
Abstract
The COVID-19 pandemic posed significant risks to children, yet there is little longitudinal research on children’s coping during this period. The current study used data from the Child Resilience and Managing Pandemic Emotional Distress (CRAMPED) Families project, a longitudinal study of 1,096 children nested within 548 families across seven timepoints from May 2020 to October 2022. We examined trajectories of child coping over 2.5 years of the pandemic and associations with COVID-19 stress, positive family adaptation, and caregiver social support. Multilevel modeling revealed a curvilinear trend of child coping, with an increase in coping in early months followed by declines over time, suggestive of allostatic load. Higher COVID-19 stress was negatively associated with coping, whereas higher family adaptation and caregiver social support were positively associated with coping. Social support buffered the association between COVID-19 stress and child coping. Despite the transition toward a “post-pandemic” society, continued focus on children’s long-term adjustment is warranted. Family-level supports appear crucial for promoting coping, and while caregiver’s social support is protective against stress, mobilization of additional resources (e.g., government, community) beyond the caregiver’s network may be necessary to promote healthy coping.
Introduction
In May 2023, the COVID-19 pandemic was officially declared no longer a global public health emergency by the World Health Organization. However, the long-term consequences of the pandemic are only now beginning to be understood. Since the initial outbreak, COVID-19 research has shifted from a focus on urgent needs (e.g., vaccines, resource scarcity) toward the more enduring psychosocial effects, including on mental health, learning gaps, and social challenges. These consequences are associated with pandemic-related adversities, such as death of loved ones, family violence, school closures, social isolation, and countless other disruptions across children’s ecological systems (Fong & Iarocci, 2020). Consistent with long-standing evidence of maladaptive outcomes following collective stress and trauma, the COVID-19 pandemic has been associated with decreased wellbeing of children, underscoring the need for strategies that foster resilience (Masten, 2021; Patrick et al., 2020). Data from cross-sectional studies suggest that depression and anxiety rates among children during the pandemic were about two times greater than pre-pandemic levels (Racine et al., 2021). COVID-19 and related mitigation strategies (e.g., school closures) have also been linked to increased sleep problems, more behavioral and conduct problems, and decreased health behaviors (e.g., physical activity) among children (Lebrun-Harris et al., 2022; Viner et al., 2022). Moreover, systematic review data highlight that the social isolation brought on by COVID-19 is associated with both worsening mental health and reduced access to services, which together create unmet health needs for vulnerable children and youth (Viner et al., 2022).
Despite the deleterious impacts of COVID-19 on child wellbeing, research in this area remains somewhat sparse, with child-focused research comprising only about 8% of initial pandemic studies (Racine et al., 2022). Even fewer of these explorations have been longitudinal or extended beyond the second pandemic year (Korczak et al., 2024), leaving a gap in our understanding of children’s long-term adjustment (Wolf & Schmitz, 2024). Existing longitudinal data emphasize the need for ongoing monitoring both to better understand the far-reaching impacts of the pandemic and to implement necessary supports to prevent additional declines in wellbeing (Larsen et al., 2023; Wade et al., 2020; Wolf & Schmitz, 2024). Moreover, considering the cumulative impact of stress and adversity over time, longitudinal explorations of child outcomes beyond the acute stage of the pandemic are crucial for understanding how best to support children in the aftermath of collective stress (Evans et al., 2013; Holmes, 2013; Wade et al., 2023).
Promisingly, even with the established risk that COVID-19 has posed for children and youth, there is emerging data suggestive of recovery and adaptation (Chen & Bonanno, 2020; Finegold et al., 2023; Overall et al., 2022). This potential to withstand and/or rebound from the impacts of such risks has been seen both historically following collective disruptions (i.e., natural disasters) and within the context of COVID-19. Meta-analytic data suggests that individuals exposed to disasters or pandemics initially showed elevated post-traumatic stress symptoms (PTSS), but these gradually reduced across the 24 months following the stressor (Newnham et al., 2022). In addition, in a review of high-quality studies from 2020 to 2021, Aknin and colleagues (2022) demonstrated that, while levels of psychological distress increased significantly in the general population in the early months of the COVID-19 pandemic, by mid-2020, those levels had returned to baseline in most studies.
Despite some evidence for the capacity to recover and adapt, most extant literature exploring the psychosocial impact of COVID-19 centers on psychopathology (e.g., depression, anxiety, PTSS; Aknin et al., 2022; Eales et al., 2021; Fong & Iarocci, 2020; Larsen et al., 2023; Racine et al., 2021). While these data are immensely valuable, solely investigating the presence or absence of mental health problems does not provide a comprehensive picture of child wellbeing. Instead, investigating internal coping resources that help children recover from pandemic disruption shifts the focus away from merely describing children’s problems toward a perspective that considers psychological sources of strength and adaptation (Masten, 2025). In the present study, we operationalize our outcome variable of child coping as a set of traits and abilities (e.g., distress tolerance, persistence) that facilitate recovery and promote wellbeing in the face of adversity (Connor & Zhang, 2006). This operationalization reflects but one component of a larger concept of child resilience, a developmental and dynamic process that extends to numerous biological, psychological, social, and ecological systems that interact to facilitate children’s successful adaptation and recovery, maintain their wellbeing, or enhance their mental health when faced with significant cumulative risk (Goldstein & Brooks, 2023; Kumpfer et al., 2002; Masten & Coatsworth, 1998; Ungar & Theron, 2020).
While extant research highlights the importance of child coping during COVID-19 (Domínguez-Álvarez et al., 2020; Olsavsky et al., 2024), it is less clear how coping (e.g., humor in the face of adversity, a growth-mind-set) has fared longitudinally during this period. Understanding child coping trajectories, and the factors that promote or hinder them across the COVID-19 pandemic, may help to inform treatment targets that yield the largest returns. This is because child coping is not only associated with reduced psychopathology but also with feelings of hope, belonging, and lower suicidal ideation (Stark et al., 2022). Considering child coping may have broad-scale benefits for wellbeing in a number of areas, the first aim of the current study is to examine children’s coping abilities from May 2020 to October 2022.
In addition to examining longitudinal trajectories of child coping, we take a family systems approach to examine risk and resilience factors that may relate to coping over time. A family systems approach is necessary because neither risk nor resilience can be solely examined at the individual level. For children, the family—and how the family system interacts with other ecological levels (e.g., family income stress due to government lockdown policies, school closures impacting child care arrangements, etc.)—is particularly important in understanding trajectories of coping during the pandemic, as this was their most proximal ecological system at the time given the confinement that COVID-19 imposed.
This family systems perspective in the context of the pandemic is perhaps best captured by the COVD-19 Family Disruption Model (Prime et al., 2020). This model theorizes that distal pandemic-related adversities (e.g., social isolation, economic strain) may bear on children’s wellbeing in a cascading fashion, with social disruptions permeating the family unit and impacting the health and wellbeing of caregivers, who in turn funnel these risks to their children through alterations in family climate, routine, values, and behavior. This model has been validated in a systematic review that highlights bidirectional pathways between family and child functioning during COVID-19 for children of ages 2–18 years (Shoychet et al., 2023).
To employ a family systems approach, the current study considers family risk and resilience factors that could explain the mixed evidence of child wellbeing in the context of COVID-19. This is important as some research suggests increased child psychological distress during the pandemic (Racine et al., 2021; Viner et al., 2022), and other evidence suggests resistance to, or recovery from, pandemic disruption (Chen & Bonanno, 2020; Finegold et at., 2024; Newnham et al., 2022). The pattern and trajectory of children’s coping during this time is likely shaped by many factors, including families’ experiences of pandemic stress. For example, child coping abilities may be depleted in response to demands on capacity imbued by family-level pandemic stressors, such as a caregiver’s job loss or family member death (Masten & Motti-Stefanidi, 2020). Extant literature shows that higher levels of pandemic-related stress experienced by families is associated with an initial reduction of child wellbeing, as measured in the Spring of 2020 (Brown et al., 2020; Gassman-Pines et al., 2020). This pattern, mainly observed in the early months of COVID-19, may persist over time, suggesting that stress experienced by families during the pandemic may also deplete children’s coping abilities over time. Therefore, the second aim of the current study is to examine how pandemic-related stress is associated with child coping over 2.5 years of the pandemic.
While the transmission of stress across the family system is commonly observed, it is not necessarily deterministic of negative outcomes, with opportunities for positive family adaptation that supports child resilience (Eales et al., 2021). Just as coping can be undermined by demands on capacity, it can be enhanced through “activation” (e.g., motivation gleaned from a challenge) or increased resources (e.g., more time with responsive caregivers; Masten & Motti-Stefanidi, 2020). For example, one study during the pandemic found that, while caregivers experienced declines in their psychological and physical health over 1.5 years of the pandemic, caregiver-child relationship quality and parenting practices remained stable, introducing the possibility that some aspects of family wellbeing may be preserved even while others are undermined (Overall et al., 2022). Possible protective factors include more parent-child conversations about emotions and stable routines (Cohodes et al., 2021), dimensions of family function that may be maintained even when caregiver stress is elevated. In addition, pandemic-related play (e.g., pretend virtual school roleplay) has been demonstrated and replicated across socioeconomic status to relate to reduced child psychopathology (Rueda-Posada et al., 2023; Thibodeau-Nielsen et al., 2021). Taken together, these studies of promotive and protective processes (Ungar and Theron, 2020) suggest that a family’s ability to adapt positively in the context of COVID-19 challenges (e.g., new family activities, more quality time, adapted routines) may be sufficient to sustain or improve child coping over time (Prime et al., 2020). Considering this evidence, the third aim of the current study was to examine how positive family adaptation (PFA) is associated with child coping over 2.5 years of the pandemic.
Finally, identifying factors that may buffer against pandemic stress and/or enhance PFA is important as we shift to long-term recovery promotion and future disaster planning. Social support—individual’s access to the resources provided by the people and relationships in their network (Cohen & Syme, 1985)—is a central facilitator of coping that has been widely associated with family and child wellbeing (Bauer et al., 2021; Hatch et al., 2020). Within resilience frameworks, social support is often conceptualized as compensatory, having a direct and beneficial association with the outcome, independent of the effect of the risk factor (Fergus & Zimmerman, 2005). For example, in the context of COVID-19, higher social support is linked to reduced burnout and mental health problems in adults (Choi et al., 2023; Moisoglou et al., 2024). Beyond compensatory effects, social support may also operate as a protective factor, defined by Fergus and Zimmerman (2005) as a variable that interacts with the risk, moderating or attenuating its negative effects. For children, the social support afforded to caregivers may be especially important in offsetting the impact of pandemic-related stress on their coping abilities. However, research examining the extent to which caregivers’ social support either buffers the effect of pandemic stress or amplifies the positive effect of PFA on children’s coping has been largely unexplored. Thus, the fourth aim of the current study is to examine caregiver’s perceived social support as a moderator of the association between COVID-19 stress and PFA on trajectories of children’s coping.
To contextualize these explorations, it is useful to consider COVID-19 not only as an unprecedented health emergency but also as a period characterized by shared and unique risk and resilience factors that bear on development. Specifically, while COVID-19 presents distinct features (e.g., global simultaneity, mandated and protracted disease mitigation efforts), it also shares core attributes with other well studied adversities (e.g., mass violence, hurricanes, institutional poverty). These attributes include imposed loss and devastation, a wide-reach, disruption to safety and daily living routines, secondary stressors, and an indeterminate endpoint, placing the pandemic at the intersection of collective trauma and chronic stress (Rose Garfin & Estes, 2024). This hybrid classification suggests that children’s responses may span both acute trauma reactions and adaptations to prolonged strain across ecological systems (Prime et al., 2020). Thus, situating COVID-19 within this dual classification allows us to link observed patterns to broader risk and resilience theory (e.g., Fergus & Zimmerman, 2005; Masten & Coatsworth, 1998) and, in doing so, identify relevant policy levers, such as income stabilization, accessible caregiver supports, and the protection of family routines that may buffer risk and promote recovery (Last et al., 2024; Masten, 2025; Prime et al., 2023).
The current study seeks to provide longitudinal evidence on child coping in the context of COVID-19, while situating children’s wellbeing in a family systems model to examine risk and resilience factors related to child coping over time. We first explore longitudinal trajectories of child coping across the 2.5 years following WHO’s declaration of the global pandemic. We then examine the contributions of caregiver-reported COVID-19 stress and PFA on child coping over time. Finally, we examine whether caregivers’ perceptions of social support buffer the putative associations between COVID-19 stress and child coping and/or amplify the putative benefit of PFA on coping. In doing so, we control for various sociodemographic factors known to correlate with child wellbeing and family functioning. Consistent with patterns outlined by Wade et al. (2020), we expected to observe an overall decline in child coping over time. However, we further predicted that this coping trajectory would be associated with families’ pandemic experiences, with greater COVID-19 stress related to decreased child coping over time, and greater PFA related to increased child coping (or less of a decline) over time. Finally, we hypothesized that caregiver social support would buffer the association between stress and child coping, and that social support would bolster the association between PFA and child coping.
Method
Participants and Study Design
The current preregistered study (https://osf.io/vrs48/) is part of the Child Resilience and Managing Pandemic Emotional Distress (CRAMPED) Families project. CRAMPED is a multi-national, seven-wave investigation of 1,098 children nested within 549 families (two siblings per family) approved by the Research Ethics Board of the University of Toronto and Waterloo University (REB code: 42112). Participants for the current study include 548 caregivers and 1,096 children who provided data on the variables of interest. One family had complete missing child coping data and was therefore removed at the outset.
In CRAMPED, families with at least two children were recruited via Prolific®. Participants were surveyed seven times from May 2020 to October 2022 (T1: May–June 2020, T2: July 2020, T3: September 2020, T4: November 2020, T5: September–October 2021, T6: January–February 2022, T7: September–October 2022). As described in existing CRAMPED publications (e.g., Prime et al., 2022), participants came from the UK (76%), the USA (19%), Canada (4%), and Australia (1%). Most families had caregivers who were married (90%), full-time workers (52%), White-European (73%), and with some post-secondary education (69%). Household income in 2019 ranged from <$15,000 to ⩾$175,000 USD (median = $50,000 to $74,999 USD). In the current sample, most caregivers were citizens (93.8%), identified as female (67.7%), and were 24 to 62 years of age (M = 41.34; SD = 6.32). Child ages ranged from 4.42 to 19.3 years (M = 10.71, SD = 3.44), and approximately half of the children were identified by their caregivers as boys (51.7%).
Measures
Pandemic Stress. Caregivers reported on their family’s experience of pandemic stress using the COVID-19 Family Stressor Scale (CoFaSS), which was previously validated in this same sample (Prime et al., 2021). The measure includes 16 items that capture COVID-19 related stress faced by caregivers. Specifically, it captures 7 items on family stressors (e.g., increased altercations with family members), 5 items of financial stressors (e.g., job disruption), and 4 items of pandemic-specific stressors (e.g., could not access essential supplies). The CoFaSS also provides a summed total stress scale. All CoFaSS scales have acceptable psychometric properties as demonstrated via a robust factor structure, strong internal consistency (α = 0.83), measurement invariance across genders, and bivariate correlations with relevant variables (Prime et al., 2021). Caregivers reported CoFaSS scores at T1. Main analysis employed the general stress scale as a predictor of child coping (M = 25.63, SD = 5.85, range: 16.00–47.00). Supplementary analyses examined subscales (i.e., family, income, and chaos stress).
Positive Family Adaptation. Caregivers reported on PFA via the Family Positive Adaptation during COVID-19 Scale (Family PACS; Shoychet et al., 2022). This previously validated measure includes 7 items (e.g., new family activity), which were rated on a 3-point Likert-type scale (1 = “Not True” to 3 = “Very True”). Items were summed to produce a Family PACS total score used as a predictor in main analyses. The Family PACS measure has demonstrated acceptable psychometric properties via an appropriate one-factor structure, strong measurement invariance across caregiver sex, and acceptable reliability (ω = 0.65; Shoychet et al., 2022). Family PACS data was collected at T1 (M = 12.63, SD = 2.68, range: 7.00–14.00).
Caregiver Perceived Social Support. Caregiver perceived social support was captured at T1 via six items taken from the National Longitudinal Study of Children and Youth (Statistics Canada, 2017). Caregivers rated items (e.g., “There are people I can count on in an emergency”) on a 4-point Likert-type scale (1 = “Strongly Disagree” to 4 = “Strongly Agree”). Reversed items were recoded to yield a total score where higher values indicated more social support (M = 20.41, SD = 3.48, range: 8.00–24.00). Internal consistency was strong (α = 0.88).
Child Coping. Child coping was assessed via the 10-item Connor-Davidson Resilience Scale (CD-RISC-10; Connor & Davidson, 2003). The scale includes items (e.g., “__ is able to handle unpleasant feelings like sadness, fear, and anger”) rated on a 5-point Likert-type scale (0 = “Not True At All” to 4 = “True Nearly All the Time”). The same caregiver reported on both of their children’s coping at each timepoint. The CD-RISC has previously been shown to be psychometrically sound (α = 0.89; test–retest reliability; ICCs = 0.87; Connor & Davidson, 2003), and in the current sample internal consistency was strong (α = 0.91). The CD-RISC-10 demonstrates higher validity and reliability compared to other published versions (Waddimba et al., 2022). The total sum of the CD-RISC-10 was the outcome variable in the current study (range = 0–40; see Supplemental Table S1 for T1–T7 means and standard deviations).
Data Analysis
Data analyses occurred in several phases. First, missingness was assessed for all study variables. One family (i.e., two children) was excluded listwise due to complete missing data on the outcome across all time points. This resulted in a final sample of N = 548 families and N = 1,096 children. Next, bivariate correlations between all variables were run in SPSS version 29 (see Table S1). Missing data for all variables, other than child coping, was <5%. Little’s MCAR test suggested that the data were missing at random. Therefore, missing data for predictors and covariates were handled via multiple imputation with predictive mean matching using the MICE package in R. Missing child coping data (the primary outcome) were handled during the multilevel modeling stage, as this statistical approach has flexibility for missing observations in the context of repeated measures over time by using maximum likelihood estimation. All predictors and covariates without a meaningful zero were centered (Field et al., 2012)—specifically, child gender, caregiver citizenship, caregiver relationship status, 2019 family income, number of people in the household, COVID-19 stress, PFA, and caregiver social support. Categorical variables were dummy-coded (0 vs. 1) and subsequently centered around their means.
A series of multilevel models were run in R to account for the nested structure of the data across the levels of time, child (i.e., sibling), and family (three-level models). Six models were run and included: (1) no predictors; (2) time; (3) time as a random slope; (4) quadratic; (5) covariates; and (6) all predictors, the interactions between social support and our two primary predictors (COVID-19 stress and PFA) on child coping and time. We also ran sensitivity analyses with our predictor model examining each COVID-19 stress subscale (family, income, and chaos stress), presented in Table S4.
Model fit (Table 1) was assessed with Maximum Likelihood (ML) parameters as we were comparing models with different fixed effects (Snijders & Bosker, 2012). However, parameter estimates from our final model were then fitted and reported using Restricted Maximum Likelihood (REML), as ML tends to underestimate variance of random effects (Zuur et al., 2009).
Multilevel Models–Fit Comparisons.
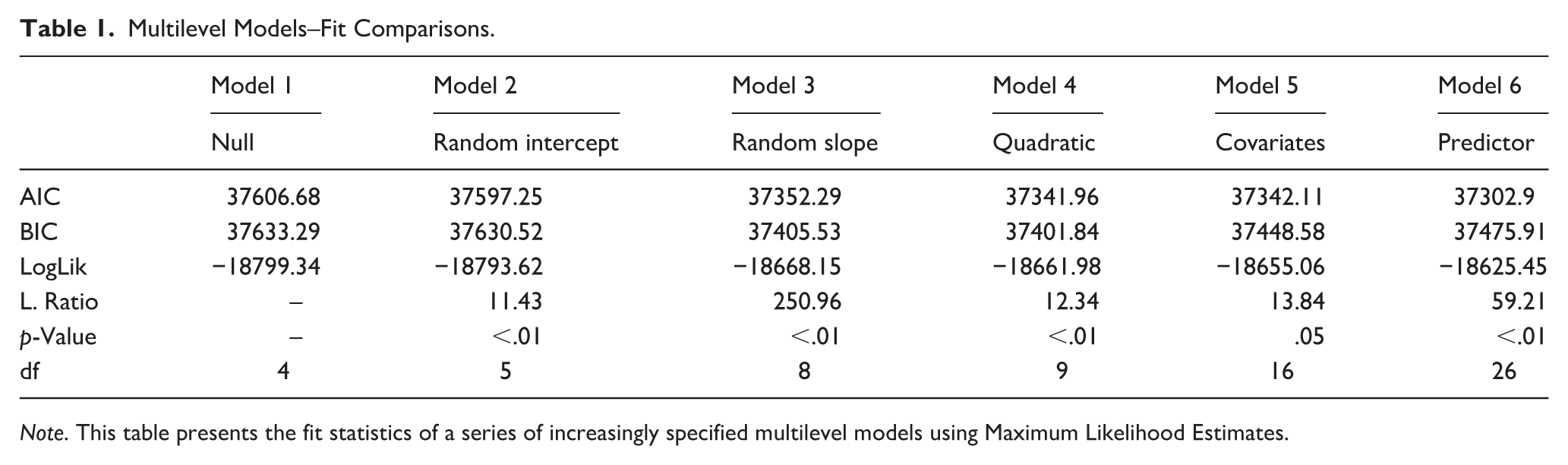
Note. This table presents the fit statistics of a series of increasingly specified multilevel models using Maximum Likelihood Estimates.
To confirm the assumptions necessary for conducting multilevel models, statistical tests for linearity, normality, and homogeneity of variance were performed. The assumption of normality was met, as demonstrated via QQ plots of the standardized residuals of child coping adhering to the normal line. The assumptions of linearity and homogeneity of variance were violated. The violation of linearity suggested curvilinear data, which was addressed by the inclusion of the quadratic time term. The violation of homogeneity of variance indicated heteroscedasticity in the outcome (child coping). In alignment with recommendations from Zuur and colleagues (2009), we incorporated the heterogeneity into our models instead of using a variable transformation so as not to lose potentially important information. Specifically, we controlled for heteroscedasticity by allowing for a greater residual variance with increasing COVID-19 stress using the weight’s function “varFixed” in R. This adjustment resulted in more evenly spread residual plots, ensuring our assumptions of homogeneity were met and allowing for more reliable and valid statistical inferences.
Results
Trajectory of Child Coping Over Time
Our final predictor model, considering both linear and quadratic effects for individual and family-level differences, offered the best fit when comparing models via ML parameters (Table 1; AIC = 37302.9, p < .01). In this model, as demonstrated via REML parameter estimates of the fixed effects presented in Table 2, average child coping at baseline was M = 26.90 (95% CI [23.87, 29.93]). There was a significant positive effect of linear time on child coping (b = 0.11, 95% CI [0.07, 0.16]), suggesting that when the data was fitted linearly, child coping scores generally increased over time. However, as shown in Figure 1, the better fitting, significant quadratic effect of time (b = −0.003, 95% CI [−0.01, −0.00]), suggested that, after an initial increase in child coping, there was a significant deceleration in coping over time.
Multilevel Models—Fixed Effects.
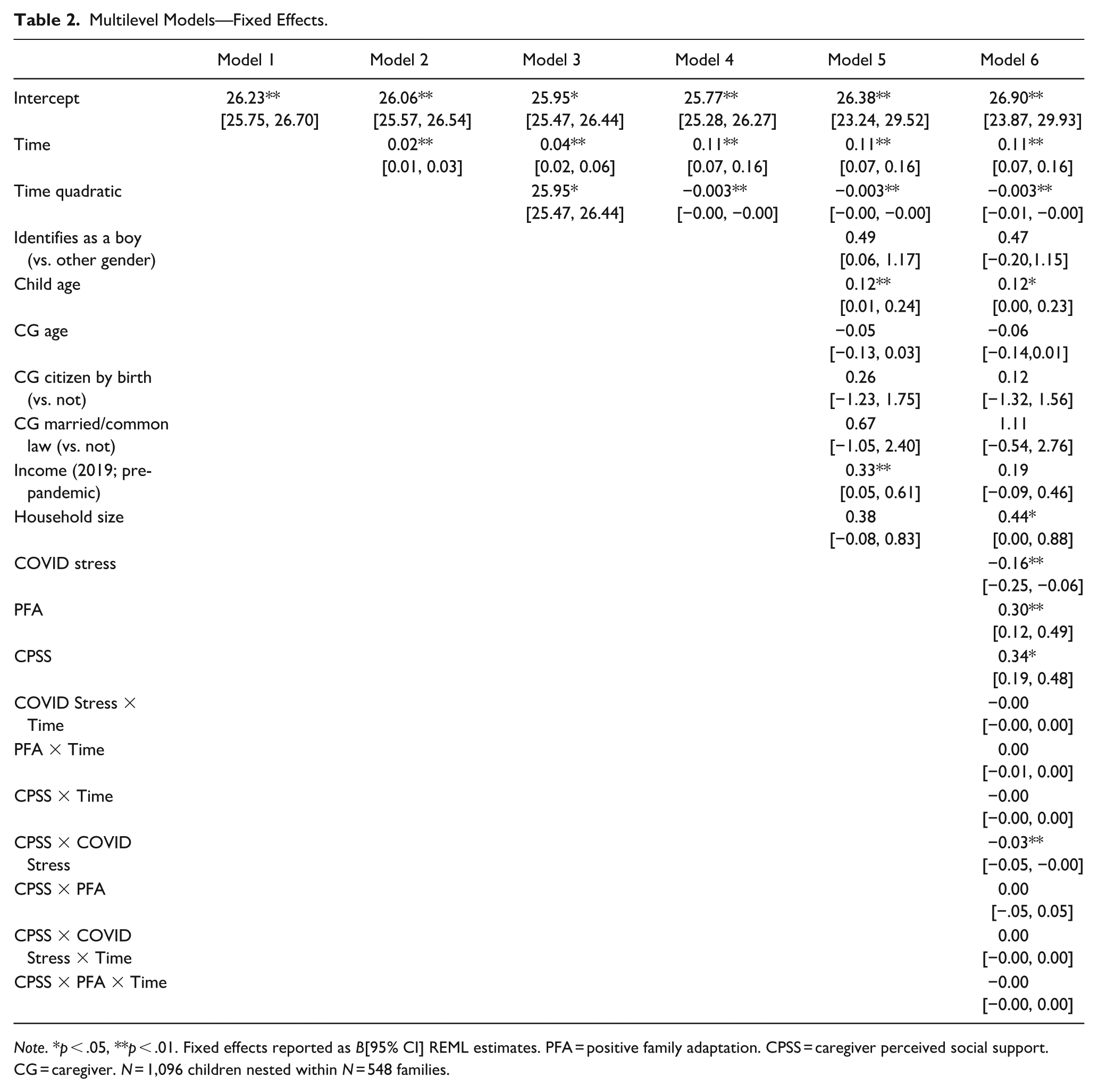
Note. * p < .05, **p < .01. Fixed effects reported as B[95% CI] REML estimates. PFA = positive family adaptation. CPSS = caregiver perceived social support.
CG = caregiver. N = 1,096 children nested within N = 548 families.
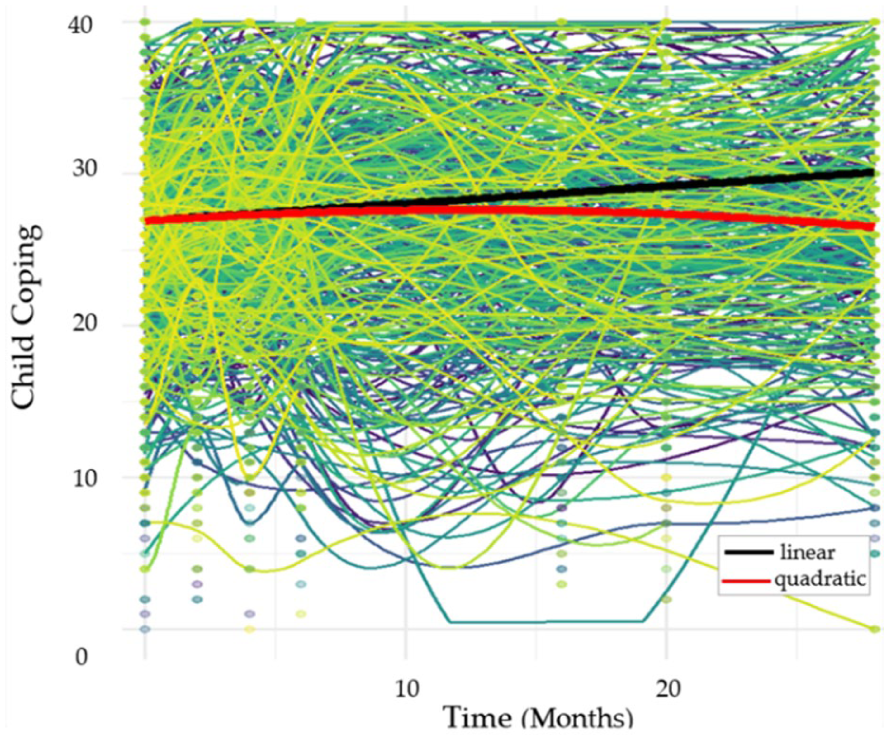
Linear and Quadratic Trends of Child Coping Over Time. Lines represent family-level coping trajectories (N = 548). Dots represent individual children’s (N = 1,096) coping scores at each of the seven timepoints.
Fixed Effects of COVID-19 Stress and PFA on Child Coping
In the final predictor model, COVID-19 stress was significantly associated with lower child coping (b = −0.16, 95% CI [−0.25, −0.06]). PFA (b = 0.30, 95% CI [0.12, 0.49]) and caregiver social support (b = 0.34, 95% CI [0.19, 0.48]) were significantly associated with higher child coping. In terms of covariates, child age (b = 0.12, 95% CI [0.00, 0.23]) and household size (b = 0 .44, 95% CI [0.00, 0.88]), were modestly related to child coping, with older children and those in larger households (i.e., more siblings) tending to cope better. Sensitivity analyses of the COVID-19 stress subscale (Table S4) indicated that family stress (b = −0.40, 95% CI [−0.56, −0.24]), and chaos (b = −0.27, 95% CI [−0.52, −0.02]) were significantly associated with lower child coping, whereas income stress was not associated with child coping (b = −0.06, 95% CI [−0.14, 0.27].
The Moderating Role of Caregiver Social Support
Contrary to hypothesis, caregiver social support did not moderate the association between PFA and child coping, as seen by the non-significant interaction term (b = 0.00, 95% CI [-.05, 0.05]; see Table 2). However, there was a significant interaction between COVID-19 stress and caregiver social support (b = −0.03, 95% CI [−0.05, −0.00]), the pattern of which is illustrated in Figure 2. While low COVID-19 stress appears generally better for child coping over time, high social support buffers against high levels of stress, as seen when comparing the High Support/High Stress to the Low Support/High Stress group.
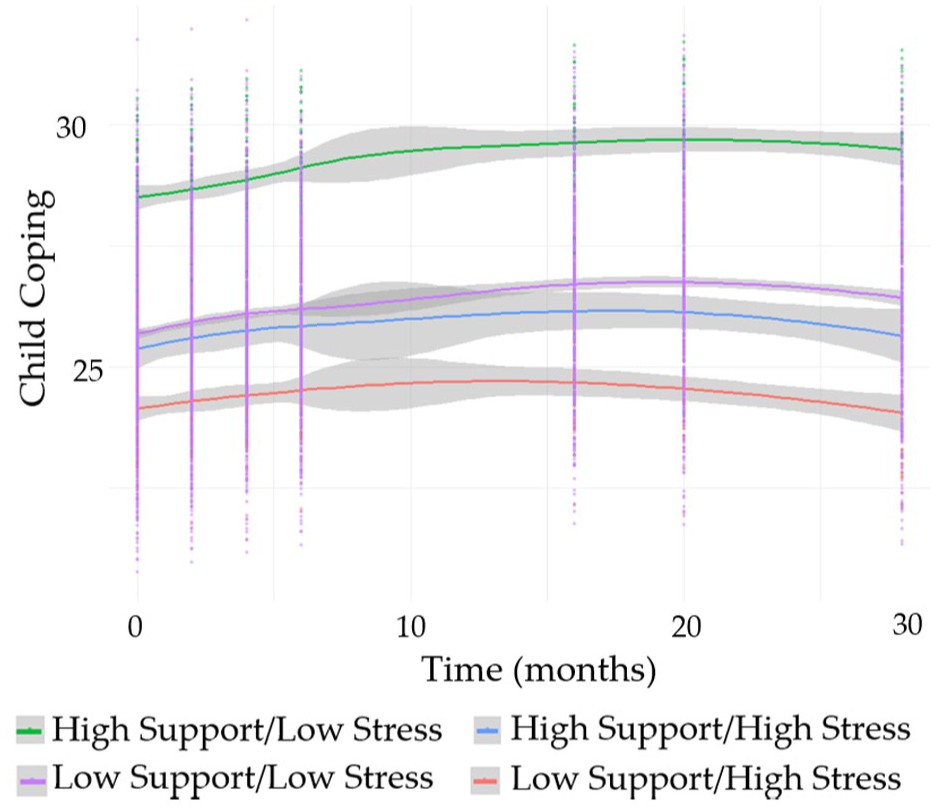
Time-Series Interaction Between COVID-19 Stress and Social Support on Child Coping. This plot visualizes the interaction between caregiver social support and COVID-19 stress on child coping over time, with four lines representing high (+1 SD) and low (−1 SD) combinations of stress and support. Gray shading indicates confidence bands. N = 1,096 children.
Random Effects and Variability Across Family, Individual, and Time Levels
Random effects, displayed in Table 3, were examined to understand the variability in intercept and slope attributable to the different levels of our model. Significant random intercepts and slopes revealed variability in initial child coping and the slope of child coping at all levels of the data: family, individual, and time. Thus, while fixed effects are significant (Table 2), there is variation between children, families, and time. Intraclass correlations (ICCs) were calculated to partition the variance across the levels, as presented in Table 4. The general pattern indicates that 46.46% of the variance in child coping was between families, 33.76% was between siblings, and 19.78% was within individuals over time. We analyzed proportional reductions in variance from the null model (see Table S7) to see how model specificity explained changes to the variance per level. The covariance at the individual level was significant (b = −0.38, 95% CI [−0.05, −0.18]).
Multilevel Model—Random Effects.
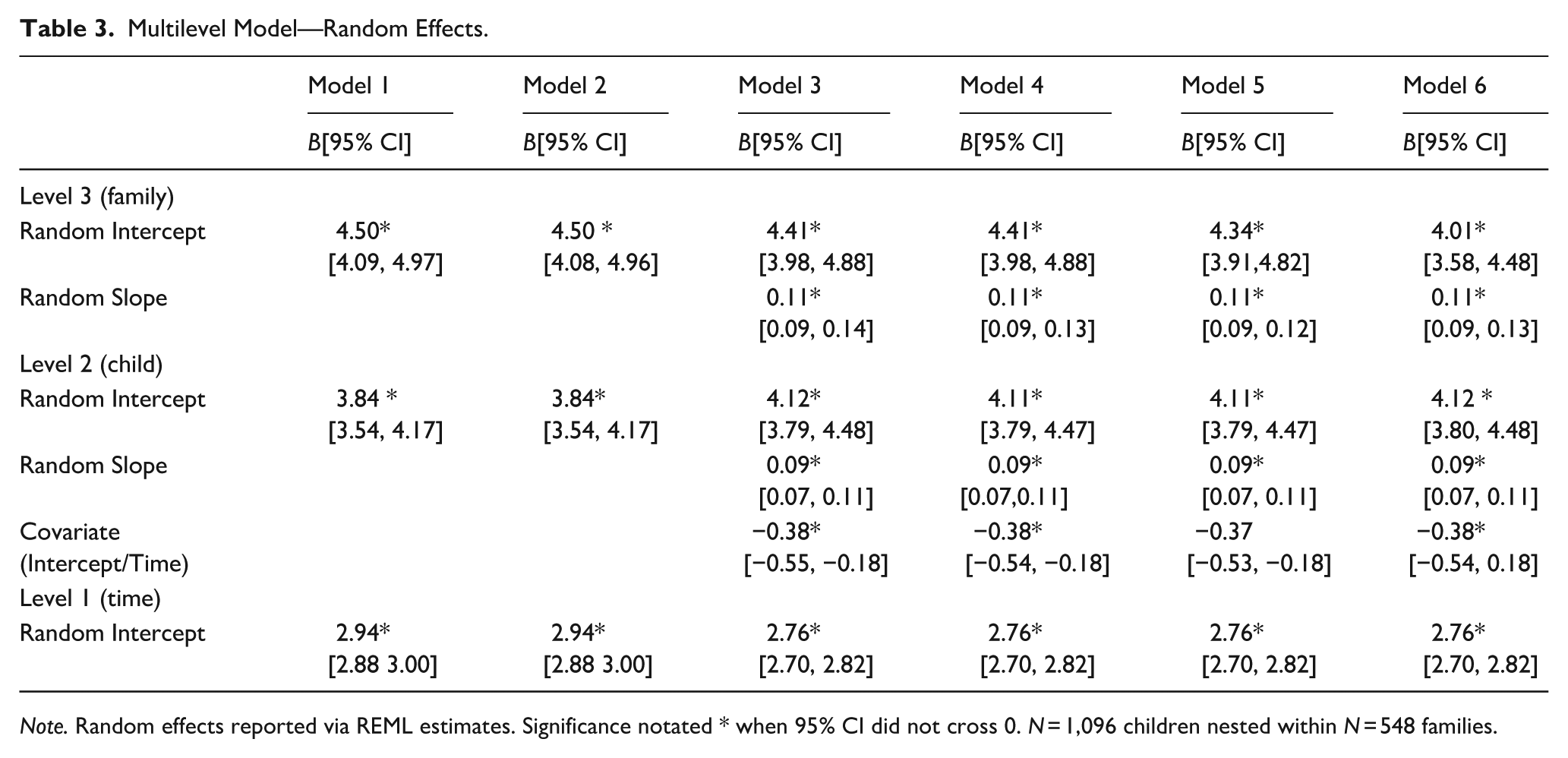
Note. Random effects reported via REML estimates. Significance notated * when 95% CI did not cross 0. N = 1,096 children nested within N = 548 families.
Intraclass Correlation Coefficient– Variance Partitioning.
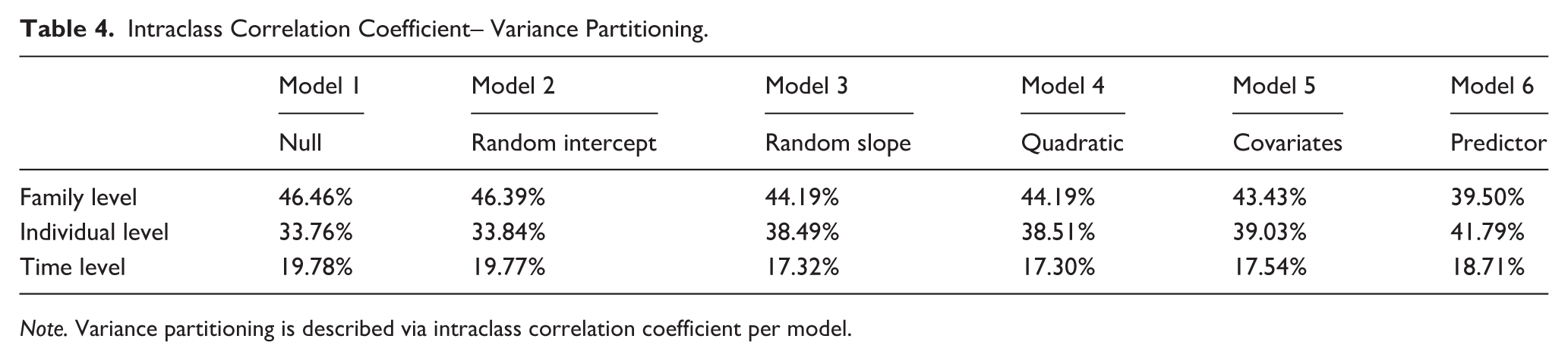
Note. Variance partitioning is described via intraclass correlation coefficient per model.
Discussion
The current study aimed to extend our understanding of the long-term effects of the pandemic on children’s coping, with an emphasis on how stress and adaptation may cascade across family subsystems. Specifically, we examined trajectories of child coping over the first 2.5 years of the pandemic and sought to understand how child coping trajectories varied as a function of family-level pandemic stressors, PFA, and caregiver perceived social support. Obtaining a clearer picture of how children’s coping abilities may have been maintained, activated, or depleted across the family system during COVID-19 may better position children and families to recover in the face of prolonged pandemic impacts, and enhance our knowledge of how to support wellbeing during future collective and/or chronic stressors.
While our data indicated a small initial increase in child coping during the early months of the COVID-19 pandemic that was suggestive of activated resilience, the curvilinear trend indicates that, as time goes on, coping decreased, consistent with allostatic load theory (Evans et al., 2013). This theory underscores how continuous activation of the body’s adaptive processes in reaction to prolonged stress results in damage to allostatic systems (McEwen, 1998). In other words, allostatic load indexes the cumulative wear-and-tear on the body due to repeated activation of multiple stress-response systems over time. Allostatic load theory has since extended beyond strictly biological models to capture a more comprehensive, biopsychosocial understanding of stress, with links to pervasive physical and psychological health consequences (Evans et al., 2013; Guidi et al., 2020; Serviant-Fine et al., 2024; Theall et al., 2012). Though the curvilinear pattern of child coping in our data shows nondramatic decreases in child coping over time, it is important to understand that, while children may be able to activate coping in response to adversity initially, exposure to prolonged stress without adequate recovery or support may generate allostatic overload, straining and depreciating coping resources. This toll on children’s coping over time is consistent with other pre- to peri-pandemic data that shows increasing child psychopathology (Wolf & Schmitz, 2024). In addition, empirical explorations of allostatic load and coping indicate an inverse relationship, making allostatic load a theoretically and empirically promising process to partially explain why the experience of COVID-19 has produced reductions in child coping over time (Guidi et al., 2020).
Considering this curvilinear trend in coping, identifying factors that exacerbate or alleviate this pattern is crucial for determining intervention targets. To this end, and as hypothesized, caregivers reporting more COVID-19 stress within their family system were significantly more likely than those with lower stress to have children with diminished coping abilities. This stress-to-coping association may reflect cumulative risk, wherein individual adversities pose tolerable stress on their own, but confer significant damage to coping resources as risks from varying sources accrue (Browne et al., 2015; Rutter, 1979). This finding converges with extant cross-sectional quantitative data on child wellbeing (Brown et al., 2020; Gassman-Pines et al., 2020) as well as systemic review data of qualitative studies of child wellbeing during the pandemic (Subasinghe & Pathiranage, 2022). The present study extends these results by showing how these pandemic effects are associated with reductions in child coping over an extended period of time covering almost the entirety of the COVID-19 pandemic.
At the same time, cumulative risk has been demonstrated to benefit from cumulative protection (Masten, 2024). As hypothesized, our data revealed that both PFA and caregiver social support related to child coping. Specifically, higher PFA and social support positively predicted child coping, suggesting these are promotive factors. The associations of PFA and social support to wellbeing have been demonstrated cross-sectionally (Cohodes et al., 2021; Ross et al., 2023; Yates & Mantler, 2023) and qualitatively (Dawes et al., 2021; Shum et al., 2023; Subasinghe & Pathiranage, 2022), with current results showing their compensatory capacity for child coping over time during COVID-19. These promotive effects suggest that both PFA and caregiver social support may shape proximal family processes that ultimately facilitate child coping. For example, PFA has been associated with positive parenting, couple satisfaction, and improved family functioning (Shoychet et al., 2022), while caregiver social support has been shown to reduce parenting stress and improve caregiver mental health (Fang et al., 2024), with longitudinal data supporting its association to increased family resources (e.g., clothing, food, additional child care; Gleeson et al., 2016). Thus, results support a strength-based family resilience orientation, emphasizing the importance of family processes in forging resistance to and/or recovery from stress (Walsh, 2003, 2020). In other words, if families can recruit resilience-enhancing factors, even in the context of stress, children may be more likely to maintain their abilities to cope. This finding further highlights the importance of investigating potential moderators of COVID-19 stress, especially those that may be more proximal to the child and directly bear on their coping abilities.
Contrary to our hypothesis, caregiver perceived social support did not amplify the association between PFA and child coping. Most items within the PFA scale relate to the ways in which families positively adjusted to major pandemic-related changes. One of the most cited changes during this period is the experience of isolation (Buecker & Horstmann, 2022; Shi et al., 2024). Many of our PFA items relate to positive practices that are largely independent of a social network beyond the immediate household, such as engaging in new family activities (Shoychet et al., 2022). This relatively narrow focus on family-specific adjustment may explain the lack of an interaction effect with caregiver social support. In other words, while family adaptation has a significant and direct benefit to child coping, it does not appear to synergistically enhance the positive effects of caregiver social support.
In contrast, and consistent with hypotheses, caregiver social support significantly moderated the association between COVID-19 stress and child coping. Specifically, the significant negative association between COVID-19 stress and coping was mitigated by higher levels of caregiver perceived social support. While high levels of COVID-19 stress appeared to weaken children’s coping abilities overall (i.e., across levels of the moderator, social support), children who faced high stress but had caregivers with high levels of social support tended to demonstrate better coping relative to those who faced high stress and had caregivers with low social support. This moderation effect aligns with emergent themes from qualitative literature (e.g., Dawes et al., 2021; Shum et al., 2023), which have identified “support bubbles,” such as moving in with grandparents, as a protective factor that buffered against pandemic-imposed stressors. Despite this buffering effect, caregiver social support did not completely ameliorate risk, as seen by the pattern of children in the High Support/High Stress group who showed consistently lower coping over time relative to the High Support/Low Stress group. If social support was able to fully guard against decrements in child coping imposed by COVID-19 stress, coping in these two groups would look similar. The limits to the protective capacity of social support in the context of COVID-19 has been previously demonstrated via structural equation modeling, with prior findings suggesting that, although social support negatively predicted mental health problems during COVID-19 when participants experienced a period of isolation for 1–2 weeks, as the isolation time increased to 3 or more weeks, social support was no longer a strong predictor of mental health (Xie et al., 2024). This pattern may be explained through resilience models in which caregiver perceived social support serves as a protective factor, partially rather than fully offsetting the impact of stress (Fergus & Zimmerman, 2005).
It is likely that the efficacy of caregiver perceived social support is context-dependent and may diminish with increased intensity and duration of a stressor. During a protracted, communal crisis such as COVID-19, stressors not only imposed prolonged hardship but also uniquely disrupted access to typical systems of support via mandated isolation, school closures, and reduced in-person contact with occupational and/or social networks, thereby potentially limiting the reach and capacity of caregiver’s social support on children’s coping outcomes under conditions of high stress. Thus, while caregiver social support is both a promotive and protective asset, additional mobilization of family, school, community, and government resources as recommended by Vaillancourt and colleagues (2021) may be necessary to more fully safeguard children’s coping, considering that the benefits of social support in the current data are greater at low relative to high levels of COVID-19 stress.
A unique finding of the current study lies within the intraclass correlations of our null model. Intraclass correlations are descriptive statistics used to make relative comparisons of within- and between-group variability of nested data. In the current study, they help us understand how much of the variance in child coping occurs between families (level 3), within families (i.e., between siblings; level 2), or within individuals (i.e., over time; level 1). The majority of variance in child coping exists between families (i.e., children from different families have the most different coping from one another in comparison to children in the same family or the same child over time). This larger proportion of variance at the family level suggests that caregivers are reporting more similar scores of child coping for both children in one household than are caregivers between different households. This trend is further outlined by the proportional reduction in variance from the null to predictor model, with a reduction (14.98%) in the variance explained by the family level when the predictors are added (Table S7). One possible interpretation of this finding, in alignment with data on single-informant bias (Achenbach et al., 1987; De Los Reyes et al., 2015), is that child coping scores reported by caregivers reflect unique features of the caregiver more so than the child’s coping itself. For example, an inherently optimistic father may report that his children believe they can achieve their goals based on his own optimism, rather than due to indicators of his children’s own coping abilities. Alternatively, a caregiver who is struggling with their mental health during the pandemic may be more likely to report that both of their children are unable to adapt when changes occur. This has important implications both for the current study as well as the large body of family explorations during COVID-19 that rely on caregiver reports and only assess one child per family (the norm in developmental research). This finding raises the possibility of undetected reporting biases that may have either underestimated or overestimated child functioning and associations with other factors during the pandemic. In general, this finding speaks to the importance of family-wide science that permits an assessment of both within- and between-family effects to better understand the nature of associations between stressors, sources of resilience, and child wellbeing.
The strengths of this study include its longitudinal design across 2.5 years of the COVID-19 pandemic and use of multilevel modeling with two siblings per family, maximizing our sample size while accounting for the nested structure of the data. There are also several limitations, including reliance on caregiver reports that may introduce reporting biases. This is a common methodological challenge in COVID-19 family systems research, and while caregiver perception is valuable, future studies should strive to explore child coping via multi-informant, observational, or direct assessment approaches (Shoychet et al., 2023). In addition, our sample is predominantly socioeconomically advantaged, with the majority of caregivers being educated, White Europeans, citizens of their country, and married/common law to their partner. This may limit the generalizability of the findings, particularly considering the disproportionate impacts of COVID-19 on racialized and economically marginalized families (Raifman & Raifman, 2020). Our socially advantaged sample may also have limited our explorations of sociodemographic covariates, such as caregiver citizenship status, income, and relationship status. Given these limitations, future studies should explore these associations in more diverse samples. Finally, the promotive, compensatory, and protective factors cited in the current study capture but a small number of variables and processes that have the potential to influence child and family resilience (Ungar and Theron, 2020). Future studies should investigate additional predictors of coping both within (e.g., household faith) and beyond family subsystems (e.g., school support, health care policies) in understandings of the cascading effects of risk and resilience. For example, prior work in this same sample has shown that caregiver coping mediates the association between caregiver mental health and religion and spirituality, a factor that may be especially relevant when social support is lacking or undermined during periods of stress and isolation (Sen et al., 2022).
Conclusion
Findings demonstrate that, despite the transition into a “post-pandemic” society and high levels of pandemic fatigue, it is imperative for scientific, policy, and service-oriented communities to recognize the ongoing psychosocial ramifications of COVID-19 that persist for many children and families. Further, congruent with the COVID-19 Family Disruption Model, findings highlight that family-level stressors and supports are critical in understanding the trajectory of child coping during the pandemic. Specifically, while the COVID-19 pandemic may have had a concerning wear-and-tear effect on child coping trajectories over 2.5 years, with accruing COVID-19 stressors relating to worsening child coping, family-level resources such as PFA and caregiver social support have been promotive of child coping. By examining how pandemic stressors and specific family-level compensatory and protective factors influence child coping outcomes over time, the present study extends our theoretical understanding of risk and resilience as dynamic, developmental, and contextual constructs. Our nested design also provides insight into multilevel variability and, more specifically, the risk of single-informant bias, advancing methodological considerations in pandemic research. Finally, our findings offer insight into intervention design and policy. Specifically, interventions that target family adaptation and caregiver support in service delivery may be especially effective for preserving child coping. For example, our results align with the demonstrated efficacy of virtual parenting interventions during COVID-19 whose treatment targets explicitly focused on reliable family routines, “sunshine” play-time, caregiver-child attunement (all potentially facilitative of PFA) and/or caregiver social support (Deotto et al., 2023; Gray et al., 2022). In parallel, policies that reduce pandemic stressors, such as income stabilization measures, flexible remote work, paid sick leave, equitable access to COVID-19 testing and treatment, and provision of digital infrastructure for online schooling, may play a critical role in reducing decrements in child coping during periods of collective crisis. Future work should continue longitudinal follow-ups with pandemic-exposed children and families, and focus on how to facilitate family adaptation strategies, bolster the protective capacity demonstrated by one element of social support, and understand what other resources can help to mitigate family-level stress to improve child coping during future collective, prolonged stressors.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254251411150 – Supplemental material for A longitudinal exploration of pandemic stress and family adaptation on child coping: The protective role of caregiver social support
Supplemental material, sj-docx-1-jbd-10.1177_01650254251411150 for A longitudinal exploration of pandemic stress and family adaptation on child coping: The protective role of caregiver social support by Victoria Parker, Imogen Sloss, Dillon Browne and Mark Wade in International Journal of Behavioral Development
Footnotes
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Board of the University of Toronto and Waterloo University (REB code: 42112; date of approval: May 17, 2020).
Author contributions
Conceptualization, V.P, M.W., and D.B.; methodology, V.P., D.B. and M.W.; formal analysis, V.P. and I.M.; resources, M.W. and D.B.; writing—original draft preparation, V.P.; writing—review and editing, M.W I.M, D.B.; supervision D.B. and M.W.; visualization, V.P.; project administration, I.M. and D.B.; funding acquisition, M.W. and D.B. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Tri-agency / Canadian Government sponsor; Canadian Government Agency: SSHRC—Social Sciences and Humanities Research Council; Program Name: Canada Research Chair; Work-order/award number: # 950–232347 [D.B.] and Society for Research in Child Development, Small Grants Program for Early Career Scholars [M.W and D.B.].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent to participate
Informed consent was obtained via the signing written consent forms from all subjects involved in the study.
Data availability statement
Restrictions apply to the datasets. The dataset presented in this article are not readily available due privacy and ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.