
Abstract
This article employs a sociological and dialogical information perspective to identify what shape information literacy practice takes for people who are hesitant about the COVID-19 vaccine. An information perspective places information and people’s relations with information at the centre of the inquiry. The study carried out 14 semi-structured interviews with UK adults who had not yet received or taken up their invitation to have the COVID-19 vaccine. Outcomes of this study suggest that information literacy practices related to vaccine hesitancy emerged through the liminal space and in relation to agentic performance, which was catalysed through engagement with experiential, corporeal and social information. This study has implications for the teaching of information literacy, in particular, the idea that being informed is an affirmative action that will automatically empower learners to make appropriate choices.
In May 2021, which marked the sixth month of the COVID-19 vaccine rollout, the United Kingdom had one of the highest rates of confidence in COVID-19 vaccines [1]. Trust in health authorities [1] and an initially successful national vaccine roll out were some of the reasons why vaccine acceptance was initially so widespread. At the same time, research demonstrated that this period also marked a significant hardening of opinions about COVID-19 vaccines with 9% of unvaccinated people in the United Kingdom indicating that they definitely would not have the vaccine, a statistic that was up from July and December 2020 [2]. Furthermore, the number of vaccinations had started to stall, plateauing at just below 70% by July 2022 [3]. This uptake was in stark contrast to that of neighbouring nations, some of which report vaccination rates of closer to 90% [4].
Information has frequently been positioned as playing a vital role within vaccination decision-making processes [5, p. 184]. Information sources have been found to constitute one of the major determinants of vaccine acceptance, while poor quality and inaccurate information or misinformation has been linked to vaccine refusal or delay [5, p. 182]. Information, health and digital literacy interventions are further positioned as a vital means of improving vaccine take-up through the work they do to counter poor quality and misinformation [6,7]. However, as Dubé et al. [5, p. 184] point out, these understandings position vaccine hesitancy as an issue that can be resolved by merely communicating better-quality information – and vaccine-hesitant people as manipulable, a knowledge deficit approach that is premised upon a lack of agency. This understanding further conceives of information literacy as a skill-based cure (or inoculation) against poor decision-making, an approach that ignores how becoming informed references situational, material and embodied ways of knowing [8]. These oversights, which risk obscuring an understanding of how people use information to learn about health, risk and prevention, also present missed opportunities for vaccine educators to meet their audience.
The study reported here examines these claims by examining vaccine hesitancy from an information literacy perspective. The research questions guiding this approach are as follows:
What shape does information literacy practice take for vaccine-hesitant people?
What are the implications of vaccine hesitancy for information literacy practice in general?
In asking these questions, this study recognises that vaccine hesitancy is a complex concept that defies an easy definition. Widely used in public commentary, the phrase has been critiqued for negative connotations [9, p. 4161] as well as its broad application, including for vaccine refusers as well as people who are merely uncertain [10, p. 6557]. Since then, vaccine hesitancy has been defined as ‘a delay in acceptance or refusal of vaccines despite availability of vaccination services’ [9, p. 4163] although this definition excludes physical barriers and gives insufficient emphasis to sociocultural influences on vaccine uptake [10, p. 6557]. For these reasons, this study adopts the common ground that is found between models of attitudes to vaccination [11, p. 1764] to position vaccine hesitancy as sitting in the middle of a continuum that ranges from ‘active demand for vaccines to complete refusal of all vaccines’ [11, p. 1764]; also see Leask et al. [12]. This approach acknowledges that people may refuse and delay certain vaccines but not others or that they may accept vaccines but be unsure doing so.
These research questions position information literacy as a sociocultural practice that draws together a suite of information activities that combine to reference contextual ways of knowing [8]. This approach precludes a focus on measuring predetermined information skills in favour of a deeper understanding of the complexity of the social, material and embodied dimensions of the practice it constrains and enables.
1. Literature review
Pre-COVID, most vaccine hesitancy research emerged from the field of public health and focused on early childhood vaccination, particularly in the wake of the fraudulent linking of the MMR vaccination with autism [11, p. 1768]. Typically centring on parental decision-making, these studies examine the social or political determinants of concerns about immunisation [9,13]. However, this research also draws attention to the information sources that people rely on when they choose not to vaccinate, albeit rarely forming the focal point. In contrast, research into later childhood and adult vaccination is less commonly explored [11, p. 1768]. Methodologically, research has tended to either interview non-vaccinating parents and groups [14,15] or analyse online discussion board posts [16]. Frequently supplemented by ethnographic data, these studies provide valuable insight into the impact of vaccination messaging. However, the focus on child vaccination and the peripheral role that is often accorded to information demonstrates the need to explore this topic further.
1.1. Information sources
Information sources form one of the most prominent themes within vaccine hesitancy literature. Often focusing on the impact of media, including traditional and new media technologies, these sources are frequently blamed for fanning the flames of vaccine hesitancy, including by undermining official messaging and promoting cognitive bias. Thus, various literature reviews point to the impact that the traditional media has on ‘keeping vaccination scares alive’ [11, p. 1765] and promoting two-sided debate [17, p. 49]. Similar ire is reserved for the Internet, which is deemed to expose people to ‘punchy’ [18, p. 105] anti-vaccination messages that are light on evidence-based scientific consensus [17, p. 51]. Social media is further singled out for the opportunity it provides for people to share personal vaccination experiences, which are deemed to muddy vaccine conversations through their focus on emotional testimonials [11, p. 1766, 17, p. 51]. However, the emphasis on a passive public, who lacks the ability to question or resist the ‘emotional sway’ of fear-laden messaging [19, p. 562], also ignores the complexity of vaccination decision-making, including the idea that information is sufficient to motivate (in)action [17, p. 53].
An underexplored form of information within vaccine hesitancy literature is the body. Hailed as influencing decision-making through drawing attention to prior inoculation pain [11, p. 1768] as well as an absence of side effects [20], the body is also positioned as a trigger for vaccine hesitancy when people personally experience or witness vaccine-related adverse health events [21, p. 4, 22, p. 1196]. The body is further referenced through the links that vaccine-hesitant parents make between salutogenic practices, including eating organic food, and the need for vaccines [23,24, p. 1121]. These ideas mirror studies into the trust that is placed in bodily focused complementary and alternative medicine practitioners [25]. One final interesting allusion to the importance of bodily information is parental instinct, which is also referred to as ‘Mother knows best’ [26, p. 868]. Constituting a form of embodied sensibility that is hard to put into spoken to written words but emerges from ‘knowing’ your child [15, p. 688], just as experienced firefighters read and recognise their platoon’s bodies as information sources [8], instinct shapes vaccine decision-making by ‘trumping’ professional advice about what the child needs [26, p. 869]. However, corporeal information remains underexplored within this literature.
A far more recognised form of information within this literature is the social network, which refers to the individuals that people go ‘to for information, direction, and advice’ [27, p. e1397], whether in-person or online. Typically comprising fellow parents, social networks are valued for the honest [28, p. 225] and visible [26, p. 867] insight that they provide into vaccination decisions. Social networks are also well-regarded due to the emotional support that information sharing between fellow members often engenders [23, p. 3]. At the same time, networks have been blamed for reinforcing vaccine-refusing views through the work they do to ‘incubate’ caution [29, p. 346] or validate parenting practices that challenge public health directives [23, p. 3]. Reich’s ethnographic research also illustrates how parents use information strategies, including withholding and deliberately distributing information, to build the social capital they need to combat negativity. Focusing on vaccine-refusing parents rather than the vaccine hesitant, this study hints at the complex ways in which health understanding is built.
A final source of information that has been noted within vaccine hesitancy literature, albeit with mixed impact, is the clinical care provider. Health professionals are often seen as useful sources of information about vaccination, particularly when medical providers take a personal interest in the vaccination decision [30, p. 14, 31, p. 1067]. Positive past experiences with medical staff are also seen as helpful [18,24] while research demonstrates that people who ‘receive information from their doctors seem less vaccine-hesitant than those who receive information from other sources’ [17, p. 46]. However, other studies indicate that clinical staff form ‘a last resort’ [26, p. 868] for vaccination information, either because they are perceived to be too busy [26,28], too inaccessible [26] or too dismissive of parental concerns [32]. Interestingly, medical professionals were also often seen as too ‘biased’ to be a useful source of information about vaccines [33], either because they were too favourable towards vaccination [17,32] or because of perceived pharmaceutical industry interference [20]. These conflicting opinions demonstrate how reliance on medical professionals is linked to issues of trust, both of care providers themselves and the information they supply.
1.2. Trust
Trust consequently forms a second important theme within vaccine hesitancy literature. Labelled as one of the three main determinants of vaccine hesitancy [9, p. 4152], trust in experts or groups is seen to reduce the uncertainty of decision-making [33, p. 355]. However, as the previous section has demonstrated, studies demonstrate that trust of healthcare workers is not always widespread, whether this is because of negative consultation experiences or broader concerns about biomedical systems. In contrast, studies are almost universally in agreement about the lack of trust that vaccine-hesitant people accord to governmental information. Tainted by the mishandling of other health and social crises [31, p. 1066], governments are also regularly accused of acting in collusion with pharmaceutical companies [28, p. 224, 30, p. 18, 31, p. 1066]. These fears, which centre on the perception that governments are withholding vaccination information, play out through increased cross-checking of official information sources [17, p. 46, 22, p. 1199, 25, p. 4]. Interestingly, given the moral panic about the impact of media messaging on vaccine hesitancy, studies also report increased cross-checking of media and Internet sources due to the scepticism that is frequently accorded these sources of information [22, p. 1199, 28, p. 224, 32, p. 1770, 34, p. 7, 35, p. 150].
In sum, rejection of public health advice means that there is growing interest into how people become informed about vaccination. At the same time, issues remain underexplored, including the idea that, contrary to popular belief, vaccine-hesitant people are often far more informed about vaccination than their vaccine-accepting counterparts. As Dubé et al. [11] point out, ‘studies have shown that parents who choose to vaccinate their child generally have limited knowledge of vaccination and vaccine-preventable diseases compared with parents who refuse to vaccinate’ (p. 1768). These allusions to the need for critical information engagement, which echo discourses that have been calling for increased personal and moral responsibility for health since the 1970s [36], have clear implications for our understanding of vaccine hesitancy.
1.3. Vaccine hesitancy and COVID
Few studies have examined the role that information plays in COVID-19 vaccination hesitancy to date, with research focusing on vaccine intentions rather than actions (though concerns noted in studies of vaccine intentions may not always translate to hesitancy) [37,38]. However, these studies have tended to corroborate the importance of trust within vaccine decisions with participants indicating that they have confidence in GPs, nurses and pharmacists rather than government when it comes to the COVID-19 vaccination [37]. Similar findings are noted in a study of healthcare professionals, who indicate that unwillingness to be vaccinated against COVID-19 is linked to a lack of trust in government rather than online misinformation [39]. Walker et al. [38, p. 5] also note how speed and time, including the feeling of being rushed, are frequently cited as complicating processes of becoming informed about the COVID-19 vaccine. A secondary strand of COVID-19 vaccination literature centres on the threat of misinformation and the role social media platforms play in propagating COVID-19 vaccine hesitancy [40,41]. Echoing many of the concerns of early vaccine hesitancy research, these fears are borne out through a UK-based survey that blames celebrity influencers and polycentric media diets for its discovery that 10% of UK adults plan to spread misinformation about COVID-19 vaccination [41, p. 10].
1.4. Vaccine hesitancy and information studies
Vaccine hesitancy has been explored far less frequently in Library and Information Science (LIS), which has tended to focus on parental deliberation related to early childhood inoculations [20,42–44] and the decision-making of healthcare workers [45]. Typically centring on the dissemination of medical information, these studies have drawn attention to the role that trusted medical care providers play in mediating vaccine hesitancy. Trust in information providers, who are seen as key to the countering of confusion and misperceptions, is also highlighted in Bossaller’s [46] examination of the comments section of vaccination news articles. Bossaller [46] further draws attention to the role that personal experience plays in vaccine hesitancy although she positions these narratives in opposition to authoritative sources of information. Since the start of the COVID-19 pandemic, studies of vaccination have tended to focus on the challenge of misinformation, particularly in relation to social media [47,48]. Examining the assessment of credibility in a Reddit discussion forum, Savolainen [48] notes that authorial expertise and presence of scientific information play vital roles in helping to ascertain the truth of vaccination claims. In contrast, there has been little focus on vaccine hesitancy within information literacy literature, which further suggests the need for research in this area.
2. Conceptual framework
The study is framed through the concepts of liminality and agency. Neither concept has been considered in detail in LIS research, and their inclusion as rich conceptual apparatus has enabled the researchers to reflect on the space that emerged in the transition from pre- to post-lock down and the implications for agency.
2.1. Liminality
Liminality refers to the in-between or the boundaries between time and space in ‘relationships, social roles and contexts’ [49]. It is characterised by ambiguity and can be employed analytically to ‘understand transition in the contemporary world’ [50, p. 1]. Liminality was originally introduced to anthropology by Van Gennep [51], who positioned transitional periods as shaped by rites of passage. These stages are described as preliminal rites (separation), which form a detachment from a stable point; liminal rites (transition), which describe an ambiguous state that is unrelatable to previous phases; and postliminal rites (incorporation), in which individuals transition into a stable new phase. The emphasis on passage and change led Van Gennep [51] to characterise liminal moments as one of the constants of social life: Life itself means to separate and to be reunited, to change form and condition, to die and be reborn. It is to act and to cease, to wait and to rest, and then to begin acting again, but in a different way. (p. 189)
From this reading, liminality attempts to encapsulate the in-between situations that occur when there is a dislocation of stable structures and the hierarchies within them, leading to uncertainty through the loss of social continuity and predictable future outcomes [50].
The liminal phase became the central focus of work by Turner [52], who defined this space as existing ‘betwixt and between’ known intra-structural states and unknown structurally invisible states. In further representing the liminal as a period of being betwixt and between social identities, Turner [53] suggests that, Social life is a series of movements in space and time, a series of changes of activities and a series of changes in status for individuals. (p. 159)
These ideas also position liminality as a time of reflection in which people attempt to scrutinise and understand social values and norms as well as ‘the powers that generate and sustain them’ [52, p. 105].
The concept of the liminal period has been picked up in the health field where considerable research has been conducted into transition [54] and patients’ experiences of disruption [55,56]. In information studies, liminality was acknowledged in research examining refugee information practices [57]. The identification of three phases of transition within this study subsequently led Lloyd [58] to describe the transitionary nature of fractured landscapes. Liminality has also been briefly explored in relation to information behaviour, albeit positioned as a theory rather than a concept [59], and information literacy, where it has been associated with threshold concepts in the ACRL’s [60] Information Literacy Framework.
2.2. Agency
The concept of agency is more complex than its dictionary entry implies. Classified by the Oxford English Dictionary as ‘action or intervention producing a particular effect’ or ‘a thing or person that acts to produce a particular result’, this definition positions agency as an effect that occurs as a ‘consequence’, which ascribes an objective dimension to the performance. However, early work by Mead [61, p. 76] contends that humans experience temporality during situated passages (transition) from old to new and these passages help to shape identity or social character by forcing them to reconstruct the past to understand the emergent present and shape the arising future. Emirbayer and Mische [62, p. 63] conceptually link agency to temporality through positioning agency as a ‘temporally embedded process of social engagement’ that is informed by understandings of past, present and future.
Understandings of agency also frequently emphasise the individual’s power to act in ways that shape experience. These ideas, which emphasise the performance of complex social activity, centralise reflexivity by highlighting that we are ‘agents precisely at the point of consciously choosing a course of action to follow in circumstances where we could have acted otherwise’ [63, p. 323]. The focus on deliberation is further underscored by the importance that is placed on both ‘knowing and having what it takes to achieve goals’ within ideas of self-empowerment [64, p. 17]. At the same time, agency forms a relational rather than an individual phenomenon as people produce effects through social connections, including through the ‘webs or networks of relations and interdependencies, both interpersonal and impersonal, in which interactants and their joint actions are embedded’ [63, p. 323].
The dialectical nature of agency is emphasised by Barad’s concept of agential realism. Barad [65] views agency as a relationship embedded ‘intra’-context rather than something that someone has; ‘knowing comes from direct material engagement with the world’ (p. 49). By this account, agential realism rejects universal knowledge for local or situated knowledge and ‘understandings that are embodied and contextual’ [66, p. 187]. Agency is consequently viewed ontologically as referencing the ways in which people understand the nature of reality and their intra-actions; ‘knowledge comes from the between of nature-culture, object-subject, matter-meaning’ [66, p. 188]. This performative understanding of agency situates context and its affordances and emerges in the way we do things or practise [67]. In this regard, materiality matters because it takes on significance (as intra-action) within the context rather than prior to it [66, p. 188].
Agency has not been explored in detail within information studies and information literacy research [68]. While the concept is often used within information practices research to acknowledge the influence of material objects as well as non-dualist ontologies [69], these ideas have not yet translated to an examination of the role that agency plays in shaping information activity or wider information decision-making.
3. Methods
The study, which was funded by a British Academy/Leverhulme grant (SRG2021\211338), adopted a qualitative design to examine the rich and multi-faceted ways in which people became informed about COVID-19 vaccines.
A total of 22 semi-structured interviews were carried out in May–July 2021, which corresponded with the later stages of the UK’s age and health-driven vaccination drive. By the time of the last interview in July, all adults in the United Kingdom had been offered the opportunity to book an initial vaccination appointment. Interviews were semi-structured to produce a broader understanding of how people became informed about the COVID-19 vaccine, but questions initially focused on useful and problematic sources of information, challenges learning about the vaccine, including information overload and ‘fake news’, and previous vaccine hesitancy. Interviews were audio-recorded using an end-to end encrypted video conference tool approved by (UCL). Recordings lasted between 25 and 45 min and were professionally transcribed. Written informed consent from each participant was obtained prior to interviews.
Participants were recruited through adverts that were placed on social and community websites where vaccination was being discussed, including Reddit coronavirus threads and Mumsnet, a parenting-focused community site. The advert called for people based in the United Kingdom who were aged over 18, and who were still making up their minds about whether to have the COVID-19 vaccine or not. Participants were offered a £20 gift card for participation. From this initial recruitment drive, a convenience sample of 22 participants was subsequently interviewed, of which 8 had already been vaccinated and 14 had not. Findings from this study are based on the responses of the 14 people who had not been vaccinated at the time of interview. Participants included six males and eight females, represented a wide range of ages, and were located throughout the United Kingdom.
Data were coded and analysed by both researchers using the inductive constant comparative techniques that are used in constructivist grounded theory methods. This method follows the procedures outlined by Charmaz [70] and as detailed in a previous article that reports on other aspects of this research [71]. Recordings and transcriptions of interviews were reviewed independently by each researcher before the initial round of open coding was discussed together over multiple online sessions to produce several emerging themes. A further round of focused coding and discussion consequently led to the establishment of the five thematic codes that are presented below. Limitations of this study include the reliance on online methods of recruitment, which may have favoured more tech-savvy respondents as well as people who were actively engaged in online debate and discussion about vaccination. Our decision to avoid collecting demographics, which was done due to the sensitivity of this topic, may also be considered a limitation.
4. Findings
Analysis and coding of interviews suggest that vaccine-hesitant people engage in five major information activities to inform themselves about the COVID-19 vaccine. These are as follows: Listening to stories, to connect with personal and emotional dimensions of the vaccine; Reading the body, to access experiential information about the vaccine; Pooling, to break down complex information about the vaccine; Confirming against expertise, to corroborate information against expert opinion and advice; and Hedging, to protect themselves against potentially misleading information. Together, these five information activities represent the agentic-focused information activities associated with information literacy that occur with the context of the COVID-19 setting. Information activities are unpacked below.
4.1. Listening to stories
Facing a barrage of impersonal, official information about the vaccine, including from the media, government and healthcare sector, vaccine-hesitant people indicate that they turn to the stories of previously immunised friends and family to develop a more nuanced understanding of the vaccination process. Providing a way for people to access experiential or embodied information, listening to stories forms a way for people to connect with trusted concrete and pragmatic knowledge [72] in a time of high risk and uncertainty.
One of the most important sources of information that vaccine-hesitant people use to become informed about COVID-19 vaccines is everyday stories about vaccination experiences, a finding that reiterates the importance of social networks within studies of childhood vaccination [26–28]. These stories, which are shared with them by people who have already been immunised, become vital sources of information because they reference situated knowledge about both vaccination and the recovery period. For some, this information helps to assuage concerns about the impact of vaccination: I have an adult daughter and she got Pfizer, and she’s doing pretty well, so that’s reassuring. (Participant B)
For others, however, listening to stories draws attention to the negative experiences of being vaccinated, including the potential impact on everyday life: Friends that have been done, my family, one of them already got injected and she had a complain with fever, with fatigues, maybe at two weeks’ time is (sic). And she was like, ‘Please, just take a minute before you just take’. (Participant G)
These warnings may be further compounded by accompanying photographs of swelling or redness (Participant U), which provide a further visual cue of the impact that the vaccine might have upon their body. Valued because of their origins in embodied performance or the accumulated experiences of others, these stories alert people to the personal and emotional dimensions of vaccination, which must then be reconciled against instrumental forms of knowledge.
At the same time, ‘real-life’ stories about vaccination were not accepted uncritically. Instead, participants indicated that they tended to rely on the stories of friends and family members who were typically further ahead in the UK’s strict vaccination roll out queue because they were seen to be highly trustworthy, something that is also noted in childhood vaccination studies [28]. People could also use personal knowledge that had developed through interaction over time, for example, to assess the credibility of their narrative: Because I know them better I kind of know if they’re being funny about something or not, giving the full story, and they will have a bit more balance about things, and not give a slant to it as such. (Participant B)
Trust was also accorded to people in the public eye when their stories were assessed to be genuine or told without an agenda, as Participant H states about listening to the experiences of Margaret Keenan, who was the first person in the United Kingdom to receive the vaccine: She was somebody who’d obviously put herself forward and she’d had it, obviously not had any side effects … [it] really felt as if it came from the heart, that she really believed it. (Participant H)
Illustrating how participants employ a range of checks and balances to ascertain the veracity of narratives, including triangulating stories with online accounts (Participant G), and checking details of individual stories (Participant U), the focus on the storyteller’s experience also demonstrates how the apportioning of trust must be seen as similarly embodied and experiential. These strategies further underscore how the ‘crucial locatedness of bodies’ [73, p. 128] becomes a specific resource for becoming informed in times of risk and uncertainty.
4.2. Reading the body
A second way in which people indicate that they inform themselves about the COVID-19 vaccine is through reading their own bodies, a strategy that encompasses a wider variety of sensory encounters than listening to stories but references a similar quest for intimate, firsthand experience. Centring the physical impact that vaccination has on people, the reliance on corporeal information further demonstrates the importance of situated forms of knowledge for becoming informed about the vaccine.
As details of the recently developed vaccine emerge, participants’ bodies begin to take on a newly important role in the process of becoming informed. For many participants, reflections on the ways in which they reacted to prior vaccination means that their body is immediately centred as a key source of information for the COVID-19 vaccination: I get quite anxious in those kind of environments and I haven’t reacted very well when I’ve had vaccines before. (Participant W)
Re-emphasising the importance that physical experience of practice has within vaccine hesitancy, as seen in childhood vaccination [21], the focus on the ways in which participants know and understand their body also illustrates how corporeal information facilitates reflection and reflexivity [74, p. 93]. Similar fears were seen with participants who became preoccupied about whether chronic illness symptoms that mimic the side effects of vaccination would obscure potential issues with immunisation, such as blood clots (Participant B). The importance of embodied knowledge to the management of disease or pain has long been recognised within studies of hospitalised and chronically ill patients [75].
Participants also monitor their own bodies as they take extra precautions to safeguard themselves and their community [71]. A focus on ‘washing hands frequently, sanitising’ (Participant M) and ‘eating healthily’ (Participant J), for example, demonstrates how participants centre their body as they adopt personal preventive measures, which is similar to the ways in which supervision helps parents make vaccination decisions [15]. While evidence that diet will provide protection against COVID-19 is still being explored [76], these actions reinforce how bodily information both shapes and directs agency, something that is also seen in studies of child vaccination decision-making [15]. Statements also seem to pick up on the health authorities’ reported concerns that COVID-19 hits obese people and those with underlying health conditions the hardest. Beyond personal measures, participants centre corporeal information through the precautions that they adopt to protect other people in shared social spaces, including wearing PPE and maintaining social distance (Participants K, L, M, N and Q). The observation of what participants perceive to form reckless behaviour by vaccinated people, for example, illustrates how people inform themselves through positioning their bodies in relation to others: I mean I also see behaviours that I find quite scary, and I avoid to be [sic] in those contexts as much as possible. (Participant K)
Demonstrating how bodies become the centre of safeguarding practice [71], these comments, which echo arguments that complementary and alternative medicine advocates make about the primacy of the corporeal [25], further highlight how vaccine hesitancy is shaped in relation to a reading of shared sensory encounters.
4.3. Pooling
The fragmented nature of COVID-19 vaccine information means that pooling information with others forms another important way in which people inform themselves about inoculation. Pooling is an activity where often ‘incomplete’ bits of information are actively shared among a group of participants to develop a more comprehensive overview or insight into a critical issue (such as the pros and cons of the suite of COVID-19 vaccines). Differing from information sharing through the emphasis on collective coping [77], pooling is valued because it forms a way to mediate different knowledges, including formal and informal sources of information. At the same time, it can also lead to tension as people share contested forms of knowledge.
As the COVID-19 vaccine information environment continues to grow in complexity, people start to pool information that they encounter with friends and family. A collective coping strategy, pooling helps people to extend their knowledge about the vaccine as well as to adjust and reframe understanding. Participants engage in pooling, for example, to tackle confusion over complex scientific or technical ideas (Participant B) as well as to cope with limited digital skills (Participants B, J and W). In an era of misinformation, pooling may even extend beyond family and friendship groups to form a way for people to cope with the spreading of unreliable information in an online sphere, as seen through the work one participant does to share the results of his research: Or if I see somebody is just trying to manipulate other people because they don’t have [unintelligible] I will just pop in and give a few facts and leave. (Participant Q)
Centring on breaking down complex sources of formal information yet taking place within everyday interactions in community-based spaces, pooling helps participants to become informed through connecting them to both institutional and more nuanced ways of knowing. The emphasis on collaborative problem-solving further illustrates how pooling references future-oriented agentic practice [71].
At the same time, participants also pool information to reinforce views and opinions, including through seeking to purposefully influence conversations in which they are involved. Pooling consequently form the means through which unsubstantiated information may be spread, as suggested by Participant K’s sharing of information that she found in Cosmopolitan magazine with her work colleagues. These ideas are also seen in childhood vaccination decision-making, where social networks have been blamed for ‘incubating’ fear about vaccines [29]. Similarly, the emphasis on collaborative coping illustrates how pooling strategies can also lead to the creation of echo chambers in which people feel safe sharing potentially controversial information with like-minded audiences: Participant L, for example, purposefully used WhatsApp to share information about vaccine side effects with sympathetic friends. Raising questions about who has the power to control and shape access to information, these experiences highlight how pooling can provoke tension particularly when opinions differ within communities or family groups; Participant L started distributing information to her vaccine-hesitant WhatsApp group, for instance, after feeling invalidated for sharing her concerns about the vaccine with her family. Providing another illustration of how information sharing is entwined with social support [75], the emphasis on inclusion and exclusion also raises questions about the role that pooling plays in helping people to mediate stigma and other barriers to engagement.
4.4. Confirming against expertise
As news and rumours about the vaccine continue to swirl throughout everyday life, the process of becoming informed is further shaped through the work that people do to confirm or corroborate information they have come across against expert opinion and advice. Centring on a quick check of information against a known institutional and professional source rather than verifying medical advice, confirming against expertise draws upon ideas of cognitive authority [78] as participants seek to assess the credibility of non-experiential evidence. At the same time, trust in these sources is not automatic, and participants continue to critically assess the contributions of experts rather than taking their recommendations as read.
Faced with fanciful stories or conflicting information about the vaccine, participants indicate that they frequently reach out to trusted sources of information to confirm the veracity of what they have heard, an approach that has also been referred to as ‘escalating authoritativeness’ [68]. One of the most important sources against which participants check information is the National Health Service (NHS) website, which is seen as credible due to the medical authority that it holds in the United Kingdom: I … make sure any time I want to read about something, I make sure I go to the right, you know, place to check. Anytime I have anything I want to check, I just go to the NHS website and check it, you know. (Participant T)
Other frequently mentioned sources are family doctors, who are seen as particularly trustworthy when people have a long-standing relationship with them, a finding that is also seen in prior childhood vaccination studies [30,31]. Valued for their professional expertise, family doctors are also prized because of their ability to assess the potential impact of the vaccine in relation to a participant’s personal medical history: Because he [the doctor] just explained to me that since I don’t have any – you know maybe any prior illnesses occurring, maybe side effects, that it’s good, I should go for it. (Participant R)
Demonstrating how becoming informed about the COVID-19 vaccine is shaped in relation to decisions about the authoritativeness of information sources [78], the emphasis on trust also demonstrates the effort that participants put into assessing what is ‘worthy of belief’ [78, p. 15]. The corroboration of news reports through comparison with national and international media (Participants R, W and X), which is also seen in childhood vaccination studies [28,32], provides a further illustration of the important role that the negotiation of plausibility plays within vaccine hesitancy.
Trust in expertise is not absolute, however, and participants indicate that they supplement their assessment of key information sources with a range of additional checks. Several participants, for example, question the worth or value of traditional markers of medical expertise in the face of a novel coronavirus, even though they generally hold medical professionals in high regard, something also noted in Greyson and Bettinger’s [20] examination of vaccine-hesitant parents: And I don’t think your average GP … they’ve got a medical background, but it doesn’t make them an expert in a new emerging virus that no-one’s met before. (Participant H) And if that’s [the vaccination production process] going to take years, how can you get something with – I don’t care what university they went to. (Participant N)
Others extend their concern to the medical profession more generally, linking apprehension that the vaccine might impact female health (Participant K) with the many historical oversights related to female illness and disease [79]. Demonstrating an increasingly critical assessment of the quality of information sources, these findings also point to how typical markers of competence and trustworthiness, such as expertise and professional titles, may not stand up in the face of high pandemic uncertainty.
4.5. Hedging
A final strategy that participants employ to become informed about the COVID-19 vaccination is to hedge against information sources that they suspect are misleading or disingenuous. Constituting an increasingly cautious engagement with information sources rather than a wholehearted acceptance of their validity, hedging forms a strategic action designed to protect people from the risk of falling for poor or misleading information rather than constituting a withdrawal from society. Hedging is consequently often linked to growing mistrust of governmental narratives or the fear of falling for overly emotional media narratives and is expressed through the gradual reduction of exposure to these sources of information.
Faced with a wide range of vaccine advice, participants start to hedge or guard against uncertainty by drawing away from specific forms of information. One of the major forms of information that participants start to be careful of is government information, which is perceived to lack detail (Participant G), contradict medical advice (Participants H, K, W and X) or, at its most extreme, constitute a deliberate attempt to deceive (Participants G and Q). Resulting in an increasing disinclination to heed or trust government messaging, which is also noted in childhood vaccination [30,31], hedging consequently forms an attempt by participants to shield themselves from poor quality information rather than excess, as Savolainen [80] found in his study of environmental activists. Another form of information that participants start to retreat from is the media or the press, which is referred to as ‘draining’ (Participant L), ‘negative’ (Participant W) and as focused on ‘fear mongering’ (Participant K). Seen to limit its credibility, the emotional focus of the media is also deemed to risk clouding or inhibiting participant judgement about vaccination. As Participant A points out, ‘you shouldn’t really use emotions to make a decision’. Suggesting that participants’ increasingly deliberate distancing from certain forms of information forms a nuanced and contingent form of self-care in the face of confusion, the emphasis on the future utility of government and media messaging also illustrates how hedging must be seen as both temporally and affectively situated.
At the same time, the decision to hedge against certain information sources does not mean that participants completely cut themselves off from ongoing vaccine news and updates. Instead, they use a variety of technological affordances to reduce engagement with specific forms of information, including by selectively monitoring the information to which they are exposed: I have removed the news from my feed, so I don’t have them appearing on my feed, but then every couple of days I still go check the news, but I just, I’m more in charge of deciding what I want to read, versus just seeing a scary headline appearing on my newsfeed on my phone. (Participant K).
Acknowledging participants’ agency to move within and through the vaccine discourses that surround them, this ‘pull’ approach to retrieving information [80, p. 613] illustrates the active role that people play in mediating vaccine information. It also draws attention to the affective demands of interacting within these information environments as people seek to take a more active role in managing their health and well-being. What is not yet clear, but would be worth exploring in future, is whether hedging during the liminal period leads to large-scale avoidance of information or its acceptance.
5. Discussion: liminality, agency and informed learning
Findings have demonstrated that COVID-19 vaccine hesitancy develops through information activities that together constitute information literacy practice within this context. Our understanding about the complex practice of hesitancy will now be unpacked through drawing on themes of liminality and agency. To do so, it is first necessary to consider the ‘space’ between pre- and post-COVID-19, which is where hesitancy emerges as an agentic performance.
Employing van Gennep’s model, the space that occurs between separation (pre-COVID-19 normal) and incorporation (the ‘new’ normal) is the liminal space. In this model, the pandemic creates a transitional environment where people move through a liminal space pre- and post-COVID-19, as represented in Figure 1:
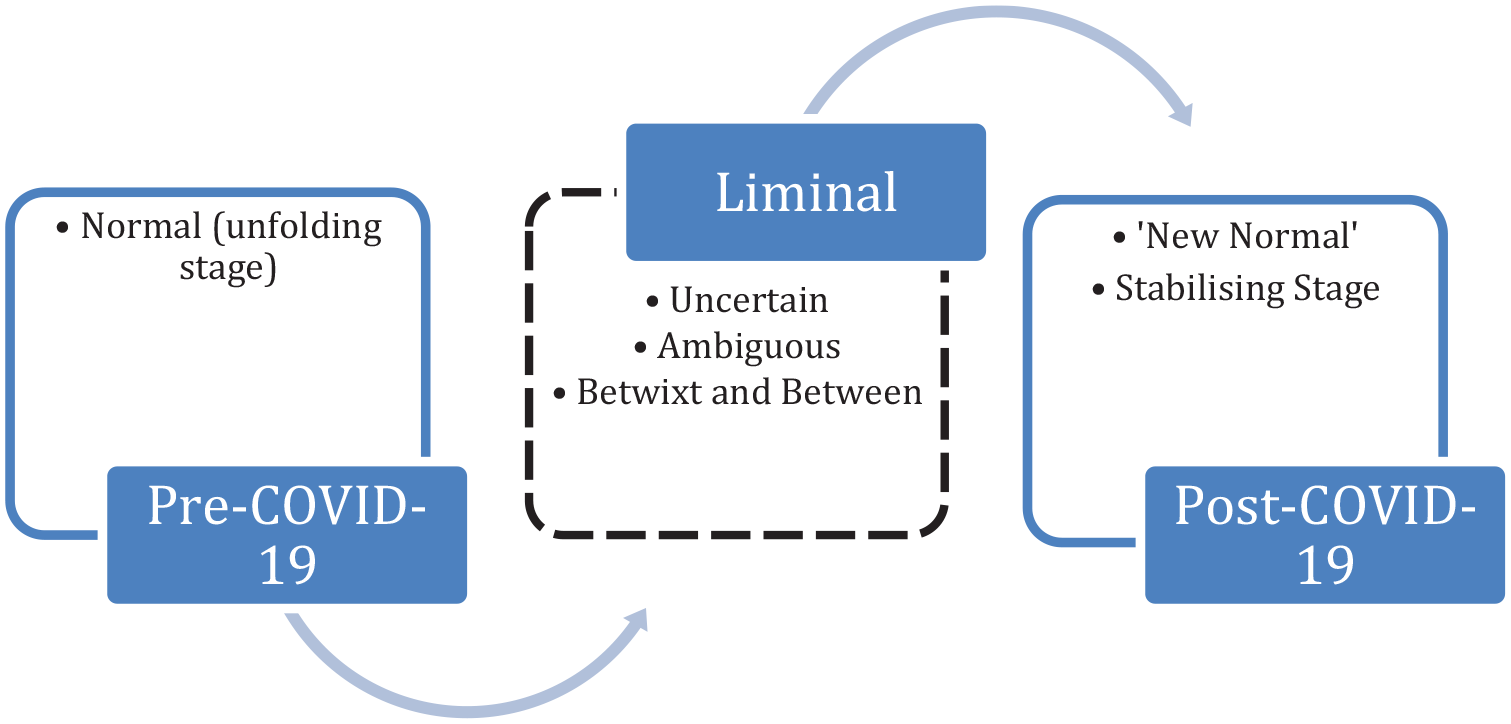
The liminal COVID-19 space.
During this time, feelings of ambiguity and uncertainty mean that the liminal space acts as a ‘sourcing’ space where versions of knowledge (including embodied and contingent experiences, institutional/epistemic knowledge and understandings of past, present and future) become contested or reconciled. This leads to a sense of disorientation when ways of knowing about COVID-19 become open to multiple interpretations as people intra-act with the virus via institutional, opinion-based and experiential information sources. It is the tension in this dynamic from which hesitancy emerges. This tension was also heightened by the UK government’s [81] positioning of the vaccine in instrumental terms, as the means to end the pandemic, and as part of the ‘common good’, to protect everyone in the community. This emphasis on social norms is also noted as important in childhood vaccination decisions [82].
Participants respond to the complexity of this time by informing themselves about the vaccine and its societal and medical consequences through employing a range of protective information activities, including shielding themselves from unsubstantiated rumours and untrustworthy information providers. These activities, which together constitute the practice of information literacy, acknowledge and work to mitigate the noise [83] created by the emerging COVID-19 environment by minimising the ambiguous and contested forms of vaccine knowledge that people encounter as they transition between the pre- and post-COVID-19 space (the betwixt and between). These strategies subsequently lead participants to make the decision to delay vaccination rather than conform to governmental and medical advice. Vaccine hesitancy consequently represents an agentic response to the ambiguity of this liminal period as participants make active decisions to embrace the solidity of experiential sources, including through drawing from stories or pooling information [77] with trusted friends and family, and to turn away from and perform additional checks of instrumental government advice. Participants’ decisions to delay are thus informed by the multiple sources of information and ways of knowing that constitute their vaccination information landscapes [8], even when they recognise that the execution of their agency to delay may lead them to become ‘othered’ as uninformed [17].
The recognition that participants had often had other vaccines (including for travel) means that agency can be disaggregated from the broader context of vaccine uptake or hesitancy. Embirbayer and Mische [62, p. 1009] note that ‘actors may be capable of switching between agentic orientations and thereby exercising mediating influences upon their contexts of action’. In this context, participants alter their actions according to the circumstances and conditions of the situation because ‘agencies are only distinct in relation to their mutual entanglement; they don’t exist as individual elements’ [65, p. 33]. Hesitancy, therefore, represents an informed relational agentic performance that is constructed within the liminal space where ‘events and ideas – and indeed “reality” itself – can be carried in different directions’ [50, p. 42]. Barad [66] refers to this as the agential cut, whereby new boundaries are constructed according to changing contextual relationships that are central and necessary for meaning making. From this perspective, the liminal space is not simply a passage but forms a contingent temporary space that is temporally bounded by thresholds that are crossed and then left again (pre- and post-COVID-19). Meaning making occurs within this temporary transitionary space where knowledge, context, discourse and agency are enmeshed in an intra-relationship [66], an idea that further highlights the contingent nature of information ‘as any difference that make a difference’ [84]. Within the pandemic context, the liminal space consequently becomes an important temporal site for decision-making that leads to agentic actions of uptake, delay or resistance.
The study also brings the role that the body plays in bringing agentic performance in space and time into view. Barad [65, p. 49] points out ‘knowing comes from direct material engagement in the world’. The temporal nature of the liminal space led participants to engage with narratives about the real and imagined consequences of vaccination via social and digital space; participants became informed through using their bodies and the bodies of others to access nuanced and situated information about the physical experience of vaccination. Hesitancy by this account is a performative act that shows up in the way people protect or shield their bodies from the effect of vaccination while agency is referenced in people’s decision to delay vaccination as well as their emphasis on others’ experiences as significant to becoming informed. Agentic performance is also reflexive, which was evidenced by the ways hesitancy emerged from the work that people do to reflect and reconcile shared understandings about the COVID-19 vaccines. The NHS, for example, which is reported as one of the most trusted sources of information, is employed to reconcile opinion-based sources derived from family and friends. These actions highlight how we establish trust in others (as opposed to a lack of trust in government sources); however, it also raises questions as to how participants judge the veracity of socially nuanced knowledge outside of their emotional/familial connection.
6. Why information literacy cannot fix vaccine hesitancy
These findings, which demonstrate that vaccine hesitancy emerges through the enactment of socially and materially situated information literacy practices, have several implications for our understanding of agentic-focused information activities within liminal spaces. In drawing attention to how these activities support the navigation and mapping of a highly contested and stigmatised information environment, these findings also challenge narratives about what travels in relation to information literacy practice.
The first narrative to be challenged relates to knowledge and understanding; unlike what may be assumed, findings from this study demonstrate that vaccine-hesitant people are both informed about the COVID-19 vaccine and, in many respects, information literate. Participants in this study, for example, reference a wide range of information skills as constituent elements of their information literacy practice, including searching, evaluating and thinking critically about the range of sources available to them. These skills are ones that would be recognised by teaching librarians and institutional information literacy guidelines alike. Furthermore, contrary to what is often found with some library studies [85,86], participants also demonstrate high levels of motivation for inquiry. The emphasis that is placed on problematising information production and use [87] means that participants could also be characterised as critically information literate. Elmborg’s [88, p. 193] portrayal of the critically information literate as people who ‘take control of their lives and their own learning to become active agents, asking and answering questions that matter to them and to the world around them’, for example, could be applied to this study’s participants. This study consequently challenges research that links vaccine hesitancy to poor information skills [28] by illustrating how vaccine-hesitant people demonstrate situated and embodied ways of finding, using and evaluating information related to the COVID-19 vaccination.
The recognition that the decision to delay vaccination represents an informed response means that findings from this study also challenge information literacy’s empowerment narrative. Empowerment is typically referenced within information literacy discourse through superficial ‘motherhood statements’, where the development or acquisition of information skills ‘empowers’ learners to engage in responsible acts of citizenship [89]. However, findings from this study complicate this narrative by demonstrating how empowerment is signified by the agentic performance of delay rather than proactive engagement with society. Illustrating how empowerment cannot uniquely be seen as affirmative [83], these findings also challenge the perception that information literacy will automatically engender social well-being. Instead, people are as empowered to take socially unacceptable decisions as much as acceptable ones. Underscoring how information literacy discourse references an unstated yet very specific set of cultural values rather than neutrally and unproblematically advancing the democratic agenda, findings from this study also extend research that has started to interrogate the influences that shape information literacy practice [89,90].
The recognition that vaccine hesitancy centres on the employment of protective and delaying information strategies rather than the precise and deliberate skills that are often privileged in information literacy curricula means that this study also challenges many of the field’s inward-facing narratives. Informed learning, for example, which has become infused as a prominent seam of research and pedagogic practice in the field, frequently positions information literacy as centred on successful, creative and responsible information use within ‘rapidly evolving information environments’ [91, p. 7–8]. However, the importance that this study places on resistance and delay, such as how people employ technology to reduce their engagement with authoritative sources, rebuts this affirmative narrative, including normative notions of what informed learning should be. After all, in a time of high personal risk and when clinical data are still emerging, what could be more responsible than taking the time to properly evaluate the evidence that is accessible to you? Findings from this study also extend recent critiques [83] of the importance that is accorded to preparatory rather than reactive elements of practice within highly cited models of information literacy; for all the emphasis that institutional guidelines place on the need for reflexivity and evaluation [90], current information literacy discourse does not often allow for the type of hesitation that is noted within this study.
What is taught in the information literacy classroom consequently forms the fourth narrative that is challenged through the findings of this study. This is particularly important given that several vaccine-hesitant studies conclude by calling for increased information, health or digital literacy interventions [6,8]. However, given the emphasis that is typically placed on positive rather than protective information activities [90] within current information literacy teaching guidelines, it is not clear how much impact current iterations of these interventions would have. More expressly, findings from this study suggest a need to re-focus attention on the processes through which people learn, particularly in complex or high-risk situations. The emphasis that this study places on liminality, for example, suggests that when information literacy teaching is offered it should centre on preparing learners [92] to deal with the uncertainty of liminality within transition, rather than uniquely focusing on separation (novice) and incorporation (expert) states. Even the ACRL [60] Framework for Information Literacy, which highlights the importance of the liminal threshold, elides this pivotal moment in its rush to achieve what it sees as an expert status. Focusing more concretely on this intermediary stage would acknowledge the importance of reflexivity within liminal processes while further accounting for the enactment of the agential cut [66].
Findings from this study consequently situate information literacy at a type of crossroads. On one hand, this study has vindicated the important role that information literacy plays in becoming informed about the COVID-19 vaccine, a finding that underscores the important work that librarians and researchers have been doing to establish information literacy as a transformative social practice that impacts all walks of life. On the other hand, findings from this study reveal that information literacy practice can no longer be autonomously associated with the advancement of the liberal agenda, wherein ‘informed learning’ [91] is mechanically associated with making ‘good, rational choices’ that fulfil citizenship obligations [93]. Instead, as demonstrated in this study and intimated by Lee et al. [94] in their study of data visualisations, information literacy is enacted wherever and in whatever form learning takes place, whether this learning is socially acceptable or not, an idea that inevitably exposes the extreme fragility of mainstream professional narratives. How, then, do we mediate this paradox? For some, the answer lies in virtue epistemology, which links morality with knowledge activities [95,96]. For others, the answer is found in radical information literacy [93], although this study has evidenced that criticism of power structures can lead to many different types of activism and political action. Perhaps, one of the most important contributions of this study, therefore, is to make it clear that much information literacy research and practice is still, at its heart, a moral enterprise that is suffused with unacknowledged, middle-class [97] assumptions about how to ‘live our lives and conduct our bodies’ [36, p. 174] rather than forming the liberatory and transformative practice that it is often made out to be.
7. Conclusion
This study has examined how vaccine-hesitant people in the United Kingdom employ information literacy practices to inform themselves about the COVID-19 vaccine. Findings indicate that, contrary to what has often been assumed, hesitancy constitutes a relational experience that emerges from and within transition. The disorienting and ambiguous nature of the liminal space (between pre-COVID-19 norms and post-COVID-19 new norms) references both spatial and temporal dimensions leading to a privileging of socially nuanced information and sites of knowledge. These sources act as concrete evidence that counters confusing and often contradictory official advice. Vaccine-hesitant and hesitant-influenced actions consequently form an agentic, informed performance that centres on protective and delaying strategies.
These findings have also allowed us to explore what travels in information literacy practice, including the idea that vaccine hesitancy is linked to poor information skills or a lack of agency. In turn, this focus has led us to suggest that vaccine-hesitant action cannot be fixed through increased or more widespread information literacy education, which typically centres positive and preparatory action rather than the challenges of liminal space. Findings from this study consequently have implications for official information literacy standards and guidelines as well as established approaches to information literacy education, such as informed learning [91]. What is perhaps of more importance, though, is the way in which findings from this study force us to confront complex questions about the less palatable side of information literacy, including how information skills can be leveraged for anti-social or morally unethical purposes linked to dark knowledge [98]. Constituting a new and emerging direction of study for information literacy, these ideas require bold further attention.
Future research should build upon these findings to examine the vaccine hesitancy spectrum in more detail, including in relation to vaccination refusers rather than merely the vaccine hesitant as well as more specifically, in relation to ethnic minority groups, who often demonstrate lower trust in health care due to structural and institutional racism, among other issues [99]. Approval of vaccinations for children means that research should additionally explore liminality and agency in relation to younger populations, other voices that have typically been under-represented within vaccine research. Research should further focus on public health applications, including how findings from this study can be used to develop interventions that have a basis in the dynamics of information activity rather than individual ignorance and prescriptive behaviour. A focused research approach would paint a far broader picture of informed relational agentic performance within liminal spaces as well as paving the way for the construction of reflexive and information-focused ways of engaging with public health issues.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the British Academy/Leverhulme, SRG2021\211338.