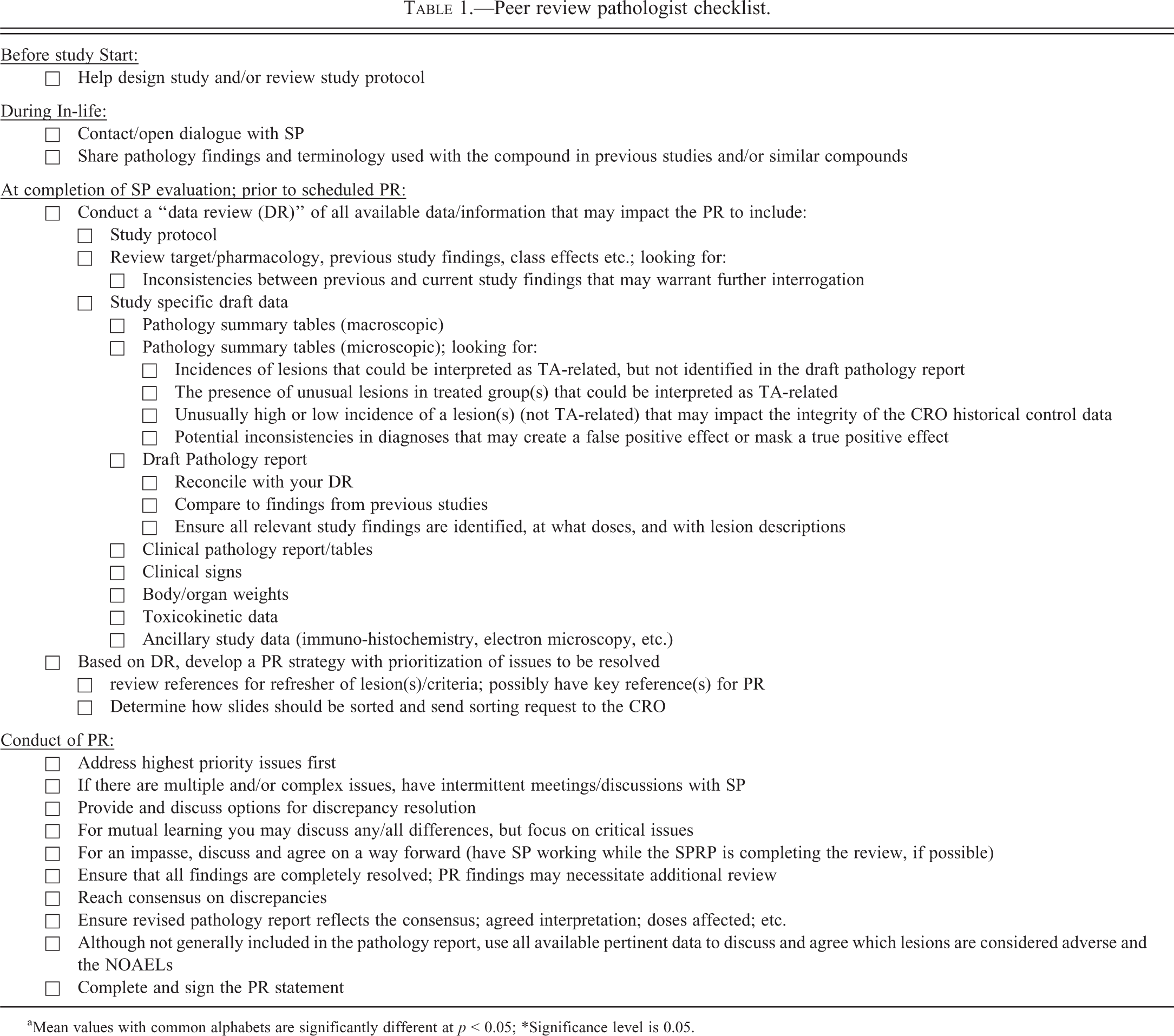
aMean values with common alphabets are significantly different at p < 0.05; *Significance level is 0.05.
Preparation for the PR (General)
If possible, the SPRP should be involved early in the process. As the studies are generally designed in
Toxicology studies are typically read in an open fashion, and similarly peer reviewed; however, informal blinding (mixing controls and dose group/dose groups) for histological evaluation may be needed during the primary read or PR to verify subtle TA-related findings, no effect levels and no adverse effect levels (NOAEL), and this application minimizes or eliminates potential bias. There are instances where such informal blinding, for a specific tissue, is needed to convince either the SP or the SPRP where the no effect level truly is for subtle microscopic changes considered relevant to the TA.
Conduct of a PR needs to be as efficient and effective as possible; therefore, it is best to prepare as much as possible before the actual start date. Conduct a “data review” of all available data that may impact the PR to include study-specific draft data (anatomic and clinical pathology; pathology report; clinical signs; body/organ weights; toxicokinetics; and ancillary study data [e.g., immunohistochemistry and electron microscopy]; Morton et al. 2010). This type of review is part of the PR process within the National Toxicology Program as well. It is generally beneficial to review or rereview target/pharmacology, previous study findings, and class effects. The data review should allow you to identify lesions/issues of concern and develop a strategy for review and resolution. Depending upon issues identified and experience level, it may be necessary to review articles/books for refresher of lesion/lesions criteria and possibly have key reference/key references available during the PR.
Once a PR strategy is decided, determine how slides can be sorted to most efficiently facilitate the PR. If not sorted appropriately, more time can be spent pulling and replacing slides than actually viewing them. If requested in advance, the CRO will usually accommodate special sorting requests, but once there, they are unlikely to have someone at your beckoning. This is of lesser concern for small studies with few findings, but can be significant for larger (e.g., carcinogenicity) studies and/or studies with numerous findings. Be aware of the impact any sorting request (e.g., all livers and/or all neoplasms in separate boxes) may have on other aspects of your PR. Use of a PR software package in which SP diagnoses are downloaded along with a column for the PR diagnosis and a column for the resulting action (Mann and Hardisty 2013) may be helpful for large and/or complex studies but obviously requires advance setup. For most studies, notes are adequate for identifying and reconciling discrepancies. These informal working notes are not retained as part of the study record since the final diagnoses represent a consensus between the SP and SPRP.
Preparation for the PR (Data Review)
All guidelines suggest some degree of examination of the “target organs.” While the draft pathology report identifies target organs, review of all pertinent data helps identify other “potential” target organs. A first step is to examine pathology data for incidences of lesions that could be interpreted as TA related, but not identified in the draft pathology report. For example, in the data review of one study, 3 of the 10 high-dose (HD) male rats had diagnoses of “cardiomyopathy” compared to none in controls. These 3 lesions were typical (size and character) of the “cardiomyopathy” lesions commonly observed in control animals from other studies, and well within the range of what the SP often sees in control groups, and therefore was not mentioned in the draft pathology report. However, for the following reasons, some may consider this finding potentially TA related, particularly with the sensitivity around cardiovascular findings in nonclinical studies: (1) This lesion occurred in 30% of HD males compared to 0% in controls; (2) some compounds can induce lesions similar to and/or exacerbate the spontaneous lesion, particularly at the lower doses; and (3) the incidence of spontaneous cardiomyopathy is underreported in the literature that I have reviewed, therefore giving the impression that 30% is high. In this instance, the heart should be added as a “potential target” for PR and at a minimum should include histological examination of all hearts from the control and HD males. If any additional cardiomyopathy lesions are identified during the PR of control and HD animals, the review should be expanded to include intermediate groups, and all groups of females. This will ensure that the data for this finding are as robust as possible, eliminating any drift that may have occurred in the primary study read which biases the result, and increases sponsor confidence that the finding is either a true positive, and is reported, or a false positive signal that is discussed and appropriately contextualized by the SPRP and SP. A review of any additional data (e.g., cardiac troponin levels and heart weight) that may impact interpretation of the finding is also warranted. In this instance, additional similar lesions were identified in the control group, therefore it became a nonissue (it was a false positive signal). Had the original data been confirmed, even if considered not TA related (consistent with background seen in other studies), this finding should be included in the pathology report along with reasons for dismissal (e.g., character of lesions, CRO historical control data, normal cardiac troponin levels and heart weight, and lack of an increase in females).
The presence of unusual lesions in a treated group/groups may also warrant further interrogation. During data review of a study, 1/10 HD males had a diagnosis of focal necrosis/inflammation of a heart valve compared to 0/10 in controls; no females were affected. Based only on an isolated microscopic finding, a single finding in an HD group of 10 is unlikely to be identified as a target; however, this is a relatively uncommon finding that raises concern. Also, with the best routine sectioning, it is likely that not all cardiac valves are included in each heart section/sections; therefore, if a TA-related response was valve-specific (e.g., aortic valve), the true incidence could be higher than 1/10. A finding in a previous study or biological plausibility may tip the scales toward “uncertain finding” or possibly even considered TA related. In this instance, at a minimum, the valves from all control and all HD males should be examined, and it is prudent to examine males from the mid-dose group and HD females, as an additional similar lesion in these groups could be meaningful. Identification of any additional similar lesions should result in a complete review of valves from all animals from all groups. The SPRP determined that all heart valves were well represented in this study, identified no additional lesions nor identified any other “reasons to believe” (biological plausibility) so was in agreement with the SP that the necrotic/inflammatory valve lesion was not considered TA related in this study.
Something else to look for in the pathology tables is unusually high or low incidence of a lesion/lesions (e.g., too many or too few liver tumors for the sex/species) across all groups including controls, even if there is no apparent dose relationship. Even if the diagnostic approach is consistent within the study, it is important to address this to ensure that there are reliable historical control data. In the data review of a carcinogenicity study, based on personal experience, published historical control data, and confirmed by the CRO historical control data set, the incidences of liver neoplasms were high across all groups. While the SP was very consistent in his or her diagnostic approach, his or her threshold from focus to adenoma and from adenoma to carcinoma was too low. Although this should be corrected with the default review (current recommendations include review of all neoplasms in carcinogenicity studies; Morton et al. 2010), awareness of the potential discrepancy should help ensure resolution. In this instance, the SP adjusted their thresholds. Had the situation been reversed with low liver neoplasms across all groups, and high thresholds, it would be necessary to include all foci in the review as well.
Potential inconsistencies in diagnoses should also be evaluated during the data review. There is variability in the diagnostic approach for some spontaneous lesions. One example is the spectrum of lesions comprising “murine cardiomyopathy.” Some pathologists use no threshold, while others use a self-defined threshold that likely varies among pathologists. Pathologists are generally very consistent within a study; therefore, this should not present a problem interpreting TA-related effects. However, be aware of the impact that it may have on the use of historical control data. “Lumpers” diagnose most or all the spectrum of murine cardiomyopathy under one term (e.g., cardiomyopathy), while “splitters” use multiple diagnoses for the varying morphologies. Although sometimes appropriate to do so, the use of multiple diagnoses increases the potential for inconsistent application of diagnostic criteria, and therefore a greater potential to create a false positive finding or mask a true positive finding.
Reviewing other study-specific or nonstudy-specific data can be helpful in identifying correlative findings that may help interpret and/or gain confidence in already identified microscopic findings. Conversely, identifying signals with no correlating microscopic finding may indicate a need to further interrogate pathology data. For example, an organ weight change, a clinical pathology signal, or a lesion diagnosed in a tissue in a previous study with similar doses, but not in the current study, may suggest the need to PR additional tissues to be confident that there truly is no microscopic correlate.
It is likely that any findings resulting from review of the “potential targets/issues” identified during data review will be subtle; therefore, blinding as discussed earlier may be critical to accurately identify lesions and/or NOELs/NOAELs. Recognizing the variability of various lesions in concurrent control groups and the limited number of controls in an individual study, the use of historical control data can be invaluable in addressing subtle findings identified during the data review and PR. As valuable as these data can be in contextualizing findings, it is important to be aware of the limitations. Historical control data, particularly for some pathology end points, may not be as robust as desired. As mentioned earlier, within a CRO or pharmaceutical company, the use of different thresholds and/or using no threshold for a specific entity may adversely affect their historical control data. Use of different diagnoses for the same lesion may also affect the historical control data. Use of different terms/diagnoses may result from pathologist’s background and/or training, and there is the “lumping and splitting” issue mentioned earlier. Awareness of the various diagnoses used for certain lesions allows mining of historical control data in a manner that will minimize any impact of using different terms.
Discrepancy Resolution
As the microscopic examination proceeds, discrepancies may be identified. Sources of discrepancies include but are not limited to unfamiliarity with lesion by SP or SPRP; different criteria for tumor classification; different threshold/thresholds for diagnosis of lesions (especially nonneoplastic aging lesions); different terminology for same lesion; and diagnostic drift (e.g., variations in grading application for the same severity of TA-related finding, particularly in large studies; Mann and Hardisty 2013).
How discrepancies are handled depends on many factors, but it is prudent to be humble and diplomatic, recognizing that it is far easier to critique via PR than to complete the initial histological evaluation. For mutual learning, it is reasonable to discuss any/all differences; however, it is unwise to quibble over borderline lesions or severity grades that do not materially impact the study outcome. In contrast, terminology, thresholds, and severity grades for TA-related findings should be consistent across all dose groups since the interpretation of these data carries through with consequence to the final toxicology report and to the TA. Be conscience of and remove any bias and clearly articulate from a position of science and evidence (provide references when possible). Provide and discuss options if possible. Having intermittent discussions with the SP to deal with multiple and/or complex issues is generally more effective and palatable. If there is an impasse on a diagnosis or issue, discuss and agree on a way forward (e.g., other opinions [who and where] and/or pathology working group–type review]. Intermittent meeting with the SP during the PR can be useful to deal with “impasse issues” while the PR is ongoing.
It is important to keep in mind that the PR involves review of a subset of slides, and although the SPRP has a strategy coming into the PR, findings or observations during the PR may necessitate additional review. For example, for “complete review” animals, protocol required tissues are generally reviewed for ∼30% of HD animals in a toxicology study and ∼10% HD animals in a carcinogenicity study (Morton et al. 2010). A finding of one additional neoplasm in the HD group of a carcinogenicity study may be indicative of a bigger problem, as 90% of the animals have not had all protocol required tissues examined. PR findings must be carefully considered to determine if and to what extent additional review is necessary. Some examples were mentioned previously.
Pathology Report Review/Finalization of the PR
Part of the PR includes ensuring that the pathology report accurately reflects and appropriately communicates study findings. At a minimum, the draft pathology report should identify all dose groups with TA-related lesions, provide brief lesion descriptions, and include the cause of all early deaths, all of which will impact study interpretation. Clear reasons and references should be included when concluding marginally increased incidence of lesions are not TA related or are judged, with a weight of evidence approach, as not toxicologically meaningful in isolation. The major study interpretations/conclusions will, of course, consider all study data and be included in the overall study report, and not in the pathology report. However, using all available pertinent data, the SPRP and SP should have discussions and agreement, if possible, about which lesions are considered adverse and the NOAELs. Because the totality of toxicology study data reported by other contributing scientists can include influential information not considered part of the PR, it can be helpful to involve the SPRP in the sponsor management review of the final toxicology report.
The SPRP completes his or her portion of the PR by signing the PR statement, the timing of which is discussed elsewhere (Morton et al. 2010).
Footnotes
Acknowledgments
The author acknowledges the immensely helpful reviews of Drs. Rick R. Adler and Jerry F. Hardisty.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.