
Abstract
Emotion regulation (ER) is central to most mental health difficulties. However, we know less about the impact of mental health on ER, particularly during vulnerable developmental periods. This study examines longitudinal associations between ER strategies and general psychopathology from adolescence to adulthood, distinguishing between- and within-person effects across 1 and 13 years. Norwegian adolescents (N = 2,464, 51% female, mean age = 13.7) were followed into adulthood (N = 1,266, 56.7% female, mean age = 27.2). Five ER strategies, including rumination, reactive impulsivity, non-acceptance, problem-solving, and seeking social support, were assessed. Using Random Intercept Cross-Lagged Panel Models, within-person analyses revealed that more than usual psychopathology predicted more than usual rumination, reactive impulsivity, and non-acceptance 1 year later. Only more than usual reactivity reciprocally predicted more than usual psychopathology 1 year later. More than usual psychopathology during adolescence predicted less social support seeking than usual during adulthood, and more social support seeking than usual during adolescence predicted fewer symptoms of psychopathology than usual during adulthood. There were no significant associations between problem-solving and psychopathology. We found reciprocal and unidirectional associations between general psychopathology and ER strategies, highlighting ER as both a risk and protective factor, but also illuminating the role general psychopathology has on ER.
Introduction
Most individuals experience common mental health difficulties at some point during their lifespan (Caspi et al., 2020), with epidemiological studies showing a typical onset during adolescence and early adulthood (Solmi et al., 2022). Symptoms across various domains, such as anxiety, depression, conduct problems, and thought problems, are thought to share a common vulnerability of general psychopathology (Caspi et al., 2014). This overarching vulnerability is linked with emotion regulation (ER) challenges (Aldao et al., 2010, 2016; Lincoln et al., 2022), suggesting that ER plays a key role in broad-spectrum mental health difficulties. This has led to the hypothesis that ER is a transdiagnostic process of general psychopathology (Cludius et al., 2020). Research has primarily examined how regulating emotions precedes and predicts symptoms (Sheppes et al., 2015). ER can also be shaped by symptoms (Aldao & Nolen-Hoeksema, 2010). For instance, fear, a common anxiety symptom, may trigger rumination, which intensifies fear and creates a self-perpetuating cycle. This illustrates a reciprocal relationship between symptoms and ER. However, empirical evidence on associations with general psychopathology remains limited and inconclusive, as most studies focus on specific symptom domains (e.g., depression and anxiety). Because co-occurring symptoms are the norm and most individuals experience symptoms across multiple domains (e.g., internalizing and externalizing symptoms; Caspi et al., 2020), it is important to examine how ER strategies shape and are shaped by broad-spectrum mental health difficulties, as domain-specific symptoms may not capture the full extent of risk. In other words, if research focuses only on one domain (e.g., anxiety), the overarching picture might be lost, restricting the study of common underlying mechanisms (e.g., ER strategies). Moreover, research suggests that a general factor of psychopathology is more associated with indicators of life impairment (e.g., suicide attempt and duration of social-welfare benefit use) than individual domains (Caspi et al., 2014). Beyond improving precision, it also offers theoretical clarity and a more parsimonious understanding of psychopathology: instead of viewing symptoms as separate entities, we can view them as expressions of a common underlying dimension. In addition, most studies have not assessed the unique contributions of multiple ER strategies, which would provide a more holistic view into ER strategy use and its links to psychopathology. Most have also conflated between-person and within-person effects (i.e., stable between-individual differences vs. fluctuating within individuals). To address these limitations, the present study investigates reciprocal relationships between five well-established ER strategies and general psychopathology, explicitly separating between- and within-person variances. We further investigate different time-lags to capture effects during adolescence and across the transition to adulthood to explore stability and change in psychopathology and ER.
Emotion Regulation
ER is broadly defined as the process by which individuals influence the intensity, duration, and expression of emotions (Tull & Aldao, 2015). ER involves being aware of, understanding, and accepting one’s emotions, to control impulsive behaviors and maintain goals in the face of negative emotions, and flexibly apply strategies to meet goals or situational demands (Gratz & Roemer, 2004). Considerable research has confirmed protective aspects of some ER strategies in reducing risk of adverse mental health outcomes, such as using reappraisal or problem-solving to change how one perceives a situation or emotion. These strategies help individuals avoid becoming stuck in prolonged emotional episodes, which can heighten vulnerability to mental health difficulties by increasing stress or reducing coping capacity. Conversely, studies have also shown how some ER strategies pose as risk factors for general psychopathology, such as persistent rumination, avoidance, and suppression of emotions (Aldao et al., 2010; Schäfer et al., 2017). Such strategies may be harmful because they can keep individuals stuck in emotional states. For example, rumination may prolong difficult emotions and suppression prevents emotional processing, reinforcing cycles that contribute to mental health difficulties (Boyes et al., 2016).
The use of emotion regulation strategies can vary across developmental periods. For example, adolescents tend to have a poorer ER repertoire (e.g., use fewer adaptive strategies) when experiencing sadness, anger, and fear than adults (Zimmermann & Iwanski, 2014), increasing their risk for general psychopathology (Lougheed & Hollenstein, 2012). Adolescents use less social support seeking and adaptive ER in comparison to adults, while rumination, avoidance, and expressive suppression is similarly used across both adolescence and adulthood, with dysregulation (conceptualized as blaming others) increasing during adulthood (Zimmermann & Iwanski, 2014). Emotional reactivity (heightened emotional reactions) peaks between ages 15 and 19 (Zimmermann & Iwanski, 2014), increasing adolescents’ susceptibility to poorer mental health (Gross & Jazaieri, 2014). During adulthood, emotional reactivity may level out, but those who tend to respond more impulsively to their emotions are at risk for both internalizing and externalizing symptoms (Carver & Johnson, 2018).
General Psychopathology
In our study, we are shifting the focus from distinct symptom domains to shared aspects across mental health conditions, known as general psychopathology or the p-factor (Caspi et al., 2014). Co-occurring symptoms are the rule rather than the exception (Caspi et al., 2020; Kessler et al., 2011) and are prevalent during adolescence and into adulthood (Choate et al., 2023; McElroy et al., 2018). Co-occurring symptoms tend to intensify during this period (ages 16–26; Richards et al., 2024). Given the salience of such comorbidity during adolescence and adulthood, identifying and understanding transdiagnostic processes that contribute to and are influenced by general psychopathology is crucial to better inform prevention and intervention research aiming to target the shared risks and outcomes rather than only targeting one problem per treatment (Sauer-Zavala et al., 2017).
Associations Between ER and General Psychopathology
Among longitudinal studies with adult samples, two studies found that a total score of ER skills predicted subsequent depressive and anxiety symptoms, whereas symptoms did not predict subsequent ER skills (Berking et al., 2012; Wirtz et al., 2014). Dawel and colleagues (2021) found that suppression and depression reciprocally predicted each other and found partial support for reciprocal effects between suppression and anxiety. Notably, anxiety consistently predicted subsequent suppression of emotions, and no significant associations were found with cognitive reappraisal. The above studies illustrate the complex associations between ER and depressive and anxiety symptoms, where increased ER skills are associated with fewer symptoms. But when focusing on specific strategies, there is some evidence of reciprocity (suppression and depressive symptoms), with more evidence for internalizing symptoms predicting more suppression of emotions. Most studies have focused on associations between internalizing problems and ER, with fewer longitudinal studies examining both internalizing and externalizing problems in adults. This may be a considerable limitation, as both conditions are prevalent from adolescence to adulthood (Richards et al., 2024).
Longitudinal studies with adolescents report similar mixed findings. A general factor of ER difficulties predicted anxiety symptoms, aggressive behavior, and eating disorder symptoms, but none of the symptoms predicted ER difficulties (McLaughlin et al., 2011). Furthermore, a total score of ER difficulties predicted social anxiety and depression, and only social anxiety reciprocally predicted ER difficulties (Masters et al., 2019). In another study, depressive symptoms consistently predicted increases in suppression, but not cognitive reappraisal (De France et al., 2019). Despite mixed findings, a recent meta-analysis of longitudinal studies shows overall support for reciprocal effects between adaptive and maladaptive ER and psychopathology during adolescence (Cavicchioli et al., 2023). However, the reciprocity of specific ER strategies was not examined. When assessing general ER, findings with adolescents show more support for ER predicting subsequent symptoms. When focusing on specific strategies, however, depressive symptoms tend to predict subsequent suppression of emotions. Overall, the summarized literature has either investigated these associations with general factors/scores (e.g., adaptive vs. maladaptive, ER skills or difficulties) or investigated specific ER strategies in separate models. Assessing more general ER or ER strategies separately limits the ability to identify the specific cognitive and behavioral strategies that may be most associated with general psychopathology (Aldao & Nolen-Hoeksema, 2010).
The Between and Within Problem
All the above-mentioned studies examine crucial questions concerning symptoms and ER. However, most have not accounted for between- and within-person differences. Consequently, individual changes are compared to group averages across time, with resulting estimates capturing a conflation of differences between people (e.g., people who have more difficulties with ER have poorer mental health, compared to people who have less difficulties) and within-person fluctuations (an individual’s deviation from their own average). Such approaches have been criticized and alternative models have been proposed to account for stable traits and within-person states (e.g., random intercept cross-lagged panel model, RI-CLPM; Hamaker, 2023; Hamaker et al., 2015). Although understanding common trajectories for people with high or low trait levels is important, the disaggregation of traits and states may provide more robust and detailed information for personalized treatments/interventions that target transdiagnostic general psychopathology (Moeller, 2022).
Within-Person Associations Between ER and Psychopathology
Several studies have investigated reciprocal within-person associations between ER and symptoms using RI-CLPM, yielding mixed results. One study following individuals from adolescence to adulthood found very little evidence for within-person reciprocal effects between ER ability (trait measure of emotional control), depressive and anxiety symptoms, and substance abuse. Instead, more than usual (deviations from an individuals’ average) depressive symptoms and substance abuse predicted decreased emotional control (Klein et al., 2022). In contrast, a study of adults reported reciprocal effects, where more than usual ER difficulties (total score) predicted increased depressive and anxiety symptoms, and more than usual depressive and anxiety symptoms predicted increased ER difficulties (Wong & Hamza, 2024). During early adolescence, one study found that more than usual emotional distress consistently predicted poorer perceived ER, and more than usual perceived successful ER predicted less emotional distress (Demkowicz et al., 2024). Although these findings address the between- and within-person problem, they focus on general ER and predominately internalizing symptoms, even though ER strategies are associated with broad-spectrum mental health problems (Aldao et al., 2016).
Overall, little evidence of within-person reciprocal effects has been found across the transition from adolescence to adulthood, although some support exists within each developmental phase, separately. In addition, to our knowledge, no studies have yet explored within-person reciprocal associations between specific ER strategies and general psychopathology. Because people often experience symptoms across multiple domains, general psychopathology may be better suited for mapping risks and protective factors (Oldehinkel & Ormel, 2023). Investigating ER strategies can reveal malleable processes that either contribute to or are affected by a broad vulnerability, or remain tied to specific domains, pointing to potential targets for prevention or intervention efforts (Cludius et al., 2020). A transdiagnostic approach is especially valuable since general psychopathology appears better suited than domain-specific approaches for understanding long-term outcomes (Sallis et al., 2019).
Current Study
The conceptual rationale is as follows: since previous research has yet to examine within-person reciprocal associations involving specific ER strategies and has primarily focused on internalizing symptoms, this study investigates the unique associations of five ER strategies rumination, reactive impulsivity, non-acceptance of emotions, social support seeking, and problem-solving—and general psychopathology. Most prior studies have either examined strategies separately or relied on global indices (e.g., ER difficulties), which do not clarify the unique contributions of individual strategies. By modeling these strategies simultaneously within a single model that allows them to correlate, we can more accurately capture transdiagnostic processes rather than associations driven by shared variance among strategies (Aldao & Nolen-Hoeksema, 2010). This approach allows us to identify which strategies function as risk or protective factors in relation to general psychopathology. A further contribution is examining whether associations observed in adolescence have enduring effects into adulthood. Using RI-CLPMs, we parse apart the between- and within-person effects and assess 1-year associations during adolescence (i.e., T1 predicting T2) and associations from adolescence to adulthood (i.e., T2 predicting T3). The ER strategies have been selected due to previous research showing associations with general psychopathology (Aldao et al., 2010; Compas et al., 2017).
Method
This study is a secondary data analysis of the Youth and Mental Health Study (YAMHS; see Kaasbøll et al., 2021), which is a representative population-based study that ran from 1998 until 2012 in Trøndelag county (central Norway). The YAMHS’ purpose was to investigate determinants of the development of mental ill-health from adolescence to adulthood, investigating various risk and protective factors (e.g., stressful life events, bullying, self-perception, and coping strategies). The sample was selected based on school size (i.e., proportional allocation), leading to 2,792 eligible students from 22 schools to be invited to the study. Data were collected via self-report surveys during two school hours. We use data from the first time-point (T1), second time-point (T2) 1 year later, and the third time-point (T3), 1 14 years after the initial assessment.
Ethics
The YAMHS study was approved by the Regional Committee for Medical Research Ethics in Central Norway (REK midt; reference number 1454). This approval was renewed in 2019 (reference number 1045) and again in 2022 to include the first and last authors as project members.
Sample
Of 2,792 eligible participants, 88.3% consented to be a part of the study. The baseline sample (T1) consisted of 2,464 adolescents in the 8th and 9th grades, 51% of the sample is female with a mean age of 13.7 (range = 12.5–15.7, SD = .6). At T2, 2,432 adolescents participated with a mean age of 14.9 (range = 13.7–17, SD = .6). At T3, 51.9% of the original adolescents, at this time adults, participated in the study (N = 1,266, 56.7% female) with a mean age of 27.2 (range = 26–28.2, SD = .6). The sample was predominately Norwegian with 93.2% of students having Norwegian born parents. In terms of socioeconomic status (SES), the adolescent sample was overrepresented with middle- and working-class parents (43.4% and 46.5%, respectively). As adults, 58.7% of the participants rated their SES as average compared to the general population.
Measures
Emotion Regulation
The measures of the ER strategies were developed and tested in a previous study (Helland et al., 2024). We used the following five strategies: rumination (five items), defined by continuously thinking about feeling sad; reactive impulsivity (four items), defined by reacting physically (e.g., tensing and losing composure) and emotionally (e.g., becoming irritated) to stress or difficult situations; non-acceptance (three items) defined by self-blame and self-criticism in response to stress or difficult situations; social support (four items) defined by seeking out and meeting with friends when feeling sad or during difficult situations; and problem-solving (four items) defined by understanding and solving the stressful or difficult situation. The five ER strategies were measured at each time point (T1, T2, and T3), and participants were asked how often they used any of the responses on a 4-point Likert-type scale ranging from almost never (1) to almost always (4). Reliability across the three time-points was determined by McDonald’s omega (ω), rumination ranged from ω = .71 to .75, reactive impulsivity ranged from ω = .75 to .78, non-acceptance ranged from ω = .68 to .78, seeking social support ranged from ω = .75 to .79, and problem-solving ranged from ω = .75 to .81.
General Psychopathology
The ASEBA system (Achenbach & Rescorla, 2004) provides comprehensive measures of psychological functioning for children, youth, and adults. We used the Youth Self-Report (YSR), which contains 112 items of symptoms of anxious-depression, withdrawal, somatic complaints, thought problems, attention problems, rule-breaking behavior, and aggressive behavior. Participants indicate how relevant the listed symptoms are currently or over the past 6 months. The responses ranged from not true (0), somewhat true (1), and very true (2). For the adult measure we used the Adult Self-Report (ASR), which contains 123 items of the same symptom domains listed above, in addition to substance abuse (not used in this study), the procedure and response scale are the same as the YSR. We used a total of 66 items from both the YSR and ASR for the following reasons: (1) the original number of items contained open-ended questions, and (2) to ensure comparability of the psychopathology construct, we included items only present during adolescence and removed any inconsistent items. This led to 13 items for anxious-depression, 8 items for withdrawal, 7 items for somatic complaints, 9 items for rule-breaking behavior, 14 items for aggressive behavior, 11 items for thought problems, and 5 items for attention problems. We created a composite score across all the items to represent general psychopathology. Previous research has shown that such a score does not usually differ from a latent general factor of psychopathology (Fried et al., 2021). Omega for psychopathology at T1 = .93, at T2 = .95, and at T3 = .94.
Statistical Analysis
All analyses were conducted in R (version 4.3), using the packages lavaan (Rosseel, 2012), tidyverse (Wickham et al., 2019), and psych (Revelle, 2007). Model fit of the structural equational models was determined by the comparative fit index (CFI) and Tucker–Lewis index (TLI) being above .90, and the root mean square error of approximation (RMSEA) and the standardized root mean square residual (SRMR) being below .08. Across the three time-points, item level missingness was 18.86% and was determined as missing at random due to a significant Little’s MCAR X2(1,304) = 1,791.14, p < .001 and no clear missingness patterns. To handle the missing data, we used full information maximum likelihood which is a reliable method with MCAR data (Li & Lomax, 2017). However, there was also attrition, with 48.1% of the sample lost by T3. We ran t-tests with Bonferroni corrections to investigate demographic and mean-level differences of psychopathology and the ER strategies between the sample lost to attrition and the retained sample, see “Results” section. In addition, we investigated normality and found several non-normal distributions. The distribution of psychopathology, rumination, and non-acceptance across both adolescence and adulthood was skewed positively. During adulthood, we also found a positive skew for reactivity. Social support and problem-solving (in both adolescence and adulthood), and reactivity during adolescence were normally distributed. We used maximum likelihood with robust standard errors (MLR) to handle the non-normal distributions. Outliers were also investigated (see Supplementary materials).
Random Intercept Panel Models
We ran an RI-CLPM (Hamaker et al., 2015) with each ER strategy and general psychopathology to assess the unique reciprocal associations to psychopathology. To capture the between-person associations, the observed variables are set to equally regress onto a latent factor (i.e., random intercept, RI) that represents shared trait-like attributes. Next, the residual variances, which are deviations from the trait (i.e., fluctuations) and not captured by the RIs, are modeled as within-person latent variables. In addition, autoregressions of the within-person variables are modeled, as well as baseline and residual correlations and variances within each time point, see Figure 1 for illustration. In each model, we added gender as a time-invariant variable predicting the observed variables, as there tends to be differences in both psychopathology and ER across gender (Nolen-Hoeksema, 2012). We use standardized regression coefficients (i.e., beta coefficients) as effect sizes, according to current recommendations for RI-CLPMs small effects are from .03, medium effects are from .07 and large effects are from .12 (Orth et al., 2024).
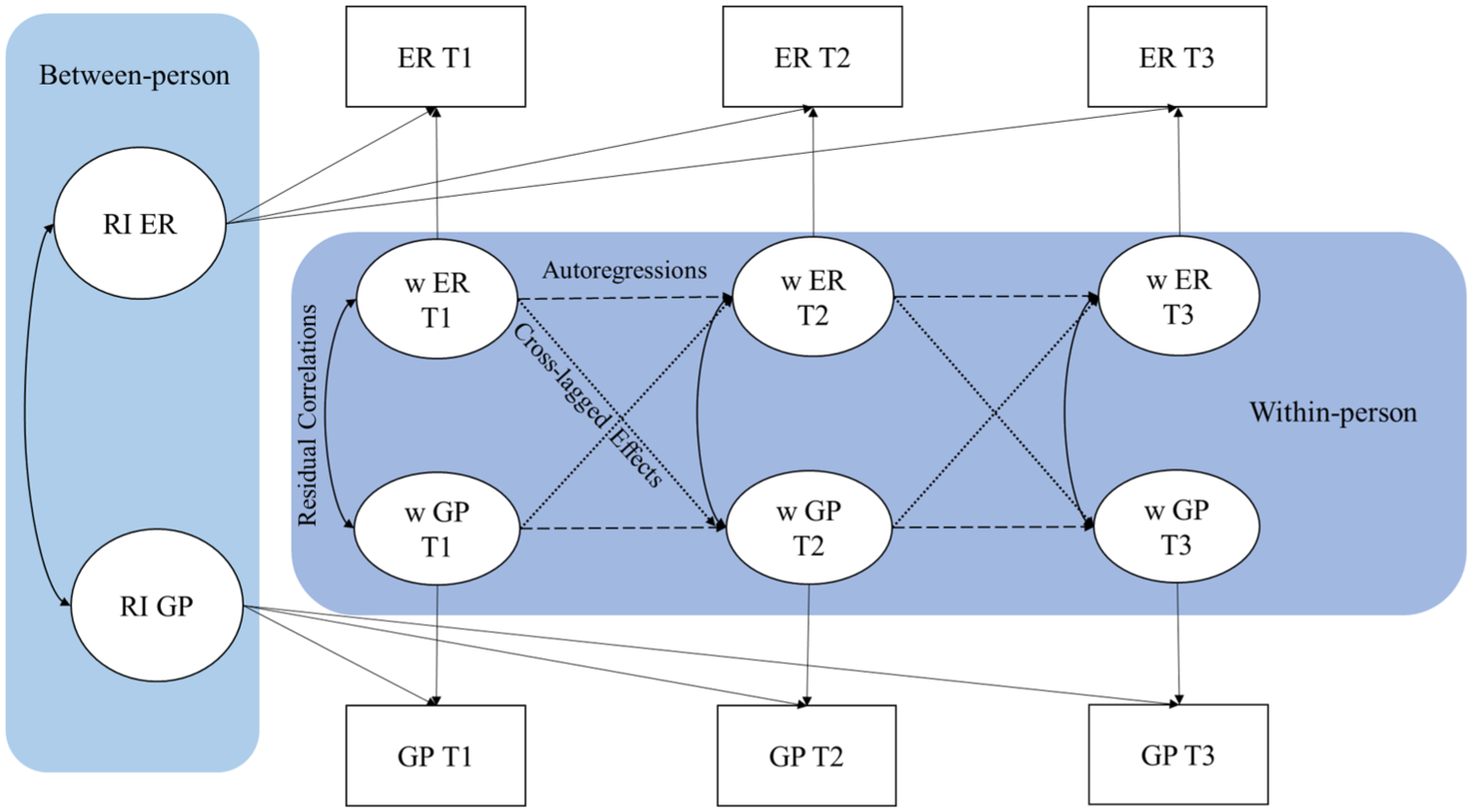
Illustration of the Random-Intercept Cross-Lagged Panel Model. RI = Random intercept. ER = Emotion Regulation. GP = General Psychopathology. Each observed variable (rectangles) is equally regressed onto their respective RIs. Dashed lines represent the autoregressive associations. Dotted lines represent the cross-lagged effects. Double arrowed lines represent the correlations.
Results
Attrition
Several t-tests revealed minor differences between the participants lost to attrition and those retained. First, there were no significant differences in psychopathology at baseline (p = .23). For ER strategies at baseline, there were no significant differences in non-acceptance, problem-solving and reactivity (p > .05), but we found a mean difference (MD) in rumination (MD = .07, p = .001), the retained sample had a higher mean compared to the sample lost to attrition. While the sample lost to attrition had a higher mean on seeking social support (MD = .11, p < .001). Generally, sample means are biased to attrition, but the identified MDs are quite small. In addition, estimates of associations between variables prove to be robust in spite of attrition (Gustavson et al., 2012). In terms of socioeconomic status, those lost to attrition had reported lower SES than those retained (MD = .27, p < .001). To get a full overview of the demographics at each time-point see Table 1 in Kaasbøll et al. (2021).
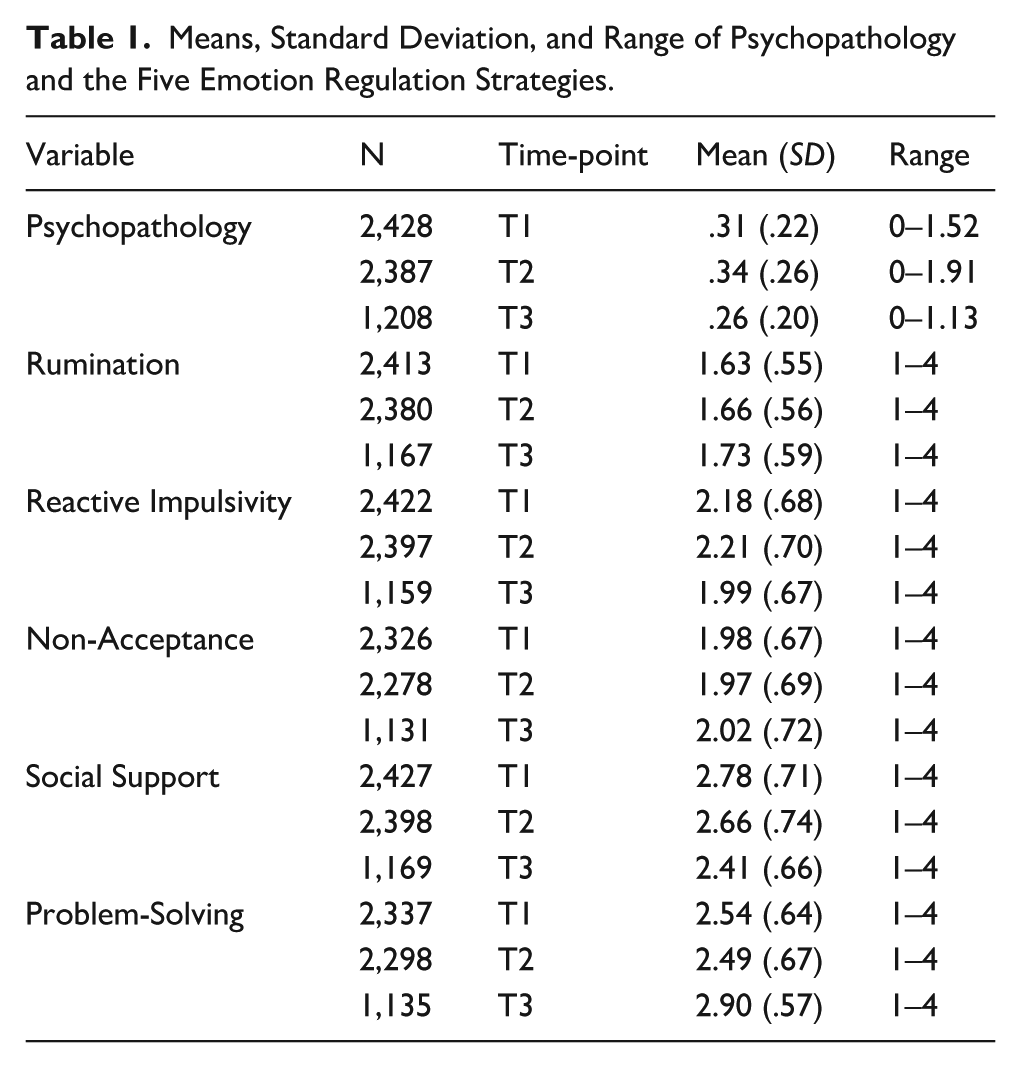
Means, Standard Deviation, and Range of Psychopathology and the Five Emotion Regulation Strategies.
Descriptive Statistics
Means, standard deviations (SD), and ranges of the variables are presented in Table 1. Correlations between each of the variables are presented in Figure 2.
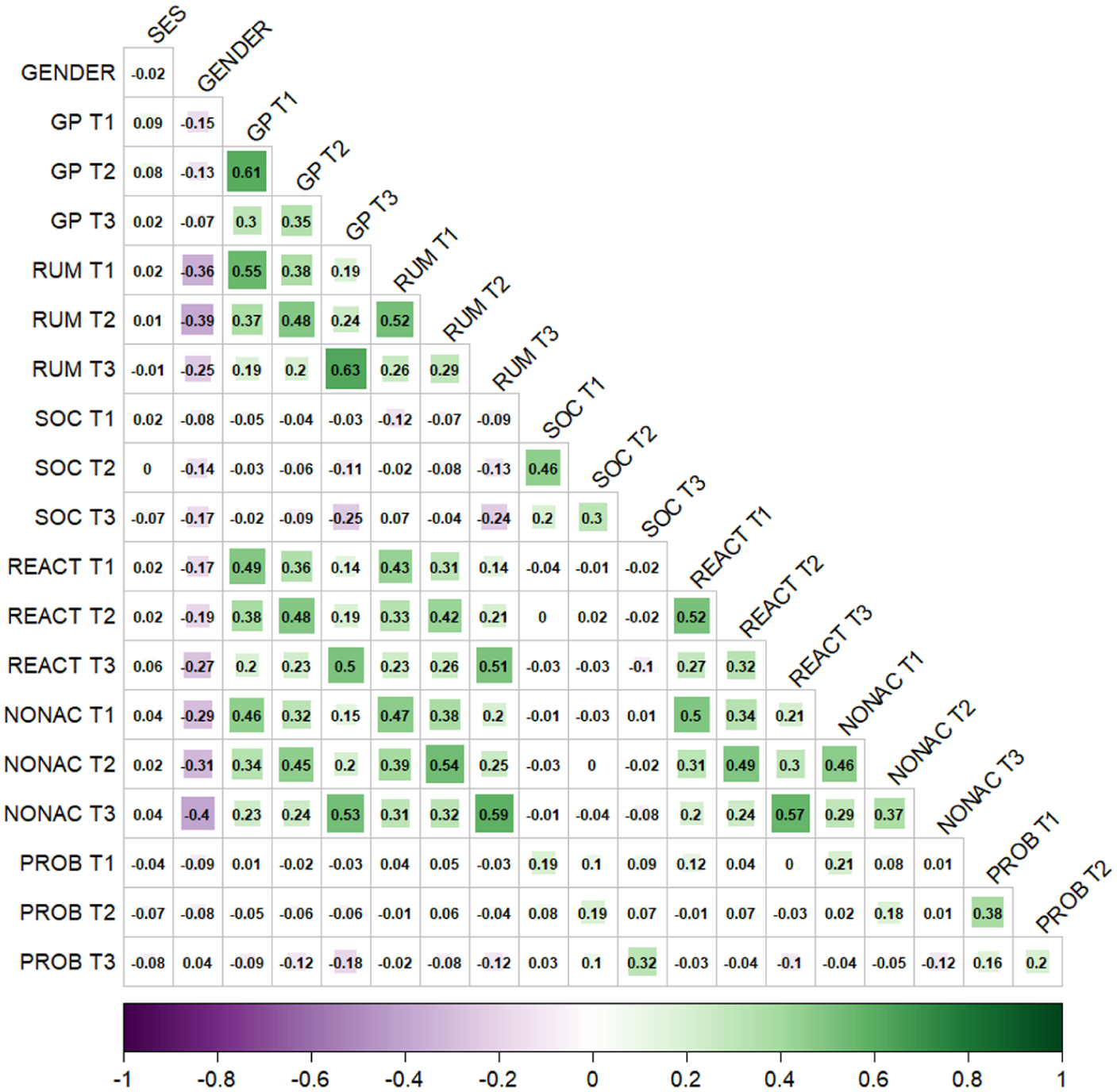
Correlations Between Each Emotion Regulation Strategy and General Psychopathology Within and Across Time. SES = Socioeconomic status. GP = General Psychopathology. RUM = Rumination. SOC = Social Support. REACT = Reactive Impulsivity. NONAC = Non-Acceptance. PROB = Problem-Solving. The number of participants per correlation ranged from 1,056 to 2,503. The lower end of participants belongs to correlations with T3 variables.
Random Intercept Cross-Lagged Panel Model
The RI-CLPM fitted the data well according to the fit indices, with CFI = .99, TLI = .93, RMSEA = .05, and SRMR = .019. All within-person estimates are reported in Table 2. See Figures 3 and 4 for a visual representation of the cross-lagged effects. Gender significantly predicted the observed variables, see Table S1 in Supplementary. We included separate models for each of the ER strategies and psychopathology in the Supplementary. The individual model findings replicated the associations in the complete model with one exception (more GP T2 predicted less PROB T3), see Supplementary for details.
Within-Person Estimates from the Random Intercept Cross-Lagged Panel Model.
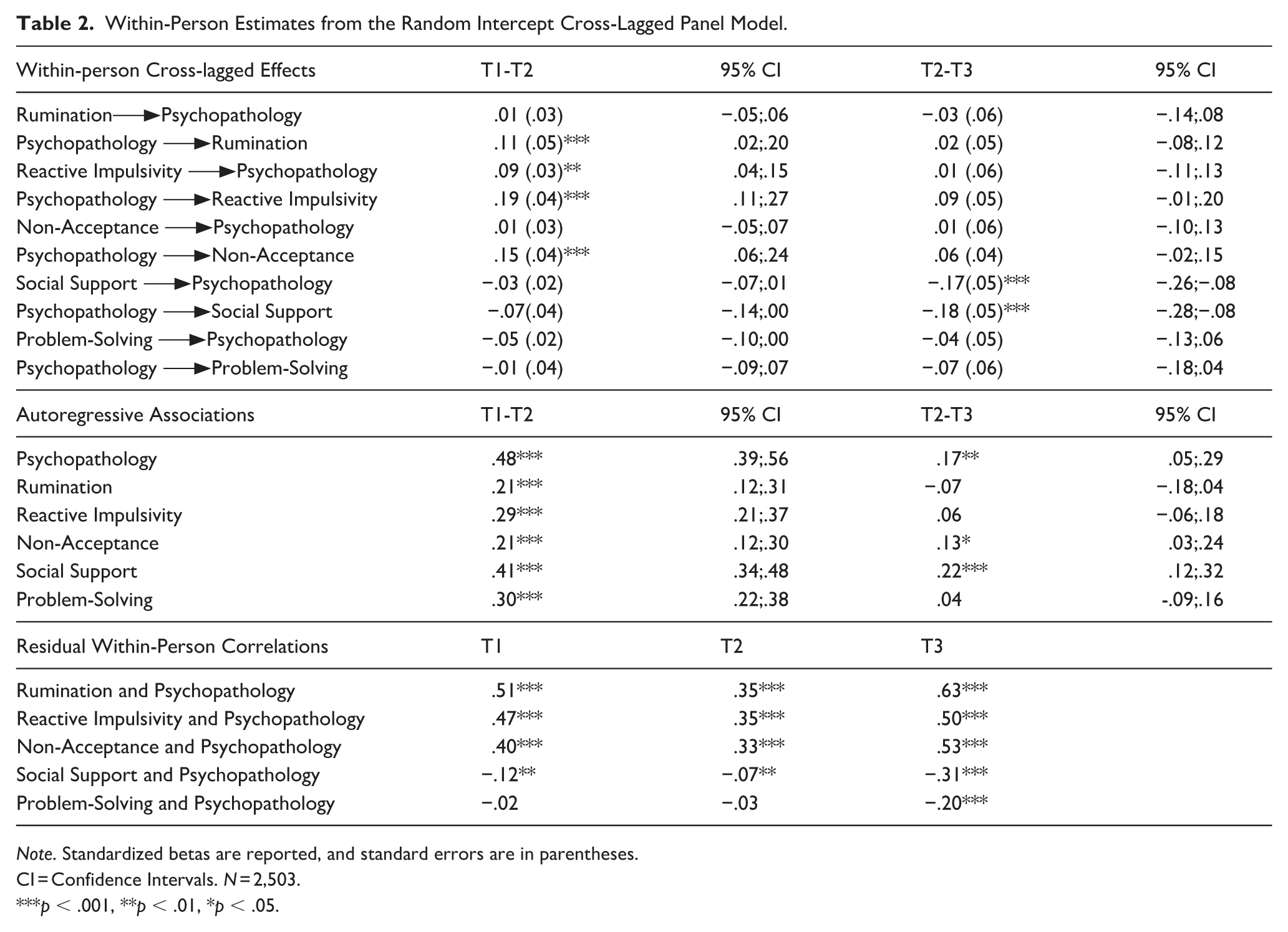
Note. Standardized betas are reported, and standard errors are in parentheses.
CI = Confidence Intervals. N = 2,503.
p < .001, **p < .01, *p < .05.
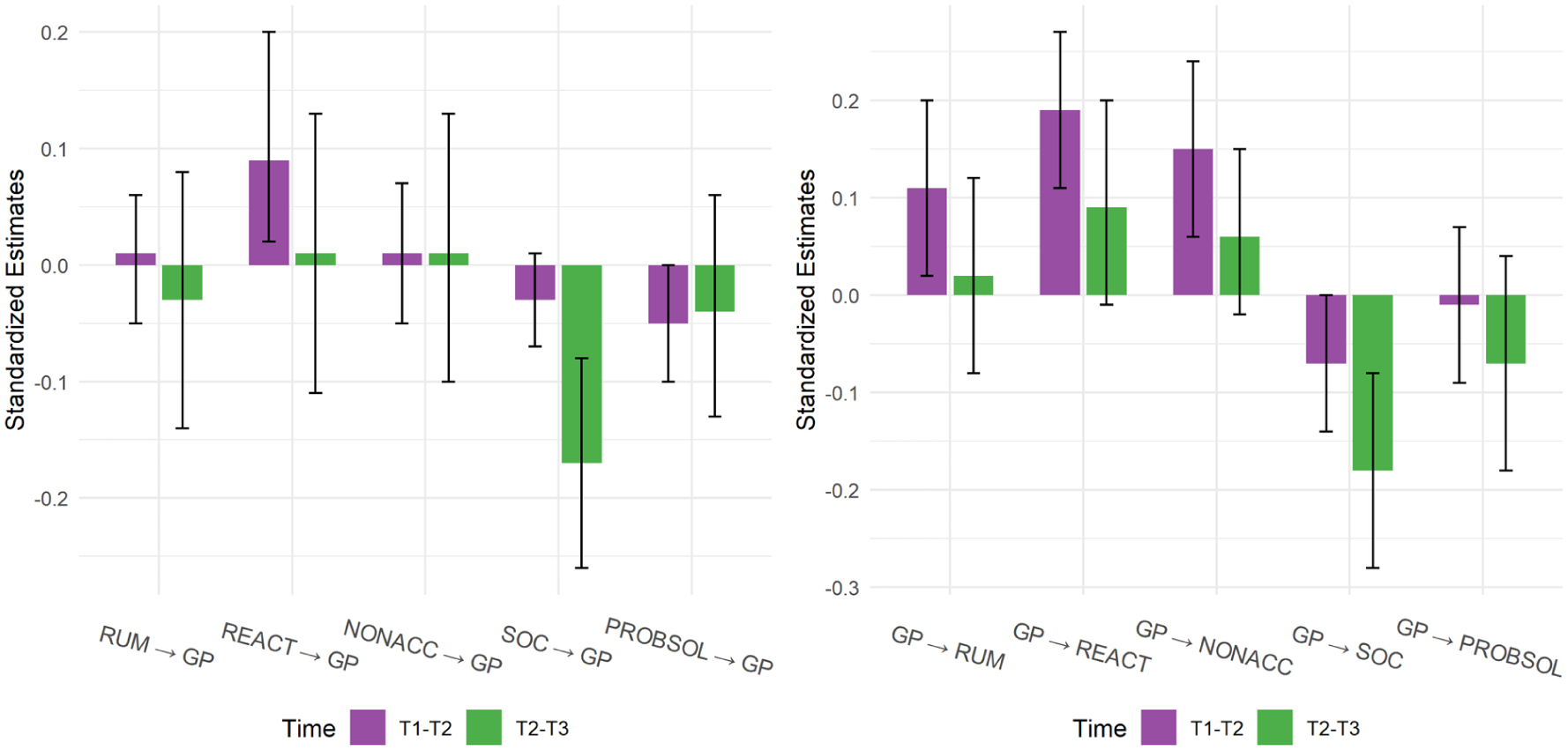
Bar Graph of the Cross-lagged Effects Between Emotion Regulation Strategies and General Psychopathology. The error bars represent the 95% confidence intervals. GP = General Psychopathology. RUM = Rumination. REACT = Reactive Impulsivity. NONAC = Non-Acceptance. SOC = Social Support. PROB = Problem-Solving. N = 2,503.
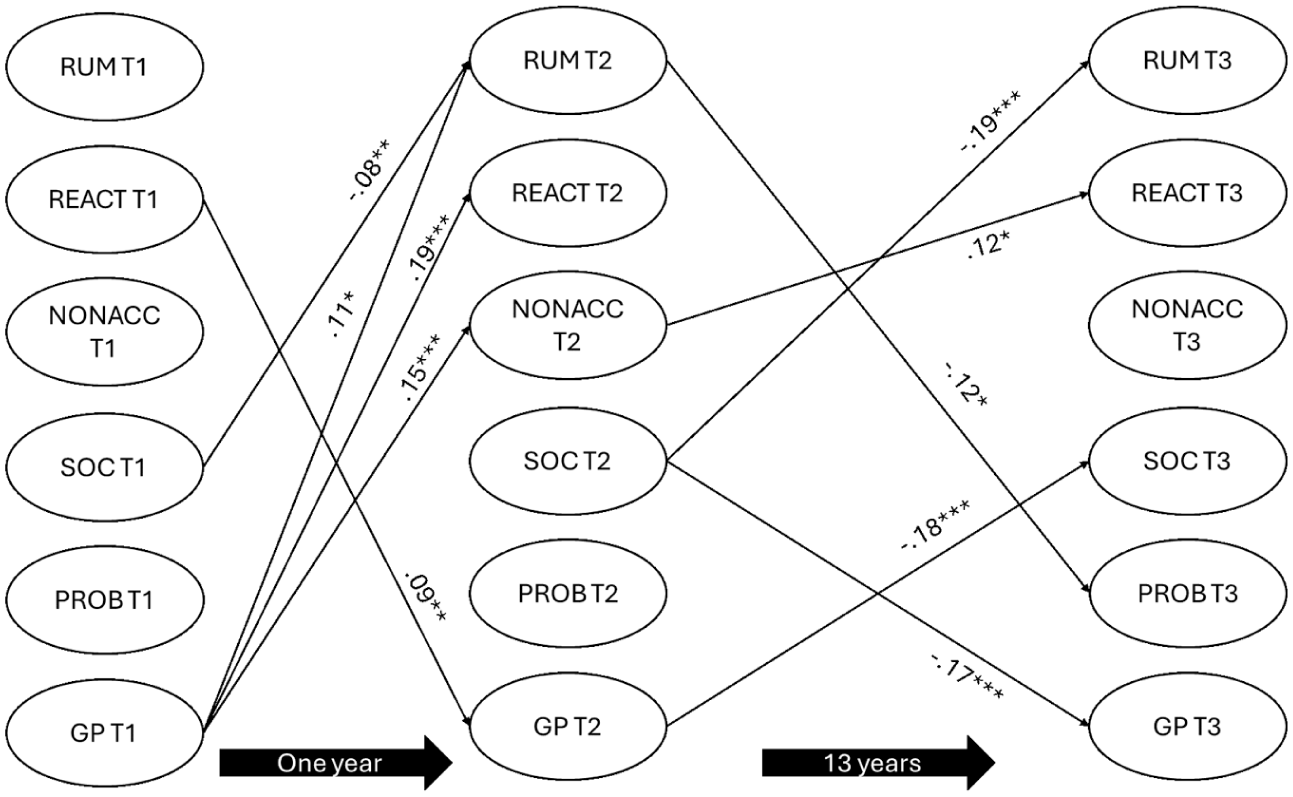
All Significant Within-Person Cross-Lagged Effects. The model allows for the ER strategies to predict each other; however, any of the significant effects across ER strategies are not of focus in this study. GP = General Psychopathology. RUM = Rumination. REACT = Reactive Impulsivity. NONAC = Non-Acceptance. SOC = Social Support. PROB = Problem-Solving.
Autoregressive Associations
All autoregressive associations for psychopathology, rumination, reactive impulsivity, non-acceptance, social support seeking, and problem-solving from T1 to T2 were significant, ranging from weak to moderate. This indicates significant carry-over effects during adolescence. From adolescence to adulthood (T2–T3), the only significant autoregressive associations were for psychopathology, social support seeking, and non-acceptance, of which were weakly associated. There were fewer carry-over effects across the 13 years between T2 and T3.
Residual (Concurrent) Correlations
We found substantial within-person correlations between several ER strategies and psychopathology at their respective time-points (see Table 2). At each time-point, deviations from an individual’s typical level of rumination, non-acceptance and reactive impulsivity were moderately to strongly correlated with deviations in psychopathology (rs = .33–.63). Deviations in social support were weakly correlated with deviations in psychopathology at T1 (r = −.12) and T2 (r = −.07) but showed a moderate correlation at T3 (r = −.31). Deviations in problem-solving were not significantly correlated with psychopathology at T1 nor T2 but were weakly correlated at T3 (r = −.20). These correlations indicate the extent to which ER and psychopathology co-develop, given the associations (or lack thereof) between the concurrent within-person deviations. See Table S2 for the correlations between the ER strategies.
One-Year Within-Person Cross-Effects
During adolescence, there were significant reciprocal effects between psychopathology and reactive impulsivity. Adolescents who experienced more symptoms of psychopathology than usual (a deviation from their average) at T1 were more reactive than usual a year later at T2, showing a large effect size (β = .19, p < .001). Adolescents who were more reactive than usual at T1 experienced more symptoms of psychopathology than usual a year later at T2, demonstrating medium effect sizes (β = .09, p = .002). No other reciprocal effects were observed. However, there were significant unidirectional cross-effects, such that adolescents who experienced more psychopathology than usual at T1 were more non-accepting of their emotions and ruminated more than usual a year later at T2 (β = .15, p < .001; β = .11, p = .001), demonstrating large and medium effects.
Within-Person Effects from Adolescence to Adulthood
From adolescence to adulthood, there were significant reciprocal effects between psychopathology and seeking social support. Adolescents who sought out more social support than usual at T2 experienced fewer symptoms of psychopathology than usual 13 years later during adulthood (β = −.17, p < .001). Adolescents who experienced more symptoms of psychopathology than usual sought out less social support than usual during adulthood (β = −.18, p < .001). Both associations had a large effect. No other significant reciprocal effects were observed.
Between-Person Associations
We found significant between-person (i.e., random intercept; RI) associations between ER strategies and psychopathology, see Table S3 in Supplementary. On average, rumination, reactive impulsivity, and non-acceptance were strongly correlated with psychopathology (rs = .51–.67, p < .05). Over the 14 years, individuals who reported a higher use of rumination, reactive impulsivity, and non-acceptance compared to others, also reported more symptoms overall. Average social support, and problem-solving were not correlated with psychopathology (p > .05). The average magnitude of observed variance explained by the RIs for psychopathology was 18% and for the ER strategies, it varied between 6% and 21%.
Discussion
Adolescence is a vulnerable developmental period characterized by a high incidence of symptom onset (Solmi et al., 2022). Transdiagnostic processes, such as ER, are thought to play an important role in the development and treatment of general psychopathology (Lincoln et al., 2022). However, while symptoms may also influence how individuals regulate their emotions, the impact of general psychopathology on ER strategies has been less explored regarding both short- and long-term effects. As both these phenomena fluctuate, it is essential to understand how changes in ER strategy use and psychopathology affect each other over time. In the current study, we investigated the possible reciprocal associations between five ER strategies and psychopathology during adolescence and from adolescence to adulthood. We investigated both within-person deviations (i.e., fluctuations from an individual’s average) and stable between-person associations while controlling for gender and previous time-points.
This study yielded several important findings. First, we found that within-person deviations in general psychopathology and some ER strategies are reciprocally and unidirectionally associated. While much of the literature emphasizes how ER strategies influence psychopathology (e.g., Aldao et al., 2010), some previous studies with adolescents have found internalizing symptoms to predict subsequent rumination (Royuela-Colomer et al., 2021) and negative self-beliefs (akin to our measure of non-acceptance; Harvey et al., 2021), but not impulsivity (Royuela-Colomer et al., 2021). Our findings indicate a more nuanced perspective and emphasize the broad risk of general psychopathology. Specifically, during adolescence, we find that more than usual general psychopathology predicted increased rumination, reactive impulsivity, and non-acceptance of emotions 1 year later. This suggests that transdiagnostic symptoms consisting of internalizing, externalizing, attention, and thought problems affect how adolescents think about and respond to their emotions in several maladaptive ways. Previous research has found that adolescents’ internalizing symptoms predict beliefs about not being able to change how they think, feel, and behave in response to their emotions (Schleider & Weisz, 2016). Perhaps what we are observing is that not only internalizing but also increased symptoms of general psychopathology affect how individuals think, feel, and behave in response to their feelings of sadness and distress. This may lead to an increased sense of helplessness regarding their emotional experiences, that is, feeling unable to change or influence their experiences. There is some support for this hypothesis, but for general ER difficulties and not individual strategies, where maladaptive thinking (e.g., feeling overwhelmed by not being able to control things) is associated with more difficulties with ER (Akbulut et al., 2025). In our study, increased general psychopathology may reflect such maladaptive thinking, resulting in a tendency to ruminate, react impulsively, and not accept difficult emotions.
Although some research has not found symptoms to predict impulsivity in adolescents (e.g., Royuela-Colomer et al., 2021), impulsivity has been linked to increased general psychopathology (Castellanos-Ryan et al., 2016). Our findings extend this work by demonstrating reciprocal associations; not only is more than usual reactive impulsivity associated with more than usual general psychopathology 1 year later, but more than usual general psychopathology also predicts more than usual reactive impulsivity a year later. To our knowledge, these reciprocal effects are novel. Prior research with children has identified reactivity as a risk factor for the development and maintenance of several symptom domains into adolescence (Forbes et al., 2017). Our results may therefore suggest that adolescents with heightened vulnerability to reactive responding are more likely to experience greater transdiagnostic symptoms during adolescence, and that these symptoms, in turn, continue to affect their reactive responses.
Seeking and receiving social support can be a helpful way to manage difficult feelings and situations during adolescence (Camara et al., 2017). Interestingly, we found no associations between seeking social support and psychopathology during adolescence. However, adolescents who sought out more social support than usual showed fewer symptoms of general psychopathology than usual during adulthood. It is unclear why seeking support is minimally associated with general psychopathology during adolescence, yet demonstrates protective long-term effects on psychopathology in adulthood. Generally, interpersonal relationships can serve as both protective and risk factors of psychopathology, depending on individuals’ own perception of the support they receive (Fleck et al., 2023). Adolescents and young adults who perceive greater social support or seek out advice tend to report lower levels of depression (Aldao & Dixon-Gordon, 2014; Rueger et al., 2016). In our study, more than usual social support seeking is a transdiagnostic protective factor as it extends to general psychopathology. We also find that more than usual psychopathology during adolescence predicted less social support seeking than usual during adulthood. Taken together, the findings suggest that those who report more transdiagnostic symptoms may become increasingly isolated or may have poorer experiences with seeking support (Lovén Wickman & Schmidt, 2023; Savaglio et al., 2023). In contrast, those who actively seek out support may develop skills and ways of coping that lead to less transdiagnostic symptoms later in life.
Second, by separating the between and within-person variances, we demonstrate stability across time such that, on average, individuals who have more symptoms of psychopathology tend to also regulate their emotions in unhelpful ways (e.g., rumination) across adolescence and into adulthood (between-person associations). However, given the unequal time intervals (1 year vs. 13 years), these RI associations should be interpreted with caution as they may not adequately reflect the trait-like differences between adolescence and adulthood. Conceptually, though, the RIs can still capture stable factors that influence the constructs (e.g., genetics; Mulder & Hamaker, 2021). Stable traits explained less than 21% of the observed variance in general psychopathology and ER strategies, suggesting that these processes are more dynamic than static. For general psychopathology, experiencing transdiagnostic symptoms in adolescence predicted more symptoms both a year later and in adulthood (the autoregressive effects). A similar pattern was found for social support seeking, which tended to carry over from adolescence into adulthood. Rumination, reactive impulsivity, non-acceptance, and problem-solving predicted greater use of these strategies 1 year later, but these carry-over effects were not observed from adolescence to adulthood. Such changes could be due to unmeasured contextual factors, such as environmental circumstances and events contributing to ER strategy use (Bonanno & Burton, 2013) and psychopathology. Overall, the carry-over effects highlight adolescence as a critical period when transdiagnostic symptoms and emotional responses are self-reinforcing; the more certain responses are practiced, the more likely they persist. Meta-analytical findings support the notion that transdiagnostic interventions have the potential to increase ER and decrease ER difficulties and symptoms (Espenes et al., 2024; Moltrecht et al., 2021); however, less is known about targeting-specific ER strategies (Lincoln et al., 2022).
Given the malleability of ER strategies, they are ideal to target in treatment and interventions. Based on our findings, we could suggest targeting adolescent reactive impulsivity through decentering, which is the practice of actively taking a step back from one’s emotions, allowing a person to reflect on what they are experiencing (Bennett et al., 2021). Decentering may help reduce strong and immediate physiological and emotional responses by de-identifying with the experience. There is research showing that decentering tendencies predict fewer depressive and anxiety symptoms in adolescents (Knight et al., 2025); however, there is a lack of studies investigating decentering with adolescents in an intervention setting (Bennett et al., 2021). Also, interventions could target rumination and non-acceptance by teaching mindfulness practices focused on observing thoughts and emotions that typically arise. By learning to observe, accept, and let go of repetitive negative thoughts and emotions, they may develop the ability to let them pass without judgment and not get caught up in their thoughts. This equips youth with tools to receive negative thoughts and emotions with openness and acceptance (Stein et al., 2022). In addition, given the long-term protective effects of social support seeking, this may be an avenue for prevention. We acknowledge, however, that expecting adolescents to initiate support seeking on their own can be challenging, particularly when the support they receive may not meet their needs (e.g., Savaglio et al., 2023). This underscores the importance of providing adequate social support training in schools and within families of individuals facing mental health difficulties (see Bauer et al., 2021). Ensuring that the most vulnerable adolescents receive sufficient support may encourage more help-seeking behaviors.
Third, the associations between rumination, reactive impulsivity, non-acceptance, and psychopathology raise the question of whether these constructs reflect overlapping phenomena. Their substantial correlations with each other within each time-point (rs = .33–.63), and their stability, suggest that they may co-develop. This in turn prompts further inquiry into the shared underlying mechanisms between these three ER strategies and general psychopathology. Research has found that impulsive responses, including both inactive (e.g., rumination) and active (e.g., lashing out) responses, neuroticism, and disordered thinking (Southward et al., 2019) are possible processes defining a general factor of psychopathology. In addition, one study that fitted a bi-factor model consisting of emotion dysregulation, self-regulation, internalizing and externalizing symptoms, found that the general factor explained between 52% and 58% of the variance and was predictive of later depressive symptoms during adolescence (Moltrecht, 2020). This may help explain why, in our study, psychopathology strongly predicts rumination, reactive impulsivity, and non-acceptance, suggesting that, at its core, general psychopathology may be defined by difficulties with ER (Deutz et al., 2020).
Strengths, Limitations, and Future Directions
A key strength of this study is its longitudinal design, which allowed us to follow the same individuals across pivotal adolescent years and into adulthood, capturing deviations in ER and psychopathology over time. However, the 13-year gap between the last adolescent and the subsequent adult assessment is longer than optimal, limiting our ability to capture developmental processes unfolding during the transition to adulthood. Moreover, there is an ongoing debate about the suitability of RI-CLPMs for such long intervals. Some argue long-term within-person deviations may be absorbed by the random intercept, thereby underestimating prospective effects (Orth et al., 2021). Others, however, emphasize that within-person fluctuations are always relative to the timescale under study, and that interpretation should therefore be guided by temporal theories of the investigated processes (Hamaker, 2023). More theoretical work on the temporal longitudinal dynamics linking ER and psychopathology is needed to better inform future longitudinal designs. Furthermore, mental health difficulties have increased in Norway since the period of data collection (Potrebny et al., 2025). The associations observed in this study may underestimate the associations between psychopathology and ER among today’s youth. Yet recent reviews highlight similar ER strategies as targets in current interventions (Helland et al., 2022; Saccaro et al., 2024), suggesting that the processes themselves remain relevant.
This study benefited from using measures that captured a wide range of symptoms to assess general psychopathology. Although we did not examine specific co-morbid conditions, we highlight the transdiagnostic nature of ER strategies by identifying within-person associations with general vulnerability. Another strength is the inclusion of multiple ER strategies. This enabled us to identify reactive impulsivity and social support seeking as particularly valuable targets for prevention and intervention, and to demonstrate the adverse effects of general psychopathology during adolescence, underscoring this developmental period as critical for intervention.
Another limitation concerns measurement. We used composite scores for both ER strategies and general psychopathology and did not account for measurement error. Attempts to model latent factors led to convergence issues, likely due to over-parameterization. Furthermore, the included ER strategies used in this study were developed and tested in previous work (Helland et al., 2024), but the original items stem from the coping literature. This raises the question of whether findings might differ with more mainstream ER measures. For example, our measure of non-acceptance focuses on self-blame and self-criticism in response to sadness, rather than directly assessing acceptance of emotional experiences. While we believe this measure captures the intended construct, some conceptual nuance may be lost. This reflects a broader challenge in the field: selecting appropriate ER measures given the diversity currently available (Mazefsky et al., 2021).
Conclusions
Our findings highlight transdiagnostic processes during adolescence, showing reciprocal associations between psychopathology, reactive impulsivity, and seeking social support. Interventions targeting these ER strategies during the adolescent years could prove useful for reducing symptoms of general psychopathology and particularly supporting adolescents through difficult feelings, as a preventive measure against future symptoms. We expand the transdiagnostic framework of ER by highlighting the adverse effects of general psychopathology on both adolescents’ and adults’ ER responses. In addition, we demonstrate that psychopathology and ER strategies show both stability and change, with more evidence for the latter. Prevention may be particularly important; by improving adolescents’ ER strategy tendencies, we may be able to tackle poor emotional responses before adolescents are impacted by their mental health difficulties.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254251401322 – Supplemental material for Reciprocal associations between general psychopathology and emotion regulation from adolescence to adulthood
Supplemental material, sj-docx-1-jbd-10.1177_01650254251401322 for Reciprocal associations between general psychopathology and emotion regulation from adolescence to adulthood by Emily G. Vira, Ragnhild B. Nes, Jannike Kaasbøll, John Kjøbli, Espen Røysamb and Siri S. Helland in International Journal of Behavioral Development
Footnotes
Acknowledgements
I would like to thank all the participants who gave their time to the YAMHS project, and I would like to thank the original principal investigators who designed and executed YAMHS. Thank you to all the funding agencies, past and present, who provided the means for this project and study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Council of Norway (EGV, JK, SSH, grant number 326941, RBN, ER, grant number 288083).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.