
Abstract
Developing urban environments that promote healthy, active living for older adults is at the forefront of global planning policy debates, resulting in concepts and design guidelines to support population ageing. However, current urban planning in India is overlooking the design of age-friendly cities. The share of older adults in India is estimated to increase from 8 per cent in 2015 to 20 per cent in 2050. This demographic shift towards a higher proportion of older adults and the associated health and social care expenditures make healthy ageing a public health priority. Existing studies in gerontology have focused on improving housing environments, but we are now understanding the significance of neighbourhood environments for active ageing. This study contributes to the knowledge on factors shaping active ageing in urban India. We present findings from 55 semi-structured interviews conducted with older adults (age > 60 years) in the metropolitan cities of New Delhi and Chennai in India. The findings explore three themes that emerged from this research: (a) neighbourhood design for active ageing, (b) social participation in community spaces and (c) navigating urban transport and mobility. Across these themes, this study highlights that access to neighbourhood amenities such as transportation, parks and green spaces, and opportunities for leisure and social interaction play a key role in determining older adults’ health and quality of life. In drawing on older adults’ lived experiences in their communities, this study informs policy efforts to improve neighbourhood supports for active ageing in urban India.
The pace of population ageing around the world is rapidly increasing. By 2050, the population aged 60 years and older is expected to be total 2 billion, which is one-fifth of the world’s population (United Nations, 2017). A majority of this increase is set to occur in the Global South, with 80 per cent of all older adults living in low- and middle-income countries (low- and middle-income countries; World Health Organization, 2019). In India, reports indicate that the share of older adults is estimated to increase from 8 per cent in 2015 to 20 per cent in 2050 (United Nations Population Fund, 2017).This major demographic shift towards a higher proportion of older adults, and the health and social care costs associated with ageing, make ageing research a public health priority in low- and middle-income countries.
Health and social care costs usually increase as people age due to a gradual decrease in physical and mental capacity, a growing risk of disease, frailty, physical injuries and cognitive health problems (Ofori-Asenso et al., 2019). Moreover, older adults are more likely to experience several health conditions at the same time with continual challenges in relation to place as they age (Gheysen et al., 2018). Some of the common and costly health challenges faced by older adults include chronic conditions such as obesity, diabetes, heart disease, stroke and some cancers. Physical activity (PA) in older adults is linked to numerous health benefits and is a protective factor for chronic health conditions such as cardiovascular disease, diabetes, stroke and some types of cancers (Langhammer et al., 2018). Regular PA is associated with lower cholesterol, blood pressure, BMI, improvements in muscle mass, bone density, psychological function, cognition and delay in the onset of dementia (Daskalopoulou et al., 2017). According to the World Health Organization, older adults should accumulate at least 150 minutes of moderate-intensity aerobic PA throughout the week (World Health Organization, 2010). Yet national statistics in India indicate that the majority of older adults are not meeting these guidelines (Chatterji et al., 2008; McCarthy et al., 2018). This has resulted in a growing interest in understanding linkages between health and place, and how different dimensions of the environment interact with lifestyle factors to influence a variety of health outcomes across the life course (UK Government Office for Science, 2016; United Nations, 2017; World Health Organization, 2019).
Limited mobility and age-related frailty make older adults more dependent on neighbhourhood amenities and services, and on local sources of social support (Ofori-Asenso et al., 2019). The neighbourhood environment can either promote or hinder walking, mobility and PA, and also affect social interaction, participation and independence in older adults (Cerin et al., 2017). Several studies have investigated the association between built environment characteristics and PA in older adults and found safe, walkable, green and aesthetically pleasing neighbourhoods with access to different destinations and amenities to be important (Barnett et al., 2017; Marquet & Miralles-Guasch, 2015; Pettersson & Schmöcker, 2010). For example, neighbourhood features related to safety (e.g., street lighting), comfort and ease of movement (e.g., pavement conditions, green space) are shown to be the strongest correlates of older adults’ mobility and PA (Musselwhite, 2017). Activity-friendly environments that support walking and other types of PA also provide opportunities for staying socially active and maintaining interpersonal relationships, thus promoting higher levels of social interaction and engagement in older adults (Smith et al., 2017).
Developing urban environments that promote healthy, active living for older adults is at the forefront of global planning policy debates, resulting in concepts and design guidelines to support population ageing. In recent years, there has been a proliferation of initiatives aimed at the development of age-friendly cities and communities. Various agendas on ‘ageing-in-place’, ‘healthy ageing’ and ‘active ageing’ have been designed to support and enable older adults to age well in urban environments (United Nations Economic Commission for Europe, 2017; World Health Organization, 2002, 2012). Whilst this literature is highly important, there is a paucity of research exploring how older adults construct and negotiate access in their built and social environments at a local level in low- and middle-income countries like India that are confronted with pressures of rapid urbanisation (Buffel & Phillipson, 2016).
Rapidly urbanising environments can challenge social integration and increase the risk of social exclusion among older adults. In India, urban spaces are perceived as unsafe and inaccessible for older adults with mobility restrictions (Chao, 2017; Prattley et al., 2020; Van Hoof et al., 2018). Cities are, for the most part, designed and structured with a younger demographic in mind. Among older adults, poorly maintained streets, lack of traffic management and lack of physical segregation between pedestrians, cyclists and motorised vehicles contribute to increased risk and fear of falling (Rosenberg et al., 2012) . Stressors from the built environment such as loud horns, speeding vehicles, lack of pedestrian facilities and physical disorder can also add to older adults’ anxiety levels (Mooney et al., 2017). This results in a compounding impact on social isolation in the most vulnerable old (Gardiner et al., 2018).
Existing studies in gerontology have focused on improving housing environments, but we are now understanding the significance of neighbourhood environments for active ageing (United Nations Population Fund, 2017).Currently, urban planning in India is overlooking the importance of designing age-friendly cities. This study contributes to the existing knowledge on factors shaping active ageing in neighbouhood environments of urban India.
Methods
Study Setting and Sampling
A purposive sample of older adults (N = 55, female = 51%) was recruited from the metropolitan areas of New Delhi and Chennai, India. Purposive sampling is known to be effective in exploring anthropological situations and is recommended by researchers who have conducted similar studies of this nature in low- and middle-income countries contexts (Oyeyemi et al., 2013). This type of sampling was appropriate for this study as it enabled the identification and selection of individuals that were especially knowledgeable about or experienced with the phenomenon of interest (Palinkas et al., 2015).In addition to knowledge and experience, purposive sampling reinforced the selection of information-rich cases intended to achieve depth of understanding on the lived experiences of older adults (Ames et al., 2019).In order to ensure selection of a diverse sample, recruitment was conducted in neighbourhoods differing by levels of socio-economic status in both cities. Neighbourhoods were divided into 10 deciles by socio-economic status. Neighbourhoods in deciles 3, 4 (low-income) and 7, 8 (middle- to high income) were selected for participant recruitment. Neighbourhoods in lowest and highest income deciles (1, 10) were excluded to avoid outliers and deciles 5 and 6 were excluded to create separation between the categories.
Multiple recruitment pathways were undertaken to reach participants, including canvassing in the local community, recruitment during social activities hosted by apartment blocks and housing areas, utilising recommendations provided by community gatekeepers, resident welfare associations, neighbourhood watch groups, resident associations and snowball sampling from an initial set of participants. Participants were contacted either in person or via telephone and asked about their interest and eligibility to participate. These residents, through their social networks, recommended older adults who were interested in participating in the study as part of the purposive sampling approach which was applied to reach a larger sample. Eligibility criteria for participation included: (a) current residents of Chennai or New Delhi, (b) residents of the city for at least six months, (c) > 60 years of age, (d) being able and willing to answer questions in English, Hindi or Tamil, which are the official languages in the study regions and (e) no visible signs of inappropriate behaviour (e.g., drunkenness and drug use). All participants that were contacted agreed to being interviewed and provided written consent.
Data Collection
Between March and August 2019, consenting participants were interviewed using a 25-item semi-structured questionnaire that was specifically developed for this study (Chennai n = 29, New Delhi n = 26).Written information sheets and interview questions were provided to all participants two days prior to the scheduled interview. Participants were given the choice of interview location to ensure their comfort and convenience. Most interviews were conducted in participants’ homes. The duration of the interview averaged between 45 and 60 minutes (mean = 54 minutes) and all interviews were digitally recorded. A conversational style was adopted during the interviews with the questionnaire guiding the conversation. The questionnaire included open-ended questions that allowed participants to speak freely about what they felt was relevant and important in terms of perceptions of ageing, age-friendly communities, their daily routine and outings, home and family setting, neighbourhood environment, work or leisure activities, modes of transportation and daily trips, social interactions and support. Ethical approval was obtained from the Research Ethics Committee, Queen’s University Belfast.
This qualitative study employed a grounded theory approach to estimate the sample size (Charmaz & Henwood, 2017). Theoretical saturation of data was used as a parameter to determine the number of participants required for a detailed analysis. There are no fixed sample sizes or standardised tests to estimate the amount of data needed for achieving saturation (Nelson, 2017). In this study, theoretical saturation was achieved where no new information, concepts or themes were emerging from the data.
Data Analysis
Interviews in Hindi and Tamil were translated by a knowledgeable bilingual person familiar with cultural terms and concepts commonly used by people residing in Chennai and New Delhi. To ensure consistency and rigour, translated interviews were reviewed by two bilingual people who were not familiar with the project. Interviews were transcribed and analysed using NVivo 12 (QSR International Pty Ltd, 2018). The interview transcripts were evaluated by means of inductive and thematic analysis, wherein data was classified according to key themes and emergent categories by identifying, analysing and interpreting patterns of meaning or themes within the qualitative data (Clarke et al., 2015). Once the transcriptions were complete, all three members of the research team read them for consistency. A consistent coding structure (team-based analytical framework) was developed by the research team for use within NVivo 12 (Ayres et al., 2003). One team member present at the interview and one not present then coded each transcript using the developed parent and child nodes for the coding structure. This coding structure was discussed with the wider research team to refine and agree codes. Any disagreement was resolved by discussion with an international advisory group from the International Physical Activity and Environment Network (IPEN;
Results
Summary Table of Themes and Sample Quotes (N = 55) Highlighting Neighbourhood Supports for Active Ageing in Urban India
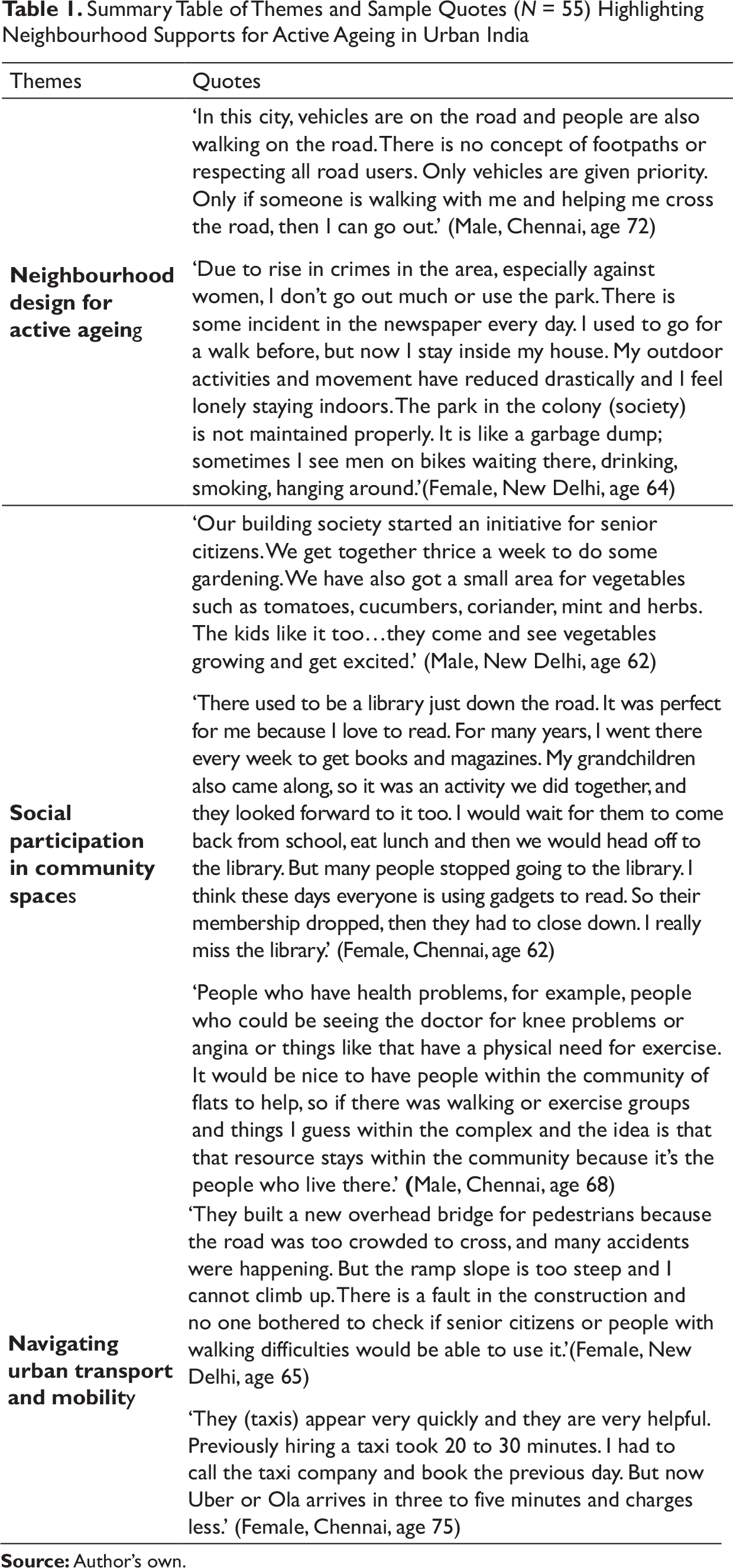
1. Neighbourhood design for active ageing: Findings highlighted that access routes between home and neighbourhood public spaces were not designed and maintained effectively to meet the needs of older adults with mobility difficulties. Participants discussed the rapid rates of urbanisation, increased traffic and congestion on roads, and critiqued their civic authorities for scant attention to planning and designing for ageing residents with no accommodation of age-related special needs in urban policies.
Many older pedestrians experienced difficulty in safely navigating complex traffic conditions. Lack of pedestrian infrastructure (e.g., safe footpaths and crossings) and age-friendly facilities (e.g., rest stops, benches and toilets) in public space made outdoor environments inaccessible to older adults. Selecting a safe gap in which to cross in front of oncoming traffic was a major problem for older adults. Specifically, older adults spoke about feeling vulnerable to increasing levels of motorised traffic and lack of priority given to pedestrian road users in local planning policy. As a result, some older adults did not leave their home alone or were dependent on others to move around the community, contributing to a sense of vulnerability and isolation:
I live in T. Nagar and it has become very congested. I moved here almost 60 years ago, and it used to be a quiet neighbourhood, very charming, with lots of trees, parks and open spaces. Now, new buildings have come everywhere up and the area is fully developed. There is no space to walk on footpaths and I am not able to cross the roads because of heavy traffic, so I don’t go out anywhere. Sometimes, my son will take me out in the car if I need to go anywhere, but otherwise I don’t go out on my own. (Female, Chennai, age 75) There’s no area big enough just to go and sit down for fresh air. I have seen some older people walking to the market and they walk so far; they have to stop for few minutes on the road because there’s nowhere for them to sit. I wish there were spaces here for us to wait and rest, even benches in a shady area. Clean toilets are another necessity. (Male, New Delhi, age 65)
Age-related fragility, illnesses and functional limitations, and traffic safety hazards were the key risk factors of senior road users. Participants recognised the detrimental impact of poor neighbourhood infrastructure on their PA levels. Inadequate maintenance of footpaths, encroachment by vehicles and poor enforcement by civic authorities were some of the physical barriers identified. Walkability was a key concern for older adults, compromising access to key services and amenities. Risk of falling created a sense of anxiety amongst older people, resulting in feelings of insecurity when moving around public space:
The footpaths are badly planned it is impossible for me to walk there. It is too high to step on the footpath and there are so many holes and cracked tiles. I tripped and fell once when I was going for a yoga class, so now I am scared to go out on my own. The civic officials and other authorities simply ignore it. There are also many encroachments, so we are forced to walk on roads.(Female, New Delhi, age 68) Walking on the streets is not easy now. I am old and my knees are weak and the pavements are not smooth, all up and down and uneven surfaces. Everyday something or the other will be dug up, some repair work will be happening on the street and they will pile all the rubbish on the pavement. They don’t give any consideration to the older people who are struggling to walk and make it very difficult for us to walk. (Male, Chennai, age 75)
Participants emphasised the lack of well-maintained, barrier-free footpaths and safe crossings on busy roads as inhibiting factors for engaging in daily activities such as running errands, visiting friends and accessing neighbourhood amenities (e.g., walking to a shop or park). This narrative was acknowledged in several interviews by several participants. For those with mobility difficulties, visiting public spaces was challenging due to additional risks from traffic congestion and overcrowding that they were not equipped to handle. In response to neighbourhood-level constraints to everyday PA, older adults conveyed a sense of frustration when ability to undertake activities of daily living such as shopping were compromised:
One lane on the side of the road is occupied by cars and motorbikes parked illegally, so where do I walk? I am forced to risk my life and end up walking in almost middle of the road. Sometimes I want to go to the neighbourhood shop and buy milk and vegetables. It’s only a 7-minute walk from my house, but every time I step out of the house, I have a harrowing experience and come back feeling very frustrated. (Male, New Delhi, age 75) I am diabetic, have been for almost 35 years. The doctor has told me to exercise and go for a walk every day. There is a park near my house that I like to go and spend time walking. But I can only go in the early morning when the rush has not started. Otherwise it is impossible for me to walk to the park because there are motorcycles parked on footpaths and I am forced to work on the road which is not safe. (Male, Chennai, age 78)
Signs of physical disorder (e.g., graffiti and litter) in the neighbourhood also constrained older adults’ walking behaviours and PA. Participants spoke about fear of crime, threats to personal safety and feeling unsafe while walking in certain areas at night. Particularly, older women expressed feeling vulnerable to crime, anti-social behavior and overall low levels of perceived safety. Residents in areas with higher perceived crime levels tended to isolate themselves from neighbourhood facilities and opportunities because of personal safety and fear of criminal victimisation issues, contributing to social isolation and overall reduced quality of life:
I don’t like to walk on the stretch of the road that connects to the station. It is very deserted, especially after dark, and the area is not nice, lots of garbage, unpleasant things written on the walls. I took the metro to return home after shopping one evening and I was not comfortable walking in that area, so I stopped using the metro. (Female, Chennai, age 61) You hear about incidents in the news everyday… especially in Delhi. I do not go out alone at night and avoid using public transport. The walk to the stations is not properly lit. Majority of the time the streetlights are not working or someone has vandalised and broken them. There are people loitering around, sometimes drunk people hanging around the corners. It is very unsafe for women. (Female, New Delhi, age 62) Graffiti is one thing. When you go to the flyover and try to walk under there, it’s covered in graffiti and there are movie posters and broken glass pieces everywhere underneath in the area. You wouldn’t let your daughter, wife or anybody go down there like. It’s quite frightening at night-time. (Male, New Delhi, age 72)
Older adults reported high levels of air and noise pollution from road traffic. Residents highlighted a decline in use of neighbourhood parks and open spaces due to poor air quality and rise in respiratory illnesses. Participants reported little respite from toxic pollutants:
I have lived in this area for the past 40 years. The streets and parks used to be clean and green. I used to go for morning walks everyday with my neighbours and friends. We also met other people in the park and it became a nice morning activity for all of us. But now, the pollution is unbearable. I have developed breathing difficulty and stopped going. I am stuck indoors and it is very lonely. (Female, New Delhi, age 68) I stand for 15–20 minutes just to cross the road! It is so congested and noisy. Air and noise pollution all around. Fumes from vehicles, non-stop honking of horns. There is no peace of mind at all and traffic is the root cause. (Female, Chennai, age 60)
Older adults who perceived destinations to be walkable and pedestrian-friendly with easy access to places and services engaged in more neighbourhood-based PA. Residents spoke positively about pedestrian-oriented design changes in their urban environments. In Chennai, the redesign of a pedestrian plaza was a recurring topic in several interviews. Older adults mentioned the benefits of safe, convenient and accessible opportunities for walking and moving around. The integration of seating, protection from hazards and ‘places to rest’ afforded welcoming urban environments for older people:
Last week I walked to the new plaza in Pondy Bazaar with my neighbour. They have made the footpaths very wide, planted some trees, installed benches and it was so nice to walk there. I went to the shops, bought a few things and then we had coffee. Earlier, I used to avoid the place because it was so crowded. Even now, cars and bikes are still there, but at least there is some protected space for walkers. It is such a change to see a free space just for walkers with level paving, seating and rest places. I will go more often now and not worry about getting into an accident. (Female, Chennai, age 63) I grew up in this neighbourhood and have seen the unfortunate takeover of streets with cars everywhere. It has become impossible to walk to the shop at the corner. Some improvements are positive, like the pedestrian plaza in Pondy Bazaar. I hope they can prioritise pedestrians in other areas of the city.(Male, Chennai, age 65)
Participants also discussed the restorative quality of green spaces as places where they could rest and recover from negative aspects experienced in home, work and community life. The integration of green spaces, if designed effectively, had the potential to improve physical and mental well-being amongst older adults:
Because I can go to the park and probably knowing me, I’ll walk briskly and pumping the heart and things like that, and maybe it’ll be pleasing…mentally pleasing, so maybe my mental health or something like that maybe a little bit better. (Male, New Delhi, age 61) We only have one park in this area. I have been going there for walks for many years now. When I was working, I always went in the morning before work and it helped me to clear my head. Now that I am retired, it gives me a good space to relax and recharge. The streets are so noisy and at home I can hear so many cars and bikes honking. There are also constant sounds from TV, phones and music. It is impossible to find a quiet spot these days. But once I am in the park, I forget all that, breathe the fresh air and immediately feel refreshed. (Male, Chennai, age 73)
2. Social participation in community spaces: In examining the role of community factors on social participation, older adults revealed places and opportunities that made it possible for them to continue to stay in their homes and participate in the activities that they value, while socialising and contributing to their communities. Social groups and activities such as gardening clubs and shopping trips, and cultural events such as festivals and music concerts provided opportunities to interact and connect with others. In the absence of these, older adults reported feeling socially withdrawn, inactive or lonely. Participants reported looking forward to social interaction as opposed to solitary activities and many of these opportunities had an intergenetational element, bringing together younger and older adults:
At this time of the year, Marghazi (annual music festival) is so popular in the city. I enjoy listening to Carnatic music and there is a sabha (congregation hall) near my house. I look forward to the concerts every year. I go there with a group of friends; we have a nice meal and enjoy the concert. It is a highlight for this time of the year. (Female, Chennai, age 68) My daughter and I go shopping sometimes. I look forward to that as it gets me out of the house. Otherwise I am always indoors, and it gets boring and lonely. I only watch TV or sleep during my spare time. Nothing else to do. (Female, New Delhi, age 62)
Access to neighbourhood amenities such as community centres, libraries, recreational programmes and educational activities provided older adults with an opportunity to meet friends, socialise and spend time in settings outside their homes:
I went to the neighbourhood community centre a few weeks ago and even there you find pensioners; they were actually coming out at six or seven in the morning to play. There is also a park nearby. That space means a lot for them, to get out of the house, meet people of the same age, make friends…. It gives us something to look forward to. (Male, New Delhi, age 72)
Some participants indicated that opportunities for outdoor PA and recreation primarily catered to younger populations. Participants expressed a need for organised learning (e.g., arts and crafts classes) and group-based recreational PA (e.g., walking groups) to help them build social networks of support and solidarity. It was important for older adults to ‘keep busy’, through engagement in mentally stimulating activities:
Most activities are geared for younger people, there’s not really much for me now… like I played cricket and I played squash and all that when I was in my 20s and 30s, but when you come to 50 and over, there’s not much. (Male, New Delhi, age 66) There’d have to be a weekly class, or something like that for the people of my age. Just like an outing, a place to go to like a college, like painting and decorating class…some kind of educational activity that gets me out of the house to meet people. (Female, Chennai, age 60) I like to knit and sew. I keep myself busy with that. I have knit a lot of sweaters and scarves for my children. I want to learn how to do quilting, but the class is really far away and I cannot go. (Female, Chennai, age 60)
Older adults living in proximity to green space were more likely to report engagement in PA, improved social interactions and well-being. Parks and green spaces provided older adults with opportunities to socialise and keep them engaged in the company of others. This provided a sense of place identity and familiarity for older adult, forging a deeper sense of connection to the community and a feeling of ‘growing old together’:
I have been going for walks in my neighbourhood park for many years now. I have made friends there now with the regulars, we wave and greet each other, and sometimes spend a few minutes sitting on the bench and talking. It makes me feel welcome and like I belong here. Otherwise I am stuck alone indoors all day and it gets very lonely. This is my only outlet. (Male, Chennai, age 72) Both of us are in our 70s and we like to walk in our apartment complex every evening. It is nice to have a friend to walk outside with and get some fresh air. We sit and chat in the garden area, exchange recipes, share what our day has been like. It’s nice to have someone in the same age group and give each other company. It’s like growing old together and makes me feel less lonely.(Female, New Delhi, age 72)
3. Navigating urban transport and mobility: Participants discussed a number of factors including provision of public transport, frequency of services, accessibility and mobility challenges, overcrowding and signage. Barriers in service design of public transport included inappropriate timetabling and scheduling, long distances to the transit stop, poor last-mile connectivity and lack of age-friendly infrastructure. The provision of disabled-access infrastructure (e.g., ramps and elevators) at transit stations was highlighted as a positive feature for users with limited mobility. However, access routes to the transit stations were compromised with lack of inclusive outdoor access such as disabled-access footpaths, handrails and non-slip surfaces:
They have invested in disabled-access at all public transport stations. All metro stations have ramps from the streets so that wheelchair-bound persons can directly access the lifts. This has been very helpful to me to get out and go to the shops on my own, but I wish they had better connectivity from the stations to my home. The disabled-access infrastructure should continue in public spaces such as footpaths and road crossings. What is the point of only having it at the stations? (Male, New Delhi, age 75) I use the buses sometimes when I have to go to the bank or pay the electricity bill or when I need to go shopping. But I only go during non-peak hours. Otherwise it’s too crowded. I cannot even board the bus because the step is too high from the road. The bus stop is a bit far from my house and I find it difficult to walk as I have arthritis, so my activities have reduced a lot and I don’t go out that much. (Male, Chennai, age 77)
Barriers in transport service provision were lack of punctuality, poor reliability, unexpected or unadvertised changes in transport service, inappropriate routes, poor connections or having no service in the area and cost-prohibitive ticket pricing:
The buses are not reliable at all. Sometimes they are an hour late and sometimes they get cancelled and we just keep waiting. There is no shaded bus-stop to wait. To go a short distance, I have to change two buses, which is very difficult for me as I have a limp and cannot walk much. (Female, New Delhi, age 68) I used to drive till I was 65, but now I find the traffic too aggressive and driving has become stressful. I would like to use public transport, but the buses are too crowded and sometimes I cannot find a seat. The new Chennai metro rail is good, but also expensive for some people. I use it sometimes, but I still struggle with getting to and from the station. I have to call someone to pick me up and get me home, so I am dependent on them. The autos charge too much and sometimes refuse to go to the destination so then I am stuck. (Male, Chennai, age 70)
Participants expressed difficulty in understanding ticketing, handling payment and navigating the transit stations due to age-related vision and hearing impairment. This created a sense of confusion and disorientation when negotiating public transport which required seeking help and assistance from others:
With age, my eyesight and hearing has reduced, so I am not confident of using public transport. I cannot read the signs or hear the announcements. I cannot handle the payments. It’s too complicated, so I don’t use it on my own. (Male, Chennai, age 74) I find everywhere has become so crowded. Earlier, I used to like to go for shopping in Karol Bagh, but now there is too much traffic. I cannot go alone and I find it all very confusing...the different metro stops, stations and announcements. I don’t know where to get off and I need some help in understanding and using the metro rail service, so I usually go with my granddaughter. (Female, New Delhi, age 75)
Older adults expressed the need for transportation alternatives, but many were intimidated by smart phones and ride-hailing apps. Some participants acknowledged that ride-hailing services made life easier for them, while others said they found it challenging to build the confidence they need to actually use digital devices and tools. Some reported relying on younger family members such as grand children to help them make reservations using ride-hailing apps:
My grandson taught me how to use Uber and Ola apps on the phone. Since then, it has become easier for me to book a taxi if I need to go out on my own, for instance, yesterday I wanted to go to the temple in the evening. Earlier I had to wait for my son or daughter to be free to take me. (Female, Chennai, age 62) I struggle with the new phones, so I need help when I need to book a taxi. I ask my grandson to help me. It’s so easy now, with a click a taxi is here and I can go out on my own. When I have to come back, I call my grandson and he books the return for me. I am learning how to use the phone, but it takes some time. (Male, New Delhi, age 69)
Discussion
This study underscores the role of neighbourhood design for active ageing in two metropolitan cities in India. To date, the majority of this research has been predominantly conducted in high-income country settings (Oyeyemi et al., 2019). Our exploratory findings established that neighbourhood design, mobility and transportation choices, and community factors are essential for delivering age-friendly cities and communities. This study makes a unique contribution to the literature by providing evidence on the influence of neighbourhood environments on active ageing in India.
Neighbourhood design was imperative for older adults’ PA and recreation. Participants discussed the need for improved neighbourhood walkability, pedestrian safety, and access to parks and community spaces for PA and social interaction, while emphasising the need for maintenance of public spaces and enforcement of traffic laws. These are key concerns in low and- middle-income countries that are deficient in environmental and infrastructure needs. Findings from other low- and middle-income countries studies have also illustrated the importance of activity-supportive neighbourhoods for higher PA, active travel and lower sedentary time in older adults (Cleland et al., 2019; Oyeyemi et al., 2019). Importantly, neighbourhoods need to offer a seamless connection between different settings, such as indoor home environments and outdoor spaces, with integrated opportunities for building social connections.
Older adults reported benefits of neighbourhood parks, open spaces and community centres as avenues for social interaction, PA, recreation, relaxation and interaction with nature. Neighbourhood parks and open spaces provided an outlet for older adults to venture out of
their homes. These spaces provided avenues for spontaneous conversations and chance encounters with friends and neighbours, thus creating opportunities for social support and fostering socialties. Notably, parks and green spaces played an important role in the community life of older adults as access to natural environments is limited in large metropolitan Indian cities. Several studies have documented older adults’ use of neighbourhood open spaces and parks linked to improved health outcomes, PA levels, sense of community and reduced stress levels (Schmidt et al., 2019; Zhai et al., 2018). These spaces might be especially important as older adults have smaller social support networks and reduced activity spaces compared to other age groups along with declining health and decreased mobility (McPhee et al., 2016).
In this study, participants emphasised the role of micro-scale urban design and street features such as seating, benches, footpath conditions and shaded areas as especially important for their age group. Many studies indicate that older adults can be more fragile, face an increased risk of falling and may need to rely on mobility aids and assistive devices such as canes, walkers or wheelchairs for active transportation (Zhang et al., 2018). Thus, the condition of streets and walking infrastructure is especially important for older adults. In this study, the most commonly perceived constraints were signs of urban disorder and crime such as graffiti, litter, broken benches, poor maintenance of parks and associated attributes, and an overall lack of safety. Poorly designed and ill-maintained footpaths with obstacles (e.g., encroachments and construction debris) and trip hazards such as uneven surface and potholes can make it difficult for older adults to navigate, thus limiting their everyday PA. Studies have found that older adults’ activity levels may be more negatively impacted by disorder than younger adults’ activity levels (Mooney et al., 2017).
Neighbourhood amenities such as libraries and community centres and community-based cultural programmes provide indispensable opportunities for social participation and community engagement. Studies have shown the positive impact of community events, participatory art and music programmes, and the overall social environment on the health and well-being of older adults. This is especially important as frequency of social participation reduces in later life, due to losses in health, social or financial resources. In our study, opportunities for social participation were restricted in areas that lacked infrastructure such as community centres, public libraries or meeting places, which bring people together, or when access to those places was compromised. These findings substantiate prior research evidence which found that older adults’ perceptions of their neighbourhood predicted their involvement in social activities, volunteering and institutional participation (Woolrych et al., 2018).
An extensive amount of research has examined the relationship between macro-scale elements of neighbourhood walkability (e.g., connectivity, land-use mix and population density), active living and health. However, altering macro-scale features can be difficult to implement in existing neighbourhood settings as it may require substantial reconfiguration of the neighbourhood layout, land subdivisions and transportation networks. On the contrary, re-designing and changing micro-scale features of neighbourhood design, for example, (a) the addition of public facilities such as toilets, rest stops along walking paths, (b) street furniture such as benches and seating, and (c) safe pedestrian environments with footpaths, tactile paving, streetlights, crossing signals, curb cuts and signage are relatively cost-effective and efficient methods of creating environments that are conducive to older adults’ mobility needs. These micro-scale changes may be especially relevant in urban India, where neighbourhoods are often overcrowded, characterised with deficient street designs, lack of pedestrian infrastructure and heavy reliance on private motorised automobiles.
Strengths and Limitations
This study is one of the first to use qualitative methods to examine the relationship between environment and ageing in India, which is a notable strength. Semi-structured interviews with open-ended questions were conducted in local languages by trained researchers until theoretical saturation was reached, providing an adequate sample size. Quality checks were conducted during data collection, translation and transcription processes to ensure rigour and consistency. Additionally, we were able to analyse results using qualitative themes and quotes, enhanced by the independent coding and agreement of codes by an advisory group, which allowed progressive validation of the themes as interviews progressed.
This study has several limitations which should be considered. It was conducted among residents of two cities in India, thus restricting variability and generalizability of findings beyond the study setting. The qualitative approach provided an insight into lived experiences of older adults, but it is not statistically representative. The use of a non-probability sampling method for choosing participants is likely to generate a low level of reliability and high level of bias. By using community gatekeepers to identify participants, the variety of opinions and perceptions present in the interview may have been limited, with a high selection bias related to interest in improving the neighbourhoods, parks and community spaces. Nonetheless, interviews provided rich, qualitative data on the lived experiences of older adults, especially those with frailty and mobility issues. Overall, our findings demonstrate that supportive neighbourhoods with age-appropriate physical and social environment features can foster significant individual and collective benefits to older adults.
Implications for Research, Practice and Policy
As Indian cities encounter a rise in ageing populations, the number of people living with declining physical and cognitive functions will continue to increase. In India, urban planning is currently centred on car use and prioritising vehicular traffic, thus discouraging pedestrians from using streets and public spaces. This may restrict olderadults’ participation in outdoor PA, sequestering them indoors, and contributing to social isolation and sedentary lifestyles. These factors are especially important for older adults with cognitive limitations. For example, the character of street networks, types of landmarks and features that make an area legible can affect the ability of older adults with dementia to understand and navigate their local urban neighbourhoods (Mitchell et al., 2004). A greater focus is needed on interventions that encourage older adults’ social connections and engagement. For example, community hubs that can provide a central access point for a range of sociocultural and recreational programmes and services (e.g., public libraries and community centres) can be promising interventions to address the social needs of older adults, foster independence and nurture a sense of purpose and belonging to a community. Urban planning policies must ensure cities are inclusive, welcoming and supportive places that actively protect and promote older adults’ needs for mobility, independence and social connectedness in later life.
Conclusion
In order to positively impact active ageing, low- and middle-income countries like India need to focus on the design of neighbourhoods, streets and public spaces. Future research is needed to better understand how older adults adapt to changes in their physical settings and social relationships as they continue to age and how environmental factors may affect environmental perceptions and health. This could inform policy efforts to improve neighbourhood supports for active ageing. There is a need to engage researchers, practitioners and policymakers both inside and outside the healthcare system to generate and reframe evidence for active ageing in low- and middle-income countries.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This project described was supported by a Global Challenges Research Fund Award on ‘Age-Friendly Cities in the Global South’ from the UK Department for Economy.