
Abstract
Cardiovascular disease is the leading cause of death in the United States and worldwide. High incidence of cardiovascular diseases has been linked to populations with elevated arsenic content in their drinking water. Although this correlation has been established in many epidemiological studies, a lack of experimental models to study mechanisms of arsenic-related cardiovascular pathogenesis has limited our understanding of how arsenic exposure predisposes for development of hypertension and increased cardiovascular mortality. Our studies show that mice chronically exposed to drinking water containing 100 parts per billion (ppb) sodium arsenite for 22 weeks show an increase in both systolic and diastolic blood pressure. Echocardiographic analyses as well as histological assessment show concentric left ventricular hypertrophy, a primary cardiac manifestation of chronic hypertension. Live imaging by echocardiography shows a 43% increase in left ventricular mass in arsenic-treated animals. Relative wall thickness (RWT) was calculated showing that all the arsenic-exposed animals show an RWT greater than 0.45, indicating concentric hypertrophy. Importantly, left ventricular hypertrophy, although often associated with chronic hypertension, is an independent risk factor for cardiovascular-related mortalities. These results suggest that chronic low-level arsenite exposure promotes the development of hypertension and the comorbidity of concentric hypertrophy.
Introduction
High incidence of cardiovascular diseases has been linked to populations with elevated arsenic content in their drinking water. Chronic arsenic exposure is connected with an array of diseases, ranging from multiple types of cancer to cardiovascular diseases such as blackfoot disease, atherosclerosis, hypertension, as well as diabetes and developmental effects (Abernathy et al. 1999; Mandal and Suzuki 2002). For this reason, exposure to environmental arsenic is a worldwide public health concern and further understanding of arsenic toxicity will help prevent or reverse associated diseases. Currently, the maximum contaminant level (MCL) for arsenic in drinking water in the United States is 10 parts per billion (ppb), which was set by the U.S. Environmental Protection Agency (EPA; 2001), reducing the MCL from the previous standard of 50 ppb prior to 2006. Importantly, these regulations are established largely on the carcinogenic properties of arsenic, and not on the cardiovascular risk associations, which have been shown to be present at lower levels than those necessary for cancer development, both in humans and mice (Medrano et al. 2010; Soucy et al. 2005).
It is critical to study the chronic effects of low-level arsenic exposure to further understand its detrimental properties on exposed populations throughout the world. Some detrimental effects such as hypertension and cardiovascular-related mortalities have been studied in arseniasis hyperendemic villages (Chen et al. 1995, 1996, 2011; Medrano et al. 2010; Rahman et al. 1999). For example, epidemiological studies by Chen et al. and Rahman et al. show strong correlations between long-term arsenic exposure and increased incidence of hypertension in a dose-response dependent manner. Similarly, Smith’s group found a significant increase in cardiovascular-related mortalities that paralleled elevated arsenic exposure through drinking water in the region II area of Chile (Yuan et al. 2007). Additional studies done by Kwok et al. have shown a significant increase in both systolic and diastolic blood pressure in healthy women consuming 50–100 ppb arsenic from the drinking water (Kwok et al. 2007). Furthermore, the relationship between arsenic exposure and cardiovascular diseases has been a subject of interest and is further described in excellent reviews (Navas-Acien et al. 2005; States et al. 2009).
Cardiovascular disease is the leading cause of death in the United States (Heron et al. 2009; Murray and Lopez 1997). An estimated 74.5 million people over the age of 20 years, or one in three adults in the United States, have high blood pressure (hypertension), as defined by an uncontrolled systolic pressure above 140 mmHg or diastolic pressure above 90 mmHg (Chobanian et al. 2003). An additional 25% of the population is considered pre-hypertensive, as defined by systolic pressure between 120 and 139 mmHg or diastolic pressure between 80 and 89 mmHg (Lloyd-Jones et al. 2010). Hypertension is one of the main risk factors that contribute both to heart disease and stroke. Heart disease and stroke are the first and third leading causes of death in the United States (National Center for Health Statistics 2011). Furthermore, hypertension is one of the primary pathological causes of left ventricular hypertrophy (LVH), a cardiac manifestation of pressure overload characterized by thickening of the ventricular wall, often resulting in impaired cardiac function and increased cardiovascular risk. Increased ventricular mass, such as that seen in concentric left ventricular hypertrophy, is a strong predictor of cardiovascular events and associated deaths, independent of other risk factors (Casale et al. 1986; Koren et al. 1991). Thus, if hypertension is observed due to chronic exposure to arsenic, we predict a concomitant detection of cardiac hypertrophy.
While hypertension is easily detectable and usually controllable, the American Heart Association has reported that the cause of 90–95% of high blood pressure cases is unknown (Carretero and Oparil 2000). High blood pressure can occur because of many factors such as lifestyle, genetics, and diet. Additionally, environmental pollutants have been previously associated with cardiovascular diseases, although their contribution is less clear. In this study, we show that chronic exposure to arsenic contributes to the onset of hypertension and consequent development of LVH in mice.
Since some epidemiological studies have been shown to have inconclusive evidence and often have significant methodological limitations (Navas-Acien et al. 2005), a degree of uncertainty still remains in the field regarding the cardiotoxic impact of arsenic. Therefore, controlled experimentation is needed to determine if chronic arsenic exposure induces cardiovascular outcomes such as hypertension. Importantly, we believe that arsenic-induced hypertension should parallel development of cardiac hypertrophy. In this study, we evaluate the cardiovascular effects of chronic exposure to low-level arsenic exposure (100 ppb) in mice through drinking water for 22 weeks. To our knowledge, this is one of the first studies looking at blood pressure changes in a mouse model exposed to environmentally relevant arsenic concentrations over a long period of time. Our findings show arsenic is a primary trigger for hypertension and cardiac hypertrophy, highlighting that cardiovascular toxicity needs to be considered in regard to setting acceptable arsenic exposure levels.
Materials and Methods
Animals and Treatments
FVB female mice were purchased from Harlan (Harlan Laboratories Inc., WI, USA). Mice were housed in sterile microisolator cages and provided diet (2019 Teklad Global 19% Protein Extruded Rodent Diet, Harlan Laboratories Inc.) and water ad libitum with either 100 ppb of sodium arsenite (NaAsO2, Sigma, St. Louis, MO, USA) or 100 ppb sodium chloride (NaCl, VWR, Aurora, CO, USA) as indicated. Water was purified through reverse osmosis and water packs were replaced weekly. Mice were exposed to treatments starting at weaning age and maintained on treatment for 22 weeks. The amount of arsenic consumed by each animal was not measured, although arsenic concentration in the drinking water was analyzed. Water samples were collected fresh after preparation from the treatment and control water packs, and additional samples were collected after 7 days, prior to replacing the water packs. These samples were stored at –80°C until analysis for arsenic content and speciation by inductively coupled plasma mass spectrometry (ICP-MS) at the analytical section of the hazard identification core of the NIEHS Superfund program. Mice were weighed weekly prior to acclimation for blood pressure studies. Animals were euthanized by CO2 asphyxiation and cervical dislocation. All animal use and experimental protocols followed University of Arizona Institutional Animal Care and Use Committee (IACUC) regulations and remained in accordance with institutional guidelines.
Measurement of Blood Pressure
Systolic and diastolic blood pressure were measured weekly on arsenic-treated and control mice while conscious using a volume pressure tail cuff transducer system coupled to a computerized data acquisition software (Coda High-Throughput, Kent Scientific Corporation, Torrington, CT, USA). This noninvasive method has been previously shown to produce reproducible data consistent with intra-arterial blood pressures (Krege et al. 1995).
Mice were placed in restraining tubes and tail cuffs were placed on their tails 10 minutes prior to each session to allow them to acclimate. Sessions of 25 cycles were done, where the first 10 cycles were not recorded and helped the mice get accustomed to the tail cuff method. Out of the recorded cycles, the highest and lowest readings and any readings associated with excess noise or animal movement were discarded, and then readings were averaged together to obtain weekly measurements as described (Pollock and Rekito 1998). Each session included 2 control and 2 arsenic-treated mice simultaneously on independent restraining tubes and tail cuffs to account for intersession variability due to handling.
Echocardiography and Anesthesia
Mice were anesthetized using a rodent isofluorane anesthesia instrument with a vaporizer, induction chamber, and mouse nose cone. Oxygen was coadministered with isofluorane. The vaporizer was set to 3% during induction and reduced down to 1.5% for maintenance during echocardiography procedure. Eyes were protected with lubricant to prevent corneal damage. Mice were secured and shaved using Nair lotion on a heated board that allowed for acquisition of vital physiological parameters such as respiratory rate, heart rate, and ECG.
Transthoracic echocardiography was done on anesthetized mice using the Vevo2100 high-resolution ultrasound imaging system (Visualsonics, Toronto, Ontario, Canada) equipped with the MS550D transducer (22–55 MHz) to assess cardiac morphology in the short axis view in M-mode images. Left ventricular (LV) mass was calculated from cineloop recordings by delineating LV walls from a minimum of four beats during the postexpiratory pause of the respiration cycle. Averages were obtained from measuring 3 independent views per mouse. Left ventricular posterior and anterior walls were measured in accordance with the American Society of Echocardiography recommendations (Sahn et al. 1978), and ventricular mass was determined using the following formula:


where a minimum of 20 cardiac cycles per mouse were used to measure end diastolic LV diameter and wall thickness. Calculations for RWT were based on measurements obtained in B-mode. Concentric hypertrophy was determined as traditionally defined to be (RWT ≥ 0.45) (Koren et al. 1991; Ganau et al. 1992). RWT data was calculated per individual mouse.
Tissue Sectioning and Histological Measurements
Hearts were harvested and rinsed in phosphate buffered solution (PBS, Mediatech, Herndon, VA, USA) and fixed in 4% paraformaldehyde (Fisher, Fair Lawn, NJ, USA) overnight. Fixed tissue was embedded in Paraplast 56°C (McCormick Scientific, St. Louis, MO, USA), and sectioned in the transverse plane into 10-µm sections using a microtome (HM 325 Microtom, Thermo Scientific, Waltham, MA, USA). Midsections of the ventricles were compared between hearts using papillary muscles as reference point. Heart sections were deparaffinized, rehydrated, and stained with hematoxylin and eosin (Thermo Scientific, Waltham, MA, USA). Gross heart morphology was captured using a dissecting microscope at 3x magnification. Interventricular septum (IVS) measurements were obtained at a 5x magnification using a Leica DFC320 camera linked to a Leica DM 2500 microscope. Measurements were done through the midsection of the heart with close attention to excluding protruding tissue as shown in detail in Figure 3D. Over 70 measurements were obtained from serial sections for each treatment group. Averages were calculated and standard deviations were obtained.
Data Analysis
Data acquisition for blood pressure measurements was obtained from the CODA software, exported into Microsoft Excel 2007 as comma separated values (.csv) files. Internal parameters of the CODA software were used to exclude and discard abnormal readings as described earlier. The remaining values were averaged together for control group (n = 5) and arsenic-treated group (n = 8), and standard deviations were obtained per group for each week. Echocardiographic measurements were done from the cineloop images where measurements were collected and averaged on Microsoft Excel. Comparison of blood pressure changes over time was analyzed by repeated measures analysis of variance (ANOVA). Average systolic and diastolic blood pressure, LV mass, IVS lengths, and RWT averages were compared using one-tailed Student’s t-test at a significance level of p ≤ .05.
Results
Arsenic Increases Blood Pressure
Epidemiologic reports show a connection between communities exposed to environmental arsenic and increased incidence of hypertension as well as morbidities related to heart disease (Chen et al. 1995, 1996; Medrano et al. 2010; Rahman et al. 1999). However, the magnitude of the direct association is uncertain because of limitations in the methodology inherent in many of these population studies. To determine whether there is a direct link between chronic exposure to low doses of arsenic in a controlled setting, mice were exposed to 100 ppb NaAsO2 or 100 ppb NaCl for controls, and cardiovascular endpoints were examined. While total arsenic consumed throughout the study was not assessed, arsenic concentration and speciation in the drinking water was determined through ICP-MS several times throughout the study, and arsenic content remained stable in the trivalent form (Table 1). Systolic and diastolic blood pressures were examined to determine whether chronic exposure to low-level arsenite impacted cardiovascular physiology in our rodent model.
ICP-MS results for total arsenic content and speciation.
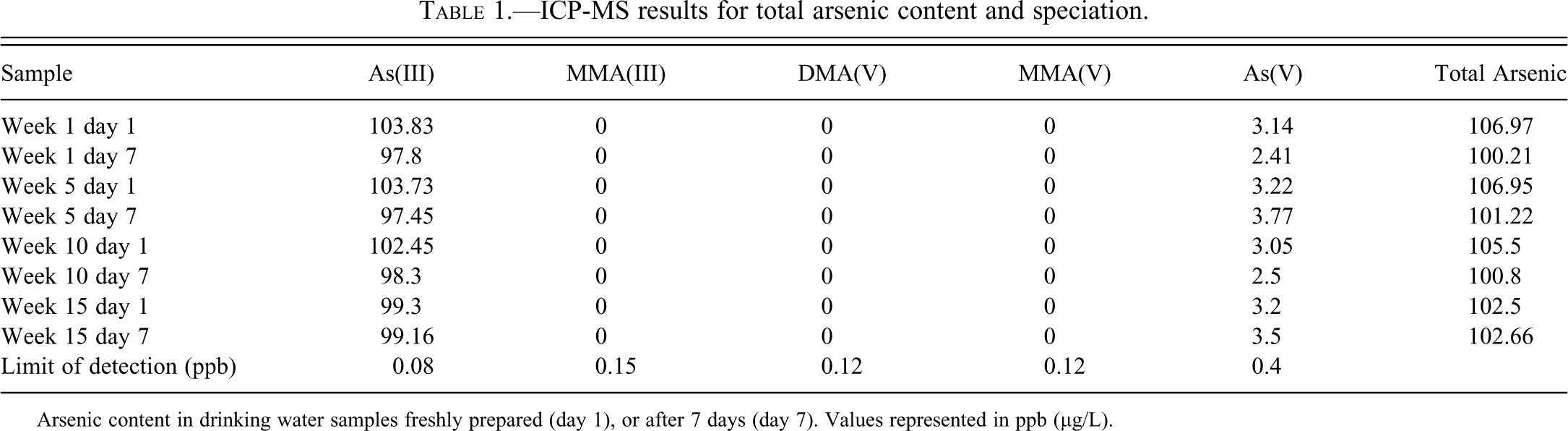
Arsenic content in drinking water samples freshly prepared (day 1), or after 7 days (day 7). Values represented in ppb (µg/L).
Control and arsenic-exposed animals had essentially similar systolic and diastolic pressure at the start of the study (127/88 mmHg and 116/86 mmHg, respectively). Systolic (squares) and diastolic (circles) blood pressure in arsenic-treated animals (black lines) increased significantly and by 4 weeks of exposure, they remained above controls (gray lines) (Figure 1A). This hypertensive response in arsenic-treated mice was maintained throughout the 22-week period. Repeated measures ANOVA was done, showing that 100 ppb arsenic exposure promoted a statistically significant increase in systolic blood pressure (p = .032). The change in diastolic blood pressure did not reach significance (p= .051), although a trend for elevated pressure was observed. Blood pressure data obtained throughout the study were averaged per treatment group (Figure 1B). The averaged blood pressures for control mice had normotensive values of 116/93 mmHg. In contrast, arsenic-exposed mice showed significantly elevated blood pressure of 150/115 mmHg. The increase in blood pressure observed in arsenic-treated animals was statistically significant for systolic values (p < .05), but not for diastolic ones.
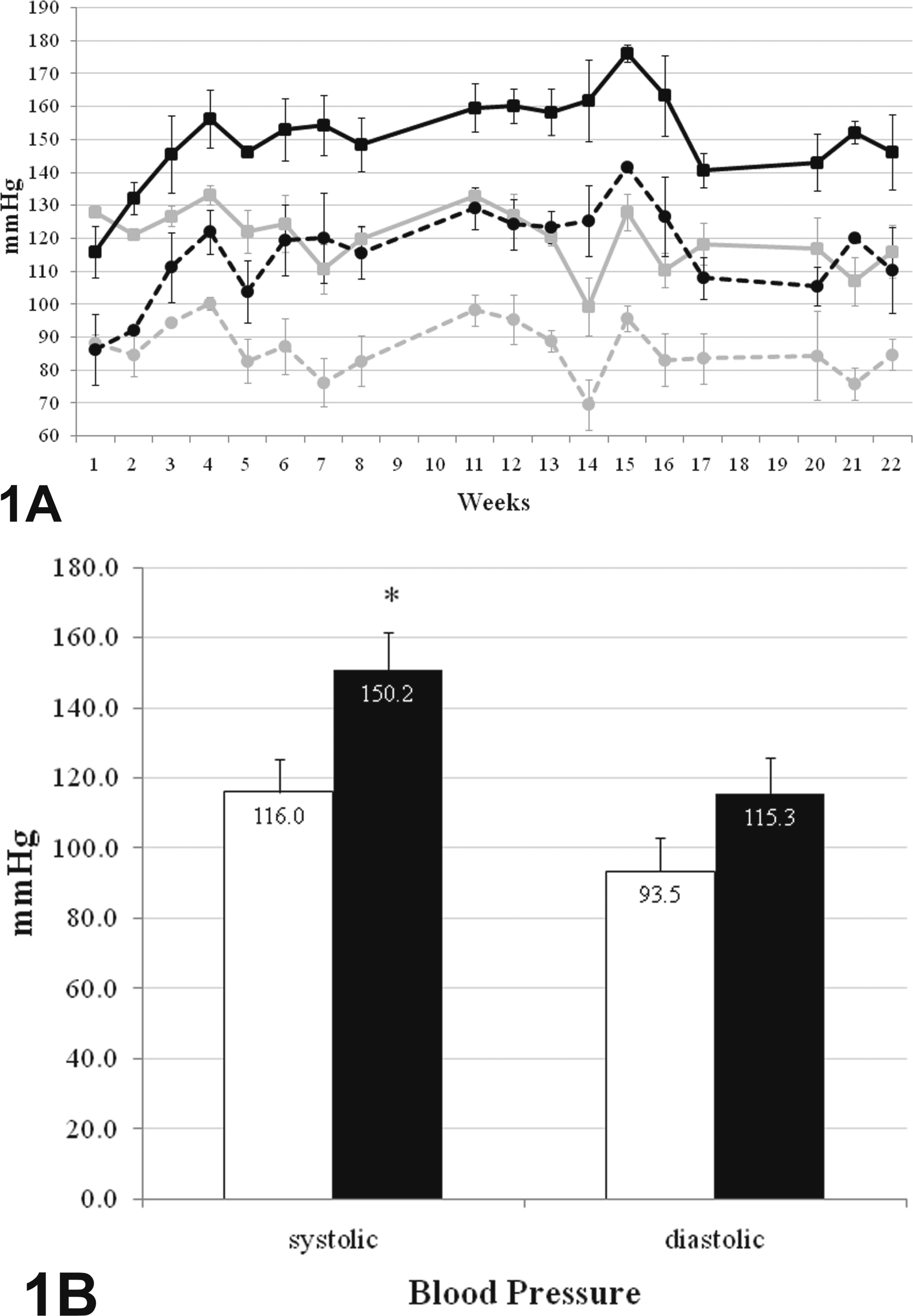
Arsenic exposure triggers hypertension. A. Blood pressure data shown for both control (gray) and arsenic-reated (black) mice throughout the 22-week exposure. Average systolic (squares) and diastolic (circles) blood pressures are shown with respective standard deviations. B. Summarized averages after concluding exposure are shown for systolic and diastolic blood pressure. Control (white); arsenic-treated (black). *p < .05.
Arsenic Promotes Left Ventricular Hypertrophy
Mice were subjected to echocardiographic analysis after the 22 weeks of arsenic exposure. Representative M-mode images for both controls and arsenic-treated mice are shown illustrating tracings of posterior and anterior ventricular walls (Figure 2). We calculated the aggregate increase in LV mass in control (Figure 2A) and arsenic-exposed mice (Figure 2B) and found a significant increase of 43% in LV mass in arsenic-exposed mice (p < .05) (Figure 2C). Importantly, this increase in LV mass did not correlate with any significant changes in body weight. These observations strongly suggest that arsenic promotes hypertension and subsequent hypertrophic cardiac remodeling. To further characterize cardiac changes, IVS lengths were measured in histological sections of hearts from control (Figure 3A, 3C) and arsenic-treated mice (Figure 3B, 3D). The average IVS length for control mice was 0.94 mm, whereas the average IVS length for arsenic-treated mice was 1.12 mm. This 19% increase in IVS length was found to be significant (p < .05) (Figure 3E). Histological assessment of interventricular septum supports the echocardiography results showing thickening of the ventricular wall of hearts in arsenic-treated mice, which is a hallmark of cardiac hypertrophy.
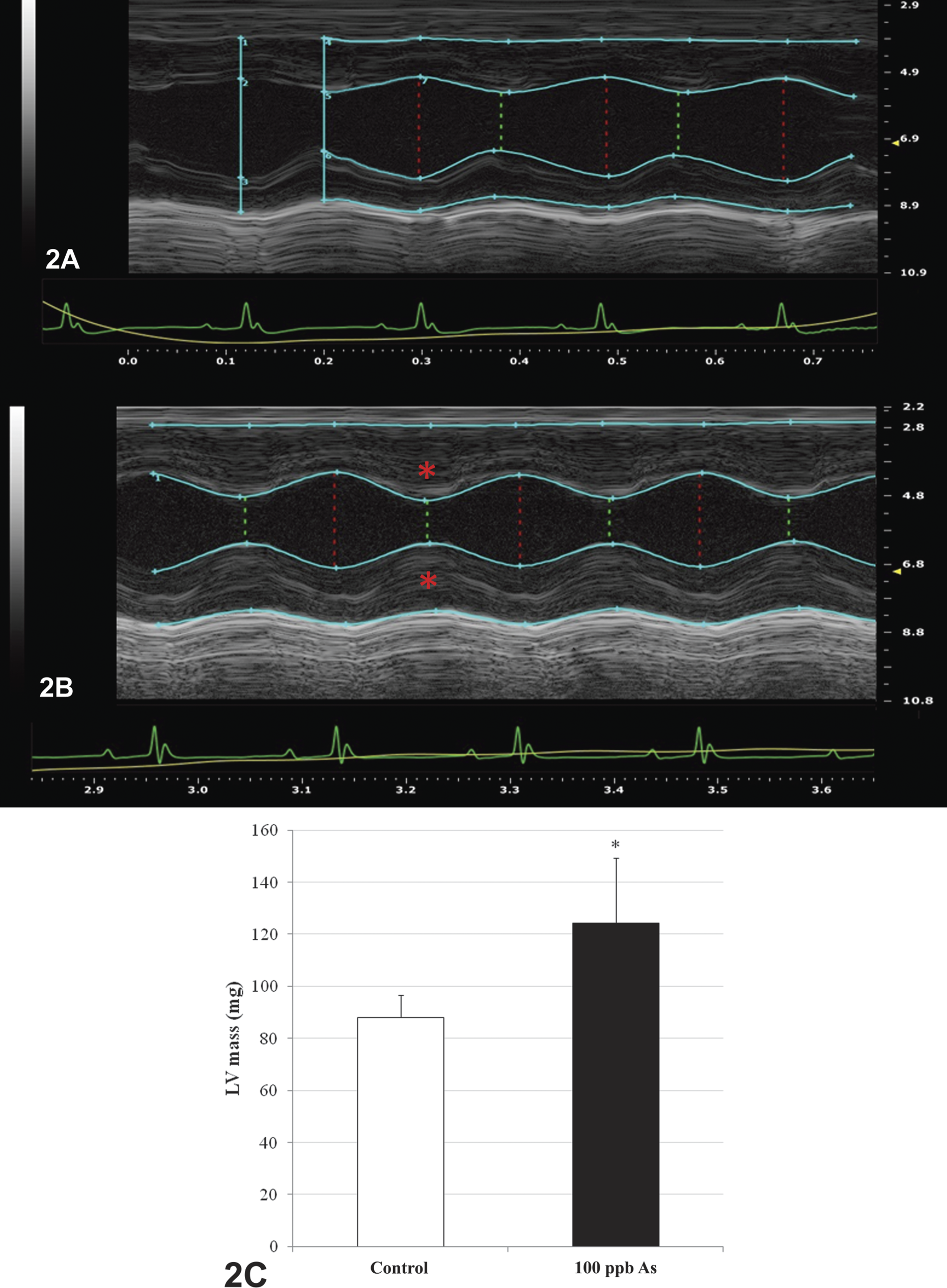
Echocardiographic analysis shows increased LV mass in arsenic-treated mice. A, B. M-mode short axis view of control (panel 2A) and arsenic-treated (panel 2B) left ventricle cineloop image. Teal tracings represent LV wall through systole (green dotted line) and diastole (red dotted line). Ventricular wall in treated animals (red asterisks) is substantially thicker than that of control animals. C. Average LV mass from control (white) and arsenic-treated (black) mice were calculated as described in the methods section. A significant increase (43% above control) was observed in arsenic-treated mice (p ≤ .05).
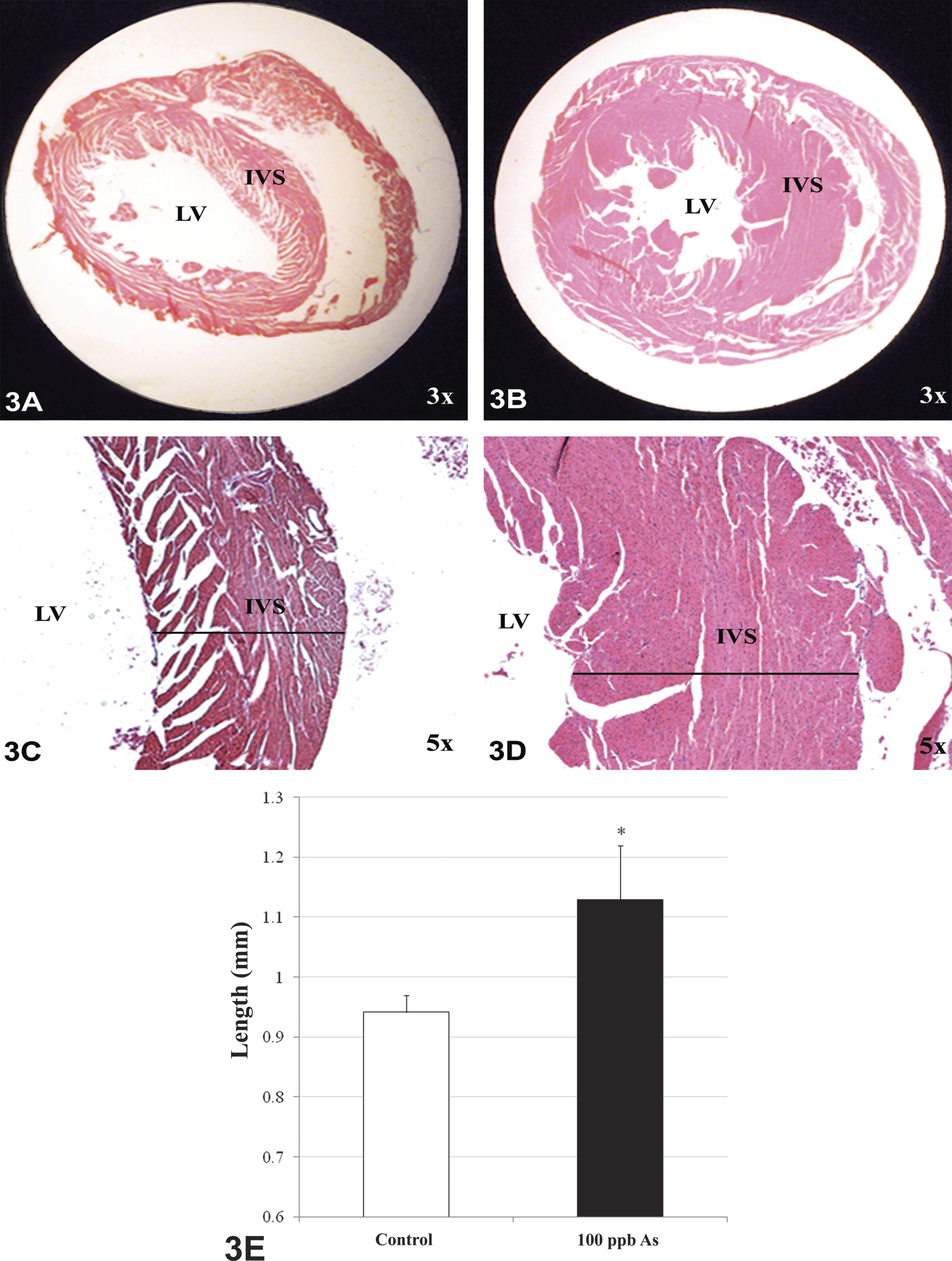
Histological assessment confirms left ventricular hypertrophy in arsenic-treated mice. Hearts were stained with hematoxylin and eosin to assess degree of IVS thickening. Control mice (A, C) showed an average interventricular septum (IVS) length of 0.94 mm, and arsenic-treated mice (B, D) had an average IVS of 1.12 mm. A significant increase in IVS lenght (19% above control) was observed in arsenic-treated mice (p ≤ 0.05).
To further evaluate left ventricular hypertrophy, we determined whether this hypertrophy was eccentric or concentric remodeling. While eccentric hypertrophy is often associated with volume overload, concentric hypertrophy is typically associated with pressure overload, such as that seen in chronic hypertension (Grossman, Jones, and McLaurin 1975). Concentric hypertrophy is classically seen in hypertensive patients and is considered to be an independent cardiovascular risk factor. Furthermore, concentric hypertrophy is associated with poor prognosis for hypertensive patients (Verdecchia et al. 1995). Therefore, ventricular wall thickness was measured in relation to left ventricular end diastolic diameter obtained by echocardiography to calculate RWT (Figure 4), where a value above 0.45 is considered concentric hypertrophy (Koren et al. 1991; Ganau et al. 1992). Four of the five control animals (open bars) had RWT below the threshold of 0.45, indicating an absence of concentric hypertrophy. In contrast, 100% of the arsenic-exposed animals (black bars) showed RWT values greater than 0.45. These arsenic-treated animals show a significant susceptibility for concentric ventricular hypertrophy when compared with control animals (p < .01). Collectively, these observations indicate that chronic exposure to low-dose arsenic promotes the development of concentric left ventricular hypertrophy.
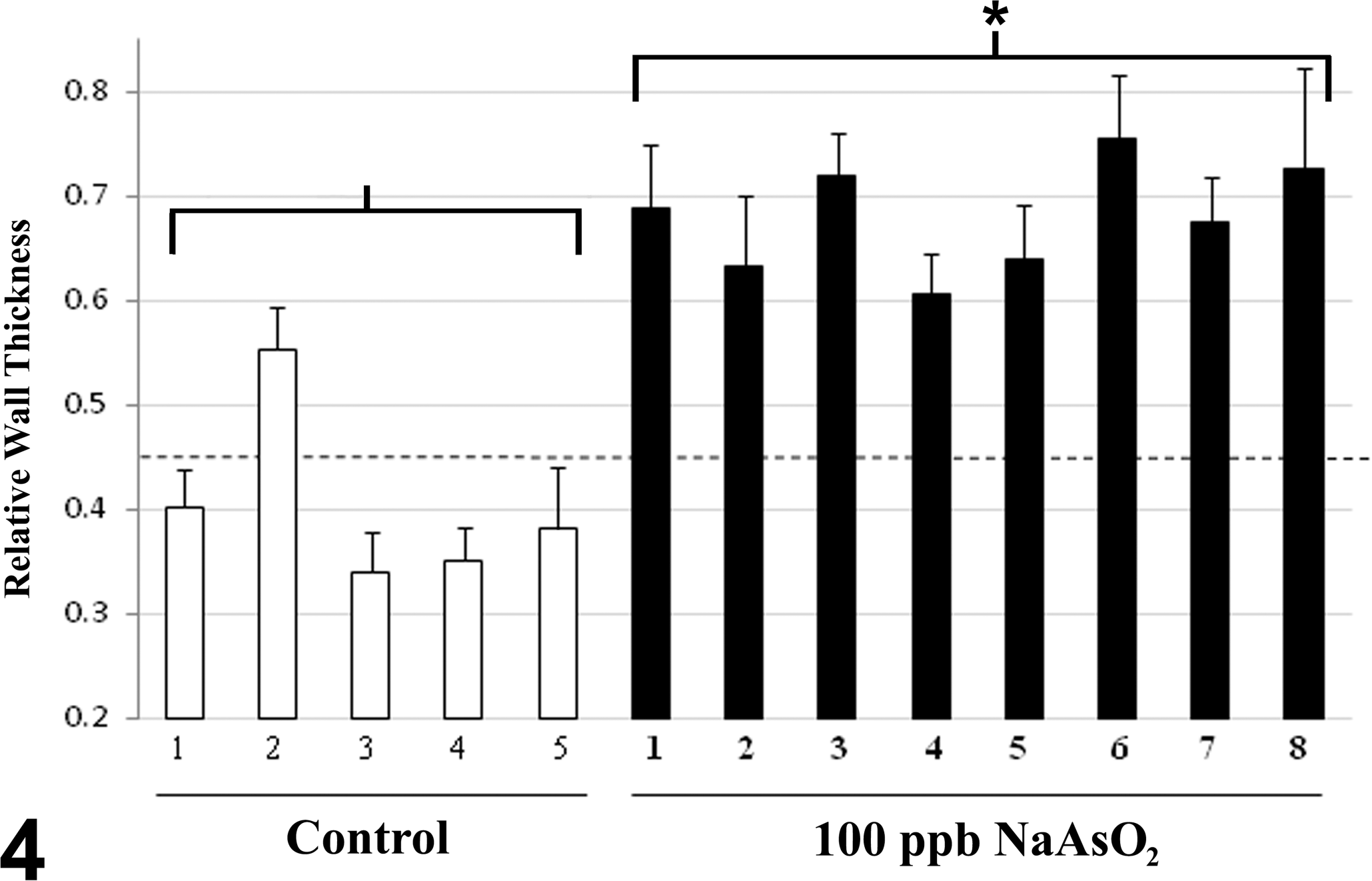
Arsenic exposure promotes concentric hypertrophy. Relative wall thickness (RWT) was calculated for each animal. Control mice (open bars) show normal values of RWT. In contrast, all arsenic-treated animals (black bars) show substantial increase in RWT indicating concentric hypertrophy (RWT > 0.45, dotted line).
Discussion
Inorganic arsenic is one of the most abundant toxic metals in our environment. It is implicated in a wide range of health ailments including multiple types of cancer, hypertension, atherosclerosis, and severe forms of peripheral vascular diseases such as blackfoot disease (Mandal and Suzuki 2002). Epidemiologic studies on the blackfoot disease arseniasis-hyperendemic villages along the southwestern coast of Taiwan are characterized by chronic exposure to arsenic-contaminated drinking water. In several of these studies, ischemic heart disease was found to be strongly associated with chronic exposure to arsenic (Tseng et al. 2003). Smith’s group studied the region II area of Chile where there was a specific period of high arsenic exposure in the public drinking water (1958–1970) and found a very significant increase in cardiovascular diseases (Yuan et al. 2007). Specifically, mortality from acute myocardial infarction paralleled the onset of exposure, showing that acute myocardial infarction deaths increased largely after exposure to elevated arsenic levels in the drinking water. Furthermore, cardiovascular-related deaths remained significantly elevated in this population, suggesting that arsenic exposure had long-term detrimental effects on cardiovascular health. This incidence was shown to remain elevated for 10 years after onset of exposure and declined following purification of arsenic out of the public water supply. Similarly, Chang observed a decrease in cardiovascular mortality rates in Taiwan after a reduction of arsenic in drinking water was accomplished (Chang et al. 2004). The incidence of cardiovascular-related mortalities discovered by these studies strongly suggests that low-level arsenic exposure poses a significant harm to humans, increasing the risk of developing cardiovascular diseases.
The onset of arsenic-induced cardiovascular diseases is not completely clear. Furthermore, the pathogenic mechanisms and physiological effects from arsenic ingestion at low concentrations commonly found in the United States remain ambiguous. Our in vivo study, using controlled and consistent exposure to 100 ppb arsenite in drinking water, shows disruption of cardiovascular homeostasis over a period of several months. To our knowledge, this is the first animal study looking at the effects of chronic exposure to environmentally relevant concentrations of arsenic to assess cardiovascular outcomes such as the development of hypertension and LVH. While previous studies have shown arsenic effects on vascular resistance and cardiac function, the doses used in these studies are at much higher levels and fail to represent environmentally relevant concentrations (Carmignani, Boscolo, and Castellino 1985).
We observed blood pressure changes in our mouse model that are consistent with previously reported epidemiological studies showing increased incidence of hypertension in arsenic-exposed populations (Chen et al. 1995; Rahman et al. 1999). Interestingly, Kwok et al. showed a very similar pattern to what we observed with female mice. In their study, healthy women exposed to elevated levels of arsenic showed a more substantial increase in systolic than diastolic blood pressure (Kwok et al. 2007). Given the similarity in cardiovascular effects observed between our studies, and epidemiological studies showing elevation in blood pressure in humans exposed to low-level arsenite, we believe that our findings could be predictive of concomitant concentric ventricular hypertrophy in human populations exposed to arsenic and should be explored in future epidemiological studies.
A limitation of our study was the minor variation in blood pressure changes during the study, although we observed a consistent trend for elevated blood pressure in mice ingesting arsenic that was maintained above control mice throughout the 22-week exposure. Furthermore, the chronic hypertension is supported by the heart morphological changes observed in the arsenic-treated mice.
Chronic hypertension often causes cardiac changes such as concentric ventricular hypertrophy, which we evaluated during the study. Although cardiac functional changes were not assessed, structural heart changes by both echocardiography, as well as histological assessment show significant concentric hypertrophy. These results were confirmed through two independent methods, and were found strikingly similar (Figures 2C, 3E), strengthening the quality of the data obtained. Moreover, we characterized the geometric changes in the left ventricle and saw characteristic concentric LVH. Importantly, LVH, although often associated with chronic hypertension, is an independent risk factor for cardiovascular-related mortalities (Verdecchia et al. 1995). These results, in conjunction with histological observations support the concept that chronic low-level arsenite exposure disrupts cardiovascular homeostasis in mammals.
Previously, we have reported that chronic low-level arsenic exposure results in down-regulation of extracellular matrix genes important for vascular integrity, such as collagen, elastin, and fibronectin. Consistent with these results, histological assessment confirmed a decrease in extracellular matrix components within the vascular walls of microvessels within the lungs and heart (Hays et al. 2008). This morphological change within the vascular architecture could result in impairment of vasomotor regulation, which would help explain the changes in blood pressure observed in our current study. Alternatively, additional mechanisms of arsenic-induced vascular dysfunction have been described by others. For example, in vitro studies have shown that arsenic, as well as its metabolite, monomethylarsonous acid (MMAIII), cause vascular smooth muscle dysfunction by increasing vasoconstrictor reactivity as well as impairing acetylcholine mediated vasorelaxation (Lee et al. 2003; Bilszta, Dusting, and Jiang 2006; Bae et al. 2008). Both of these reported effects of arsenic would likely result in impairment of blood pressure regulation and could be likely mechanisms contributing to hypertension due to chronic arsenic ingestion. Importantly, both hypertension and LVH have been shown to be associated with impairment in endothelium-mediated relaxation (Treasure et al. 1993). Additional studies have also shown that arsenic negatively influences the production of nitric oxide and reduces endothelial nitric oxide synthase (Lee et al. 2003), an important system necessary for proper smooth muscle relaxation in blood vessels. Furthermore, arsenic has been shown to increase circulating levels of reactive oxygen species (ROS; Wu et al. 2001) and could likely be contributing to endothelial cell dysfunction (Kumagai and Pi 2004).
In our studies, we observe that arsenic had two different effects on the cardiovascular system, causing hypertension and promoting concentric left ventricular hypertrophy. Whether arsenic is promoting concentric left ventricular hypertrophy through additional mechanisms independent of increased blood pressure still remains unclear. The observed cardiovascular dysfunction upon arsenic exposure, is likely a sum of the previously mentioned mechanisms. While our previous study described a novel effect by which arsenic disrupted vascular integrity, and thus a potential mechanism for onset of cardiovascular diseases (Hays et al. 2008), the current study puts those observations in the context of disease, by showing that chronic exposure to environmentally relevant arsenic concentrations results in the development of hypertension and concentric hypertrophy. We are currently utilizing this animal model to further elucidate arsenic-mediated cardiovascular disease onset, and additional molecular mechanisms of cardiovascular toxicities.
Footnotes
Acknowledgments
We would like to acknowledge Dr. Klewer and F. Roger for helpful discussions and Dr. Gandolfi for critical review of the article. Also, we would like to thank Dr. Witte for access to the Vevo2100 ultrasound system and Mike Kopplin and the Analytical Section of the Hazard Identification Core of the NIEHS Superfund Program for performing the ICP-MS analyses.
This work was supported by the National Institute of Environmental Health Science (NIEHS ES-04940) and the Southwest Environmental Health Sciences Center (SWEHSC 006694).