
Abstract
Living apart together (LAT) combines intimacy with autonomy and flexibility but, possibly, with lower commitment to exchanging support and care compared with first marriages, remarriages, and cohabitation of older adults. Data from 50- to 79-year-old respondents in the Family and Fertility Survey 2013 (Statistics Netherlands; N = 4,108) showed that older LAT partners are most often involved in exchanging emotional support. No differences were found in the receipt of daily care. Multivariate analyses showed that receiving support and care from the partner was associated with more health problems, higher quality of the partner relationship, and a broader support network. When in poor health, LAT partners were less likely to receive daily care, but not emotional support, from their partner compared with the other types. Partner relationships in later life are well equipped to provide emotional support, but partner care is facilitated largely by help from others.
Keywords
Introduction
Over recent decades, salient changes in societal norms and values have been observed regarding repartnering of older adults after divorce or widowhood. The norms and values of timing the start of (new) partnerships and the specific choices of partnership types and associated living arrangements are more varied than in the past. After finding a new partner, older adults nowadays can opt not only just for remarriage but also for cohabitation or for living apart together (LAT) relationships.
Cohabitation is defined as a coresidential intimate partnership, in which the partners are not (re)married. A LAT relationship is defined as a noncoresidential intimate partner relationship, in which the partners maintain separate households and share living quarters on an intermittent or temporary basis, for example, several days per week or at weekends (De Jong Gierveld, 2004, Levin, 2004). Transient LAT relationships are most characteristic for younger adults, where LAT is a temporary period prior to cohabitation (Turcotte, 2013); long-term stable LAT relationships are more common in older adults (Connidis, Borell, & Karlsson, 2017; Lewin, 2017; Régnier-Loilier, 2016), and a preferred type of partner relationship among those who value and experience social and financial independence. However, Lewin (2017) showed that this independence may be at the expense of the quality of the relationship, as LAT partners reported lower levels of happiness in their relationships and lower levels of emotional support received from their partner than other types of partner relationships.
Being in a supportive and committed partner relationship is particularly important in later life when health problems and need for care arise. Older persons generally provide the bulk of the support and care their partners need, and the uptake of the caregiver role is generally motivated by the strong personal bond between the partners and largely facilitated by coresidence (Broese van Groenou, de Boer, & Iedema, 2013). Yet as LAT relationships are typically not coresiding, they may lack relationship quality (Lewin, 2017) and often prioritize providing support to children, grandchildren, siblings, and other family members over supporting their partner (De Jong Gierveld, 2015; Noël-Miller, 2011). Building on studies of partner support (Lewin, 2017) and caregiving (Broese van Groenou et al., 2013), we will answer two research questions:
In the following, we provide a picture of the state of the art in relation to partner relationship types and develop our theoretical framework and hypotheses.
Varying Types of Partner Relationships in Older Age
A growing number of repartnered older adults are involved in LAT relationships (De Jong Gierveld, 2004; Lewin, 2017; Strohm, Seltzer, Cochran, & Mays, 2009; Turcotte, 2013). As regards the prevalence of LAT relationships, in Sweden the percentage of people in LAT relationships in the age group 60 to 90 years was 5% of the total population in this age group (Öberg & Bildtgard, 2014). Concentrating on the “risk” population of older adults living alone or living as parents without partners, the percentage of older adults in LAT partnerships is 26% in the age group 40 to 50 years, 20% in the age group 50 to 65 years, and 9% among those aged 65 to 79 years, according to data for the Netherlands (Otten & te Riele, 2015). Data on LAT in the United States show that 14% of unmarried noncohabiting adults aged 65 to 74 years were involved in a romantic partnership, while among those aged 75 to 85 years, the figure was 9% (Brown & Shinohara, 2013). Considering those adults in a partner relationship, data from the American NSHA survey (Wave 2005-2006) showed that 62% of adults aged 57 to 85 years are in a first marriage, 28% were remarried, 3% were in unmarried cohabitation, and 7% were involved in a LAT relationship (Lewin, 2017).
Starting a LAT relationship in later life, after divorce or widowhood, can be an attractive alternative for coresidential couple relationships. LAT arrangements can shield children and families from perceived interlopers (Cross-Barnet, Cherlin, & Burton, 2011; De Jong Gierveld & Merz, 2013; Levin, 2004; Or, 2013; Strohm et al., 2009; Turcotte, 2013; Upton-Davis, 2015) or they can support personal preferences, such as a desire for independence (Funk & Kobayashi, 2016; Haskey, 2005). Most of the older adults in LAT relationships intend to continue living independently in order to combine intimacy with flexibility, to enable to accommodate other (social) demands in their lives within the context of life course constraints (Coulter & Hu, 2017; De Jong Gierveld, 2004; De Jong Gierveld & Merz, 2013; Lewin, 2017). The proportion of LAT partners who continue to live apart over a period of 6 years or more in France is up to 50% for those aged 53 to 79 years. Moving in together is particularly rare (about 12%) over a period of 6 years among LAT partners in this age group (Régnier-Loilier, 2016).
Accordingly, LAT relationships in older age should be seen as long-term intimate bonds, but the question remains as to how they compare with (re)marriage and cohabitation.
Exchange of Support and Care
Nontangible support, such as emotional support, can be exchanged at all times and independently of geographical distance by telephone or e-mail. Instrumental support, encompassing support with household tasks or help with transportation, requires time, and living in vicinity facilitates this. Daily care tasks, the obligatory care for a dependent recipient that encompasses different types of demanding physical care, such as dressing, bathing, getting in or out of bed, and using the toilet, are considered to be the most intensive and time consuming and largely facilitated by living in vicinity (Brandt, Haberkern, & Szydlik, 2009). In this study, we focus on two types of support and care exchanges between partners in later life, one less dependent on geographical distance, namely emotional support, and one that is strictly dependent on daily presence: daily personal caregiving. The exchange of emotional support and personal care may differ between LAT and other types of partner relationships, but in different ways and for different reasons.
Expected Differences in Support and Care in LAT Versus Other Relationship Types
Emotional Support
The increasing importance of close relationships in later life and the preference of continuation of strong bonds at the expense of less strong bonds has been shown by Carstensen (1995.). The majority of older adults favor emotional close bonds above other types of bonds. This strategy of prioritizing close emotional bonds is especially salient in the lives of older LAT partners. Both partners keep their own living quarters, enabling them to continue relationships with children and other family members, including attention for realizing an affective rich relationship with the new partner (De Jong Gierveld, 2004). Additionally, several studies showed that the low level of organization of LAT relationships and the absence of many commitments and ties that characterize marriage put the focus on the emotional side of the relationship (Borell & Karlsson, 2003; Connidis et al., 2017; Karlsson & Borell, 2005; Lyssens-Danneboom & Mortelmans, 2015). Exchanging emotional support is not prevented by the absence of coresidence (Koren, 2015), nor by geographical distances between the living quarters of LAT partners (Benson & Coleman, 2016; Karlsson & Espvall, 2016). Given the dominant focus on commitment and intimacy in the LAT partner relationship, it is hypothesized that LAT partners may receive the same level or even more emotional support than in other partner relationship types (Hypothesis 1a).
Daily Personal Care
Research suggests that the level of care provided by cohabiting older partners is less intensive than the care provided by older married partners (Noël-Miller, 2011). Additionally, research by Duncan, Phillips, Carter, Roseneil, and Stoilova (2014) on intracouple support and care provided by LAT partners showed that a substantial portion of partners in LAT relationships support one another in everyday activities, but when it comes to providing care during illness, LAT partners provide less care than cohabiting partners. Karlsson, Johansson, Gerdner, and Borell (2007) found that very few LAT partners would end their relationship because of their partner’s ill health, but most of them envisage providing a relatively limited amount of care to their partner. Benson and Coleman (2016) interpreted the outcomes of their study among 25 older LAT partners as follows: they were not averse to providing some level of care to their partners should their partner’s health status require it, but they were cautious about making indefinite “for better or for worse” promises like the ones espoused in marriage. Forgoing marriage or cohabitation to avoid these obligations was strong. (p. 803)
Based on qualitative research among 25 LAT partners, De Jong Gierveld (2015) showed that dedicated care behavior is noted in all LAT partners who have been confronted with illness of the partner. Nevertheless, many LAT partners who accepted care felt uneasy about having done so. (Europe, Netherlands: De Jong Gierveld, 2015; Canada: Kobayashi, Funk, & Khan, 2017; Australia: Upton-Davis, 2015; United States: Lewin, 2017). Yet being cautious or uneasy about exchanging personal care may not be typical for LAT partners only, whereas it is clear the living arrangements of LAT partners, characterized by absence of continuous coresidence (Koren, 2015) and by geographical distance, offer less optimal opportunities for exchanging care (Benson & Coleman, 2016; Karlsson & Espvall, 2016). We therefore expect that LAT partners may receive less daily personal care than in the other types of relationships (Hypothesis 1b).
General Drivers of Support and Care: Explanatory Factors
The above argued that the saliency of the LAT relationship and the lack of continuous coresidence may explain why LAT partners receive more emotional support and less personal care compared with other partner relationship types. Yet there are other general drivers of emotional support and personal care that may in part explain differences in support and care among types of partner relationships. We distinguish between (a) the need for care, (b) the relational quality, and (c) the social context in which the couple is embedded and the help received from others.
First, the need for care is an important driver for the receipt of care and generally indicated by the physical and mental condition of the care recipient (Andersen & Newman, 2005; Broese van Groenou & de Boer, 2016). In the case of physical health problems, both emotional support and personal care may be needed to deal with growing disabilities to enable the performance of activities of daily living. In all types of partner relationships and under the assumption that the partner is willing and able to provide care, we can expect that poor health increases emotional support and personal care received from the partner. Differences in physical health between LAT and the other types of partner relationships may thus in part explain the differences in emotional support and personal care received (Hypothesis 2a). Yet the qualitative studies presented above suggested that in LAT relationships both the commitment and opportunity to receive personal care are rather limited. Also, physical health impairment limits the possibilities for social participation and leisure activities which may put a strain on the LAT relationship and increase the risk for dissolving the relationship (Lewin, 2017). This suggests that the associations between physical health on the one hand and emotional support and personal care on the other hand are weaker among LAT relationships compared with the other types of relationships (Hypothesis 2b).
Second, the quality of the bond between the partners is also an important driver of the receipt of support and care. In particular, the strong emotional bond is an important motivator for partner care (Broese van Groenou et al., 2013). There is also evidence that marital quality and the receipt of spousal support are positively interrelated (Acitelli, 1996) and that lower marital quality may lead to lower marital support, but also vice versa. This study only takes the perspective of the recipient into account as it lacks data on the partner’s motivation to provide support and care. Yet when the care recipient is less committed to the relationship or reports a lower relationship quality, he or she may be less likely to ask for support and care or may perceive a lower receipt of support and care compared with care recipients that are more committed to and happier in the relationship. This is assumed to be the case in all types of relationships. Therefore, differences in commitment to the relationship and relationship quality between LAT and other types of partner relationships may explain differences in the receipt of emotional support and daily personal care (Hypothesis 3).
Third, the partner relationship is part of a wider social context and the receipt of support and care from a partner may be associated with the emotional support and care that others are providing. Receiving less emotional support from the social network, for whatever reason, may be compensated and therefore positively associated with emotional support from the partner, and the other way around. For LAT partners, the relationship with their own social network may be somewhat disturbed as their partner is often not yet perceived to be part of the new family network (De Jong Gierveld, 2015). If consequently, LAT partners receive less emotional support from their network compared with other types of partner relationships, they may receive more emotional support from their partner to deal with these disadvantages (Hypothesis 4a). The availability of network members—both kin and nonkin—and professional caregivers who will assist in the caregiving are considered as positively impacting on the possibilities of de facto caregiving and receiving (Broese van Groenou & de Boer, 2016; Koren & Lipman-Schiby, 2014). Yet LAT partners do not share a household and need to rely more on others from outside the household for help. In general, single older care recipients are more likely to receive formal and informal care than coresiding older adults (Jacobs, Aartsen, Deeg, & Broese van Groenou, 2018). LAT partners may receive more care particularly from their adult children, as they greatly value filial responsibilities (De Jong Gierveld, 2015). It is expected that LAT partners less often receive personal daily care from their partners, as they more often receive care from professional caregivers and their social network (Hypothesis 4b).
Controls
In the analyses, we will also control for background variables such as gender, age, socioeconomic status, and marital history (divorce or widowhood) as these vary systematically among the types of partner relationships. LAT relationships more often evolve after widowhood in later life, whereas remarriage occurs after divorce earlier in the life course (De Graaf & Kalmijn, 2003), so that LAT partners tend to be older than those in other types of partner relationships (De Jong Gierveld, 2004; Lewin, 2017). They are also more often found among the higher educated, as this group values financial independence more than the lower educated (De Jong Gierveld, 2004). Among partnered older adults, men are more likely to be (re)married or cohabiting than women, because older women are more reluctant to embark on new partnership types with a high risk of traditional duties and obligations (Karlsson & Espvall, 2016). Older widows, in particular, may conclude that remarriage requires too great a sacrifice and hesitate to take on the traditional obligations associated with (re)marriage (Lewin, 2017); they are therefore more inclined than men to start a LAT relationship (De Jong Gierveld, 2004).
Method
Respondents
Data for this study were drawn from the Family and Fertility Survey by Statistics Netherlands. Interviews with a selected sample of men and women aged between 18 and 79 years, drawn from the Dutch Population Registers, took place in 2013. Of the 16,500 selected persons, 10,255 participated, a response rate of 57%. To arrive at the analytical sample, all persons aged 50 to 79 years were selected (N = 5,123). We excluded 1,012 persons who were not in a relationship and 3 persons whose relationship status was missing, leaving a sample of 4,108 respondents aged 50 years and older with a spouse or intimate partner for the current study. The age of 50 years is relatively low for a study of later-life partner relationships, but selecting a higher age would have reduced the number of LAT relationships considerably. Content relevant to the current study included information on respondents’ partner type status and partner history, living arrangements, socioeconomic indicators, health, quality of the spouse/partner relationship, size and composition of the personal network of relationships with kin and nonkin, as well as information about exchanging several types of support and care. Given the importance of knowledge of the partner status and history, we first differentiate between older adults in first marriage (n = 3,227; 78.6%), remarried men and women (n = 420; 10.2%), older adults in unmarried cohabitation (n = 291; 7.1%), and older adults in an LAT relationship (n = 170; 4.1%). Table 1 presents the sample characteristics of the 4,108 respondents, differentiated according to the four partner status categories.
Sample Characteristics of Respondents Aged 50 to 79 Years, by Type of Partner Relationship (N = 4,108).
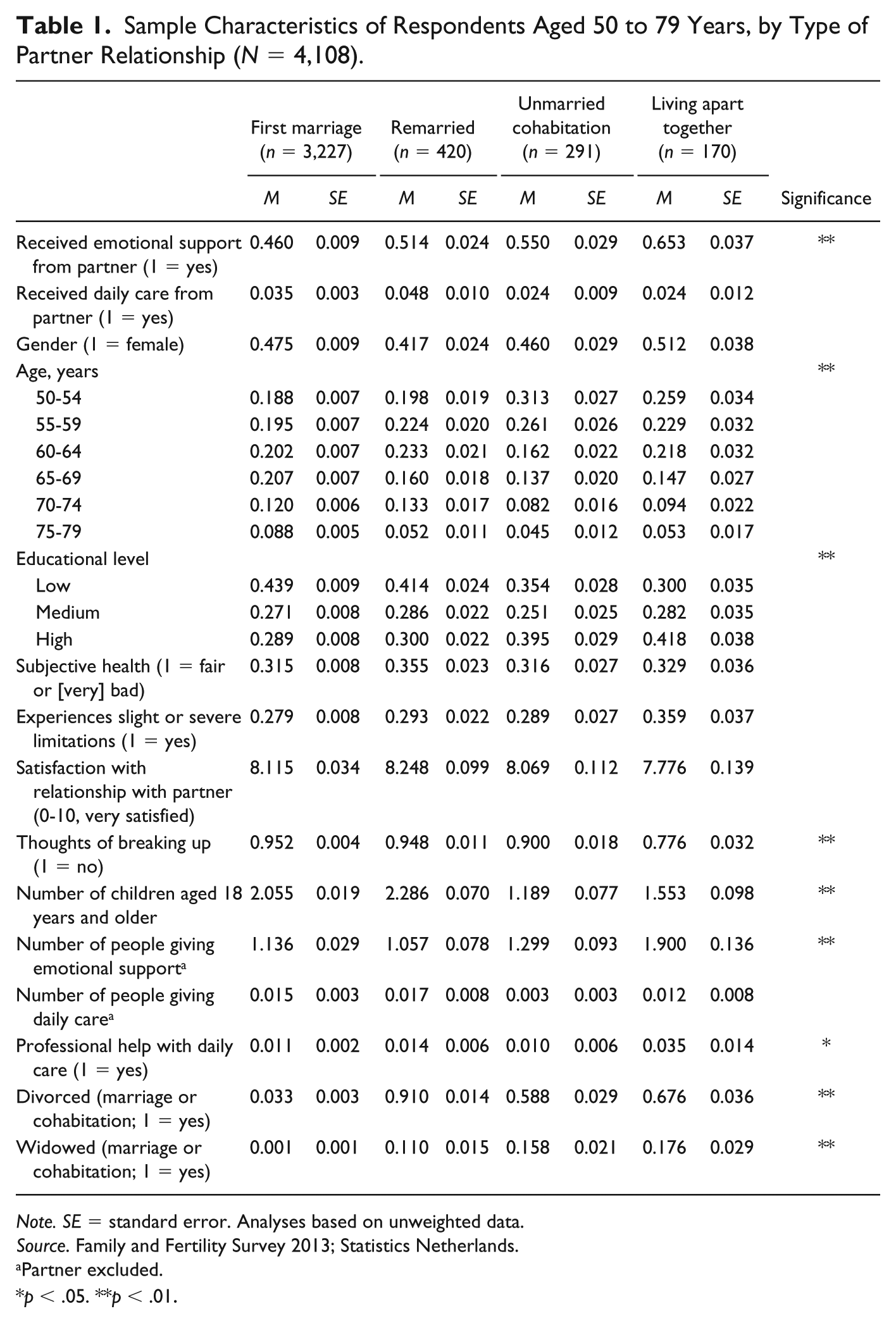
Note. SE = standard error. Analyses based on unweighted data.
Source. Family and Fertility Survey 2013; Statistics Netherlands.
Partner excluded.
p < .05. **p < .01.
Measurement Instruments
Dependent Variables
All respondents were asked whether they had received emotional support or personal care. The questions were formulated as follows: (a) From time to time people talk to others about things that are important to them. It could be about things that went well or badly, dilemmas or other important concerns or emotions that someone has. During the past 12 months, have you talked to others about your personal concerns? and (b) During the past 12 months, have you received nonprofessional daily care, such as help with getting dressed, washing, eating, getting in and out of bed, or going to the toilet? If respondents mentioned receiving emotional support or daily care from one of the members of their informal social network, additional questions were asked about the relationships between recipient and provider. Categories encompassed partner, children, siblings, other family, neighbors, colleagues, and friends. We used the support and daily care received from the partner as the two dependent variables (0, 1).
Health was measured via a direct question on subjective health, (very) good = 0, fair or (very) poor = 1, and a question about disabilities (no disability and disability with no limitations = 0, disability, mild, or severe limitations = 1).
The quality of the spouse/partner relationship was measured using the following question “Could you indicate how satisfied or unsatisfied you are with the relationship with your partner?” on an 11-point scale ranging from 0 (not satisfied at all) to 10 (very satisfied). For commitment to the relationship, we used a one-item recording of whether the respondent had “thoughts about breaking off the relationship,” a dichotomous variable (no = 0, yes = 1).
The Social Network Surrounding Intimate Partners
As an indicator of family size, the number of children aged 18 years and older was used as a continuous variable. The support network was defined as all unique persons mentioned as giving support to the respondent. The number of people (excluding the partner, but including adult children and grandchildren) giving emotional support and the number of people providing daily care were used as continuous variables. Use of formal care was identified by asking whether the respondent had received personal care from a professional on a regular basis during the preceding 12 months (no = 0, yes = 1).
Controls
Sex was used as a dichotomous variable (male = 0, female = 1), while age was differentiated into categories at 5-year intervals. Educational level was measured as a categorical variable; in this study we used three categories (low = 0, middle = 1, and high = 2) with low corresponding to ISCED 0-2, middle to ISCED 3-4,and high to ISCED 5-8. In 4% of the cases, respondents indicated to have received some other type of education. They were classified as lower educated. Ever having been divorced and ever having been widowed were dichotomous variables (never divorced = 0, ever divorced = 1; never widowed = 0 and ever widowed = 1). Separations and widowing of cohabiting couples were also taken into account.
Statistical Analysis
Means of all variables were estimated and analyzed using F tests, comparing the four types of partner relationships (Table 1). Additionally multivariate logistic regression models were used to examine the contribution of the variables to variation in receiving support and care, for the two measures of support and care receiving; see Tables 2 and 3. The model variables were arranged in four models: control variables, health-related variables, quality of the partner relationship, and contextual or social network characteristics. Partner history (ever having been divorced/widowed) was not included in the multivariate regression models as this feature did not apply to those in their first marriage. Interaction effects between the two health variables and type of relationship were explored for both dependent variables (Hypothesis 2b).
Logistic Regression for Receiving Emotional Support From Partner, Adults Aged 50 to 79 Years (N = 4,108).
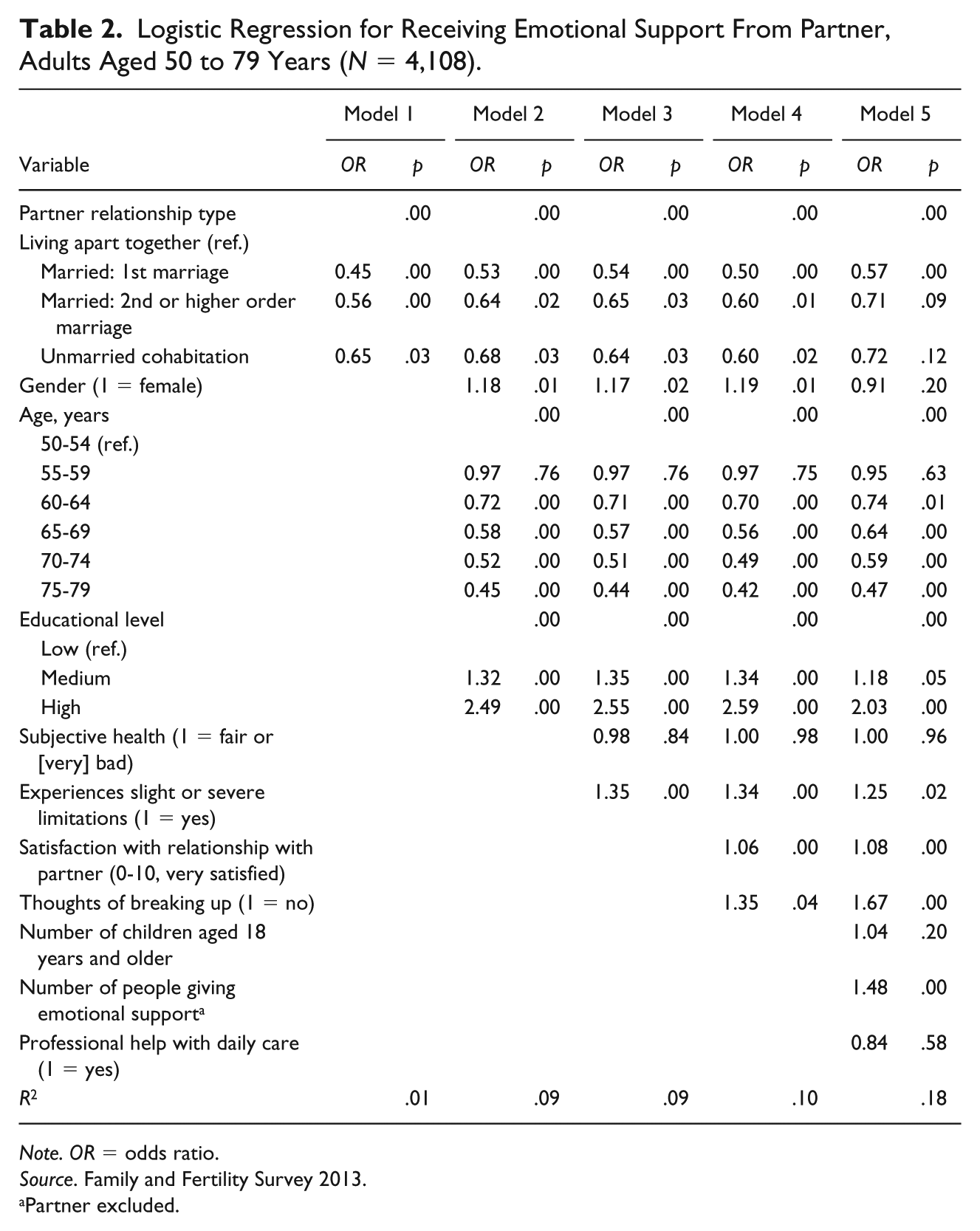
Note. OR = odds ratio.
Source. Family and Fertility Survey 2013.
Partner excluded.
Logistic Rregression for Receiving Daily Personal Care From Partner, Adults Aged 50 to 79 Years (N = 4,108).
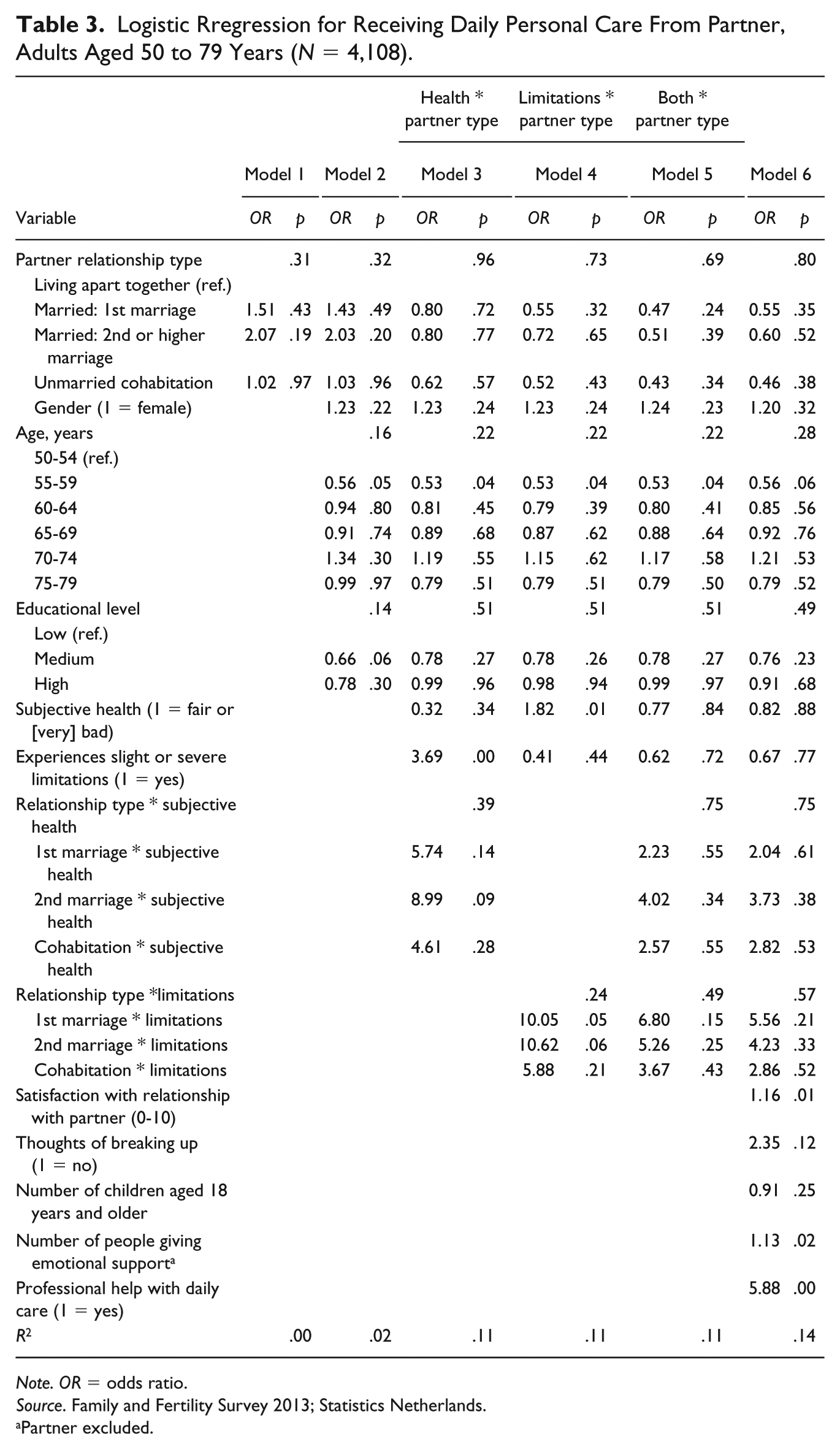
Note. OR = odds ratio.
Source. Family and Fertility Survey 2013; Statistics Netherlands.
Partner excluded.
Results
Partner Relationship Types
Table 1 showed that out of the 4,108 respondents aged 50 to 79 years, the majority were involved in first marriage (78.6%), 10.2% were remarried, and 7.1% were cohabiting partners. The LAT partners elicited in this survey comprised 4.1% of the respondents.
Receiving emotional support from the partner differed significantly across the four groups: 65.3% of the LAT-partners received emotional support from their partners, compared with 46% of married respondents, 51.4% of remarried respondents, and 55% of the cohabiting respondents.
Daily personal care, by contrast, is one of the types of support and care that is less commonly received, primarily because many respondents in the Netherlands in the 50 to 79 years age group are able to live independently in their own homes. Only 2.4% of the LAT partners received daily personal care, compared with 3.5% of the married respondents, 4.8% of the remarried partners, and 2.4% of the cohabitants. Differences are not statistically significant.
As regards the control variables, the partner relationship type proved to be significantly associated with age (the percentage of married and remarried partners is highest in the oldest age categories), with educational level (the percentage of married and remarried partners is highest in the lower education levels), with ever having been widowed (highest among LAT partners), and with ever having been divorced or separated (highest among remarried partners). No differences were found with regard to gender.
As regards the other factors, partner relationship type was associated with commitment (with thoughts of breaking off the relationship highest among LAT partners), with mean number of children aged 18 years and older (lowest mean numbers among the LAT partners and highest among married and remarried older adults), and with size of the emotional support network and receipt of formal care (highest mean numbers among the LAT relationship type). No significant associations were found between partner relationship types and subjective health, experienced disabilities/limitations, and satisfaction with the partner relationship.
Receiving Emotional Support
The findings of the multivariate logistic regression analyses are presented in Table 2.
Table 2 shows in Model 1 that, without taking other factors into account, older adults in LAT relationships had significantly higher odds of receiving emotional support from their partners than older adults in first marriages, in second or higher order marriages, and in unmarried cohabitation (supporting Hypothesis 1a). After taking into account differences in sex and age composition and in educational level (Model 2), all differences compared with the LAT partners reduced somewhat but remained statistically significant. The explained variance increased, from .01 in Model 1 to .09 in Model 2.
In Model 3 (Table 2) two health indicators were added. This hardly affected the odds for receiving emotional support in the different types of partner relationships, showing, partly contrary to Hypothesis 2a, that subjective health and experiencing limitations are not major drivers of emotional support differences in partner relationship types. The findings do indicate that disability, but not subjective health, directly increases the odds for receiving emotional support, regardless of relationship type. We also checked for interaction effects of health indicators and type of relationship, but they appeared to be not significant (not shown), and Hypothesis 2b was rejected. Explained variance in Model 3 remained at .09.
In Model 4, the quality of the partner bond was introduced; this increased the odds for receiving emotional support somewhat in all three relationship types compared with the LAT type. Taking into account the lower satisfaction in LAT relationships and higher prevalence of thoughts of breaking off the relationship, thus makes the differences between LAT and the other relationship types a little more apparent. Relationship quality acts more as a suppressor of differences than as a mediator, which contradicts Hypothesis 3. It can be concluded that, in all types of relationships, being satisfied with the relationship and having no thoughts of breaking it off increases the odds for receiving emotional support. Explained variance increased in Model 4 from .09 to .10.
Finally, in Model 5, the social network factors were introduced. The size of the network providing emotional support, in particular, reduces the odds for receiving emotional support to a nonsignificant level for remarried and cohabiting partners, but the odds remain significant for partners in a first marriage. This suggests that the higher emotional support received from others (kin and nonkin) in LAT relationships is associated with receiving more emotional support from their partner compared with remarried and cohabiting older adults, which is contrary to Hypothesis 4a. Having children aged older than 18 years and the number of persons providing daily care did not increase the odds for receiving emotional support from the partner. Explained variance increased in Model 5 from .10 to .18. It can be concluded that LAT partners have higher odds of receiving emotional support compared with the other three relationship types, and that relationship quality and network support are important drivers of these differences.
Receiving Daily Personal Care
The findings regarding daily personal care receiving are presented in Table 3. Model 1 showed that, without taking control variables into account, older adults in LAT relationships do not differ significantly from those in first, second, or higher order marriages or in unmarried cohabitation relationships as regards receiving day-to-day care from their partner. Also, adding the control variables, and indicators for health, relationship quality, and the contextual factors did not change the significance of the odds (not shown). It can be concluded that, both unadjusted and adjusted for other factors, there is no difference in daily care received from the partner between LAT and the other types of relationships (rejecting Hypothesis 1b).
Given the importance of health for daily care, we added interaction effects of health and type of relationship to the full model for the two health indicators separately (Models 3 and 4 in Table 3) and together (Model 5). The results in Model 4 showed relatively large odds for physical limitations. Compared with those in LAT relationships, older adults in first marriages and remarriages are about 10 to 11 times as likely to receive daily care from their partner when they experience health limitations (odds ratio = 10.1, p = .05 for married partners; odds ratio = 10.6, p = .06 for remarried partners). This difference is illustrated in Figure 1: a higher proportion of those with physical limitations received daily care compared with those without physical limitations, in particular among married and remarried couples, but this difference is reversed among LAT partnerships, supporting Hypothesis 2b. When interaction effects of both health indicators are added together (Model 5), the odds are no longer statistically significant, probably due to a lack of power as few people receive daily care and the LAT sample is rather small.
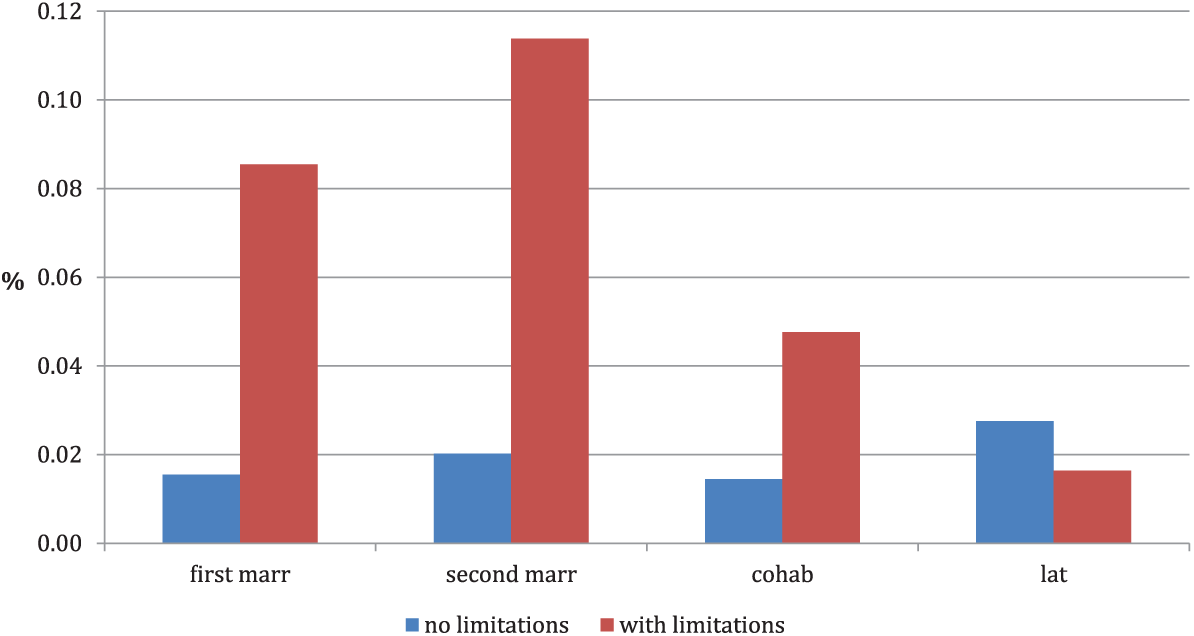
Proportion of older adults receiving daily care, by type of partner relationship and functional limitations.
The full model (Model 6) shows that relationship satisfaction, the number of people giving emotional support, and in particular the assistance from professional helpers, all increase the odds for receiving daily care from the partner, regardless of the type of relationship. Explained variance was 0.14 in Model 6.
Discussion
This study provided an insight into associates of support and partner care in LAT relationships versus other types of partner relationships in later life. The findings contribute to three conclusions: (a) the type of partner bond of older adults is important and related to significant differences in the probability of exchanging emotional support in later life. Partners in LAT relationships experienced higher emotional support than partners in first marriages, remarriages, and cohabitation, and these differences were only partly explained by relational and social factors. (b) There are no significant differences regarding the receipt of personal care between LAT and the other three types of partner relationships, yet the results hint at the possibility that physical limitations trigger daily care among (re)married couples but not in LAT relationships. (c) Health problems, the level of satisfaction with the partner bond, and a diversified support network are the most significant triggers of support and care received from older intimate partners, regardless of the type of partner relationship.
An important finding is that the type of partner bond with the lowest level of structural commitment, namely the LAT relationship, is the partner bond characterized by the highest level of exchanging emotional support. This outcome contrasts with the findings of Lewin (2017) that people in LAT relationships receive less support from their partner compared with (re)married and cohabiting partners. Differences in measurement may be a factor here; our study asked, “if you discuss personal concerns, with whom do you do that?” as an indicator for receiving emotional support from the spouse, whereas support measure used by Lewin included two questions about “opening up to a partner about worries” and “reliance on help in case of a problem,” which may have combined emotional and instrumental support. Still it remains unclear why a large majority of partners in the U.S.-based study report partner support (e.g., 90% of married partners report partner support and 84% of LAT partners), while in our study a lower share reported partner’s emotional support (e.g., 45% of married and 65% of LAT partners); however, this may be due to measurement differences.
Our findings are more in line with other recent studies on LAT relationships (Connidis et al., 2017; Karlsson & Espvall, 2016; Lyssens-Danneboom & Mortelmans, 2015), who state that the emotional content of the LAT relationship is the most important for these older couples. If true, this implies that in the event of falling relationship quality, people would opt out of a LAT relationship more easily than in other types of partner relationship. This self-selection effect would leave LAT partners happier and more supportive than in any other type or relationship. However, our study shows the proportion of people who were dissatisfied with the relationship and/or had considered breaking off the relationship to be higher in LAT partnerships than in the other types of relationships, suggesting that some do stay in a LAT relationship even when relationship quality is not all they would wish. This illustrates the diversity among the LAT relationships and, more empirical evidence on a larger scale is needed on this group. In particular, more information regarding relationship expectations and commitment, for example, in terms of level of intimacy, contact frequency, daily discussions, and disagreements, may shed more light on differences regarding relationship quality and support between LAT relationships and other types of partnership.
As regards personal care, no differences between the four relationships types were found, as all types reported a very low level of care use. This, and also the small number of LAT relationships in our study, explains the lack of statistical power of the interaction with health indicators. However, the results do provide a detailed insight into the contributions of the relationship quality and the support network to our understanding of the probability that daily personal care will be exchanged. In particular, support from formal care sources increased the odds of receiving partner care, showing the complementarity between partner care and other helpers (Jacobs et al., 2018). Table 1 shows that people in LAT relationships in particular use formal home care, probably because these couples do not share a household and LAT partners may not live in close proximity. The findings also suggest that partners in LAT relationships may have limited sources of informal care as they have fewer children aged older than 18 years than those in the other relationship types. They do have the largest emotional support network, but this may consist more of nonkin and age peers, who are less likely to provide daily care when needed. Further research with a longitudinal design could shed light on how kin and nonkin relationships of LAT partners develop into informal caregivers and how formal care plays into this.
We included gender as a control variable, but the data show that gender is not a distinguishing factor in types of relationships (Table 1). We did find that women were more likely to receive emotional support than men, regardless of the type of partner relationship. This gender difference only attenuated when the support network was also taken into account in Model 5 (Table 2). Given that women are more in favor of LAT relationships than men (Karlsson & Espvall, 2016), this calls for gender-stratified analyses to examine whether women receive more emotional support in LAT relationships than men. Given that women are more often caregivers than men, but suffer from higher caregiver burden than men (Swinkels, van Tilburg, Verbakel, & Broese van Groenou, 2017), this also calls for more insight into gender differences in caregiving within LAT relationships in later life. The question is whether these gender differences double the risk for caregiver burden in LAT relationships, in which women want to remain independent but the need for partner care makes it difficult to remain so.
Limitations of the study include the low level of partner care. The lack of differential effects of partner types on the use of personal care is probably due to the small number of older persons actually receiving day-to-day personal care. Studying this specific type of partner support in a sample of higher ages might have shown more variation, but then the number of LAT partners would have been very low. Research into characteristics of LAT relationships in older age has to date mostly relied on qualitative research among a relatively small number of men and women, with a few exceptions such as De Jong Gierveld (2004) and Lewin (2017). This study used a large-scale survey data set including 170 older persons involved in LAT relationships, in addition to 291 persons in unmarried cohabitation, 420 remarried older adults and 3,227 adults in first marriage. Another limitation concerns the lack of information regarding the partner, in particular the capacity and commitment to provide care. Lewin (2017) showed that the partner’s health was positively associated with partner support. More partner information would have allowed dyadic comparisons, which are important in explaining spousal health and well-being (Korporaal, Broese van Groenou, & van Tilburg, 2008). One strength of the data set is the diverse set of relevant variables regarding the quality of the partner relationship and the social embeddedness of older adults in personal networks, which together offered a fairly unique opportunity to answer the research questions as formulated. Repeating this survey and study in 10 years’ time might indicate a higher percentage of older adults in LAT relationships, because these relationships are on the rise. Panel research, allowing a more exhaustive explanation of causes and consequences of LAT relationship characteristics in relation to the provision of support and care has to be welcomed. For the time being, this study has provided reliable evidence about the differences and similarities between types of partner relationships and emotional support and care behavior.
Finally, this study sheds more light on the (lack of) difference between traditional and new types of partner relationships among older adults. Relationship quality and a large support network are important for all couples dealing with health problems at a specific point in time. Our findings imply that, apart from investing in the relationship, the development of a large and diversified social network is beneficial for all types of partner relationships before entering later life. Further research is needed on how support and care affect well-being in traditional and new types of relationships, and what part gender plays in this.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.