
Abstract
Racial discrimination affects individuals and families, especially Black American mothers, who often rely on coping strategies like the Superwoman Schema—reflecting stress, resilience, and societal expectations shaped by racism and sexism. This study examines how personal and vicarious racial discrimination (experienced through their adolescent children) relate to depressive symptoms, perceived stress, and anxiety among 319 Black American mothers. It also explores whether dimensions of the Superwoman Schema mediate these effects. Confirmatory factor analyses identified two key dimensions: the obligation to manifest strength and the obligation to help others at the expense of self-care. Only the latter mediated the relationship between both forms of racial discrimination and mental health outcomes. No mediation was found for the obligation to manifest strength. These findings underscore the need to address culturally relevant stressors and coping mechanisms in understanding the mental health of Black American mothers.
Racial discrimination, defined as the behavioral expression of racism and the social structures and interpersonal actions rooted in White supremacy and oppression (Pieterse & Powell, 2016), is a common experience for many Black American adults (Vines et al., 2017). As a chronic social stressor, racial discrimination disrupts both psychological and physiological stress regulation systems. Across its various forms—systemic, personally experienced, and vicariously experienced—racial/ethnic discrimination has been consistently linked to adverse mental and physical health outcomes, including depression (Antilla & Johnson, 2024; Vines et al., 2017), anxiety (Antilla & Johnson, 2024; Moody et al., 2023), and higher allostatic load (Allen et al., 2019). While much of the existing literature has focused on the direct effects of personally experienced discrimination, emerging research highlights the harmful impact of vicarious discrimination—when individuals witness or learn about discriminatory events targeting others (Ong, 2021). For Black American mothers, this dual exposure to both personal and vicarious racial discrimination, particularly when their children are the targets, creates a compounded burden of race-related stress.
In navigating these layered challenges, Black American women and mothers have adopted many ways of coping with racial discrimination, often showing resilience and strength within an unfair and harmful context (Boyd-Franklin, 2003; Sheehan et al., 2024). Coping, traditionally defined as the use of mental and behavioral efforts to manage explicit external and/or internal stresses that are appraised as taxing (Spencer et al., 1997; Woods-Giscombé, 2010), is an essential component of the stress process and influences the relationship between racial discrimination and health. Superwoman Schema is a culturally relevant, multidimensional psychological construct reflecting common internalizations of Black American women, such as obligations to show strength, succeed, suppress emotions, resist showing vulnerability, and help others even to the postponement of self-care (Woods-Giscombé, 2010; Woods-Giscombé et al., 2019). These psychological internalizations often emerge in Black American women in response to the stressors and expectations they experience because of racism and sexism in the United States (Woods-Giscombé, 2010; Woods-Giscombé et al., 2019). Black American women are often not only expected to endure adversity with resilience (Sheehan et al., 2024) but also to serve as caregivers and resource-sharers within their families and communities (Chance, 2022; Lewis et al., 2013; Platt & Fanning, 2023). While these coping strategies may offer short-term protection, sustained reliance on Superwoman Schema has been linked to negative psychological and physical health outcomes, including elevated stress, depression, and physiological wear and tear (Allen et al., 2019; Jones et al., 2025; Leath et al., 2022; Nelson et al., 2022; Platt & Fanning, 2023). The present study aims to examine the relationships among personal and adolescent-experienced racial discrimination, endorsement of Superwoman Schema, and psychological distress among Black American mothers of adolescents.
Theoretical Framework
To guide this investigation, the study draws from the Sociocultural Family Stress Model, building upon both intersectionality and the mundane extreme environmental stress perspectives (McNeil Smith & Landor, 2018; Peters & Massey, 1983). This framework suggests that Black American families experience general stressors, as well as consistent stressors related to their social positions such as discrimination (Antilla & Johnson, 2024; Boyd-Franklin, 2003; McNeil Smith & Landor, 2018). Their level of risk or resilience in the face of these stressors depends on individual, family, and community resources and coping strategies, as well as the family members’ perceptions of the stressors (Butler‐Barnes & Martin, 2023; McAdoo, 2007; McAdoo & McAdoo, 1985; McNeil Smith & Landor, 2018; Sheehan et al., 2024). These appraisals and coping responses are further influenced by each family member’s unique social location and lived experiences. As a result, variations in exposure to and interpretations of oppression, such as racism, sexism, classism, and colorism, can lead to diverse coping repertoires within Black American families (Boyd-Franklin, 2003; Butler‐Barnes & Martin, 2023; Jacob et al., 2023; McAdoo, 2007; McAdoo & McAdoo, 1985). For instance, Black American mothers, who often face intersecting forms of oppression, may develop distinct beliefs about how to respond to stress and adopt culturally specific coping strategies, such as those reflected in the Superwoman Schema (Butler‐Barnes & Martin, 2023; Chance, 2022; McAdoo, 2007; McAdoo & McAdoo, 1985; Sissoko et al., 2023).
Coping strategies are not static; rather, they are often activated or reinforced in response to specific stressors. Although a coping response set that includes the obligations to show strength, succeed, suppress emotions, resist showing vulnerability, and help others even to the postponement of self-care may be beneficial in some domains such as academic and work success, this effortful coping orientation can also have negative consequences for both physical and psychological health (Perez et al., 2023; Woods-Giscombé, 2010). If one’s coping orientation is to constantly strive to meet the expectations of Superwoman Schema, this may lead to emotional exhaustion, avoiding support from others, and chronic stress (Perez et al., 2023; Woods-Giscombé, 2010). Although many Black American women take pride in demonstrating resilience and success in the face of adversity, coping strategies characterized by high-effort endurance, emotional suppression, and caretaking have been linked to increased psychological distress and the onset or progression of physical health conditions (Jones et al., 2025; Knighton et al., 2022; Leath et al., 2022; Nelson et al., 2022; Perez et al., 2023). These findings suggest that when Black American women encounter stressors for which they lack adequate resources, reliance on the Superwoman Schema may intensify the negative effects of those stressors. Therefore, the present study explores the relationships among multiple forms of racial discrimination, endorsement of Superwoman Schema, and psychological distress.
Racial Discrimination and Mental Health Among Black American Women
This focus is especially important given the deleterious mental health implications of experiencing racial discrimination both personally and vicariously (see Vines et al., 2017, for a review). One’s experiences of discrimination and racism, whether experienced directly or observed or learned about, contribute to stress. For Black American mothers, this burden is compounded by concerns about their children’s exposure to racial discrimination (Turner, 2020). Child-experienced racial discrimination can negatively affect their parents, specifically by reducing parent–child relationship quality (Riina & McHale, 2012) and reducing positive parenting practices, such as involved-vigilant parenting (i.e., parental responsiveness and demandingness; Varner et al., 2019), as well as increasing risk of parental substance use (Gibbons et al., 2004), poor mental health (Jelsma et al., 2022, 2024), and poor self-rated health (Colen et al., 2019; Jelsma et al., 2024). These findings reflect principles of life course theory and particularly the notion of “linked lives” (Elder, 1998; Elder et al., 2003), specifically that human lives are lived interdependently, and the events that impact one individual will have consequences for others in their social environment (Gee et al., 2012).
Despite this known interdependence, there remains a paucity of research documenting how Black American mothers’ mental health is affected by witnessing or learning about their child’s experiences of racial discrimination. Vicarious discrimination generally, such as reading racist comments or seeing racist videos online, has been shown to elicit similarly negative physical and psychological responses to personally experienced racial discrimination (Moody et al., 2023). Qualitative studies have highlighted that racial discrimination targeting their children is a significant source of concern for Black American mothers (Turner, 2020). However, quantitative research specifically measuring the psychological toll of child-experienced racial discrimination for Black mothers is scarce. To date, only one study (using the same sample as the current investigation) has found that adolescent-experienced racial discrimination is associated with elevated maternal depressive symptoms (Holloway & Varner, 2023). Relatedly, within a sample of mostly (but not exclusively) Black American mothers, Gibbons and colleagues (2004) reported that adolescent experiences of discrimination were linked to increased parental substance use. Taken together, these findings underscore a critical and underexplored dimension of Black American women’s mental health that warrants further investigation.
Superwoman Schema as a Mediator
Expanding this line of inquiry is particularly important given that, as discussed above, vicariously experienced racial discrimination is known to negatively influence health in a pattern like personally experienced racial discrimination (Moody et al., 2023). For Black American mothers raising Black children, their children’s experiences of racial discrimination may be a pervasive and unremitting race-related stressor. In this context, the Superwoman Schema may serve as a culturally shaped coping orientation, characterized by the suppression of personal emotions in order to meet the emotional needs of others and manage multiple social and familial expectations (Woods-Giscombé, 2010). Superwoman Schema reflects multiple dimensions of coping often expected of Black American women including an obligation to manifest strength, suppress emotion, resist showing vulnerability, help others even to the extent of postponement of self-care, and an intense motivation to succeed (Chance, 2022; Woods-Giscombé, 2010). While these coping strategies may be adaptive in some contexts, prior research has linked endorsement of Superwoman Schema to heightened levels of stress, anxiety, and depression among Black American women (Erving et al., 2024; Jones et al., 2025; Knighton et al., 2022; Leath et al., 2022; Nelson & Cherry, 2024; Platt & Fanning, 2023).
Illustrating the connection between stress, Superwoman Schema, and mental health, Knighton and colleagues (2022) found that among educated, middle-class African American women, endorsing an obligation to show strength/suppress emotions mediated the relationship between perceived racial microaggression and psychological distress. Of note, this previous study only tested one type of race-related stressor (perceived microaggressions), one dimension of Superwoman Schema (a combined construct reflecting an obligation to show strength and suppress emotion), and one mental health outcome (combined depressive and anxiety symptoms). We use this preliminary evidence to motivate a further examination of the relationships between multiple dimensions of race-related stressors, Superwoman Schema, and mental health. Given prior research indicating that the internalized expectation to remain strong, emotionally restrained, and self-sacrificing can significantly tax the mental health of Black American women (Jones et al., 2025; Knighton et al., 2022; Nelson & Cherry, 2024; Nelson et al., 2022; Platt & Fanning, 2023), we hypothesize that stronger endorsement of Superwoman Schema may help explain how personally and vicariously experienced racial/ethnic discrimination undermine psychological well-being. Superwoman Schema is particularly relevant for Black American mothers, who are often expected to serve as emotional anchors for their children and to model strength in the face of adversity (Woods-Giscombé, 2010).
Purpose of the Present Study
Recognizing the unique pressures faced by this population, the present study examined the relations among personally and vicariously experienced (experienced by the one’s adolescent child) racial discrimination, Superwoman Schema, and Black American mothers’ mental health (depressive symptoms, perceived stress, anxiety). Based on previous research with personal (Vines et al., 2017) and child-experienced racial discrimination (Colen et al., 2019; Gibbons et al., 2004), we hypothesized that personally experienced and adolescent-experienced racial discrimination would be associated with higher depressive symptoms, perceived stress, and anxiety for Black American mothers. Previous research suggests that the expectations of Superwoman Schema to display strength and suppress emotion are harmful for Black American women’s mental health (based on unidimensional measures of mental health; Knighton et al., 2022). Therefore, we hypothesized that when examining multiple forms of race-related stress (personally experienced and adolescent-experienced), Superwoman Schema would mediate the influence of both forms of race-related stress on three dimensions of mental health: depressive symptoms, perceived stress, and anxiety. Figure 1 illustrates the hypothesized model. To account for potential confounding influences, we statistically controlled for maternal and adolescent age, adolescent gender, maternal marital status, maternal education level, and the racial composition of the adolescent’s school, given prior evidence that these factors are associated with both reported experiences of discrimination (Williams, 2016) and psychological distress (Araya et al., 2003; Brummer et al., 2014; Krain & Kendall, 2000; Simon, 1998). Conceptual model linking personally or adolescent-experienced racial discrimination, all four dimensions of Superwoman Schema, and mental health. Personally and adolescent-experienced racial discrimination were examined in separate statistical models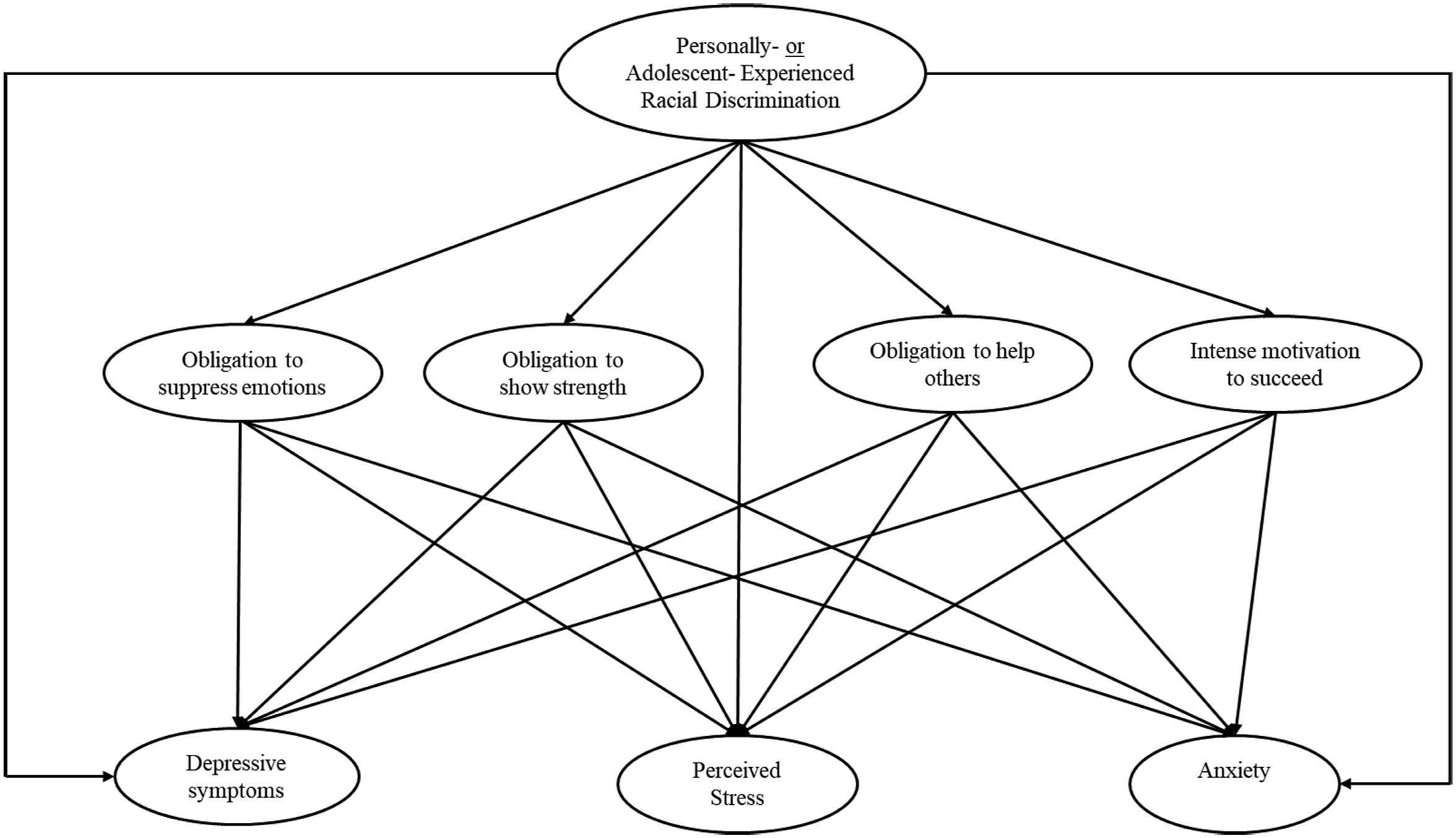
Method
Participants
Sample characteristics
Procedure
The study was approved by the Institutional Review Board, and then we collected data through Survey Sampling International (SSI; now called Dynata, https://www.dynata.com), an online survey panelist provider that uses a variety of incentives to compensate participants for completing surveys. This recruitment strategy meant that participants of the current study had previously signed up with SSI/Dynata to receive online surveys to complete in exchange for points, with the number of points determined by effort required and the length of the survey, which was estimated to take 30 minutes. Participants also had to complete screening questions to verify eligibility. To be included in the study, participants had to indicate that they were the parent of a child between ages 11 and 18 years (stepparents and grandparents were excluded). Participants who had multiple children in the age range were instructed to complete the survey responding only about one child, referred to as the “focal child.” SSI/Dynata alerted participants who met the agreed upon criteria (African American or Black adult over 18 years old, with children aged 11–18) that a survey was available. Invitations were distributed using email invitations, as well as desktop and in-app alerts. SSI/Dynata offered $2.50 in points to participants that could be used to purchase gift cards, charity donations, and other prizes. Participants were instructed to answer all parenting- or child-related questions referencing one adolescent of their choosing, referred to as the focal child. The survey questions were presented in the same order for all participants. Participants were screened out during data collection if they responded incorrectly to two or more careless responding items (e.g., “please select ‘Rarely’ for this item”), removing 180 mothers. Parents who reported a less than 10-year age difference between themselves and their focal child were also excluded from the present analyses (removing five mothers). These exclusion criteria brought the final sample size to 319 women.
Measures
Personal Racial Discrimination
Participants reported their daily experiences of racial discrimination using Williams et al.'s (2008) Extended Everyday Discrimination Scale (EDS). For the current study, participants were instructed to think only about discrimination because of their race. This scale consisted of 10 items (e.g., “you are treated with less courtesy than other people”). Participants responded to each item using a 6-point rating scale that ranged from 1 = never to 6 = almost every day (higher scores reflect more discrimination). Cronbach’s alpha was .92. Findings have shown this measure demonstrates significant convergent validity with another nine-item dichotomous measure of overt discrimination due to race/ethnicity (Stucky et al., 2011), Williams and colleagues' (1997) Major Experiences of Discrimination Scale (Williams et al., 2018), and Williams and colleagues’ (2018) Trauma-Symptoms of Discrimination Scale. The EDS measure has shown discriminant validity in low correlations with Roberts and colleagues’ (1999) 12-item Multigroup Ethnic Identity Measure (Williams et al., 2018). Research with this sample using this scale has been published previously (Holloway & Varner, 2021a, 2021b).
Perceived Adolescent-Experienced Racial Discrimination
Participants reported their adolescents’ daily experiences of racial discrimination also using items adapted from Williams and colleagues' (2008) Extended Everyday Discrimination Scale. This 10-item scale was adapted to measure how frequently their child experiences daily discrimination because of their race with the same items but referencing their child (e.g., “your child is treated with less courtesy than other people”). Participants responded to each item using a 6-point rating scale that ranged from 1 = never to 6 = almost every day to describe how often their adolescents had experienced different types of racial discrimination (higher scores reflect more discrimination). Cronbach’s alpha was .93. This adapted scale (reporting on child’s discrimination) has not been previously tested for convergent or discriminant validity (see above for convergent and discriminant validity of the original scale); however, we have previously published using this adapted measure with a different subsample of this dataset (Jelsma et al., 2022). We also conducted a preliminary exploratory factor analysis (EFA) to confirm this adapted measure still functioned as expected, χ2 (45) = 2447.19, p < .001, CFI = .98, TLI = .96, SRMR = .02.
Superwoman Schema
A brief version of the Giscombé Superwoman Schema Questionnaire (Woods-Giscombé et al., 2019) was administered to the participants. This assessment contains 23 items from the original questionnaire and combines obligation to suppress emotions and resistance to show vulnerability (the two most conceptually related and empirically correlated constructs from the original measure). Thus, there were four subscales: obligation to present an image of strength (e.g., “I have to be strong”; 4 items; α = .76); obligation to suppress emotions and resist vulnerability (e.g., “I hide my stress”; 7 items; α = .79); intense motivation to succeed (e.g., “The only way for me to be successful is to work hard”; 4 items; α = .64); and obligation to help others even to the postponement of self-care (e.g., “I put everyone else’s needs before mine”; 8 items; α = .52). Response options ranged from 1 = not true for me to 4 = true for me all the time (higher scores reflect more Superwoman Schema). Previous research shows adequate reliability and construct validity for all the subscales (Woods-Giscombé et al., 2019). Subscales are typically examined as individual variables in previous research (Allen et al., 2019; Jones et al., 2025; Knighton et al., 2022; Leath et al., 2022; Nelson & Cherry, 2024). Subscale succeed showed convergent validity with subscale strength (r = .51, p < .001), emotion suppression (r = .70, p < .001), and help others (r = .52, p < .001). Subscales emotion suppression and help others also showed convergent validity (r = .53, p < .001). Subscale strength showed discriminant validity with subscale emotion suppression (r = .27, p < .001) and help others (r = .14, p = .09).
Depressive Symptoms
An 11-item brief version of the Center for Epidemiologic Studies-Depression Scale (CES-D; Radloff, 1977) was administered to participants. This assessment covers symptoms from the past week (e.g., “I felt lonely” and “I could not get going”; α = .83). Response options ranged from 0 = rarely or none of the time (less than 1 day) to 3 = most or all of the time. Certain items were reverse coded to reflect higher scores as more frequent depressive symptoms. The CES-D short-form scale is a widely used measure of depression and has demonstrated adequate reliability, concurrent validity, and construct validity among other samples of Black/African American adults (Radloff, 1977; Torres, 2012). This measure shows high convergent validity with perceived stress (r = .80, p < .001) and anxiety (r = .87, p < .001) in this sample. The CES-D has demonstrated discriminant validity by demonstrating low correlations with age, gender, and socioeconomic status in another Black and African American adult sample (Taylor et al., 2024).
Perceived Stress
The 10-item Perceived Stress Scale (PSS; Cohen, 1988) was administered to participants. This assessment covers perceived stress from the past month (e.g., “How often have you been upset because of something that happened unexpectedly?” and “How often have you felt nervous and stressed?”; α = .81). Response options ranged from 1 = never to 5 = very often. Certain items were reverse coded to reflect higher scores as higher perceived stress. The PSS has demonstrated adequate reliability, criterion-related validity, and predictive validity in other samples of Black American women (Adkins‐Jackson & Levine, 2020; Platt & Fanning, 2023). This measure showed high convergent validity with depressive symptoms (r = .80, p < .001) and anxiety (r = .82, p < .001) in this sample. Regarding discriminant validity, Catabay and colleagues (2019) found significant negative associations between the PSS and Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988) and the PSS and Conner-Davidson Resilience Scale (CD-RISC 10; Campbell-Sills & Stein, 2007) within another sample of Black American women.
Anxiety
The 7-item Generalized Anxiety Disorder Scale (GAD-7; Spitzer et al., 2006) was administered to participants. This instrument assesses anxiety over the past 2 weeks and asks how often you have been bothered by issues such as “feeling nervous, anxious, or on edge” or “not able to stop or control worrying” (α = .93). Scale responses ranged from 1 = not at all to 4 = nearly every day (higher scores reflect more anxiety). The GAD-7 scale is a well-validated instrument and has shown adequate reliability and a single-factor structure other samples of Black/African American adults (Cleland et al., 2021; Parkerson et al., 2015). This measure showed high convergent validity with depressive symptoms (r = .87, p < .001) and perceived stress (r = .82, p < .001) in this sample. Regarding discriminant validity, Hubbard and colleagues (2022) found significant negative associations between the GAD-7 and two subscales (racial centrality and racial private regard) of the Multidimensional Inventory of Black Identity (MIBI; Sellers et al., 1998) and with Social Provisions Scale (a measure of perceived social support; Cutrona & Russell, 1987) within a sample of Black young adults.
Covariates
Analyses controlled for age (parent age in the personal discrimination model, focal child age in the adolescent discrimination model), focal child gender (dummy coded female = 1, male or other = 0 in order to account for the effect of sharing the same gender as the adolescent experiencing discrimination, which could be particularly triggering if the child’s experiences resemble the mothers’ own experiences in adolescence), parental marital status (1 = married, 0 = never married/divorced/separated/widowed), and parent highest level of education (1 = completed junior high school or less to 9 = doctoral (PhD/M.D./J.D.)). To better contextualize adolescent-experienced racial discrimination, we also controlled for the racial composition of the adolescent’s school, as previous research shows school racial composition can influence both perceptions of discrimination and subsequent well-being (Seaton & Yip, 2009) (1 = almost all Black people to 5 = almost no Black people).
Data Analysis Plan
Beginning with a confirmatory factor analysis (CFA) with the total sample, the sample variance-covariance matrices were examined in order to determine whether all items significantly and strongly loaded onto the corresponding latent construct of interest. We then used Structural Equation Modeling (SEM) to test whether Superwoman Schema mediated the influence of both forms of racial discrimination (personally and adolescent-experienced) on three forms of psychological distress (depressive symptoms, perceived stress, and anxiety). We report bias-corrected bootstrap estimates using 1,000 iterations. Due to model nonconvergence when including all latent variables with bootstrapping in one model, we separated the mediation analyses into one model with personally experienced racial discrimination, and the other model with adolescent-experienced racial discrimination. For CFA and SEM, final acceptance or rejection of models was based on three indices and their cut-off points (Brown, 2015; Hu & Bentler, 1999; Kline, 2023) to assess goodness of fit for the models: the comparative fit index (CFI; values of .95 or greater suggesting close fit, values greater than 0.90 suggesting acceptable model fit), the root-mean-square error of approximation (RMSEA; values of .06 or less), and the standardized root-mean-square residual (SRMR; values of .08 or less). In addition, we examined an alternative model switching the mediators and outcomes (as is best practice with cross-sectional SEM; MacCallum et al., 1993), testing mental health as mediators between personally and adolescent-experienced racial discrimination and the Superwoman Schema constructs.
Results
Descriptive Statistics and Preliminary Analysis
Before conducting primary analyses, data were cleaned and screened for outliers. Missingness rates of key variables were low (0.3 to 2.8%), consistent with a Missing at Random (MAR) mechanism and suggests missing values are evenly distributed across the variables of interest with no single variable exhibiting substantial nonresponse (Little et al., 2014). Therefore, using full-information maximum likelihood (FIML) estimation in Mplus 8.11 was chosen as the most optimal technique to yield unbiased estimates of parameters and their standard errors (Little et al., 2014; Muthén & Muthén, 2018). The data for all observed variables were screened to evaluate distributional qualities including outliers, normality, collinearity, non-zero variances, independent and random normally distributed errors, linearity, and homoscedasticity; all assumptions were met.
Means, Standard Deviations, Reliability, and Correlations of Latent Study Variables
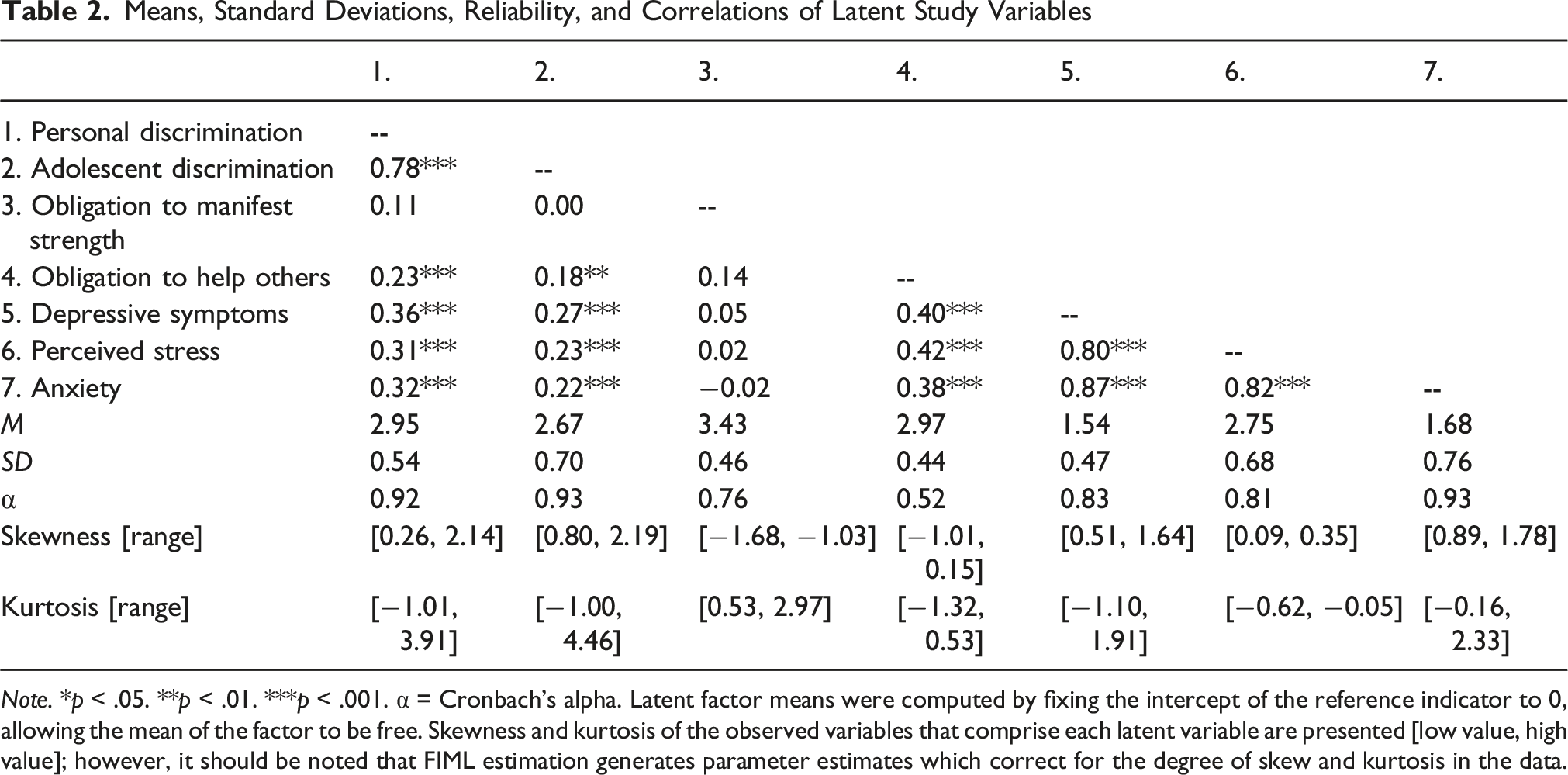
Note. *p < .05. **p < .01. ***p < .001. α = Cronbach’s alpha. Latent factor means were computed by fixing the intercept of the reference indicator to 0, allowing the mean of the factor to be free. Skewness and kurtosis of the observed variables that comprise each latent variable are presented [low value, high value]; however, it should be noted that FIML estimation generates parameter estimates which correct for the degree of skew and kurtosis in the data.
Measurement Model
The initial measurement model/CFA included all indicators for personally and adolescent-experienced discrimination, mental health outcomes (anxiety, depressive symptoms, and perceived stress), and the four Superwoman Schema domains: obligation to present an image of strength, obligation to suppress emotions and resist vulnerability, intense motivation to succeed, and obligation to help others even to the postponement of self-care. However, we could not confidently specify a model for SEM that contained the full number of items due to poor model fit: χ2 (2376) = 4968.32, p < .001, comparative fit index (CFI) = 0.80, root mean square error of approximation (RMSEA) = 0.06 [CI: 0.06, 0.06], and standard root mean-square residual (SRMR) = 0.07. Problems with the Superwoman Schema measure lied specifically with inconsistent loadings and inadequate model fit of obligation to suppress emotions and resist vulnerability and intense motivation to succeed. These problems with the full Superwoman Schema scale led us to drop the poorly defined factors of obligation to suppress emotions and resist vulnerability and intense motivation to succeed and proceed only using the well-defined factors obligation to show strength and obligation to help others even to the postponement of self-care. Previous research has also used obligation to show strength and obligation to help others even to the postponement of self-care as stand-alone measures (Allen et al., 2019; Knighton et al., 2022). The results of the CFA with all measured variables also resulted in four reverse-coded items being removed from the Perceived Stress Scale, which is aligned with a previous research study failing to find adequate factor loadings for these items (Ezzati et al., 2014). Two reverse coded items from the CES-D were also subsequently removed from the model due to unacceptable factor loadings. After making these refinements to the models, the model fit indices for the Personal Discrimination measurement model/CFA were χ2 (885) = 1563.95, p < .001, CFI = 0.91, RMSEA = 0.05 [CI: 0.05, 0.05], and SRMR = 0.06, and for the Adolescent Discrimination model were χ2 (885) = 1557.06, p < .001, CFI = 0.92, RMSEA = 0.05 [CI: 0.05, 0.05], and SRMR = 0.05. The loadings of the remaining measured variables on the latent variables were statistically significant at p < .05, suggesting that the latent variables were defined well by the measured variables (post-refinement). Among the latent variables, all correlations were significant except for those with obligation to manifest strength.
Structural Models
The structural model with personally experienced racial discrimination fits the data adequately, χ2 (1086) = 1815.72, p < .001, CFI = 0.90, RMSEA = 0.05 [CI: 0.04, 0.05], and SRMR = 0.05. The structural model with adolescent-experienced racial discrimination also fits the data adequately, χ2 (1115) = 1851.39, p < .001, CFI = 0.91, RMSEA = 0.05 [CI: 0.04, 0.05], and SRMR = 0.06.
Personal Discrimination Model
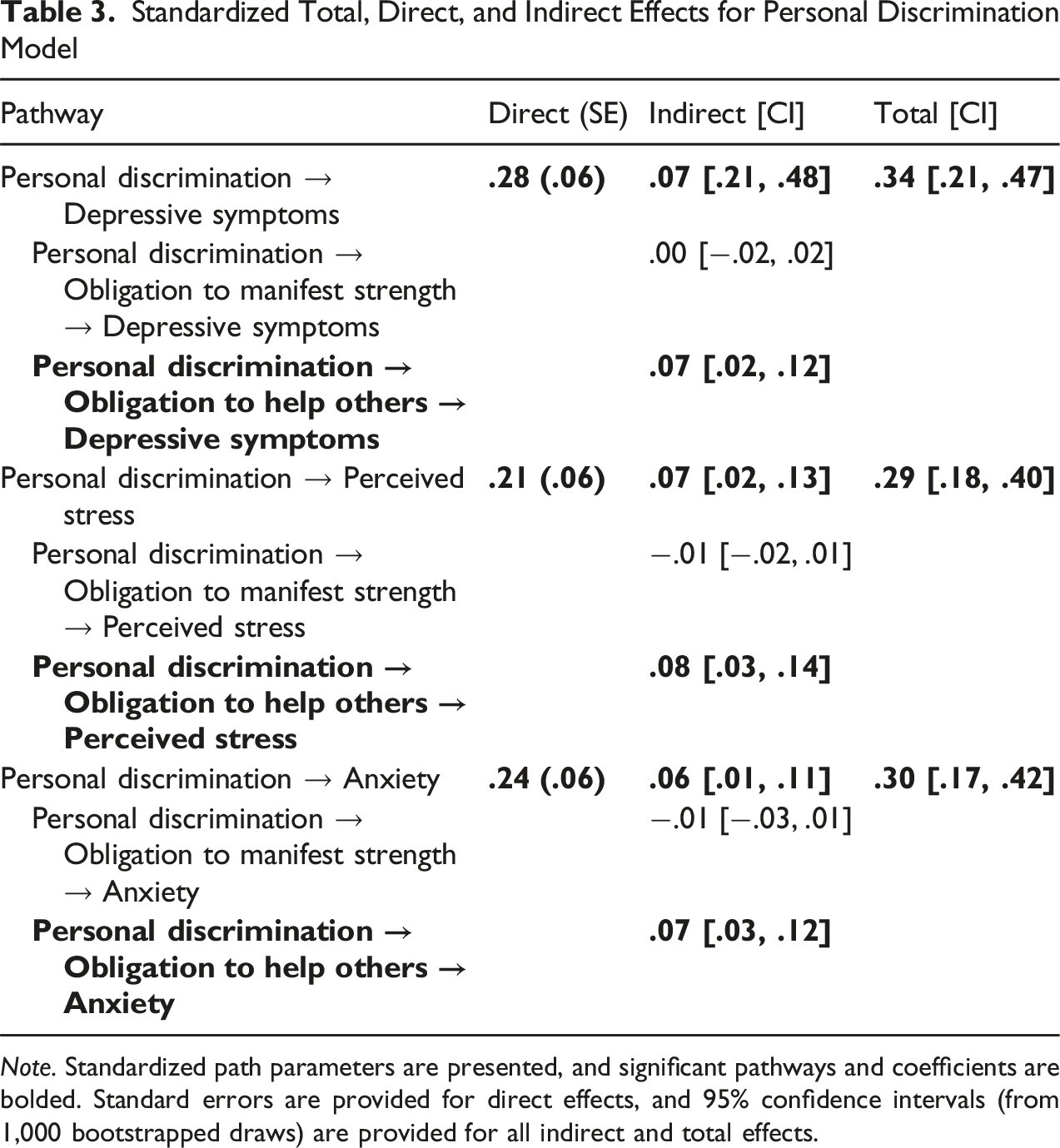
The standardized path parameters for the personally experienced racial discrimination model are presented in Figure 2. Personally experienced racial discrimination was directly related to more depressive symptoms (β = .28, p < .001), perceived stress (β = .21, p < .001), and anxiety (β = .24, p < .001). In the mediation model testing obligation to manifest strength and obligation to help others even to the extent of postponement of self-care as mechanisms linking personal discrimination and mental health, obligation to help others emerged as a significant mediator between personal discrimination and all three mental health outcomes (see Table 3). Specifically, personal discrimination was related to higher obligation to help others, which was then related to higher depressive symptoms, perceived stress, and anxiety. There were no significant indirect effects through obligation to show strength. Mediation model linking personally experienced racial discrimination, obligation to show strength and obligation to help others even to the postponement of self-care, and mental health. Standardized path parameters are presented. Covariances were estimated between the endogenous variables, but they are not shown for the sake of simplicity. Significant paths are shown in solid line, and non-significant paths are shown in dashed line. *p < .05, *p < .01, and ***p < .001 Standardized Total, Direct, and Indirect Effects for Personal Discrimination Model Note. Standardized path parameters are presented, and significant pathways and coefficients are bolded. Standard errors are provided for direct effects, and 95% confidence intervals (from 1,000 bootstrapped draws) are provided for all indirect and total effects.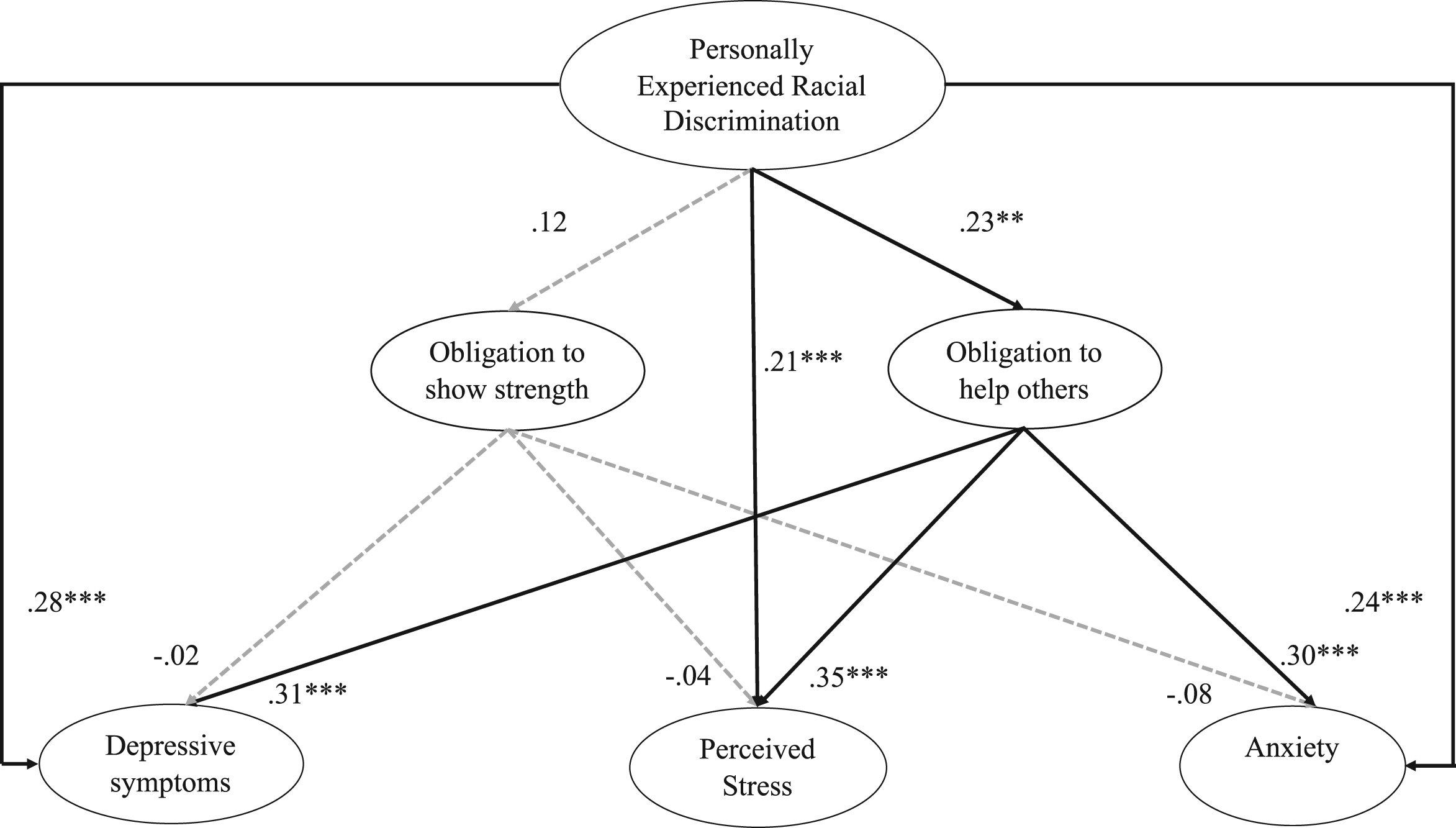
Adolescent Discrimination Model
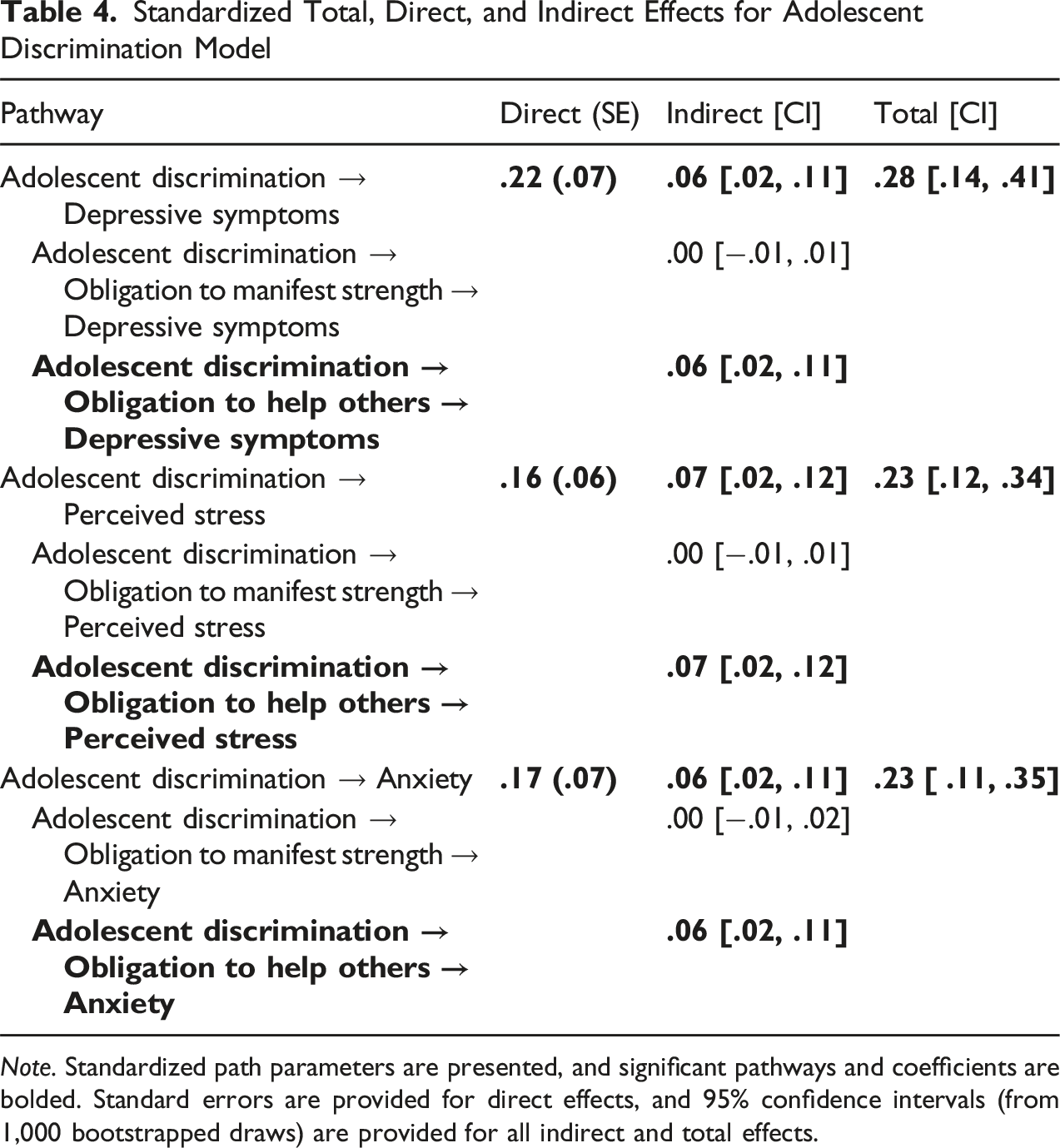
The standardized path parameters for the adolescent-experienced racial discrimination model are presented in Figure 3. Adolescent-experienced racial discrimination was directly related to more depressive symptoms (β = .22, p = .002), perceived stress (β = .16, p = .004), and anxiety (β = .17, p = .01). In the mediation model testing obligation to manifest strength and obligation to help others even to the extent of postponement of self-care as mechanisms linking adolescent discrimination and mental health, obligation to help others emerged as a significant mediator between personal discrimination and all three mental health outcomes (see Table 4). Specifically, adolescent discrimination was related to higher obligation to help others, which was then related to higher depressive symptoms, perceived stress, and anxiety. Again, there were no significant indirect effects through obligation to show strength. Mediation model linking adolescent-experienced racial discrimination, obligation to show strength and obligation to help others even to the postponement of self-care, and mental health. Standardized path parameters are presented. Covariances were estimated between the endogenous variables, but they are not shown for the sake of simplicity. Significant paths are shown in solid line, and non-significant paths are shown in dashed line. *p < .05, *p < .01, and ***p < .001 Standardized Total, Direct, and Indirect Effects for Adolescent Discrimination Model Note. Standardized path parameters are presented, and significant pathways and coefficients are bolded. Standard errors are provided for direct effects, and 95% confidence intervals (from 1,000 bootstrapped draws) are provided for all indirect and total effects.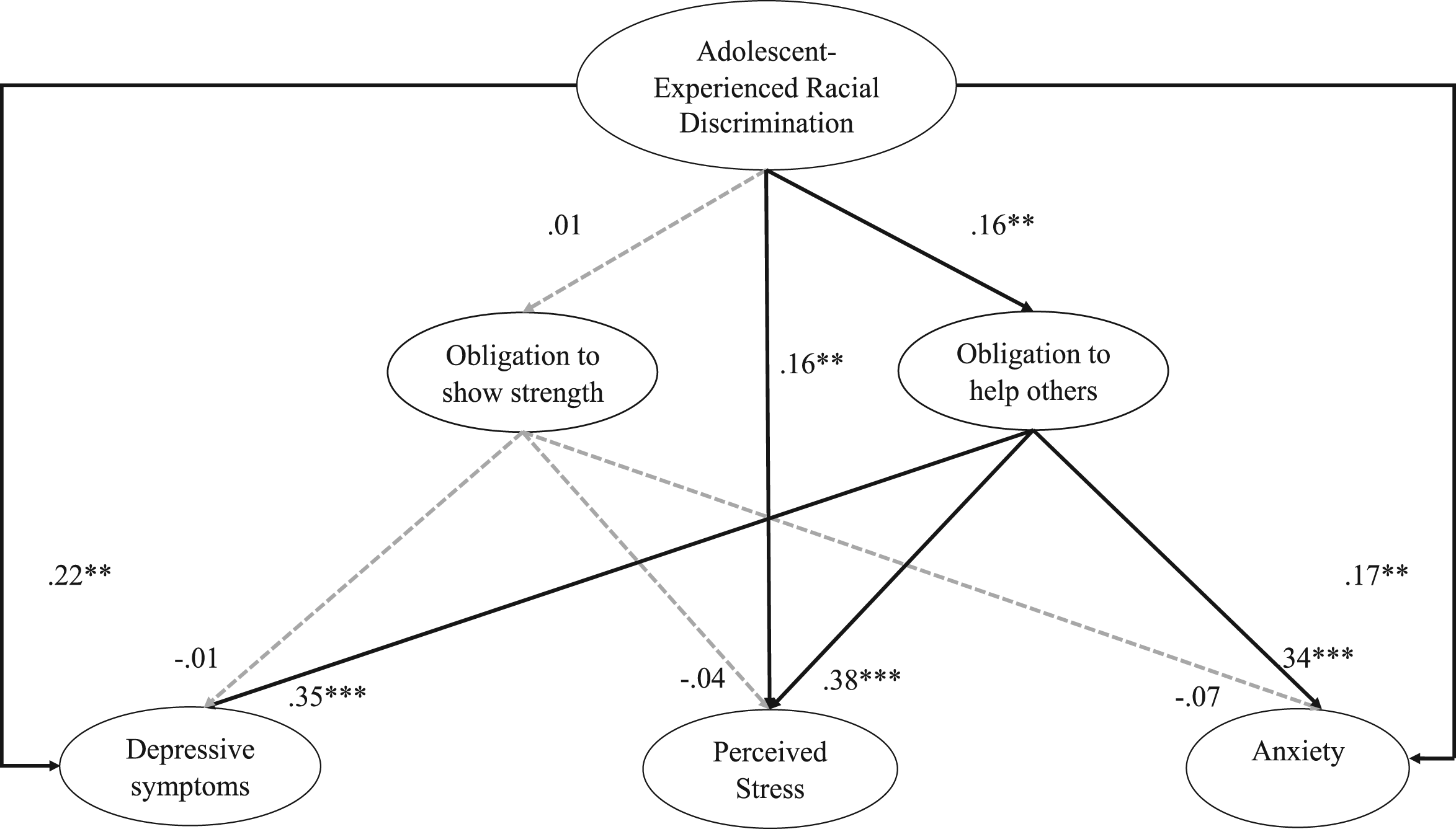
Alternative Models
We tested alternative models with mental health (depressive symptoms, perceived stress, and anxiety) as mediators between personally and adolescent-experienced racial discrimination and the Superwoman Schema constructs (obligation to manifest strength and obligation to help others even to the extent of postponement of self-care). The model fit indices of the alternative models were worse than the proposed models for both the personal discrimination model (χ2 (1093) = 2366.67, p < .001, CFI = 0.83, RMSEA = 0.06 [CI: 0.06, 0.06], and SRMR = 0.15) and the adolescent discrimination model (χ2 (1093) = 2380.19, p < .001, CFI = 0.84, RMSEA = 0.06 [CI: 0.06, 0.06], and SRMR = 0.16). We did not move forward with these models because of poor fit with the data.
Discussion
The current study examined the relationship between two forms of race-related stress (personally and vicariously experienced racial discrimination), Superwoman Schema, and three mental health outcomes (depressive symptoms, perceived stress, and anxiety) among Black American mothers with an adolescent child. Our results demonstrate that both forms of race-related stress were related to increased depressive symptoms (9 of the 11 originally measured symptoms), perceived stress (6 of the 10 originally measured symptoms), and anxiety. Due to inadequate model fit, only two of the four Superwoman Schema subscales measured were able to be tested as mediators between discrimination and mental health. The mediation analyses indicated that endorsing an obligation to help others even to the extent of postponement of self-care partially explained the relationship between racial stressors and psychological distress. This finding extends prior scholarship by elucidating the unique mechanisms by which racial discrimination might become distressing for Black American women.
Our findings are consistent with previous evidence of the negative implications of personally experienced (Vines et al., 2017) and vicariously experienced (Colen et al., 2019; Ong, 2021) racial discrimination for Black American adult health. The finding that adolescent-experienced racial discrimination was related to mothers’ higher depressive symptoms, perceived stress, and anxiety reflects the tenets of the “linked lives” principle of life course theory (Elder, 1998; Elder et al., 2003), specifically that events that impact one individual will have consequences for others in their social environment. Although previous research has demonstrated that child-experienced racial discrimination may influence parents’ self-rated physical health (Colen et al., 2019), substance use (Gibbons et al., 2004), and parent–child relationship quality (Riina & McHale, 2012), the current study contributes to the growing body of research demonstrating the mental health consequences of having one’s adolescent child experience racial discrimination. For Black American mothers, adolescent-experienced racial discrimination may be adding to one’s burden of stress, which can erode mental health over time. The current study provides evidence of the “spillover” effects of racial discrimination, indicating that the negative impacts of race-based discrimination may not be limited to only those who directly experience the race-related stressors.
The current study also contributes to the understanding of culturally sensitive coping (Boyd-Franklin, 2003; Butler‐Barnes & Martin, 2023; McAdoo, 2007; McAdoo & McAdoo, 1985), specifically by expanding our knowledge of the mental health implications of some dimensions of Superwoman Schema as a mediator of the relationship between racial discrimination and mental health among Black American adult women. Superwoman Schema (Woods-Giscombé, 2010) is an intersectional and multidimensional framework developed to understand stress burden and coping among Black American women, outlining core features of obligations and expectations often placed upon their shoulders. Of note, we excluded two of the Superwoman Schema dimensions—intense motivation to succeed and obligation to suppress emotions and resist vulnerability—from our analyses since they did not fit the data. It is therefore possible that our findings may not hold up when replicated. We are cautiously reassured about the reliability of our primary finding indicating that an obligation to help others even to the extent of postponement of self-care partially explains the relationship between racial stressors and psychological distress since other studies also show such an obligation is significantly related to higher prevalence of psychological distress (Erving et al., 2024; Jones et al., 2025; Leath et al., 2022; Nelson & Cherry, 2024; Platt & Fanning, 2023). Emphasizing this link is pertinent to psychological well-being because prior studies have elucidated the psychological toll of postponement of self-care (Woods-Giscombé et al., 2016). Feeling the obligation to put oneself last in conjunction with experiencing race-related stressors might reasonably erode mental well-being over time. Culturally specific interventions which take these unrelenting stressors and expectations into account are necessary to properly serve the mental health needs of Black American mothers.
We did not find support for any mediation by obligation to manifest strength. Interestingly, obligation to manifest strength had no direct links with either form of discrimination or any of the mental health outcomes within this sample. This finding is contrary to previous research which has found obligation to manifest strength directly related to depression and anxiety (Abrams et al., 2019; Jones et al., 2025; Nelson & Cherry, 2024) as well as a mediator of the relation between racial microaggression and psychological distress (Knighton et al., 2022) among Black and African American women. It is possible that women who feel significant pressure to embody strength might also cope by suppressing emotional issues and needs (Abrams et al., 2019; Jones et al., 2025), and could underreport feelings of depressive symptoms, perceived stress, and anxiety on a survey. Poor mental health can often be ignored when it is perceived as a display of strength (Abrams et al., 2019). Women who score high on obligation to show strength might, through suppressing vulnerability and manifesting resilience, not appraise racial discrimination as threatening and feel capable to cope with or manage it (Sheehan et al., 2024). In a previous study examining the moderating effect of obligation to manifest strength for allostatic load, Black women who scored higher on manifesting strength were protected from the negative effects of racial discrimination for allostatic load (Allen et al., 2019). Specifically, the association between racial discrimination and allostatic load was null among those in the high strength group (Allen et al., 2019). Our sample generally scored very high on obligation to manifest strength (on a scale from 1 to 4, the average score of each of the four indicators ranged from 3.23 to 3.61) and might explain the lack of association between discrimination, obligation to manifest strength, and mental health in this high strength sample.
Contributions
There are several strengths of the current study. First, this study demonstrates the indirect links from two different forms of racial discrimination (personally and vicariously experienced by one’s child) to multiple domains of mental health (depressive symptoms, perceived stress, and anxiety) via a culturally relevant coping strategy for Black American women (obligation to help others even to the extent of postponement of self-care). It is important to incorporate Black American mothers’ unique experience of being expected to help others even to the detriment of their own well-being to understand the full effect of racial discrimination for mental health. Second, whereas most of the existing research on racial discrimination and mental health only focuses on personally experienced discrimination, the current study added a salient vicarious form of discrimination exposure, adolescent-experienced discrimination, to show that Black American mothers are negatively affected by not only their own experiences of discrimination but also their children’s experiences (Turner, 2020). Another strength is our use of structural equation modeling with latent variables, which reduces measurement error and thus improves interpretability of the results (Seo et al., 2016).
Limitations
Although the current study contributes to the existing literature, limitations should be noted. First, the generalizability of the current findings to other samples of Black American mothers should be tested. Participants of the current study were generally highly educated and due to the nature of the survey, had access to a computer, time to complete the survey, and signed up to participate in surveys from SSI. Future research would greatly benefit from different methods of data collection as well as collecting data from a larger sample of low-income Black American parents. Second, poor model fit of the Superwoman Schema dimensions not included in this study prevented us from testing the mediating roles of other potentially relevant coping dimensions. The results of the CFA also resulted in some items being removed from the depressive symptoms and perceived stress latent variables (due to unacceptable factor loadings). This study should be replicated with a larger sample of Black American mothers, and a different set of robust measures allow for further testing of all the Superwoman Schema constructs and retaining all items from the mental health scales. Third, with only cross-sectional data, we are not able to make any firm conclusions on causality.
Implications and Conclusions
Despite these limitations, this study is novel in testing the role of two culturally relevant coping mechanisms in mediating the influence of two separate and salient forms of racial discrimination for Black American mothers’ mental health. With the knowledge that an obligation to help others even to the postponement of self-care may help explain how personal and vicarious discrimination is related to more mental health problems for Black American mothers, culturally sensitive interventions might encourage Black American women to seek professional help and prioritize self-care before mental health symptoms become concerning (Boyd-Franklin, 2003; McAdoo, 2007; McAdoo & McAdoo, 1985). It is important to recognize, however, that Black women who endorse an obligation to help others even to the postponement of self-care may avoid therapy or self-care for variety of reasons, including excessive strain and lack of time or resources to seek this kind of help, or cultural bias against seeking mental health care (Abrams et al., 2014). Feeling an obligation to help others even to the postponement of self-care may be a legitimate barrier to getting Black women into therapy and should be considered by mental health care professionals providing services to Black American mothers (Abrams et al., 2014). Culturally sensitive interventions should also recognize that many Black Americans are part of extended kin, community, and church networks in which there is strong reliance on mutual support, which can be helpful in navigating stressors such as racism and discrimination (Boyd-Franklin, 2003; McAdoo, 2007; McAdoo & McAdoo, 1985; Murry et al., 2018; R. J. Taylor et al., 2016). These support networks can also increase cultural expectations to help others and for reciprocity, particularly among Black women (Boyd-Franklin, 2003; Cross et al., 2018; McAdoo, 2007; McAdoo & McAdoo, 1985). Since we were not able to include the other two forms of Superwoman Schema, there is also a need for more research on the multidimensional nature of the Superwoman Schema scale in relation to Black women’s mental health. Black women’s patterns of endorsement of various Superwoman Schema beliefs may also shape their mental health. Feeling an obligation to help others even to the postponement of self-care may be something Black American women, who experience racial discrimination both personally and vicariously through their children, might do unconsciously as a means of surviving in an anti-Black environment (Jacob et al., 2023). This warrants further examination in future research. Clinicians can share with Black American women how acting on this obligation can be problematic for mental health. Integrating understanding of culturally relevant coping schemas such as Superwoman Schema will improve mental health care provided to Black American mothers.
Footnotes
Acknowledgments
We appreciate the helpful feedback offered by Aprile Benner, Bridget Goosby, Elizabeth Muñoz, and Cheryl Woods-Giscombé in the preparation of this manuscript.
Ethical Consideration
This study received ethical approval from the University of Texas at Austin IRB.
Consent to Participate
All participant information was de-identified, and participant consent was not required.
Author Contributions
Jelsma contributed to original draft preparation, conceptualization, data curation, and formal analysis. Varner contributed to review and editing, conceptualization, data curation, and supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant, P2CHD042849, Population Research Center, awarded to the Population Research Center at The University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Participant data will not be shared with third parties.