
Abstract
Grandmothers are influential caregivers for young children, yet their contributions to child development remains understudied. This study characterized trajectories of grandmother caregiving from infancy to 2 years and examined their associations with child development. Data came from a longitudinal birth cohort study in rural Pakistan (n = 959). Grandmother caregiving behaviors were maternally reported at 3 months, 1 year, and 2 years postpartum using a 24-hour recall. Child development (cognitive skills, socioemotional development, and mental health) outcomes were assessed at 6 years. We found 4 distinct grandmother caregiving trajectories during infancy: (1) Low (34.9%), (2) Unstable Medium (9.3%), (3) Stable Medium (40.8%), and (4) High (14.9%). Early life grandmother caregiving trajectories longitudinally predicted specific developmental domains in middle childhood. Children with grandmothers in the High trajectory group had higher inhibitory control, and children with grandmothers in the Unstable Medium group had greater socioemotional problems. No meaningful differences with verbal comprehension, working memory, or anxiety scores were observed. Future research should characterize key family members’ caregiving patterns throughout childhood to capture the dynamic nature of caregiving. In addition to parents, interventions that engage grandmothers may help create a cohesive caregiving environment and improve child development.
Keywords
Introduction
Across many societies, and particularly in low- and middle-income countries (LMICs), multiple caregivers other than biological parents are involved in raising children, such as grandmothers (Sear, 2021). Globally, extended lifespans and demographic changes in family arrangements (e.g., increased maternal employment and multigenerational households) have underscored the caregiving roles of grandmothers (Bol & Kalmijn, 2016; Dunifon, 2013; Mehta & Thang, 2011). Across settings, grandmothers are influential for women and children, serving as designated advisors, caregivers, and powerful decision-makers on maternal and child health issues (Aubel, 2012, 2021). Despite being a key member of the family system, grandmothers’ contributions to child cognitive and socioemotional development have been largely overlooked (Smith & Wild, 2019).
Grandmothers as Alloparents
Family systems theory underscores the family as a social system, which has its own rules and norms around roles, responsibilities, communication, and social status (Cox & Paley, 1997; Olson, 2000; Parke, 2004). Understanding grandmother contributions to children’s development requires understanding the social and cultural contexts. Most existing studies on grandmothers have been conducted in WEIRD (Western, Educated, Industrialized, Rich, and Democratic) countries (Henrich et al., 2010), such as the United States, where the nuclear family system is normative and grandmothers often serve as custodial caregivers for children only when parents have negative life events, such as illness, divorce, or incarceration (Smith & Wild, 2019). Outside of WEIRD settings, studies on grandmothers are primarily conducted in contexts with skipped-generation families, such as China where grandmothers typically serve as primary caregivers for “left-behind” children in rural areas while parents migrate to urban areas for better employment opportunities (Fellmeth et al., 2018).
In contrast, in non-WEIRD, multigenerational contexts, joint and extended family systems are normative and alloparenting—cooperative care for children by individuals other than biological parents—is common, with grandmothers serving as the most common alloparent (Sear, 2016). Grandmothers often have high social status within families given their roles as advisors to younger women and transmitters of sociocultural knowledge and traditions (Aubel, 2012, 2021). In such family systems, childrearing is culturally shared among alloparents and there is often great overlap in the caregiving roles and responsibilities between parents and grandparents (Hoang & Kirby, 2020). In families with substantial alloparenting, children may form strong attachment relationships with multiple people, including grandmothers (Meehan & Hawks, 2014). However, few studies on grandmothers have been conducted in non-WEIRD, multigenerational contexts.
Pakistani Context
In Pakistan, over 60% of children live in joint and extended family systems (National Institute of Population Studies & ICF, 2019). Patrilocal customs dictate that married women to move into the husband’s homes, which often includes co-resident in-laws. Thus, paternal grandmothers are more often involved in the daily lives of mothers and children compared to maternal grandmothers. Childrearing is a communal responsibility among multiple family members (Zaman, 2014) and grandmothers typically serve as secondary caregivers, providing additional support to mothers and fathers (Babu et al., 2017). The extent to which grandmothers are involved in child rearing may differ by family-level factors, such as family system structure (e.g., nuclear vs. joint/extended) or household income. Given larger family systems, grandmothers are often responsible for multiple children at a time, typically between 1 and 4 (Rahat et al., 2023). Prior studies in Pakistan found grandmothers engage in instrumental care for young children, such as feeding, bathing, and play, as well as serve in disciplining, comforting, and teaching manners and family values to children (Babu et al., 2017; Chung et al., 2020; Hoang & Kirby, 2020; Lingam et al., 2014). Furthermore, the level of grandmother involvement was positively associated with children’s cognitive and socioemotional development (Chung et al., 2020) and higher emotional closeness with grandparents helped buffer against negative associations between parental authoritativeness and adolescent social skills (Akhtar et al., 2017).
Measuring Grandmother Caregiving Behaviors
As a primary alloparent, grandmothers may serve as important sources of cognitive stimulation or social and emotional support to young children and may alleviate stress in the family system by providing additional resources or support, particularly to mothers (Aubel, 2021). Studies in LMICs have documented the influential roles of grandmothers in the first 2 years of life, primarily in infant feeding practices by shaping maternal breastfeeding behaviors and directly engaging in complementary feeding to young children (Aubel, 2012; Martin et al., 2021). Additional studies have found grandmothers engage in many behaviors that promote cognitive and socioemotional development, such as playing, soothing, and singing (Chung et al., 2020; Hollowell et al., 2019; Sichimba et al., 2017; Yue et al., 2019). However, most existing quantitative research on grandmothers in LMICs have operationalized caregiving as contact or presence—whether she is alive or living with the grandchild (Gibson & Mace, 2005; Masvie, 2006; Pulgaron et al., 2016; Reynolds et al., 2018; Schrijner & Smits, 2018a, 2018b; Scott et al., 2018). Such indicators limit our understanding because they do not capture actual caregiving behaviors. In multigenerational, family systems, grandmother co-residence with grandchildren is highly prevalent. Therefore, measuring grandmother caregiving behaviors is important to understand intensity and type of grandmother involvement.
Longitudinal Patterns of Grandmother Caregiving
Grandmother caregiving behaviors will change across a child’s life course. Some of these changes are in response to developmental aging of children. For instance, grandmothers may be more involved in early life, providing instrumental care (e.g., complementary feeding) and socioemotional care (e.g., soothing infants). As children transition to school, grandmother care may adapt to behaviors like teaching values, passing down cultural knowledge, and disciplining children. In addition, in multigenerational family systems, grandmother caregiving for a specific child may change over time for multiple reasons, such as changes in her own health, transitions in family structures (e.g., a multigenerational household to a nuclear system or vice versa) or shifts in a grandmother’s attention (e.g., a newborn infant, a family member with a serious illness).
Assessing longitudinal patterns of grandmother caregiving may help identify whether specific patterns are associated with children’s development. For instance, unstable patterns (e.g., decreasing intensity of care) or stable patterns of low intensity care may be negatively associated with children’s cognitive and socioemotional development whereas stable patterns of high intensity care may be positively associated. Disruptions in care stemming from family instability (e.g., serious illness, divorce, or conflict) negatively impacts children’s cognitive and socioemotional development (Lee & McLanahan, 2015; Waldfogel et al., 2010). Chronically elevated trajectories of family instability in early childhood have been associated with greater externalizing behaviors in middle childhood and adolescence (Womack et al., 2022) as well as slower progress in math and reading performance in middle childhood (Y. Sun & Li, 2011).
Extrapolating from this research, it may be that different patterns of grandmother caregiving in early life may affect child development later. Yet, to our knowledge, there have only been two studies that have characterized patterns in grandparent caregiving, one in China and another in Korea (Li et al., 2022; Park, 2022). Using trajectory analyses, researchers identified 5 and 3 distinct trajectories in China and Korea, respectively, that characterized various decreasing and increasing patterns. While these studies demonstrate grandparent caregiving patterns change over time, neither study reported specific ages of grandchildren, which influences the intensity and type of involvement, nor examined whether the caregiving trajectories were related to child outcomes. Capturing the potential dynamic changes in grandmother caregiving behaviors may help identify important longitudinal patterns of care.
Grandmother Caregiving and Child Outcomes
Given grandmothers’ diverse roles in instrumental and socioemotional care (Hoang & Kirby, 2020), examining multiple child developmental domains is important. Grandmothers may engage in behaviors that promote specific developmental domains. For instance, grandmothers often teach social and cultural values to young children, such as patience, morals, and family cohesion, which may support socioemotional development (Babu et al., 2017; Shwalb et al., 2019; Tan et al., 2024). Grandmothers who play and sing with young children may promote certain cognitive domains over others. The relationships between grandmother involvement and cognitive and socioemotional development are mixed (Sadruddin et al., 2019). Therefore, it is important to consider how distinct patterns of grandmother care affect different developmental domains. Yet, to our knowledge, no studies to date have examined longitudinal associations between grandmother caregiving patterns and child cognitive and socioemotional development.
Present Study
We conducted an exploratory analysis to understand how grandmother caregiving across the first 2 years of life relates to children’s development using a longitudinal birth cohort in rural Pakistan. We aimed to (1) characterize grandmother caregiving trajectories from 3 months to 2 years, and (2) examine longitudinal associations between early-life grandmother caregiving trajectories and child development at 6 years. Informed by previous empirical work (Li et al., 2022; Park, 2022), we expected to find increasing, decreasing, stable grandmother caregiving patterns across the first 2 years of life. Within the stable caregiving patterns, we expected to find low and high caregiving trajectories based on prior studies (Chung et al., 2020). We hypothesized more optimal cognitive and socioemotional child development outcomes among increasing and higher stable grandmother caregiving groups compared to decreasing or lower stable groups.
Methods
Participants
Data came from the Bachpan Cohort, a birth cohort with an embedded perinatal depression intervention in rural Pakistan. Briefly, all women in the third trimester of pregnancy across 40 village clusters were screened for depression using the Patient Health Questionnaire (PHQ-9) (Gallis et al., 2018). Depressed women (PHQ-9 ⩾ 10) were overrepresented and randomized to control or intervention trial arms. Approximately 1 out of every 3 non-depressed women (PHQ-9 < 10) from the same village cluster was enrolled in the cohort follow-up. All survey measures were interviewer-administered, either verbally in Urdu or by observation. Further details can be found elsewhere (Maselko et al., 2020; Sikander, Ahmad, Bates, et al., 2019). Mothers (n = 1,154) were enrolled in the third trimester of pregnancy (baseline). The current analysis used follow-up data when children were 3 months and 1, 2, and 6 years old. Of the 1,154 families, 195 (16.9%) were missing data on grandmother caregiving (Supplemental Appendix Figure 1). We used available data on the remaining 959 families to identify distinct grandmother caregiving trajectories. Of the 959 families, 131 (13.7%) were missing data on covariates or outcomes. We estimated associations between grandmother caregiving trajectories and child development on the remaining 828 families, accounting for potential bias due to missing data with inverse probability missingness weights (IPMW; further details below in Statistical Analysis). Ethical approval was obtained from the Human Development Research Foundation in Pakistan (IRB/1017/2021) and the University of North Carolina at Chapel Hill (#20-1433).
Measures
Grandmother Caregiving
We measured grandmother involvement in caregiving behaviors at 3 months and 1 and 2 years using the “Day-in-the-Life” (DIL) (O’Donnell et al., 2022). Mothers were guided through open-ended prompts to describe the past 24 hours of their child’s life, focusing on who provided care to the child throughout the day. Interviewers recorded household members’ participation in 20 specific caregiving behaviors across three domains: instrumental (e.g., feeding and bathing); social/socioemotional (e.g., playing and soothing); and support (e.g., caregiving support when mother was unwell) (for the full interview, see O’Donnell et al., 2022). Drawing from theoretical perspectives on intergenerational coparenting in multigenerational contexts (Bai et al., 2023) and consistent with previous work (Chung et al., 2020, 2022), we operationalized grandmother caregiving as a composite score, summing across the 20 caregiving behaviors for each timepoint, to represent global grandmother caregiving involvement. Internal consistencies were α = 0.87 (3 months), α = 0.94 (1 year), and α = 0.90 (2 years). In addition, we sought to characterize overall grandmother caregiving over the first 2 years of life, regardless of origin and co-residence; thus, we combined paternal and maternal grandmothers into a total grandmother score (range: 0–40). Prior work did not find meaningful differences in child outcomes by paternal vs. maternal grandmother at these same timepoints (Chung et al., 2020).
Child Outcomes
All measures were previously translated, adapted to account for cultural and linguistic differences, used by the research team in the study area, and assessed at 6 years. Details on the adaptation process have been published elsewhere (Maselko et al., 2015). We used the Weschler Preschool and Primary Scale of Intelligence (WPPSI-IV) (Wechsler & Psychological, 2012) to measure verbal comprehension, vocabulary, and working memory. Trained interviewers administered four subtests: Information, Similarities, Vocabulary, and Picture Memory. We summed the scaled Information and Similarities subscores to create the Verbal Comprehension Index (range: 0–38) and used scaled WPPSI subscores for Vocabulary and Picture Memory (ranges: 0–19). Internal consistencies were α = 0.77 (Information), α = 0.91 (Similarities), α = 0.86 (Vocabulary), and α = 0.90 (Picture Memory). Interviewers also administered the Stroop Day-Night Task to measure inhibitory control (Gerstadt et al., 1994). Children were shown two cards, one with a sun (day card) and another with a moon (night card) and instructed to say “Night” when the day card was shown and “Day” when the night card was shown. We used the total number of correct responses from 16 trials (range: 0–16; α = 0.94).
We used the Strengths and Difficulties Questionnaire (SDQ) to capture parent-reported behavioral and emotional problems and prosocial behaviors (Goodman, 1997). Mothers responded to 25 items across 5 domains: Emotional problems, Conduct problems, Peer problems, Hyperactivity, and Prosocial Behaviors. Response options were Never True (0); Somewhat True (1); Certainly True (2). Positively worded items that were not on the Prosocial scale were reverse coded. We calculated the SDQ Total Difficulties score (SDQ-TD), where higher scores indicate greater difficulties (range: 0–40; α = 0.65), and the Prosocial score, where higher scores suggest more positive behaviors (range: 0–10; α = 0.69). While internal consistency was modest, the SDQ remains a widely used instrument for behavioral screening, with prior reviews supporting its use across cultures and populations (Stone et al., 2010). The SDQ has been validated in Pakistan (Samad et al., 2006) and previously used in the study area (Maselko et al., 2015). We also used the Spence Children’s Anxiety Scale (SCAS) to measure parent-reported anxiety (Spence, 1998). We used the 6-item generalized anxiety subscale (e.g., “My child worries about things.”). Response options were Never (0); Sometimes (1); Often (2); Always (3). We summed the items, where higher scores indicate greater anxiety (range: 0–16; α = 0.63).
Covariates
We used directed acyclic graphs (DAG) to identify appropriate confounders to estimate the total association of grandmother caregiving trajectories on child development (Glymour & Greenland, 2008). We used sociodemographic information collected at baseline, including maternal age (standardized), education (none, primary to middle (1–8 years), secondary or higher (9+ years)), parity (first-time mother vs. one or more children), current major depressive episode (yes/no using the Structured Clinical Interview for DSM-IV Disorders (SCID)), maternal perceived stress using Cohen’s Perceived Stress Scale (Cohen et al., 1994), and any intimate partner violence (IPV) in the past year (yes/no using the WHO Violence Against Women instrument; World Health Organization, 2005).
We also included child gender (boy/girl), whether the husband travels for work (yes/no to being continuously away for more than a month at a time), household structure (nuclear vs. joint/extended), household size, socioeconomic status (SES) asset index, family conflict (yes/no), and trial arm (control, intervention, and non-depressed). SES was operationalized as an asset index using principal components analysis (Maselko et al., 2018). Family conflict was operationalized as any endorsement of the following Life Events Checklist items (Brown & Harris, 1989): In the last year, (1) “You or other family members have had rows/quarrels among themselves,” (2) “Your relations with any of your close relatives or friends have been troubled,” and (3) “Your marital relations with your spouse have had problems.” We were unable to include mother or father involvement as covariates given minimal variation (Supplemental Appendix Table 2). However, we included the average number of caregivers, calculated as the total number of caregivers reported in the DIL and averaged across 3 months and 1 and 2 years (range: 0–10).
Statistical Analysis
Identification of Trajectories
Using group-based trajectory modeling (GBTM) (Nagin & Odgers, 2010), we identified similar trajectories of grandmother caregiving across 3 months and 1 and 2 years based on the DIL total score. GBTM can identify latent subgroups of individuals who share similar patterns of grandmother caregiving and allows us to capture both stability and intensity over time. We included those with at least two DIL measures across 3 months and 1 and 2 years (n = 959). Following recommendations by Nagin and Odgers (2010), we first identified the appropriate number of trajectories by exploring 1, 2, 3, 4, and 5 class models using Bayesian Information Criteria (BIC) for model selection. We then determined the shape of each trajectory by exploring intercept-only, linear, quadratic, and cubic functional forms based testing all combinations for the best fitting line. Finally, we used posterior probabilities of group membership to assess the final model, which included 4 trajectories, each with a linear functional form, (Nagin & Odgers, 2010). We ran all GBTM with the traj macro in Stata using a censored normal distribution and sampling weights (Jones & Nagin, 2013).
Grandmother Caregiving Trajectories and Child Outcomes
To estimate the associations between grandmother caregiving trajectory membership and child outcomes, we conducted weighted linear regressions, accounting for sampling and potential selection bias due to missingness. We conducted separate models for each child outcome because we hypothesized grandmother caregiving may have differential associations with child cognitive and socioemotional domains. As described above, we used DAGs to identify appropriate confounders. We included child gender, maternal age, education, parity, any IPV, depression, perceived stress, whether the husband travels for work, average number of caregivers, household size, nuclear family, and SES asset index. We included a squared term for maternal age and interaction terms between grandmother caregiving trajectory group and the following covariates: maternal education, depression, child gender, and family conflict. We obtained average marginal mean differences (MD) and 95% confidence intervals (CI) using the margins command in Stata.
All analyses and descriptive statistics used cluster-specific sampling weights. To account for potential selection bias due to loss-to-follow-up and missingness, we used IPMW, which creates a pseudo-population whereby observed individuals are weighted to represent the starting population (non-missing and missing) based on observed characteristics (Seaman & White, 2013). Given we had nonmonotonic missing data, we employed the unconstrained maximum likelihood estimator (Supplemental Appendix Methods 1) (Ross et al., 2022; B. Sun et al., 2018). Sampling weights and IPMW were multiplied together and used in weighted linear regressions. Robust variances were used to account for clustering and weights. We performed analyses using Stata 14 and R (4.1.0).
Sensitivity Analyses
We conducted multivariable sensitivity analyses to (1) assess modification of grandmother caregiving trajectories and child outcomes by child gender; (2) explore whether children’s cognitive and socioemotional outcomes at 6 months and 1 year predicted future grandmother caregiving at 2 years; and (3) assess whether interviewer effects substantially changed our estimates. Further details regarding selection of these sensitivity analyses, methods, and results can be found in Supplemental Appendix Sensitivity Analyses 1.
Results
Among 959 families included in our analysis, mothers were, on average, 27 years (Table 1). Almost half of mothers had not completed secondary education and 31% were in their first pregnancy. The average household size was 9 and 2/3 were living in joint or extended households. In 70% of households, grandmothers were co-residing with the index child and 36% of mothers reported some form of family conflict. A quarter of women had a current major depressive episode and 41% experienced IPV in the past year.
Sample Characteristics of Households Included in Group-Based Trajectory Analysis, Bachpan Cohort, Rural Pakistan (n = 959).
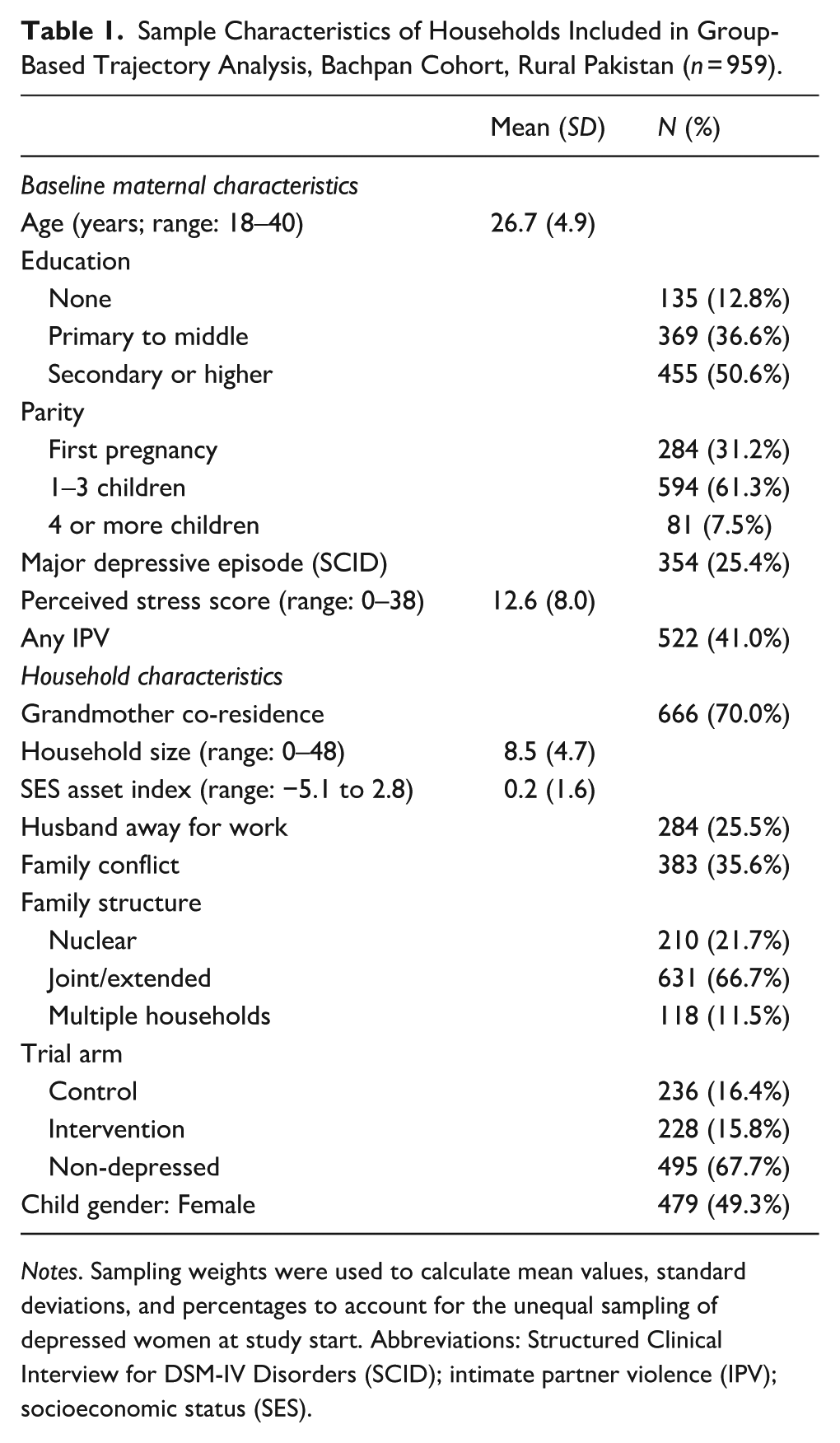
Notes. Sampling weights were used to calculate mean values, standard deviations, and percentages to account for the unequal sampling of depressed women at study start. Abbreviations: Structured Clinical Interview for DSM-IV Disorders (SCID); intimate partner violence (IPV); socioeconomic status (SES).
Grandmother Caregiving Trajectories
Grandmother caregiving was measured at 3 months and 1 and 2 years of age. We found 4 distinct trajectories of grandmother caregiving engagement: (1) Low (34.9%), (2) Unstable Medium (9.3%), (3) Stable Medium (40.8%), and (4) High (14.9%) (Figure 1). The average posterior probabilities of membership into each group were 0.92, 0.75, 0.85, and 0.78, respectively, suggesting adequate modeling of trajectories (Nagin & Odgers, 2010).
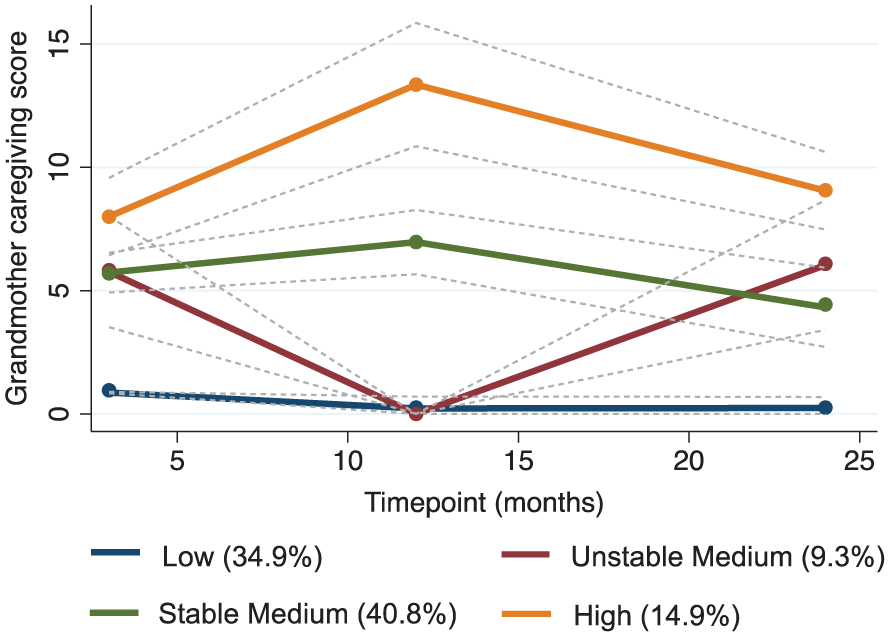
Grandmother Caregiving Trajectories Among Families in rural Pakistan, Bachpan Cohort (n = 959).
Table 2 describes caregiving scores over time stratified by trajectories. In the Low group, the mean caregiving scores were roughly 0–1 activities from 3 months to 2 years. The Unstable Medium group had an average of 6.4 activities (4.2) at 3 months, a drop to 0 at 1 year, and an increase to 6.4 (3.8) at 2 years. In the Stable Medium group, grandmothers participated in roughly 4–7 activities on average (3 months : 5.6 (3.3); 1 year: 7.3 (3.3); 2 years: 4.3 (3.4)). In the High group, the mean scores were between 8 and 11 activities from 3 months to 2 years. Across all trajectories, mothers reported paternal grandmothers engaging in caregiving more often than maternal grandmothers across the first 2 years of life (Supplemental Appendix Table 2). Further details on each caregiving behavior stratified by trajectory group are in Supplemental Appendix Table 2.
Sample Characteristics Across Grandmother Caregiving Trajectory Groups, Bachpan Cohort, Rural Pakistan (n = 959).
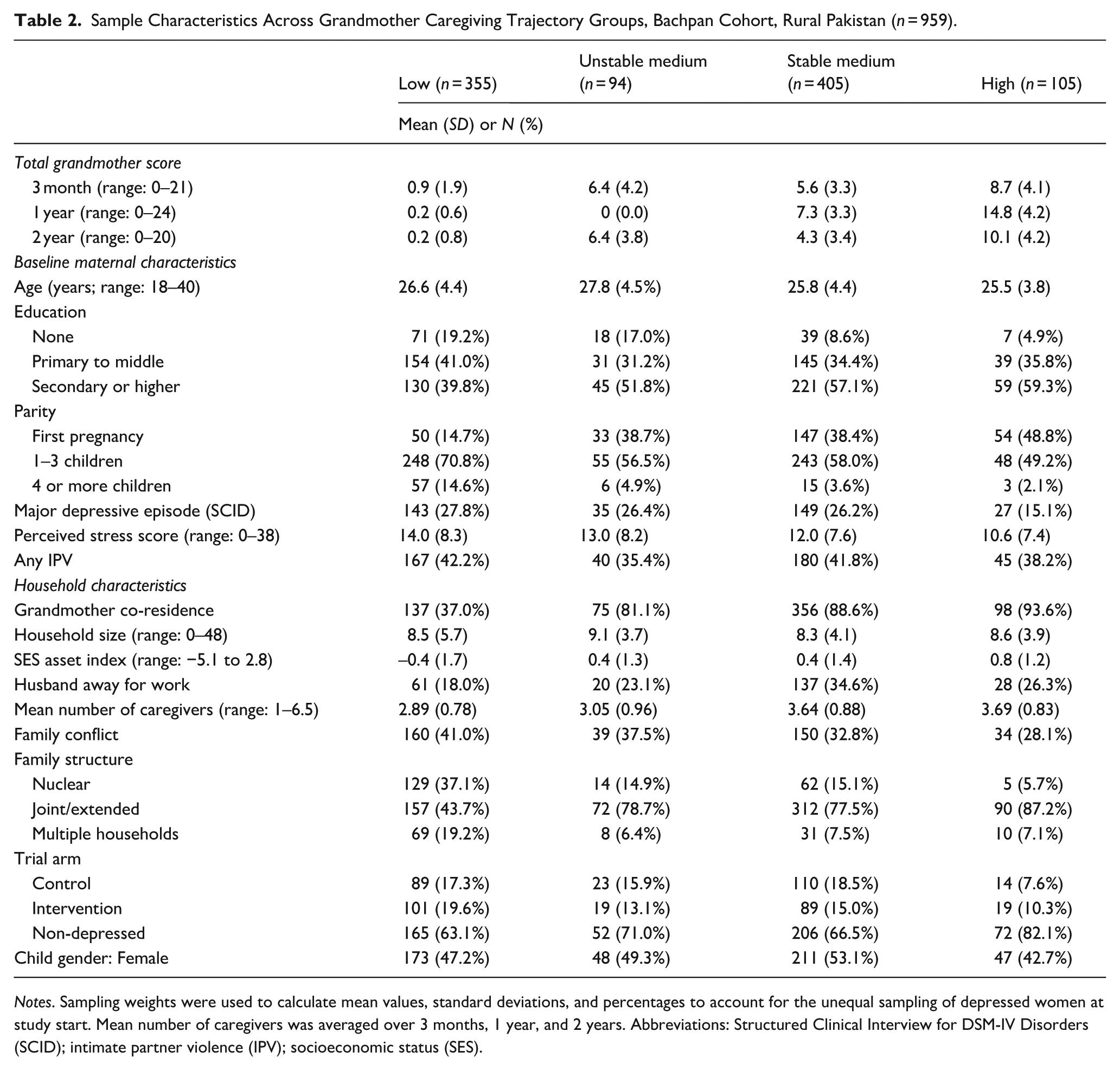
Notes. Sampling weights were used to calculate mean values, standard deviations, and percentages to account for the unequal sampling of depressed women at study start. Mean number of caregivers was averaged over 3 months, 1 year, and 2 years. Abbreviations: Structured Clinical Interview for DSM-IV Disorders (SCID); intimate partner violence (IPV); socioeconomic status (SES).
Sociodemographic Differences Between Trajectories
Compared to families with grandmothers assigned to the Low and Unstable Medium groups, those with grandmothers in the Stable Medium and High caregiving trajectories had higher maternal education, household SES asset index, and grandmother co-residence as well as lower prevalences of maternal depression, perceived stress, and family conflict (Table 2). Across the cohort, when grandmothers were involved in early life, they were, on average, 1 of the 4 caregivers. Aside from mothers, other commonly reported caregivers included paternal grandmothers, aunts/uncles, fathers, and siblings. The mean number of caregivers averaged over the 3 timepoints increased from the Low group to the High group. Further details on these differences are in Supplemental Appendix Table 3.
The distinct feature of the Unstable Medium group was the drop to 0 activities at 1-year postpartum. Given this was an unexpected finding, we descriptively compared characteristics across trajectories at 1 year (Supplemental Appendix Table 4). In general, families with grandmothers in the Unstable Medium group were similar to the Stable Medium group in terms of maternal parity, depression, perceived stress, grandmother co-residence, household SES, and family structure, but they had larger households (9.1 (3.7)), primarily due to a greater number of extended family members, such as sisters-in-law and cousins. Compared to other groups, mothers in the Unstable Medium group reported a greater number of household changes and household stressors at 1-year postpartum (Supplemental Appendix Table 4). For example, a greater percentage of mothers in the Unstable Medium group had additions to their families (56.4% vs. 26.4%, 14.3%, and 13.2% in the Low, Stable Medium, and High groups, respectively), serious illness of a family member (20.4% vs. 20.5%, 16.6%, and 18.9% in the Low, Stable Medium, and High groups, respectively) and experienced troubled relations with close relatives or friends (15.8% vs. 14.4%, 8.4%, and 8.4% in the Low, Stable Medium, and High groups, respectively).
Associations Between Grandmother Caregiving Trajectories and Child Outcomes
We present our findings on the associations between membership in grandmother caregiving trajectories and child cognitive and socioemotional development at 6 years in Figures 2 and 3. Descriptive statistics on the outcomes and full estimates and 95% CIs are in Supplemental Appendix Table 5.
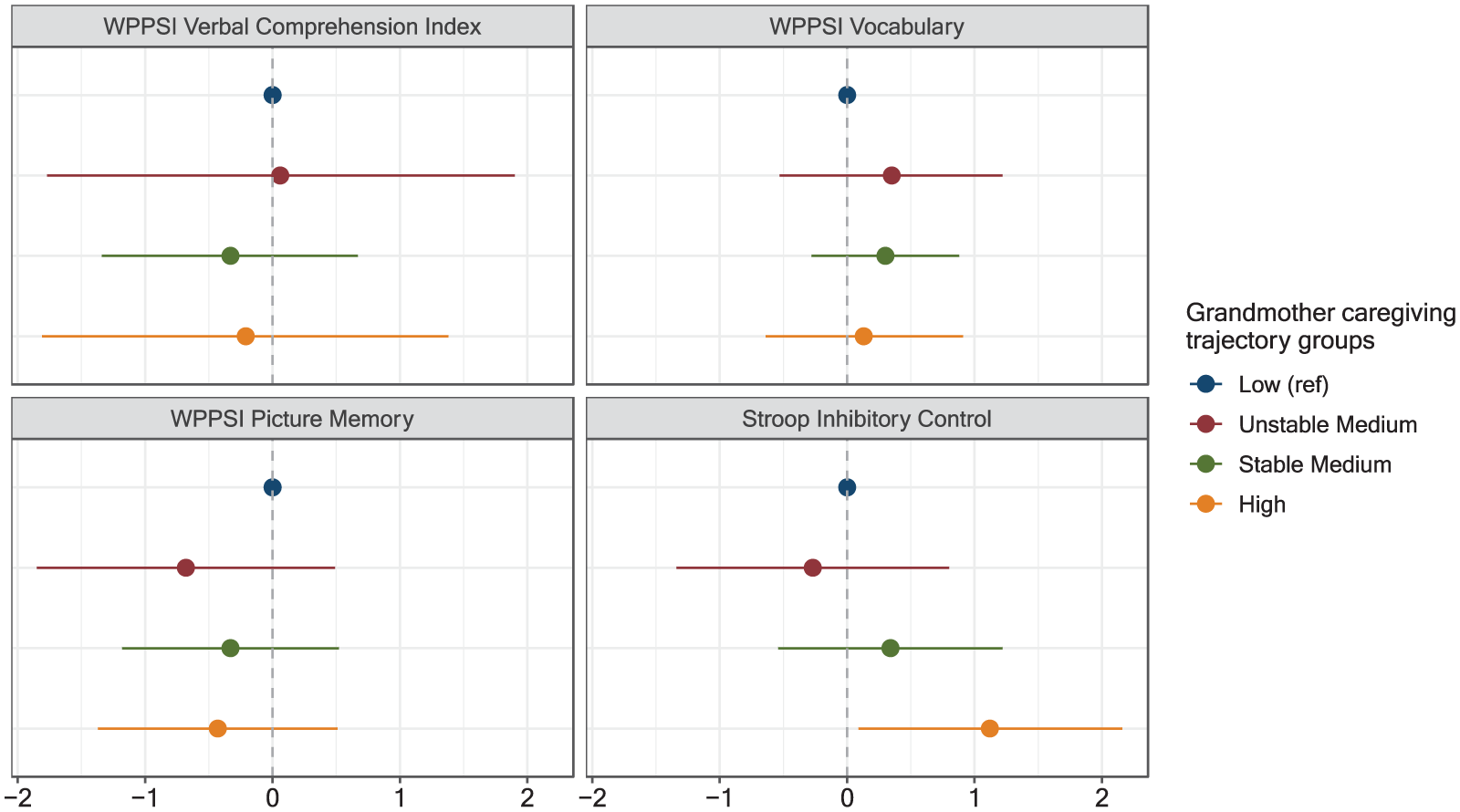
Associations Between Grandmother Caregiving Trajectories and Child Cognitive Outcomes Among Families in Rural Pakistan, Bachpan Cohort (n = 828).
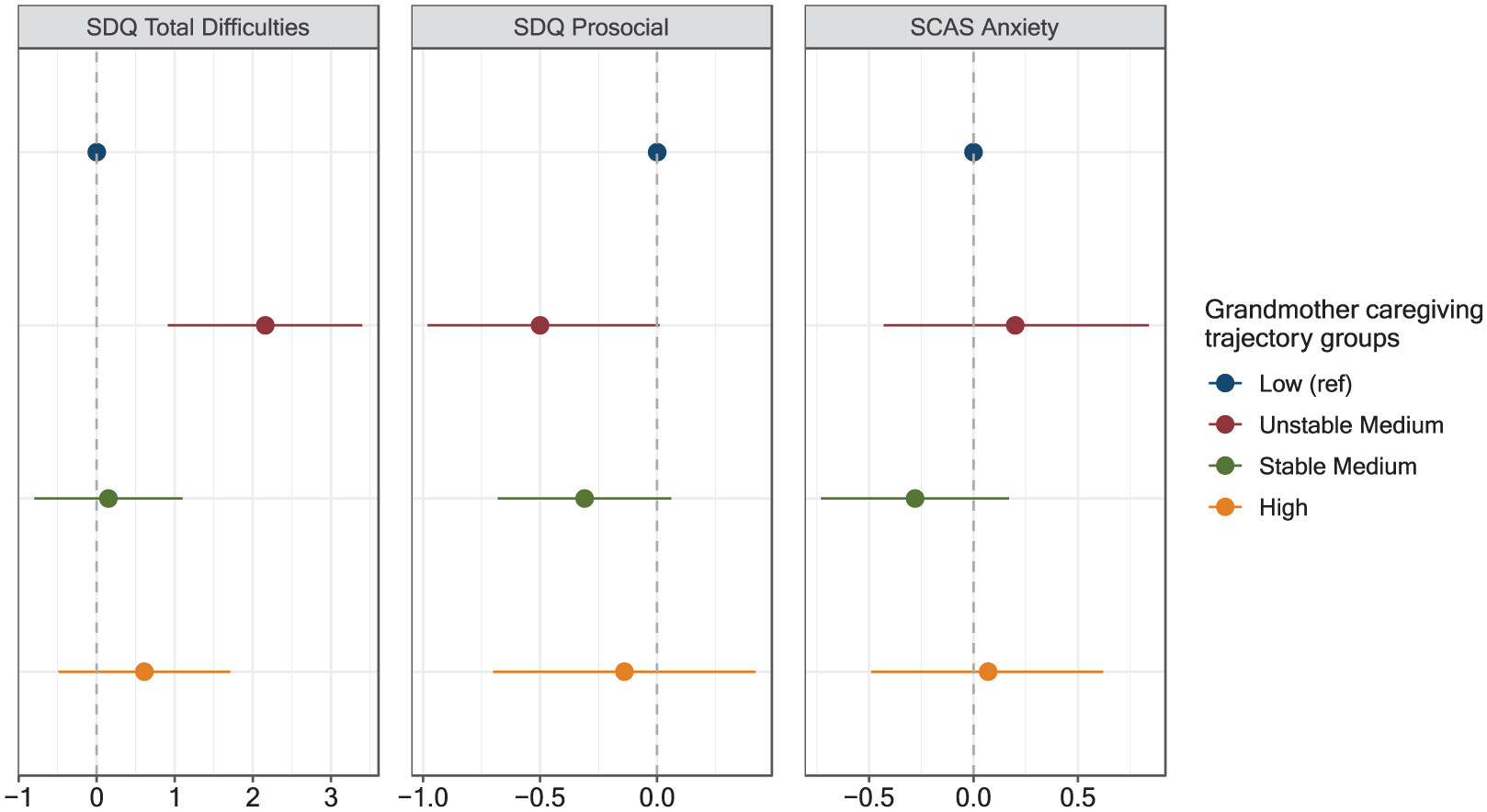
Associations Between Grandmother Caregiving Trajectories and Child Socioemotional and Mental Health Outcomes Among Families in Rural Pakistan, Bachpan Cohort (n = 828).
For cognitive outcomes (Figure 2), compared to children with grandmothers in the Low group, those with grandmothers in the High trajectory group had higher inhibitory control scores (MD [95% CI]: 1.12 [0.09, 2.16]). Grandmother caregiving trajectories did not meaningfully predict any of the WPPSI-IV subscales, which includes the Verbal Comprehension Index, Vocabulary, and Picture Memory domains (Figure 2).
For socioemotional and mental health outcomes (Figure 3), children whose grandmothers belonged to the Unstable Medium trajectory group had worse outcomes. Specifically, compared to children with grandmothers in the Low group, those in the Unstable Medium group had greater behavioral and emotional problems (2.16 [0.91, 3.40]) and fewer prosocial behaviors (–0.50 [–0.98, –0.01]). The pattern with anxiety scores was similar, though attenuated, with slightly higher anxiety scores in the Unstable Medium group relative to the Low group (0.20 [–0.43, 0.84]). Children whose grandmothers were classified in the Stable Medium and High caregiving trajectories tended to have mean socioemotional outcome scores that fell between the Low and Unstable Medium groups (Figure 3).
Discussion
Leveraging longitudinal cohort data in rural Pakistan, we characterized grandmother caregiving trajectories across the first 2 years of life and assessed associations between these trajectories and child cognitive and socioemotional development at 6 years. We found 4 distinct grandmother caregiving trajectories across the first 2 years of life: (1) Low, (2) Unstable Medium, (3) Stable Medium, and (4) High. Families with High grandmother caregiving trajectories had higher maternal education, higher household assets, lower prevalence of baseline maternal depression, and less family conflict. Those in the Unstable Medium trajectory group had similar maternal and household characteristics to the Stable Medium group, but had larger household sizes and greater changes in household composition and stressors at 1-year postpartum. Children with grandmothers in the High caregiving trajectory had higher inhibitory control scores compared to those in the Low group. Children with grandmothers in the Unstable Medium group had greater behavioral and emotional problems and fewer prosocial behaviors.
Longitudinal Patterns of Grandmother Caregiving
Consistent with our hypotheses, we found 4 trajectories that varied in terms of stability and intensity over time: (1) Low, (2) Unstable Medium, (3) Stable Medium, and (4) High. Studies from China and Korea allow us to consider our results in other Asian contexts (Li et al., 2022; Park, 2022). However, direct comparisons are difficult due to differences in the age of grandchildren and measurement of caregiving. Grandmother caregiving is markedly different at various stages of childhood (e.g., first 2 years of life in the present study vs. later childhood or adolescence in Park, 2022). Nevertheless, given the sparse literature, we assess general trends between our studies. In China, researchers identified 5 grandparent caregiving trajectories: (1) Sharply decreasing (5.4%), (2) Never or rarely (56.7%), (3) Slowly decreasing (9.4%), (4) Increasing (21.0%), and (5) Continuously High (7.5%) (Li et al., 2022). In Korea, researchers found 3 trajectories: (1) Low-level decrease (80.2%), (2) High-level decrease (16.5%), (3) Low-to-high increase (3.3%) (Park, 2022). In our study, we found similar low and high caregiving trajectory shapes, but the proportions differed (present study “Low”: 34.9% vs. Li et al. “Never or rarely”: 56.7% vs. Park “Low-level decrease”: 80.2%; present study “High”: 14.9% vs. Li et al. “Continuously High”: 7.5%). Although we did not find distinct Decreasing and Increasing patterns, our Unstable Medium group follows a similar shape of sharply decreasing and increasing caregiving. This unique group highlights the dynamic nature of grandmother caregiving across the first 2 years of life and emphasizes the importance of measuring grandmother caregiving behaviors longitudinally. Future research using trajectory modeling can help illuminate the dynamic nature of grandparent caregiving and the changing roles across early, middle, and later childhood.
Context of Grandmother Caregiving
We found grandmother caregiving trajectories differed by the social contexts of family organization. Over 1/3 of families were classified into the Low grandmother caregiving group. This group had the highest proportion of nuclear (37%) and multiple household family structures (19%). Prior studies in Pakistan found grandmothers in nuclear or multiple family structures may have minimal or no time with a specific grandchild due to limited contact and frequency or due to restricted attention between multiple grandchildren at a given time (Babu et al., 2017; Rahat et al., 2023). However, almost 2/3 of our sample had grandmothers in Medium to High caregiving trajectories and these groups had the highest proportions of joint/extended family structures (78% and 87%, respectively). When grandmothers were involved, they were, on average, 1 of the 4 caregivers for children. Our findings support the alloparenting norm of multigenerational family contexts and suggests grandmothers primarily served as complementary caregivers to mothers as opposed to primary caregivers, consistent with previous work in Pakistan (Babu et al., 2017; Rahat et al., 2023).
Associations Between Grandmother Caregiving Patterns and Child Development
Patterns of grandmother caregiving in early life were associated with specific domains of child cognitive and socioemotional development in middle childhood. As hypothesized, we found children with grandmothers in higher stable trajectories had more optimal development outcomes. We also found differential associations between grandmother caregiving patterns and developmental domains. For cognitive outcomes, children with grandmothers in the High caregiving trajectory had better inhibitory control scores at 6 years compared to the Low group. We found no substantial differences between grandmother caregiving trajectories for verbal comprehension, vocabulary, or working memory. For socioemotional outcomes, we found children with grandmothers in the Unstable Medium group had greater behavioral and emotional problems, fewer prosocial behaviors, and greater anxiety scores than children in the Low group. Grandmothers help teach children important skills, such as the ability to control impulsive behaviors and ignore distractions, which promote key social values, such as obedience, patience, and self-control (Babu et al., 2017; Tan et al., 2024). The transmission of these social values and manners may help to explain the different associations between patterns of grandmother caregiving across inhibitory control and socioemotional skills. These domain-specific findings are also consistent with previous work in Pakistan, which found higher grandmother caregiving at 1 year was positively associated with children’s fine motor and socioemotional development, but not language (Chung et al., 2020). Research from high-income countries document grandparent contributions to verbal comprehension (Reynolds et al., 2018). However, many grandmothers in rural Pakistan are illiterate with little to no schooling. It may be that grandmothers engage with children in ways that do not specifically enhance memory or vocabulary development (Makunga et al., 2018). Alternatively, it may be that grandmother caregiving patterns during the first 2 years of life are not as salient for children’s verbal and working memory development during school-age years. It may be that other types of grandmother care, such as financial support, are more salient for children’s cognitive skills during this time. Nevertheless, these differential associations suggest grandmothers may contribute to unique child development skills.
Exploring the Unstable Medium Trajectory of Grandmother Caregiving
The Unstable Medium trajectory group was a unique V-shaped grandmother caregiving trajectory which was an unexpected finding. Notably, grandmothers were reported participating in an average of 6 activities at both 3 months and 2 years, but were absent at 1 year. This inconsistent pattern of grandmother caregiving was associated with greater behavioral and emotional problems and fewer prosocial behaviors in middle childhood. Our finding supports prior family instability research that showed trajectories with greater family disruptions negatively impacted children’s cognitive and socioemotional development (Y. Sun & Li, 2011; Womack et al., 2022).
We speculate children in the Unstable Medium group were exposed to greater household stressors as evidenced by the higher percentage of changes in family composition, serious illness or death of a family member, and troubled relations with their close relatives or friends (Supplemental Appendix Table 4). Family instability and grandparental death have negative impacts on young children’s cognitive and behavioral development (Lee & McLanahan, 2015; Livings et al., 2023). While we do not have specific information on which family member was added, ill, or passed away, such household changes can often shift the responsibilities of family members. For example, grandmothers may change their caregiving with one child because a new child was born in the larger family system or because she needed to care for a sick family member. Ultimately, these changes can drastically change the amount, type, and quality of caregiving from both grandmothers and mothers. More studies are needed on how family instability in multigenerational households may affect child development.
Limitations and Strengths
Our results should be interpreted with some limitations. First, our measure of grandmother caregiving was maternally reported. Mothers may not provide a comprehensive picture of grandmother caregiving. This may differ by maternal depression, strained interpersonal relationships, or family conflict and may lead to potential misclassification bias. Future research should include grandmother reported caregiving. Second, we created a composite score of grandmother caregiving across the first 2 years of life, reflecting the combined influence of instrumental, socioemotional, and support behaviors. However, disentangling domain-specific pathways of grandmother caregiving would be an invaluable next step. Furthermore, we only had 3 timepoints to characterize grandmother caregiving trajectories. Future research that includes more measures of grandmother caregiving may help characterize dynamic caregiving patterns. Third, this was a longitudinal study with loss-to-follow up and missingness. We implemented IPMW to account for potentially informative missingness based on observed characteristics. However, there may be residual bias due to unobserved variables. There may also be uncontrolled confounding or modification due to unmeasured grandmother characteristics, such as age or health status (Schrijner & Smits, 2018a, 2018b), as well as potential genetic factors. For example, life history theory from evolutionary biology posits that life history strategies (e.g., caregiving investment and inhibitory control) are partially heritable and associated with psychopathology (Kaplan & Gangestad, 2015). Finally, there may be potential for reverse causation in which children’s behaviors may affect grandmother caregiving. Our sensitivity analyses suggested grandmothers engaged in slightly fewer caregiving activities with infants who showed greater socioemotional difficulties (Supplemental Appendix Sensitivity Analyses 1 and Supplemental Table 7). Future research should incorporate measures of grandmother responsivity to children and investigate the extent to which children’s behaviors may affect grandmother caregiving. Analyses could explore whether and how grandmothers respond to children with greater needs (e.g., fussier babies or children who “act out”).
Although we had some limitations, our study has many strengths. We utilized data from a population-representative sample of rural Pakistani women and children with rich data on maternal characteristics and family dynamics. We used detailed information on grandmother caregiving behaviors, leveraged a longitudinal cohort study, and included multiple domains of child development outcomes. In addition, we used GBTM to identify distinct longitudinal patterns of grandmother caregiving, allowing us to assess both stability and intensity over time. We add to the limited literature on grandparent caregiving in non-WEIRD countries and non-skipped-generation contexts. Our study’s findings may apply to other similar contexts where multigenerational family structures and alloparenting are prevalent and where grandmothers serve as complementary caregivers rather than custodial guardians.
Conclusion
We contribute to a scarce literature on the longitudinal relationships between grandmother caregiving on child cognitive and socioemotional outcomes. We identified 4 distinct groups of grandmother caregiving trajectories across the first 2 years of life in rural Pakistan. Grandmother caregiving patterns had domain-specific associations with child cognitive and socioemotional development in middle childhood, suggesting that grandmothers may contribute to unique developmental skills for children. Children with grandmothers in the Unstable Medium trajectory may be at particularly higher risks of poor socioemotional development and future mental health issues. Future research should characterize key family members’ caregiving patterns throughout childhood to capture the dynamic nature of caregiving and better understand how caregivers shape children’s development. This may help inform intervention targeting and fortify strategies to promote child development.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254251386761 – Supplemental material for Early life grandmother caregiving trajectories and child development: A longitudinal study
Supplemental material, sj-docx-1-jbd-10.1177_01650254251386761 for Early life grandmother caregiving trajectories and child development: A longitudinal study by Esther O. Chung, Allison Frost, Stephanie L. Martin, Brian W. Pence, Sean Y. Sylvia, Siham Sikander and Joanna Maselko in International Journal of Behavioral Development
Footnotes
Acknowledgements
The authors are deeply grateful to the women, children, and communities of the Bachpan Cohort. We would also like to thank the team at the Human Development Research Foundation (HDRF) including Rakshanda Liaqat, Tayyiba Abbasi, Maria Sharif, Samina Bilal, Quratul-Ain, Anum Nisar, Amina Bibi, Shaffaq Zufiqar, Sonia Khan, Ahmed Zaidi, Ikhlaq Ahmad, and Najia Atif for their meaningful contributions to the study’s design and implementation. We also thank the larger Bachpan and SHARE CHILD study teams. We are grateful to Linda Adair for her guidance and feedback on the analyses and manuscript.
Ethical considerations
Ethical approval was obtained from the Human Development Research Foundation in Pakistan (IRB/1017/2021) and the University of North Carolina at Chapel Hill (#20-1433). Written informed consent (or witnessed if the participant was illiterate) was obtained.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Bachpan Cohort was supported by the National Institute of Mental Health (U19MH95687), and National Institute of Child Health and Development (R01 HD075875). The Carolina Population Center provided training and general support (P2C-HD050924). EOC received training support from the National Institute of Child Health and Development (T32 HD091058; R01 HD075875) and from a P.E.O. Scholar Award. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available from Joanna Maselko upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.