
Abstract
Although feeling younger has been found to be related with various health benefits, associations are complex, and most prior studies have used self-reported health indicators rather than objective, performance-based health measures and biomarkers. We investigated between-person and within-person associations of subjective age with pulmonary function (peak expiratory flow), a biomarker associated with mortality risk. Data from the German Aging Survey were used, with a sample of 9,782 middle-aged and older adults assessed up to four times over 9 years. Longitudinal multilevel regression models controlling for socio-demographic and health-related measures revealed predictive effects at the between-person level and at the within-person level, and in both directions. At the between-person level, study participants who felt overall younger showed better pulmonary functioning, and those with overall better pulmonary function felt younger. At the within-person level, on measurement occasions when participants felt younger, they exhibited better pulmonary function, and on measurement occasions when participants’ pulmonary function was better, they felt younger. Our findings thus suggest that there are meaningful between-person and within-person associations between pulmonary function and subjective age. Even subtle changes in biomarkers such as pulmonary function may affect how old people feel, which has consequences for their behaviors, health, and well-being.
An individual’s subjective age indicates how old a person feels, which can be considerably discrepant from one’s chronological age. Indeed, most middle-aged and older adults exhibit a “subjective age bias” (Teuscher, 2009; Weiss & Weiss, 2019)—they feel younger than they are chronologically (Pinquart & Wahl, 2021; Rubin & Berntsen, 2006).
Subjective Age and Health in the Second Half of Life
Subjective age has been conceptualized as an “alternative marker of development” (Montepare, 2009, p. 42), and a younger subjective age has been found to be associated with various beneficial developmental outcomes (Alonso Debreczeni & Bailey, 2020; Kotter-Grühn et al., 2015; Stephan, Sutin, Terracciano, et al., 2018), including better mental and physical health (Blöchl et al., 2021; Spuling et al., 2013; Westerhof et al., 2023), shallower age-related cognitive decline and a lower dementia risk (Stephan, Sutin, Luchetti, et al., 2018), decelerated epigenetic aging (Stephan et al., 2021), better protection against the detrimental effects of stressors (e.g., Shrira & Hoffman, 2021; Wettstein et al., 2021), and lower mortality hazards (Stephan, Sutin, Terracciano, 2018; Westerhof et al., 2023).
So far, many studies that addressed associations between subjective age and health relied exclusively on subjective health indicators. As a consequence, the estimated strength of associations might be biased due to the self-report assessment format of both measures. Therefore, the current study investigates longitudinal associations between subjective age and objectively measured lung function (peak expiratory flow), which is a biomarker and key indicator of general, objective health. We use middle-aged and older adults’ data from the German Aging Survey (Klaus et al., 2017; Vogel et al., 2022), with up to four measurement occasions between 2008 and 2017. To do so, we adopt a statistical framework that disentangles between-person from within-person associations.
Subjective Age and Pulmonary Function
According to Khan et al. (2017), “lung function represents one of the few consistently reliable physiological markers of aging” (p. 627). Lung or pulmonary function, as assessed by indicators such as the peak expiratory flow (Nunn & Gregg, 1989), is an important health marker not only because of its objective, performance-based nature, but also because it is related with physical and cognitive function (Cook et al., 1995) as well as with psychosocial factors such as social network diversity (Cheng et al., 2014). Moreover, peak expiratory flow is predictive of crucial outcomes such as disability, frailty, dementia, risk of falls, cardiovascular disease, and mortality risk (Donahue Patrick et al., 2023; Johansson & Thorvaldsson, 2021; Roberts & Mapel, 2012; Smith et al., 2013; Trevisan et al., 2019, 2020; Vaz Fragoso et al., 2008; Zhang et al., 2023) and can therefore be considered a “marker of general robustness in older adults” (Trevisan et al., 2019). However, to our knowledge, although peak expiratory flow is an age-sensitive health marker that exhibits decline already prior to midlife (Nunn & Gregg, 1989), little is known about the role of psychosocial factors such as subjective age for within-person changes in that health marker. Associations between subjective age and lung function might be reciprocal. Specifically, subjective age might predict peak expiratory flow as a younger subjective age is associated with beneficial health behaviors, such as regular physical activity (Stephan et al., 2017), which in turn contribute to better lung functioning (e.g., Chaitra & Maitri, 2011). Regarding the opposite direction, Stephan et al. (2015a) described peak expiratory flow as a “perceptible marker of biological aging,” and they found, based on cross-sectional data, that it was significantly related with subjective age, whereas other, non-perceptible biomarkers such as telomere length were not. Decline in pulmonary functioning is thus probably a process that individuals become aware of and which they might attribute to their aging. As such, because of reduced pulmonary functioning, individuals might feel older. Barrett and Gumber (2020) investigated the role of everyday body problems, including self-reported breathing problems, on subjective age in older adults. They found that such everyday body problems were associated with older subjective ages, probably because they are perceived by individuals as what Barrett and Gumber (2020) have labeled “aging body reminders” (see also Karp, 1988). However, the study by Barrett and Gumber did not assess objective pulmonary function, and their analyses did not differentiate between-person and within-person associations.
With regard to other studies that investigated how indicators of lung health beyond peak expiratory flow are related with subjective age, Thyagarajan et al. (2019) included lung disease as one component of self-reported comorbidity and found, based on cross-sectional analyses, that individuals with higher comorbidity scores felt older. Unfortunately, the authors did not investigate specific associations of lung disease with subjective age.
In conclusion, although lung function is a crucial biomarker and objective health indicator, prior empirical findings on potentially bidirectional associations between subjective age and lung function are scarce, particularly longitudinal evidence and findings with a focus on objectively assessed lung function.
The Importance of Separating Between-Person Effects and Within-Person Effects
Among the available longitudinal studies that investigated associations of subjective age with health—with the exception of a few microlongitudinal diary studies (for an overview, see Neupert & Bellingtier, 2022), which do not allow for investigation of long-term developmental processes, and one macro-longitudinal one, which focused, however, on a subjective health indicator, namely pain, rather than on objective health (Wettstein et al., 2024)—none disentangled between-person associations from within-person associations of subjective age with health, although between-person vs. within-person associations can be quite discrepant. Studying intraindividual processes and phenomena inherently requires longitudinal data as well as analytical approaches that allow statistically disentangling between-person from within-person associations (Curran & Bauer, 2011; Hoffman & Stawski, 2009; Raz & Lindenberger, 2011).
In the context of subjective age views, such an approach of separating between-person and within-person associations is particularly important, as it will “allow us to determine for whom (between-person effects) and under which situations or contexts (within-person effects) subjective views of aging function as antecedents and consequences of health and well-being” (Neupert & Bellingtier, 2022). Specifically, whereas between-person associations of subjective age with lung function refer to associations that are due to enduring interindividual differences in subjective age and in lung function, thereby reflecting the structure or the trait component of the variables analyzed, within-person associations indicate the extent to which changes in those variables are interrelated, thereby estimating intraindividual associations at the heart of processes driving both variables. Both associations of structures and processes require attention when investigating subjective age-lung function relations, given that both comprise a trait/structure component, and at the same time, they comprise a process component and change with aging, but these age-related changes reveal substantial interindividual variability.
The Present Study
The aim of this study is to investigate longitudinal associations between subjective age and lung function (peak expiratory flow = PEF) as a performance-based, objective health marker in a sample of middle-aged and older adults. Specifically, our goal is to quantify between-person associations and within-person associations between these two variables. We use data from the German Aging Survey (Klaus et al., 2017; Vogel et al., 2022), including all measurement occasions when both subjective age and PEF were assessed (2008, 2011, 2014, 2017). Taking into account the summarized evidence on mutual subjective age—lung function associations and distinguishing between-person from within-person effects, our hypotheses are as follows:
Subjective age as a predictor: At the between-person level (between-person differences in subjective age), we expect that participants with an overall younger subjective age show better lung function performance (i.e., a higher PEF score). At the within-person level (within-person subjective aging), we assume that on measurement occasions when participants feel younger, they show better lung function.
Subjective age as an outcome: At the between-person level (between-person differences in lung function), we expect that participants with overall better pulmonary function feel younger. At the within-person level (within-person lung aging), we assume that individuals feel younger on measurement occasions when their pulmonary function is better.
Our analyses center on the relations between the processes of subjective age and pulmonary function in adulthood. Yet, to uncover how one’s subjective age may affect and be affected by one’s pulmonary function, it is crucial that we consider also chronological age at both between- and within-person levels of analysis. The within-person chronological aging effect reflects the extent of age-related change in PEF and subjective age and is required as both PEF (Nunn & Gregg, 1989) and subjective age (Pinquart & Wahl, 2021; Wettstein, Wahl, et al., 2023) change with advancing chronological age. The between-person effect of chronological age refers to between-person differences in chronological age and reflects to what extent individuals of different chronological ages differ with regard to PEF and subjective age; these between-person age differences in both variables can be remarkable (Nunn & Gregg, 1989; Pinquart & Wahl, 2021; Wettstein, Wahl, et al., 2023) and therefore need to be empirically addressed. Both the between- and the within-person chronological age effects might interact with the between- and within-person effects of subjective age and lung function; specifically, associations between subjective age and health have been found to vary by chronological age (Bergland et al., 2014; Hubley & Russell, 2009), and age-related change in subjective age might be predicted by lung function (and vice versa), which requires an inclusion of a within-person chronological age*lung function (and within-person chronological age*subjective age) interaction. Therefore, our analyses include interactions, at both the between- and within-person levels, of chronological age with both subjective age and pulmonary function. Given the already described paucity of empirical findings—particularly longitudinal ones—on associations between lung function and subjective age, we decided not to derive specific a-priori hypotheses, but to investigate the moderating effects of within-person and between-person chronological age in an exploratory manner.
In our analyses, we control for socio-demographic factors (gender, education, region of residence), physical activity, body mass index (BMI), body height, health (number of chronic diseases), and depressive symptoms. These factors are potential confounders because these are meaningfully related with both subjective age (Choi & DiNitto, 2014; Schönstein et al., 2021; Stephan et al., 2020; Stephan, Sutin, Terracciano, et al., 2018; Wettstein, Wahl, et al., 2023) and lung function (Beller et al., 2024a, 2024b; Ji et al., 2021; Mutz & Lewis, 2021; Nunn & Gregg, 1989; Wang et al., 2023). They are also associated with age-related change in subjective age and in lung function; therefore, we will also test interactions between chronological age and these factors (at both within-person and between-person levels).
Method
Transparency, Openness, and Data Availability
The data presented in this study as well as study materials are available from the German Centre of Gerontology (n.d.), Research Data Centre. Materials, questionnaires, and interview codebooks can be obtained from Engstler et al. (2022). The analytic code for the following analyses can be obtained from the Online Supplemental Material. The design, hypotheses, and analytic plan of the current manuscript were not pre-registered. In the following section, we report how we determined our sample size, as well as any data exclusions, all data preparatory steps, and we describe all measures used for our analyses.
Sample
Data from the German Aging Survey (Deutscher Alterssurvey, DEAS; Klaus et al., 2017; Simonson et al., 2023; Vogel et al., 2022) were analyzed. The DEAS is a nationwide, cross-sequential survey which comprises samples of middle-aged and older individuals (40–85 years at their first measurement occasions). The first study sample was drawn in 1996, and individuals were re-assessed in 2002, 2008, 2011, 2014, 2017, 2020 (summer), and 2020/21 (winter). Additional samples were drawn in 2002, 2008, and 2014 and also re-assessed at later measurement occasions. Study inclusion criteria are that individuals have to reside in Germany, and they have to be able to understand and speak German. Only for the first two measurement waves (1996 and 2002), German citizenship was specified as an additional inclusion criterion for study participation. The vast majority of all individuals who have participated so far (n = 19,745; 95.3%) have a German citizenship; 9.3 % (n = 1,921) reported to have migration background.
The sample sizes of samples drawn in 1996, 2002, 2008, and 2014 ranged between n = 3,084 (2002) and n = 6,205 (2008). From 2008 on, sample sizes of n > 6,000 were obtained to make sure that all categories of every stratification variable (age group, gender, region of residence) and all cross-categorization (e.g., older East German men) are sufficiently represented for group-differential analytical approaches (Klaus & Engstler, 2017).
For the following analyses, we used observations from 9,782 individuals (mean age = 61.89 years, SD = 11.42 years) who provided one or more valid scores on the study variables (including covariates) on at least one of the measurement occasions between 2008 and 2017. Measurement occasions prior to 2008 and after 2017 were not included because lung function was only assessed in the study period 2008–2017. Participants contributed on average 2.28 observations (range 1–4; n = 2,298 [23.5%] provided all four observations). When comparing those with only one observation (30.1%) with those who provided two or more observations (69.9%) with regard to the study variables at baseline, we found that individuals with only one observation had poorer pulmonary function (Cohens d = -.14), felt less young (d = .16), and were chronologically older (d = .15) than those providing more observations. In both groups, about 51% were male. Individuals with only one study participation had lower levels of education (d = -.31), (negligibly) more chronic diseases (d = .03) and reported more depressive symptoms (d = .09). Their body height was below the one of those who provided more observations (d = -.08), and they were less physically active (d = -.28), but BMI levels were very similar between groups (d = -.01). All these differences were below medium effect size, according to Cohen (1992).
Ethical approval was not obtained because this is not required for general surveys in Germany. The German Aging Survey does not employ any invasive methods. The survey maintains an academic advisory board which ensures its scientific quality. All study participants provide informed consent prior to study participation.
Measures
Pulmonary Function (Peak Expiratory Flow)
Peak expiratory flow, which measures the speed of air exhalation from the lungs via the mouth, was assessed after the interview by trained interviewers and based on two trials, using a mini Wright peak flow meter. In line with the standard procedure (Nunn & Gregg, 1989), the higher of both scores was used as peak expiratory flow indicator. The unit is l/min. 1 The mini Wright peak flow meter could assess scores that were greater than 60 l/min2 or below 880 l/min2; scores that are not within the range are very rare (Cook et al., 1991; Johansson & Thorvaldsson, 2021; Nunn & Gregg, 1989) and rather implausible.
Subjective Age
Subjective age was assessed by asking individuals “How old do you feel?” For our analyses, we computed a subjective age difference score by calculating the difference between subjective age and chronological age, with negative scores indicating a subjective age that is younger than one’s chronological age. Following usual procedures (e.g., Stephan, Sutin, & Terracciano, 2018), subjective age difference scores that were more than 3 SD above or below the mean were considered as outliers and set to missing (between 0.2% and 1.8% of all subjective age scores per measurement occasion from 2008 to 2017).
Covariates
We added chronological age, gender, year of study entry (1996, 2002, 2008, or 2014), region of residence (West vs. East Germany), education, physical activity, number of chronic diseases, depressive symptoms, body height, and body mass index (BMI) as covariates. Covariates that were assumed stable over time (gender, year of study entry, region of residence, education, body height) were specified as time-invariant, whereas all other covariates (physical activity, number of chronic diseases, depressive symptoms, BMI) were specified as time-varying. Education was assessed based on the International Standard Classification of Education (ISCED) coding (United Nations Educational, Scientific and Cultural Organization [UNESCO], 2012), which takes school and professional education into account and differentiates between four educational levels (low, medium, elevated, and high education). Physical activity was assessed based on the item “How often do you do sports, such as hiking, soccer, gymnastics or swimming?” We recoded the response format so that higher scores indicated more frequent physical activity (range 1 = never to 6 = daily). The assessment of the number of chronic diseases was based on a list of 11 chronic conditions (e.g., diabetes, cancer, cardiovascular diseases). Depressive symptoms were assessed by a 15-item German adaptation (Hautzinger & Bailer, 1993) of the Center for Epidemiological Studies Depression Scale (CES-D scale; Radloff, 1977). Study participants indicated how often they had experienced 15 depressive symptoms during the past week (e.g., “I felt sad,” “My sleep was restless”). The response format was a 4-point Likert-type scale ranging from “rarely or none of the time (less than 1 day)” to “most or all of the time (5–7 days).” A sum score across all items was computed, ranging from 0 to 45, with higher scores indicating more frequent depressive symptoms (Cronbach’s α = .85 both in 2008 and in 2014). Body height was assessed based on self-reports, and the computation of BMI (BMI = weight/height2) was based on study participants self-reported body weight and body height. Reported BMI scores further than three SDs from the mean were considered as outliers and set to missing (between 1% and 1.1% per measurement occasion).
Data Preparation and Data Analyses
Longitudinal multilevel models were computed using SAS PROC MIXED (Littell et al., 1998; Ram & Grimm, 2015). Between-person and within-person effects (Hoffman & Stawski, 2009) were specified for subjective age (with PEF as outcome), for peak expiratory flow (with subjective age as outcome) as well as for chronological age (for both outcomes). In additional models, we controlled for gender, year of study entry, education, physical activity, BMI, body height, number of chronic diseases, and depressive symptoms, as well as their interactions with within-person chronological aging and with between-person differences in chronological age.
Because PEF, subjective age, and chronological age were assessed multiple times (up to four times) and change over time, these contain information about both between-person differences (e.g., some individuals have better lung functioning than others) and within-person change (e.g., at a specific measurement occasion, a person might have better lung functioning than at other occasions). The multilevel framework allows for a statistical separation of these two components (e.g., Raudenbush & Bryk, 2002), which, if not explicitly separated, are fully confounded. In Equation 1, we show the components of the multilevel model for PEF as outcome.
For each individual i, their mean on the predictors was calculated across all of their available repeated assessments (e.g., mean subjective age = SA—score across all available measurement occasions). This person-specific mean corresponds to the between-person predictor (bpSAi). Subtracting this person-specific mean from each individual’s repeated assessments leads to the within-person predictor effect (e.g., wpSAit), which varies across time t.
We centered the person-specific means for subjective age (bpSAi) and chronological age (bpCAi) at the overall sample mean. This person-centered approach we applied is typical of the multilevel approach and has been proposed by Raudenbush and Bryk (2002) to effectively separate group from individual effects, when individuals behave differently within different groups.
In addition, interactions of within- and between-person effects of chronological age with the within- and between-person effects of subjective age and—when switching outcomes—lung functioning were tested. Please note that the within-person chronological aging effect (wpSAit) corresponds to the estimated annual linear (age-related) change in PEF. Accordingly, the interaction term of within-person chronological age with between-person subjective age indicates whether the extent of age-related change in PEF is different for individuals who feel overall younger versus for individuals who feel overall less young.

In follow-up analyses with additional predictors (see Equation 2), gender, year of study entry, region of residence, education, number of chronic diseases, depressive symptoms, physical activity, BMI and body height were included, as well as their interactions with the within- and between-person effects of age; we abbreviate the list of covariates in the equation by using the generic term “covariateik, where k refers to the kth covariate (k = 1–9).” These interactions indicate whether within-person age-related change in PEF varies according to these predictors (e.g., gender) or whether between-person differences according to chronological age are larger or smaller in certain groups (e.g., women vs. men, individuals with more vs. fewer chronic diseases).

Individual-specific random effects around the intercept (u0i) and around the slope of chronological age (u1i) were specified, and time-specific residuals (rit) were included. The model for subjective age as outcome was analogous, with predictor effects of subjective age replaced by the predictor effects of PEF. Our general methodological approach is in line with other previously published work (Drewelies et al., 2022; Thorvaldsson et al., 2012, 2020; Wettstein et al., 2024; Wettstein, Ghisletta & Gerstorf, 2023). Given the large sample size, we considered coefficients with p < .01 as statistically significant, to avoid the identification of statistically significant effects with trivial effect sizes. For the sake of model parsimony, we removed nonsignificant interaction terms of subjective age, lung function or any of the covariates with between-person chronological age and with within-person chronological age from the final model. 2
We computed two R² measures, namely explained variance in “Between-person diffs. in age bp” (i.e., the proportional reduction of the random intercept variance when including predictors/correlates) and explained variance in “Within-person aging wp” (i.e., the proportional reduction of the random slope variance when including predictors/correlates).
In follow-up sensitivity analyses, study participants who answered “yes” to the question whether they suffered from “respiratory problems, asthma, shortness of breath” were excluded (n = 1,367); these individuals might represent a special group with high lung function vulnerability and very low peak expiratory flow scores, and their lung function scores might affect estimated associations of peak expiratory flow with subjective age.
Statistical Power
No a-priori power analyses were conducted because of the lack of comparable previous evidence; however, samples sizes of n > 6,000 were obtained in the DEAS from 2008 on, which are largely sufficient to detect even small to medium effect sizes based on both theoretical and empirical (simulation-based) work on power in multilevel models (Arend & Schäfer, 2019; Moerbeek et al., 2008; Snijders & Bosker, 1993). Specifically, our study sample size was close to 10,000 participants with more than 18,000 observations.
Results
Table 1 summarizes the main characteristics of the study sample. The proportion of women in the sample was about 49%. At baseline, individuals felt on average 8 years younger than they were chronologically. Cross-sectionally, subjective age and PEF were unrelated (r = .01).
Descriptive Statistics at Baseline Assessment and Intercorrelations for Study Measures.
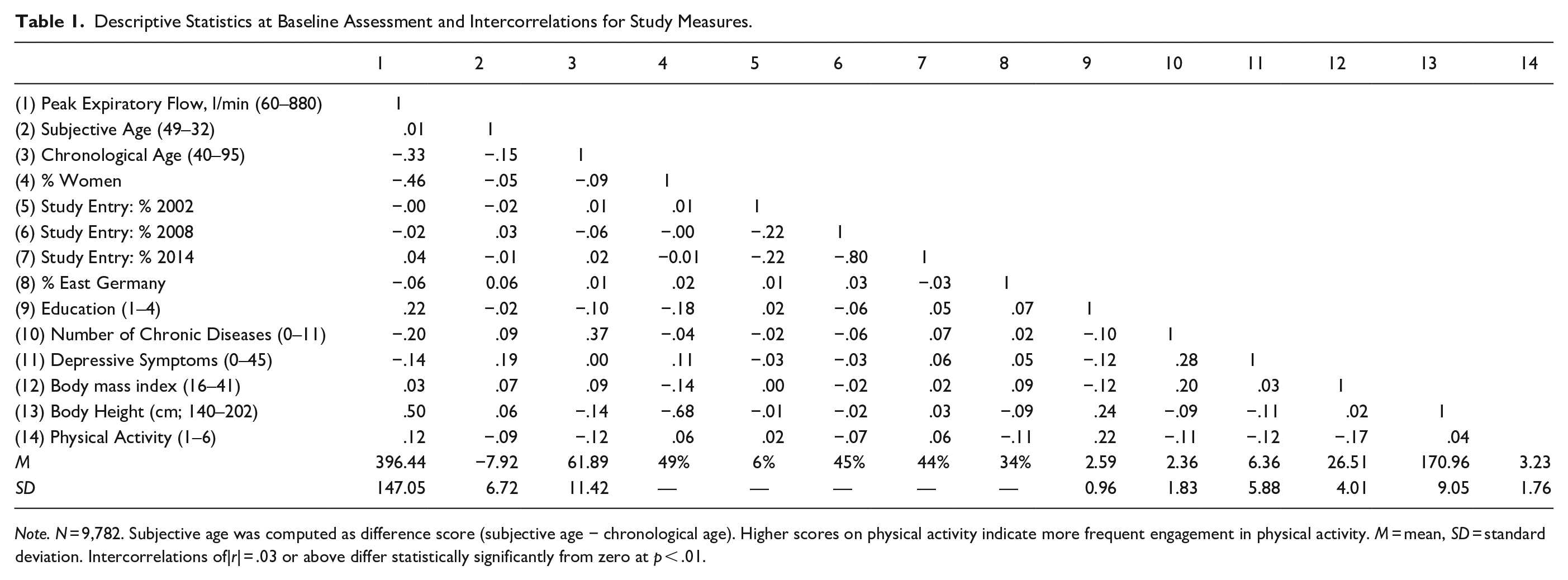
Note. N = 9,782. Subjective age was computed as difference score (subjective age − chronological age). Higher scores on physical activity indicate more frequent engagement in physical activity. M = mean, SD = standard deviation. Intercorrelations of|r| = .03 or above differ statistically significantly from zero at p < .01.
We computed the intraclass correlation (ICC) coefficients for lung function, subjective age and chronological age, based on intercept-only models, to quantify the extent of between-person vs. within-person variation in each variable. For lung function, the ICC coefficient was .75, indicating that 25% of the overall variability in lung function was due to within-person variation. The ICC coefficient for subjective age was .54, which means that almost half of the total variability in subjective age (46%) were due to within-person variation. For chronological age, the ICC coefficient was .89, indicating a proportion of within-person chronological age variation that amounted to 11%. As all three variables thus revealed a proportion of within-person variation that is greater than 10%, our approach of differentiating between-person effects from within-person effects seems justified.
Predictors of Peak Expiratory Flow
Findings from the models without covariates are shown in Supplemental Table 1.
In the model including covariates, with peak expiratory flow as outcome, lung function was predicted both by the between-person component and the within-person component of chronological age (see Table 2): At the between-person level, being one year chronologically older was associated with a by more than 4 l/min reduced peak expiratory flow (: bpCA γ01 = −4.45, p < .01). At the within-person level, with each year of aging, peak expiratory flow decreased by an average of 1.41 l/min (wpCA γ10 = −1.41, p < .001). These associations are illustrated in Figure 1.
Growth Models of Pulmonary Function (PEF) and Subjective Age (Including Correlates).
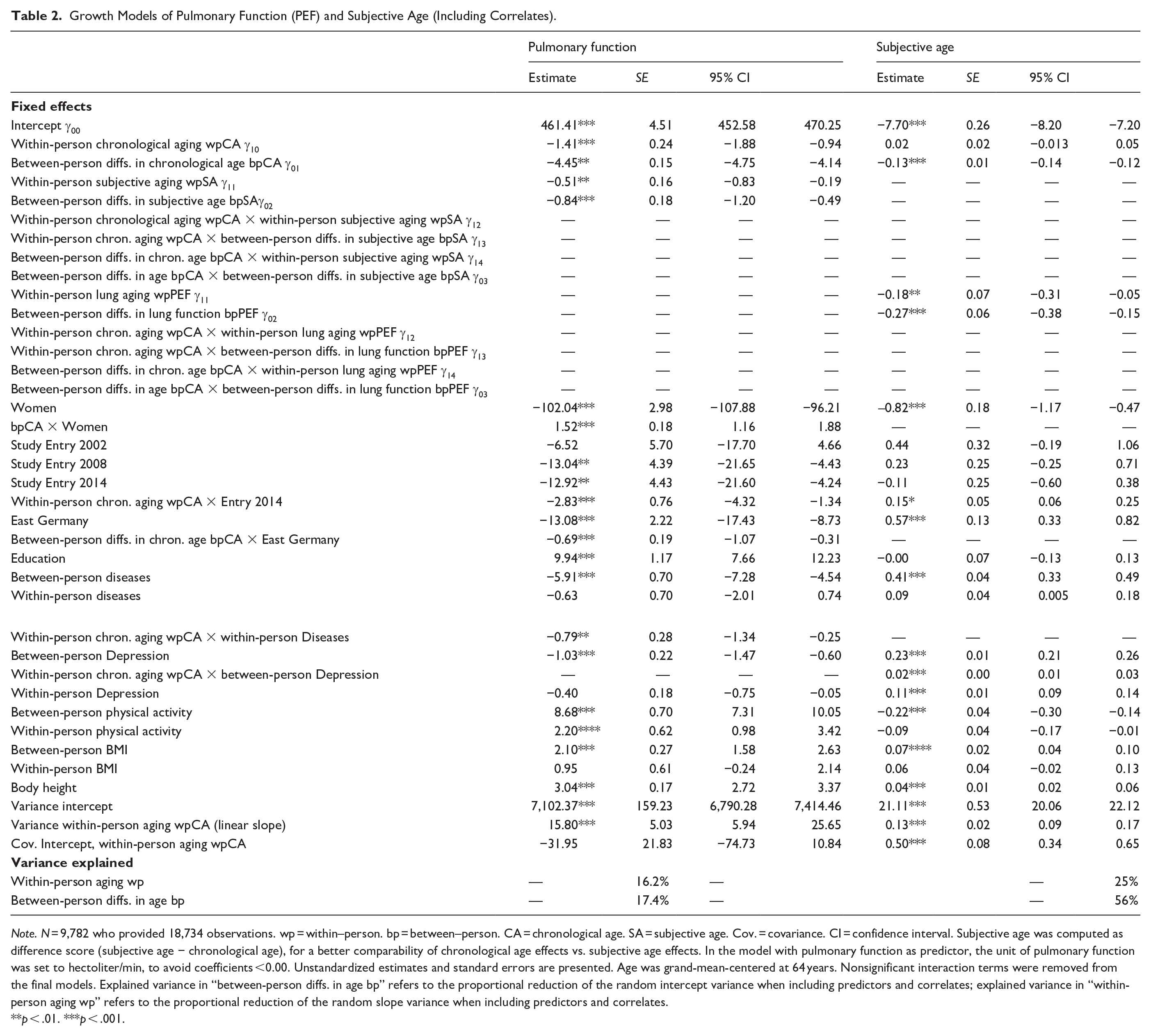
Note. N = 9,782 who provided 18,734 observations. wp = within–person. bp = between–person. CA = chronological age. SA = subjective age. Cov. = covariance. CI = confidence interval. Subjective age was computed as difference score (subjective age − chronological age), for a better comparability of chronological age effects vs. subjective age effects. In the model with pulmonary function as predictor, the unit of pulmonary function was set to hectoliter/min, to avoid coefficients <0.00. Unstandardized estimates and standard errors are presented. Age was grand-mean-centered at 64 years. Nonsignificant interaction terms were removed from the final models. Explained variance in “between-person diffs. in age bp” refers to the proportional reduction of the random intercept variance when including predictors and correlates; explained variance in “within-person aging wp” refers to the proportional reduction of the random slope variance when including predictors and correlates.
p < .01. ***p < .001.
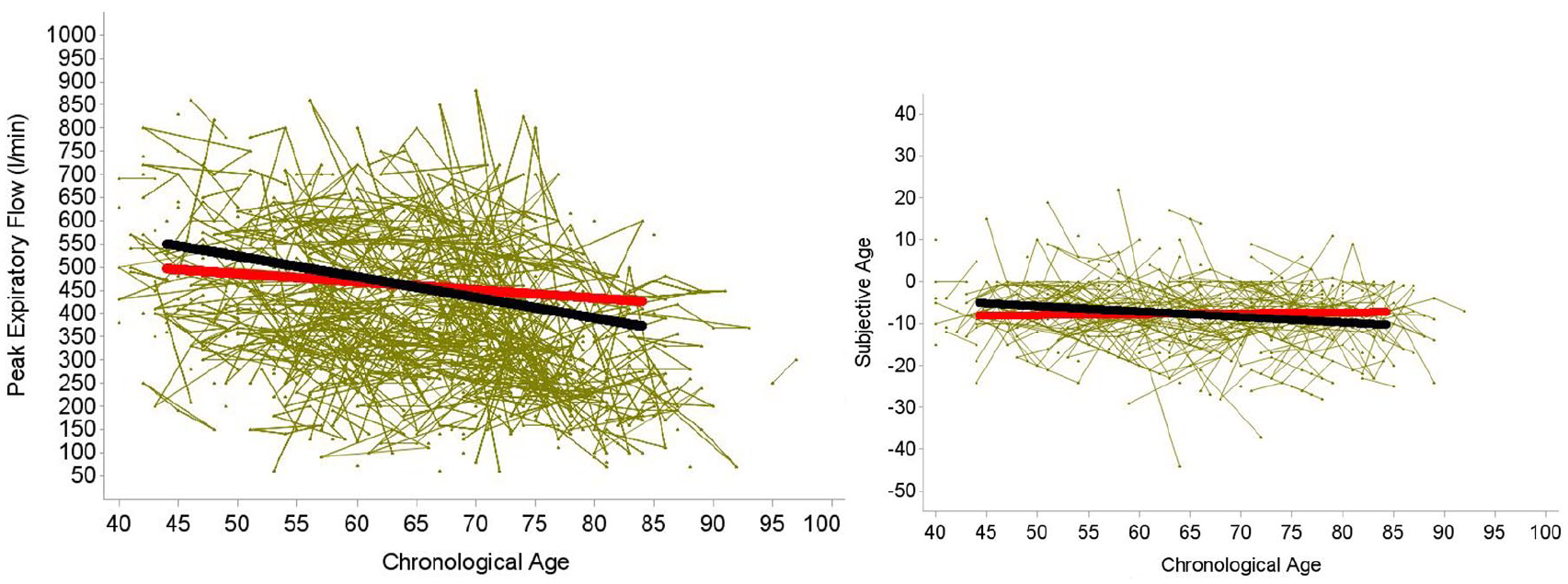
Between-Person Associations (Black Line) and Within-Person Associations (Red Line) of Chronological Age With Pulmonary Function as Indicated by Expiratory Peak Flow (l/min; Left Figure) and Subjective Age (Right Figure; Subjective Age Difference Computed as Subjective Age − Chronological Age). Based on models including correlates (see Table 2). At the between-person level, participants who were older had poorer pulmonary function. At the within-person level, as people age, their pulmonary function declines. For subjective age, the within-person effect of age was not statistically significant, indicating that the difference between subjective and chronological remains on average stable when individuals get older. The between-person effect of age on subjective age was statistically significant, indicating that chronologically older individuals feel younger. The green lines illustrate individual trajectories for a random subsample (586 individuals).
In addition, the effects of between-person subjective age and of within-person subjective age were statistically significant: Individuals who felt overall 1 year younger than others had a peak expiratory flow score that was on average higher by almost 1 l/min (bpSA γ02 = −0.84, p < .01), and on measurement occasions when individuals’ subjective age difference was larger by 2 years than their average (i.e., when they felt additionally younger by 2 years), their peak expiratory flow was higher by more than 1 l/min (wpSA γ11 = −0.51, p < .01). Both effects are illustrated in Figure 2. Interactions of within-person subjective age and of between-person subjective age with within-person chronological age and with between-person chronological age did not reach statistical significance, and these interactions were therefore trimmed from the final models.
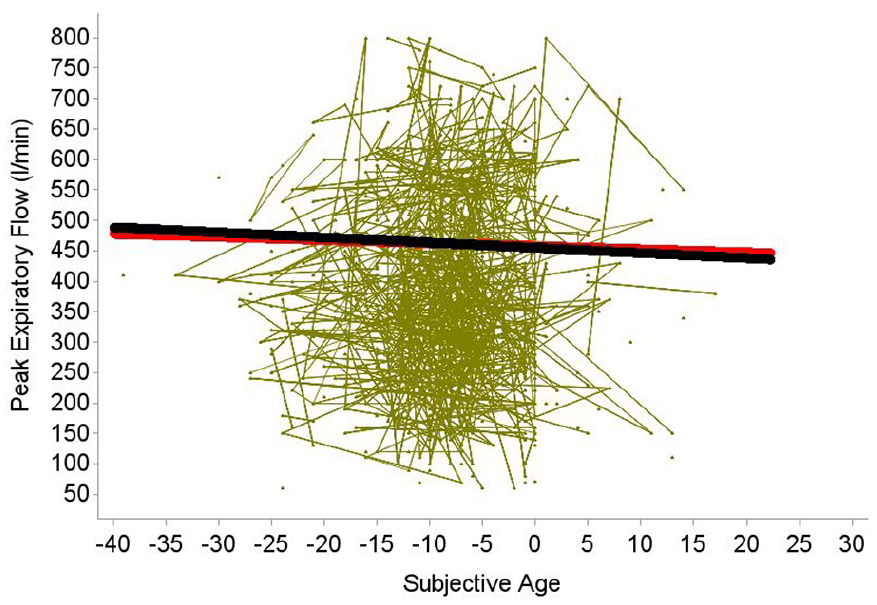
Illustrating the Between-Person Age Association (Black Line) and the Within-Person Age Associations (Red Line) of Subjective Age (Difference Score: Subjective Age − Chronological Age) With Pulmonary Function as Indicated by Expiratory Peak Flow (l/min). Based on the model including correlates (Table 2). The between-person effect and within-person effect of subjective age on pulmonary functioning are negative and significant. Individuals with an overall older subjective age have poorer pulmonary function, and on occasions when individuals feel older, their pulmonary function is lower. The green lines illustrate individual trajectories for a random subsample (586 individuals).
Predictors of Subjective Age
In the model including covariates with subjective age specified as outcome (Table 2), chronologically older individuals reported relatively younger subjective ages, and a difference of 10 years in chronological age was associated with a difference of more than 1 year in the subjective age difference score (bpCA γ01 = −0.13, p < .001). In contrast, the within-person age effect was not significant (wpCA γ10 = 0.02, p = .25), indicating that subjective age (i.e., the relative difference between subjective age and chronological age) remained on average stable when individuals got older. Associations are illustrated in Figure 1.
In addition, the between- as well as the within-person effects of lung function on subjective age were statistically significant (see Figure 3): Individuals whose overall peak expiratory flow score was higher by 100 l/min had a subjective age that was younger by 0.27 years (bpPEF γ02 = −0.27, p < .001), and on measurement occasions when an individual’s peak expiratory flow was higher by 100 l/min, they felt younger by about 0.2 years (wpPEF γ11 = −0.18, p < .01). Interactions of within-person peak expiratory flow and of between-person peak expiratory flow with within-person and between-person chronological age did not reach statistical significance, and these interactions were therefore trimmed from the final models.
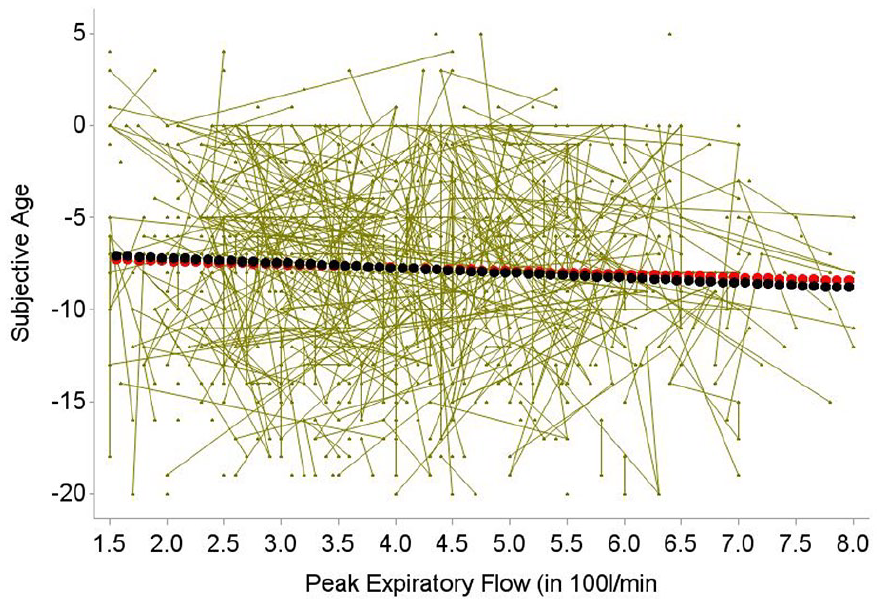
Illustrating the Between-Person Age Association (Black Line) and Within-Person Age Association (Red Line) of Pulmonary Function as Indicated by Peak Expiratory Flow (in 100 l/min) with Subjective Age (Calculated as Subjective Age-Chronological Age). Based on the model including correlates (Table 2). Overall poorer pulmonary function is significantly associated with an older subjective age. At the within-person level, individuals report a younger subjective age on measurement occasions when their pulmonary function is better. The green lines illustrate individual trajectories for a random subsample (586 individuals).
For lung function, 14.7% of the between-person variance as well as 8.3% of the within-person age variance could be accounted for by the between-person and within-person effects of chronological age and subjective age (see Supplemental Table 1); these proportions increased to 56% and 25%, respectively, when adding the covariates (see Table 2). For subjective age, explained variance proportions were 4.3% for between-person variance and 1% for within-person variance in the zero-order model (see Supplemental Table 1) and 17.4% and 16.2%, respectively, when adding the covariates (see Table 2). When predicting lung function, adding between-person and within-person effects of subjective age contributed to an increment in R² of 0.4% in between-person differences and of 1.3% in within-person changes, which corresponds to a small effect size. When predicting subjective age, adding between-person and within-person effects of lung function contributed to an increment in R² of 0.4% in between-person differences and of 0.8% in within-person changes, which again reflects a small effect. A detailed description of the effects of the covariates and their interactions with between-person and within-person chronological age is provided in the Online Supplemental Material.
Follow-Up Sensitivity Analyses
In a set of follow-up analyses, we tested the robustness of the findings obtained. Specifically, we excluded participants reporting respiratory problems, asthma, and shortness of breath (n = 1,367) because these might represent a special group with very low peak expiratory flow scores and particular dynamics. Theoretically, the associations observed between peak expiratory flow and subjective age might have been driven by the inclusion of individuals with respiratory problems, as severe restrictions in lung function might be related with feeling older, whereas lung function might be less strongly related with subjective age as long as it is not severely compromised. However, in the models with peak expiratory flow/subjective age as outcome and without as well as with correlates, most significant effects could be replicated. Specifically, in the model specifying peak expiratory flow as outcome and including all correlates, the within-person chronological aging effect on peak expiratory flow was no longer significant (wpCA γ10 = −1.30, p = .09), whereas all other effects of chronological and subjective age were statistically significant (bpCA γ01 = −4.91, p < .001; wpSA γ11 = −0.53, p < .01; bpSA γ02 = −0.83, p < .001). In the model including correlates that specified subjective age as outcome, most effects were identical to the findings when including the subgroup of individuals with respiratory problems, such as the nonsignificant within-person chronological age effect (wpCA γ10 = 0.004, p = .94) and the significant effects of between-person chronological age (bpCA γ01 = −0.10, p < .01), and between-person peak expiratory flow (bpPEF γ02 = −0.29, p < .001); however, the within-person peak expiratory flow effect now failed to reach statistical significance (wpPEF γ11 = −0.16, p = .02), which could to some extent also be due to the reduced sample size after excluding 1,367 individuals. Generally, these sensitivity analyses imply that associations between subjective age and lung function do not seem to be limited to individuals with major respiratory problems. As additional sensitivity analyses, we considered respiratory problems as additional predictor and specified its interactions with subjective age and pulmonary function. Not surprisingly, individuals with respiratory problems had a lower PEF score (γ = −55.302, p < .001), and they also reported feeling less young (γ = 1.372, p < .001) as compared to individuals without respiratory problems. However, all interactions terms of respiratory problems with subjective age and lung function were not statistically significant, indicating that between-person and within-person associations between subjective age and lung function are similar among those with respiratory problems and those who do not have such respiratory complaints.
Discussion
In this study, we examined how subjective age and lung function are longitudinally interrelated in a sample of middle-aged and older individuals. We statistically disentangled between-person and within-person associations and controlled for relevant socio-demographic and health-related correlates to investigate the robustness of associations. We also analyzed the extent to which associations between subjective age and lung function are moderated by within-person or between-person chronological age.
Multiple Co-Occurrences of Subjective Age and Pulmonary Function
All between-person and within-person associations between lung function and subjective age were statistically significant and remained robust and similar in size in models adjusting for further correlates, in line with our original expectations. Specifically, individuals with overall better lung function feel younger and vice versa, and on occasions when individuals exhibit a higher peak expiratory flow score, they also feel younger and vice versa. In prior analyses based on the same data, Wettstein et al. (2024) found that between- and within-person associations between subjective age and pain in midlife and later life are significant and robust. The findings of the present study thus demonstrate that such between- and within-person associations between subjective age and health are not limited to subjective health indicators (such as pain), but can be also observed for objective health indicators and biomarkers such as pulmonary function, although underlying pathways might vary according to the specific health domain that is considered. The associations were small in terms of effect sizes, but independent of (time-varying) factors such as depressive symptoms, physical activity, or chronic diseases. These factors might thus not be major mediators of the associations between subjective age and peak expiratory flow. We also replicated most effects of subjective age on peak expiratory flow and vice versa when excluding individuals with respiratory problems (such as asthma) and when considering respiratory problems as additional predictor and moderator, so effects do not seem to be solely driven by the impact of such respiratory problems on peak expiratory flow and subjective age.
Our findings can be seen in line with prior findings that demonstrated reciprocal associations between subjective age and health (e.g., Spuling et al., 2013; Wettstein et al., 2024), though such prior findings were mostly restricted to subjective health indicators. Subjective age thus seems to be reactive to physiological changes, which might contribute to its association with biomarkers and biological age (Schönstein et al., 2022; Stephan et al., 2022, 2015a, 2015b; Thyagarajan et al., 2019). At the same time, subjective age might be a predictor of these physiological changes, such as change in lung function, possibly via its associations with lifestyle factors such as physical or social activity (Schwartz et al., 2020; Stephan et al., 2014; Stephan, Sutin, & Terracciano, 2018), which—according to one study—also precede a younger subjective age (Stephan et al., 2020).
Although we found associations that were robust, they were modest in size. As one example, a between-person or within-person difference in subjective age of one year makes a difference of less than 1 l/min in peak expiratory flow. This is in line with other findings. For instance, Westerhof et al. (2023) found, based on their meta-analysis on the effects of subjective aging on health outcomes, overall small effects. There is thus a robust association between subjective age and lung functioning, but various other predictors seem to play a role as well.
Another noteworthy finding is that, apart from very few exceptions, associations between lung function and subjective age were not moderated by within-person or between-person effects of chronological age. These associations thus seem to remain stable across the second half of life and are similar in midlife, old age, and very old age (see also Spuling et al., 2013). These findings inform the larger debate in the literature about whether or not associations between subjective age and health vary with chronological age. While age moderation effects might have emerged in a study sample including young adults, our findings suggest that the extent to which good lung function is relevant for feeling younger and vice versa does not change within the second half of life, so that efforts to promote lung health and younger subjective ages should not be restricted to a specific age group but rather address middle-aged as well as older and very old adults.
Study Limitations
In closing, we note limitations of our study sample, measures, and design. As limitations of our sample, we would like to point out that chronologically very old adults were somewhat underrepresented in our study, with > 99% of the sample being younger than 85 years. Therefore, our data cannot test whether associations are different in very old age or in vulnerable subgroups such as hospitalized individuals or nursing home residents as the DEAS sample is a non-clinical sample of community-dwelling middle-aged and older individuals. This could result in an underestimation of the extent to which lung function declines over time, also due to selective dropout of study participants, particularly of those with lower levels of education and physical activity, although our selective dropout analyses revealed effects that were all below medium effect size, and the use of Full Information Likelihood estimation as well as the inclusion of dropout-informative covariates (such as chronic conditions or depressive symptoms) should have minimized the impact of selective dropout on the estimated effects.
As limitations of our measures, we note that although peak expiratory flow is meaningfully related with health and mortality (Cook et al., 1991; Donahue Patrick et al., 2023; Roberts & Mapel, 2012; Trevisan et al., 2019, 2020; Vaz Fragoso et al., 2008; Zhang et al., 2023), there are other lung function markers such as forced expiratory volume, that are not necessarily strongly related with peak expiratory flow and might thus capture additional facets of lung health (e.g., Hegewald et al., 2007). Future research should thus investigate and compare how different lung function tests may relate to subjective age and views on aging. We also note that with the exception of lung function, all study variables were assessed based on self-reports, and peak expiratory flow was the only objective health information available in the German Aging Survey, so that we could not investigate associations of subjective age with a broader set of objective health or biomarker variables. As pointed out above, associations might vary across biomarkers, as Stephan et al. (2015a) found that “perceptible biomarkers” such as peak expiratory flow or grip strength are associated with subjective age, whereas not-perceptible ones, such as telomere length, are not. More research is needed to determine whether associations with subjective age permeate across various biomarkers and to establish discriminant validity of each single biomarker.
Moreover, the observational study design does not allow for detection of short-term changes or fluctuations in subjective age and lung function, and it does not allow for firm causal conclusions. For instance, the within-person association of a younger subjective age with better peak expiratory flow could either imply that feeling younger leads to better peak expiratory flow or vice versa (or reciprocal influences). Investigating time-lagged associations, for example, by means of bivariate dual change score models, might allow for conclusions with regard to temporal ordering of effects, but based on this method, a differentiation of between-person effects vs. within-person effects is not possible. Random-intercept cross-lagged panel models (Hamaker et al., 2015) allow for the estimation of cross-lagged associations while controlling for between-person differences via adding random intercept components, but they do not contain a long-term change component (Usami et al., 2019), which is, however, required whenever lifespan developmental phenomena (such as lung function)—which are by definition changeable over time—are investigated. Long-term change is represented in our model by the effects of within-person chronological age. Although our analytical approach may be limited with regard to causal interpretation, it “is currently regarded as best practice for the disaggregation of between-person and within-person effects in multilevel growth models” (Curran & Bauer, 2011, p. 591).
To better understand the causality, mechanism-oriented research is needed to investigate potential mediators of the associations as well as experimental approaches (e.g., does manipulating subjective age alter peak expiratory flow?). We hypothesize that, while strengthening the internal validity of the subjective age-pulmonary function associations, an experimental study would most likely address associations on widely different time scales, over much shorter epochs than those typically investigated in an observational study, which addresses mechanisms unfolding over decades, rather than days or weeks (Hopwood et al., 2021).
Conclusion
In a sample of middle-aged and older adults, we found evidence in support of meaningful between-person and within-person associations of subjective age and lung function. Better lung functioning is associated with a younger subjective age and vice versa. Given the considerable relevance of subjective age for health and mortality (Stephan, Sutin, & Terracciano, 2018; Westerhof et al., 2023), our findings highlight another important health domain that is predicted by subjective age, namely lung health. Moreover, our study findings suggest that subjective age is also reactive to changes in lung health. At the same time, effect sizes were modest. However, in terms of practical implications, an older subjective age is, unlike an older chronological age, a modifiable risk factor with regard to lung functioning, so that promoting younger subjective ages—which seems possible (e.g., Stephan et al., 2013)—could contribute, via behavioral (e.g., physical and social activity) and other factors, to healthy aging, including better lung functioning. Also, prevention and interventions to promote lung functioning seem to be promising to contribute to younger subjective ages, which in consequence have a positive impact on health and longevity.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254251331177 – Supplemental material for Subjective age and pulmonary function in midlife and old age: Evidence for between-person associations and within-person co-occurrence
Supplemental material, sj-docx-1-jbd-10.1177_01650254251331177 for Subjective age and pulmonary function in midlife and old age: Evidence for between-person associations and within-person co-occurrence by Markus Wettstein, Paolo Ghisletta, Ilja Demuth and Denis Gerstorf in International Journal of Behavioral Development
Footnotes
Data Availability Statement
Data from the German Aging Survey can be obtained via the German Centre of Gerontology (n.d.), Research Data Centre (https://www.dza.de/en/research/fdz/access-to-data; for materials, questionnaires, interview codebook, see Engstler et al., 2022). The analytic code for the following analyses can be obtained from the Online ![]() . Analyses and hypotheses were not pre-registered. There was no prior dissemination of the reported study findings.
. Analyses and hypotheses were not pre-registered. There was no prior dissemination of the reported study findings.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article reports data from the German Aging Survey (DEAS), which was funded under Grant 301-6083-05/003*2 by the German Federal Ministry for Family, Senior Citizens, Women, and Youth. The content is the sole responsibility of the authors.
Ethical Approval and Informed Consent Statement
Ethical approval was not obtained because this is not required for general surveys in Germany. The German Aging Survey does not employ any invasive methods. The survey maintains an academic advisory board which ensures its scientific quality. All study participants provided informed consent prior to study participation.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.