
Abstract
Purpose:
Patients with fractures of the pelvis and/or lower extremities are at a high risk of developing postoperative venous thromboembolism (VTE). The purpose of this study was to determine whether the thrombin–antithrombin III complex (TAT) tests could be used for postoperative screening of VTE in patients with lower limb or pelvic fractures.
Methods:
We enrolled 133 patients who underwent surgical treatment for fracture of the pelvis or lower extremities. TAT and D-dimer levels were compared in patients with and without VTE. Receiver operating characteristic (ROC) curve analysis was done and the appropriate TAT and D-dimer cutoff levels were determined for VTE screening.
Results:
VTE was diagnosed in 41 patients (30.8%). Patients with VTE had significantly higher levels of TAT and D-dimer on postoperative days 1, 3, and 7 than those without VTE, respectively. ROC curve analysis suggested that TAT test at postoperative day 7 had the highest accuracy for predicting postoperative VTE. With the optimal cutoff TAT level of 3.0 ng/mL, sensitivity and specificity were 93.3% and 70.1%, respectively. With the optimal cutoff D-dimer level of 7.4 µg/mL, sensitivity and specificity were 93.3% and 57.0%, respectively.
Conclusion:
TAT levels measured at postoperative day 7 could be the most useful parameter for screening postoperative VTE. TAT can be used as a screening tool for screening postoperative VTE in patients with lower limb and pelvic fractures.
Keywords
Introduction
Venous thromboembolism (VTE), including deep venous thrombosis (DVT) and subsequent pulmonary thromboembolism (PTE), is an important postoperative complication in major orthopedic surgery. 1 –3 Patients with fractures of the pelvis and/or lower extremities are at high risk of developing postoperative VTE. 4 –6 As PTE can be fatal, the diagnosis of VTE is clinically important. For the efficient diagnosis of postoperative VTE, it would be desirable to have a reliable and simple screening tool that can help determine whether imaging examinations such as contrast-enhanced computed tomography (CECT) or ultrasonography (US) should be performed. The plasma D-dimer level has been frequently used for this purpose and the clinical relevance of D-dimer test for screening postoperative VTE in fracture patients has been reported. 7 –11 However, it has been shown that D-dimer values are normal in about 30% of patients with DVT distal to the knee and in 5% of patients with DVT proximal to the knee. 12 Although a very high sensitivity of D-dimer test is reported in the diagnosis of VTE, its specificity is relatively poor. 1,7,11 In addition, the specificity decreases with increasing age. 13 Therefore, other more specific screening techniques are needed for the efficient prediction of VTE.
Thrombin–antithrombin III complex (TAT) is induced by thrombin and is a sensitive parameter of the latent activator of the clotting pathway. 14 Therefore, TAT test has been suggested as a sensitive parameter for VTE. 15 –18 Previous studies indicated that TAT levels were useful for predicting VTE after hip or knee replacement surgery. 15,16,18 However, the utility of TAT measurement in screening postoperative VTE of patients with fractures has not yet been evaluated.
We hypothesized that TAT test could improve the predictive accuracy of existing D-dimer tests for postoperative VTE in patients with fractures. The purpose of this study was to investigate TAT levels in patients with lower limb or pelvic fractures and determine whether TAT tests can be used as a screening procedure for postoperative VTE in these patients.
Materials and methods
Patients
This study was performed at our hospital from March 2009 to July 2015. Two hundred and eighty-three patients who underwent surgical treatment for fractures of the pelvis or lower extremities were eligible for this study. We excluded patients with VTE before surgery and those who had been receiving anticoagulation therapy before fractures. Patients with liver insufficiency, and aortic aneurysm, and those who received prophylactic anticoagulation therapy after surgery were also excluded. A total of 133 patients were included in this prospective study. There were 71 men and 62 women (mean age 55.9 years; range, 13–99 years); 11 had multiple fractures, 12 had isolated pelvic fractures, and 110 had isolated lower extremity fractures. Patients were considered to have multiple fractures if they had two or more simultaneous fractures of the pelvis and long bones of one lower extremity or simultaneous fractures in both lower extremities. 11 The pelvic fractures included pelvic ring fracture and acetabular fracture. The ethics committee of our institution approved this study.
VTE prophylaxis
All patients wore compression stockings and underwent intermittent pneumatic compression from the time of admission except during external fixation, skeletal traction, or casting or if there were contraindications to using these mechanical prophylactic devices. Prophylactic drugs were not administered. When graduated compression stockings and intermittent pneumatic compression could not be applied to the injured leg, they were still applied to the uninjured leg. All patients participated in active range of motion exercises for the ankles and toes.
Diagnosis of VTE
All patients routinely underwent US approximately 3 days preoperatively and 1 week postoperatively. Contrast-enhanced computed tomography (CECT) was also performed routinely at the same time points for patients with pelvic fractures or multiple fractures. Aplio XV (Toshiba Medical Systems, Tokyo, Japan) was used for US examinations. The following veins were investigated to detect DVT: common iliac vein, external iliac vein, common femoral vein, superficial femoral vein, popliteal vein, anterior tibial vein, posterior tibial vein, fibular vein, sural vein, and soleal veins. Compression methods and color Doppler were used. Aquilion 64 (64-row; Toshiba Medical Systems) was used for the CECT examinations. Veins of the lower extremities (from pelvis to ankle) were scanned to detect DVT in addition to scanning the chest with CECT to detect PTE.
TAT and D-dimer assays
Venous blood was sampled on postoperative days 1, 3, and 7 for TAT and D-dimer. TAT levels were measured using an enzyme immunoassay method (Mitsubishi Chemical Medicine, Tokyo, Japan). The normal TAT level is < 3.0 ng/mL. D-dimer levels were assayed using a latex photometric immunoassay method (Mitsubishi Chemical Medicine). The normal D-dimer level is < 1.0 μg/mL. TAT and D-dimer levels were analyzed and compared between patients with and without VTE at each time point. The day of surgery was defined as the day of definitive surgery for the internal fixation of the fractures. Temporary external fixation performed on the day of injury was not considered as surgery.
Statistical analysis
The Mann–Whitney U test was used to investigate the significance of differences in TAT and D-dimer levels between patients with and without VTE at each time point. A value of p < 0.05 was considered statistically significant. To determine the clinical performance of the TAT and D-dimer assays, receiver operating characteristic (ROC) curve analysis was performed. The area under the curve (AUC), 19 an important measure of the accuracy of the clinical test, was calculated. A guide for classifying the accuracy of a diagnostic test is as follows: 0.90–1 = excellent accuracy, 0.80–0.90 = good, 0.70–0.80 = fair, 0.60–0.70 = poor, and 0.50–0.60 = fail. The cutoff levels for TAT and D-dimer tests for VTE screening were also determined by the ROC analysis using the Youden index. 20
Results
VTE incidence
Of the 133 patients, 41 patients (30.8%) were diagnosed with postoperative VTE. All patients with VTE were asymptomatic. Seven patients (5.3%; 3 with multiple fractures, 3 with pelvic fractures, and 1 with a femoral shaft fracture) were diagnosed with PTE. Of the seven patients with PTE, four patients (two with multiple fractures and one with pelvic fracture) also had DVT (proximal in one and distal in two). Thirty-seven patients (proximal in 9 and distal in 28) were diagnosed with DVT.
TAT and D-dimer levels
Table 1 shows the mean levels of TAT and D-dimer assays between patients with and without VTE. Patients with VTE had significantly higher levels of TAT on postoperative days 1, 3, and 7 than those without VTE (p < 0.05, p < 0.01, and p < 0.01, respectively). As for D-dimer, there were significant differences in the mean levels between patients with and without VTE on postoperative days 1, 3, and 7 (p < 0.01).
Differences between patients with and without VTE in TAT and D-dimer assays.

TAT: thrombin–antithrombin III complex; VTE: venous thromboembolism.
aValues are mean ± SD.
bThe p value refers to differences between patients with and without VTE.
AUC
The AUC of ROC curves were analyzed (Table 2 and Figure 1). AUC in TAT assay on postoperative days 1, 3, and 7 were 0.6543 (poor accuracy), 0.7058 (fair accuracy), and 0.8592 (good accuracy), respectively. AUC in D-dimer assays on postoperative days 1, 3, and 7 were 0.7465 (fair accuracy), 0.7633 (fair accuracy), and 0.8033 (good accuracy), respectively. These results indicated that TAT test at postoperative day 7 had the highest accuracy for predicting postoperative VTE in patients with lower limb or pelvic fractures.
AUCs of ROC curves at each time point.

AUC: area under the curve; ROC: receiver operating characteristic; TAT: thrombin–antithrombin III complex

ROC curve analysis for (a) TAT and (b) D-dimer at postoperative day 7. In each diagram, AUC is given. ROC: receiver operating characteristic; TAT: thrombin–antithrombin III complex; AUC: area under the curve.
TAT and D-dimer cutoff levels
Since the AUC analysis revealed that both TAT and D-dimer tests at postoperative day 7 had higher accuracy, we determined their cutoff levels by using the Youden index. Their cutoff levels, sensitivity, and specificity are summarized in Table 3. It was found that the optimal cutoff levels of TAT and D-dimer tests at postoperative day 7 were 3.0 ng/mL and 7.4 µg/mL, respectively. With a cutoff TAT level of 3.0 ng/mL, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were 93.3%, 70.1%, 51.9%, and 96.8%, respectively. With a cutoff D-dimer level of 7.4 µg/mL, sensitivity, specificity, PPV, and NPV were 93.3%, 57.0%, 43.0%, and 96.1%, respectively.
Cutoff levels and performances of TAT and D-dimer assays at postoperative day 7.
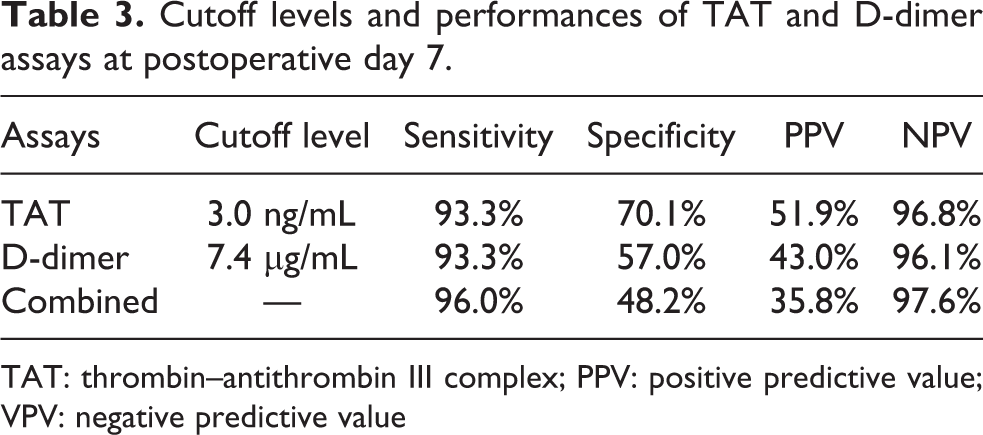
TAT: thrombin–antithrombin III complex; PPV: positive predictive value; VPV: negative predictive value
In the seven patients with confirmed pulmonary embolism (PE) by CECT, all their TAT and D-dimer levels at postoperative day 7 exceeded the cutoff levels. Among the 41 patients for whom VTE was diagnosed, 2 patients who had distal (calf) DVT were overlooked with the TAT cutoff level. Of these two patients, one patient had a D-dimer level of greater than 7.4 µg/mL. With the D-dimer cutoff value, two of the 41 patients with VTE, who had distal DVT, were overlooked. Of these two patients, one patient had a TAT level of greater than 3.0 ng/mL. When TAT and D-dimer tests were combined, taking the cutoff ranges of TAT and D-dimer tests, one patient who had distal DVT was overlooked, and the sensitivity, specificity, PPV, and NPV were 96.0%, 48.2%, 35.8%, and 97.6%, respectively (Table 3).
Discussion
VTE remains an important cause of perioperative morbidity and mortality in patients with lower limb and/or pelvic fractures. 21,22 Several authors recognized the impact of surgical interventions to increase the risk for VTE after fractures. 4 –10 A less invasive and highly accurate screening tool for VTE is needed that would allow immediate treatment. In this study, both TAT and D-dimer levels were higher in patients with postoperative VTE than in those without postoperative VTE, with statistical significance on postoperative days 1, 3, and 7. The ROC curve analysis revealed that TAT and D-dimer tests at postoperative day 7 had good accuracy for predicting postoperative VTE, with the TAT test at postoperative day 7 exhibiting the highest accuracy. TAT specificity at postoperative day 7 was higher than that of D-dimer, although TAT sensitivity was the same value as that of D-dimer. Collectively, these results suggest that TAT assay could be a useful screening test to predict VTE following surgery in patients with lower limb and pelvic fractures. This is the first study to show the usefulness of TAT measurement in screening for postoperative VTE in patients with fractures.
D-dimer is a measure of fibrin/fibrinogen degradation product decomposed product D fraction and has been reported to be a representative predictor for VTE. 7 –11 However, since D-dimer reflects secondary fibrinolysis after clot formation, it may not be useful as an early predictive marker for VTE. 23 When screening VTE, it would theoretically be more appealing to use markers that are more closely related to thrombin generation than to fibrinolysis. TAT is generated in the process of thrombin formation. The rise of TAT suggests that the thrombin is generating and the antithrombin is being depleted continuously. Therefore, TAT is the direct evidence of the increased activation of coagulation and the consumption of inhibitors. 14,24 The half-life of TAT is short, whereas that of D-dimer is long. 25 Thus, TAT levels increase rapidly and diminish relatively soon after the onset of VTE.
The diagnostic capability of the TAT and D-dimer tests was calculated by AUC analysis, and the AUC in the TAT and D-dimer tests at postoperative day 7 exhibited superior accuracy for predicting postoperative VTE (Table 2). TAT test on postoperative day 7 was the most reliable assay based on the AUC (0.8592). However, TAT test on postoperative day 1 had the lowest accuracy. Although there was a significant difference in the mean TAT levels at postoperative day1 between patients with and without VTE (p < 0.05; Table 1), the mean level in patients without VTE was higher than those on postoperative days 3 and 7. As fracture surgery is associated with inflammation, microvascular thrombosis, and surgical wound bleeding, the surgery itself causes elevated TAT levels. On postoperative day 1, surgery may induce a significant increase in TAT levels without any relationship to VTE development. As TAT in plasma has a shorter circulating half-life, this effect may diminish within a few days after surgery. Alternatively, surgery could cause a very transient and moderate activation of coagulation, leading to the generation of TAT in plasma, but without reaching the stage of thrombus formation. These hypotheses would explain the poor accuracy of TAT test at postoperative day 1 in the current study.
With the optimal cutoff levels calculated by the Youden index at postoperative day 7, sensitivity and specificity of TAT tests were 93.3% and 70.1%, respectively, whereas those of D-dimer tests were 93.3% and 57.0%, respectively (Table 3). PPV and NPV of TAT tests were 51.9% and 96.8%, respectively, whereas those of D-dimer tests were 43.0% and 96.1%, respectively. Combined with the results of the AUC, TAT could be a more useful marker than D-dimer for screening postoperative VTE of patients with fractures than D-dimer. Among the 41 patients for whom VTE was diagnosed, two patients with distal DVT were overlooked with the cutoff levels of TAT and D-dimer tests, respectively. When TAT and D-dimer tests were combined, only one patient with distal DVT was overlooked, and the sensitivity and specificity were 96.0% and 48.2%, suggesting that both measurements of TAT and D-dimer increase the sensitivity for screening of postoperative VTE. Sassa et al. 26 reported that both measurements of TAT and D-dimer led to high efficacy for prediction of VTE with the sensitivity of 84% and specificity of 96%. Although their subjects consisted of patients whose PE or edema of the leg had given rise to a clinical suspicion of VTE, they concluded that the combined measurement was very useful in screening for an acute VTE. Collectively, the combined measurement of TAT as a parameter of thrombin generation and D-dimer for fibrin dissolution at postoperative day 7 may provide valuable information for postoperative VTE screening.
There have been limited studies to evaluate the performance of D-dimer test in predicting postoperative VTE in patients with fractures. Niikura et al. 11 conducted D-dimer tests in 57 patients whose fractures caused by high-energy injuries were treated surgically, and they reported that the sensitivity and specificity of D-dimer tests at postoperative day 7 were 100% and 56.5%, respectively, at a cutoff level of 8.2 µg/mL. The AUC in the D-dimer test was 0.811. Terao et al. 8 performed D-dimer measurement at postoperative day 7 in 75 patients with proximal femur fracture who underwent surgery. Although they arbitrarily set the cutoff level as 10.0 µg/mL, the specificity and sensitivity were 71.8% and 85.4%, respectively. In contrast, to our knowledge, there has been no study that has investigated the efficacy of TAT for predicting postoperative VTE in patients with fractures. In our study, the sensitivity, specificity, and AUC of D-dimer tests at postoperative day 7 were comparable to those reported in the study of Niikura et al., 11 though the patient population was different. Our results revealed that TAT tests at postoperative day 7 exhibited superior sensitivity, specificity, and predictive accuracy compared to those of the D-dimer tests.
There are some limitations to this study. First, the study was conducted at a single institution and the number of enrolled patients was relatively small. Larger studies would be more beneficial. Second, we investigated only VTE that had developed by 7 days postsurgery. TAT and D-dimer levels in late-onset cases of VTE were not measured. However, there have been no published guidelines regarding the best time to screen, and serial daily screening till later time points is impractical. Bakhshi et al. 9 reported that 87.5% cases of postoperative VTE occur during the first 7 days after surgery in patients with lower limb fractures. It would be interesting to perform TAT and D-diner tests to determine their usefulness at later periods such as postoperative day 14.
Conclusion
TAT can be used as a screening tool for screening postoperative VTE in patients with lower limb and pelvic fractures. TAT levels were significantly higher in patients with postoperative VTE than in those without postoperative VTE on postoperative days 1, 3, and 7. The ROC curve analysis revealed that TAT tests at postoperative day 7 had the highest accuracy for predicting postoperative VTE, and the specificity, PPV, and NPV of TAT tests at postoperative day 7 was higher than those of D-dimer tests. Thus, TAT levels measured at postoperative day 7 could be the most useful parameter for screening postoperative VTE. In addition, the combined measurement of TAT and D-dimer at postoperative day 7 provides valuable approximations for VTE screening.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.