
Abstract
The Lines-of-Defense model postulates that older adults should engage in important health goals and behaviors for as long as possible and adjust them downwardly only when they become impossible to pursue. This process is thought to be supported by goal engagement and self-protective control strategies. We tested this model in a 4-year longitudinal study of 236 older adults by predicting the maintenance of physical activity using accelerometers. We hypothesized that older adults would exert shifts from more strenuous (e.g., vigorous and moderate intensity) to less strenuous (e.g., light intensity) physical activity over time. In addition, we expected that these processes would be supported by the use of health-specific control strategies. Multilevel modeling revealed that older adults experienced declines in moderate and vigorous physical activity but increases in light physical activity. Health engagement predicted an accelerated increase in light physical activity, and exerted substantial, but longitudinally decreasing, benefits for moderate physical activity. Health-related self-protection, by contrast, predicted the maintenance of vigorous physical activity over time. These results support the Lines-of-Defense model by demonstrating that control strategies can predict the maintenance of older adults’ physical activity levels.
Introduction
Older adults face age-related challenges related to morbidity and mortality (Statistics Canada, 2018). Adaptive health behaviors, such as physical activity, have been shown to ameliorate these challenges. Physical activity ranges from light (e.g., housework) to moderate (e.g., brisk walking) and vigorous (e.g., running) intensity behaviors, and has been positively associated with older adults’ mental and physical health. Physical activity, however, often deteriorates in older adulthood (McAuley et al., 2006). Here, we use the Lines-of-Defense model (Heckhausen et al., 2013) to understand the motivational processes that may counteract an age-related decline in physical activity. This model postulates that older adults should maintain the pursuit of health-related goals and activities for as long as possible, and only downwardly adjust them if further pursuit has become truly impossible. In addition, these processes are thought to be facilitated by an orchestrated use of health-specific control strategies (Heckhausen et al., 2013). Control strategies may promote the pursuit of still feasible health behaviors, protect motivational and emotional resources needed for adaptive action, or facilitate adaptive goal disengagement (Heckhausen et al., 2010). We hypothesized that older adults would show longitudinal reductions in their levels of more strenuous physical activity (e.g., moderate or vigorous intensity), but increases in less strenuous physical activity (e.g., light intensity; for compensation of physical activity, see Rowland, 1998). In addition, health-specific control strategies were expected to modulate these trajectories by supporting the maintenance of still feasible physical activity.
Physical Activity in Older Adults
According to the World Health Organization (WHO, 2022) guidelines, older adults should engage in at least 150 min of moderate intensity or 75 min of vigorous intensity physical activity per week. Importantly, a lack of physical activity is one of the five leading risk factors for death (WHO, 2010), and might elevate blood pressure, glucose levels, cognitive decline, and obesity (Taylor et al., 2004). Despite this, older adults are considered to be the most physically inactive population (Azagba & Sharaf, 2014). Age-related challenges (e.g., onset of chronic conditions, fewer social support, reduced access to lower cost facilities) can lead to mobility constraints and decreases in motivation (Picorelli et al., 2014; Smith et al., 2017; Statistics Canada, 2018). As this population continues to grow, physical inactivity may pose major problems for quality of life and the health care system (Azagba & Sharaf, 2014).
To date, most research related to the benefits of physical activity is based on self-report measures that introduce overestimations of behaviors. Self-reporting is based on intentional, routine, and planned physical activity and these reports often miss important unintentional bouts of activity that may contribute to health outcomes. It can also be affected by age-related deficits in memory and understanding (Arvidsson et al., 2019; Haskell, 2012). Device-measured physical activity can overcome these limitations, and accelerometry is now the most widely used measurement device for physical activity and is reliably associated with mortality and physiological biomarkers (Taylor et al., 2004).
The Importance of Control Strategies for the Management of Goals
To examine motivational factors that could facilitate physical activity, our study is informed by the Motivational Theory of Life-Span Development (MTD; Heckhausen et al., 2010), and its companion theory, the Lines-of-Defense model (Heckhausen et al., 2013). The MTD’s aim is to understand individuals’ capacity to optimize their development across the lifespan throughout significant transitional periods using motivational processes (Heckhausen et al., 2010). Based on biological, socio-structural, and age-normative factors, people’s capacity to successfully pursue important goals increases during the earlier parts of adulthood, plateaus in midlife, and exerts sharp declines in older adulthood (Heckhausen & Schulz, 1995).
To manage the waxing and waning opportunities for producing adaptive outcomes, people can engage in different types of control strategies that support either goal attainment (e.g., goal engagement) or psychological adjustment to goal failure (e.g., self-protection or goal disengagement; Heckhausen et al., 2010). Goal engagement strategies involve the investment of time and effort, recruitment of external resources, and an increase in motivational focus of a goal, and should be most adaptive during life periods when goals are attainable and constraints on behavior can be overcome. However, when it becomes increasingly difficult or impossible to pursue a goal-related activity, people might engage in self-protective strategies (e.g., positive reappraisals or protective attributions). These strategies include reframing adverse health-related circumstances in a more positive way through “silver lining” or positive reappraisals, as well as avoiding self-blame for health-related problems (Heckhausen et al., 2010). The use of these strategies may help maintain a person’s motivational and emotional resources for adaptive action and facilitate acceptance and goal disengagement.
Much empirical research from different domains of life (e.g., childbearing, financial, or partnership goals; Heckhausen et al., 2001; Wrosch et al., 2000; Wrosch & Heckhausen, 1999) has supported the assumption that, as people advance in age, they exert adaptive shifts from goal engagement to self-protection (for reviews, see Heckhausen et al., 2019, 2024). In the health domain, cross-sectional and longitudinal investigations show that both health engagement and health-related self-protection benefit older adults’ subjective well-being, physiological regulation (e.g., cortisol and inflammation), and physical health (Rueggeberg et al., 2012; Wrosch et al., 2009; Wrosch & Schulz, 2008). In addition, the adaptive effects of health engagement strategies appear particularly evident among older adults who confront potentially manageable health threats, but not relatively intractable health problems (Wrosch & Schulz, 2008). The latter pattern of findings indicates that in addition to self-protective strategies, active engagement in still feasible health goals and behaviors also remains important in old age.
Lines-of-Defense Model and Older Adults’ Physical Activity
The Lines-of-Defense model can be used to study adaptive motivational processes in the context of progressive health threats (Heckhausen et al., 2013, 2019, 2024). It postulates that people should hold a line of defense to protect the pursuit of important health goals or behaviors for as long as possible. This process may begin with cutting back on the duration or scope of goal-related activities that have become difficult to maintain (e.g., running at shorter distances). Only when it becomes impossible to perform the activity any longer, people should step behind the next line of defense by replacing the original goal with another, still feasible activity (e.g., cycling or walking instead of running). In the context of physical activity, older adults may thus reduce, over time, moderate and vigorous physical activity, but increase less strenuous physical activity (e.g., light intensity) to remain engaged in the pursuit of important health-related activities (Heckhausen et al., 2024).
The latter process is thought to be facilitated by an orchestrated use of control strategies (Heckhausen et al., 2013) where health engagement strategies could be useful for maintaining the pursuit of a threatened health behavior. Moreover, they should promote a newly adopted and still feasible health-related activity, in particular those with favorable opportunities (Wrosch & Schulz, 2008). In terms of physical activity, health engagement strategies may then show stronger effects on the pursuit of less strenuous activity (e.g., light intensity), as compared with more strenuous activity (e.g., moderate or vigorous intensity).
With respect to self-protective strategies, our theoretical rationale would suggest two contradictory scenarios. First, health-related self-protection could help maintain motivational and emotional resources needed for adaptive action (Heckhausen et al., 2019, 2024). It may support that people do not abandon the pursuit of a health-related activity prematurely but continue their engagement or reduce its scope to the level of feasibility. However, arguably those self-protective strategies that help maintain motivational and emotional resources for action may be less needed for pursuing health behaviors that involve favorable opportunities since people should be able to engage in those behaviors without using self-protection. With respect to physical activity in older adulthood, it would thus be reasonable to assume that health-related self-protection can be less effective for light-intensity physical activity but more effective for more strenuous moderate and vigorous physical activity.
Second, self-protective strategies have been conceptualized to support disengagement from unattainable goals by enabling people to accept that they can no longer be pursued (Heckhausen et al., 2019). This possibility, however, would lead to a different set of predictions. If self-protection promotes disengagement from unfeasible health behaviors, it may result in a higher likelihood of engaging in downwardly adjusted health behaviors, but in a lower likelihood of engaging in difficult/unfeasible health behaviors. In terms of physical activity, it could thus also promote the engagement in light-intensity physical activity but exert a reversed effect on the pursuit of more strenuous physical activity.
The Present Study
This study examined the roles of health-specific control strategies for maintaining objective physical activity in a longitudinal study of older adults. We hypothesized that older adults would show longitudinal increases in their levels of light-intensity physical activity and reductions in more strenuous moderate and vigorous physical activity. We also hypothesized that health-specific control strategies would moderate older adults’ trajectories of physical activity. We expected health engagement strategies to positively predict the maintenance of all intensities of physical activity with stronger effects for predicting less, as compared with more, strenuous physical activity. With respect to health-related self-protection, our hypotheses remain explorative because the theoretical rationale allowed for two contradictory scenarios. Specifically, self-protective strategies may help maintain resources needed for adaptive action, facilitating engagement in more, as compared with less, strenuous physical activity. Alternatively, they may foster acceptance and disengagement from unfeasible health goals and predict a reduction of more strenuous physical activity, but an increase in less strenuous physical activity.
Method
Participants
The present study included a longitudinal assessment of older adults who participated in the Montreal Aging and Health Study (MAHS) which launched in 2004 with an original sample size of 215. Participants consisted of a heterogeneous sample of community-dwelling older adults recruited through local newspaper advertisements in Montreal. After baseline, participants were followed every 2 years, and the cohort was refreshed at Time (T) 6 in 2014 (N = 268; 95 original and 173 new participants). To determine sample size, power was estimated in the original grant proposal, using the available literature for the magnitude of effect sizes and interaction effects. The study’s power estimates had a range of .88 to 1.00 and .97 to .77 for main effects and interaction effects respectively (Barlow et al., 2022). This study (“Self-Regulation of Health Challenges in Old Age: Benefits for Older Adults’ Psychological and Physical Health”) was approved by the Concordia University Human Research Ethics Committee (#10000402).
We examined data from T6 through T8, a period of 4 years, because physical activity was only measured with accelerometers beginning at T6 (N = 268). Participants were included if they were over the age of 60 years and had completed the self-reported measures. One participant turned 60 the year of data collection and was retained in the sample. Based on the obtained distribution of wear time of the accelerometer, outliers were identified, and physical activity data were excluded for days when the accelerometer was worn for less than 7 hr. Most participants (94.9%) wore the accelerometer for more than 10 hr. After excluding 28 participants due to missing physical activity data and four participants for missing data on health-related control strategies, the final sample consisted of 236 participants (MAge = 74.84, range = 59–93, SDAge = 7.79, 39% male). The excluded participants were on average older, M = 79.06, SD = 7.37; t(266) = 2.90, p < .01, than included participants. They did not differ from included participants on any other covariate or main study variable used in this study (ps > .18).
The subsequent waves, T7 and T8, included 188 and 159 participants, respectively. Study attrition over T6 to T8 was attributable to death (n = 19), refusal to participate (n = 37), illness (n = 6), inability to contact (n = 24), inability to follow directions (n = 3), or personal reasons (n = 1). Participants who dropped out of our study sample were significantly older at baseline (M = 78.07, SD = 7.40) than participants who remained, M = 73.53, SD = 7.66; t(193) = -3.00, p < .01, but did not differ on any other baseline variables.
Materials
Health-Specific Control Strategies
We measured health-specific control strategies at T6 using 12 items from a previously validated instrument (Rueggeberg et al., 2012). Health engagement control strategies included the average of nine items designed to measure three types of control strategies pertaining to the attainment of health goals: selective primary control (three items; for example, “I do whatever is necessary to be as healthy as I possibly can be”), selective secondary control (three items; for example, “When I decide to do something about a health problem, I am confident that I will achieve it”), and compensatory primary control (three items; for example, “If I develop a new health problem, I immediately get help from a health professional”). Health-related self-protection was measured as the average of the remaining three items, including positive reappraisals (e.g., “When I am faced with a bad health problem, I try to look at the bright side of things”) and self-protective attributions (e.g., “When I find it impossible to overcome a health problem, I try not to blame myself”). Participants responded to all items on a 5-point Likert-type scale, ranging from 1 (almost never true) to 5 (almost always true). Cronbach’s alphas for health engagement and health-related self-protection were .85, and .66, respectively.
Physical Activity
Measurements of physical activity were taken using portable waist Actigraph GT3X accelerometers (Pensacola, FL). Participants were asked to wear the accelerometer on their hip during waking hours for 3 non-consecutive days during each study wave (T6–T8), excluding periods involving water activities (e.g., bathing, showering). Participants were asked to select days that they consider as normal, and consecutive days were avoided to minimize the possibility that certain events (e.g., medical appointment) may affect the measurement across all three days. The number of daily hours during which the accelerometer was worn was also recorded. Light (100–1,951 counts/min), moderate (1,952–5,724 counts/min), and vigorous (>5,725 counts/min) physical activity were calculated on evidence-based manually applied cut-off points using ActiLife, a data analysis and management software (Freedson et al., 1998). Using these cut-off points, physical activity was computed for each of the intensities in minutes as the average over the 3 non-consecutive days. The 3 days were significantly correlated (rs > .62, ps < .001). Sedentary behaviors were not included in the obtained physical activity measures.
Covariates
The covariates in this study were assessed at T6 and included age, sex, education level, chronic illness, and wear time of the accelerometer. Sex was coded as 0 (Male), 1 (Female). For education level, participants reported their highest degree of education, ranging from no educational history (coded as 0) to a doctoral degree (coded as 16). Chronic illness was assessed as the sum of 17 different chronic health problems which participants self-reported (e.g., high blood pressure, arthritis, cancer, and diabetes; Wrosch et al., 2007). Wear time was computed as the average amount of time in minutes that participants wore the accelerometer at T6.
Missing Data
We used multilevel modeling when analyzing the data (HLM 8.2, Raudenbush & Congdon, 2021), which has the capacity to handle missing data at Level 1, but not at Level 2. Level 1 variables represent intra-individual differences across time (i.e., physical activity variables and time in study) and were used to explore how physical activity varied across time. Level 2 variables reflect inter-individual differences and were used to predict average levels of physical activity and change in physical activity over time by the covariates, including age, sex, chronic illness, and wear-time, and the predictor health-related control strategy variables. Since Level 2 missing data corresponded to less than 5% of the total sample, we replaced the missing data with the sample mean for those variables (Tabachnick & Fidell, 2018).
Data Analyses
We computed descriptive statistics and zero-order correlations among variables. Hierarchical linear modeling was used to test the study’s main hypotheses. Separate Level 1 models predicted how physical activity varied across T6 to T8 as a function of an intercept, person-centered scores of time (in years), and a residual term. The intercept represented average levels of light, moderate, and vigorous physical activity across the study waves. The time slopes referred to yearly change in physical activity levels. Prior to the analyses, Level 2 predictor variables were standardized. The Level 2 model predicted the intercept and slopes obtained in Level 1 by participants’ health engagement and health-related self-protection strategies, and the study covariates (age, sex, education level, chronic disease, and wear time). Significant cross-level interactions were followed-up by simple slope analyses.
Results
Descriptive Findings
The means, standard deviations, and percentages of the main study variables are reported in Table 1. At T6, baseline, participants were on average 74.84 years old (range = 59–93), 39% male, and had an average wear time at T6 of 811.26 min. Participants reported on average 2.34 chronic illnesses and 57.6% reported their highest level of education as a college diploma or higher.
Means, Standard Deviations and Frequencies of Main Study Variables.
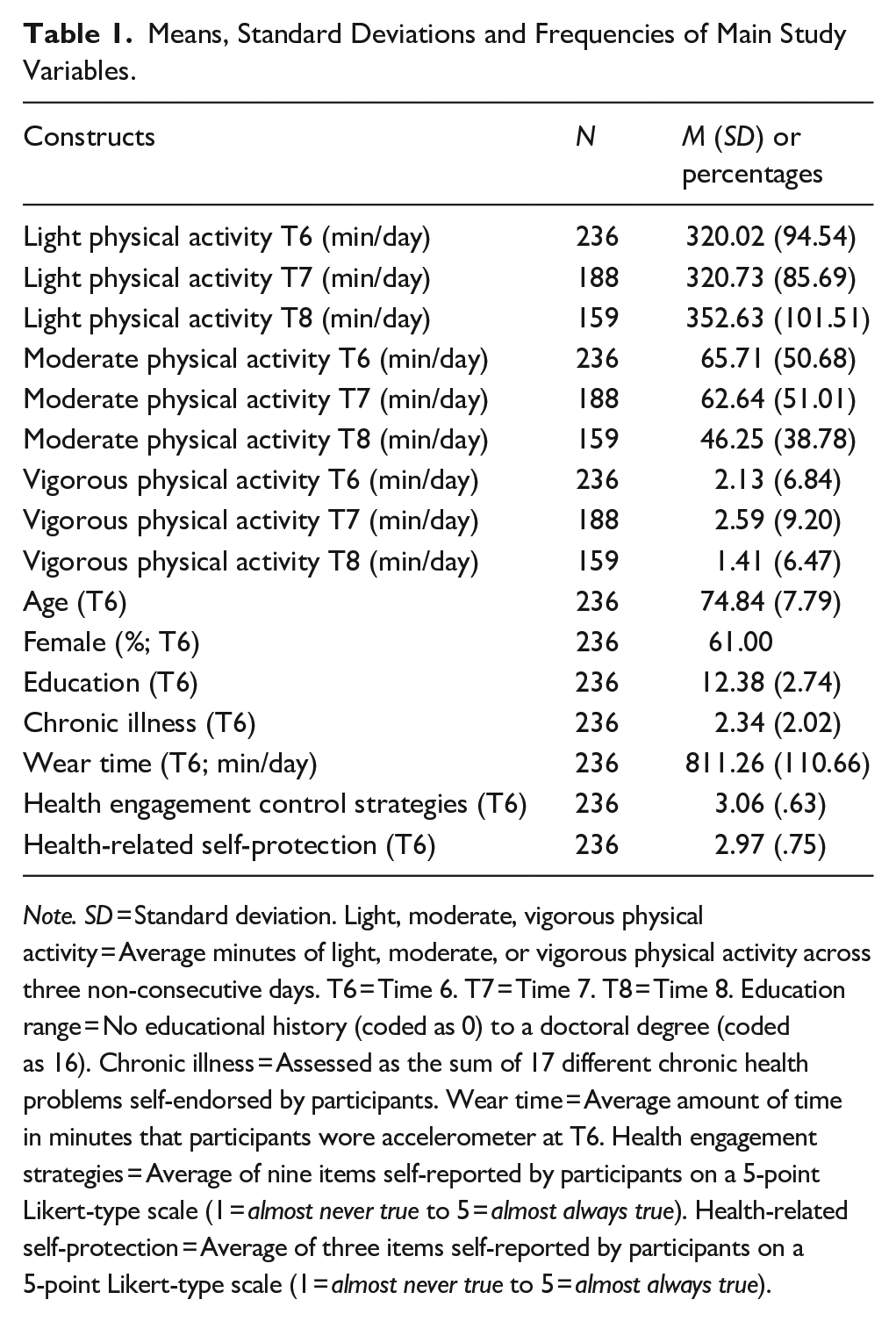
Note. SD = Standard deviation. Light, moderate, vigorous physical activity = Average minutes of light, moderate, or vigorous physical activity across three non-consecutive days. T6 = Time 6. T7 = Time 7. T8 = Time 8. Education range = No educational history (coded as 0) to a doctoral degree (coded as 16). Chronic illness = Assessed as the sum of 17 different chronic health problems self-endorsed by participants. Wear time = Average amount of time in minutes that participants wore accelerometer at T6. Health engagement strategies = Average of nine items self-reported by participants on a 5-point Likert-type scale (1 = almost never true to 5 = almost always true). Health-related self-protection = Average of three items self-reported by participants on a 5-point Likert-type scale (1 = almost never true to 5 = almost always true).
The zero-order correlations among the main study variables are reported in Table 2. In terms of significant associations, lower average levels of light, moderate, and vigorous physical activity were significantly associated with older age. Age was also positively associated with chronic illness and negatively associated with education level and wear time. Identifying as female was positively associated with higher average levels of light physical activity at T6 and T7. Education level was positively associated with moderate physical activity at T6 and was negatively associated with chronic illness. Chronic illness was also associated with lower levels of light physical activity at T8; moderate physical activity at T6, T7, and T8; vigorous physical activity at T6; and a lower wear time at T6. Higher levels of health engagement strategies were positively associated with higher levels of light physical activity at T6, moderate physical activity at T6, vigorous physical activity at T7, and health-related self-protection. Light physical activity at T6 was significantly positively associated with corresponding levels at T7 and T8 and with moderate physical activity from T6 to T8. Moderate physical activity at T6 was further positively associated with corresponding levels at T7 and T8, and with vigorous physical activity from T6 to T8. Finally, vigorous physical activity at T6 was positively associated with corresponding levels at T7 and T8.
Zero-Order Correlations of Main Study Variables.
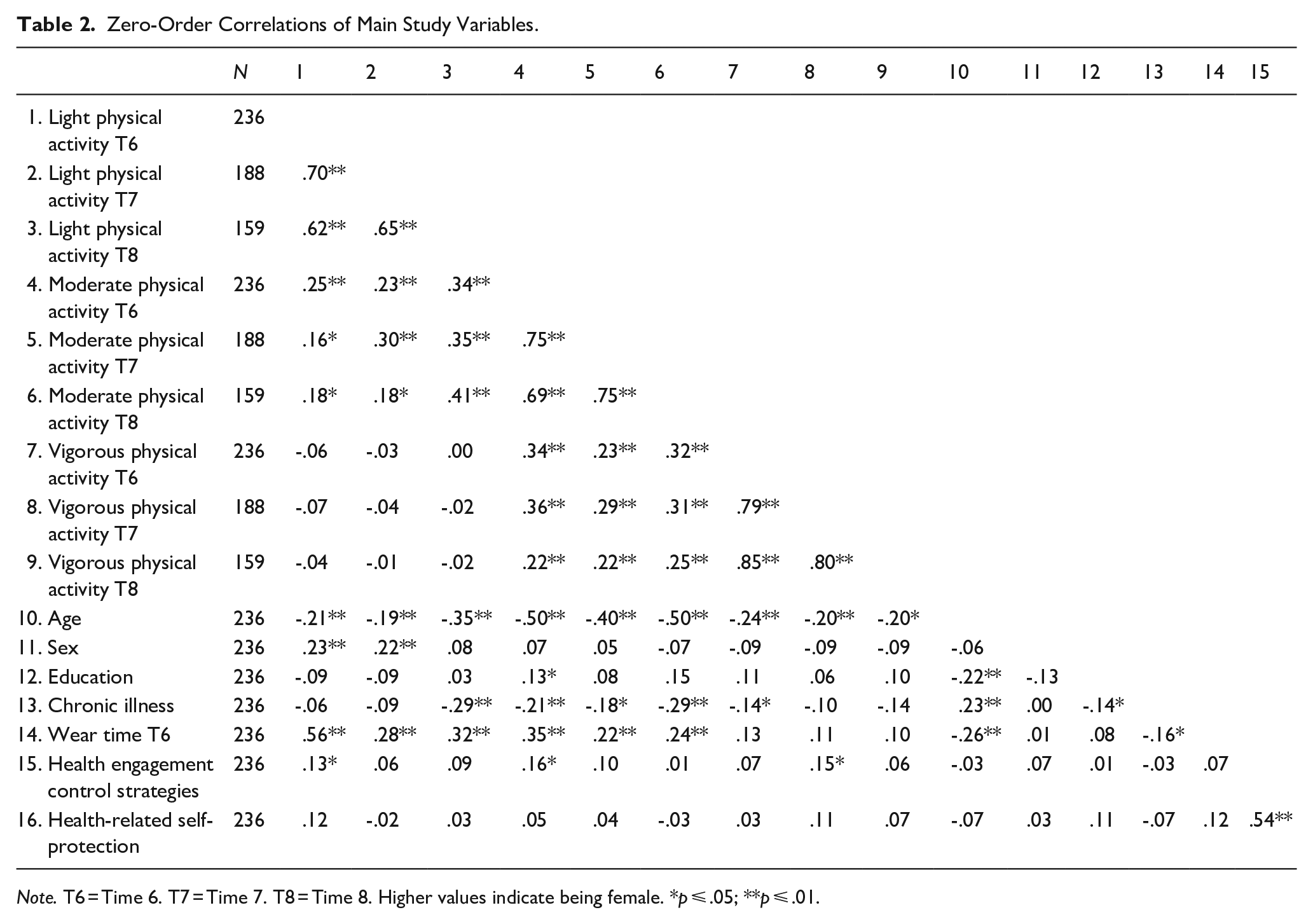
Note. T6 = Time 6. T7 = Time 7. T8 = Time 8. Higher values indicate being female. *p ⩽ .05; **p ⩽ .01.
Trajectories of Physical Activity
The results of the Level 1 models are reported in Tables 3 to 5. The intercepts for the models were significant, suggesting that average levels of light, moderate, and vigorous physical activity were different from zero. On average, participants engaged in a daily level of 324.14 min of light physical activity, 58.72 min of moderate physical activity, and 1.98 min of vigorous physical activity.
Results From Hierarchical Linear Models Predicting Average Levels and 4-Year Changes in Light Physical Activity as a Function of Health-Specific Control Strategies and Covariates (N = 236).
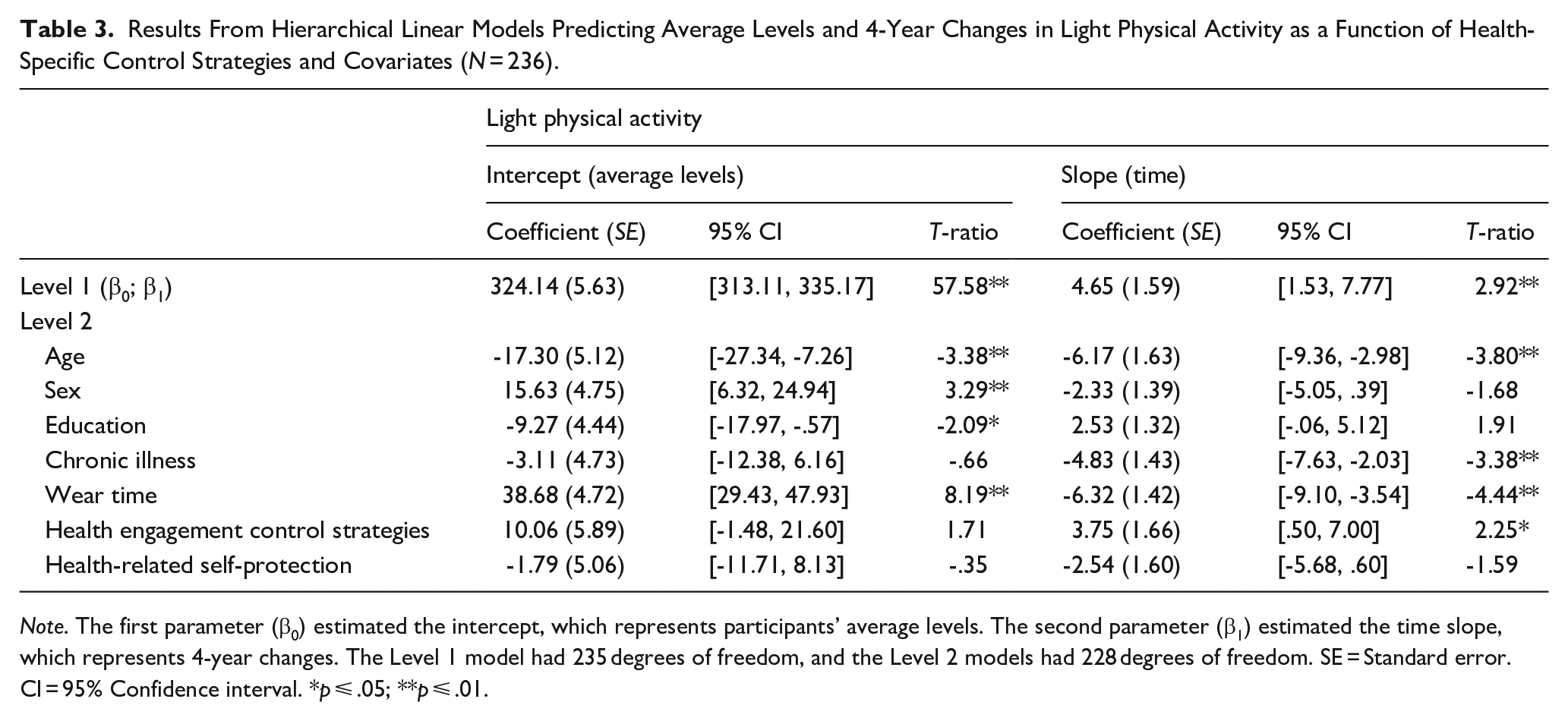
Note. The first parameter (β0) estimated the intercept, which represents participants’ average levels. The second parameter (β1) estimated the time slope, which represents 4-year changes. The Level 1 model had 235 degrees of freedom, and the Level 2 models had 228 degrees of freedom. SE = Standard error. CI = 95% Confidence interval. *p ⩽ .05; **p ⩽ .01.
Results From Hierarchical Linear Models Predicting Average Levels and 4-Year Changes in Moderate Physical Activity as a Function of Health-Specific Control Strategies and Covariates (N = 236).
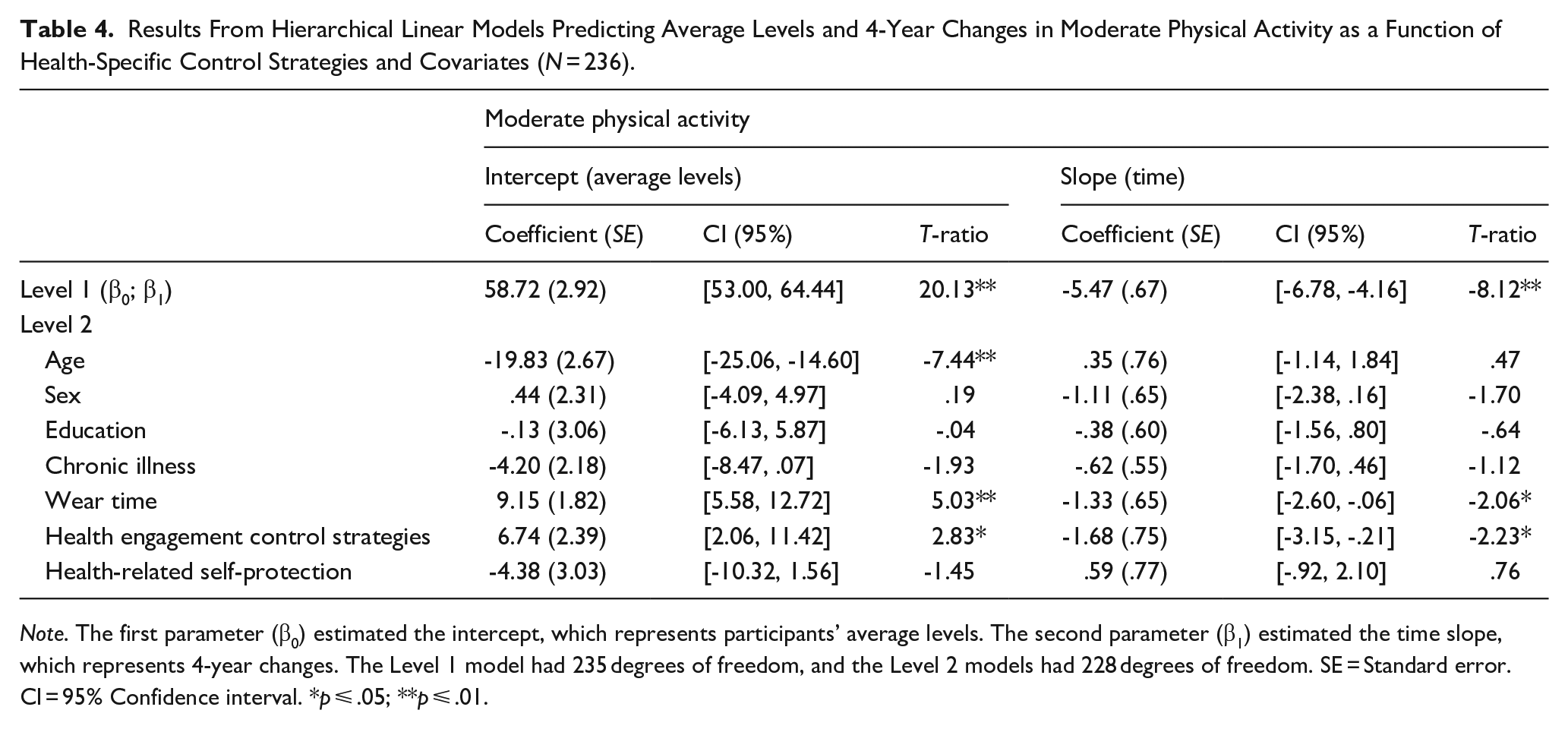
Note. The first parameter (β0) estimated the intercept, which represents participants’ average levels. The second parameter (β1) estimated the time slope, which represents 4-year changes. The Level 1 model had 235 degrees of freedom, and the Level 2 models had 228 degrees of freedom. SE = Standard error. CI = 95% Confidence interval. *p ⩽ .05; **p ⩽ .01.
Results From Hierarchical Linear Models Predicting Average Levels and 4-Year Changes in Vigorous Physical Activity as a Function of Health-Specific Control Strategies and Covariates (N = 236).
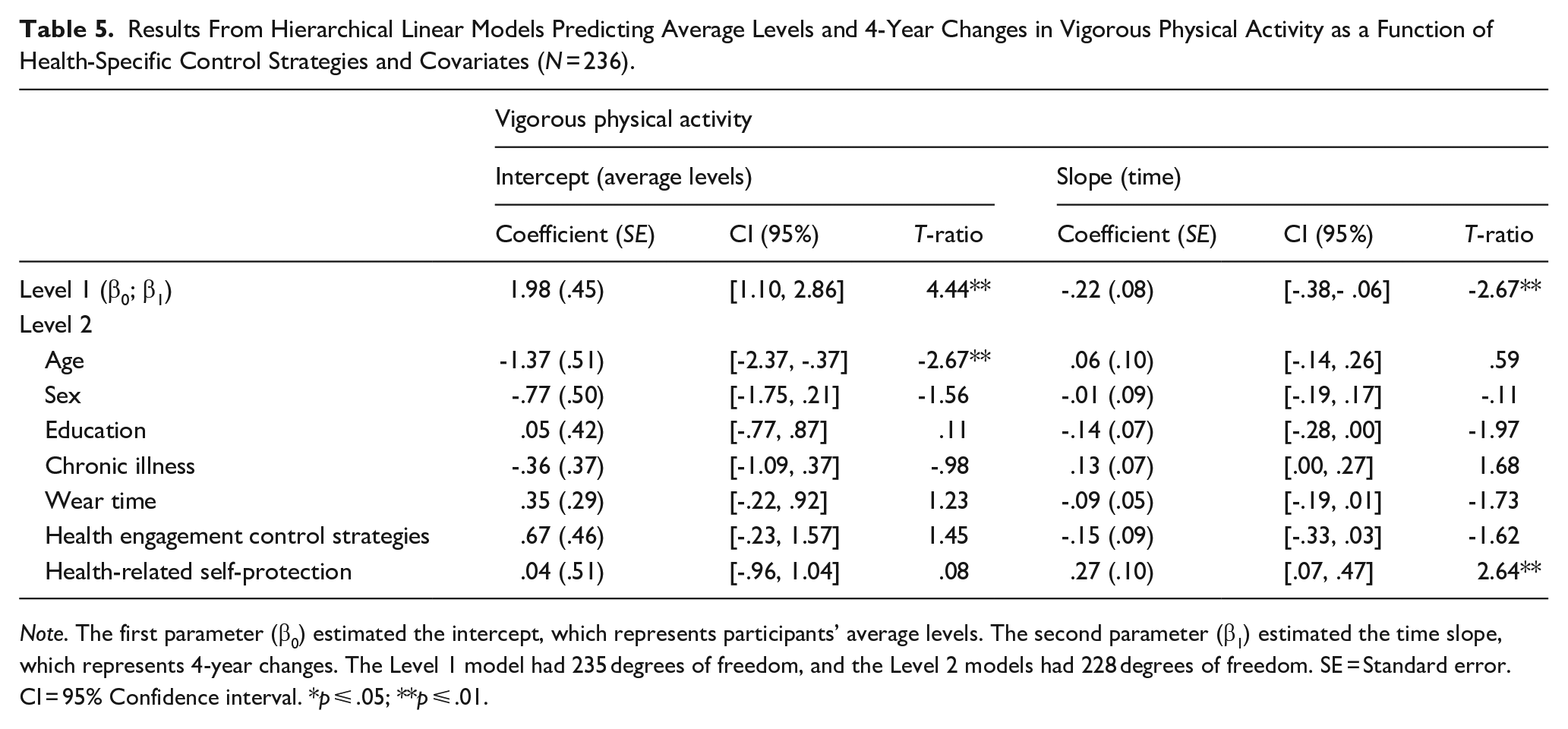
Note. The first parameter (β0) estimated the intercept, which represents participants’ average levels. The second parameter (β1) estimated the time slope, which represents 4-year changes. The Level 1 model had 235 degrees of freedom, and the Level 2 models had 228 degrees of freedom. SE = Standard error. CI = 95% Confidence interval. *p ⩽ .05; **p ⩽ .01.
The Level 1 models also revealed that the time slopes for all three physical activity intensities were significant. We plotted these trajectories in Figure 1 for light (upper panel) moderate (middle panel), and vigorous (lower panel) physical activity. Figure 1 shows that while light physical activity significantly increased over time (4.65 min per year), moderate (-5.47 min per year) and vigorous (-.22 min per year) physical activity decreased. The Level 1 model further showed considerable variation in participants’ light (χ2 = 1,391.44, p < .001), moderate (χ2 = 1,802.80, p < .001), and vigorous physical activity (χ2 = 2,200.22, p < .001) intercept values, and time slopes (Light: χ2 = 253.53, p = .01; Moderate: χ2 = 229.12, p = .08; Vigorous: χ2 = 181.84, p > .50), suggesting potential individual differences in these parameters.
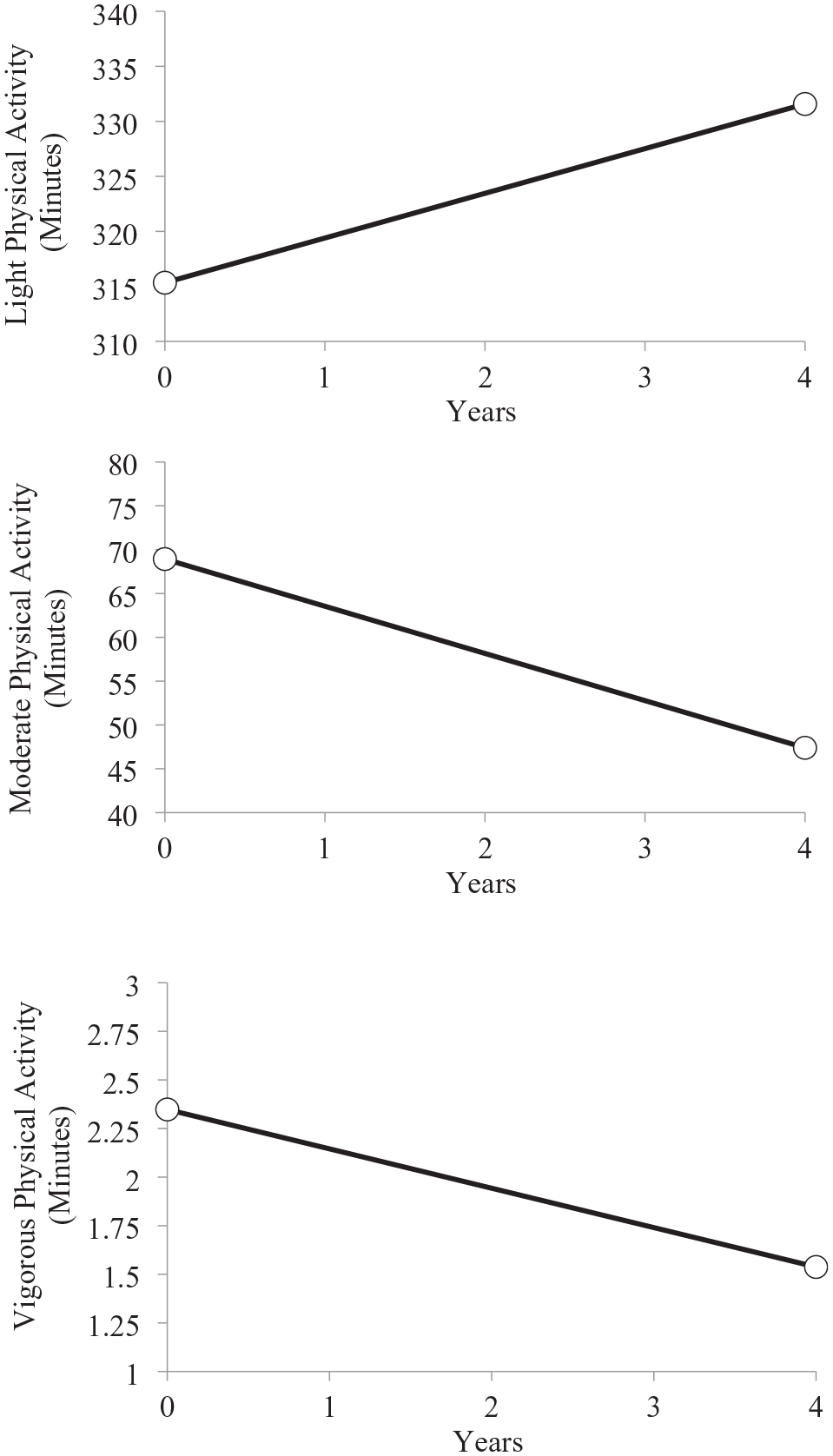
Trajectories of Light, Moderate, and Vigorous Physical Activity Over 4 Years of Study (N = 236).
The Level 2 models for predicting participants light, moderate, and vigorous physical activity by the covariates and health-specific control strategies are presented in Tables 3 to 5. For light physical activity, the results suggest that age, sex, education level, and wear time significantly predicted the intercept (i.e., average levels). Participants who identified as female had higher average levels of light physical activity than their male counterparts. In addition, older and higher educated participants engaged in lower average levels of light physical activity than younger and less educated participants. Wear time was positively associated with levels of light physical activity.
Regarding the time slope, age, chronic illness, and wear time predicted longitudinal changes in light physical activity (see Table 3). To examine these cross-level interactions, simple slope analyses were conducted separately for participants with high (averaged upper quartiles) and low (averaged lower quartiles) values for the Level 2 variables. The results showed that light physical activity significantly increased over time at lower ages (coefficient = 12.57, SE = 1.04, T-ratio = 12.07, p < .01), but declined among participants who were comparatively older (coefficient = -4.04, SE = 1.67, T-ratio = -2.41, p = .02). In addition, light physical activity increased among participants with low levels of chronic illness (coefficient = 8.88, SE = 1.41, T-ratio = 6.30, p < .01), but declined among their counterparts with higher levels of chronic illness (coefficient = -2.68, SE = 1.31, T-ratio = -2.04, p = .04). Participants who wore the accelerometer less increased their light physical activity over time (coefficient = 13.08, SE = 2.07, T-ratio = 6.32, p < .01), while participants who wore it longer decreased their levels of light physical activity (coefficient = -3.27, SE = 1.38, T-ratio = -2.36, p = .02).
Concerning moderate physical activity, the Level 2 models showed that age and wear time predicted participants’ intercept (see Table 4). A younger age and a higher wear time were positively associated with higher levels of moderate physical activity. In addition, the analysis showed that wear time predicted the time slope of moderate physical activity. Participants with a higher wear time exerted steeper reductions in moderate physical activity (coefficient = -6.93, SE = .64, T-ratio = 10.88, p < .01) than participants with a lower wear time (coefficient = -3.48, SE = .31, T-ratio = -11.08, p < .01).
For vigorous physical activity, only age predicted the intercept (see Table 5). Younger participants engaged in higher average levels of vigorous physical activity across study waves than their older counterparts. None of the covariates predicted the time slope of vigorous physical activity.
Health-Specific Control Strategies
The intercept effects of health engagement and self-protection were not significant for light physical activity (see Table 3). However, health engagement, but not health-related self-protection, significantly predicted the time slope of light physical activity. We plotted the significant health engagement effect in Figure 2, by illustrating the trajectory of light physical activity separately for participants who scored low versus high on the health engagement scale (lower and upper averaged quartiles). As depicted in the upper panel, levels of light physical activity did not differ much at the beginning of the study period. Toward the end of the study period, however, participants who reported high, as compared with low, levels of health engagement strategies engaged in substantially higher levels of light physical activity. Simple slope analyses supported this by showing that participants who used high levels of health engagement strategies increased their levels of light physical activity over time (coefficient = 8.73, SE = 1.04, T-ratio = 8.44, p < .01), while those with low levels of health engagement did not (coefficient = -1.07, SE = 1.64, T-ratio = -.65, p = .52).
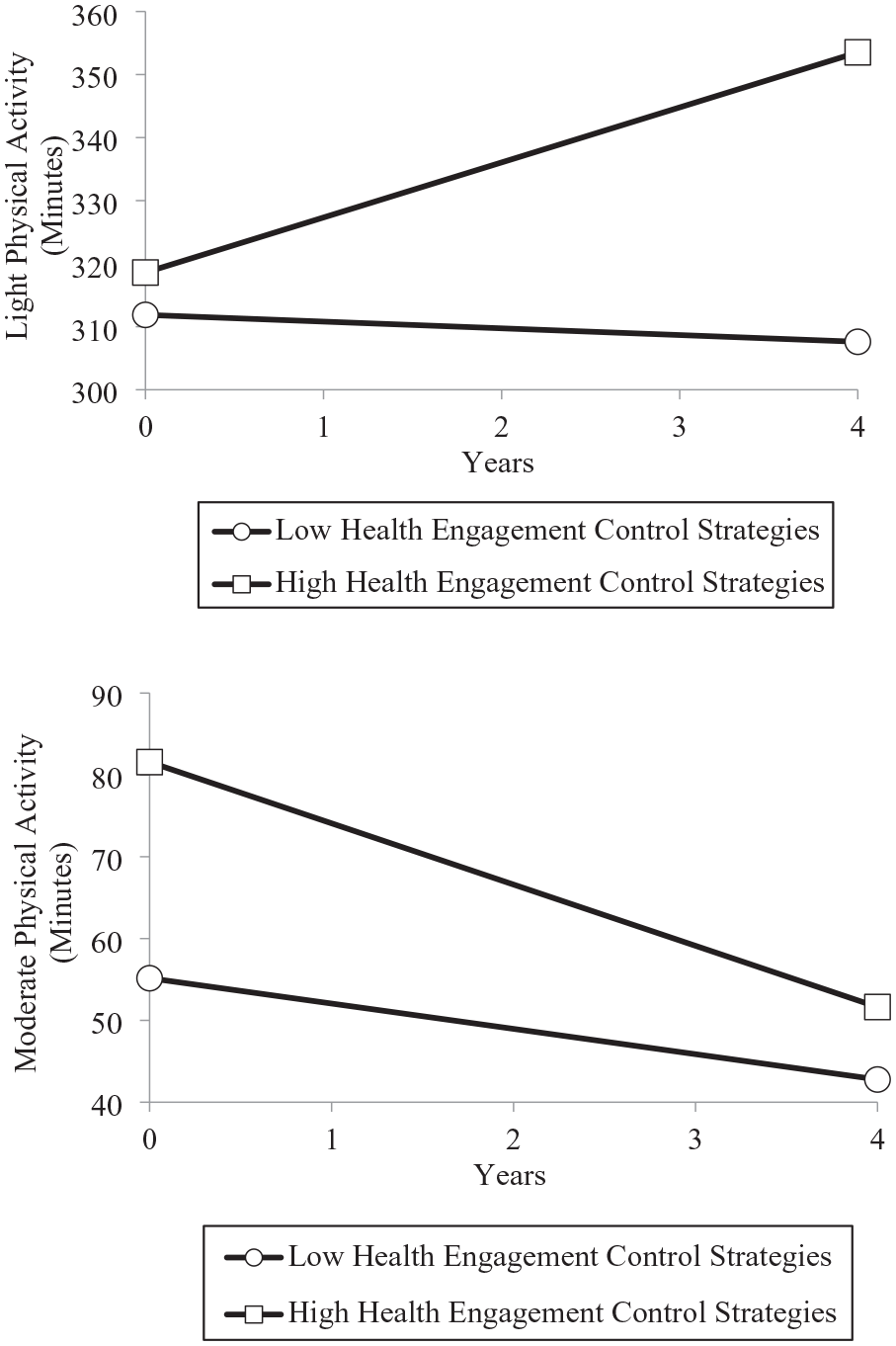
Trajectories of Light (Upper Panel) and Moderate (Lower Panel) Physical Activity Over 4 Years Among Participants With Low and High Levels of Health Engagement Control Strategies (N = 236).
With respect to moderate physical activity, the Level 2 models showed that health engagement strategies, but not health-related self-protection predicted participants’ intercept (see Table 4). Participants who reported high levels of health engagement had higher levels of moderate physical activity than participants who reported low levels. In addition, health engagement strategies, but not health-related self-protection, predicted the time slope of moderate physical activity. The significant health engagement effect is illustrated in the lower panel of Figure 2 by plotting the trajectory of moderate physical activity separately for participants who scored low versus high on the health engagement scale (lower and upper averaged quartiles). Figure 2 shows that health engagement strategies were associated with substantially higher levels of moderate physical activity across the entire study period. This effect, however, was stronger at the beginning of the study period, and became weaker toward the end. Simple slope analyses supported this by showing that levels of moderate physical activity declined over time at a higher rate among participants who reported high (coefficient = -7.48, SE = .28, T-ratio = 26.34, p < .01), as compared with low (coefficient = -3.09, SE = .71, T-ratio = 4.37, p < .01), levels of health engagement strategies.
Finally, the Level 2 models showed that neither health engagement strategies nor health-related self-protection predicted the intercept (see Table 5) of vigorous physical activity. The results did indicate that health-related self-protection, but not health engagement was significantly associated with the time slope of vigorous physical activity. We illustrated the latter effect in Figure 3 by plotting the trajectory of vigorous physical activity separately for participants who scored low versus high on health-related self-protection (lower and upper averaged quartiles). The obtained pattern and conducted simple slope effects showed that participants who did not engage in health-related self-protection exerted a significant decline in vigorous physical activity over time (coefficient = -.57, SE = .20, T-ratio = 2.89, p < .01). Their counterparts who used self-protective strategies to a larger extent did not show declines in vigorous physical activity over time (coefficient = .14, SE = .19, T-ratio = .72, p = .47).
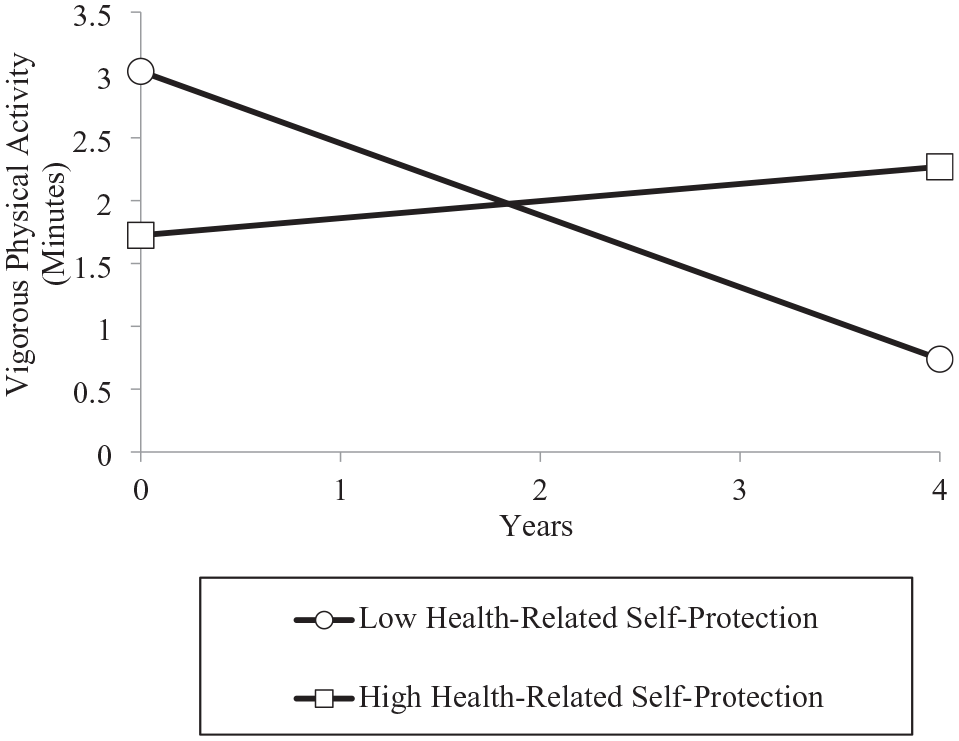
Trajectories of Vigorous Physical Activity Over 4 Years Among Participants With Low and High Levels of Health-Related Self-Protection (N = 236).
Discussion
Trajectories of Physical Activity
The results of this study showed that while older adults exerted declines in vigorous and moderate physical activity over time, they increased their light physical activity (for compensation in physical activity, see Rowland, 1998). The observed age-related declines in more strenuous physical activity levels likely reflects the many physical and psychological changes that occur with aging. In addition, the obtained increases in light physical activity support the Lines-of-Defense model, which postulates that older adults can manage progressive health threats by replacing health behaviors and goals that have become too difficult to pursue with those that are still feasible (Heckhausen et al., 2013, 2019, 2024).
The analyses also identified factors that qualified the obtained trajectories of physical activity. To this end, chronological age and chronic illness moderated changes in light physical activity over time. While people in early old age showed a significant increase in light physical activity, a decline was observed in advanced old age. Similarly, only among participants with low levels of chronic illness, light physical activity increased over time, while the reverse effect was observed among those with high levels (for chronic illness and physical activity, see Ashe et al., 2009). These findings may imply that there are limiting circumstances that prevent older adults from engaging in even less strenuous physical activity (for vulnerable populations in the aging process, see Charles, 2010; Gerstorf et al., 2010).
Although a lower wear time of the accelerometer at baseline predicted increases in light physical activity over time, a higher wear time showed a reversed effect. We did not expect the latter finding and suspect that it could relate to a statistical artifact, such as regression to the mean, given that wear time was substantially correlated with initial levels of light physical activity (see Table 2). Alternatively, it might be helpful to better understand the variables associated with individual differences in wear time. For example, some older adults could not wear the accelerometer when they were inactive, or a lower wear time might be associated with a temporary disease. If such people recover and become more active, a relatively lower wear time could predict increases in physical activity. Accelerometers provide important information on duration and intensity of physical activity but are unable to record the specific activities people engage in, which can also contribute to older adults’ health (i.e., strength, balance, and flexibility training; Arvidsson et al., 2019).
We further observed effects of age, sex, education, and wear time on average levels of physical activity across the study period. Chronological age was associated with lower levels in all intensities of physical activity, reflecting commonly observed age differences of 30 years (McAuley et al., 2006). In addition, consistent with previous research, participants with a higher education level showed higher average levels of moderate physical activity compared with their lower educated counterparts (Azagba & Sharaf, 2014). Finally, a longer wear time was associated with higher average levels of light and moderate physical activity, which supports our decision to control the analyses for this variable.
Health-Specific Control Strategies
The study’s findings suggest that the use of control strategies could facilitate the process of holding a line of defense and downwardly adjusting unfeasible health goals and behaviors. Importantly, the longitudinal increase in light physical activity was observed only among older adults who used high levels of health engagement. Moreover, it predicted generally higher levels of moderate physical activity. This effect was substantial and potentially clinically important, as high, compared with low, levels of health engagement predicted at study entry approximately 25 more minutes of daily moderate physical activity (see Figure 2). Note, however, that the effect of health engagement on moderate physical activity became significantly smaller over time, indicating that strategies such as persistence and effort can become less effective over time.
The latter pattern of findings suggests that a shift in older adults’ physical activity engagement could be supported by the use of health engagement strategies. Health engagement promoted increasing levels of light physical activity and slowed down a decline in moderate physical activity. Our results suggest that health engagement is conducive for holding a line of defense with respect to moderate physical activity, and for supporting light physical activity when moderate or vigorous physical activity often becomes unfeasible. These findings further support our prediction that the adaptive value of health engagement becomes paramount for the regulation of health goals that involve favorable opportunities for goal attainment, such as less strenuous physical activity (Wrosch & Schulz, 2008).
We observed different effects of health-related self-protection on changes in physical activity patterns. In particular, self-protection was only associated with the maintenance of vigorous physical activity. In terms of our theoretical rationale, this may imply that self-protective control strategies can provide resources needed for adaptive action, enabling older adults to hold a line of defense (i.e., vigorous physical activity; Heckhausen et al., 2019, 2024). For example, when older adults recognize that they cannot run anymore for as long as they used to, they may be at risk of abandoning this activity altogether. Here, self-protective strategies, such as positive reappraisals, may help participants decide to go for shorter runs instead of abandoning running. For the pursuit of less strenuous physical activity, opportunities should be generally more favorable and older adults may be able to successfully engage in less strenuous physical activity without using these strategies.
It is important to note that our hypotheses for self-protection were exploratory with two contradictory scenarios. In addition to the above hypothesis, we had also suggested that these strategies could foster acceptance and promote goal disengagement, thus predicting a reduction in those increasingly difficult/unfeasible activities (Heckhausen et al., 2019). Our data did not support this possibility. Self-protective strategies were not related to reductions in any type of physical activity. One plausible explanation is that levels of vigorous physical activity were already quite low in our sample and the process of abandoning vigorous physical activities may have happened earlier in our sample. Future research may conduct research with older adults who exert higher levels of vigorous physical activity to provide data on whether health-related self-protection can also support acceptance of age-related declines and disengagement from more strenuous physical activity.
Note that the relatively low levels of vigorous physical activity might raise the question of how important small increases in vigorous physical activity are in old age. We would argue that even small bouts of moderate and vigorous physical activity can affect health-relevant physiological regulation and mortality (Sabiston et al., 2018; Saint-Maurice et al., 2018). It would therefore be useful to include in future studies measures of psychological well-being, physiological functioning, and clinical health outcomes to assess the practical relevance of observed levels and changes in physical activity for older adults’ quality of life.
Overall, the findings from the present study carry substantial implications for theory and research in motivational and lifespan psychology. First, they contribute to motivational theories by suggesting that people can counteract progressive age-related challenges and keep pursuing health-related activities through an orchestrated use of control strategies. This process may involve using self-protective and health engagement strategies to keep pursuing important health behaviors for as long as possible. In addition, if it becomes impossible to further pursue a health-related activity, health engagement strategies can facilitate the pursuit of downwardly adjusted activities (as shown for light physical activity). These ideas are core postulates of the Lines-of-Defense model, which was developed to examine the management of progressive age-related declines (Heckhausen et al., 2013, 2019).
In addition, the findings suggest that health-specific goal engagement remains important in old age. While there has been demonstrated adaptive age-related shifts from goal engagement to self-protection and goal disengagement in other domains of life (e.g., childbearing or intimate relationship goals, Heckhausen et al., 2001; Wrosch et al., 2009), abandoning health-related activities altogether likely would have adverse consequences.
Finally, our findings suggest that there may be limits to holding a line of defense and adjusting health-related activities. To this end, the analyses showed that older adults with high levels of chronic illness and in advanced old age did not increase, but instead reduced their levels of light physical activity. In fact, advanced old age has been related to an increasing incidence of morbidity and mortality (Gerstorf et al., 2010), which may prevent older adults from maintaining even less strenuous physical activity, thereby posing limits to processes of adaptive developmental regulation (Charles, 2010). Theory and research are needed to illuminate how older adults in such precarious circumstances may be able to counteract threats to their health.
Limitations and Future Research
Although the present study has many strengths as it is theory-based, longitudinal in nature, and included an objective measurement of physical activity, it is not without limitations. First, while our sample was diverse in terms of age, sex, and education, it contained a relatively small sample from a limited geographic region in Canada. Future research should aim to replicate these findings with larger and more diverse samples (e.g., inclusion of ethnicity; Bryan et al., 2006).
Second, our study could not infer causality as it is based on longitudinal data and did not experimentally manipulate any of the variables. Since control strategies are modifiable psychological factors, future research may engage people in adaptive control strategies to optimize their physical activity behavior (e.g., writing interventions; Wrosch et al., 2009). Research along these lines may also be useful for practitioners who work with older adults and patients to enhance physical activity in vulnerable populations.
Third, beyond the included covariates, there may be other factors that could have influenced the results. For example, illness that manifests in functional disability or body mass index (BMI) could play a role. In addition, while wear time was relatively stable in our study, it could change over time. Supplemental analyses showed that almost all hypothesized effects remained significant if we controlled our findings for either functional disability, BMI, or time-varying wear time. Only the effect of health engagement on changes in moderate physical activity was reduced to a trend effect when controlling for BMI (p = .10). The latter reduction may be due to the possibility that people who use health engagement strategies frequently also have a lower BMI (for effects of physical activity on weight reduction, see Chin et al., 2016).
Fourth, we observed significant attrition in our longitudinal data, relating to mortality, illness, refusal, or inability to contact participants. Although our attrition analyses showed that only age, but none of the other baseline measures (including chronic illness) were associated with study attrition, attrition could have contributed in part to the patterns obtained in our study. For example, it would be possible that adaptive shifts in physical activity patterns were most pronounced in participants who remained healthy enough to continue the study or did not pass away. While we feel it is difficult to estimate physical activity scores of people who drop out of a study for health or mortality reasons, more recent research has explored models including death as a competing factor when studying older adults (Frison et al., 2019; Pichardo et al., 2022). Future research might incorporate these analytic strategies to optimize the generalizability of study conclusions.
Fifth, our study examined health-specific control strategies, but did not measure older adults’ physical activity goals nor the feasibility of older adults’ physical activity behaviors. We do not feel, however, that these limitations compromise our rationale or the interpretation of findings. Our analyses were based on previous work, suggesting that it becomes increasingly difficult for older adults to engage in physical activity (Hallion et al., 2019). In addition, health goals are thought to be pursued through the use of control strategies (Heckhausen et al., 2010, 2019). Nonetheless, future research should examine the feasibility of physical activity directly as well as specific physical activity goals and control strategies.
Sixth, although the Lines-of-Defense model makes predictions about the role of goal disengagement (Heckhausen et al., 2013), this process was not addressed in our study because the measurement tool did not include goal disengagement items (see also Rueggeberg et al., 2012). Future work may therefore formulate new items that also measure disengagement from health-related goals. Such items already exist for domain general and specific control striving in other domains and could be adapted for health research (e.g., Heckhausen et al., 2001). In addition, we note that the reliability of the self-protection scale (α = .66) was lower than the reliability of the health engagement scale (α = .85). This difference is likely related to the smaller number of items in the self-protection scale, given that reliability is linearly related to the number of items.
Finally, future work is needed to expand our approach to examining the impact of control strategies on the management of progressive health threats in older adulthood. For example, it would be interesting to examine changes and fluctuations in control strategies over time and link those trajectories to important health behaviors and bio-medical outcomes. In addition, while our analyses examined sample levels (and subsample levels) of physical activity over time, studies could link different intensities of physical activity over time within older adults. Clearly, more research on how older adults can manage progressive health threats is needed and likely to contribute to our understanding of motivational pathways to health aging.
Conclusion
This study examined motivational predictors of objective physical activity in a longitudinal sample of older adults. Results showed longitudinal increases in engagement in light physical activity and reductions in moderate and vigorous physical activity. In addition, health-specific control strategies were identified as factors that support engagement in and maintenance of older adults’ physical activity. These findings support the Lines-of-Defense model. As people grow older and confront increasing levels of age-related constraints, they do not have to abandon important health-related activities altogether. Instead, they might adjust their health behaviors to the levels of feasibility using adaptive control strategies.
Footnotes
Authors’ Note
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study has been supported by grants from Canadian Institutes of Health Research and Social Sciences and Humanities Research Council of Canada to Carsten Wrosch, the Canada Research Chair program to Catherine Sabiston, and fellowships from Fonds de recherche du Québec Société et Culture to Jasmine Kotsiopoulos and Irene Giannis.