
Abstract
We have previously reported that dental caries progress in spontaneously and chemically induced diabetic rodent models. The aim of this study was to clarify the relationship between hyperglycemia and dental caries by evaluating the preventive effect of glycemic control with insulin on the progression of the lesions in diabetic rats. Male WBN/KobSlc rats aged 15 weeks were divided into groups of spontaneously diabetic rats (intact group), spontaneously diabetic rats with insulin treatment (INS group), alloxan-induced prolonged diabetic rats (AL group), and alloxan-induced prolonged diabetic rats with insulin treatment (AL + INS group). The animals were killed at 90 weeks of age, and their oral tissue was examined. Dental caries and periodontitis were frequently detected in the intact group, and the lesions were enhanced in the AL group (in which there was an increased duration of diabetes). Meanwhile, glycemic control with insulin reduced the incidence and severity of dental caries and periodontitis in the INS group, and the effects became more pronounced in the AL + INS group. In conclusion, glycemic control by insulin prevented the progression of dental caries and caries-related periodontitis in the diabetic rats.
Introduction
Some experimental studies using diabetic animal models have indicated that hyperglycemia increases the risk and severity of dental caries (Borghelli et al. 1966; Hartles and Lawton 1958). Hyperglycemia has also been suggested to increase the risk of dental caries in humans (Jawed et al. 2011; Miralles et al. 2006; Twetman et al. 2002). Meanwhile, other researchers have detected no significant difference in susceptibility to caries between diabetic and nondiabetic patients (Canepari, Zerman, and Cavalleri 1994; Collin et al. 1998; Tagelsir et al. 2011). Consequently, no firm conclusions can be drawn about the relationship between hyperglycemia and dental caries.
Dental caries and caries-related periodontitis develop in db/db mice, a spontaneously diabetic animal model of type 2 diabetes (Sano et al. 2011), and dental caries progress further in spontaneously diabetic male WBN/KobSlc rats compared to nondiabetic female rats of the same strain (Kodama et al. 2011). In addition, chemically induced hyperglycemia with alloxan treatment may cause rapid-onset and progressive dental caries and periodontitis in F344 and Wistar rats (Claudino et al. 2007; Nakahara et al. 2012). These results suggest that a hyperglycemic condition may contribute to the development of dental caries in diabetic rodent models; however, no reports have investigated the preventive effect of glycemic control on the development of dental caries in diabetic animals. Thus, the direct causal relationship between hyperglycemia and dental caries is unknown.
The aim of this study was to evaluate whether glycemic control with insulin treatment prevents the progression of dental caries in spontaneously or chemically induced diabetic rats.
Materials and Methods
Animals and Housing Conditions
Male WBN/KobSlc rats were supplied by Japan SLC, Inc. (Hamamatsu, Japan). The animals were housed in stainless-steel cages at a temperature of 20°C to 26°C and a relative humidity of 40% to 70% under a 12-hr/12-hr light/dark cycle; they were ventilated with filtrated fresh air. They were allowed free access to tap water and a widely used standard pelletized diet for experimental mice and rats (Charles River Formula 1 [CRF1], Oriental Yeast, Tokyo, Japan). The animals were handled according to the principles for all experimental procedures outlined in the Guide for the Care and Use of Laboratory Animals prepared by our institution (Setsunan University) and the Japanese Association for Laboratory Animal Science.
Experimental Design
The experimental design is shown in Figure 1. Male rats of the WBN/KobSlc strain develop spontaneous diabetes after 40 weeks of age (Nakama et al. 1985; Tsuchitani et al. 1985), and this strain of rats is susceptible to dental caries (Fukuzato et al. 2009). A total of 60 male WBN/KobSlc rats were randomly divided into 4 groups. Fifteen intact rats showing spontaneously occurring diabetes were used as the control (intact group). Fifteen rats were treated with sustained-release insulin implants (LinShin Canada Inc., Ontario, Canada; release rate: ∼2 U/24 hr/implant for >40 days) by subcutaneous injection 3 weeks after they showed spontaneously occurring severely diabetic state (INS group). Alloxan, a pancreatic β-cell cytotoxic agent, was used to stimulate early-onset (prolonged) diabetes. Thirty rats, aged 15 weeks, were given a single dose (40 mg/kg of body weight) of alloxan (Sigma-Aldrich Japan, Tokyo, Japan) via the tail vein. The dose of alloxan was chosen because a rat that receives this dose usually survives for a long period (>50 weeks) after the onset of diabetic symptoms (Kodama et al. 2006). Fifteen of 30 alloxan-induced diabetic rats were kept without treatment (AL group). The remaining 15 alloxan-induced diabetic rats were treated with insulin implants according to the same method as the INS group (AL + INS group). The moribund animals were necropsied, as were the dead animals (a total of 18 rats), during the examination period. The causes of death or the moribund condition in these rats were malignant lymphoma, hypoglycemia caused by the insulin treatment, urinary tract infection, and ketoacidosis resulting from severe diabetes. The remaining 42 rats were sacrificed at 90 weeks of age for morphological examinations.
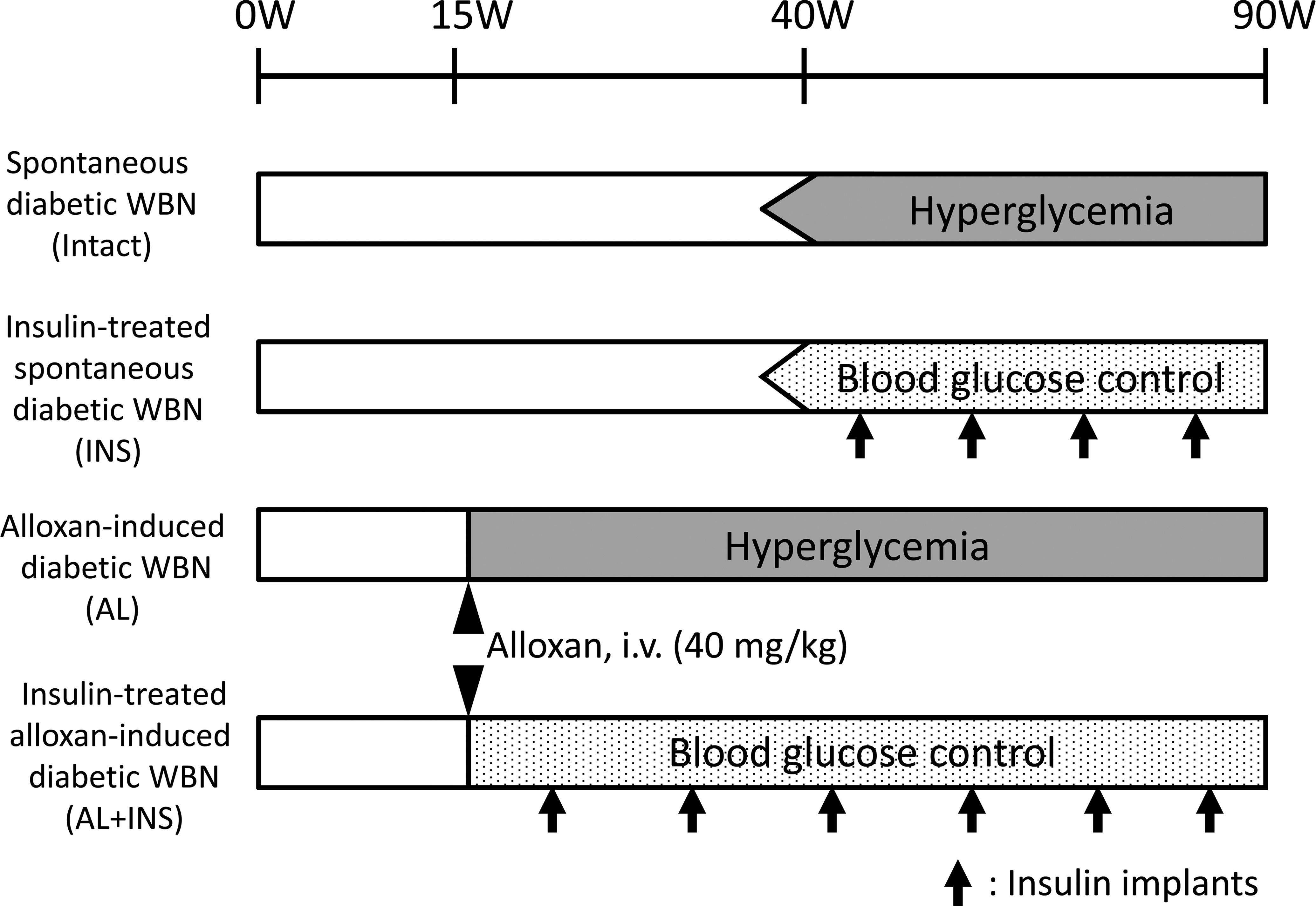
Study design.
Glycosuria and Glycemia Monitoring
Urinary glucose levels in fresh urine were measured semiquantitatively with a urine test paper (Wako Pure Chemical Industries, Osaka, Japan), and blood glucose levels in the tail vein samples were also measured semiquantitatively by using the glucose oxidase method (Glutest E, Sanwakagaku, Aichi, Japan). The urinary and blood glucose levels of the spontaneously diabetic rats (intact and INS groups) were measured monthly after the rats reached 40 weeks of age. The urinary glucose levels of the alloxan-treated diabetic rats (AL and AL + INS groups) were measured daily from days 1 to 3 after dosing, weekly for 1 month after the first week, and monthly thereafter. The blood glucose levels of the alloxan-treated diabetic rats were measured monthly from the fourth week after the alloxan injection. Blood samples from the tail vein and fresh urine were collected between 1:00 pm and 4:00 pm for measuring the fasting blood glucose level. The severity of hyperglycemia was defined as follows: normal, <200 mg/dl; mild, >200 mg/dl; moderate, >300 mg/dl; or severe, >400 mg/dl (Butler 1995). The severity of glycosuria was defined as follows: normal, <100 mg/dl; mild, >100 mg/dl; moderate, >250 mg/dl; or severe, >500 mg/dl.
Grading for Caries and Alveolar Bone Resorption by Soft X-ray Examination
The animals were euthanized by exsanguination from the abdominal aorta under deep anesthesia at the end of each scheduled period. Subsequently, the mandible and maxilla were removed and fixed in 10% neutral-buffered formalin (pH 7.4). After a 24-hr fixation, a soft X-ray examination was performed. Soft X-ray images of the mesiodistal plane were taken under conditions of 35 kV and 2 mA for 4 min. The teeth were classified into five groups according to the characteristics of the caries observed and measured on radiographs: grade 0, no radiolucent change; grade 1, radiolucent area only on the occlusal surface of the crown; grade 2, radiolucent areas on the occlusal surface and on either of the mesiodistal surfaces of the crown; grade 3, radiolucent areas over the entire surface of the crown; and grade 4, radiolucent areas over most of the surface of the dental root. The alveolar bone resorption in each tooth was evaluated by measurement of the radiolucent area around each molar root on the soft X-ray image. Resorption was graded as follows: grade 0, no radiolucent change; grade 1, 0.01 to 0.20 mm2; grade 2, 0.21 to 0.40 mm2; grade 3, 0.41 to 0.60 mm2; and grade 4, more than 0.61 mm2. The mean scores of caries and alveolar bone resorption were used as indicators for comparing the severity of these lesions between the groups and were calculated as follows:

Histopathological Examination
After soft X-ray examination, a histopathological examination was performed on the mandibles and maxillae of all the rats. After fixation with 10% neutral-buffered formalin, the sample was decalcified in a 5% solution of ethylenediaminetetraacetic acid 4 Na (EDTA 4 Na) for 2 weeks at 4°C. After decalcification, the specimens were trimmed; they were then dehydrated in a sequential ethanol series using an automated processor and embedded in paraffin wax. Serial 7-µm thick sections on the mesiodistal plane were made through the centers of all the molars and were then stained with hematoxylin and eosin for examination by light microscopy. The caries lesions were graded as follows: mild, if the dentin caries were localized in the occlusal surface of the dentin; moderate, if the dentin caries extended into dental pulp with pulpitis and pulp necrosis; and severe, if the corona dentis was decayed. Gingivitis was evaluated on the basis of inflammatory cell infiltration in the gingival tissue and mucosal hyperplasia as follows: mild, if few inflammatory cells infiltrated into the mucosal epithelium; moderate, if the inflammatory cells were scattered throughout the gingival connective tissue with mucosal hyperplasia. Marginal periodontitis was evaluated according to inflammatory cell infiltration and alveolar bone resorption as follows: mild, if localized inflammatory cell infiltration was observed in the cervical area and/or resorption of the alveolar bone crest was observed; moderate, if the inflammatory cell infiltration was observed and alveolar bone resorption extended to the radicular area. Apical periodontitis was also evaluated on the basis of inflammatory cell infiltration and alveolar bone resorption as follows: mild, if localized inflammatory cell infiltration and/or alveolar bone resorption were observed in the apical part of the molar root; moderate, if extensive inflammatory cell infiltration and alveolar bone resorption were observed in the tissue around the molar root.
Statistical Analysis
The Wilcoxon rank sum test was used to compare the differences between the groups in the mean scores of caries lesions and alveolar bone resorption as assessed by soft X-ray examination. The chi-square test was used to determine the incidence of histopathologic lesions by histological examination in each group of rats. P < .05 was regarded as statistically significant. The Pearson correlation was used to examine the associations between molar caries and alveolar bone resorption.
Results
Blood and Urine Glucose Levels
Mild to severe hyperglycemia (>200 mg/dl) and glycosuria (>100 mg/dl) were observed in the intact group of approximately 40 weeks of age. In contrast, the blood glucose level of the INS group fluctuated between normoglycemia (<200 mg/dl) and hyperglycemia. Although blood glucose levels were kept under 200 mg/dl immediately after treatment with insulin implants, they gradually increased before the next treatment. In the AL group, severe hyperglycemia (>400 mg/dl) and glycosuria (>500 mg/dL) persisted for approximately 75 weeks from the day after the injection of alloxan to the time of scheduled necropsy. The blood and urine glucose levels of the AL + INS group fluctuated similarly to those in the INS group during the monitoring period (Figure 2).
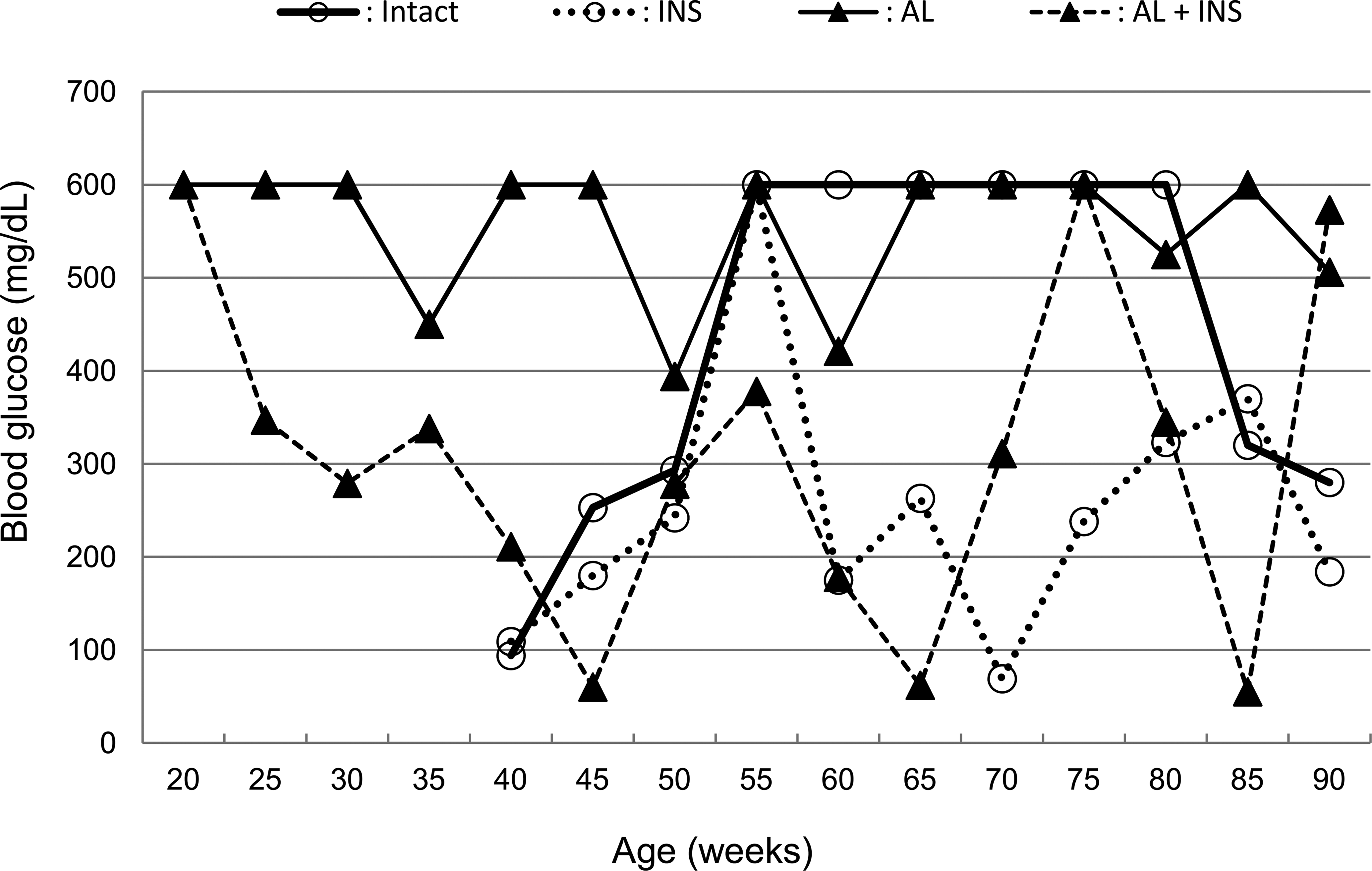
Change in mean blood glucose levels.
Caries Scores by Soft X-ray Examination
The incidence of teeth with caries in the mandibular and maxillary molars based on each scoring is shown in Table 1. In all of the groups, dental caries were detected as radiolucent lesions in the dental crown. In the intact group, 71.7% of the maxillary molars and 58.3% of the mandibular molars were affected with dental caries, and the mean caries scores of the maxilla and mandible were 2.06 and 1.62, respectively. Meanwhile, in the INS group, only 33.3% of the maxillary molars were affected, and the mean caries score of the maxilla (1.13) was significantly lower (p < .01) than that in the intact group. The incidence (55.6%) and mean score (1.26) of caries in the mandibular molars also tended to be less in the INS group, but there was no significant difference between the 2 groups. Furthermore, compared with the intact group, the incidence and mean scores of caries were higher in the AL group; 100% of the maxillary and mandibular molars were affected, and the mean caries scores of the maxilla and mandible were 3.86 and 3.59, respectively. By contrast, in the AL + INS group, the incidence of caries (maxilla, 41.7%; mandible, 63.3%) and the mean caries scores (maxilla, 1.08; mandible, 1.77) were significantly lower (p < .01) than those in the AL group (Table 1 and Figure 3).
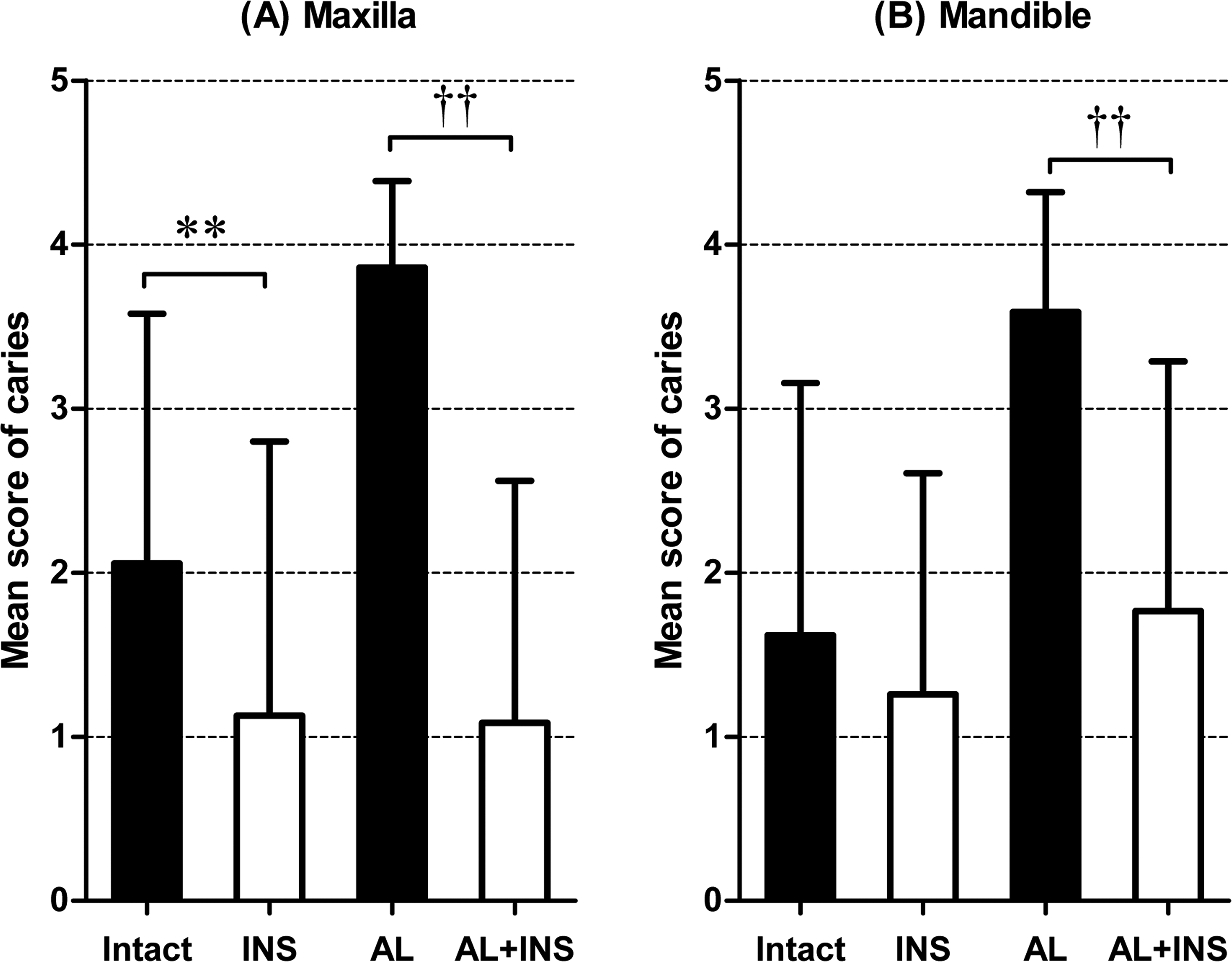
(A), Mean caries scores in the maxillary molars. (B), Mean caries scores in the mandibular molars. Significant differences from the intact (**p < .01) and alloxan-induced prolonged diabetic rats with insulin treatment (AL + INS) group (††p < .01).
Incidence and grading of caries in the molars of the male WBN/KobSlc rats (soft X-ray examination).
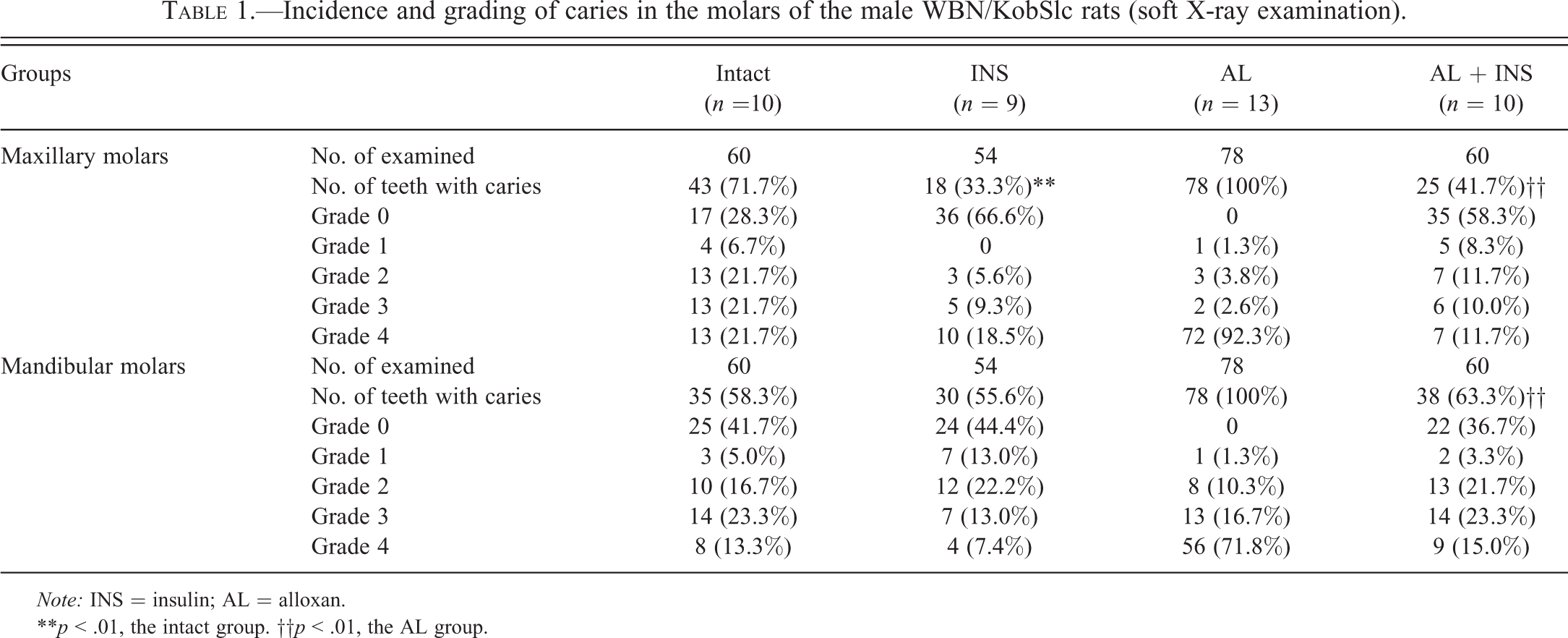
Note: INS = insulin; AL = alloxan.
**p < .01, the intact group. ††p < .01, the AL group.
Changes in Alveolar Bone Resorption by Soft X-ray Examination
The incidence of teeth with alveolar bone resorption in the mandible and maxilla according to grade is shown in Table 2. Alveolar bone resorption was frequently detected in the intact group, and half (50.0%) of the maxillary molars and almost half (41.7%) of the mandibular molars were affected, and the mean bone resorption scores of the maxilla and mandible were 1.04 and 0.82, respectively. Meanwhile, in the INS group, only 20.4% of the maxillary molars were affected, and the mean bone resorption score of the maxilla (0.30) was significantly lower (p < .01) than that in the intact group. The incidence (35.2%) and mean score of bone resorption (0.48) in the mandible of the INS group also tended to be low in comparison with those in the intact group, but there was no significant difference between the 2 groups. Furthermore, compared with the intact group, the incidence and mean score of bone resorption were higher in the AL group; nearly three-quarters of the maxillary (73.1%) and mandibular molars (75.6%) were affected, and the mean bone resorption scores of the maxilla and mandible were 1.33. By contrast, in the AL + INS group, the incidence of bone resorption (maxilla, 25.0%; mandible, 50.0%) and the mean bone resorption scores (maxilla, 0.43; mandible, 0.85) were significantly lower (p < .01) than those in the AL group (maxilla and mandible, 1.33; Table 2 and Figure 4). Alveolar bone resorption was mainly observed in the apical area adjacent to the carious molars (Figure 5A and B). However, there was no radiolucent change in the alveolar bone surrounding the noncarious molars (Figure 5B). There was a highly positive correlation between alveolar bone resorption and caries scores (mandible: r = .75, p < .01; maxilla: r = .70, p < .01).

(A), Mean scores for alveolar bone resorption in the maxillary molars. (B), Mean scores for alveolar bone resorption in the mandibular molars. Significant differences from the intact (**p < .01) and the alloxan-induced prolonged diabetic rats with insulin treatment (AL + INS) group (††p < .01).
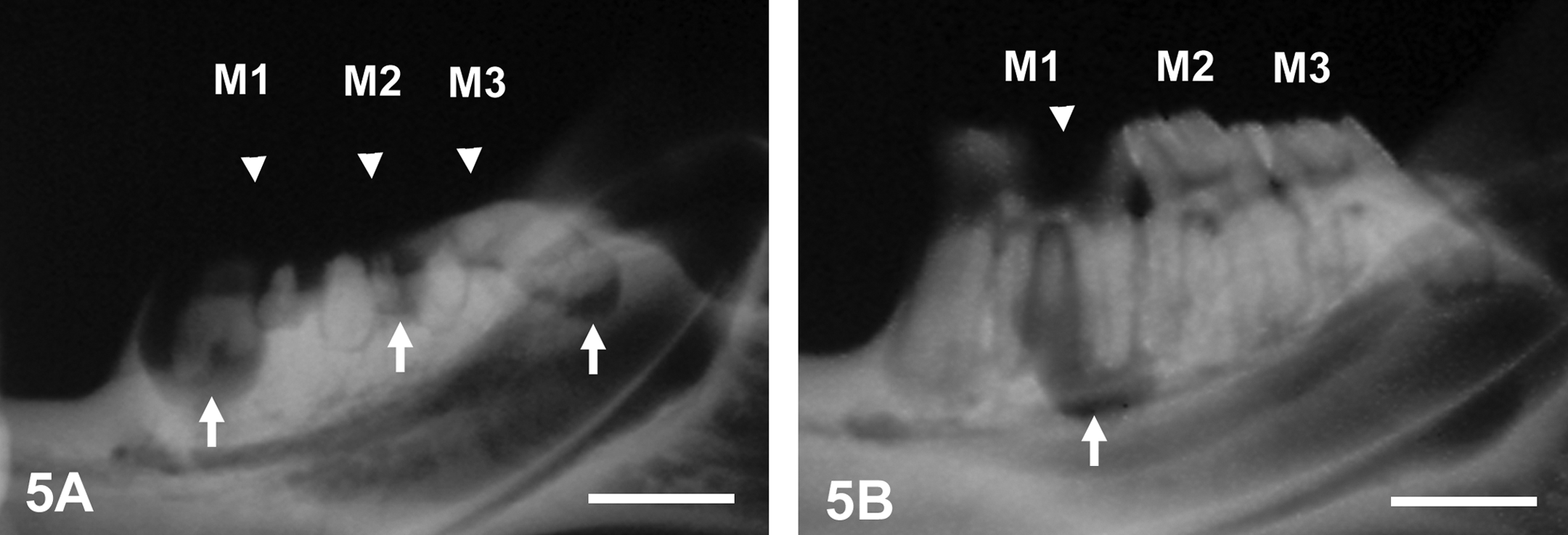
Soft X-ray images of molar caries and alveolar bone resorption. M1 = the first molar; M2 = the second molar; M3 = the third molar. (A), The mandible of a spontaneously diabetic rat (intact group). Moderate to severe caries with an extensive radiolucent area in the dental crown is observed (all the molars, arrowheads). In the alveolar bone surrounding the carious molars, focal radiolucency at the apical part of the dental root is frequently detectable (arrows). Scale bar, 2 mm. (B), The mandible of an insulin-treated diabetic rat (INS group). Alveolar bone resorption is observed in the area adjacent to the carious molars (M1, arrow), but there is no radiolucent change in the alveolar bone surrounding the noncarious molars (M2 and M3). Scale bar, 2 mm.
Incidence and grading of alveolar bone resorption in the male WBN/KobSlc rats (soft X-ray examination).
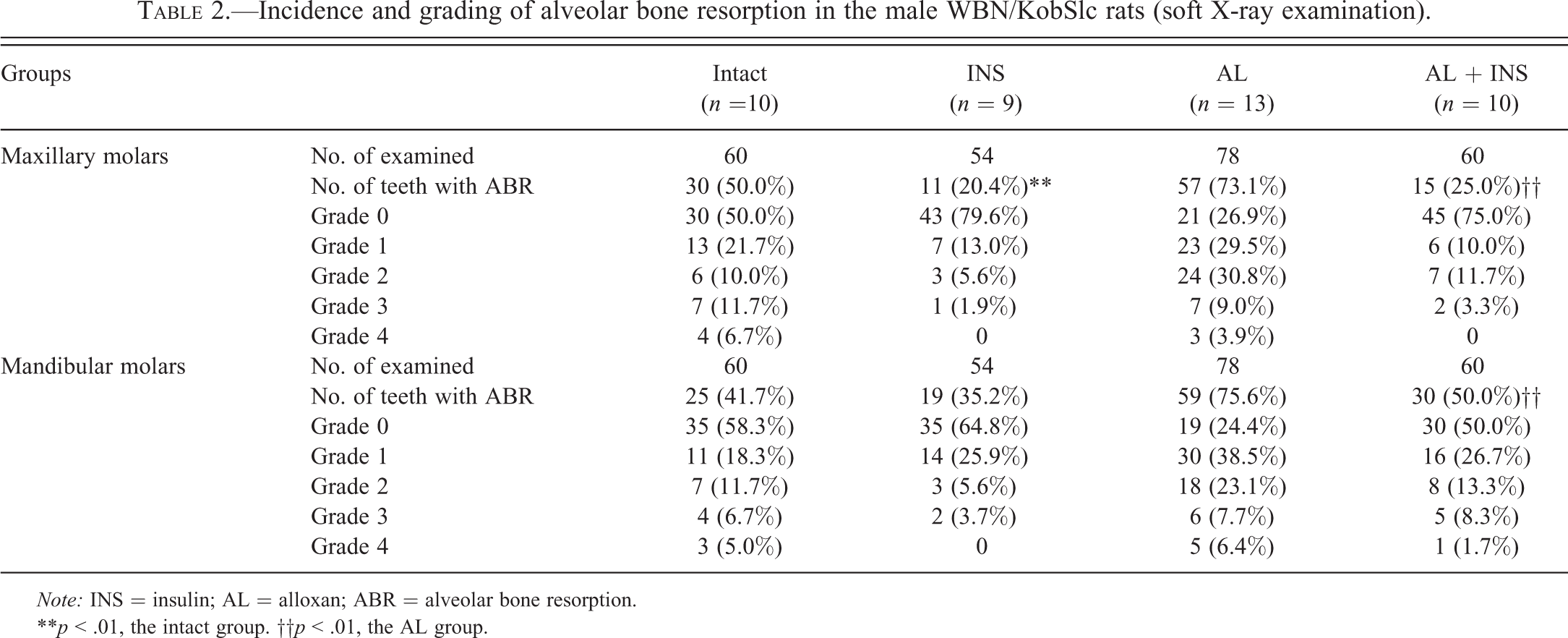
Note: INS = insulin; AL = alloxan; ABR = alveolar bone resorption.
**p < .01, the intact group. ††p < .01, the AL group.
Histopathological Findings
The incidence of dental and periodontal lesions is summarized in Table 3. Similar to the results of soft X-ray examination, the incidences of diabetes-enhanced dental caries and periodontal inflammation were also suppressed in the histopathology for both the insulin-treated groups. The incidences of caries lesions were 44.4% and 52.5% in the INS and AL + INS group, respectively, and significantly lower (p < .01; p < .01) in comparison with those in the intact (72.8%) and AL groups (100%). Many of the caries lesions in all of the groups were moderate to severe, such as the dentin caries developing into pulpitis and pulp necrosis or a completely decayed crown. In many carious teeth, the inflammatory changes expanded the pulp through the apical foramen to the apical tissue, and apical periodontitis developed (Figure 6A and C). The incidences of apical periodontitis were 30.6% and 35.0% in the INS and AL + INS group, respectively, and significantly lower (p < .05; p < .01) in comparison with those in the intact (43.3%) and AL groups (70.5%). Moderate apical inflammation expanded into the surrounding periodontal tissue, and the lesions were usually accompanied by alveolar bone resorption with widening of the periodontal connective tissue space corresponding to the radiolucent areas in soft X-ray examination (Figures 5A and 6A). The incidence of marginal periodontitis was almost the same as the rate of apical periodontitis, and the incidences in the INS (27.8%) and AL + INS groups (40.8%) were, similarly, significantly lower (p < .05; p < .01) than those in the intact (46.7%) and AL groups (76.4%). The incidence of gingivitis in the INS (79.6%) and AL + INS groups (77.5%) was also significantly lower (p < .05; p < .01) than in the intact (84.2%) and AL groups (100%). The incidence of periodontal lesions accompanying a noncarious molar is shown in Table 4. Almost no periodontal lesions other than gingivitis were detected around the molars without caries (Figure 6B and D). The incidence of gingivitis near the noncarious molars was comparable in the intact and INS groups (Table 4, Figure 7A and B). The AL and AL + INS groups could not be compared because of the absence of noncarious molars in the AL group.
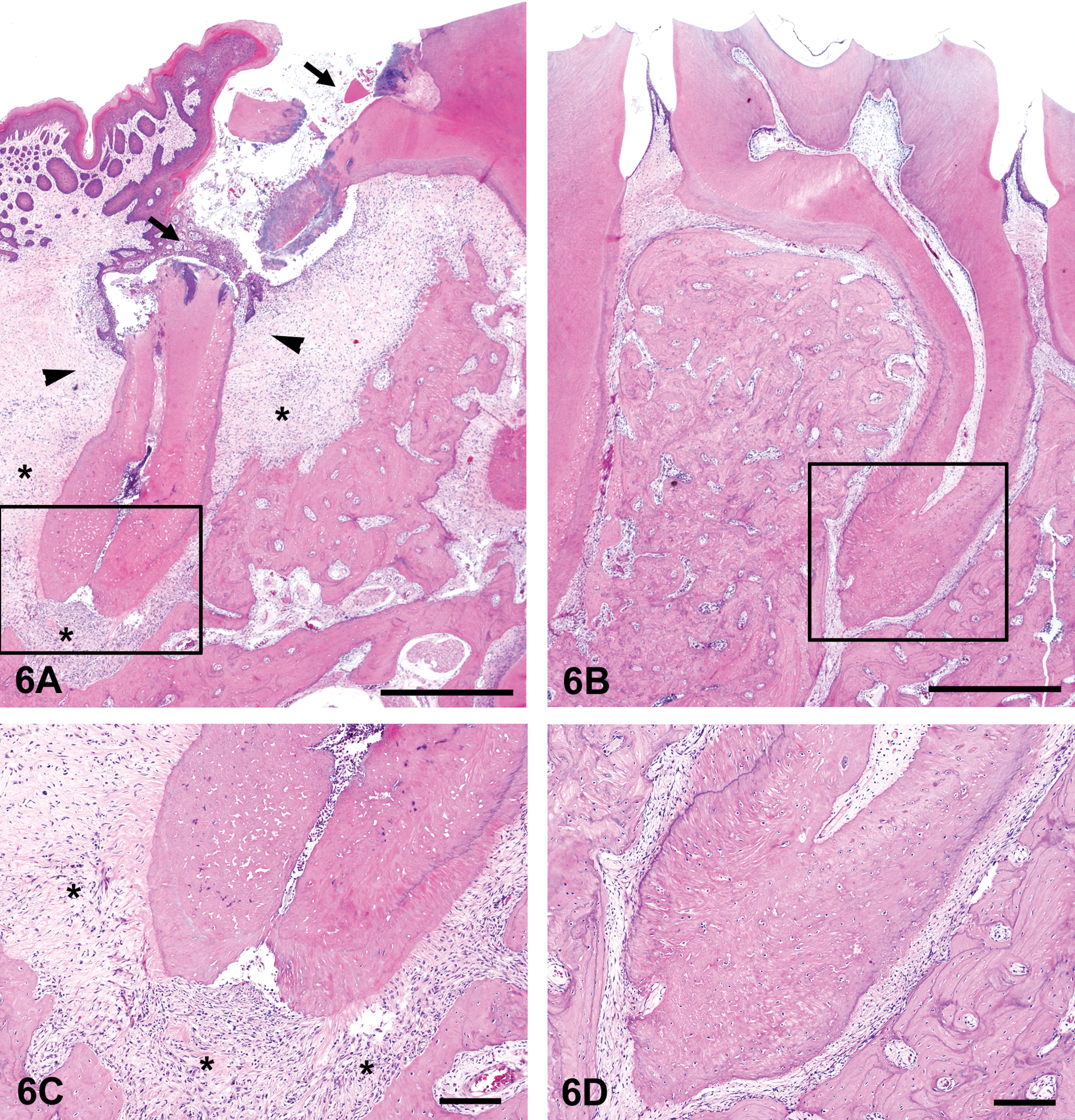
Histopathologic features of the inflammatory lesions in the mandibular periodontal tissues. Boxes in (A) and (B) correspond to (C) and (D). (A), Periradicular tissue adjacent to carious molar (arrows) in a spontaneously diabetic rat (intact group). Note that the inflammatory granulation tissue (asterisks) expands to the space surrounding the dental root, corresponding to the radiolucent area in soft X-ray image. Apical periodontitis is connected with adjacent marginal periodontitis, and marginal periodontitis is combined with gingivitis (arrowheads). Scale bar, 500 µm. (B), Periradicular tissue adjacent to noncarious molar in an insulin-treated diabetic rat (INS group). No change in the periodontal tissues surrounding the dental root of the noncarious molar. Scale bar, 500 µm. (C), Higher magnification of the apical area is shown in (A). Pulpitis spread into the dental root, entered the periodontal connective tissue via the apical foramen, and developed the inflammatory granulation tissue (asterisks) Scale bar, 100 µm. (D), Higher magnification of the apical area is shown in (B). Normal apical periodontal tissue. Scale bar, 100 µm.
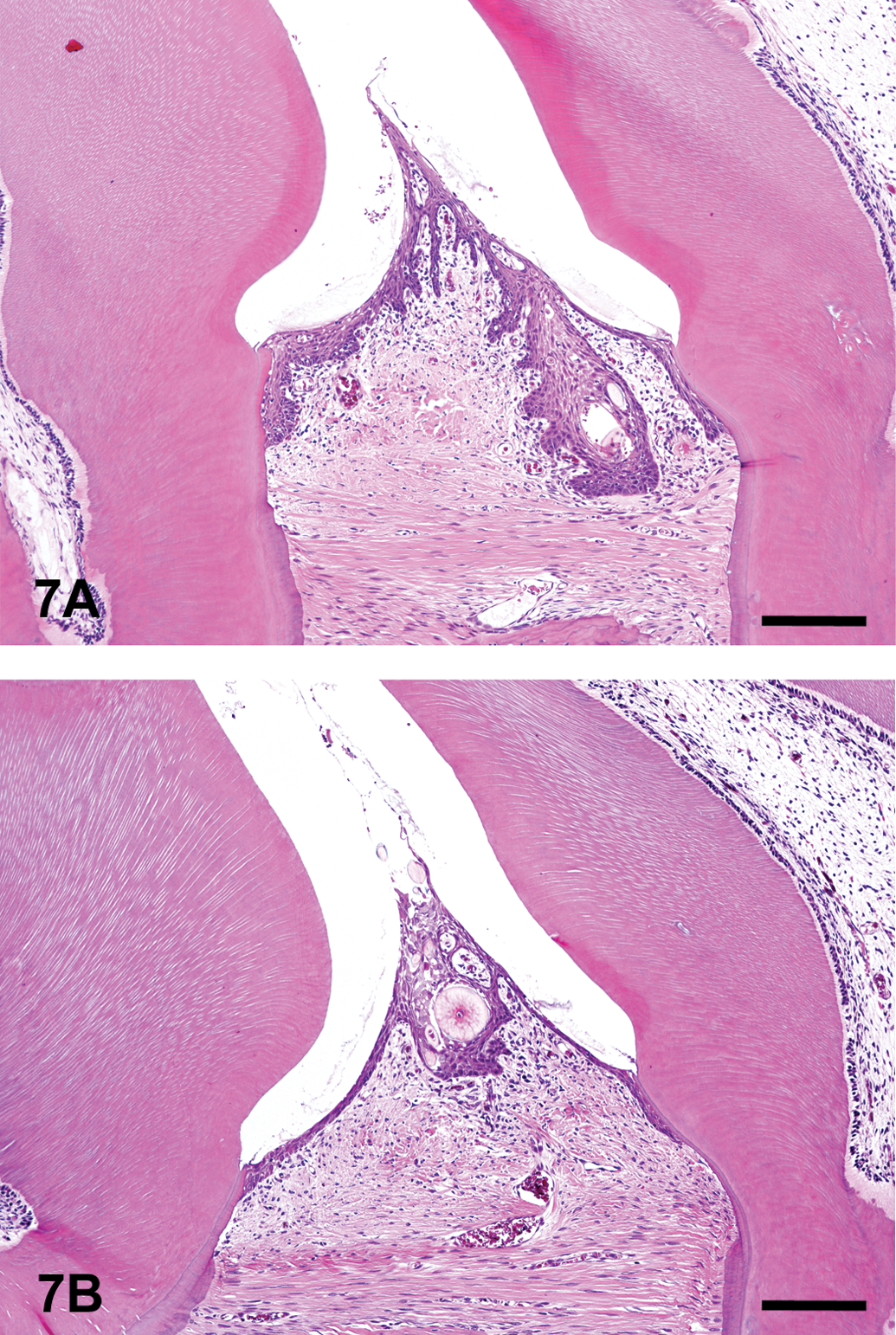
Histopathologic features of the inflammatory lesions in the mandibular gingival tissues adjacent to noncarious molars. (A), Gingival tissue adjacent to noncarious molars in a spontaneously diabetic rat (intact group). Periodontal tissues surrounding the noncarious molars that show mild inflammatory change or are almost normal. Scale bar, 100 µm. (B), Gingival tissue adjacent to noncarious molars in an insulin-treated diabetic rat (INS group). There is no effect of insulin on the periodontal tissues surrounding the noncarious molars. Scale bar, 100 µm.
Incidence of histopathologic lesions in the maxillae and mandibles of the male WBN/KobSlc rats.
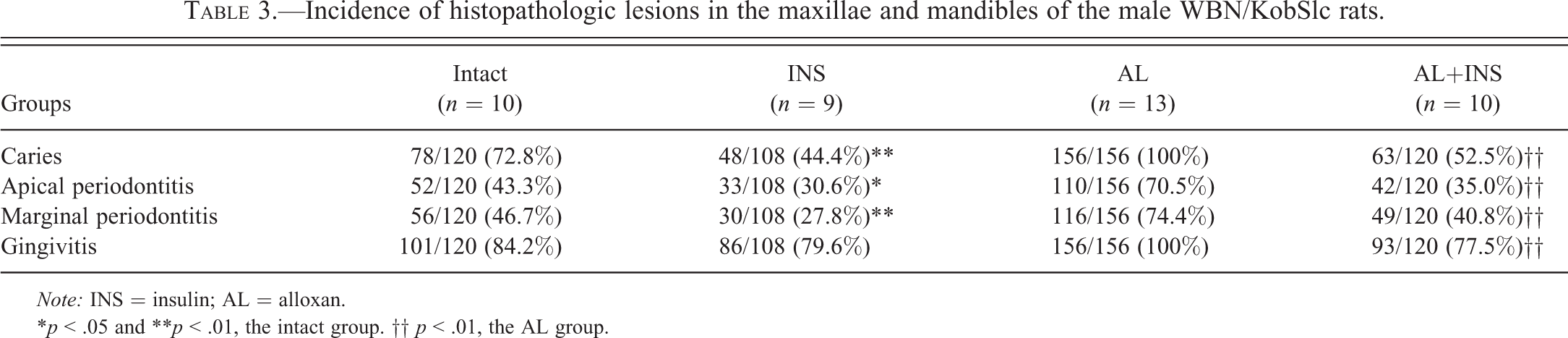
Note: INS = insulin; AL = alloxan.
*p < .05 and **p < .01, the intact group. †† p < .01, the AL group.
Incidence of histopathologic lesions surrounding the noncarious molars in the maxillae and mandibles of the male WBN/KobSlc rats.

Note: INS = insulin; AL = alloxan.
No significant difference between the groups.
Discussion
In the present study, a spontaneously or chemically induced diabetic condition was strongly associated with a higher incidence and severity of dental caries, as was noted in our previous reports (Kodama et al. 2011; Nakahara et al. 2012; Sano et al. 2011). Compared to the caries incidences of age-matched nondiabetic female WBN/KobSlc (mandible, <30%; maxilla, <4%) and F344 rats (both mandible and maxilla; <4%) in our previous study (Kodama et al. 2011), diabetic male WBN/KobSlc rats in this study had a much higher incidence of dental caries. In addition, when the hyperglycemic condition was ameliorated by glycemic control with insulin, the incidence and severity of dental caries in the spontaneously diabetic rats were mildly (only in the maxilla) and markedly (both in the mandible and maxilla) decreased in the alloxan-induced diabetic rats. Thus, it is highly probable that the lack of glycemic control is a major factor contributing to the onset and progression of dental caries.
Although the pathogenesis of dental caries in diabetic patients and animals has not been fully elucidated, it is well known that diabetic patients are predisposed to various infectious diseases (Sentochnik and Eliopoulos 2005). Diabetic animals are also especially susceptible to bacterial and fungal infections (Saiki et al. 1980; Sano et al. 2009a). Meanwhile, it has been suggested that good glycemic control with insulin therapy decreases susceptibility to infection in diabetic humans and animals (Lewis et al. 2004; Sano et al. 2009b). Considering that dental caries is an infectious disease caused by oral cariogenic bacteria (Tanzer 1995), it is likely that the improvement of the compromised immune system in diabetic animals because of reduced hyperglycemia resulting from insulin treatment may have prevented the onset and progression of dental caries in this study.
There are some reports suggesting that periodontal disease similar to that in diabetic humans can be induced in diabetic rodents (Claudino et al. 2007; Pontes Andersen et al. 2006; Tesseromatis et al. 2009). In our present study, periodontal inflammation and alveolar bone resorption were also observed in the diabetic WBN/KobSlc rats. The incidence of these lesions was reduced in the insulin-treated diabetic rats. However, the incidences of marginal periodontitis and alveolar bone resorption were highly correlated with that of apical periodontitis, and apical and marginal periodontitis were frequently connected. Furthermore, almost no marginal periodontitis was observed around the molars without caries, and insulin treatment had no effect on the incidence of periodontal inflammation surrounding the noncarious molars in the spontaneous model of diabetes. Histopathologic evidence in our previous and present studies showed that the inflammatory changes of crown caries origin extend across the apical foramen and the resultant apical periodontitis. Apical periodontitis occurred due to pulpal infection, which is caused by dental caries or traumatic injuries in human (Basavaraj, Chandrasheker, and Khuller 2010; Shenoy and Shenoy 2010). In experimental animals, apical periodontitis is also produced by experimental destruction of corona dentis and exposure of dental pulp, and apical inflammation in diabetic rats were more severe than that in nondiabetic controls (Armada-Dias et al. 2006; Kohsaka et al. 1996). Additionally, advanced gingivitis and marginal periodontitis may result from mechanical irritation of the gingival and periodontal tissues due to the destruction of dental crown and multiple stimuli, such as impact of foreign materials (hair shafts or food particles), microorganism accumulation in diabetic animals. These results suggest that the prevention of dental caries by glycemic control with insulin may reduce caries-derived periodontal inflammation in diabetic rats.
In conclusion, glycemic control by insulin treatment prevented the occurrence and progression of dental caries and caries-related periodontitis in spontaneously and chemically induced diabetic rats, suggesting that hyperglycemia may be a major factor influencing the development of dental caries.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.