
Abstract
Increasing reports of racial microaggressions raise concerns about their impact on young adults’ mental health. Social support can act as a protective process in the association between racial microaggressions and mental health symptoms. In this article, we used an egocentric network approach to examine the extent to which network size and functions of support moderated the effect of racial microaggressions on anxiety among racialized and White young adults. Results from structural equation modeling indicated that a larger network size and support in the emotional, instrumental, and informational domains reduced the effect of racial microaggressions on anxiety for racialized participants. Findings have implications for supporting young adults who experience racial microaggressions and have reduced social supports.
Introduction
There is an increasing focus on racialized and migrant individuals’ experiences of racial microaggressions (subtle, covert acts of racism and discrimination targeting people of color or people from minoritized groups; Sue et al., 2007; Williams et al., 2021). Like racial discrimination (Pascoe & Smart Richman, 2009), racial microaggressions have been identified as a risk factor for mental health problems. Racist experiences are negatively associated with physical and mental health, exacerbate externalizing and delinquency problems, and undermine academic performance, both concurrently and over time (e.g., Benner et al., 2018; Cave et al., 2020; Civitillo et al., 2024). Such experiences may be particularly detrimental for the mental health of young adults or university students, who are already at high risk for mental health problems (e.g., Hoeflich et al., 2023). The COVID-19 pandemic resulted in increases in mental health symptoms, including anxiety, among young adults, and was marked by reductions in social networks and social supports (Elmer et al., 2020; Li et al., 2021). Social support, however, is a key process that can potentially mitigate the impact of these negative experiences on young adults’ mental health. In the present study, we sought to examine the extent to which social support moderated the impact of racial microaggressions on anxiety in young adults.
Racial Microaggressions and Mental Health
Sue et al. (2007) defined racial microaggressions as brief, everyday experiences of subtle aggression against people of color in nine areas of everyday interactions (e.g., assumptions of nativity, colorblindness). The construct of racial microaggressions has since been updated to include four superordinate categories (pathologizing differences, denigrating and pigeonholing, excluding and rendering invisible, perpetuating color-blind racial attitudes) and 16 areas of everyday interaction, highlighting the pervasiveness of these experiences in the lives of minoritized people (Spanierman et al., 2021; Williams, 2021; Williams et al., 2021). Microaggressions can take many forms, including verbal and nonverbal and may be intentional or unintentional, reflecting implicit or explicit bias or prejudice (Dovidio et al., 2018; Mekawi & Todd, 2021; Turner et al., 2021). Most research on racial microaggressions comes from qualitative studies with clinical populations, and quantitative studies with young adults and university students in North America. Findings indicate that up to 81% of Black people experience some form of racial microaggressions in their day-to-day life and up to 78% of Asian Americans report similar experiences within the past two weeks in the United States (Douds & Hout, 2020; Ong et al., 2013). Such experiences are associated with mental and physical health problems (Spanierman et al., 2021): depression, anxiety, and trauma symptoms (e.g., Auguste et al., 2021; Blume et al., 2012; Choi et al., 2022; Nadal et al., 2014), substance use (Blume et al., 2012; Ogunyemi et al., 2020), low self-esteem (Nadal et al., 2014), and increased worry about future employment (Salami et al., 2021). In a meta-analysis, Lui and Quezada (2019) reported that racial microaggressions were related to emotional problems, stress, negative emotionality and adjustment more so than physical health or externalizing problems. In comparison with Pascoe and Smart Richman’s (2009) findings on racial discrimination and adjustment outcomes, Lui and Quezada (2019) reported that racial microaggressions were associated with adjustment to the same degree as racial discrimination did in Pascoe and Smart Richman’s study. In addition to quantitative studies, qualitative research further demonstrates higher levels of mental health problems, including anxiety, stress, depression, and lower self-regard, among racialized women, and increased emotional, behavioral, academic problems and feelings of powerlessness among youth (e.g., Keels et al., 2017; Loyd et al., 2022; Sue et al., 2008).
These patterns align with the general strain theory and stress models (e.g., Agnew, 1992; Mays et al., 2007; Ong et al., 2009), which suggest that stressful events, including racial discrimination, can lead to poor mental health outcomes. In Canada, rates of racial microaggressions have been estimated between 50% and 94% in young adults in the past year (Cénat et al., 2022), and similar effects on mental health have been observed as in the United States, with higher levels of racial microaggressions associated with more anxiety, depression, and posttraumatic stress disorder (PTSD) symptoms, less belonging and adjustment, lower life satisfaction, and a reduced likelihood of seeking psychopharmacological mental health treatment (Cénat et al., 2022; Feng et al., 2023; Houshmand et al., 2014; Kogan et al., 2022).
Racial microaggressions can be particularly detrimental to the mental health of young adults as this age group is marked by significant school transitions into university and changes in social support networks (e.g., Wrzus et al., 2013). Around the globe, the prevalence of depression and suicide-related outcomes in university students is estimated at 21%, suggesting a significant mental health burden in this population (Sheldon et al., 2021). Rates of mental health problems were exacerbated during the COVID-19 pandemic (Patterson et al., 2021), reaching as high as 35% to 88% in some studies (e.g., Chirikov et al., 2020; Lee et al., 2021). Alongside depression, anxiety, and stress, loneliness, substance use, and disordered eating also increased during the pandemic (Ernst et al., 2022; Kim et al., 2021). In Canada, 39% of university students reported clinically significant levels of depressive and anxiety symptoms (Duffy et al., 2020). The added experience of negative racist events such as racial microaggressions or discrimination can further exacerbate mental health problems in this population (e.g., Auguste et al., 2021). Anxiety is often comorbid with other conditions, including depression and loneliness. Decades of research have demonstrated a comorbidity rate ranging between 20% - 70% for lifetime co-occurrence with anxiety, spanning subclinical symptoms to clinical disorder levels (e.g., Kalin, 2020). Individuals experiencing poor mental health, including anxiety, also tend to report greater loneliness and social isolation (e.g., Wang et al., 2018).
Emerging adulthood involves major educational/work transitions and changing support systems (e.g., Conley et al., 2014). During this time, support from family and schools often decreases, leaving youth more vulnerable to mental health and adjustment challenges (Ruberman, 2014; Wood et al., 2017). University students face distinct pressures: they consistently report higher stress and mental health difficulties compared with nonstudents (e.g., McCloud et al., 2023; Wiens et al., 2020), making them a critical population for study. Racialized youth experience additional challenges, including ongoing identity exploration and exposure to discrimination. Universities, while more diverse than high schools, can also present hostile environments. Notably, discrimination from professors often remains higher than discrimination from peers, with negative effects on academic outcomes, well-being, and mental health (Blume et al., 2012; Bravo et al., 2023; Castro et al., 2024; Cave et al., 2020; Del Toro & Hughes, 2020). Some racialized groups (i.e., Asian, Indigenous, Black) appear particularly affected, with teacher-perpetrated discrimination linked to elevated anxiety and stress (Bravo et al., 2023). Social networks can buffer these risks, supporting both academic success and mental health (Brouwer et al., 2022; Stadtfeld et al., 2019). However, transitions from high school often disrupt these networks, especially for international students (e.g., Sundqvist et al., 2024).
Racial Microaggressions and Social Support
Along with racial discrimination, poor social support is a risk factor for mental health problems in young adults (Sheldon et al., 2021). Social support refers to perceived or actual resources available within formal and informal relationships, such as family, friends, partners, coworkers, or acquaintances (e.g., Gottlieb & Bergen, 2010). Social support takes many forms, with instrumental, informational, or emotional functions being the focus of most psychological research (e.g., Gottlieb & Bergen, 2010). These involve helping or advising, providing material or other tangible assistance, or offering warmth and nurturance, respectively (Taylor, 2007). According to the stress buffering hypothesis, social support is a mechanism that people can draw from when dealing with stressors and can provide psychosocial benefits through psychological and material resources (Cohen, 2004). Social support, therefore, is often conceptualized as an adaptive coping strategy in the face of stress (Cohen, 2004; Thoits, 1995). The importance of social support in promoting positive mental health has been well-documented across studies, samples, and stressful experiences (e.g., Harandi et al., 2017).
For racial discrimination, however, research indicates mixed findings regarding the role of social support in reducing the negative impact of racial microaggressions on mental health and general functioning. Some researchers found that social support was not associated with reduced mental health problems when experiencing racial discrimination or microaggressions in racialized adults (e.g., Lemon et al., 2022). In other studies, social support has been found to have a buffering effect (e.g., Cénat et al., 2022; Lee & Waters, 2021), with findings varying depending on the levels of social support. For example, people who report low levels of social support were three times more likely to have physical symptoms (Jung et al., 2022) and more depression compared with those with higher levels of support (Lee & Waters, 2021). The positive role of social support in well-being when experiencing racial discrimination has been further supported by studies focusing on Asian groups during the COVID-19 pandemic (e.g., Lu & Wang, 2022). Collectively, these studies indicate that social support, although moderately associated with mental health when facing discrimination, can contribute to the well-being of victimized individuals.
Social Support From a Social Networks Approach
Social support has traditionally been measured with composite scores from questionnaires on the quality of support received from different sources (i.e., family, friends). A social network approach focuses on the structure and function of each relationship and can provide a more nuanced understanding of social support and its links to mental health (e.g., Kawachi & Berkman, 2001). Egocentric networks assess a focal individual’s unique and complete network. In this type of analysis, an individual indicates the number and function of people in their network without needing the total number of people available in the network (alters) to be present in specific contexts such as a classroom.
Network structure can be measured using relational and structural network indicators, such as density (i.e., interconnections among people in a network), components (i.e., subgroups), centrality (i.e., importance of nodes to the key individual; ego), homophily (i.e., similarity in some characteristic) and proximity of network members to the focal individual (ego) (Feng et al., 2024; Schwarzer & Leppin, 1991). Social network structure can also comprise size, which refers to the number of people in a network that comprise a person’s social network (e.g., Tiv et al., 2022), and function, which refers to the role of each relationship and the resources offered (e.g., Cofie et al., 2017).
These characteristics have been independently associated with different outcomes. A larger social network has been associated with less loneliness in young adults, whereas having fewer people to talk to about personal concerns, to ask for help, or to socialize with has been linked to more loneliness (Richardson et al., 2024). Network characteristics beyond size and structure can also affect mental health: university students whose network was composed of depressed individuals or individuals who engaged in substance use also reported more depression/loneliness or substance use (Amo et al., 2025; Russell et al., 2021). During COVID-19, several studies supported the importance of social network structure in university students’ mental health, such that students who reported depressive symptoms and loneliness perceived their networks to experience these as well (Amo et al., 2025). In contrast, an increased number of close contacts and a more interconnected network have been associated with lower levels of loneliness (Hopp et al., 2022; Richardson et al., 2024).
In the present study, we examined associations between racial microaggressions, anxiety, and social support using an egocentric network approach, focusing on respondents’ (egos’) reports of their social network size and function in eight different domains. Data collection took place in Fall 2021, a time during which Canadian universities transitioned to remote learning. Recent findings demonstrated that social networks and the number of connections among university students were reduced during COVID-19 (Smith et al., 2022), highlighting the risk of lack of social support and its impact on mental health. First, we examined the extent of group differences in rates of racial microaggressions and anxiety between White and racialized young adults. Second, we examined the extent to which social support, as indicated by social network size and function, moderated the impact of racial microaggressions on anxiety. Due to the intercorrelations between anxiety and depression and anxiety and loneliness, we controlled for these experiences in our current analyses.
Method
Participants
Participants were recruited from the University of Ottawa, Ontario, Canada from the university’s participant pool and through student associations. The survey was administered using an online survey platform (Qualtrics), and participants were eligible to receive course credit or enter a draw to win one of 20 US$50 gift certificates. There were 1,919 17- to 25-year-old (Mage = 19.22, SD = 1.62, 74% female) students recruited. Participants who failed more than 75% of the attention checks were removed from analyses, resulting in a final sample of 1,445 students (Mage = 19.12, SD = 1.54, 74.7% female). Regarding ethnicity, the final sample was comprised of 40.5% White students and 59.5% racialized students (15.4% Black, 13.8% Middle Eastern, 11.7% South Asian, 4.6% East and Southeast Asian, 3.0%, Hispanic/Latine, 1.6% Indigenous, 5.1% Multiracial, and 4.6% indicating other). This study was approved by the Research Ethics Board Committee at the University of Ottawa in 2021 (H-06-21-7101REG-710).
Measures
Racial Microaggressions
Racial microaggressions were assessed using the Racial Microaggressions Scale (RMAS; Torres-Harding et al., 2012), which includes 32 items on microinsults and microinvalidations in the following domains: alien in own land, ascription of intelligence, colorblindness, criminality, invalidation of interethnic differences, exoticized, myth of meritocracy, pathologizing cultural values and communication styles, second-class citizenship, environmental invalidations, and invisibility (e.g., “Because of my race, other people assume that I am a foreigner”). Items were rated on a 4-point Likert-type scale (0 = not at all, 3 = high level), which were averaged into one total score for analyses. Scale reliability was estimated at α = .96.
Depression
Depression, assessed along with loneliness and anxiety, was used as outcomes in the analyses. Depression was assessed using the Center for Epidemiologic Studies Depression Scale (CES-D-10; Radloff, 1977; Zhang et al., 2012), which is rated on a 4-point Likert-type scale (0 = Rarely or some of the time, 3 = Most or all of the time). An average score was calculated for analysis (α = .85).
Loneliness
Loneliness was assessed using the six-item UCLA Loneliness Scale (Russell et al., 1980), which was rated on a 4-point Likert-type scale (0 = never, 3 = often; α = .85).
Anxiety
Anxiety was assessed using the Generalized Anxiety Disorder-7 items (GAD-7; Löwe et al., 2008; Spitzer et al., 2006). The GAD-7 is rated on a 4-point Likert-type scale (0 = not at all, 3 = nearly every day). A total score was calculated by averaging all items (α = .90).
Egocentric Networks
An egocentric or personal network approach (Perry et al., 2018) measures the size and functions of participants’ (ego) relationships with members of their network. We selected this form of social analysis because it allows for anonymity and can yield complete information on each individual’s unique social network structure. Instructions were adapted from Vehovar et al. (2008) and Smith (2002). First, a name generator was used to elicit the names of people in one’s network, and second, a name interpreter was used to link each member of the network to specific relational functions. That is, participants were first asked to enter the names of up to 24 people in their network, and these included people they interact with at their current school and outside of school (e.g., people they know from their childhood, neighborhood, and community centers). Then, each name appeared in a drop-down list, and participants were asked to indicate which of the social support functions were fulfilled by that person. Participants were also asked to indicate the demographic characteristic of each member in their network (e.g., age, race/ethnicity).
Eight categories of social support function were assessed: intimate disclosure (e.g., telling secrets), companionship (e.g., hanging out), instrumental aid (e.g., getting help), self-validation (e.g., feeling sure of yourself), emotional security (e.g., feeling better if anxious), youth culture (e.g., talking about youth culture), academic support (e.g., school help, future aspirations), and caring (e.g., feeling loved). These items were adapted from the Network of Relationships Questionnaire (Buhrmester & Furman, 2008), the McGill Friendship Quality Scale (Mendelson & Aboud, 1999) and the Longitudinal Student Immigrant Adaptation Study (Suárez-Orozco et al., 2008). For each category, the participants could have nominated up to three people in their network. On average, participants listed between 2.47 and 2.88 people across all of the categories (with the full range of 0–3).
Analytic Plan
Structural equation modeling with Full Information Maximum Likelihood in Mplus, version 8.11 (Muthén & Muthén, 2012) was used to examine and control for the associations between each outcome variable (loneliness, depression, and anxiety). We then tested the effects of racial microaggressions on each outcome simultaneously, accounting for their shared associations. Given the lack of normality in the outcomes and the measure of racial microaggressions, robust maximum likelihood estimation was used. Models were considered acceptable if the χ2 statistic was not significant, comparative fit index (CFI) ⩾ .90, root mean square error of approximation (RMSEA) ⩽ .06, and standardized root mean square residual (SRMR) ⩽ .08 (Kline, 2016). Next, the potential moderating impact of the eight social support functions from the egocentric network variables were tested separately (see Figure 1). Finally, the analyses were split between White and racialized participants to elucidate group differences in the associations (based on significant decreases to the χ2 statistic).
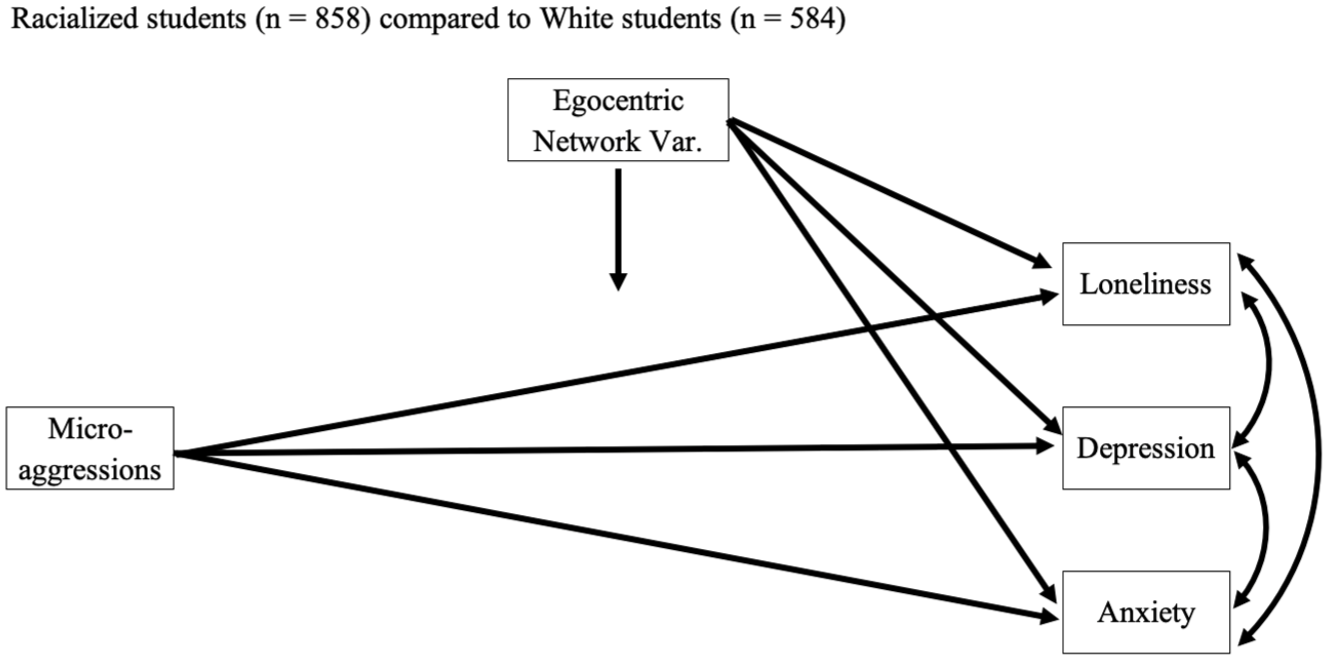
Conceptual Model of the Tested Associations in the Current Study.
Results
Descriptive analyses indicated that racialized participants (M = 1.04, SD = 0.67) experienced higher levels of racial microaggressions than White participants, M = 0.28, SD = 0.38; t(1,397.23) = 27.62, p ⩽ .05. The two groups did not differ significantly on anxiety levels, but White participants scored lower on loneliness, M = 2.30, SD = 0.78; t(1,208) = 3.85, p ⩽ .05, and depression, M = 1.24, SD = 0.65; t(1,288.20) = 2.43, p ⩽ .05, compared with racialized participants, M = 2.46, SD = 0.78, and M = 1.33, SD = 0.68, respectively.
Meanwhile, the average network size ranged from 0 to 24 people and was higher for White (M = 22.42, SD = 3.91) than for racialized (M = 21.64, SD = 4.45) participants, t(1,353.63) = 3.49, p ⩽ .001. Correlations between racial microaggressions and each outcome were positive and statistically significant (r’s = .21–.31). Correlations between all of the student variables are presented in Table 1.
Correlations Between Study Variables for Racialized (n = 858) and White (n = 584) Participants.
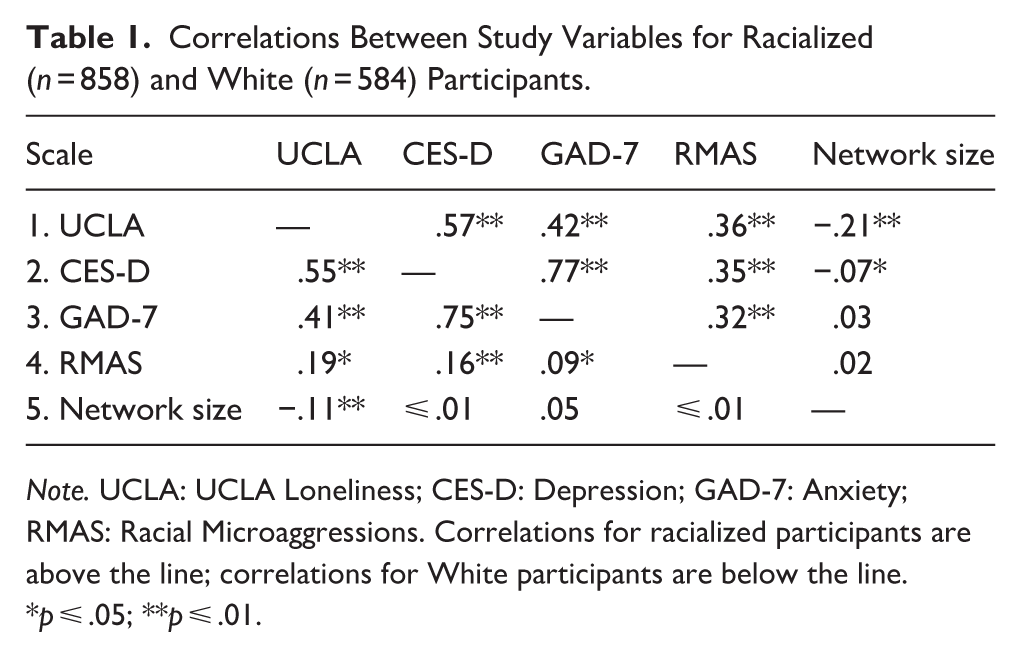
Note. UCLA: UCLA Loneliness; CES-D: Depression; GAD-7: Anxiety; RMAS: Racial Microaggressions. Correlations for racialized participants are above the line; correlations for White participants are below the line.
p ⩽ .05; **p ⩽ .01.
Hypothesis testing began by correlating the outcomes to each other. We assessed the effect of racial microaggressions on each outcome, above and beyond their shared associations. As expected, reports of racial microaggressions were positively related to loneliness (β = .31, z = 12.95, p ⩽ .01), depression (β = .28, z = 11.44, p ⩽ .01), and anxiety (β = .21, z = 8.32, p ⩽ .01). Students who perceived having been the victim of racial microaggressions were more likely to report feeling simultaneously lonely, depressed, and anxious. Racial microaggressions accounted for 9.50%, 7.70%, and 4.60% of the variability in loneliness, depression, and anxiety, respectively.
We tested the main effect of the egocentric network variables (examining each variable separately). A number of main effects emerged. As depicted in Table 2, each egocentric network variable was associated with lower loneliness (β’s = −.08 to −.17, p ⩽ .01). Moreover, academic support and caring were linked to lower depression (β = −.06 and −.05, p ⩽ .05, respectively). One additional unexpected association was observed. The number of people in a network that participants can talk to about their secrets was positively related to anxiety (β = .08, z = 2.89, p ⩽ .05). This indicates that individuals who reported having more people to discuss their private feelings and things they do not want others to know were more likely to report more anxiety, explaining an additional .60% of the variability in anxiety.
Main Effects of Egocentric Network Variables (β Values) on Each Outcome.
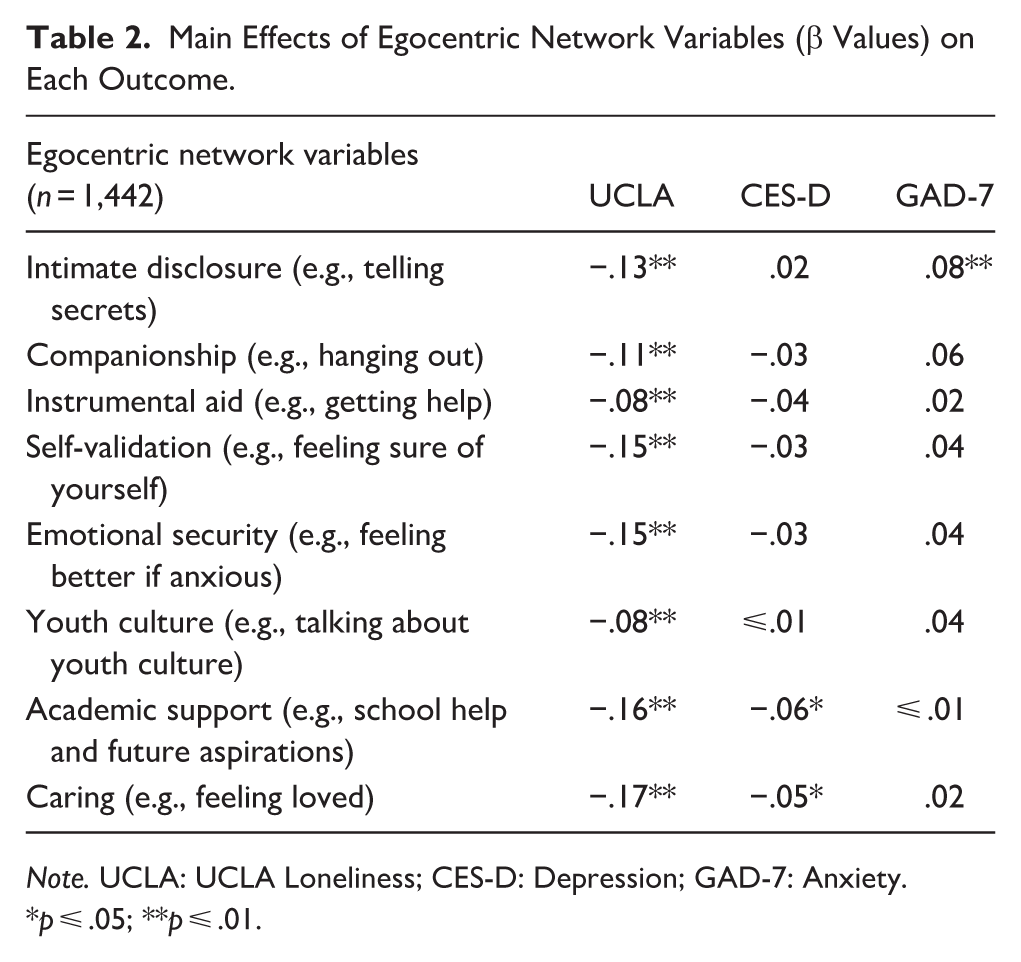
Note. UCLA: UCLA Loneliness; CES-D: Depression; GAD-7: Anxiety.
p ⩽ .05; **p ⩽ .01.
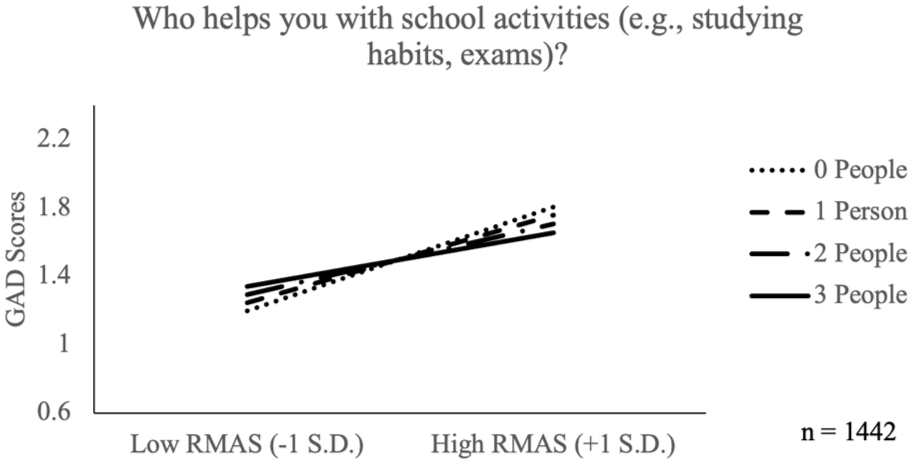
The potential two-way interactions between racial microaggressions and each of the egocentric network variables were explored next. No moderating effect of the egocentric variables on racial microaggressions were found for loneliness. However, two moderating effects of the number of reported people in the network emerged for racial microaggressions on depression. Specifically, those who nominated more people in their network had a buffered effect of racial microaggressions on depression when seeking support for: youth culture (ΔR2 = .30%) and instrumental aid (ΔR2 = .20%). Finally, moderating effects of the number of people in their network were revealed for racial microaggressions on anxiety as well. Namely, those who nominated more people in their network had a buffered effect of racial microaggressions on anxiety when seeking support for: caring (ΔR2 = .30%), instrumental aid (ΔR2 = .30%), companionship (ΔR2 = .20%), emotional security (ΔR2 = .20%), youth culture (ΔR2 = .20%), and intimate disclosure (ΔR2 = .20%). For example, Figures 2 and 3 illustrate how the effect of racial microaggressions were weaker among participants who reported more people who provide instrumental aid on depression and anxiety.
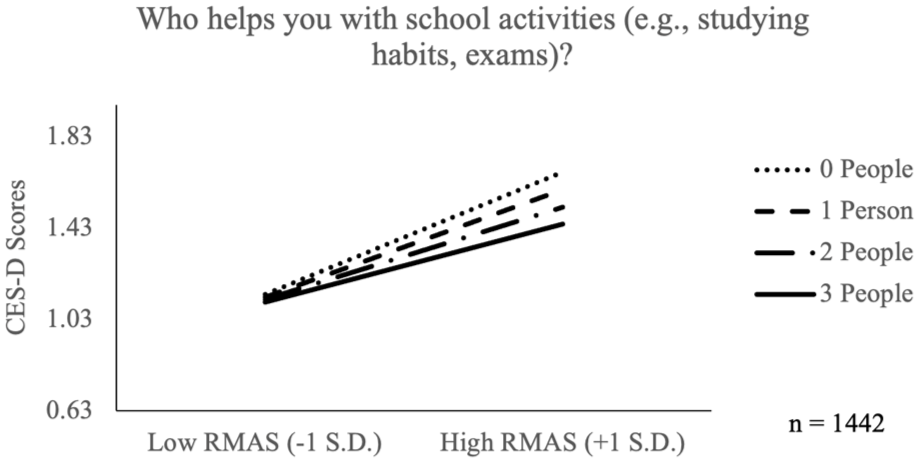
Racial Microaggressions as a Function of Number of People in One’s Network Who Provide Instrumental Aid on Depression. The y-axis has been truncated to highlight the effects (±1SD around the mean). CES-D: Depression. RMAS: Racial Microaggressions.
Racial Microaggressions as a Function of Number of People in One’s Network Who Provide Instrumental Aid on Anxiety. The y-axis has been truncated to highlight the effects (±1SD around the mean). GAD-7: Anxiety; RMAS: Racial Microaggressions.
Finally, we tested whether the main effect of racial microaggressions, the egocentric network variables and their interactions varied between racialized and White participants. To accomplish this, we split models by group and then constrained each of the effects one at a time to see if model fit decreased significantly. A number of differences between the groups emerged. Namely, the moderating effect of emotional security on the effect of microaggressions for both depression and anxiety scores differed between White and racialized students. As depicted in Figures 4 and 5, the buffering was more pronounced among racialized students, R2(depression) = 12.40%, R2(anxiety) = 10.40%, compared with White students, R2(depression) = 4.80%, R2(anxiety) = 2.20%. The final model was a good fit to the data, χ2(6) = 4.06, p > .05; CFI = 1.00; RMSEA = .02, 90% CI [.00, .04]; SRMR = .01.
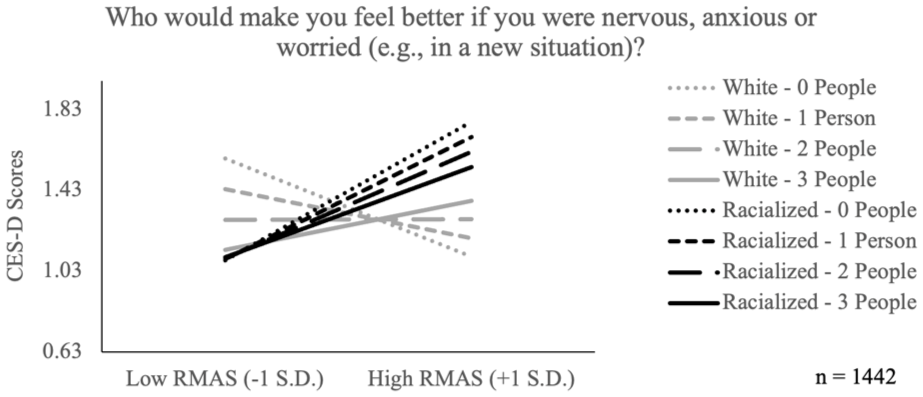
Racial Microaggressions as a Function of Number of People in One’s Network Who Provide Emotional Security on Depression Among White and Racialized Students. The y-axis has been truncated to highlight the effects (±1SD around the mean). CES-D: Depression. RMAS: Racial Microaggressions.
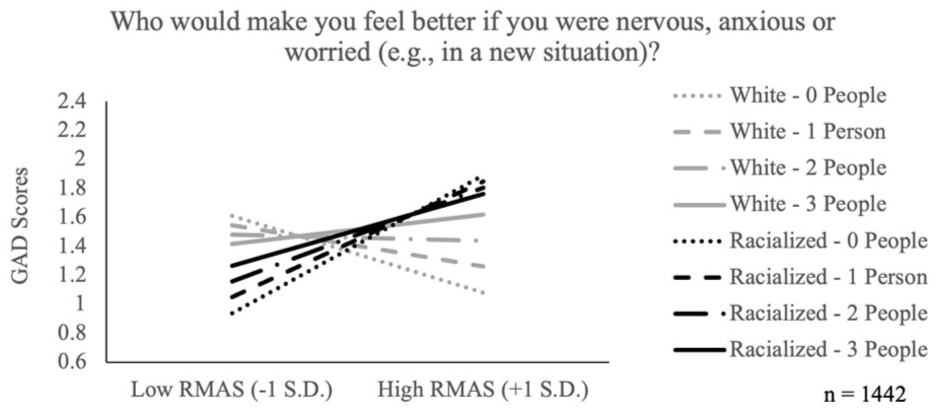
Racial Microaggressions as a Function of Number of People in One’s Network Who Provide Emotional Security on Anxiety Among White and Racialized Students. The y-axis has been truncated to highlight the effects (±1SD around the mean). GAD: Anxiety; RMAS: Racial Microaggressions.
Moreover, the moderating effect of youth culture on the effect of microaggressions for both depression and anxiety scores differed between White and racialized students. As depicted in Figures 6 and 7, the buffering was more pronounced among racialized students, R2(depression) = 12.50%, R2(anxiety) = 10.60%, compared with White students, R2(depression) = 2.90%, R2(anxiety) = 1.39%. The final model was a good fit to the data, χ2(6) = 12.92, p > .05; CFI = .99; RMSEA = .03, 90% C.I. [.00, .06]; SRMR = .01. Otherwise, all other effects between the groups were able to be fixed to be the same without any deterioration in the model fits.
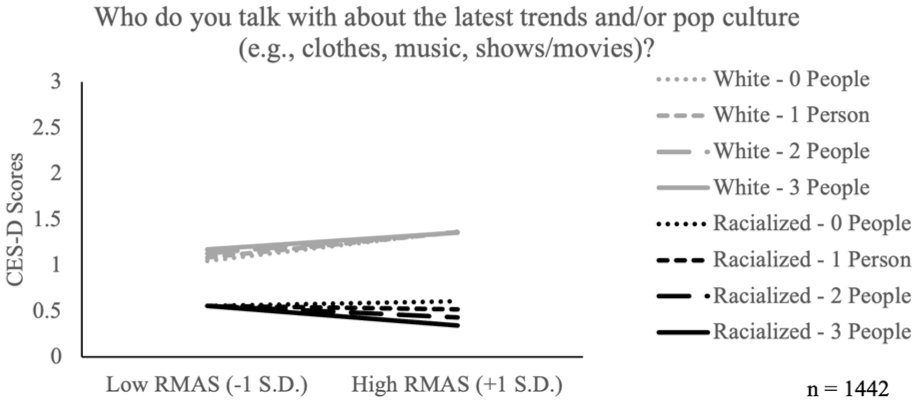
Racial Microaggressions as a Function of Number of People in One’s Network to Talk About Youth Culture on Depression Among White and Racialized Students. CES-D: Depression. RMAS: Racial Microaggressions.
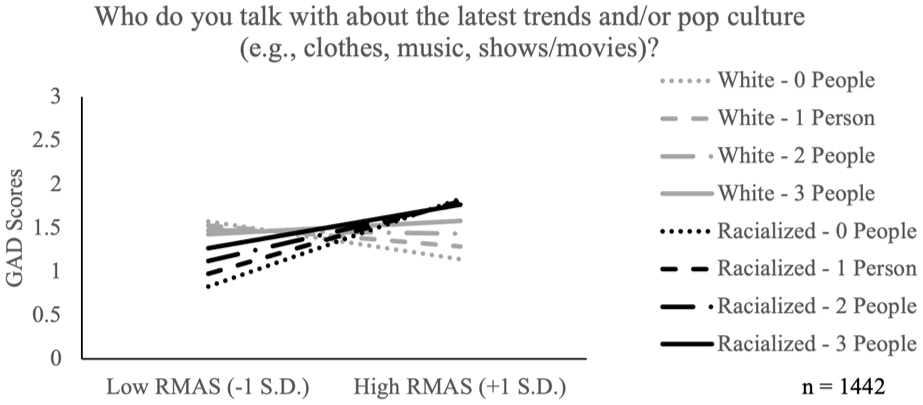
Racial Microaggressions as a Function of Number of People in One’s Network to Talk About Youth Culture on Anxiety Among White and Racialized Students. GAD-7: Anxiety; RMAS: Racial Microaggressions.
Discussion
We examined associations between racial microaggressions, anxiety, and social support in a sample of Canadian university students, using an egocentric (personal) network approach to assess social support. Increased levels of racial microaggressions predicted more anxiety, as well as more loneliness and depression (included in this study as covariates). Our main findings indicated that a larger social network size across different domains of social support (e.g., feeling better, disclosing secrets, and feeling loved) was associated with lower levels of anxiety when experiencing racial microaggressions. This effect, as expected, was more pronounced among racialized participants.
Consistent with an emerging literature on racial microaggressions, our results demonstrated that higher levels of racial microaggressions predicted worse mental health problems. In prior research, mental health has been found to range from nonclinical symptoms to clinical levels, and included primarily depression, anxiety, and trauma (Choi et al., 2022; Williams et al., 2018). Similarly, in our study, racial microaggressions predicted higher levels of depression, anxiety, and loneliness. We did, however, find that network size and function of social support moderated the association between racial microaggressions and anxiety, while controlling for depression and loneliness. These findings align with the stress-buffering hypothesis (e.g., Kawachi & Berkman, 2001), suggesting that social support can offer a buffering effect when facing stress—in this case, racial microaggressions. Similar findings have been reported in other studies, which indicated that network density and network structure are positively associated with well-being (Lee et al., 2018; Lin et al., 2019).
One of the strengths of our study was the assessment of social network size and social support functions across different domains. Our study is among the first to examine associations between racial microaggressions and anxiety using an egocentric network approach for social support. Prior research with young adults has examined social networks in relation to substance use, depression, loneliness, and exercise (Amo et al., 2025; Patterson et al., 2021; Pokhrel et al., 2016; Richardson et al., 2024; Russell et al., 2021; Tiv et al., 2022), and other research has focused on health outcomes (e.g., Cheyne et al., 2021; Messer et al., 2020) and clinical samples for mental health outcomes (Fullana et al., 2021; Wyngaerden et al., 2019, 2022). We found that the size of network mattered in the association between racial microaggressions and anxiety, a finding that has found mixed support in prior studies. Our results are in line with Carmichael et al.’s (2015) study in which a larger social network in early adulthood matters more than quality of relationships. Developmentally, the social network size also seems to peak in mid-20s (Wrzus et al., 2013), which is the age group of our sample. As such, this is an important consideration to address in efforts to improve young adults’ mental health, particularly for those who have small networks.
In addition to network size, it is important to contextualize our findings within the broader literature of social relatedness, self-efficacy, and social support, as these processes can bolster a person’s fundamental need to belong and ability to cope with stressors through their access to social resources (e.g., Baumeister & Leary, 1995; DeLongis et al., 1988). According to the enabling hypothesis, individuals drawing support from their networks have the opportunity to model behaviors that can contribute to their well-being and to overcoming adversity (Korth et al., 2025; Schwarzer & Knoll, 2007). It may also be the case that individuals with larger networks have greater self-efficacy in the domain of social relationships and greater ability to reach out to obtain social support in stressful situations (Benight & Bandura, 2004). Therefore, participants’ capacity to draw social support from their social network is an adaptive social cognitive process.
Limitations and Future Directions
The main limitations of our study pertain to the cross-sectional nature of the data and the use of a young adult sample from a single site. Our sample consists exclusively of university students, who may differ in social, economic, and mental health characteristics from nonstudents or youth not pursuing postsecondary education. As a result, the findings may not fully generalize to all emerging adults, and caution is warranted when extending conclusions to other populations. Nonetheless, nonstudent young adults experience the same developmental transitions, and transitions to work environments, which potentially pose similar risks. Future work should focus on longitudinal associations and trajectories of racial microaggressions, social support, and mental health over time. This approach will contribute a deeper understanding of the temporal relationships among these processes, particularly in at-risk populations for mental health problems. Given the correlational nature of the data, it was not possible to establish a causal relationship; thus, it remains unclear whether having people with whom to share very private feelings and secrets leads to increased anxiety, or if individuals with higher anxiety levels tend to seek out more people with whom to discuss such private feelings.
The examination of these associations would benefit from a broader sample of adults, as well as adolescents, focusing on the transition from secondary to postsecondary school—a developmental transition marked by increased levels of mental health problems among youth. These patterns should be replicated with adolescents to better understand their early experiences with racial microaggressions and the potential buffering effect of different types of social support. Our findings are particularly relevant to universities and educational institutions for providing stronger supports that can contribute to students’ mental health, academic achievement, resilience and coping strategies. The egocentric network approach used in this study allowed us to examine the number and functions of different sources of support, which provides a more fulsome understanding of social networks compared with general self-report measures of social support. This approach provides a nuanced understanding of network size and social capital that can inform interventions in the area of health and well-being for marginalized populations. Future measurements of social support should include the assessment of tailored support for racial microaggressions or discrimination (e.g., who do you talk to when you feel discriminated against). In this study, we assessed general functions of social support, which is critical in our understanding of the general ways in which social support might protect against heightened anxiety. There is, however, limited evidence indicating that social support tailored to address issues relevant to racial stress and discrimination is more effective in protecting mental health than general forms of social support (Seawell et al., 2014). Future research should also consider who the perpetrators of racial microaggressions are, how they are connected to a person’s social networks and hinder social support, potentially leading to more anxiety and other mental health problems.
Conclusion
Our study adds to an emerging literature highlighting the impact of racial microaggressions on young adults’ mental health, particularly among those in university settings. Using an egocentric network approach, our findings show that larger social network sizes and specific functions of social support (e.g., emotional, intimate disclosure) can help buffer the negative effects of racial microaggressions on anxiety, with stronger effects among racialized participants. Our results align with the stress-buffering hypothesis, which suggests that social support is an important protective factor against mental health impacts in stressful experiences.
Footnotes
Acknowledgements
The research team thanks all research assistants, volunteers, and participants on this study.
Ethical Considerations
This research had ethical approval from the University of Ottawa (H-06-21-7101—REG-710).
Consent to Participate
All participants provided informed consent prior to completion of the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Seed Funding Opportunity, Faculty of Social Sciences, University of Ottawa Grant awarded to Dr Vitoroulis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The corresponding author can provide additional results if requested. Data not available due to ethics restrictions.