
Abstract
In this paper we ask how interpersonal connectivity can be achieved at a geographic distance. This is in contrast with extant literature that focuses on states of connectivity rather than the work needed to achieve it. We draw on phenomenological ideas of embodiment, presence and distance, in combination with empirical material from an extreme remote work context – telenursing in Australia. The nurses we interviewed triage patients entirely by telephone. We argue that even with low social and technical connectivity, interpersonal connectivity is achievable through skilful work with technology. We explore the work that goes into ‘being there with and for distant others’ by combining the phenomenological concepts of ‘maximal grip’ and ‘intentional arc’ with empirical examples. We propose that interpersonal connectivity is oriented empathetically towards both the other person and agentically towards the joint situation. We thereby develop a conceptual model of interpersonal connectivity work, which argues that distributed workers need to skilfully balance the dualities of freedom/control and nearness/farness to achieve interpersonal connectivity. Achieving and maintaining interpersonal connectivity is an important skill, particularly for leaders who operate in work contexts that are increasingly distributed, flexible and temporary.
Keywords
Introduction
Most organizations today depend on distributed work. Particularly during the Covid-19 pandemic, employees dial in to meetings from home and collaborate while sitting at opposite ends of the globe (Aroles, Mitev, & de Vaujany, 2019; Fried & Hansson, 2013). Such distributed working is possible because of connectivity – both technical and social. Achieving balanced connectivity, known as ‘requisite connectivity’ (Kolb, Collins, & Lind, 2008) is an ongoing challenge. It is particularly difficult yet important for leaders of remote workers to stay connected with employees who are geographically distant and distributed (Fried & Hansson, 2013; Kiesler & Cummings, 2002; Kolb, Prussia, & Francoeur, 2009). Until managers of remote workers learn to lead those who are ‘out of sight’ (Hinds & Bailey, 2003), the many benefits associated with remote work are unlikely to be realized (Baruch, 2000). While the search for the right amount and right kind of connectivity is vital to ensuring that work can be performed effectively in the context of new organizational forms, it is not yet clear how this connectivity is achieved, nor what kind of skill is involved.
We have learned much already about states of connectivity (Kolb, Caza, & Collins, 2012), and how these states are regulated by knowledge workers who adapt their devices and routines to stay in the loop without getting overwhelmed (Dery, Kolb, & MacCormick, 2014; MacCormick, Dery, & Kolb, 2012; Oostervink, Agterberg, & Huysman, 2016). But we don’t yet know what exactly it takes to ‘build a connection’ with someone who is geographically far away. In this paper we therefore investigate the question: what is involved in achieving interpersonal connectivity between two geographically distant people, where interpersonal connectivity is ‘the person-to-person contact we make with others’ (Kolb, 2008, p. 184)?
The paper utilizes a brief empirical case of telenursing to motivate and illustrate theory development (Alvesson & Kärreman, 2007; Alvesson & Sköldberg, 2017). We are inspired to explore the skill of interpersonal connectivity by speaking with a group of workers who we identify as being experts in building interpersonal connectivity at speed at a distance: telenurses who help strangers with medical complaints entirely over the phone. The lean communication medium in this case provides us with an opportunity to study the skill involved in interpersonal connectivity work without the additional influence of more advanced technology features.
We notice that the telenurses are able to connect with others who are geographically far away swiftly and effectively, without prior social interaction. Recognizing this ability leads us to investigate interpersonal connectivity conceptually, by delving into holistic nursing literature and related work by existential phenomenologists, in particular Marcel, Merleau-Ponty and Dreyfus. From this exploration and aided by reflection on selected empirical material, we derive a conceptual model of what we term interpersonal connectivity work.
With this conceptual model we put forward the proposition that interpersonal connectivity work relies on embodied skill. Specifically, we elicit two dimensions from combining conceptual and empirical material that we argue are important for achieving interpersonal connectivity with geographically distant others: becoming present and situated with someone who is geographically far away (the empathetic dimension), and assuming control of the situation in order to be there for the other (the agentic dimension). In both dimensions, requisite distance has to be skilfully found and enacted. Establishing and maintaining interpersonal connectivity efficiently and effectively at a distance is a skill that we suggest will be in demand in coming years, and so deserves both further research and management attention.
Connectivity Literature: From State to Skill
Prior research on connectivity has differentiated types, states and amounts of connectivity, and has investigated the task of managing these states towards an optimum point (requisite connectivity and connective flow) (Kolb, 2008; Kolb et al., 2008, 2009, 2012; Leonardi, Treem, & Jackson, 2010; Wajcman & Rose, 2011). In this section we offer an overview of types of connectivity, the ‘amounts’ of connectivity that are associated with different states, and how the issue of agency has been framed in the literature. We then home in on one particular type, interpersonal connectivity, and consider what it is made up of. This sets up an opportunity to reflect on the underexplored question of how interpersonal connectivity is achieved.
States of connectivity as a matter of degrees
The concept of ‘connectivity’ initially referred to a technical property of networked internet protocols. Such technologies made instant communication possible across the globe and were much revered, even promising the ‘death of distance’ (Cairncross, 1997; for a critical response see Olson & Olson, 2000). Connectivity later also became a metaphor for the social connection that these technologies make possible between people, groups, and organizations (Dery et al., 2014; Kolb, 2008; Kolb et al., 2008).
Social and technical connectivity are in this new formulation related but distinct: we may ‘technically’ have the capacity to connect with distant others (e.g. telephone numbers of academics are often available online), but we may not have the social connectivity that is required to actually make a connection (e.g. if we do not know a person, it is unlikely we would call them). The opposite situation (social connectivity without technical connectivity) also results in a deficiency. Sufficient social and technical connectivity are therefore needed for information and communication technologies to afford connectivity across geographic distances.
The ‘degree’ of social and technical connectivity that is needed in teamwork and organizational settings has been the focus of much recent research. Kolb et al. (2008, p. 187), for instance, ask: ‘First, is more always better? Second, how much is enough? And, finally, is a balanced state of connective flow possible in a highly connected world?’ To address these questions, Kolb et al. (2012) define different states of connectivity: hypo-connectivity (too little); hyper-connectivity (too much); requisite connectivity (just enough). These concepts primarily relate to degrees of connectivity. Building on this work, Dery et al. (2014) introduce the notion of ‘connective flow’, which reflects the finding that knowledge workers play an active role in managing their own connectivity. The authors found that, like turning a tap to adjust the intensity of water flow, workers use their communication devices to balance connectivity, according to their needs throughout the day (Dery et al., 2014).
Leonardi et al. (2010) also argue that workers have some control over connectivity. Remote workers were found to use technology strategically to create both a sense of closeness and to reassert some sense of distance from geographically dispersed peers (Leonardi et al., 2010). Workers have a degree of agency in negotiating, managing and resisting the sense or pressure of ‘constant connectivity’ (Wajcman & Rose, 2011) that can arise through what Mazmanian, Orlikowski and Yates (2013) have termed ‘escalating engagement’. Kolb et al. (2012) further point out that even in the face of social pressure to be ‘constantly connected’ (Mazmanian et al., 2013; Wajcman & Rose, 2011), ‘disconnects’, whether technical or social, intentional or unintentional, remain a feature of working life.
In the connectivity literature so far, agency primarily plays a role in how workers regulate their degree of connectivity and thereby the state of connectivity in their organizational context. This is relevant for scholarship that is concerned with navigating the new landscape of digitally enabled work and organizing, because this literature examines tensions between individual agency versus collective pressure when it comes to digital communication (Leonardi et al., 2010; Mazmanian et al., 2013), also relevant to debates around ‘work life balance’ (MacCormick et al., 2012; Wajcman, Bittman, & Brown, 2008). Typical questions in extant connectivity studies are then: How much connectivity is too much? How much is enough? How can the ‘right amount’ be achieved and maintained? What pressures get in the way of achieving the ideal state of requisite connectivity?
While these questions are important and much can still be learned by asking them, we take an alternative approach by considering two more fundamental questions. We ask: how can we conceptualize interpersonal connectivity, and how is interpersonal connectivity achieved at a distance when using technology?
Interpersonal connectivity
Interpersonal connectivity is a sub-category of social connectivity. It is defined as ‘the person-to-person contact we make with others’ (Kolb, 2008, p. 184). Interpersonal connectivity may have a strong connotation of face-to-face interaction that takes place in a non-mediated, technology-free environment; however, Kolb (2008, p. 184) points out that technology has supported interpersonal connectivity for millennia, ‘since writing first appeared around 5,000 years ago’ (see also King & Frost, 2002; Kolb, 2013). Now that ICTs proliferate, it is normal to engage in technologically supported interpersonal connectivity, even though ‘achieving intimacy and community through computer-mediated communication seems counter-intuitive to many at first’ (Kolb, 2008, p. 184).
The recent democratization of communication technologies has made it possible, and then in turn necessary, to stay interpersonally connected with geographically distant others. For example, families are now often spread out across the world, perhaps even because of the possibility to remain interpersonally connected via phone, SMS, video conferencing, emails, etc. (see also Sennett, 1998). A similar pattern is seen in the ongoing shift towards distributed and remote work, where technology enables effective work practices but in turn also makes organizations more dependent on technologies that keep their workforce connected (Cristea & Leonardi, 2019; Fried & Hansson, 2013).
Interpersonal connectivity can be considered a valuable guard against negative impacts of distributed organizing (e.g. loneliness, isolation, problems in coordinating effectively), but at the same time cannot be considered a feature of particular technologies, nor is it easily implemented through standardized practices. In fact, achieving interpersonal connectivity is considered challenging. Cultural misunderstandings can for example lead to disconnects that need to be ‘repaired’, which is in turn more difficult if the range of communication channels available is limited (Kolb et al., 2008). Although interpersonal connectivity is possible in a digitally connected world, it remains ‘vulnerable to connective gaps’ on both social and technical dimensions (Kolb, 2008, p. 184).
What remains under-explored is how one can establish interpersonal connectivity at a geographic distance. In particular, it remains unclear how those in a somewhat asymmetrical relationship, for example those in a position of responsibility to others, such as leaders of remote workers, ‘can develop a sense of closeness with others, whether they be down the hall or around the world’ (Kolb et al., 2009, p. 342). We therefore first consider what exactly interpersonal connectivity might be ‘made of’ in order to then theorize the effortful work that goes into achieving it.
How is interpersonal connectivity achieved?
In this paper we are interested in what interpersonal connectivity is made of and how it is achieved at a geographic distance. We theorize the skilful work that goes into this achievement.
Recent literature has highlighted the need to study work as it is the ‘micro-foundation’ of organizations and organizing (Barley & Kunda, 2001; Lawrence, Suddaby, & Leca, 2011; Orlikowski & Scott, 2016). Our focus on work also falls within a sociotechnical, practice perspective on organizing, which holds that reality is an active achievement involving human and non-human actors, rather than a pre-given fact (Latour, 2005; Leonardi, 2011; Orlikowski, 2010; Orlikowski & Scott, 2008; Riemer & Johnston, 2017). Aligned with this perspective, we consider both the social and technical aspects of the work that makes interpersonal connectivity possible between people who are not physically collocated, as well as the often-overlooked role of the body in working effectively with technology (Sergeeva, Faraj, & Huysman, 2020).
In prior research, Symon and Pritchard (2015) looked at processes of connectivity and argue that connectivity depends on a performance of sociomaterial agency. The authors focus on the effects of connectivity and how these effects are produced and used as a resource by employees. They consider how workers enact their presence and their employee identities through mobile technologies (Symon & Pritchard, 2015). In this paper, instead of looking at the effects of interpersonal connectivity, we consider the sociotechnical ‘work’ that goes into achieving interpersonal connectivity at a distance, particularly when there is a dependency– responsibility relation. In sum, the gap we address is the need to look beyond states towards the skilful work that goes into achieving interpersonal connectivity.
In the following, we first outline our research approach. We introduce an illustrative case of telenursing, and explain how the case prompted us to engage with existential phenomenology to develop theory on ‘interpersonal connectivity work’, which we argue can enrich connectivity research with new phenomena, questions and implications for practice. We later draw connections between this new conceptual material and case details to theorize a type of skilful work that we argue is needed for connecting with others ‘in a world where far is the new close and close is the new far’ (Kolb, 2013, p. 188).
Research Approach and Case Material
We first outline our abductive research approach. We then give a background of an illustrative case of an extreme remote working context – telenursing in Australia – that has prompted us to develop theory on what we call ‘interpersonal connectivity work’.
Abductive research
Our research follows an abductive logic: ‘Empirical material’ is thus seen as a critical ‘dialogue partner’ (Alvesson & Kärreman, 2007) in the process of critical reflection. This approach does not try to conceal the constructed nature of knowledge, and the researcher is recognized as having an active role in the way in which they place empirical and theoretical material in critical dialogue (Alvesson & Sköldberg, 2007). Rigor is pursued in abductive research through a reflexive process wherein both theoretical and empirical material are held accountable to one another, while relevance is defined by whether insights are formed that are of interest to the wider research and practitioner community (Alvesson & Sköldberg, 2007).
Accordingly, we are here inspired to investigate interpersonal connectivity by insights from interviewing telenurses who, surprisingly, were able to connect with patients over the phone instantly and skilfully. While empirical material provides the impetus for the study, it is further used to inform and illustrate the theory development, which itself is based on existential phenomenology as the main lens. True to our abductive yet theory-led approach, we bring in empirical material as it becomes relevant, to reflect on and illustrate key concepts. This iterative approach helps us to develop a conceptual model of interpersonal connectivity work.
The research that resulted in the empirical material used in this paper was conducted over a period of eight months and comprises 13 interviews (10 with telenurses and three with managers of telenurses). All of the nurses interviewed are women. The research also involved repeated interactions with our main managerial contact, including a feedback session where the research findings were shared and discussed. Furthermore, the lead researcher made two site visits to the HealthOrg (a pseudonym) head office in a major city in Australia. The lead researcher was given a demonstration of the software system and listened in on a recorded, de-identified call. All except one interview with nurses were conducted over the phone. 1 The conversations were recorded, transcribed and compiled for manual coding.
We proceeded iteratively with our analysis, discussing the interview material and how connectivity was, according to the nurses’ descriptions, being achieved with their callers, for whom they were for a brief time responsible. In this way we went back and forth between theory and our transcriptions, noting where and how what the nurses reported gave us insight on how they built a connection with callers, in a way that illuminated theoretical ideas.
While we draw on phenomenology, we acknowledge that our empirical material does not stem from a phenomenological methodology. Further, we neither derive theory from the data, nor do we intend this material to serve as definitive proof of our theorizing (Alvesson & Kärreman, 2007; Alvesson & Sköldberg, 2017). Rather, empirical material is used reflexively, for the purposes of illustration and reflection, to assist in theory development.
The HealthOrg case
HealthOrg is a pseudonym for a large Australian health services organization, which is contracted by the Australian government to provide a telenursing service to the general public. Registered nurses with two or more years of clinical experience are employed to work from their homes. They answer calls from the public, who describe their own or their dependents’ medical issues verbally. The nurse uses a computer system and her phone equipment while guiding the patient 2 through a triage process over the phone. At the conclusion of the call the patient is advised on the appropriate action to take: stay at home, see a doctor, or go to hospital.
The government funds this contracted service in order to reduce visits to the emergency ward and thereby reduce emergency room waiting times, an important government indicator of the Australian public health sector’s performance. The nurses triage callers by drawing on their clinical training, with the assistance of a Decision Support System (DSS). A call is referred to as an ‘encounter’. At the conclusion of the encounter, a ‘disposition’ is reached with the DSS, which advises patients to either monitor their medical situation, see a doctor, or attend an emergency department. In some encounters the nurse will override the disposition reached by the DSS (an action that their managers can later ask them to defend). The nurse can also arrange an ambulance or refer the patient to other services.
The primary focus of the nurses’ work is on triaging patients over the phone. Calls are allocated via a central system and a nurse will see basic details of the call they are about to take, such as where the person is calling from. The nurse then needs to juggle getting basic contact details from the caller with making a quick initial assessment of what kind of situation is at hand – is this an emergency, or is there time to discuss the patient’s condition? Once an initial clinical assessment is made, the nurse will open the relevant ‘guidelines’ on their computer system and will follow a series of questions prompted by the DSS. Though some patients expect it, the nurses are not permitted to diagnose the medical condition. The aim of the call is to quickly and safely triage the patient with the help of an approved scripted decision tree.
Empirical observation as prompt for theorizing
When interviewing the nurses and their leaders (who also had nursing experience, because this was deemed vital to being able to lead nurses), we were at first interested in learning about their remote work practices – what the role of a telenurse involves and how the nurses cope with working from home. But surprisingly, we found that the physical distance between nurse and patient was mostly not a problem, as the nurses were in most instances satisfied with the way in which they could handle patients’ issues over the phone. Several in fact reported that physical distance was part of what attracted them to the job, having been physically assaulted at some stage in their clinical nursing careers. Some had injuries or disabilities (examples were back injuries and PTSD associated with nursing work). Others had caring responsibilities that were incompatible with the varied rosters of standard hospital shifts. For these workers, sitting down in a comfortable and safe home environment was highly desirable and in some cases the only way in which they could continue to practise nursing.
What struck us about this case was that these nurses were able to connect with geographically distant callers on a personal level under highly challenging conditions. They had never met the caller, were under time pressure (from their management and because of the potential urgency of the case) and were using low-bandwidth technology (audio only). Although a host of software and hardware supports the call (e.g. switchboard, DSS, microphone headsets worn by the nurses), the call itself is voice only and conducted over the phone.
According to connectivity theory, the nurses have a very low degree of social connectivity with their patients. They have no prior contact with the people who call them, and if the caller does not volunteer (truthful) information about themselves, they also cannot be contacted again. This is a challenging basis from which to build a personal connection. From a technical perspective too, the case features very low technical connectivity. We therefore deemed their apparent capacity to be there ‘with and for’ geographically distant strangers under challenging circumstances noteworthy, which prompted our exploration of how interpersonal connectivity under these conditions can be achieved at a distance, particularly when some degree of responsibility needs to be taken for the distant other. We operate under the premise that reflecting on theoretical material using this special case for reflection can illuminate the phenomenon of interpersonal connectivity work in distributed contexts more broadly.
In the following section we outline the conceptual grounds from which we proceed to theorize ‘interpersonal connectivity work’: we outline key concepts from existential phenomenology. Afterwards we show how the telenursing case allows us to reflect upon and extend these concepts. This reflexive, abductive process leads us eventually to propose a model of interpersonal connectivity work.
Theory Lens: Phenomenology and Embodiment
We turn to existential phenomenology because of its sensitivity to issues of presence and skill, both concepts that we deem important to understanding the skilful work that goes into achieving interpersonal connectivity.
Interpersonal connectivity is defined as ‘the person-to-person contact we make with others’ (Kolb, 2008, p. 184). It is not however clear what the unique nature of such contact is, nor what goes into achieving it. Symon and Pritchard (2015, p. 256) link connectivity conceptually to ideas of ‘being known and knowable – having presence in the organization’s life’. As we are interested specifically in interpersonal connectivity, we zoom in on this idea of ‘presence’ and what it means to be present with another at a geographic distance.
We find rich literature on the concept of presence in existential phenomenology. Several scholars in this tradition have given significant thought to the experience of being present with another, and have reflected on why one can feel close to someone who is geographically distant, and in turn far away from someone who is physically proximate (see Wilson, Boyer O’Leary, Metiu, & Jett, 2008, for another perspective on this phenomenon).
In the following section we outline how existentialist philosophers, specifically Marcel (1965), and holistic nursing scholars, make sense of what it means to become present with another person. We find that presence is skilful, yet it cannot be taught. While this insight could represent somewhat of a conceptual impasse, we find a way forward in a phenomenological analysis of ‘skill’, which ultimately prompts us to pay attention to the important role of embodiment and negotiation of phenomenal distance in the work of becoming present with a geographically distant other. We later explore the concepts introduced here by drawing on illustrative case material, then use the insights gained from putting conceptual and empirical material in dialogue to put forward a model of interpersonal connectivity work.
Presence
The notion of presence is relevant to understanding interpersonal connectivity, because both concepts are concerned with ‘the person-to-person contact we make with others’ (Kolb, 2008, p. 184). Presence has been explored in a rich way in existential phenomenology and in holistic nursing literature, which builds on the phenomenological tradition. In holistic nursing, presence is equated with ‘being-there-for and being-there-with’ the patient, in a way that is healing and transformative for both nurse and patient (Kleiman, 2009, p. 6). We adopt this notion and investigate its origins further.
Importantly, we first learn from existential phenomenology that presence does not imply a mere physical co-existence. In particular, Marcel (1965, pp. 204–5) dismisses the idea that physical proximity equates to presence:
We could say that the man sitting beside us was in the same room as ourselves, but that he was not really present there, that his presence did not make itself felt. But what do I mean by presence, here? It is not that we could not communicate with this man. . .[yet] between ourselves and him a kind of physical, but merely physical, communication is possible. . .One might say that what we have with this person, who is in the room, but somehow not really present to us, is communication without communion: unreal communication, in a word. He understands what I say to him, but he does not understand me: I may even have the extremely disagreeable feeling that my own words, as he repeats them to me, as he reflects them back at me, have become unrecognizable.
We take from this that interpersonal connectivity is achieved when the other feels close, no matter how geographically distant they are. On the other hand, when someone does not feel understood, it fails. In such situations, one is left alienated and distant not only from the other but also from oneself.
Existential phenomenology’s take on space and distance is useful for considering these points further. While objective distance is often understood based on a model of Cartesian space, as a measurable expanse between two coordinates, what is near is in existential philosophy understood subjectively in terms of what is being attended to, that is, what matters to a particular person. This subjective experience of distance is sometimes called phenomenal distance. An important insight here is that concern for another is more important than geographic location, and relatedly that a key requirement for achieving interpersonal connectivity is skilful ‘involvement’, defined as ‘the ability to see and respond to the other’ (Benner, 2000, p. 14).
Marcel (1965) insists that this ability to be present with another cannot be explicitly taught nor codified. While it is possible to teach the behaviours associated with presence it is not the same as learning the skill of presence itself:
. . .it would be quite chimerical to hope to instruct somebody in the art of making his presence felt: the most one could do would be to suggest that he drew attention to himself by making funny faces. . .teaching people to make their presence felt, is the very height of absurdity.
Although presence is skilful, it cannot itself be taught because to turn it into a set of procedures would negate the importance of uniquely attending to the other. This is why presence is considered an important care intervention in nursing but nursing scholars and professionals resist the idea that it can be codified and taught (Doane, 2003; Nelms, 1996).
This insight places us at an apparent conceptual impasse when trying to understand the skilful work that goes into being there with and for distant others. However, we find a way forward by turning to Merleau-Ponty (2012/1962) as interpreted in the model of non-representational skill acquisition developed by Dreyfus (2002) and Dreyfus and Dreyfus (2005). 3 We focus in particular on two concepts that Dreyfus, building on Merleau-Ponty, argues are essential to the acquisition of practical skill: the intentional arc and maximal grip. 4 We outline how skill in this framework is based in embodied experience, is temporally framed, and depends on active involvement and the negotiation of phenomenal distance.
Intentional arc: involvement draws on past embodied experience
The intentional arc is the temporal framework of involvement (Dreyfus, 2002; Merleau-Ponty, 2012/1962). It describes how our past and future surrounds us and plays a role in how we directly perceive and cope with the world in the course of everyday action (Chan, 2005). Merleau-Ponty posits that it is because of past embodied experiences, and the anticipated future, that we are able to effectively perceive and become situated in the world in everyday life: ‘This intentional arc creates the unity of the senses, the unity of the senses with intelligence, and the unity of sensitivity and motricity’ (Merleau-Ponty, 2012/1962, p. 137). Our experiences, as interpretations of reality, build up over time and become our pre-understanding by which new situations appear to us and inform how we orient ourselves to get a better grip on them.
Here a ‘situation’ is not a context in the Cartesian sense, of being a container in which an encounter takes place, rather a situation is brought about through involvement with it. Further, these prior experiences are not ‘stored’ as mental representations, rather they are with us in the form of ‘dispositions to respond to the solicitations of situations in the world’ (Dreyfus, 2002, p. 386). The process by which we perceive the world is therefore not dependent on representations or conscious work, it is already given to us in what matters to us according to our embodied histories and anticipated futures (Dreyfus, 2002).
We take from the concept of the intentional arc the following: becoming present with another requires becoming situated with them. And to get oriented within a situation requires being ‘involved’ with the other made possible through past embodied experience. Such experience is drawn upon when dealing with another in order to seek out common ground and understanding. In other words, becoming present with another in a situation requires skilful work that is learned over time.
It is then additionally important to become involved in a way that is appropriate to the situation at hand. This is particularly the case when a degree of responsibility needs to be taken for the other, within the frame of interpersonal connectivity. Here we continue to draw on Dreyfus’ interpretations of Merleau-Ponty (2012/1962) and in particular his concept of ‘maximal grip’. Where the intentional arc describes the temporal dimension of the skill required to become situated in the present, maximal grip describes how one can bring the situation ‘into focus’ so that action can be directed in an appropriate way, at the right phenomenal distance.
Maximal grip: negotiating distance during involvement
According to Merleau-Ponty (2012/1962) and as elaborated by Dreyfus (2002), a generic component of skilful activity is the embodied negotiation of phenomenal distance in order to achieve ‘maximal grip’. At the point of maximal grip one reaches the appropriate distance from which something – an object, a situation, a problem – comes into focus and is ‘grasped’ appropriately, where ‘at a shorter or greater distance we have merely a perception blurred through excess or deficiency’ (Merleau-Ponty, 2012/1962, p. 302). Working to ‘grasp’ something here means that we are involved in finding the ‘optimum distance from which it requires to be seen’ (Merleau-Ponty, 2012/1962, p. 302). Maximal grip therefore describes the ‘body’s tendency to respond to [temporal] solicitations in such a way as to bring the current situation closer to the agent’s sense of optimal gestalt’ (Dreyfus, 2002, p. 386).
A skilled practitioner will be good at finding maximal grip, by adjusting how they are oriented to a situation in response to tensions, which are experienced in an embodied way:
According to Merleau-Ponty, finite, involved, embodied coping beings are constantly ‘motivated’ to move so as to achieve the best possible grip on the world. . .acting is experienced as a steady flow of skilful activity in response to one’s sense of the situation. Part of that experience is a sense of whether or not coping is going well. When one senses a deviation from the optimal body-environment gestalt, one’s activity tends to take one closer to an optimal body-environment relationship that relieves the ‘tension.’ As Merleau-Ponty puts it, ‘our body is not an object for an “I think”, it is a grouping of lived-through meanings that moves towards its equilibrium’. (Dreyfus, 2005, p. 137)
The tendency to find maximal grip describes a person’s skill in holding unfolding action at an appropriate distance. It requires an ongoing process of balancing distance in seeking focus.
Merleau Ponty’s (2012/1962) metaphor of a traditional microscope is a useful analogy for thinking about maximal grip and also how technology plays a role in this skilful process, as equipment, rather than focal ‘tool’ (Riemer & Johnston, 2017). A student investigating a cell is not focused on the microscope – she just adjusts wheels back and forth, alternating between fine and coarse adjustments, eye pressed to the machine. The student could not see the cell without the microscope, but it is not the microscope that causes the cell to appear. Rather, the embodied skill she has developed over time in dealing with and adjusting the microscope to the ‘right’ distance means it can be equipment for magnification and focusing. Her involvement and past experience in the practice of studying cells as well as the functioning technology are equally important for making it possible for the student to see the cell, but it is her embodied and active tendency towards the ‘maximum of visibility’ (Merleau-Ponty, 2012/1962, p. 302 316) that brings the cell into focus.
The intentional arc and maximal grip are linked through an emphasis on the role of embodiment in skilled involvement: ‘the intentional arc is enriched and refined through the body’s tendency towards maximum grip’ (Chan, 2005, p. 26). We take from this ‘conceptual toolkit’ a phenomenological understanding of presence: presence first requires skilful involvement based on past embodied experience and concern, and second an ongoing active balancing of phenomenal distance to grasp the object of concern appropriately. We now develop these insights further, through reflection on the telenursing case.
Illustration with Case Material: Dimensions of Interpersonal Connectivity Work
In the following we illustrate how the intentional arc and maximal grip manifest in action and further consider how these ideas help us to theorize interpersonal connectivity work. We first show with examples from the telenursing case how becoming present with distant others is skilful work that draws on past embodied experience. In doing so we reveal that such presence is directed towards both the patient and towards their situation and the matter at hand. The nurse has to become both a caring presence in an empathetic sense with the other and take control of the situation in an agentic sense for the other. We then demonstrate that both dimensions require assuming a requisite distance as conceptualized by the notion of maximal grip, to avoid being too close or too far from either the person or the situation.
The intentional arc in action: becoming present with distant others
Becoming present with a geographically distant other is skilful work that draws on past experience. For example, in order to help their clients within an efficient timeframe, the nurses reported working hard to get a good sense of the other person, in order to ‘see’ the ‘full clinical picture’. To overcome the limitations of low technical connectivity, nurses reported drawing heavily on past experiences of working in emergency rooms to help them listen and question carefully, in order to quickly ‘visualize’ what they were encountering, before engaging the DSS.
This activity of ‘visualizing’ provides an example of how nurses skilfully draw on past experience in an embodied way to quickly become present with the caller:
. . .you’ve got to visualize straight away, is this an old person who’s struggling who can’t even talk to me or is it a younger person who’s generally in good health but this is a short-term problem? So every question you ask you’ve got to be visualizing what might be happening. You draw on your own experience as you’re always visualizing in your own head. I’ve seen this before. This sounds like. This feels like. Then with it – with that thinking, you then go into one of the algorithms and start going through a process of set questions. But in that initial assessment you’ve got to be visualizing what could be happening. That is vital. You’re thinking on your feet.
In orienting herself in the encounter, a nurse would not assess the patient based purely on their symptoms in a scripted sense as guided by the DSS, but rather would be drawing on embodied experience and bodily senses to perceive the patient and their situation directly as some form of deviation from a situation she previously encountered.
We further illustrate the important role of embodiment and past experience in the following example. One nurse described an encounter with a patient who had been in a farming accident. She immediately perceived the sounds of a farm on the basis of her own backgrounded understanding. This enabled her to place herself into the caller’s situation, in that she anticipated the existence of a utility vehicle (a ‘Ute’) that could act as a wind buffer to improve the quality of the call. As a consequence she was able to take control of the situation and direct the caller to shelter from the wind:
You can hear that it’s really windy when someone talks to you on a mobile – so I go, ‘can you get down low beside the Ute just so you can stop the wind?’ They’ll go ‘yeah no worries. . .’ They’ve got a broken ankle but they’ll still do it for you. ‘That’s better, now we can talk okay, so I’ll get the ambulance out to you.’ They go ‘right-o’. I say ‘whereabouts are you on the property?’ Then they tell you and you get a better idea. I’m lucky in that way that I have that diversity of background. . .we lived on a little property for a while so I know what it’s like to be down in the back paddock with the animals when something happens.
Even though she is geographically distant, the nurse is describing how she becomes present with the patient, by relating what she is hearing to her prior experiences and using this embodied understanding. This skill is emphasized repeatedly in the nurse’s descriptions of translating the DSS’s prompts to make them relevant to the caller, so as not to offend the caller with redundant questions.
Importantly, the nurse’s involvement is directed both towards the caller, in the sense of being there with the patient, and towards the situation at hand in the sense of being there for the patient in that she is able to take action to resolve the situation. In the following we draw on this distinction as an additional dimension for understanding skilful interpersonal connectivity work: such connectivity is oriented empathetically towards both the other person and agentically towards the joint situation.
Maximal grip in action: assuming requisite distance
A key part of this work involved translating a balance of ‘close’ and ‘far’ that is second nature in a hospital environment – getting a closer look, standing one’s ground, using the body to signal both intimacy and separation – into a process of listening, questioning and asserting. As much as the nurses described working to bring about a familiar closeness with their patients, for example by working to ‘visualize’ the patient and using everyday objects as reference points for size and colour, they were also involved in balancing this intimacy and sense of nearness with a sense of separation and farness. We associate this effort to achieve the ‘right’ distance from their callers and the matter at hand with the concept of maximal grip.
In a hospital context, balancing intimacy and separation in order to find the ‘requisite’ social distance from patients has been carefully institutionalized. In hospitals, a nurse touches bodies in a way that is not appropriate in ordinary settings. The nurse’s uniform and other mechanisms like a rotating roster help to create the social distance necessary for both patient and nurse to cope with such intimacy. Achieving this balance was reportedly more difficult over the phone. Nurses wanted to establish intimacy in order to care for their patients, but also needed a sense of separation to avoid questions about their own lives, to help the caller, and keep the call on track (especially under time pressure).
To do this, the nurses described cultivating their ‘phone voice’. This ‘phone voice’, together with the headset that is worn during calls, became the distributed equivalent of a nurse’s uniform:
When you’re in a uniform [in a hospital] and you’ve got your name and your designation and you’re in that environment – it is a buffer between who you are and what job you’re doing – what you need to do. . ..I do, definitely, have a phone voice that I use. So I think that is another separation. . .the same as if you are nursing someone in hospital. You don’t just, like, stand there with your shoulders hunched and say, ‘oh. . .’ – while they’re just talking at you. . .You kind of need to assert your presence and look interested and really be available. . .
This quote highlights the careful balancing act that goes on, in balancing intimacy and separation, nearness and farness, in order to ‘really be available’ and become present with the other in a way that both enacts and preserves the nurse’s professional identity. In a distributed context, this balancing of distance requires constant adjustment and the development of new skills, such as cultivating a ‘phone voice’ and enrolling technologies such as the headset, to re-imagine the techniques that have long been established in co-located settings (e.g. not standing too close nor too far away, not shaking a hand too tightly or too loosely, being engaged but not aggressive, etc).
Similarly, the nurse also has to assume a requisite distance to the matter at hand. For example, one nurse told us that having a photograph of a rash would be useless, because it is impossible to understand its proportions without context. She preferred to ask questions that related the size and colour of the rash to everyday objects that both parties would be familiar with (‘is it about the size of a ten cent coin?’). This provides an illustration of how the nurse works to achieve an appropriate distance from which the rash ‘comes into focus’ and is fully ‘visible’ to the nurse, even at a geographic distance. Bringing the patient’s medical problem into focus so that the nurse can intervene appropriately again requires embodied, effortful work.
Empathetic and agentic dimensions of interpersonal connectivity
Together, the concepts of intentional arc and maximal grip help us to see the role of skill and experience, as well as the importance of balancing intimacy and separation in the flow of distributed action. Moreover, highlighted throughout the above examples is the important role of the body and embodied experience in becoming present with and for geographically distant others. This is an important insight, as it may be tempting to see such distributed ‘virtual’ interactions as somehow ‘disembodied’.
The nurses’ background understanding, when skilfully drawn upon, represents the intentional arc: it provided a bridge between the nurse and patients’ physical contexts and made it possible for the nurse to empathize and connect with the caller in order to be present with them. Maximal grip helps us to make sense of the way that nurses constantly balance intimacy and separation to achieve the requisite distance from the caller and matter at hand.
To conclude this section, we elicit two dimensions from our combining of conceptual and empirical material that we argue are important for achieving interpersonal connectivity with geographically distant others. First, we contend that part of interpersonal connectivity work is to become present and situated with someone who is geographically far away. We will refer to this as the empathetic dimension of interpersonal connectivity, the ability to assume a shared situation with the other. Second, to coordinate action and be there for the other, the person initiating interpersonal connectivity needs to assert themselves and, if needed, assume control of the situation in order to help resolve a matter at hand. We term this the agentic dimension of interpersonal connectivity work. In both dimensions requisite distance has to be skilfully found and enacted. In the following we utilize these insights to present a model that conceptualizes interpersonal connectivity work.
A Conceptual Model of Interpersonal Connectivity Work
In this section we introduce our conceptual model of interpersonal connectivity work, visualized in Figure 1 and further illustrated in Table 1. We conceptualize interpersonal connectivity work as the balancing of two dualities of distance: nearness/farness in becoming present ‘with’ the other in an empathetic sense, and freedom/control in becoming present ‘for’ the other in an agentic sense. While analytically separable, the model posits that these dualities are fundamentally linked in practice and require ongoing balancing, which requires embodied, skilful work.
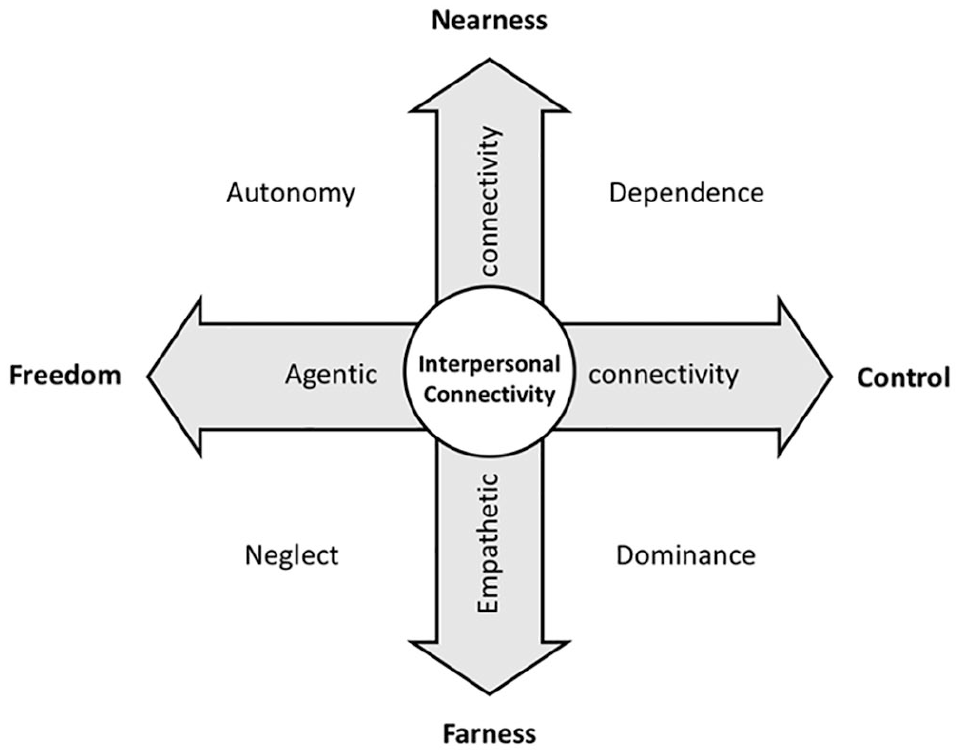
A Model of Interpersonal Connectivity Work.
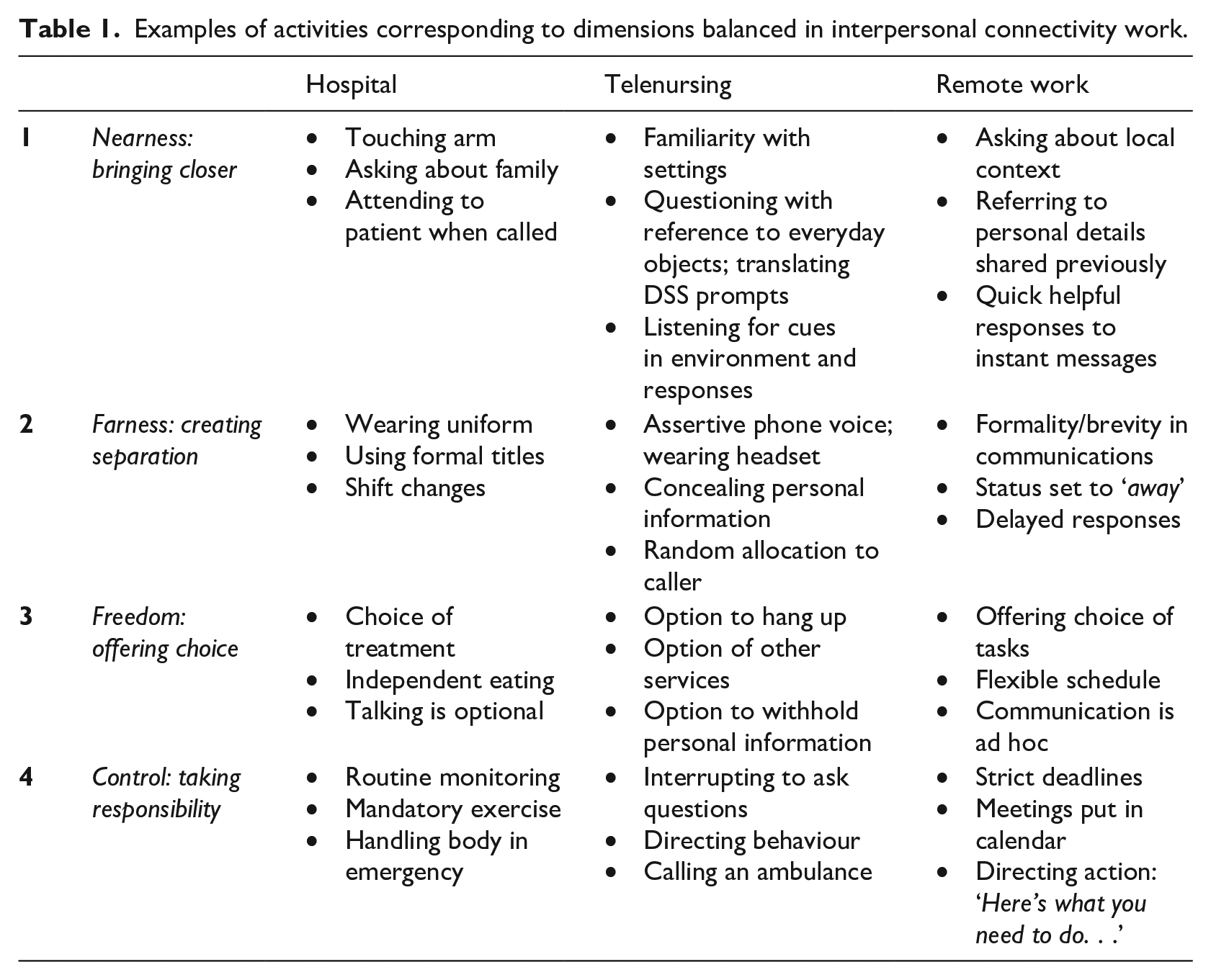
Examples of activities corresponding to dimensions balanced in interpersonal connectivity work.
In Figure 1, the cross-hairs denote a point of balance at which requisite interpersonal connectivity is achieved. By ‘point of balance’, we mean an ongoing correction that is akin to the movements that need to be made in order to stand on a physiotherapy ‘balancing board’ (a disc with half a ball attached to the centre, on which one stands and balances to increase core and joint strength). It takes effort and skill to remain stationary in the desired ‘centre’ when standing on such a board, because there are always pulls and pushes to contend with that take one off course – staying balanced requires ongoing work. With this metaphor in mind, we now introduce interpersonal connectivity work as a skilful balancing along the two dimensions.
With this model we further propose that interpersonal connectedness does not stand in a straightforward binary relationship to disconnectedness. Rather, it is possible to enact different modes of interpersonal connectivity. The ideal or requisite mode of interpersonal connectivity is depicted at the centre of the two dualities where balance is achieved (however temporarily). We depict divergent modes as showing up in the relational experiences of autonomy, dependence, domination and neglect. The divergent quadrants show the modes of interpersonal connectivity that are enacted when balance is not maintained. We do not intend to imply that these quadrants are ‘bad’ in any normative sense but rather that they are shades of what may be experienced in the inevitable and necessary adjustments involved in the course of interpersonal connectivity work.
To further explain our model, we offer illustrative examples of activities that could align with each point of the axes in Table 1. We include a column for a hospital setting, a telenursing setting, and a remote work setting, to demonstrate how we see these dimensions translating from one context to another. Table 1 illustrates potential components of interpersonal connectivity work across different contexts. It is also possible to explore the divergent quadrants, or modes of interpersonal connectivity, using the rows of the table. For example, neglect is exemplified by considering rows 2 and 3 in isolation, because the activities that create separation (farness) and offer choice (freedom) are performed without the balancing actions illustrated in the remaining rows. This lack of balance pulls the mode of interpersonal connectivity into one of neglect. The same is true for considering autonomy, as rows 1 and 3; dependence as rows 1 and 4, and domination as rows 2 and 4. This illustration is possible because we have argued that interpersonal connectivity work involves a balancing act of dualities, so that when the dualities are out of balance, the result tends towards more extreme modes. It is therefore the negotiation of these dualities that exemplifies the skill of interpersonal connectivity work.
We now explain the divergent quadrants in more detail, using illustrative examples from the nursing case, with speculative connections to a broader remote work leadership context. We later build on this link to remote work leadership in the implications section.
Autonomy: being there with, but not for the other
Where nearness is established in an encounter between two people, for example through listening attentively and using common frames of reference, and where interactions offer significant freedom of choice, interpersonal connectivity tends towards a mode of autonomy, where presence is experienced in a relatively passive way. In the nursing case, this would mean the caller is counselled but largely left to cope with their situation without the guidance of the nurse. For example, a nurse describes leaving certain callers to make their own decision about what care they receive:
‘Or if you really want to go to the emergency and you don’t want to stay on the phone with me, then go now.’ So I’ll give them the option, as opposed to, I guess, really trying to talk to this hysterical person. Because some people actually just do need to go to the emergency department, because they can’t calm down.
The caller here may feel empowered and perhaps comforted, but also frustrated, because they are left without expert attention and need to make decisions about their care themselves.
In a remote work leadership context, this could mean that a manager is in touch with their direct report, for example checking in on personal matters via instant messaging, but does not give much direction or feedback on tasks and assignments, which might result in feelings of insecurity and at worst confusion.
Dependence: being there with and for the other (too much)
Where only nearness is enacted and control is exerted, interpersonal connectivity tends towards dependence. In this scenario there is an intimacy between the two parties and one party is dependent on the other for direction. This involves a sense of excessive presence combined with constraint and control that may be overwhelming.
To illustrate, here a nurse reflects on her conduct when she started telenursing. In trying to do everything for her patient, she would offer up more information than was actually helpful:
[I used to get] defensive [about my long call times]. ‘I’m just giving a good service to my client.’ Now I just think, no you weren’t, you were just talking too much. There is such a thing as over servicing because patients do not take in that much. If you give them too much information, they’ll only take away 10 per cent of it.
In this mode, a caller might feel that they are being talked down to and patronized, treated like a child, and with little sense of how they might cope without the nurse. Self-disclosure efforts would be entirely guided by the nurse’s questioning.
In a remote work leadership context, a manager in this mode would be constantly checking in on their direct report using various communication technologies. Tasks would be micro-managed, for example via always-on collaboration tools. The remote worker has little freedom to express a desire to try new assignments and has little say in guiding discussion during mentoring calls.
Domination: being there for, but not with the other
Where a detachment is exerted but control is maintained, interpersonal connectivity appears in the form of dominance. This is a regulatory influence that may be felt as an acute, oppressive yet detached presence. One party keeps the other at arm’s length without much empathizing, and yet they exert a defining influence on the other’s activities. A mild example is illustrated here, where the nurse describes her practice of interrupting callers in order to get the information she needs:
. . .I do interrupt people now. I do definitely get what they call ‘call control’. So I just keep interrupting and saying, ‘I need to stop you there, now’ – by using a clear, I guess, direct voice.
In more extreme examples, dominance may come about if a nurse pressures the caller in order to get the call finished as quickly as possible to satisfy her quotas. The patient feels brusquely dealt with and does not have room to ask questions or express themselves fully. The patient may feel bullied or ill-treated.
In a remote work leadership context, this mode of interpersonal connectivity would be marked by orders ‘from up high’. For example, meetings are put into the worker’s diary without consultation. The worker is pulled from one assignment to another without explanation or input. Even though the manager is a defining force in the remote employee’s experience of work, there is not a sense that they are well understood or appreciated. The relationship is perceived as instrumental. 5
Neglect: neither being there with nor for the other (deficient)
When one party is involved with another but maintains a strong sense of detachment while the other is also given complete freedom, interpersonal connectivity is experienced as a kind of absence understood as neglect. In taking no responsibility for the other while enacting detachment, this form of interpersonal connectivity is experienced as intense disconnection.
This quadrant presents as a form of disconnect because it stands against an involvement – one party is important to another but is not there with them in an empathetic sense, nor there for them in an agentic sense. In the nursing case this can for example manifest as disengaging from a difficult call until ‘someone hangs up’:
You still will get your average idiot who wants to be rude. You’re just like ‘mate I don’t need to help you. I’ll give you one more warning. I don’t need to help you.’ Then they either hang up or you hang up or someone hangs up.
Essentially this translates into a kind of non-performance, as consistently remaining in this quadrant, showing disinterest towards the caller and not asking them questions, would likely eventually result in the nurse’s dismissal.
In a remote work context, a manager tipping into the neglect mode of interpersonal connectivity would be similarly aloof. They are technically assigned as leader of a particular worker, but are rarely accessible via email, phone, or other media and don’t respond to requests to connect. This kind of disconnect is felt acutely because the manager is formally connected to the worker but fails to be there with or for the worker in any way.
Summary
Our conceptual model frames interpersonal connectivity as something that needs to be constantly worked at, not by simply completing a set of actions or tasks or by using a particular technology, but rather through drawing on past experience and balancing phenomenal distance in how one relates to a situation and another person. We have illustrated four different modes of interpersonal connectivity that are balanced in the course of interpersonal connectivity work.
We draw particular attention to the important role of embodiment in performing interpersonal connectivity work with technology at a geographic distance. Technology here is the ‘equipment’ (Riemer & Johnston, 2017) with which and through which interpersonal connectivity is maintained and negotiated. The degree to which this is successful in comparison with co-located engagements depends, we argue, largely on how skilfully interpersonal connectivity work is enacted – it is therefore in this model not practical to explain which technologies will create connectivity, rather the model is meant to assist in the exploration of how practitioners perform the balancing act of interpersonal connectivity work with and through the technologies that have become part of their shared practice (Sandberg, Langley, & Tsoukas, 2017), no matter how lean or rich a particular communication technology is.
Implications and Conclusion
In the following we consider how interpersonal connectivity work may apply in a broader remote work context. Although our case material comes from telenursing, we have used this material to investigate a more fundamental phenomenon, which we argue these nurses are experts in. Accordingly, we propose that our insights and model are of relevance to other distributed work contexts. The extent to which the model holds in these contexts requires further research. We now discuss what value further investigations could bring and thereby open up avenues for future inquiry that can further enrich our understanding of interpersonal connectivity and the work that goes into achieving it.
Applicability beyond the nursing context
The theorizing in this paper is informed by existential phenomenology and empirical research conducted in a specific context. Rather than skew or restrict the contribution of the theorizing, the empirical material has proven to be fertile ground from which to consider how interpersonal connectivity is achieved by a particularly skilled cohort in an extreme context where there is a lot at stake. We contend that traditional nurses are experts in becoming present with their patients and appropriately guiding action (Doona, Haggerty, & Chase, 1997), and that it therefore is useful to look at how they are translating these skills into a distributed work environment.
We first recognize that the theorizing in this paper and the resultant model may be particularly relevant to future research on telenursing. In particular, we join conversations that seek to investigate how technology plays a role in care, even though these two constructs have traditionally been placed in opposition to one another: technology as cold and inhuman, care as warm and human (Mol, 2008). Here we have illustrated how distributed interpersonal connectivity relies on technology but also on embodied, effortful work.
Second, we propose that the skill of achieving interpersonal connectivity at a geographic distance is one that is exercised in, and increasingly important to, a range of work contexts. We recognize that the context we studied relies on lean media in a particular context; however, we suggest that our model and the theory development put forward in this paper could be applicable in other contexts where there is a relationship of care and responsibility between one party and another. Specifically, we here relate our theorizing to the context of leadership in remote work, because this is an important avenue of future enquiry for connectivity research (Kolb et al., 2009), and because achieving interpersonal connectivity at a distance is an increasingly important skillset for managers, particularly in times of the COVID-19 pandemic.
Implications for practice
It is necessary for leaders of remote workers to develop new skills to ensure they can achieve interpersonal connectivity in relation to those they are tasked with leading, even at a geographic distance (Kolb et al., 2009). As a feeling of alienation and disconnection can be distressing for remote workers (Hafermalz, 2020) managers may be advised to invest in reflective practice regarding their balancing of the dualities of freedom/control and nearness/farness in relation to each individual they manage remotely.
Our model could for example be used to create connectivity ‘journeys’, as a tool for coaching and development conversations. For example, both worker and manager could mark on the model where they feel they are in relation to one another at set intervals over a period of time, for example twice a day for a week. In joining these marks over time a journey line is created that shows how the worker has experienced interpersonal connectivity in relation to the manager over time, which can be compared with how the manager feels they have been there with and for the worker over the same period.
Producing such graphics could prompt conversation about how interpersonal connectivity work is experienced and to what extent balance is achieved over time. In its potential for facilitating reflective conversations about such interpersonal connectivity work, this model makes a potential contribution to worker and management relationship development and remote work coaching initiatives that can enhance the empathetic and agentic dimensions of the skill needed to become present with and for distant others. The technique also addresses a limitation of this study, which has focused on the person enacting interpersonal connectivity (the telenurses, or remote work leaders) and does not capture the experience of those ‘on the other side’ (patients, or remote workers).
Implications for research
Finally, we draw several important links to the extant connectivity literature and suggest directions for future research. First, we return to the concept of connective gaps, which occur due to social and technical disconnects (Kolb, 2008; Kolb et al., 2008). Our model of interpersonal connectivity work would suggest that such deficiencies can at least to some extent be buffered or overcome through embodied skill, which is gained through experience and is exemplified in an ability to balance the dualities of nearness and farness, freedom and control. Our theorizing also builds on earlier critiques of media richness theories (Lee, 1994) in arguing that the ‘richness’ of a communication medium is at least not completely technologically determined. Rather, we argue that media ‘richness’ also depends on how skilfully the practitioners involved are able to use these technologies in practice for interpersonal connectivity work.
Being able to quickly and effectively establish and maintain interpersonal connectivity remotely, in the way that we suggest the nurses are able to do, is also a particularly relevant skill in an emerging business context where organizational forms are optimized for flexibility and adaptability. ‘Responsive organizations’ are now often comprised of ‘highly interdependent teams of skilled individuals’ who are brought together on an ad-hoc basis to ‘complete demanding, complex, time-pressured projects’ (Wildman et al., 2012, p. 138). Such teams have been characterized (a) to be comprised of well-trained experts who have no previous work experience with one another, (b) to perform their team task almost immediately on team formation, and (c) to face high stakes from their inception (Mckinney, Barker, Davis, & Smith, 2005; Wildman et al., 2012). We liken elements of ad-hoc organizing to a challenge the nurses face, of establishing interpersonal connectivity quickly without prior social contact.
So far, such ad-hoc and temporary forms of organizing have been studied mainly from the perspective of trust. The idea of ‘swift trust in temporary groups’ (Meyerson, Weick, & Kramer, 1995) has in particular been influential. The notion of trust is however primarily concerned with addressing the risks of interdependence, whereby a party is willing to engage with the other in the first place. Interpersonal connectivity however takes a more positive stance in the sense that (in our formulation) it speaks to what it takes to create the constructive basis for effective remote team work to take place. We thus contend that the model of interpersonal connectivity work we have presented here could productively inform future ethnographic and phenomenologically informed process research on how different cohorts enact and, from the other side, experience interpersonal connectivity, in particular in remote leadership and also ad-hoc distributed group settings.
In conclusion, we have proposed that interpersonal connectivity work takes ongoing, skilful embodied work with technology to achieve and maintain. Future research could adopt a practice perspective (Orlikowski, 2010) to carefully study in a variety of distributed settings how interpersonal connectivity work is performed, how it is experienced, its sociotechnical nature, and how it can be fostered as a way to build resilience against connective gaps.
Footnotes
Acknowledgements
We are grateful to the special issue co-editors and to the anonymous reviewers for their helpful feedback. We also wish to thank the nurses who spoke to us in their own time for this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.