
Abstract
The Society of Toxicologic Pathology (STP) and American Society for Veterinary Clinical Pathology (ASCVP) convened a Clinical Pathology in Carcinogenicity Studies Working Group to recommend best practices for inclusion of clinical pathology testing in carcinogenicity studies. Regulatory guidance documents and literature were reviewed, and veterinary pathologists from North America, Japan, and Europe were surveyed regarding current practices, perceived value, and recommendations for clinical pathology testing in carcinogenicity studies. For two-year rodent carcinogenicity studies, the Working Group recommends that clinical pathology testing be limited to collection of blood smears at scheduled and unscheduled sacrifices to be examined only if indicated to aid in the diagnosis of possible hematopoietic neoplasia following histopathologic evaluation. Additional clinical pathology testing is most appropriately used to address specific issues from prior toxicity studies or known test article–related class effects. Inadequate data were available to make a recommendation concerning clinical pathology testing for alternative six-month carcinogenicity assays using genetically modified mice, although the Working Group suggests that it may be appropriate to use the same approach as for two-year carcinogenicity studies since the study goal is the same.
Introduction
The primary purpose of carcinogenicity studies is to characterize the carcinogenic potential of pharmaceutical and other chemicals. To this end, these studies are typically conducted to provide near-lifetime exposures at dose levels up to the maximum tolerated dose. In addition to the two-year rodent bioassay, alternative carcinogenicity assays such as six-month studies using genetically modified mice have been increasingly used to identify the carcinogenic potential of xenobiotics (Long et al. 2010; MacDonald et al. 2004; Robinson and MacDonald 2001). Clinical pathology parameters are routinely included in repeat-dose toxicity studies and recognized as sensitive biomarkers of chemically induced changes in various organs (Smith et al. 2002; Thompson et al. 1992; Weingand et al. 1996). Guidance documents addressing carcinogenicity studies make only limited reference to the inclusion of clinical pathology testing as part of a two-year rodent bioassay, and none specifically for six-month genetically modified mouse assays.
The Society of Toxicologic Pathology (STP) and American Society for Veterinary Clinical Pathology (ASCVP) convened a Clinical Pathology in Carcinogenicity Studies Working Group to recommend best practices for inclusion of clinical pathology testing in carcinogenicity studies, namely, two-year rodent bioassays, but also six-month genetically modified mouse assays. The Working Group included members from the STP, ASVCP, British STP, and European STP. The standard designs of combined chronic toxicity/carcinogenicity studies, which are commonly used for chemical testing, routinely include clinical pathology testing, and these studies will not be discussed in this article. To aid in making specific recommendations, the Working Group reviewed available regulatory guidelines and literature, surveyed current practices of companies/organizations that conduct carcinogenicity studies, and gathered opinions of pathologists (mostly veterinary clinical pathologists, but some anatomic pathologists) who routinely evaluated data from carcinogenicity studies. This article provides a review of regulatory guidelines and pertinent literature, a summary of the survey data gathered by the Working Group, and recommendations regarding clinical pathology testing in carcinogenicity studies.
Review of Regulatory Guidelines for Clinical Pathology Testing in Carcinogenicity Studies
A uniform approach to clinical pathology testing in carcinogenicity studies does not exist among the guideline documents of the major regulatory bodies and professional standards organizations, and the International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH) has never directly addressed clinical pathology recommendations and/or requirements for preclinical toxicology studies. Regulatory guidelines can be roughly divided into those that focus on hematology tests and those that recommend a broader selection of tests, as briefly summarized in Table 1 .
Overview of clinical pathology testing recommendations in carcinogenicity study regulatory guidelines.
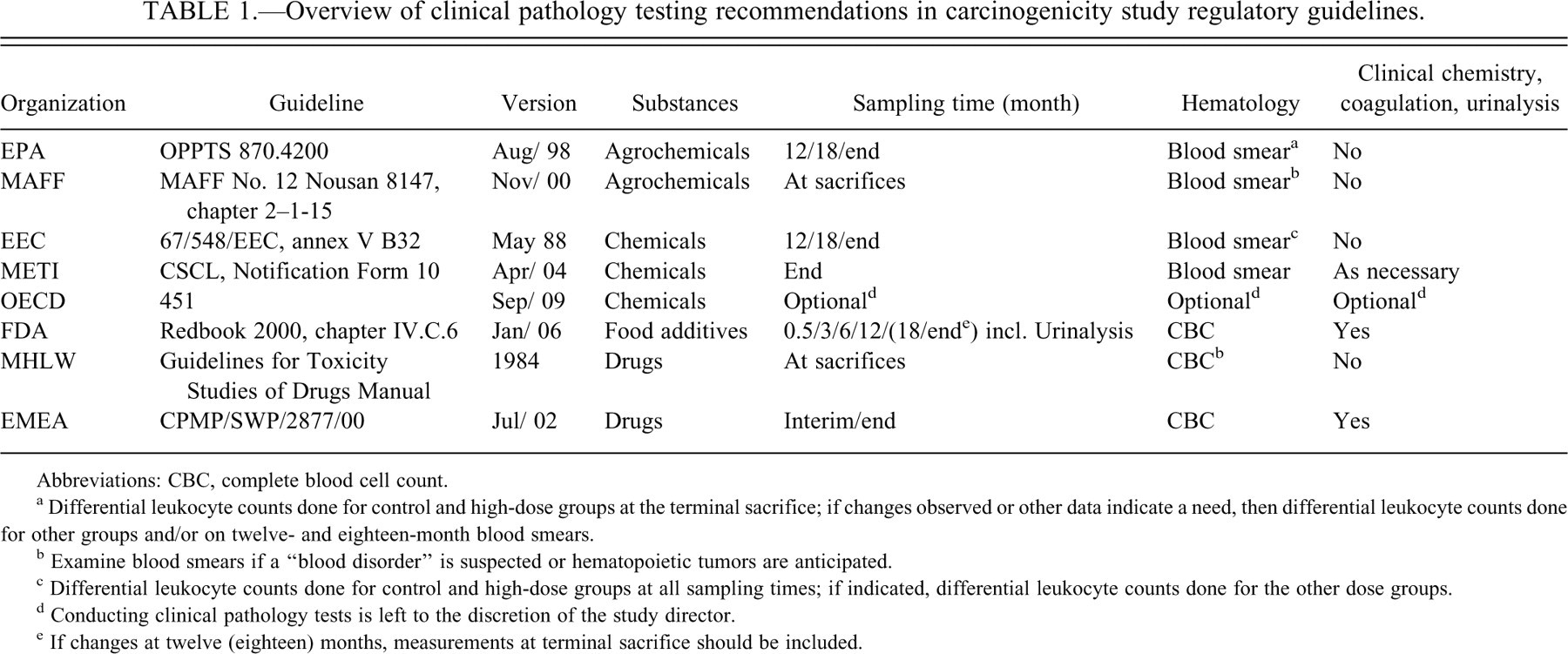
Abbreviations: CBC, complete blood cell count.
a Differential leukocyte counts done for control and high-dose groups at the terminal sacrifice; if changes observed or other data indicate a need, then differential leukocyte counts done for other groups and/or on twelve- and eighteen-month blood smears.
b Examine blood smears if a “blood disorder” is suspected or hematopoietic tumors are anticipated.
c Differential leukocyte counts done for control and high-dose groups at all sampling times; if indicated, differential leukocyte counts done for the other dose groups.
d Conducting clinical pathology tests is left to the discretion of the study director.
e If changes at twelve (eighteen) months, measurements at terminal sacrifice should be included.
Guidance documents focused on hematology tests include those from the United States Environmental Protection Agency (EPA), European Economic Community (EEC), Japan’s Ministry of Health, Labor, and Welfare (MHLW), Japan’s Ministry of Agriculture, Forestry, and Fisheries (JMAFF), and Japan’s Ministry of Economy, Trade, and Industry (METI). The EPA (U.S. EPA 1998) and EEC (EEC 1988) guidelines for carcinogenicity studies recommend obtaining a blood smear from all animals at twelve and eighteen months and at terminal sacrifice. The EEC guidelines recommend performing “differential blood counts” on the blood smears from control and high-dose animals at all three collection intervals. The EPA guidelines recommend performing “differential blood counts” for these groups only on the terminal sacrifice blood smears. If these or other data indicate a need (e.g., “a major discrepancy between the highest group and the controls”), differential blood counts should be performed on smears from lower-dose groups and/or earlier test intervals. The EPA and EEC guidelines also indicate that differential blood counts should be performed on animals with clinical observations suggesting deterioration in health. The EPA and EEC guidelines make no mention of obtaining total white blood cell counts in order to calculate absolute differential leukocyte counts.
The JMAFF (JMAFF 2000) and MHLW (MHLW 1999) guidelines are similar to each other in that both indicate blood smears should be made for animals that become moribund and animals at the terminal sacrifice. The blood smears should be examined if a “blood disorder” is suspected or “hematopoietic tumors are anticipated” based on other data and/or observations (e.g., anemia, enlargement of thymus, lymph nodes, liver, or spleen). In contrast to JMAFF guidelines, the MHLW guidelines also recommend red and white blood cell counts be done on the blood collected for preparation of blood smears. The METI guidance document (METI 2004) states, “During the autopsy, create a blood smear for all groups and measure the blood cell count and conduct a blood biochemistry test as necessary.” Since METI requires the conduct of a separate rodent chronic toxicity study that includes full hematology and clinical chemistry testing, “blood biochemistry” tests should rarely be necessary in carcinogenicity studies for METI.
Guidance documents recommending a broader selection of clinical pathology tests include those from the Center for Food Safety and Applied Nutrition (CFSAN) of the United States Food and Drug Administration (FDA) and the European Agency for the Evaluation of Medicinal Products (EMEA). The FDA Redbook guidelines for food ingredients (FDA 2006) are the most extensive and recommend hematology (including tests of “clotting potential”), clinical chemistry, and urinalysis tests be performed on at least ten animals/sex/group during the first two weeks of the study (hematology and clinical chemistry only) and at three, six, and twelve months. Urinalysis tests are also recommended before dosing begins. Ideally, the same animals should be sampled at each collection time point, and specific tests are recommended in the guideline. With respect to further testing, the Redbook guideline states, “If data trends or significant parameter changes (biological or statistical) that are of concern are observed at the twelve-month measurement, then an eighteen-month measurement should be included” and additional testing “should be conducted at the end of the study if data trends or significant parameter changes are observed at 18 months.” The EMEA guidance (EMEA 2002) simply states, “Monitoring of biochemical and haematological parameters as well as urinalysis should be considered during the study and should be performed at study termination.”
Although the primary objective of a carcinogenicity study is to determine the carcinogenic/tumorigenic potential of the material tested (this objective is specifically stated in most, but not all, of the guidance documents mentioned above), none of the guidance documents indicates how the recommended clinical pathology testing will help achieve that objective. Although it may be assumed that hematology testing is directed at the identification of hematopoietic neoplasia (i.e., leukemia), it is unclear how standard clinical chemistry, coagulation, or urinalysis tests contribute significantly to the identification of hematopoietic or nonhematopoietic neoplasia. In addition, standard clinical pathology tests contribute little, if anything, to the understanding of carcinogenicity mechanisms. The EMEA guidance document contains a statement that, although not directed specifically to clinical pathology, perhaps comes closest to a rationale for including clinical pathology testing. It states, “The primary purpose of a carcinogenicity study is to evaluate a drug’s tumourigenic potential. However, studies should be designed to obtain the maximum amount of information from the animals used.”
The recently published Organisation for Economic Cooperation and Development (OECD) carcinogenicity guideline (OECD 2009) takes a different approach. It states that samples may be taken for hematology, clinical biochemistry, and urinalysis at the discretion of the study director, although the value of such examination for the assessment of carcinogenic/oncogenic potential has been questioned (Weingand et al. 1996). Further references of OECD guidance documents are made (OECD draft guidance No. 116 2009; OECD Guidance Notes 2002), but these documents do not spell out the value of clinical pathology measurements for carcinogenicity studies.
Review of Literature
In the 1990s, recommendations were published by two different scientific groups regarding clinical pathology testing in animal toxicity and safety studies, including recommendations for two-year rodent carcinogenicity studies. The Joint Scientific Committee for International Harmonization of Clinical Pathology Testing recommended that blood smears should be made only from unscheduled terminations (decedents) and at study termination to aid in the identification and differentiation of hematopoietic neoplasia. Quantitative clinical pathology testing during the second year of a two-year rodent carcinogenicity study was considered generally inappropriate and was not recommended (Weingand et al. 1996). Previously, the AACC-DACC/ASVCP Joint Task Force recommended collection of blood samples approximately thirteen, twenty-six, and fifty-two weeks after initiation of chronic toxicity, carcinogenicity, and combined studies. However, the committee specifically recommended against conduct of quantitative clinical pathology testing during the second year of a two-year rodent study. Instead, it was recommended that blood smears be collected from all animals at study termination for qualitative assessment of hematopoietic neoplasia, if needed (Weingand et al. 1992). A commentary by Long and Symanowksi (1998) reiterated this opinion and stated that the “evaluation of clinical pathology parameters in rodents in oncogenicity studies should be limited to qualitative assessment of hematopoietic neoplasia, if needed.”
Both expert working groups recommended against quantitative clinical pathology in the second half of two-year studies based on their collective experience with increasing incidence of natural disease conditions during this time, but they did not provide literature references or data. Although there is no known report focusing specifically on this topic, there is scattered literature detailing increasing incidence with age of various organ and systemic diseases that introduce variation and outliers into clinical pathology data (Lindena et al. 1980). Furthermore, there is a gradual diminishing of function of organs and the endocrine system resulting in specific age-dependent variation in various clinical pathology parameters (Davies 1992; Nachbaur et al. 1977). Hepatic, renal, and cardiac changes have been especially noted. Glutamate dehydrogenase activity increases four- to five-fold over the lifespan of the rat, alanine aminotransferase activity increases approximately two-fold, and aspartate aminotransferase increases by an intermediate amount (Lindena et al. 1980). These increases have been attributed to degenerative hepatic changes associated with aging. The Sprague-Dawley rat strain is commonly affected by an age-dependent and sex-modified, spontaneous cardiomyopathy (Kemi et al. 1996; O’Brien et al. 2006). Chronic progressive nephropathy is a very common aging change in many strains of rats (Hard and Khan 2004). Glomerular filtration rate decreases with age in rodents resulting in a progressive rise in urea nitrogen and creatinine (Lindena et al. 1980), whereas glomerular leakage increases with age, resulting in albuminuria and proteinuria (Neuhaus and Flory 1978; Wolford et al. 1986).
Survey Conduct and Summary
To document current practices in the evaluation of clinical pathology testing in carcinogenicity studies, a questionnaire was sent to or discussed by phone with representatives from pharmaceutical and chemical companies, contract research organizations (CROs), research institutes, and private veterinary clinical pathology consultants located in North America, Japan, and Europe. Emphasis was placed on surveying pathologists with experience interpreting data from carcinogenicity studies, since the Working Group not only wanted to survey standard practices, but also sought scientific opinions from these individuals regarding the perceived value of the clinical pathology data currently being collected and what clinical pathology testing was most appropriate for carcinogenicity studies, assuming no regulatory guidelines.
For North America and Europe, most of the representatives were veterinary clinical pathologists and included members of the Working Group. Many smaller companies do not conduct their own carcinogenicity studies and pathologists employed by these companies typically had little or no experience interpreting data from carcinogenicity studies and thus were not included in the survey. For those pathologists with experience interpreting data from carcinogenicity studies, the participation rate was very high (i.e., >95%), although not all pathologists answered all the questions in the survey. For Japan, the survey was provided to individual scientists with an interest in clinical pathology at various Japanese companies, CROs, and research institutes. Written responses to the survey were provided back to the Working Group.
Current practices data were compiled for two-year rodent bioassays and six-month studies using genetically modified mice (Table 2 ). For CROs, the current practices reflected the company’s standard study design. Respondents were also asked whether current practices had changed following publication of the EMEA’s 2002 guidance for carcinogenicity studies, which states, “Monitoring of biochemical and haematological parameters as well as urinalysis should be considered during the study and should be performed at study termination.” The survey responses were compiled, and responses for two-year rat bioassays are summarized in Table 2. Respondents included representatives from 14 North American- or European-based pharmaceutical companies; 11 Japanese pharmaceutical companies; 8 CROs, chemical companies, and consultants from North American and Europe; and 8 CROs, research institutes, and chemical companies from Japan. Responses from North American- and European-based companies were similar and were tabulated together.
Survey responses for clinical pathology testing in two-year rat carcinogenicity studies. a
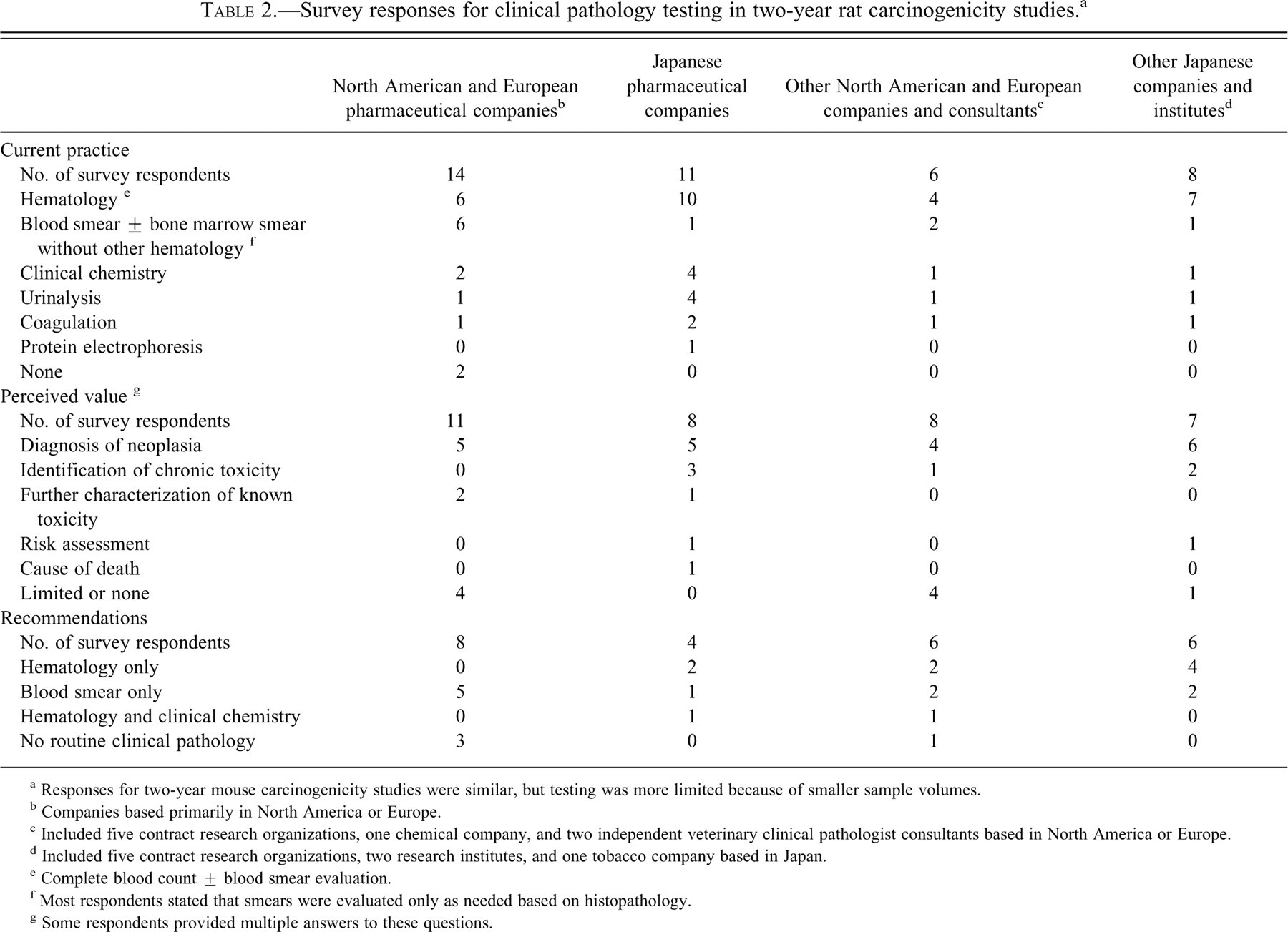
a Responses for two-year mouse carcinogenicity studies were similar, but testing was more limited because of smaller sample volumes.
b Companies based primarily in North America or Europe.
c Included five contract research organizations, one chemical company, and two independent veterinary clinical pathologist consultants based in North America or Europe.
d Included five contract research organizations, two research institutes, and one tobacco company based in Japan.
e Complete blood count ± blood smear evaluation.
f Most respondents stated that smears were evaluated only as needed based on histopathology.
g Some respondents provided multiple answers to these questions.
Current practices for two-year rodent carcinogenicity studies ranged from performing an extensive clinical pathology assessment to performing no clinical pathology testing. Hematology was commonly assessed by doing a complete blood count (69%), with or without blood smear evaluation, whereas other companies just collected blood and/or bone marrow smears and only evaluated these specimens as needed based on the hematology and/or histopathology assessment (26%). A minority did not collect any samples for hematology or other clinical pathology testing (5%). The next most common clinical pathology testing was clinical chemistry (21%), followed closely by urinalysis (18%). Coagulation testing and serum protein electrophoresis were rarely performed (13% and 3%, respectively). Most companies collected samples only at final necropsy, although respondents who recommended including more extensive clinical pathology testing often recommended collecting interim samples. As shown in Table 2, Japanese-based companies performed more clinical pathology testing than did North American- or European-based companies. No respondents indicated they had changed their procedures in response to the 2002 EMEA guidelines.
Concerning the perceived value of clinical pathology testing in carcinogenicity studies, the most common response was for the diagnosis of hematopoietic neoplasia (59%). The next most common response was that such testing was of limited or no value (26%). A minority of respondents considered clinical pathology data potentially useful for identification of unknown chronic toxicity, further characterization of a known toxicity, or for aiding in the determination of the cause of death. Regarding the question of what clinical pathology testing should be recommended for carcinogenicity studies, assuming no regulatory guidelines, the most common response was blood smears only to be evaluated as needed based on histopathology (41%), followed by a complete blood count (33%). The third most common recommendation was to do no clinical pathology testing (26%). In the minority were individuals who recommend both hematology and clinical chemistry testing (8%). No respondents recommended coagulation or urinalysis testing.
Six-Month Carcinogenicity Studies Using Genetically Modified Mice
Only six companies provided survey data concerning current practices in clinical pathology testing for six-month carcinogenicity studies using genetically modified mice. Responses varied, with some companies designing these studies like a multidose toxicology study with standard hematology and clinical chemistry testing, whereas other companies collected only blood smears, as is done for many two-year rodent carcinogenicity studies. Few opinions were shared regarding recommendations for clinical pathology testing in such studies.
Recommendations
Based on our review of existing regulatory guidance documents, review of relevant literature, results from the survey discussed above, and personal experience of the Working Group members, this Working Group proposes the following recommendations with respect to clinical pathology testing in two-year carcinogenicity studies: Blood smears should be routinely collected from all sacrificed animals (scheduled and unscheduled), but these specimens should only be examined as necessary following a histopathologic assessment. Routine collection of other hematologic, clinical chemistry, coagulation, or urinalysis data is not recommended. Additional clinical pathology testing, including the collection of bone marrow smears, may be included on a case-by-case basis (e.g., to address specific issues identified in prior toxicity studies or known test article–related class effects that were not adequately addressed in earlier studies).
These recommendations are consistent with previous recommendations regarding clinical pathology testing in carcinogenicity studies, in which clinical pathology testing was not recommended after fifty-two weeks of age (Long and Symanowksi 1998; Weingand et al. 1992; Weingand 1996). To assess toxicity at earlier time points, separate smaller chronic toxicity studies are conducted or an alternative combined chronic toxicity/carcinogenicity study design is used. Clinical pathology data from rodents sacrificed prior to the end of a carcinogenicity study lack concurrent control data for comparison, and interpretation of the data is often confounded by spontaneous diseases of aging. Conducting clinical pathology testing near or at the termination of a two-year carcinogenicity rodent study for the purpose of general screening for chronic toxicity is unlikely to contribute meaningful new data. In addition, routine clinical pathology testing is not a sensitive method for detecting nonhematopoietic neoplasia in rodents, nor would it be expected to contribute to determining carcinogenic mode of action.
For two-year rodent carcinogenicity studies, the Working Group recommends that blood smears be routinely collected from all sacrificed animals (scheduled and unscheduled), but that these specimens be examined only as necessary following a histopathologic assessment. Resources associated with collection and retention of these specimens are small compared to those necessary for conducting the overall study. Evaluation of blood smears may further support or characterize a histopathologic diagnosis of hematopoietic neoplasia or test article–related hematologic change. The value of additional clinical pathology testing at interim time points during the study must be weighed against the risk of compromising the integrity of the carcinogenicity portion of the study owing to increased stress or mortalities associated with blood collection in aging rodents. Interim blood sample collections are not feasible for mouse studies because of the small size of the animals. For a specific test article, additional clinical pathology testing may be useful to further characterize a test article–related effect detected in earlier studies, evaluate a test article class effect, or investigate a theoretical risk based on the mechanism of action of the test article. In addition to standard clinical pathology parameters, such testing may include nonstandard assays and/or novel biomarkers. In general, if data from multiple interim time points are to be collected, it may be more feasible to conduct specifically designed investigative studies in parallel with the carcinogenicity study or include additional animals/groups, as is done for combined chronic toxicity/carcinogenicity studies.
The design and use of alternative carcinogenicity assays such as six-month studies using genetically modified mice is still evolving, and only a subset of the Working Group members and survey respondents had experience with these assays. Thus the Working Group does not make a specific recommendation concerning clinical pathology testing for six-month carcinogenicity studies using genetically modified mice, but it suggests that it may be appropriate to use the same approach as for two-year carcinogenicity studies, since the study goal is the same. Additionally, reference intervals for clinical pathology data and strain-specific responses to toxicity and spontaneous disease are not well characterized in these genetically modified mice.
Conclusions
The primary purpose of rodent carcinogenicity studies is to characterize the carcinogenic potential of pharmaceutical and other chemicals. Routine clinical pathology testing in such bioassays is considered to be of limited value and is most appropriately used to aid in the diagnosis and further characterization of hematopoietic neoplasms. For two-year rodent carcinogenicity assays, this Working Group recommends that clinical pathology testing be limited to collection of blood smears at scheduled and unscheduled sacrifices to be reviewed only if indicated following the histopathologic evaluation. For alternative six-month carcinogenicity studies using genetically modified mice, it is premature to make a recommendation regarding best practices, although the Working Group suggests that clinical pathology testing in these studies should also be limited.
Footnotes
Abbreviations
This paper represents recommendations formulated by a joint working group of the Society of Toxicologic Pathology and the American Society for Veterinary Clinical Pathologists. In addition, the recommendations in this article are endorsed by the European Society of Toxicologic Pathology and the British Society of Toxicologic Pathology.
This is an opinion article submitted to the Regulatory Forum and does not constitute an official position of the Society of Toxicologic Pathology or the journal Toxicologic Pathology. The Regulatory Forum is designed to stimulate broad discussion of topics relevant to regulatory issues in toxicologic pathology. Readers of Toxicologic Pathology are encouraged to send their thoughts on these articles or ideas for new topics to