
Abstract
Child-to-parent violence (CPV) is a unique form of externalising behaviour which is prevalent and destructive, yet there are very few evidence-based interventions to address CPV available. Parent mental health may be related to the experience of CPV, and may be a possible intervention target; however, evidence to support these links, and the directionality of potential links, is currently unclear. This study aimed to systematically review studies measuring parent mental health and experience of CPV. Eleven studies which met the inclusion criteria were identified through systematic searches of PsycINFO, MEDLINE, CINAHL, SOCI Index, Scopus, and EMBASE databases. Study quality was assessed using the Cambridge Quality Checklists. Included studies suggest that parent symptoms of depression, stress, anxiety, self-efficacy, impulsivity, and experience of trauma may be positively related to the experience of CPV; however, findings regarding depression and anxiety symptoms are mixed. There is a dearth of research to draw on and limited replication between these studies, highlighting the need for further research to understand the mental health impact of CPV on parents (particularly those related to trauma), how the onset and maintenance of CPV may be related to parent mental health, and to determine the role of addressing parent mental health in interventions for CPV.
Background
Child-to-parent violence (CPV) is an acute manifestation of conflict between a child and their parent, including physical violence (e.g., punching) and non-physical aggression (e.g., humiliating). Globally, the average prevalence of CPV in families is approximately 35% (Dahouri et al., 2025). However, these numbers can vary substantially between studies, ranging from 10% for more severe (i.e., physical) forms, to over 80% for psychological or verbal forms (Dahouri et al., 2025). In some cases, prevalence estimates may be under-representative of true incidence as families are often hesitant to report CPV (Arias-Rivera et al., 2021; Miles & Condry, 2016). On the other hand, measurement of CPV in ways which approach developmentally normative conflict between parents and their children (i.e., verbal conflicts) can inflate estimates. CPV is multi-causal and dyadic (i.e., often bidirectional; Gallego et al., 2019), which means that conceptualisations of CPV should consider how parent factors are implicated in the manifestation and maintenance of CPV. Despite this, there appears to be limited empirical understanding of parents who experience CPV, beyond their parenting behaviours. A clearer understanding of the mental health of parents who experience CPV may deepen our understanding of the familial context surrounding CPV but also be an important consideration for families involved in intervention.
Parent mental health is closely related to many physical, social, and mental child developmental outcomes (Pierce et al., 2020; van Santvoort et al., 2015). Thus, it is highly likely that parent mental health is also implicated in the development and maintenance of CPV. Early studies on child–parent conflict indicate that the wellbeing of the mother is related to increases in the intensity of conflict (Silverberg & Steinberg, 1987), whereby CPV can be conceptualised as a distinct and severe manifestation of conflict. The mental health of the parent may contribute to inconsistent responsiveness, reduced monitoring (Van Loon et al., 2014), the adoption of harsh parenting strategies (Midouhas & Oliver, 2023), as well as parental withdrawal (Mulder et al., 2018), all of which are implicated in the development and maintenance of CPV (Harries et al., 2023, 2024). Furthermore, traumatic experiences, such as intimate partner violence, are common for parents in families experiencing CPV (Lyons et al., 2015). The effects of such experiences (e.g., traumatic stress), can negatively impact the quality of parenting and the parent-child relationship (Christie et al., 2019), which may predispose externalising towards the parent (Moss et al., 2004). Early qualitative studies into CPV also describe a potential negative mental health impact of CPV on parents, such as guilt and shame (e.g., Bobic, 2002; Edenborough et al., 2008; Williams et al., 2017).
Parent mental health may also impact on the efficacy of CPV intervention or the identification of CPV. Parents with poor mental health, including depression, stress, and helplessness, may be more likely than those without these symptoms to drop out of parenting interventions (Morawska & Sanders, 2006). Certain mental health problems may also impact on capacity to implement strategies learnt during intervention. For example, depression is related to diminished motivation, and behavioural activation (Grahek et al., 2019; Pinto-Meza et al., 2006), which may create difficulty initiating and sustaining cognitive and behavioural effort during intervention. Furthermore, those with anxiety may be sensitive to the experience of shame (Cândea & Szentagotai-Tătar, 2018) and respond adversely to parenting interventions where there is anticipation of blame, a common occurrence for parents experiencing CPV (Eckstein, 2004; Edenborough et al., 2008; Murphy-Edwards & Van Heugten, 2018). Parents under substantial stress and overwhelm may employ a coping strategy whereby they reduce demands (Durukan et al., 2008), which may include emotional, logistical, and cognitively difficult and time-consuming tasks such as intervention. Alternatively, they may simply avoid the issue which intervention serves to address (Steeger et al., 2013). Finally, the cognitive effects of dissociation can create a responsivity issue (i.e., they do not have the cognitive capacity/ability to engage with the intervention) and hinder intervention outcomes in treatment (Kleindienst et al., 2011). As such, it is important to understand the parent’s mental health during intervention for CPV. Indeed, interventions which target both parent mental health and parenting strategies have efficacy for child outcomes (Al Sager et al., 2024).
Existing reviews highlight the relationship between parent and child mental health but may not be generalisable to CPV. Generally, both maternal and paternal mental health are associated with an increased risk of externalising behaviours in the child (Dean et al., 2018). However, it is important to note that CPV is a distinct form of childhood aggression. The parent-child dyad involves an asymmetry of power that substantially favours the parent and is different to more egalitarian sibling and peer relationships (Maccoby, 1999; Sherman, 1983). This means that aggression towards the parent is less likely and indicative of substantial disruption to the developmentally critical parent–child relationship (Harries et al., 2024). From the parent’s perspective, it is reasonable to assume that being directly targeted with aggression is, experientially, very different to having a child who is aggressive towards others, particularly when considering the impacts of trauma and stress. Furthermore, forensic studies suggest that young people who use CPV also have different risk factors for their behaviours, compared to young people with general externalising charges (e.g., Contreras & Cano, 2016). As such it is not scientifically appropriate to generalise findings from studies assessing a broad spectrum of externalising or aggression to understanding CPV.
Overall, the relationship between parent mental health and CPV is not clear. Specifically, it is unclear whether parent mental health difficulties precede CPV, impacting on parenting behaviours and increasing the likelihood of conflict within the family, or whether they are a result of the experience of CPV, or whether it is a combination of both. Considered through the lens of family systems theory (Bowen, 1993), the interrelated emotional connections within a family mean that addressing the mental health concerns of a parent should cascade to produce positive outcomes across the family as a whole, allowing issues to stabilise and eventually reduce the incidence and further likelihood of CPV occurrence. The mental health of parents in families experiencing CPV may be critical in understanding the onset and consequences of CPV, as well as how best to intervene. However, current CPV literature appears focused on parent behaviour (i.e., parenting), and potentially overlooks the parent’s internal experiences, which can impact on the parent’s behaviour. The current systematic review aims to synthesise empirical studies on parent mental health factors and how these relate to the experience of CPV (i.e., occurrence, frequency, and type).
Method
A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Page et al., 2021). Ethical approval was not sought as no new data was generated for this review.
Search Strategy
A comprehensive search for terms and concepts associated with CPV was conducted across several databases, including PsycINFO, MEDLINE, CINAHL, SOCI Index, Scopus, and EMBASE. The specific search strategies, tailored to suit the requirements of each database, are detailed in Table 1. The search strategy was trailed and developed iteratively; compared against lists of included studies from past CPV reviews to ensure that it was performing as intended. The final searches were completed in November 2024. The reference lists of included studies were also screened for inclusion, however, this yielded no additional studies.
Search Strategy.
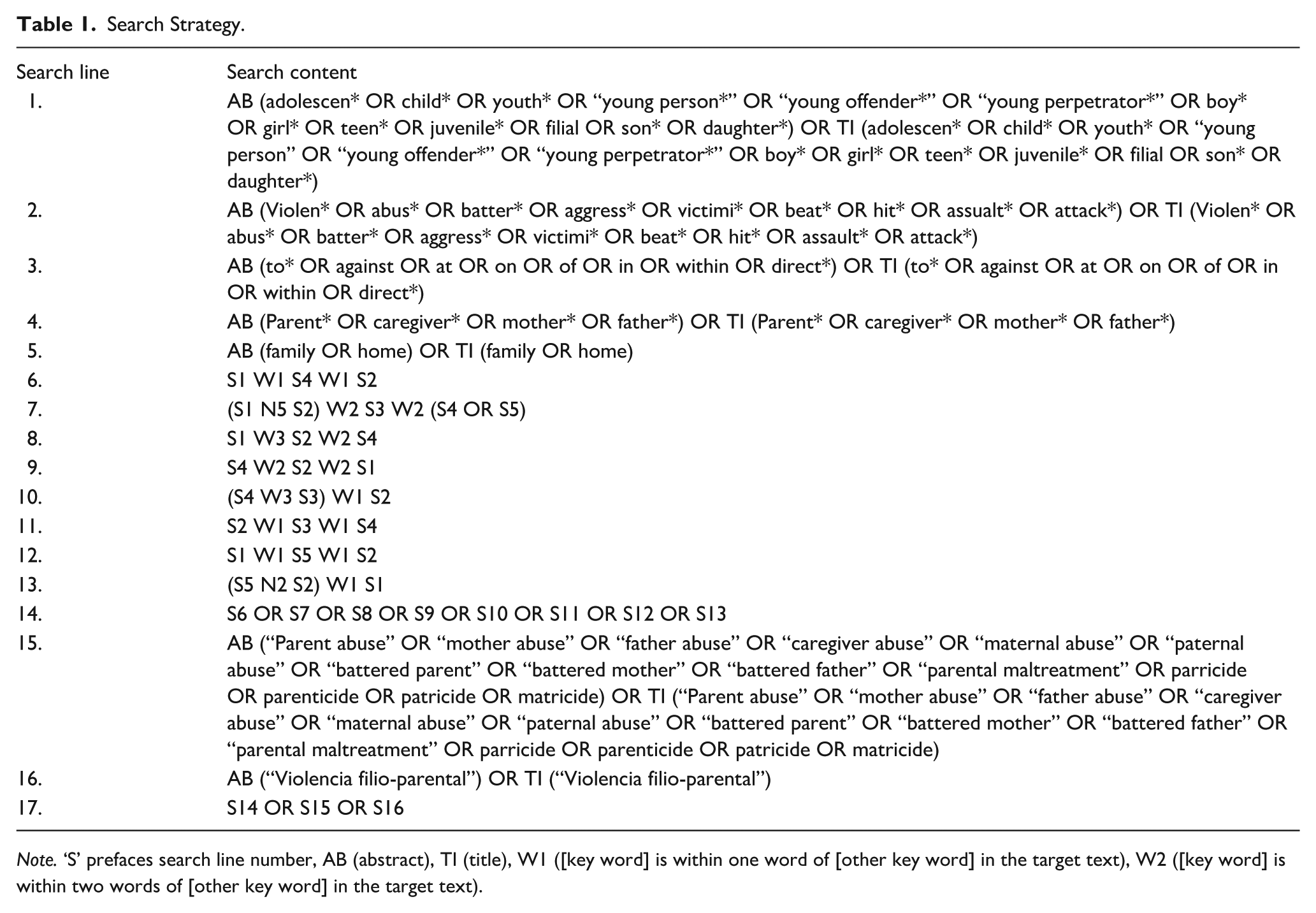
Note. ‘S’ prefaces search line number, AB (abstract), TI (title), W1 ([key word] is within one word of [other key word] in the target text), W2 ([key word] is within two words of [other key word] in the target text).
Study Eligibility
Inclusion Criteria
This review included peer-reviewed journal articles that examined the relationship between parental mental health factors and CPV, specifically its occurrence (e.g., prevalence, incidence) or characteristics (e.g., severity, type of violence). Parental mental health factors were defined consistent with the Achenbach system (Achenbach et al., 2017): internalising problems (e.g., depression/anxiety), thought problems (e.g., hallucinations), social problems (e.g., dependence), attention problems (e.g., impulsivity), or mixed problems (e.g., suicidal ideation). Externalising problems (e.g., aggression) were not included in this review, as they are mostly covered within an existing review (Gallego et al., 2019). Studies published in any language were considered for inclusion.
Exclusion Criteria
Articles were excluded if they were measuring the efficacy of an intervention, reported case studies or only qualitative results, were a review article, a book chapter, or a conference paper. Furthermore, studies were excluded if the sample mean age was less than 5 years 1 or greater than 24 years, or if the sample was conflated with young people who use sibling aggression, elder abuse, undirected aggression in the home, or violence against a grandparent where they are not the primary caregiver.
Screening
The title and abstract screening were performed by a single reviewer utilising Rayyan and Endnote. To ensure reliability, a secondary researcher independently screened a small subset (10%) of de-duplicated articles without knowledge of the primary reviewer’s decisions. The application of strict inclusion and exclusion criteria resulted in complete agreement (100%) between the reviewers. Full-text screening was then carried out on articles deemed eligible at the title and abstract screening stage. The results of the full screening process are detailed in Figure 1.
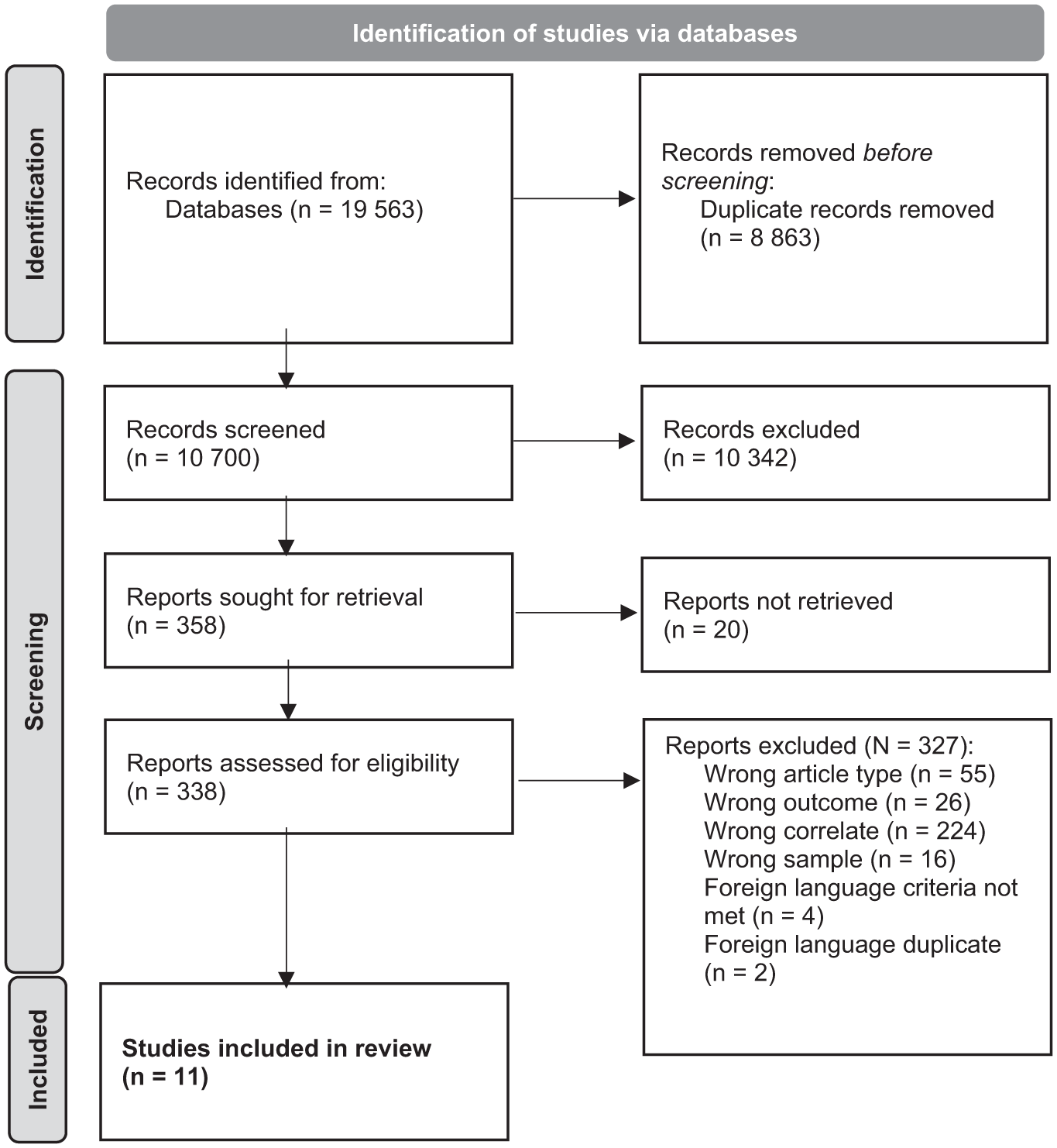
PRISMA flowchart.
Foreign Language Articles
A considerable body of CPV research originates from non-English-speaking countries, with Spain being a particularly prominent contributor. Although English-language reviews frequently exclude non-English studies, this practice may compromise the completeness of a review, particularly in a field like CPV where the literature base is relatively small yet expanding. To address this limitation and mitigate the potential for language bias, we included relevant studies published in languages other than English.
The screening of non-English articles was conducted using a variant of the approach described by Busse et al. (2014), modified to align with the objectives of this review. For an article to be considered eligible, it had to satisfy the following criteria: (1) the title, (2) the abstract, (3) the measures employed, and (4) the inclusion of statistical analyses needed to indicate its relevance. However, in the current review, no non-English studies met these criteria.
Data Extraction Process
Relevant results and effect sizes were extracted from included studies by a single researcher (T.H.). The key findings presented were then cross-checked by another member of the research team.
Results
Following the removal of duplicate records, a total of 10,700 articles were retained, and the abstracts and titles were assessed against the inclusion and exclusion criteria. As a result of this process, 10,342 papers were deemed not eligible for the review and were removed (see Figure 1). The 338 records which remained were sourced and read in full, applying the same criteria, which lead to the exclusion of a further 327 papers. A total of 11 studies met the inclusion criteria for the review. The characteristics and key findings from each are presented in Table 2. Where possible, results are presented for CPV against the mother and father separately, and/or based on direct or indirect association between the correlate and the outcome.
Characteristics and Key Findings of Included Studies.
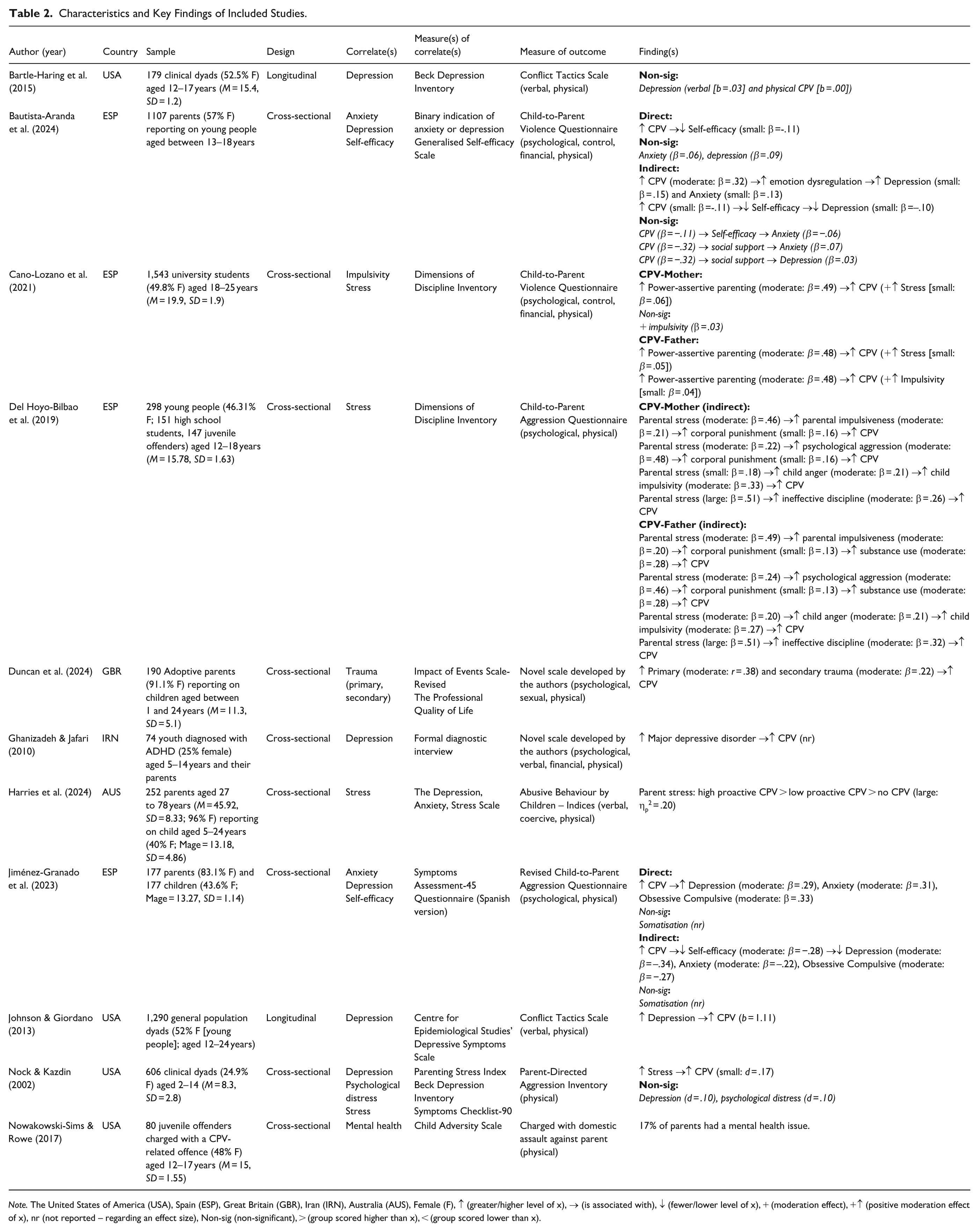
Note. The United States of America (USA), Spain (ESP), Great Britain (GBR), Iran (IRN), Australia (AUS), Female (F), ↑ (greater/higher level of x), → (is associated with), ↓ (fewer/lower level of x), + (moderation effect), +↑ (positive moderation effect of x), nr (not reported – regarding an effect size), Non-sig (non-significant), > (group scored higher than x), < (group scored lower than x).
Characteristics of Studies
Most studies were conducted in Spain (n = 4) or the United States (n = 4) and sampled the general population (n = 6), clinical population (n = 3), and forensic population (n = 2). Five studies sampled dyads, three sampled just the young person, and three sampled just parents. Sample sizes ranged from 74 (clinical sample) to 1543 (community sample), with the average sample size being 527.
Measurement
Regarding measurement of the correlate, depression was measured using the Beck Depression Inventory in two studies (Bartle-Haring et al., 2015; Nock & Kazdin, 2002), while the remaining studies measured depression using the Centre for Epidemiological Studies’ Depressive Symptoms Scale (n = 1; Johnson & Giordano, 2013) and the Symptoms Assessment-45 Questionnaire (n = 1; Jiménez-Granado et al., 2023), or via a diagnostic interview (Ghanizadeh & Jafari, 2010) or a single question (Bautista-Aranda et al., 2024). Stress was measured using the Dimensions of Discipline Inventory in two studies (Cano-Lozano et al., 2021; Del Hoyo-Bilbao et al., 2019), as well as the Depression, Anxiety, Stress Scale (Harries et al., 2024) and Parenting Stress Index (Nock & Kazdin, 2002) in single studies. Anxiety was measured either via a single question (n = 1; Bautista-Aranda et al., 2024) or the Symptoms Assessment-45 Questionnaire (n = 1; Jiménez-Granado et al., 2023)
Regarding measurement of the outcome (CPV), there was very little consistency between studies. However, two studies used the Conflict Tactics Scale (Bartle-Haring et al., 2015; Johnson & Giordano, 2013), two studies used the Child-to-Parent Aggression Questionnaire (Del Hoyo-Bilbao et al., 2019; Jiménez-Granado et al., 2023), and two studies used the Child-to-Parent Violence Questionnaire (Bautista-Aranda et al., 2024; Cano-Lozano et al., 2021). All studies measured CPV as including physical aggression, while most also incorporated measurement of verbal or psychological aggression (n = 9; Bartle-Haring et al., 2015; Bautista-Aranda et al., 2024; Cano-Lozano et al., 2021; Del Hoyo-Bilbao et al., 2019; Duncan et al., 2024; Ghanizadeh & Jafari, 2010; Harries et al., 2024; Jiménez-Granado et al., 2023; Johnson & Giordano, 2013). Some also measured items related to controlling or financial aggression (n = 4; Bautista-Aranda et al., 2024; Cano-Lozano et al., 2021; Ghanizadeh & Jafari, 2010; Harries et al., 2024). One study also included items related to sexual behaviours (Duncan et al., 2024).
Risk of Bias
The Cambridge Quality Checklist was applied to each included study (Murray et al., 2009). Each study was scored based on three criteria: Correlate (5 points; sample/sampling method, response rate, reliability of measures), Risk Factor (3 points; study design), and Causal (7 points; attribution of causality). Each study was assessed by two reviewers independently. There were no discrepancies. Overall, risk of bias was high across studies, with most studies employing non-randomised sampling (n = 10) and small samples (n = 7), both contributing to the low average ‘correlate’ score. Further many studies were cross-sectional (n = 9) and uncontrolled or inadequately controlled designs (n = 9), contributing to low ‘risk factor’ and low ‘causal’ scores. The results of the quality assessment are presented in Table 3.
Risk of Bias Assessment.
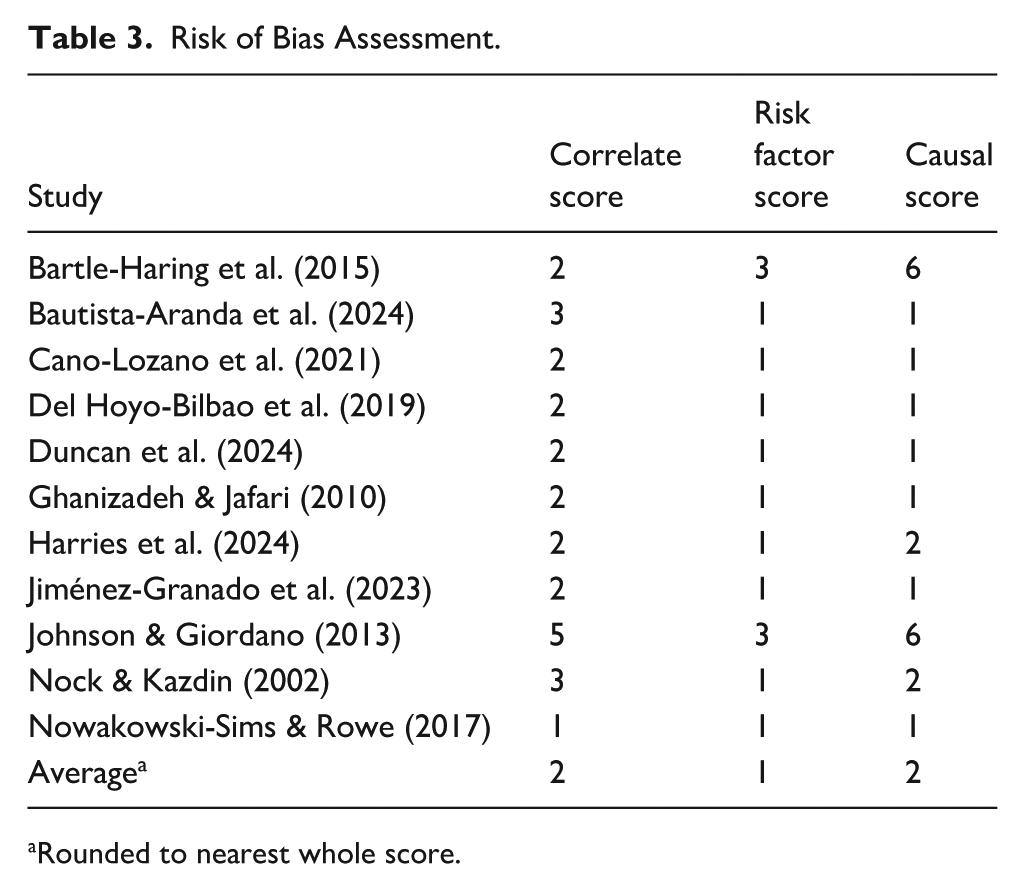
Rounded to nearest whole score.
Key Findings
Most included studies (n = 8) examined internalising problems related to symptoms of depression or stress. Anxiety symptoms and self-efficacy were measured in two studies, while trauma symptoms and impulsivity (attentional problem) were each examined in single studies. We found no studies which examined social or thought problems (such as those which appear within more severe mental health presentations, e.g., schizophrenia)
Depression
Five studies explored the relationship between parent symptoms of depression and CPV. Three 2 of these studies found a positive relationship (Bautista-Aranda et al., 2024; Jiménez-Granado et al., 2023; Johnson & Giordano, 2013), whereas two studies found no significant relationship (Bartle-Haring et al., 2015; Nock & Kazdin, 2002). Both studies which found no significant effect (including one longitudinal study with 6 months between assessments; Bartle-Haring et al., 2015) explored CPV with a clinical sample (where all children displayed behavioural problems), as opposed to a community sample where a significant relationship was detected. Thus, it may be that the depressed mood of parents is more related to the experience of child behaviour problems more generally, rather than CPV uniquely. However, one study which explored the relationship between parent diagnosis of Major Depressive Disorder and CPV in a sample of young people diagnosed with attention-deficit/hyperactivity disorder (ADHD) found a significant positive relationship (Ghanizadeh & Jafari, 2010). Across studies, this suggests that, where symptoms are severe enough to warrant diagnosis, depression may be uniquely associated with CPV above and beyond general child behaviour problems.
There was evidence that the relationship between symptoms of depression and CPV may be indirect, via parenting behaviours. Longitudinal analyses (with 1 year between assessments) by Johnson and Giordano (2013) suggest that the effect of parental depressed mood on CPV may be explained by the use of coercive parenting strategies. The deleterious effect of CPV on parental self-efficacy (or vice versa) may also expose greater risk of depression symptoms (Bautista-Aranda et al., 2024; Jiménez-Granado et al., 2023). CPV may also be positively associated with depressive symptoms via lower emotion regulation in the parent, but not lower social support (Bautista-Aranda et al., 2024). However, these mediation pathways are highly tentative as they are based on very few studies and are mostly small in effect.
Stress
Four studies explored the relationship between parent stress and CPV. All studies found that that stress was positively related to CPV behaviours (Cano-Lozano et al., 2021; Del Hoyo-Bilbao et al., 2019; Harries et al., 2024; Nock & Kazdin, 2002). However, there were no longitudinal studies to determine the direction of this relationship; both directions are plausible. Two studies suggested that stress may also relate to CPV via parenting behaviours. Cano-Lozano et al. (2021) found that stress strengthened the positive relationship between power-assertive discipline and CPV, while Del Hoyo-Bilbao et al. (2019) found that parental stress increased risk of parental impulsiveness and psychological aggression, which then increased risk of corporal punishment and CPV. Parental stress was also indirectly associated with CPV via a positive relationship with ineffectiveness of discipline (Del Hoyo-Bilbao et al., 2019).
Anxiety
Two studies explored the relationship between CPV and parent anxiety symptoms. One study found that there was a positive direct and indirect relationship (via lower parental self-efficacy). The same study also found the same positive relationship with obsessive-compulsive symptoms and somatic symptoms (Jiménez-Granado et al., 2023). In contrast (though modelled in the opposite direction 3 ), Bautista-Aranda et al. (2024) found no significant direct effect of CPV on anxiety symptoms, or (cross-sectional) indirect effects via lower self-efficacy or social support. However, CPV was positively associated with anxiety symptoms (cross-sectionally) through the negative association between CPV and emotion regulation (Bautista-Aranda et al., 2024). Overall, there are mixed results for anxiety, with one study finding a positive relationship, and one study finding no significant relationship.
Self-efficacy
Two studies suggest that parent self-efficacy is directly and negatively related to CPV (alongside being implicated in the pathway between depression and anxiety, and CPV; Bautista-Aranda et al., 2024; Jiménez-Granado et al., 2023).
Trauma
One study explored the relationship between CPV and parental symptoms of primary and secondary trauma, finding a positive relationship with CPV for both (Duncan et al., 2024).
Impulsivity
One study explored the relationship between CPV and parental impulsivity, finding that higher levels of impulsivity strengthened the positive association between power-assertive discipline and CPV (Cano-Lozano et al., 2021). However, this effect was only found for CPV against the father, not the mother.
General Mental Health
Two studies reported on generalised mental health problems that could not be otherwise categorised. One forensic study found that 17% of young people charged with a CPV offence reported that their parent had a mental health problem (Nowakowski-Sims & Rowe, 2017). One other study examined psychological distress in parents and found no significant relationship with CPV (Nock & Kazdin, 2002).
Discussion
This systematic review aimed to synthesise the empirical literature related to parent mental health and CPV. We found a dearth of literature that met the inclusion criteria, highlighting the space as an important research imperative moving forward. More than half of the included studies were only published within the last 5 years. Nonetheless, based on the reviewed literature, it appears that CPV could co-occur with a range of mental health symptoms in the parent, predominantly depression symptoms and stress.
We found that parents who experience CPV are more stressed than those who do not, which is not unexpected. The effect may be bidirectional, whereby stress appears to increase alongside progressively more severe and entrenched CPV (Harries et al., 2024). However, the experience of CPV is stressful and this stress may also encourage parents to use more negative parenting strategies, which in turn expose greater risk of CPV (Cano-Lozano et al., 2021; Del Hoyo-Bilbao et al., 2019). This means that parent stress could be an important intervention consideration, as there is the potential for negative feedback loops to form and perpetuate and escalate CPV over time via hostile discipline. Indeed, coercive or power-assertive parenting could precipitate a reactive type of CPV (Harries et al., 2022), as well as train this response over time to develop into a more proactive type of CPV (Granic & Patterson, 2006). Along these lines, it is worth noting that although this study did not review externalising symptoms, our findings suggest that many internalising symptoms may interact with or have an effect via externalising, such as aggressive forms of discipline. This aligns with the demonstrated comorbidity between internalising and externalising problems (Achenbach et al., 2016).
Parents in families experiencing CPV may also be more depressed. Again, this is not surprising given the well-understood mental health correlates of conflict within the family (Du Rocher Schudlich et al., 2015; Hanington et al., 2012). However, interestingly, the findings regarding depression symptoms remain mixed, possibly because not all families who experience CPV experience the same risk factors; there is substantial heterogeneity between families (Harries et al., 2024). It is apparent that the effect is currently limited to community samples (Jiménez-Granado et al., 2023; Johnson & Giordano, 2013) and almost absent from clinical samples (Bartle-Haring et al., 2015; Ghanizadeh & Jafari, 2010; Nock & Kazdin, 2002). It may be that the rates of parental depression within clinical samples (i.e., where the young person has a diagnosed [usually behavioural/neurodevelopmental] condition) is already elevated compared to community samples (Bonis, 2016; Dumas et al., 1991), and the experience of CPV is not uniquely associated within any greater depression when measured at the symptom level. Whereas, in community samples, the baseline depressive symptomology could reasonably be lower, meaning that any association with CPV becomes more salient. Indeed, when using diagnostic criteria for Major Depression (i.e., depression with clinically substantial symptomology), Ghanizadeh and Jafari (2010) found that mothers with a depression diagnosis were more likely to experience CPV in a clinical sample.
On balance, this review indicates that it is likely that CPV co-occurs with symptoms of parental depression. The experience of CPV could reasonably generate depressive symptoms; CPV is associated with shame and guilt in parents (Bobic, 2002; Williams et al., 2017), as well as helplessness (Harries et al., 2024), all of which are related to the development of depression (Kim et al., 2011). Like stress, parents with depressive symptoms may also use more negative parenting strategies (Chau & Giallo, 2015; Hentges et al., 2021), as well as have less self-efficacy in their parenting (Bautista-Aranda et al., 2024; Jones & Prinz, 2005), which could impact on their ability to consistently implement effective behaviour control (Chau & Giallo, 2015; Rominov et al., 2016). This may increase the risk of CPV, and thus, further helplessness (i.e., low self-efficacy) and symptoms of depression. Indeed, this review also found that parents who experience CPV had lower self-efficacy; however, like all findings in the review, the direction of this relationship is unclear owing to a lack of longitudinal research methods. It is likely bidirectional; the experience of CPV may lead parents to think of themselves as ‘failures’ by blaming themselves (Williams et al., 2017) while simultaneously hindering parental efforts to then control the occurrence of future CPV. This may be important for intervention, whereby caregiving helplessness is implicated in the development of severe proactive CPV, rather than just situational reactivity against the parent (Harries et al., 2024).
Depression and anxiety symptoms frequently co-occur (Jacobson & Newman, 2017); however, we found much less empirical investigation into anxiety and CPV, compared to depression. The available studies also produced partially mixed results, while both studies found an overall positive relationship between anxiety symptoms and CPV, the direct effect was only significant in Jiménez-Granado et al. (2023). Bautista-Aranda et al. (2024) found that CPV was only related to increased anxiety symptoms where there was greater emotion dysregulation more generally. However, it is important to note that Bautista-Aranda et al. (2024) used only a single item to measure the presence or absence of anxiety, compared to a more comprehensive symptom checklist used by Jiménez-Granado et al. (2023).
The lack of studies exploring parent trauma symptomology and CPV is stark given the context in which CPV emerges and the impact of CPV on parents. Indeed, this review found only one study which measured parent trauma symptoms, which indicated that these symptoms may be higher among (adoptive) parents who experience CPV, compared to those who do not (Duncan et al., 2024). Much CPV may occur in the context of broader family violence (Contreras & Cano, 2016; Lyons et al., 2015), which can be traumatising for the parent (Dillon et al., 2013). Furthermore, developmental attachment theories posit that CPV is linked to a disorganised attachment (Moss et al., 2004), that may stem from the caregiving of a traumatised parent (Liotti, 2004; Lyons-Ruth & Block, 1996; Main & Hesse, 1990). Unresolved trauma and associated dissociative symptoms may lead to parents being inconsistent between and within caregiving interactions, which can increase the likelihood of attachment disruption and externalising in the young person (including CPV; Lecompte & Moss, 2014; Moss et al., 2004). Such inconsistency may ‘train’ a more proactive presentation of CPV over time, which may develop as a means to control the uncertainty associated with caregiving inconsistency (Moss et al., 2004). CPV also has the potential to be traumatising for the parent and, like other mental health symptoms, may form a negative feedback loop. However, this review found that no quantitative studies have explored such an effect.
There was also only one study which examined parents’ mental health diagnoses (depression; Ghanizadeh & Jafari, 2010). The impact of trauma can precipitate conditions such as post-traumatic stress disorder (Tortella-Feliu et al., 2019) and borderline personality disorder (Yuan et al., 2023), among others (Danese & Baldwin, 2017). There is also nascent evidence that a substantial amount of CPV may occur in families where the young person has a neurodevelopmental disorder (Harries et al., 2024; Holt, 2023). First, this scenario could intensify mental health outcomes of parents by adding caregiver stress. For example, parents of young people with Autism often report stress from societal reactions to the child’s difference, and managing treatment and support systems, alongside challenging behaviours (Gentles et al., 2024; Tathgur & Kang, 2021). However, it may also be that many of these parents themselves have these disorders (or traits of these disorders; Scheeren & Stauder, 2008), given the hereditary nature of neurodevelopmental disorders like autism and ADHD (Lichtenstein et al., 2010). Instead, most studies in the current review measured symptoms of psychopathology, which may fail to distinguish clinically relevant mental health problems from sub-clinical experiences of isolated symptoms.
The current review has strength in its broad reach – we set no publication limits regarding year of publication or language. However, we only included studies which measured CPV specifically. It is reasonable to assume that CPV can also be captured (albeit incidentally) within studies measuring general externalising behaviour, for example, aggression within the home or aggression in early childhood, as well as within studies on challenging behaviours within samples of young people with neurodevelopmental disorders (e.g., Quetsch et al., 2023). Such studies are not represented in this review. However, as explained previously, CPV is a unique form of externalising behaviour and therefore should be understood through targeted studies. Our review was also limited in capacity to look for subgroup effects, owing to the small number of studies which met the inclusion criteria. For example, we could not confidently assess differences in results between longitudinal and cross-sectional studies, or studies which sampled dyads and those which sampled on the parent or the young person. Such differences may nevertheless exist and potentially confound the conclusions of this review.
Overall, this review found that parent mental health could be a key consideration related to the occurrence of CPV, as well as a potential outcome of the experience. However, the lack of studies in this space, alongside the heterogenous results within those conducted, presents an uncertain picture. Future studies should aim to understand how parent mental health (particularly that which is associated with trauma) relates to CPV, whereby the effect on parenting behaviours may be a central mechanism for this relationship. However, studies in the current review were predominantly cross-sectional. Longitudinal studies are thereby needed to confidently model such indirect effects. This would also aide in modelling the likely bidirectionality of the relationship between parent mental health and CPV. Furthermore, many studies in the current review included analyses which were under-controlled. For example, the effect of parent mental health may differ depending on the age of the child; where the young person is more dependent on the caregiver, the impact of depression, self-efficacy, or anxiety could reasonably be more acute, compared to adolescence where the young person is more autonomous. As such, future studies should look to control for the age of the child or target younger age ranges to compare to the results of the mostly adolescent samples in the current review.
Understanding the impact of CPV on parents, as well as how parent mental health may buffer or expose risk of CPV, could aid clinicians and services working with families experiencing CPV, particularly where CPV interventions become more parent-focused. While the conclusion made from the current review is preliminary (owing to a lack of studies), they do suggest that targeting both child factors, as well as parent factors, would likely be beneficial to interventions which address CPV (Al Sager et al., 2024). For example, working to therapeutically manage the stress and overwhelm in parents experiencing CPV could help parents to engage in more positive parenting behaviours which are taught within existing programmes (Toole-Anstey et al., 2021). However, more research is needed in clinical samples specific to CPV, and particularly within intervention evaluations, to understand how best to work with parent mental health in this context.
Footnotes
Acknowledgements
None.
Ethical Considerations
No ethical approval required.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Not applicable (no data generated).