
Abstract
Astrocytes assume multiple roles in maintaining an optimally suited milieu for neuronal function. Select astrocytic functions include the maintenance of redox potential, the production of trophic factors, the regulation of neurotransmitter and ion concentrations, and the removal of toxins and debris from the cerebrospinal fluid (CSF). Impairments in these and other functions, as well as physiological reactions of astrocytes to injury, can trigger or exacerbate neuronal dysfunction. This review addresses select metabolic interactions between neurons and astrocytes and emphasizes the role of astrocytes in mediating and amplifying the progression of several neurodegenerative disorders, such as Parkinson’s disease (PD), hepatic encephalopathy (HE), hyperammonemia (HA), Alzheimer’s disease (AD), and ischemia.
1. Introduction
The past several decades have given rise to many important discoveries and novel insights into the role of astrocytes in normal brain function and disease, firmly establishing concepts that describe the dynamic and reciprocal signaling networks between astrocytes and neurons. This article briefly delineates a select set of astrocytic functions within the mature central nervous system (CNS), followed by a short discussion emphasizing the astrocytic modulation of neurodegenerative injuries, including Parkinson’s disease (PD), Alzheimer’s disease (AD), hepatic encephalopathy (HE), hyperammonemia (HA), and ischemia. For an excellent and thorough review on the various functions of mature astrocytes, the reader is referred to a recent article by Kimelberg (2010). For a review on astrocytic glial toxicants and their role in the pathogenesis of human neurodegenerative diseases such as AD and PD, please refer to Aschner and LoPachin (2001).
1A. Select Functions of Mature Astrocytes and Metabolic Relationships to Neurons
The metabolic relationship between neurons and astrocytes is perhaps best exemplified by the neuronal dependence on astrocyte-derived thiols for the maintenance of stable concentrations of glutathione (GSH) (Dringen and Hirrlinger 2003). GSH is synthesized in a two-step process. First, the action of γ-glutamylcysteine (γ-GS) synthase forms γ-glutamylcysteine from cysteine and glutamate; then glycine derived from GSH synthetase is added, completing the process. GSH is a major antioxidant that constitutes ~90% of the intracellular nonprotein thiols. Conjugation with GSH detoxifies and eliminates toxic molecules from cells, and de novo GSH synthesis ensures the maintenance of intracellular redox status. In general, GSH levels are lower in neurons than in astrocytes (Sagara, Miura, and Bannai 1993), thus rendering neurons more susceptible to injury as a result of oxidative stress. Furthermore, cysteine derived from astrocytes is essential for the maintenance of stable GSH levels in neurons (Dringen, Pfeiffer, and Hamprecht 1999; Kaur, Aschner, and Syversen 2007; Shanker et al. 2001; Wang and Cynader 2000).
The metabolic interaction between astrocytes and neurons is also critical for energy metabolism as well as for the synthesis of de novo glutamate and γ-aminobutyric acid (GABA). Furthermore, this important interaction is also responsible for the termination of glutamatergic and GABAergic activity, which is achieved by the re-uptake of both neurotransmitters, especially glutamate, into astrocytes (see below). Optimal synaptic glutamate concentrations are maintained by glutamate aspartate transporter (GLAST) (Storck et al. 1992) and glutamate transporter 1 (GLT1) (Lehre et al. 1995), both of which are preferentially localized on astrocytes. This re-uptake ensures low synaptic extracellular glutamate concentrations, thus protecting neurons from excitotoxicity (Rothstein et al. 1996).
In addition to expressing glutamate-specific transporters (see above), astrocytes and neurons express enzymes that are specific to each cell type (Hertz et al. 1992). This unique compartmentalization originally advanced the hypothesis purporting that these two cell types engage in the exchange of metabolites (Berl, Lajtha, and Waelsch 1961; Lajtha, Berl, and Waelsch 1959). Also derived from this theory is the concept of the glutamate-glutamine cycle, which links glutamatergic neurons and astrocytes (van den Berg and Garfinkel 1971). In the glutamate-glutamine cycle, glutamate released from neurons is predominantly removed by astrocytic GLT1 and GLAST (Gegelashvili and Schousboe 1997, 1998), thereby ensuring a constant flow of glutamine (catalyzed from glutamate by the astrocyte-specific enzyme, GS) from astrocytes to neurons.
Another important concept is that anaplerosis, a requisite reaction for the operation of the tricarboxylic acid (TCA) cycle in the CNS, is exclusively inherent to the astrocyte-specific enzyme, pyruvate carboxylase (PC) (Cesar and Hamprecht 1995; Shank et al. 1985; Yu et al. 1983). PC is a mitochondrial ATP-dependent enzyme containing a biotin prosthetic group, requiring magnesium or manganese and acetyl coenzyme A (CoA). High levels of ADP inhibit the phosphorylation of the enzyme, while acetyl-CoA acts as an allosteric activator of the enzyme. Anaplerosis generates a molecule of oxaloacetate by de novo synthesis. This oxaloacetate molecule then condenses with acetyl-CoA, resulting in the net synthesis of the TCA cycle intermediate, α-ketoglutarate, from which glutamate is formed by transamination (Westergaard et al. 1996). Subsequently, glutamine is synthesized from glutamate in a reaction catalyzed by glutamine synthase (GS), which, analogous to PC, in the CNS, is exclusively expressed in astrocytes (Martinez-Hernandez, Bell, and Norenberg 1977).
Neurotransmitter-mediated metabolic coupling between astrocytes and neurons also invokes lactate release from astrocytes for utilization as an energy source in neurons. The coupling, referred to as the astrocyte neuronal lactate shuttle hypothesis (ANLSH), proposes that glucose enters the CNS via the astrocytic processes. Once in the CNS, glucose then unsheathes the capillaries where it is catabolized to lactate by aerobic glycolysis. Lactate, in turn, can then be shuttled into neurons as an energy source (Magistretti et al. 1994; Pellerin and Magistretti 2004). While remaining somewhat controversial, support for a net lactate transfer between astrocytes and neurons in vivo exists, as recently demonstrated (Pellerin et al. 2007). Enhanced neuronal metabolism occurring in conjunction with elevated levels of CNS electrical activity has been shown to be associated with lactate generated from a non-neuronal compartment, most likely astrocytes (Pellerin et al. 2007; Serres et al. 2004, 2005, 2003). The fact that such a transfer increases with the level of activity is consistent with in vitro observations that have described the redistribution of glucose away from neurons and toward astrocytes upon increased demand. This redistribution reflects enhanced astrocytic glycolysis upon sustained activation to ensure the requisite lactate necessary to maintain ongoing neuronal energy needs (Pellerin et al. 2007). Table 1 summarizes some properties of astrocytes, including their physiological and supportive roles for neurons.
Major functions of astrocytes.
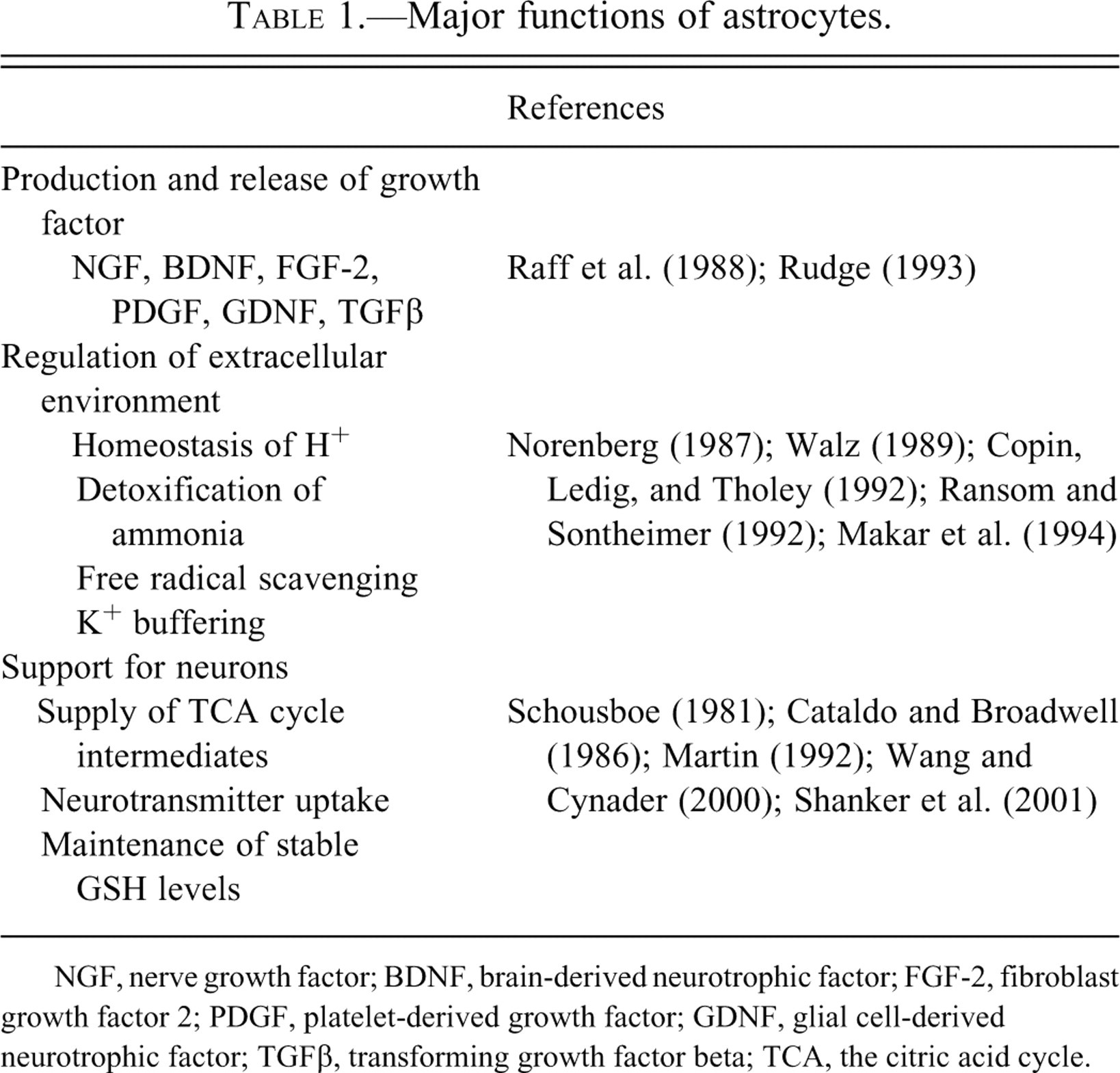
NGF, nerve growth factor; BDNF, brain-derived neurotrophic factor; FGF-2, fibroblast growth factor 2; PDGF, platelet-derived growth factor; GDNF, glial cell-derived neurotrophic factor; TGFβ, transforming growth factor beta; TCA, the citric acid cycle.
2. What Is the Evidence in Favor of Astrocytic Modulation of Neurodegeneration?
2A. Role of Astrocytes in Parkinson’s Disease
Parkinson’s disease (PD) is a neurodegenerative disorder associated with the loss of dopamine neurons in the substantia nigra pars compacta (SNpc). It is characterized by slowed movement, rigidity, rest tremor, and bradykinesia (Hornykiewicz and Kish 1987; Lang and Lozano 1998). Metabolism via monoamine oxidase-B (MAO-B) of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP), a synthetic heroin analog to its active metabolite, MPP+, is known to occur within astrocytes. This pathway has been invoked as the major pathway of MPTP bioactivation and dopamine-specific cell damage, resulting in a Parkinsonian-like syndrome (Heikkila et al. 1989). However, other studies have also invoked astrocytic neuroprotection in the course of exposure to MPTP. Such protection is exemplified by the increased immunoreactivity of the astrocytic marker, glial fibrillary acidic protein (GFAP), in the striatum (Dervan et al. 2004). Moreover, increased numbers of astrocytes and GFAP immunoreactivity have been found in the SNpc of PD postmortem cases (Mirza et al. 2000). Notably, a recent study also showed that α-synuclein immunoreactivity, a major component of Lewy bodies and Lewy neurites appearing in the postmortem brain of PD, is restricted to GFAP-expressing astrocytes (Gu et al. 2010). Astrocytes exert a neuroprotective effect on dopaminergic neurons by secreting a number of neurotrophic factors, such as brain-derived neurotrophic factor (BDNF), glial cell-line-derived neurotrophic factor (GDNF), and mesencephalic astrocyte-derived neurotrophic factor (MANF), as well as numerous antioxidants (Knott et al. 2002; L. F. Lin et al. 1993; Petrova et al. 2003). Release of neurotrophic factors from astrocytes protects dopaminergic neurons in midbrain neuronal/glial cultures (P. S. Chen et al. 2006; Zhang et al. 2005). Astrocytes may also act as scavengers for reactive oxygen species (ROS). Dopamine derived from neurons can be metabolized by astrocytic MAO-B or catechol-O-methyl transferase (COMT), and the resultant free radicals are eliminated by glutathione peroxidase (GPX) (Hirsch et al. 1999; Przedborski and Jackson-Lewis 2000). Moreover, the upregulation of astrocytic protease-activated receptor-1 (PAR-1) in PD has been shown to exert a neuroprotective effect that is mediated by increased levels of GPX (Ishida et al. 2006).
Increased oxidative stress is associated with neuronal cell death in PD (Navarro and Boveris 2009). The transcription factor, NF-E2-related factor (Nrf2), binds to a DNA consensus sequence, antioxidant response element (ARE), and initiates the transcription of genes encoding phase II detoxication enzymes and factors essential for neuronal survival under conditions of oxidative stress (Lee et al. 2005; Rushmore, Morton, and Pickett 1991). Recent reports also indicate that Nrf2 expression that is restricted to astrocytes mediates neuroprotection in the MPTP model (P. C. Chen et al. 2009). Modulation of the Nrf2-ARE pathway in astrocytes may therefore represent a promising therapeutic strategy for the treatment of PD.
2B. Role of Astrocytes in Alzheimer’s Disease
Alzheimer’s disease (AD) is a neurodegenerative disorder and is the most common form of dementia in later life. AD is manifested by the progressive deterioration of cognitive functions such as memory and mental processing (McKhann et al. 1984). Histopathological features of AD include large extracellular senile plaques (SPs) composed of the amyloid-β (Aβ) plagues and neurofibrillary tangles, which are intracellular inclusions of hyperphosphorylated tau protein in selective regions of the brain (Koistinaho et al. 2004; Nagele et al. 2003). Aβ is a peptide of 42 amino acid residues produced by the selective proteolytic cleavage of transmembrane amyloid precursor proteins (APP) by β- and γ-secretases (Haass and Selkoe 1993). Aβ can directly induce neuronal cytotoxicity, but the relevance of such toxicity to the disease is controversial (Pimplikar 2009; Yankner, Duffy, and Kirschner 1990). Morphological characterization of GFAP-positive astroglial cells performed on AD mouse model at different ages showed an age-dependent reduction in GFAP expression (Rodríguez et al. 2009). These authors suggested that in an AD transgenic, reactive hypertrophic astrocytes surround the neuritic plaques, whereas astroglial cells in other brain regions undergo atrophy, which may account for early changes in synaptic plasticity and cognitive impairments inherent to AD. In the AD human tissue, prominent astrogliosis occurs in the cells surrounding amyloid plaques, and these activated astrocytes accumulate large amounts of Aβ42, which are derived from neuronal debris and associated with plaques (Nagele et al. 2003). Moreover, astrocytes from patients with dementia show significantly decreased complexity compared to the healthy brain (Senitz, Reichenbach, and Smith 1995). In the 3xTg-AD transgenic animal model, which closely resembles the human AD pathology, astrocytes undergo reactive hypertrophy surround the neuritic plaques; whereas throughout the brain parenchyma astrocytes undergo atrophy (Rodríguez et al. 2009; Olabarria et al. 2010).
Astrocytes play an important protective role in AD. While microglial cells are the driving force in SPs formation, astrocytes are crucial in plaque degradation as evidenced by the ultrastructural three-dimensional reconstruction of human classical plaques in different stages of development (Wegiel et al. 2000). Aβ peptides are preferentially internalized by astrocytes, and astrocytic hypertrophic processes degrade Aβ-containing plaques (Kurt, Davies, and Kidd 1999), thus preventing the formation of the deposits of extracellular Aβ (Wyss-Coray et al. 2003). The precise mechanism by which astrocytes recognize and degrade Aβ is not known, but apolipoprotein E (ApoE), which is almost exclusively expressed in astrocytes, has been proposed to be responsible for this cellular action. ApoE is essential for astrocytes to attract chemically, internalize, and degrade Aβ deposits in brain sections in vitro (Koistinaho et al. 2004). Astrocytes also exert protective effects in AD by inhibiting activated microglia. Aβ-induced TGF-β derived from astrocytes can suppress inducible nitric oxide synthase (iNOS) activity in microglia (Vincent, Tilders, and Van Dam 1997). Moreover, astrocyte-conditioned medium from proliferative cultures suppresses activated microglia-induced NO production and phagocytosis of SP cores (DeWitt et al. 1998).
However, the failure of astrocytes to properly degrade Aβ results in the accumulation of Aβ-containing neuronal debris in astrocytes and astrocytic plaque formation (Nagele et al. 2003). Additionally, astrocytes are activated by accumulated Aβ and produce inflammatory mediators, such as interleukin 1β (IL-1β) and tumor necrosis factor-α (TNF-α), which may induce neuronal injury (Johnstone, Gearing, and Miller 1999). Aβ-induced TNF-α increases calcium-dependent glutamate release, which may lead to neuronal death in AD (Rossi et al. 2005). Oxidative stress has also been linked to Aβ toxicity as Aβ stimulates ROS production and decreases GSH levels in these cells (Abramov, Canevari, and Duchen 2004; Canevari, Abramov, and Duchen 2004). In addition, Aβ disturbs glucose metabolism in astrocytes, leading to the impairment of neuronal viability (Allaman et al. 2010).
Impairment of glutamatergic neurotransmission associated with excitotoxicity has been implicated in the progression of AD. The glutamate transporter, GLT1, which is preferentially localized in astrocytes, is the major mediator of glutamate clearance in humans. Loss of GLT1 has been reported in the brains of patients with AD (Tian et al. 2010). This effect may be partially mediated by oxidative stress and the differential activity and complex balance between the MAP kinase signaling pathways (Matos et al. 2008).
3. Astrocytes in Neurological Diseases/Conditions
3A. Role of Astrocytes in Ischemia
Prolonged occlusion of cerebral vessels due to cardiac arrest, stroke, or head trauma initiates processes inherent to brain ischemia. Astrocyte swelling is a prominent as well as the earliest response in anoxia-ischemia (Petito et al. 1990). Moreover, the cytoplasm of these astrocytes contains increased numbers of mitochondria and rough endoplasmic reticulum, and the nuclei are enlarged and pale (Norenberg 1981). Astrocytes are known to be critically involved in the pathophysiology of ischemia (Anderson et al. 2003). However, their response to stroke and their role in neuroprotection are not completely understood. Formation of the glial scar during ischemia significantly inhibits functional recovery and processes of regeneration (Fawcett and Asher 1999). Furthermore, focal cerebral ischemia induces astrocytic swelling and leads to an increase in intracerebral pressure, thereby significantly intensifying the ischemic event (Ayata and Ropper 2002). Astrocytic swelling may also reduce the uptake and release of glutamate, potentially initiating excitotoxicity (Anderson et al. 2003). It is known that under ischemic conditions, astrocytic gap junction channels, small pores responsible for homeostasis modulation, may be involved in mediating brain damage by diffusing pro-apoptotic substances and calcium ions to surrounding healthy cells (Budd and Lipton 1998; J. H. Lin et al. 1998; Rouach et al. 2002). These gap junctions may also contribute to the induction of spreading depression, which has been implicated in infarct expansion (Largo, Cuevas, and Herreras 1996). Notably, rats treated with gap junction blockers, such as octanol and halothane, exhibit reduced infarct volume as well as neuronal death in the permanent focal ischemia model (Saito et al. 1997). Connexin43 (CX43), a principal gap junction forming protein of astrocytes, is associated with protection from ischemic injury (Thompson and MacVicar, 2008). Mice lacking Cx43 in astrocytes showed a significantly increased infarct volume and amplified inflammatory response and apoptosis (Siushansian et al. 2001; Nakase et al. 2004). Astrocytes, on the other hand, have been shown to play a significant role in regeneration during the chronic phase after injury. Astrocytes support neurons by scavenging transmitters released during synaptic activity, controlling ion and water homeostasis and secreting a number of neurotrophic and neuroprotective factors (Y. Chen and Swanson 2003). Many studies also provide evidence for astrocyte-mediated neuroprotection from oxidative stress via a GSH-dependent mechanism (Dringen 2000; Haberg et al. 2001; Iwata-Ichikawa et al. 1999; see also above, Section 1). The inhibition of GSH synthesis increases cortical infarction and edema after ischemia (Mizui, Kinouchi, and Chan 1992). Furthermore, the astrocyte-targeted overexpression of heat shock protein 72 (Hsp72) or superoxide dismutase 2 (SOD2) significantly reduces the loss of CA1 hippocampal neurons in a forebrain ischemia model (Xu et al. 2010). Astrocytes may extend neuronal damage as well as provide neuronal protection under ischemic conditions. Therefore, future efforts aimed at understanding their underlying mechanisms during ischemia are necessary to provide valuable insight into potential therapies.
Formation of the glial scar during ischemia significantly inhibits functional recovery and processes of regeneration (Fawcett and Asher 1999). Furthermore, focal cerebral ischemia induces astrocytic swelling and leads to an increase in intracerebral pressure, thereby significantly intensifying the ischemic event (Ayata and Ropper 2002). Astrocytic swelling may also reduce the uptake and release of glutamate, potentially triggering excitotoxicity (Anderson et al. 2003).
3B. Role of Astrocytes in Hyperammonemia and Hepatic Encephalopathy
The impairment of detoxification processes in chronic or acute liver failure results in increased blood levels of several toxic compounds. One of these compounds, ammonia, readily crosses the blood-brain barrier and accumulates in the central nervous system, where it evokes a number of neuropsychiatric disturbances collectively known as hepatic encephalopathy (HE) (Ferenci et al. 2002; Mullen 2007). Although other toxins involved in HE have been described (Baraldi et al. 1984; Blom et al. 1991; Dejong et al. 2007; Mizoguchi et al. 2001; Montes et al. 2001; Montoliu et al. 2009; Pares et al. 2009), hyperammonemia (HA) is considered to be the primary cause of this disease (Butterworth 2002; Shawcross and Jalan 2005). Cognitive, intellectual, emotional, and behavioral symptoms characterizing HE include the following: circadian rhythm alterations; loss of concentration; depression or euphoria; forgetfulness; confusion; irritability; somnolence; loss of consciousness; and coma, which is the final stage of the disease and usually precedes death (Conn 1994).
The exact mechanisms of ammonia neurotoxicity are not completely known. However it is commonly accepted that astrocytes are the cells that are primarily affected in HE, and neuronal pathology is, to a great extent, secondary to glial dysfunction (Albrecht 2005). The most prominent histopathological changes found in HE that accompanies chronic liver failure include Alzheimer’s type II astrocytosis, (enlarged astrocytes with pale, large nuclei and prominent nucleoli) (Norenberg 1977; Pilbeam, Anderson, and Bhathal 1983) and pronounced astrocytic swelling, leading to brain edema in cases of acute HE (Traber et al. 1987; Wright et al. 2010). Morphological alterations in neurons are observed much less frequently (Butterworth 2007). The high susceptibility of astrocytes to HA may be explained by the fact that when the urea cycle is dysfunctional in the brain, ammonia is detoxified through its condensation with glutamate to form glutamine (Gln). This reaction is catalyzed by the astrocyte-specific enzyme, glutamine synthase (GS) (Cooper et al. 1979; Martinez-Hernandez, Bell, and Norenberg 1977). Increased levels of brain Gln are found in patients suffering from both acute (McConnell et al. 1995; Record et al. 1976) and chronic HE (Laubenberger et al. 1997; Lavoie et al. 1987), as well as in many animal models (Cordoba, Gottstein, and Blei 1996; Hawkins et al. 1993; Hilgier et al. 2008; Zielinska et al. 2004), and are considered to be a key factor in the pathogenesis of this syndrome (Shawcross et al. 2004; Warren and Schenker 1964).
Additionally, a correlation between Gln accumulation and astrocytic swelling has been observed in vivo (Blei et al. 1994; Rama Rao et al. 2010; Takahashi et al. 1991) and in vitro (Norenberg and Bender 1994). However, the hypothesis supporting a direct osmotic effect of Gln (Olafsson, Gottstein, and Blei 1995) appears unlikely (Cordoba et al. 1999; Jayakumar et al. 2006; Zwingmann et al. 2004). Experiments with inhibitors of different mitochondria-related events have shown that the Gln-induced dysfunction of mitochondria may play a key role in astrocytic swelling (Jayakumar et al. 2006; Pichili et al. 2007; Rama Rao et al. 2003). Gln is degraded by the mitochondrial enzyme, phosphate activated glutaminase (PAG) (Bak et al. 2008), and acceleration of this process in HA (Dolinska, Hilgier, and Albrecht 1996; Romero-Gomez et al. 2006) may cause a significant elevation of ammonia levels in astrocytic mitochondria (Albrecht and Norenberg 2006; Kosenko et al. 1996). Increased ammonia concentrations in these organelles lead to the impairment of their functionality as reflected by mitochondrial permeability transition, the loss of mitochondrial transmembrane potential (Bai et al. 2001; Pichili et al. 2007; Rama Rao et al. 2003), a decrease in Krebs cycle activity (Diaz-Munoz and Tapia 1989; Faff-Michalak and Albrecht 1991, 1993; Hindfelt, Plum, and Duffy 1977; Zwingmann et al. 2003), and the loss of ATP (Kosenko et al. 1994; Pichili et al. 2007).
Furthermore, the dysfunction of astrocytic mitochondria may result in oxidative stress. Increased ROS generation has been found in primary astrocytes exposed to ammonia (Murthy et al. 2001) and has been shown to be closely related to accelerated astrocytic Gln metabolism (Jayakumar et al. 2004; Pichili et al. 2007). Oxidative stress has also been observed in animal models of HA and HE (Hilgier et al. 2003; Jiang, Desjardins, and Butterworth 2009; Kosenko et al. 1997). However, very few studies have addressed the role of oxidative stress in HE in humans (Harrison et al. 1991; Jones 1998). Under conditions of HA, the activity of astrocytes in the detoxification of ammonia leads to the overproduction of Gln, the amino acid responsible for a number of pathological cellular processes, thereby significantly contributing to the pathogenesis of HE.
4. Conclusions
Astrocytes play a critical role in normal function of the mammalian nervous system. Astrocytes regulate synaptic transmission and plasticity, protect neurons against toxic compounds, and support metabolically to ensure their optimal functioning. In numerous pathological states, such as AD, PD, or ischemia, astrocytes are involved in neuroprotective mechanisms. As discussed in this review, they support neurons by providing growth factors, cytokines, as well as extracellular matrix molecules, all of which are essential for repair and regeneration. In other conditions, such as HE, disturbances in astrocytic metabolism are implicated in disease pathogenesis. Therefore, modulation of astrocyte functioning may prove to be an efficient therapeutic strategy in many CNS disorders.
Footnotes
This article was supported in part by a Public Health Service Grant from the National Institutes of Health, NIEHS 07331, NIEHS 016931, and NIEHS 10563.