
Abstract
Given the substantial increase in children attending center-based childcare over the past decades, the consequences of center-based childcare for children’s development have gained more attention in developmental research. However, the relation between center-based childcare and children’s neurocognitive development remains relatively underexplored. The aim of this study was therefore to examine the relations between quantity of center-based childcare during infancy and the neurocognitive development (both functional brain networks and self-regulation) of 584 Dutch children. Small-world brain networks and children’s self-regulation were assessed during infancy (around 10 months of age) and the preschool period (2–6 years of age). The findings revealed that the quantity of center-based childcare during infancy was unrelated to individual differences in children’s functional brain networks. However, spending more hours per week in center-based childcare was positively related to the development of self-regulation in preschool age children, regardless of children’s sex or the levels of exposure to risk and maternal support in the home environment. More insight into the positive effects of center-based childcare on children’s development from infancy to toddlerhood can help to increase our insight into a better work–life balance and labor force participation of parents with young children. Moreover, this study highlights that Dutch center-based childcare offers opportunities to invest in positive child outcomes in children, including self-regulation.
Keywords
Introduction
Similar to other countries, the growing number of parents returning to work after maternity leave has led to a substantial increase in children attending center-based childcare in the Netherlands (Organisation for Economic Co-operation and Development [OECD], 2017). In 2022, 376,000 children (i.e., an estimated 54% of the Dutch population between 0 and 4 years) attended Dutch center-based childcare settings (Central Bureau of Statistics, 2023). The age that Dutch children enter center-based childcare is often around 3 months (i.e., after maternity leave). However, there is high variability in the number of hours that Dutch children spent in center-based childcare, because Dutch parents often make use of additional options for non-parental childcare, such as childminders or grandparental care (Ministry of Social Affairs and Employment [SZW], 2023). Yet, on average, Dutch children spent approximately 20 hr per week in center-based care (OECD, 2023). Center-based care is therefore the second most important environment in which the early development of children takes place, next to the home environment (Lamb & Ahnert, 2007).
There has been a long-standing debate about whether early and extensive center-based care may have adverse effects on children’s development, and under which conditions. Previous research has yielded mixed findings, with some studies showing that a higher quantity of center-based childcare was related to lower levels of behavior problems (e.g., Broekhuizen et al., 2017; Votruba-Drzal et al., 2004) and enhanced cognitive performance (Sylva et al., 2011). In contrast, other studies have linked it to increases in children’s behaviors problems (Belsky, 2001; Coley et al., 2013; NICHD ECCRN, 2003) and lower socio-emotional adjustment (Kohl et al., 2020). Recently, a meta-analysis by Rey-Guerra and colleagues (2023) showed no relation between quantity of center-based care and externalizing behaviors across the preschool age period. However, the impact of center-based care on children’s neurocognitive development remains relatively underexplored, despite the critical role of early experiences in children’s brain development (Hofstee et al., 2022; Tau & Peterson, 2010). The aim of this study was therefore to examine the relation between the quantity of early center-based childcare and children’s neurocognitive development during infancy and early childhood.
Neurocognitive development encompasses brain maturation and the development of associated cognitive skills, which both are shaped by early environmental experiences (Bowlby, 2007; Rueda et al., 2004). For instance, during the initial stages of brain maturation, the brain undergoes a process of overproduction of neural connections between different brain regions. Subsequently, guided by information from the environment, the process of overproduction is followed by the elimination (i.e., pruning) of redundant neural connections (Hodel, 2018; Tau & Peterson, 2010). The pruning of less activated neural connections allows the brain to adapt to unique environmental experiences, including those in center-based care, and enhances the efficiency of functional brain networks over time (Cao et al., 2017). Examples of efficient brain networks are small-world networks that consist of densely connected local brain areas (i.e., high clustering coefficients) with long-range connections to other clusters of brain areas (i.e., short path lengths), as assessed by the measure small-worldness (Muldoon et al., 2016).
Previous research comparing individuals across different age groups on the development of small-worldness revealed mixed results, with one study showing an increase in small-worldness from middle to late childhood (Wu et al., 2013) and one study showing a decrease in small-worldness from birth through adolescence (Gozdas et al., 2019). The first study to examine the maturational changes in small-worldness during infancy and early childhood, however, demonstrated that the development of small-worldness is a highly dynamic process that shows a nonlinear growth over time (Hofstee et al., 2024). Specifically, the levels of small-worldness showed an increase during infancy, followed by a decrease in small-worldness from infancy into the preschool age period. These dynamic maturational processes are assumed to shape children’s cognitive and behavioral development and possibly allow for more complex behaviors to arise during early childhood, such as self-regulation (Cao et al., 2017; Tau & Peterson, 2010).
The development of small-worldness was indeed positively related to self-regulation in the preschool period, controlling for self-regulation during infancy (Hofstee et al., 2024). Therefore, the nonlinear development of small-worldness might reflect an effective neural reorganization of the brain, that lays foundations for essential skills, such as self-regulation (Tau & Peterson, 2010). Self-regulation refers to the ability to control thoughts, emotions, and behaviors and develops rapidly during early childhood (Nigg, 2017). In contrast to a large body of research examining the impact of experiences in the home environment, particularly parenting behaviors (e.g., Bernier et al., 2010; Fay-Stammbach et al., 2014), there is limited research on the possible effects of center-based childcare on child self-regulation. More insight into the effects of the quantity of center-based care on the early neurocognitive development of young children is therefore needed, given that higher levels of self-regulation have been found to promote mental and physical health, as well as academic performance later in life (Moffitt et al., 2011).
Center-Based Childcare and Children’s Neurocognitive Development
Based on the discrepancy between negative results of some US studies (e.g., Belsky, 2001; NICHD ECCRN, 2003) and more positive outcomes of studies from other countries (e.g., Norway), some researchers have recently highlighted the importance of examining the effects of quantity of center-based care in various countries to explore results in largely different childcare systems (Backer-Grøndahl & Nærde, 2017; Kohl et al., 2020; Linberg et al., 2020). Possibly, negative effects on children’s development are reported in center-based care contexts with extensive childcare experiences at an early age and with highly varying levels of quality. In contrast, results may be more positive in a childcare system with relatively homogeneous, high quality levels. Seen from this perspective, it seems important to investigate quantity effects in the Dutch childcare context, which is characterized as a childcare system with relatively homogeneous, favorable structural quality characteristics (e.g., small group sizes) and relatively high levels of process quality (e.g., high levels of support toward children), as indicated by recent national quality assessments (Romijn et al., 2023; Slot et al., 2019).
Given that the general maternity leave period for Dutch mothers is 3 months, rather than around 15 months in most other EU countries, the Dutch childcare context is characterized by a relatively early age that infants enter center-based childcare (OECD, 2017). According to attachment theory (Bowlby, 1969), young infants heavily rely on consistent and supportive behaviors from stable caregivers to buffer the developing stress system and to support the regulation of internal states (Ainsworth, 1969; Engel & Gunnar, 2020). However, caregiver stability in center-based childcare can be affected by frequent changes of caregivers during the week (Fukkink, 2022). Moreover, the absence of the primary caregiver during extensive center-based childcare attendance might lead to stress in young infants (for a review, see Jarvis, 2022). Subsequently, higher levels of stress may negatively affect the experience-dependent maturation of functional brain networks in young children (Blair, 2010; Blair & Raver, 2016; Wagner et al., 2016).
With regard to self-regulation, caregivers in center-based care have to divide their supportive behaviors over a relatively large and heterogeneous group of children (Fukkink, 2022). As a result, children might receive less external regulation from caregivers in center-based childcare compared with their primary caregivers, which could negatively affect the development of self-regulation (Bernier et al., 2010). Despite the concerns raised in prior work, findings of a study performed in Norway showed that more hours in center-based childcare during infancy (i.e., at 12 months of age) was not significantly related to self-regulation, measured with a battery of self-regulation tasks at 48 months of age (Backer-Grøndahl & Nærde, 2017). These results are in line with studies on preschool age children, showing that the quantity of center-based care per week in Switzerland was unrelated to variations in self-regulation as assessed by an inhibitory control task (Zysset et al., 2018) and teacher-reported measures in the United States (Melo et al., 2022). These studies suggest that child self-regulation is unaffected by the quantity of center-based childcare during infancy. However, the relation between quantity of center-based childcare and children’s self-regulation development within the Dutch childcare context is, to our knowledge, still unknown.
Moderating Effects of Risk Factors and Parental Support in the Home Environment
More hours in center-based care might also offer benefits for children’s development, especially for children from less advantaged families. For instance, center-based care can provide greater and more structured learning opportunities compared with children’s home environments (Berry et al., 2016; Fuller et al., 2004). These enriched learning opportunities have been found to positively affect functional brain networks (Huttenlocher, 2009), as well as child self-regulation (Fay-Stammbach et al., 2014). In children from low-income families in Chile, attendance in center-based care under 2 years of age was indeed positively related to self-regulation (Noboa-Hidalgo & Urzùa, 2012). Likewise, more hours in center-based care between 7 and 36 months have been related to higher levels of self-regulation (assessed by a battery of executive-function tasks) in a predominantly low-income sample in the United States, specifically in children with low levels of basal cortisol (Berry et al., 2014b). These findings indicate that there are individual differences in the way how children are affected by their early childcare experiences (Loeb et al., 2007).
In the US context, negative effects of quantity of center-based childcare have primarily been reported among relatively advantaged families (Huston et al., 2015), whereas positive effects have been reported for disadvantaged groups (e.g., Berry et al., 2016). Even within the same study, more hours in center-based care between 7 and 36 months of age were related to lower levels of cortisol at 48 months of age in children with exposure to multiple risk factors in the home environment (e.g., low socioeconomic status [SES], no spouse/partner living in the home), whereas in children with low exposure to risk, more hours in center-based care were associated with higher cortisol levels at 48 months (Berry et al., 2014a). As a chronic elevation of cortisol levels in children is thought to negatively impact long-term neurocognitive outcomes (Blair, 2010; Blair & Raver, 2016; Wagner et al., 2016), children with exposure to multiple risks in the home environment may reap the benefits of spending more time in center-based care, whereas spending more time in center-based care might be less beneficial for infants with low exposure to risk in the home environment (Berry et al., 2014a).
The relation between quantity of center-based childcare and children’s neurocognitive development may also depend on the levels of parental support that children receive in their home environment. For example, higher levels of parental support can help to regulate the stress levels of young children in challenging situations, such as during separation from the primary caregiver in center-based childcare (Ahnert et al., 2004; Loman & Gunnar, 2010). However, in contrast to the study with toddlers of Ahnert and colleagues (2004), previous research in the Netherlands revealed that infants who received more parental support showed increased cortisol levels in center-based care, whereas children who received less parental support showed decreased cortisol levels in center-based care (Albers et al., 2016). This demonstrates that for infants from supportive home environments, the unavailability of the primary caregiver for an extended period of time might be more stressful than for infants who are not used to high levels of support in the home environment. Therefore, parental support may moderate the effects of center-based care on the neurocognitive development of children as well. Yet, research on the moderating role of the home environment (i.e., exposure to risk and parental support) in the relation between quantity of center-based care and the neurocognitive development of children is, to our knowledge, still lacking.
Moderating Effect of Children’s Sex
The effects of center-based care attendance on children’s neurocognitive development may also differ for boys and girls. For instance, boys tend to lag behind girls in their early neurocognitive development, as is evident in less mature patterns of brain activity (Cuevas et al., 2016) and lower self-regulatory abilities compared with girls (for meta-analyses, see Else-Quest et al., 2006; Silverman, 2021). As a result, young boys might rely more heavily on supportive behaviors from caregivers to help them regulate their own internal states (Ainsworth, 1979; Engel & Gunnar, 2020). However, forming a secure relationship with caregivers in center-based care appears to be more challenging for boys than girls (Ahnert et al., 2006). It has therefore been suggested that, for their positive development, boys rely for more on high quality, well-structured care environments with more supportive caregivers, compared with girls (Votruba-Drzal et al., 2010).
Previous research demonstrated that boys in general appear to be more susceptible to the effects, either positive or negative, of quantity of center-based care. For instance, in a low-risk sample, boys were more affected by the negative effects of center-based childcare (i.e., spending more time away from their primary caregivers in large group sizes) on language and cognitive measures than girls (Bornstein et al., 2006). In contrast, in a low-income sample, attending high quality center-based care was more protective for the development of externalizing problems in boys than in girls (Votruba-Drzal et al., 2004). These findings suggest that the positive or negative effects of the quantity of center-based care on children’s neurocognitive development may also be more pronounced in boys than girls. To our knowledge, however, no study has examined sex differences in the relationship between the quantity of center-based care and children’s neurocognitive development.
The Current Study
More research on the effects of center-based childcare attendance on the development of young children in particular is important because of their vulnerability to increased stress levels and because they still heavily rely on secure and supportive environments to help them regulate their internal states (Bowlby, 1969; Engel & Gunnar, 2020). In addition, it is unclear whether the effects of center-based childcare on neurocognitive development vary for children from different home environments and for boys and girls. Therefore, this study aimed to provide a better understanding of how quantity of center-based care during infancy (at T1 and T2) is related to the neurocognitive development (both functional brain networks and self-regulation) of Dutch children during infancy (T2) and during the preschool period (T3). In addition, we examined whether the relation between quantity of center-based childcare during infancy and variations in the neurocognitive development of children is moderated by exposure to risk, parental support, and children’s sex.
Based on findings from previous research (Backer-Grøndahl & Nærde, 2017; Melo et al., 2022; Zysset et al., 2018), no main effect of quantity of center-based care during infancy on the neurocognitive development of children was expected. However, several moderating effects were expected. First, for both children from lower risk home environments and children with more supportive home environments, we expected that more hours in center-based care would be related to lower levels of small-worldness at T2 and higher levels of small-worldness at T3, as well as lower levels of self-regulation at both T2 and T3. In contrast, for both children from higher risk home environments and children from less supportive home environments, we expected that more hours in center-based care would be related to higher levels of small-worldness at T2 and lower levels of small-worldness at T3, as well as higher levels of self-regulation at both T2 and T3. Finally, we hypothesized that the relations (either positive or negative) between quantity of center-based childcare and variations in small-worldness and self-regulation would be stronger in boys compared with girls.
Method
Participants
Participants of this study were part of the YOUth Baby & Child cohort, a large-scale ongoing longitudinal study conducted in the Netherlands. Data were derived from three waves (T1 = around 5 months of age, T2 = around 10 months of age, T3 = around 3 years of age). The sample consisted of participants that had continued participating in the YOUth cohort study up until the third measurement wave of the YOUth Baby & Child cohort at the start of this study. Participants were excluded if they did not provide data on the quantity of center-based childcare at both waves (N = 17). Due to the limited number of fathers who served as the primary caregivers 1 (N = 4), it was not feasible to examine the role of fathers in this study. Therefore, the final sample consisted of 584 children (52% girls) and their mothers (i.e., primary caregivers). Participants in the current sample were predominantly from high SES families (see Table 1 for the demographics). Mean age of the children was 23.04 weeks (SD = 3.40) at T1, 44.80 weeks (SD = 3.88) at T2, and 188.34 weeks (SD = 44.54) at T3.
Participant Demographics.
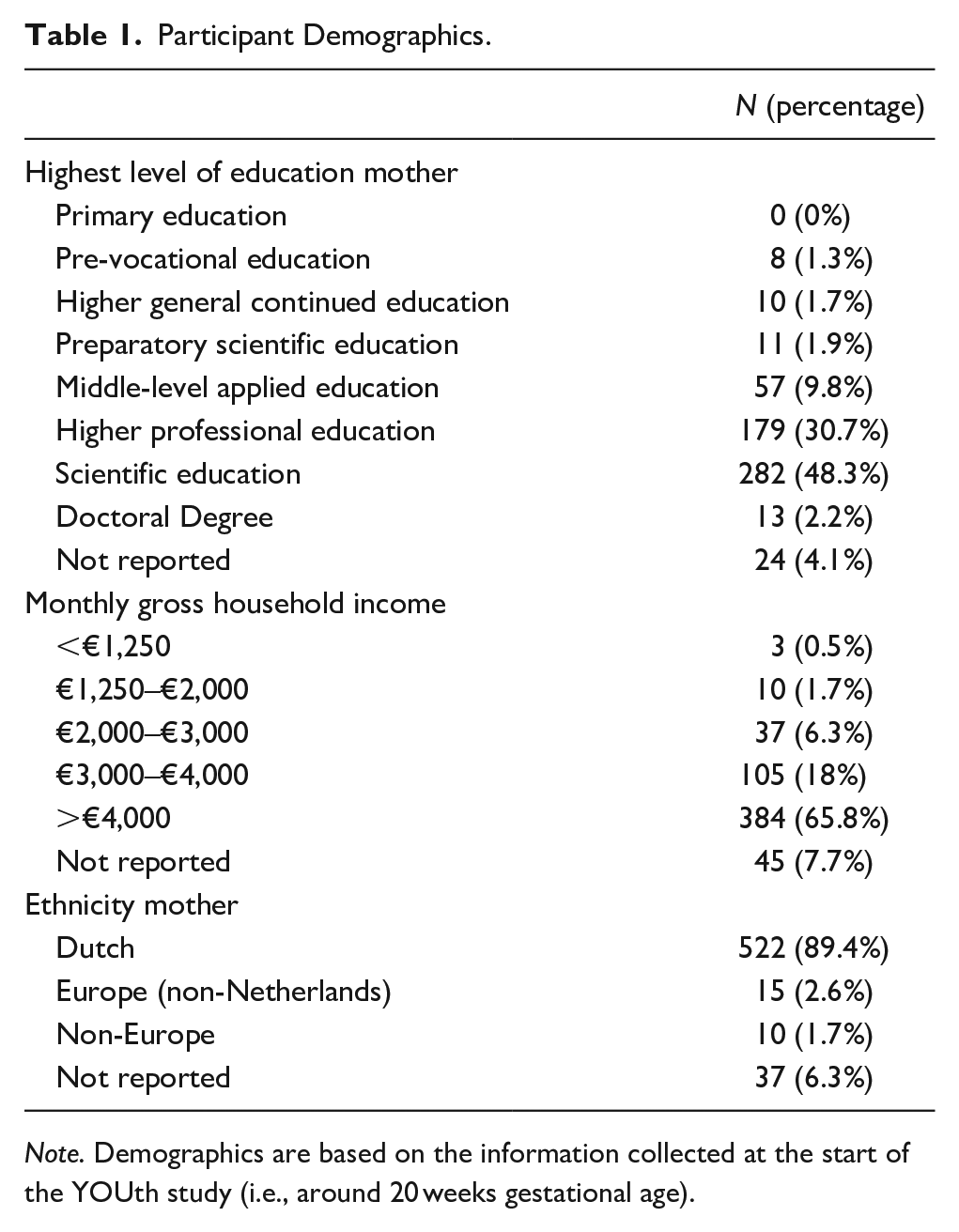
Note. Demographics are based on the information collected at the start of the YOUth study (i.e., around 20 weeks gestational age).
Procedure
The participants of the YOUth cohort study were recruited through 32 midwifery practices and the primary care midwifery practices of five large hospitals in the region of Utrecht. Inclusion criteria required that parents had authority over their children and a proficient understanding of the Dutch language to comprehend all study-related information and instructions. Children were excluded from the YOUth cohort study if they were not born full-term (i.e., less than 38 weeks), had a birth weight under 2,500 g, or when the health care providers reported developmental delays or abnormalities in visual or auditory processing that can influence brain or behavior development. Informed consent from both parents was a prerequisite for inclusion in the study at each measurement wave.
Participants who met the inclusion criteria were invited to the research laboratory of YOUth at Utrecht University, the Netherlands (Onland-Moret et al., 2020). During the lab visit, children and one of their parents took part in a variety of measurements. A team of well-trained and experienced researchers and research assistants were responsible for the data collection and parents received a compensation of €30 for each lab visit. More information on the measurements of YOUth can be found on the website: https://www.uu.nl/en/research/youth-cohort-study. In addition to the measurements in the research laboratory, both parents filled out several online questionnaires during and shortly after the lab visit. The Medical Research Ethics Committee of the University Medical Center Utrecht approved the study protocol (METC 14-616).
Measures
Center-Based Childcare
To assess the quantity of center-based childcare, primary caregivers were asked to report the number of hours per week their children spent in center-based childcare at T1 and T2. Responses were grouped into six categories: 0 hr (1), <8 hr (2), 8–<16 hr (3), 16–<24 hr (4), 24–<32 hr (5), and 32–40 hr (6). To create a global score on quantity of center-based childcare during infancy (i.e., the average of T1 and T2), the median number of hours of each category was used. For example, the 16 to 24 hr category was recoded as 20 hr. Subsequently, the quantity of center-based childcare during infancy was determined by averaging the number of hours in center-based childcare at T1 and T2 (r = .79). This represented a global measure of quantity of center-based childcare in the first year of life, similar to prior work (e.g., Berry et al., 2014b; NICHD ECCRN, 2003).
Functional Brain Networks
Functional brain networks at T2 and T3 were evaluated using resting state EEG (i.e., quiet wakefulness). The EEG recordings were conducted in a quiet and dimly lit room, with children seated on their parents’ lap or in a car seat positioned at eye level, 65 cm away from the computer screen. Two videos, one featuring singing women and the other displaying moving toys without human interference, were employed to capture a period of resting physiology (Bell & Cuevas, 2012). Each video had a duration of 1 min and was repeated three times with short breaks in between. EEG data was collected using a cap fitted with 32 electrodes (ActiveTwo system, BioSemi), arranged according to the international 10/20 system. The recording were made from the frontal pole (Fp1 and Fp2), medial frontal (F3 and F4), lateral frontal (F7 and F8), central (C3 and C4), temporal (T7 and T8), medial parietal (P3 and P4), lateral parietal (P7 and P8), and occipital (O1 and O2). The Common Mode Sense (CMS) and Driven Right Leg (DRL) electrodes served as an active ground. EEG recordings were sampled at a rate of 2,048 Hz.
The EEG recordings were cleaned and analyzed in MATLAB, using functions of the FieldTrip toolbox (Oostenveld et al., 2011). The original 2,048-Hz data were down sampled to 512 Hz through chip interpolation and bandpass filtered in the range of 0.1–70 Hz using a two-way Butterworth filter. Artifacts were removed from the continuous EEG data, including trials with excessively high amplitudes (>250 uV), jumps (detected with ft_jump_removal.m), excessive non-normality (kurtosis > 7), flatlining electrodes (inverse of variance > 0.1), or excessive noise (variance > 1,500). If it was determined that there were more than two problematic channels, meaning that over 40% of the signal in the channel contained artifacts, the specific EEG recording was treated as missing data. The cleaned data was bandpass filtered into eight frequency bands and segmented into 3-s epochs. In this study, the infant theta (3–5.9 Hz) was used at T2 and the toddler theta (4–6.9 Hz) was used at T3. 2
Functional connectivity between all pairs of electrodes was computed using the phase lag index (PLI). The PLI characterizes the asymmetry in the distribution of phase differences between pairs of signals and is slightly more reliable compared with the debiased weighted PLI in young children (Stam et al., 2007; van der Velde et al., 2019). Following this, various graph measures were derived from the individual connectivity matrices obtained. For this study, the small-world propensity (SWP) was used as a measure of functional brain networks (Muldoon et al., 2016). The SWP is calculated as the ratio between the normalized clustering coefficient and the normalized characteristic path length of the network or graph. Here, the clustering coefficient measures the degree to which local brain areas in the functional brain network cluster together, whereas the characteristic path length quantifies how efficiently information can be transmitted between distinct clusters of brain areas across the functional brain network (Humphries & Gurney, 2008). In a small-world network, the clustering coefficient is relatively high, indicating that neighboring brain areas are highly interconnected. In contrast, the characteristic path length is relatively short, indicating that the network facilitates efficient global communication (Muldoon et al., 2016). SWP values could span from 0 to 1, with a value closer to 1 indicating higher levels of functional brain networks. Functional brain networks with a small-world propensity of 0.4 and higher are considered small-world networks (Bassett & Bullmore, 2017).
Self-Regulation
Self-regulation at T2 (i.e., orienting/regulatory capacity) was assessed with the Infant Behavior Questionnaire–revised–short form (IBQ-R-SF; Putnam et al., 2014). Self-regulation at T3 (i.e., effortful control) was assessed with the Early Childhood Behavior Questionnaire–short form (ECBQ-SF; Putnam & Rothbart, 2006) and Children’s Behavior Questionnaire–very short form (CBQ-SF; Putnam & Rothbart, 2006), depending on the age of the child (ECBQ-SF for children < 3 years and CBQ-SF for children > 3 years). The IBQ-R-SF, ECBQ-SF and the CBQ-SF are developmentally equivalent measures that have been shown to have longitudinal stability (Putnam et al., 2008). The self-regulatory behaviors of the children were rated on a 7-point Likert-type scale ranging from never/extremely untrue (1) to always/extremely true (7). An example item of the IBQ is: “When you patted or gently rubbed your baby’s body, how often was your baby immediately comforted?” An example item of the CBQ is “Your child can wait with new activities if requested.”
Parent-reported child self-regulation at T2 was derived by calculating the mean of the scores on the Duration of Orienting (N = 6 items), Low-Intensity Pleasure (N = 7 items), Cuddliness (N = 6 items), and Soothability (N = 7 items) subscales of the IBQ-R-SF (Putnam et al., 2014). Parent-reported child self-regulation at T3 was derived by calculating the mean of the scores on the Attention Focusing (N = 6 items), Attention Shifting (N = 8 items), Cuddliness (N = 6 items), Inhibitory Control (N = 6 items), and Low-Intensity Pleasure (N = 6 items) subscales of the ECBQ-SF (Putnam & Rothbart, 2006), or the Attention Focusing (N = 6 items), Inhibitory Control (N = 6 items), Perceptual Sensitivity (N = 6 items), and Low-Intensity Pleasure (N = 8 items) subscales of the CBQ-SF (Putnam & Rothbart, 2006). Good internal consistency was found for all self-regulation scales (α = .84 for IBQ-R-SF, α = .86 for ECBQ-SF, and α = .84 for CBQ-SF).
Exposure to Risk in the Home Environment
Scores on exposure to risk in the home environment were created by summing multiple psychosocial and psychological indicators of risk at T2. These indicators were (1) low marital quality (i.e., divorce or conflicts), (2) work-related stress within the family (i.e., fired, partner became unemployed, troubles with colleagues), (3) physical health problems within the family (i.e., long-term illness, life-threatening disease, hospitalization, accident), (4) loss (i.e., loss of a close relative or friend), (5) financial problems within the family (i.e., income dropped significantly, large debts), (6) maltreatment within the family (i.e., sexual abuse, domestic violence, physical abuse), (7) anxiety symptoms, and (8) depression symptoms. 3 The risk factors were chosen to reflect distinct stressful life events and symptoms of mental health problems that often lead to distress in parents and may lead to stressful family contexts in which young children grow up (Evans et al., 2013; Nair et al., 2003).
Participants reported on the presence or absence of a risk factor in the past 12 months with a binary response (yes/no). The first six psychosocial risk indicators were in line with questions from the widely used Life Event and Difficulty Schedule (LEDS; Brown & Harris, 1989). The questions of the LEDS (e.g., “Did you go through a divorce or separation in the past 12 months?”) are considered reliable and suitable for assessing exposure to risk in community samples (Brown & Harris, 1989; Wethington et al., 1995). Given that the LEDS typically focuses on external psychosocial events and stressors rather than internal psychological risk factors, two additional psychological risk factors were included in this study. The psychological questions (e.g., “Did you ever had a period of feeling very sad or depressed, for at least 2 weeks in a row, in the past year?”) were in line with other reliable and valid measures of distress and psychopathology (e.g., UM-CIDI; NIMH DISC-IV Shaffer et al., 2000; Wittchen et al., 1995). The presence of a risk factor was coded as “1,” while the absence of a particular risk factor was coded as “0..” Subsequently, scores on exposure to risk (0–8) were created by summing the individual risk indicators, such that higher scores indicated greater exposure to risk.
Parental Support
The levels of support of the mothers toward their children were assessed using the Comprehensive Early Childhood Parenting Questionnaire at T2 (CECPAQ; Verhoeven et al., 2017). The CECPAQ is a reliable measure of various parenting behaviors within five domains (support, structure, stimulation, harsh discipline, and positive discipline). In the original study of Verhoeven et al. (2017), the answers are scored on a 6-point Likert-type scale, with responses ranging from never (1) to always (6). However, due to an error within the online questionnaire, the answers on parental support were rated on a 5-point Likert-type scale ranging from never (1) to often (5) in this study. An example item of the CECPAQ is: “I know exactly what my child wants or feels.” Parental support was derived by calculating the mean of the Sensitivity (N = 4 items), Responsiveness (N = 5 items), and Affection (N = 4 items) subscales. The items used to create the score on parental support had good internal consistency (α = .86).
Data-Analysis
Path analyses 4 were conducted to examine the main effects of quantity of center-based childcare on functional brain networks and child self-regulation, as well as the potential moderating effects of exposure to risk, parental support, and children’s sex. The analyses were carried out in Mplus 8.8 (Muthén & Muthén, 2017). Due to the dissimilarity in variable scales, the variables were standardized in Mplus before the analysis. This approach can help avoid issues regarding multicollinearity, as the interaction terms cannot be affected by the scaling of the original variables (Aiken & West, 1991). The interaction terms (Childcare × Parental Support, Childcare × Risk, Childcare × Children’s sex) were derived by multiplying the standardized predictor and mediator variables.
Given the broad age ranges at T3, children’s age was included as a covariate in the moderation model. Furthermore, levels of functional brain networks and self-regulation at T3 were controlled for prior levels of functional brain networks and self-regulation at T2. The model was estimated using the maximum likelihood (ML) estimator. In addition, 10,000 bootstrap samples were employed to estimate the sampling distributions. Model fit was assessed using goodness-of-fit statistics, including the chi-square divided by the degrees of freedom (χ2/df), the comparative fit index (CFI), the root mean square error of approximation (RMSEA) and the standardized root mean square residual (SRMR). Good model fit was indicated by a χ2/df value less than 3, a CFI value above .95, a RMSEA value less than .06, and a SRMR value less than .08 (Schreiber et al., 2006). Statistical significance was determined based on a two-tailed p-value of .05.
Missing Data
The percentage of missing data on quantity of center-based childcare was 6% at T1 and 11% at T2. Regarding parent-reported self-regulation, 12% was missing at T1 and 10% at T2. The percentage of missing EEG data was 37% at T1 and 25% at T2. In addition, 11% of the participants had missing data on exposure to risk and 13% of the participants had missing data on the levels of support. The results of Little’s (1988) missing completely at random test indicated that the missing data did was missing not at random, χ2 = 377.362, p < .001. This likely stems from nonresponse by the primary caregiver on the parent-reported questionnaires (χ2 = 84.931, p = .004) rather than the EEG recordings of the children at both waves (χ2 = 2.320, p = .314). As Multiple Imputation (MI) leads to less bias compared with listwise deletion when data are missing not at random (van Ginkel et al., 2020), MI was applied to address the missing data. Fifteen imputed datasets were created through Bayesian analysis, by using all relevant information in the dataset (Rubin, 1976). Parameter estimates were averaged across the imputed datasets and standard errors were computed based on the average over the imputed datasets, while accounting for the within and between imputation variation in estimates (Muthén & Muthén, 2017).
Exploratory Analysis
Dutch children generally enter elementary school at the age of 4. As a result, children above 4 years of age quickly improve important skills, such as academic, language, and social skills (Leseman et al., 2001; Melhuish et al., 2015). As these skills might influence the neurocognitive development of young children (Ramsook et al., 2020; Slot & von Suchodoletz, 2018), an exploratory analysis was performed to examine whether the findings were different for children under 4 years of age (N = 378) or above 4 years of age at T3 (N = 206). The hypotheses, study design, and planned analyses of this study were preregistered at the Open Science Framework (https://osf.io/57dnx).
Results
Descriptive Statistics
The descriptive statistics for the variables are shown in Table 2. Quantity of center-based childcare varied from 0 to 36 hr per week, with an average of 17.07 hr per week for children attending center-based childcare at T1 and an average of 17.48 hr per week for children attending center-based childcare at T2. All children demonstrated the characteristics of a small-world network, indicated by small-worldness scores above the threshold of .40 (Bassett & Bullmore, 2017). Overall, children showed relatively high levels of self-regulation at T2 and T3. The number of risk factors ranged from 0 to 8, but on average, parents were exposed to very few risk factors. In addition, mothers showed relatively high levels of support toward their children.
Correlations for Study Variables (N = 584).
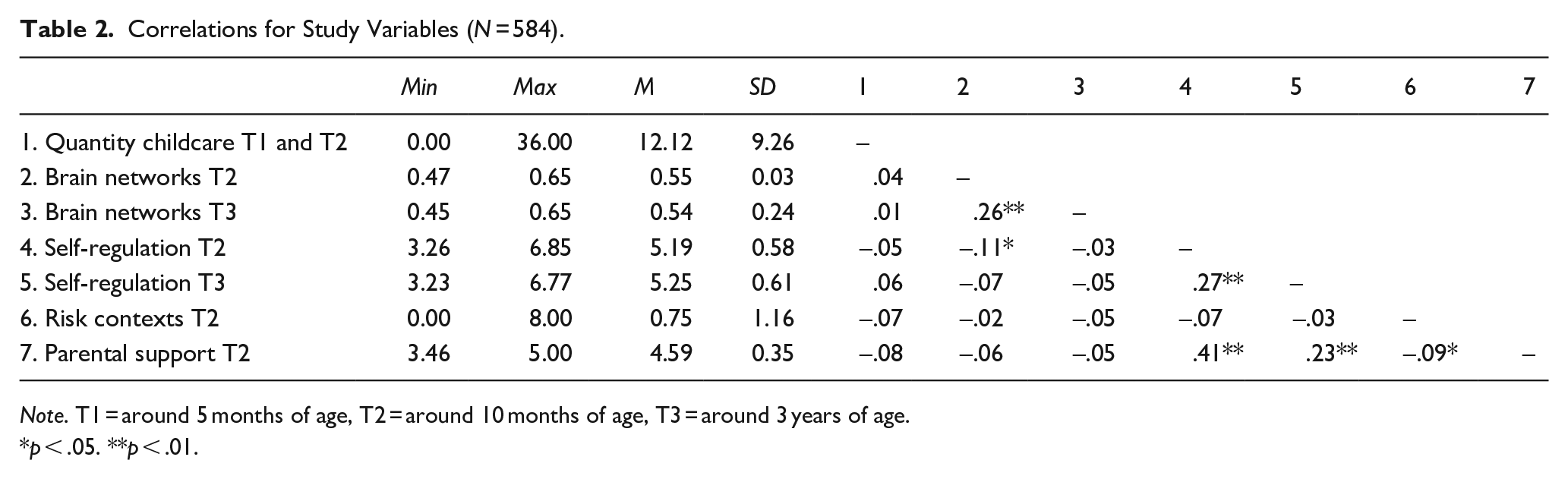
Note. T1 = around 5 months of age, T2 = around 10 months of age, T3 = around 3 years of age.
p < .05. **p < .01.
No significant differences were found between boys and girls at T2, but at T3, girls had significantly higher scores on self-regulation than boys, t(530) = −2.608, p = .009. Boys and girls did not differ in their small-worldness levels. The skewness and kurtosis values for all variables fell within the range of −1 to 1, indicating that the assumption of normality was met (George & Mallery, 2010).
One outlier was found for self-regulation at T1, indicated by a value of 3.29 SD below the mean (Tabachnick et al., 2013). However, the score appeared to represent a valid data point (e.g., close to the lowest non-outlying score) and there was no justifiable reason to change or remove the outlier, as the results remained the same without this outlier. Therefore, the score was retained in the analysis. Results of the Pearson correlation test showed that quantity of center-based childcare was unrelated to variations in both functional brain networks and self-regulation at T2 and T3 (Table 2). Higher levels of exposure to risk were related to lower levels of the levels of parental support. However, no relations emerged between exposure to risk and both functional brain networks and self-regulation. Parental support was positively associated with self-regulation at T2 and T3, but not with functional brain networks at T2 and T3. Self-regulation at T2 was positively related to self-regulation at T3, and functional brain networks at T2 were positively related to functional brain networks at T3. In addition, lower levels of functional brain networks at T2 were related to higher levels of self-regulation at T2.
Center-Based Childcare and Children’s Neurocognitive Development
In the longitudinal moderation model, the effect of quantity of center-based childcare on functional brain networks and self-regulation was estimated, controlling for prior levels of functional brain networks and self-regulation (see Figure 1). In addition, exposure to risk, parental support, and children’s age were added as moderators to the model. All fit indices indicated that the model was a good fit to the data, χ2/df = 1.69, CFI = .981, RMSEA = 0.034, SRMR = 0.022. The parameter estimates, their standardized errors, and the lower and upper bounds of the confidence interval are presented in Table 3. Model results showed a significant association between spending more hours in center-based childcare during infancy and higher levels of self-regulation at T3, controlling for prior levels of self-regulation. However, quantity of center-based childcare was neither related to self-regulation at T2, nor to functional brain networks at T2 and the change in functional brain networks from T2 to T3. Exposure to risk was unrelated to the outcome variables. Higher levels of parental support were related to higher levels of self-regulation at both T2 and more growth in self-regulation from T2 to T3. In addition, sex of the children was a significant predictor of growth in self-regulation from T2 to T3, but not of the level of self-regulation at T2. None of the interaction terms significantly predicted individual differences in self-regulation and functional brain networks at T2 and changes from T2 to T3.
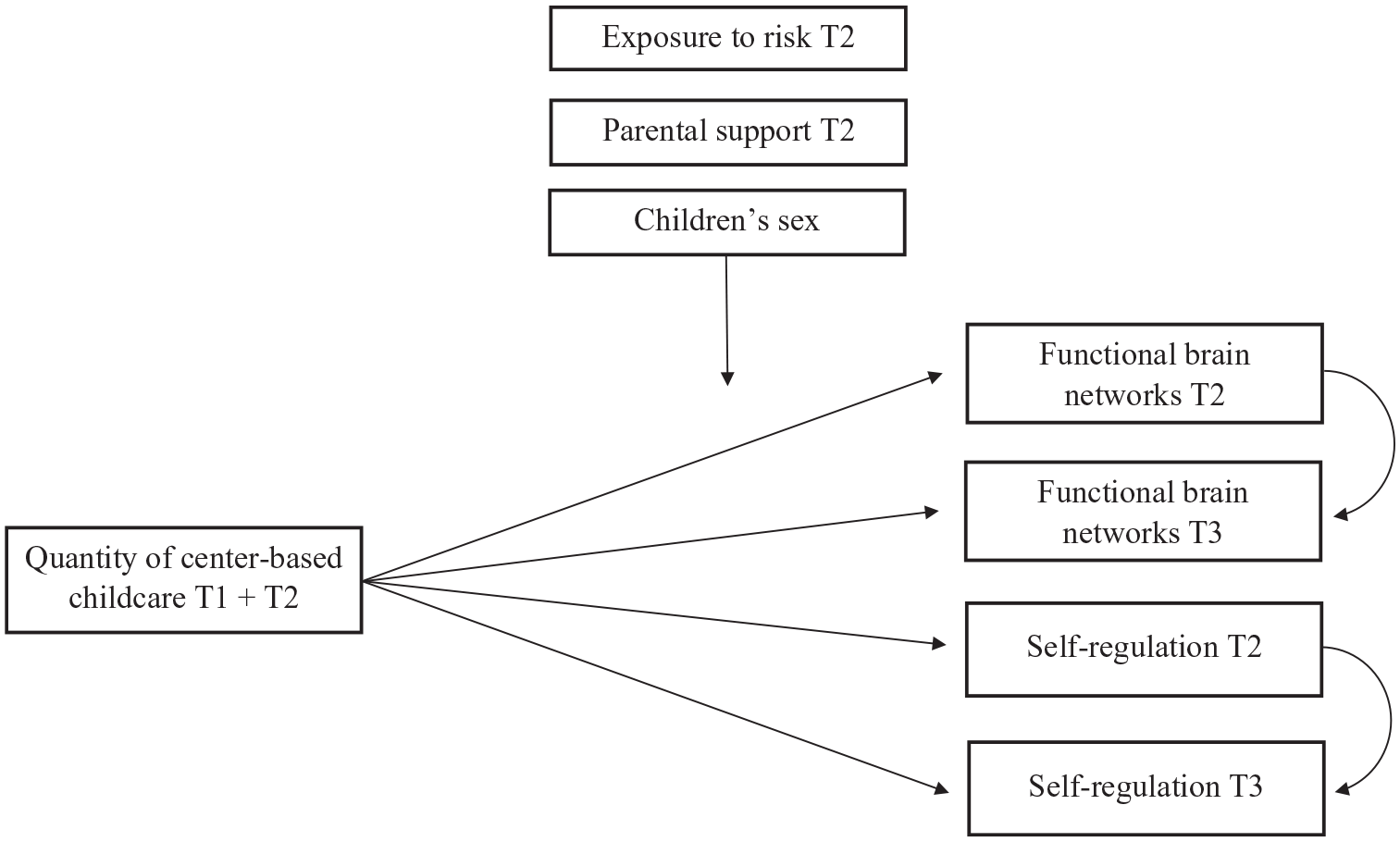
The Hypothesized Model to Test the Relation Between Quantity of Center-Based Childcare and Children’s Neurocognitive Development.
Parameter Estimates for the Longitudinal Moderation Model (N = 584).
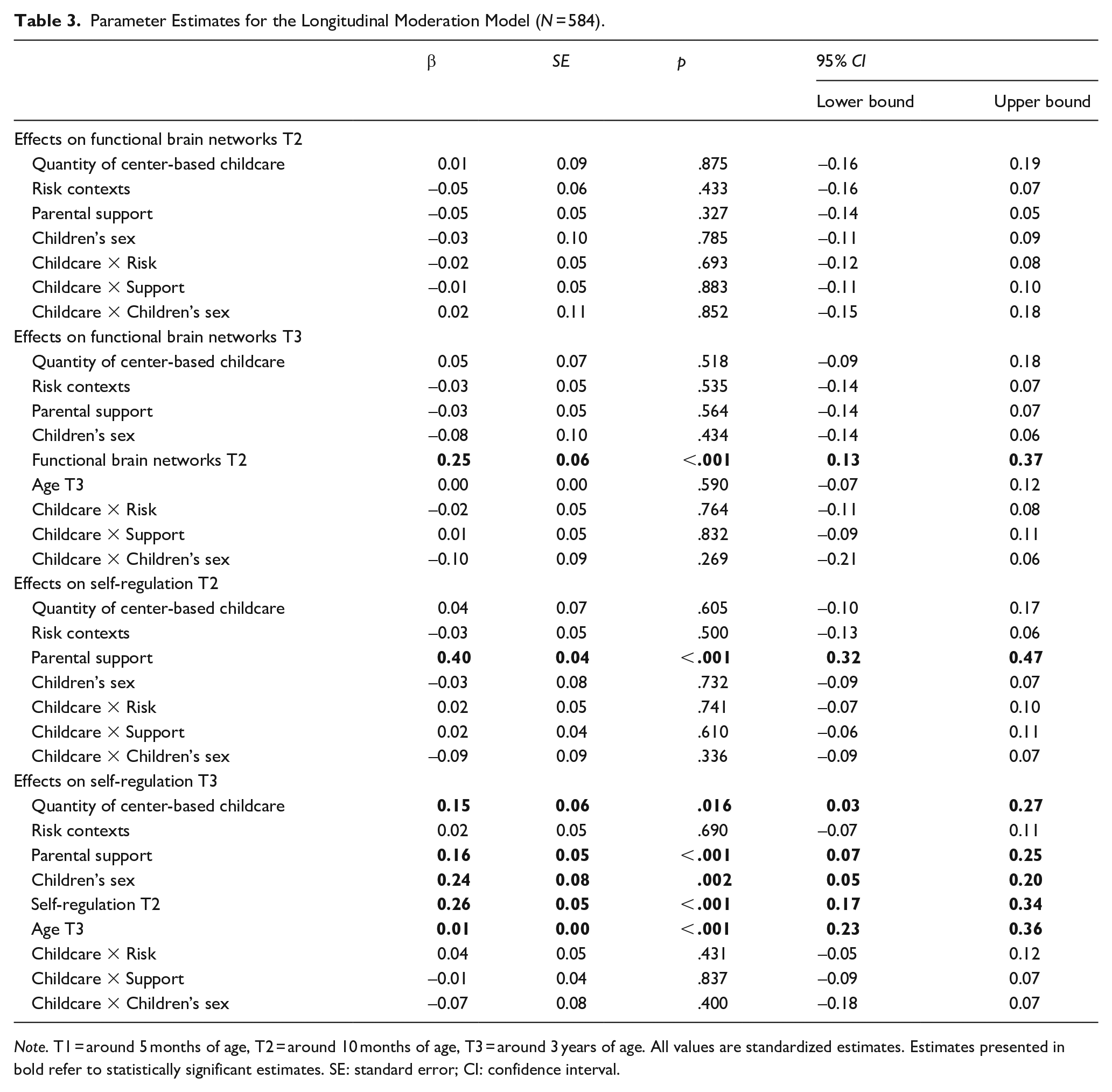
Note. T1 = around 5 months of age, T2 = around 10 months of age, T3 = around 3 years of age. All values are standardized estimates. Estimates presented in bold refer to statistically significant estimates. SE: standard error; CI: confidence interval.
Exploratory Analyses
To examine whether the results are different for children under or above 4 years of age, the model was rerun for the age groups separately. The model showed a good fit to the data for children under 4 years of age, χ2/df = 0.81, CFI = 1.000, RMSEA = 0.000, SRMR = 0.022, as well as for children above 4 years of age, χ2/df = 1.52, CFI = 0.949, RMSEA = 0.050, SRMR = 0.038. The model results demonstrated that quantity of center-based childcare was unrelated to the outcome variables in both subgroups (see Tables 4 and 5). In addition, exposure to risk was unrelated to the outcome variables. In children under and above 4 years of age, greater parental support was associated with higher levels of self-regulation at T2 and a greater increase in self-regulation from T2 to T3. Children’s sex was not related to self-regulation in children under 4 years of age, but significantly predicted changes in self-regulation from T2 to T3 in children above 4 years of age. Similar to the main analysis, none of the interaction terms were significant. Thus, the findings in the main analysis were not driven by child age.
Parameter Estimates for the Longitudinal Moderation Model for Children under 4 Years of Age (N = 378).
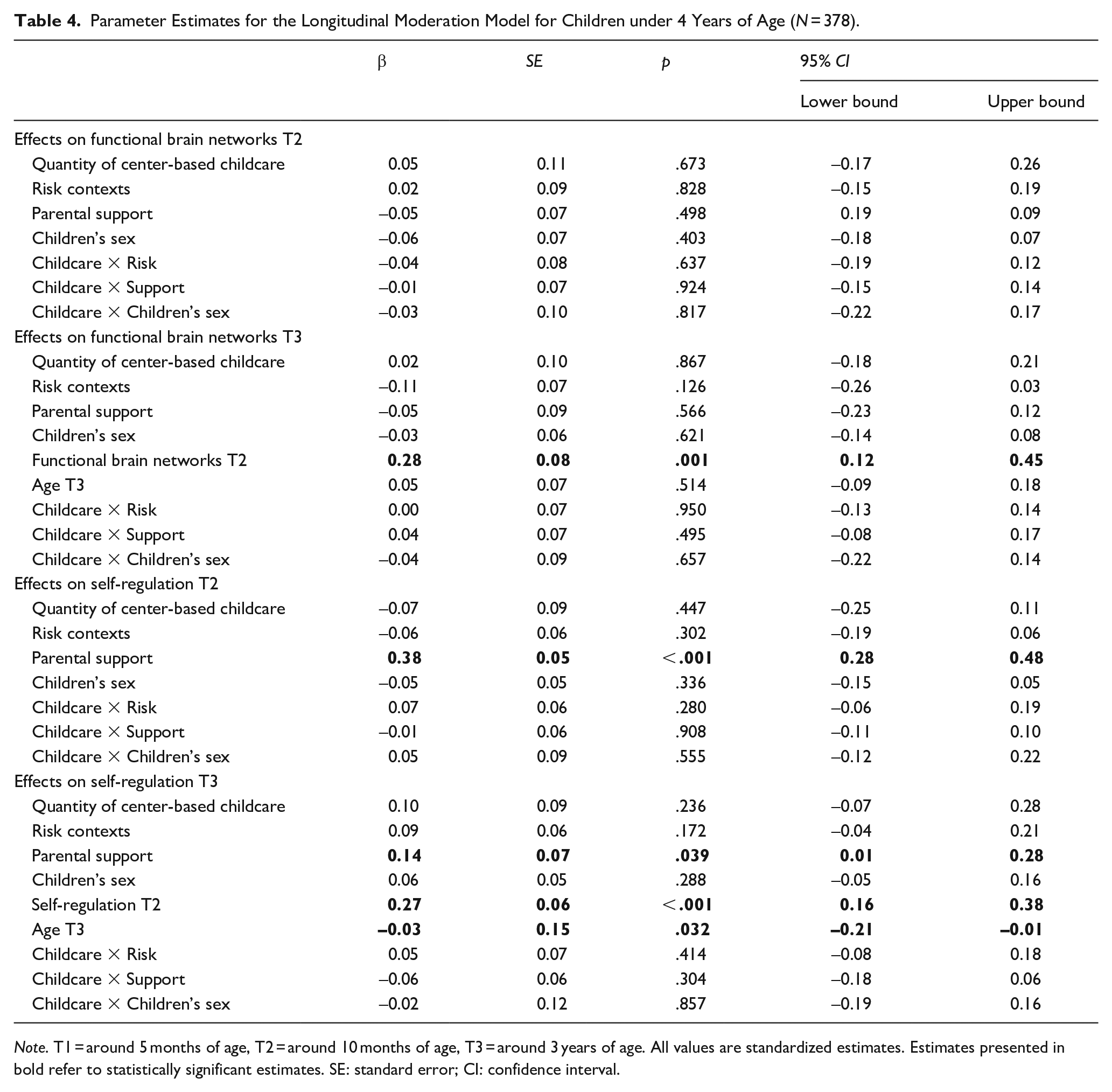
Note. T1 = around 5 months of age, T2 = around 10 months of age, T3 = around 3 years of age. All values are standardized estimates. Estimates presented in bold refer to statistically significant estimates. SE: standard error; CI: confidence interval.
Parameter Estimates for the Longitudinal Moderation Model for Children above 4 Years of Age (N = 206).
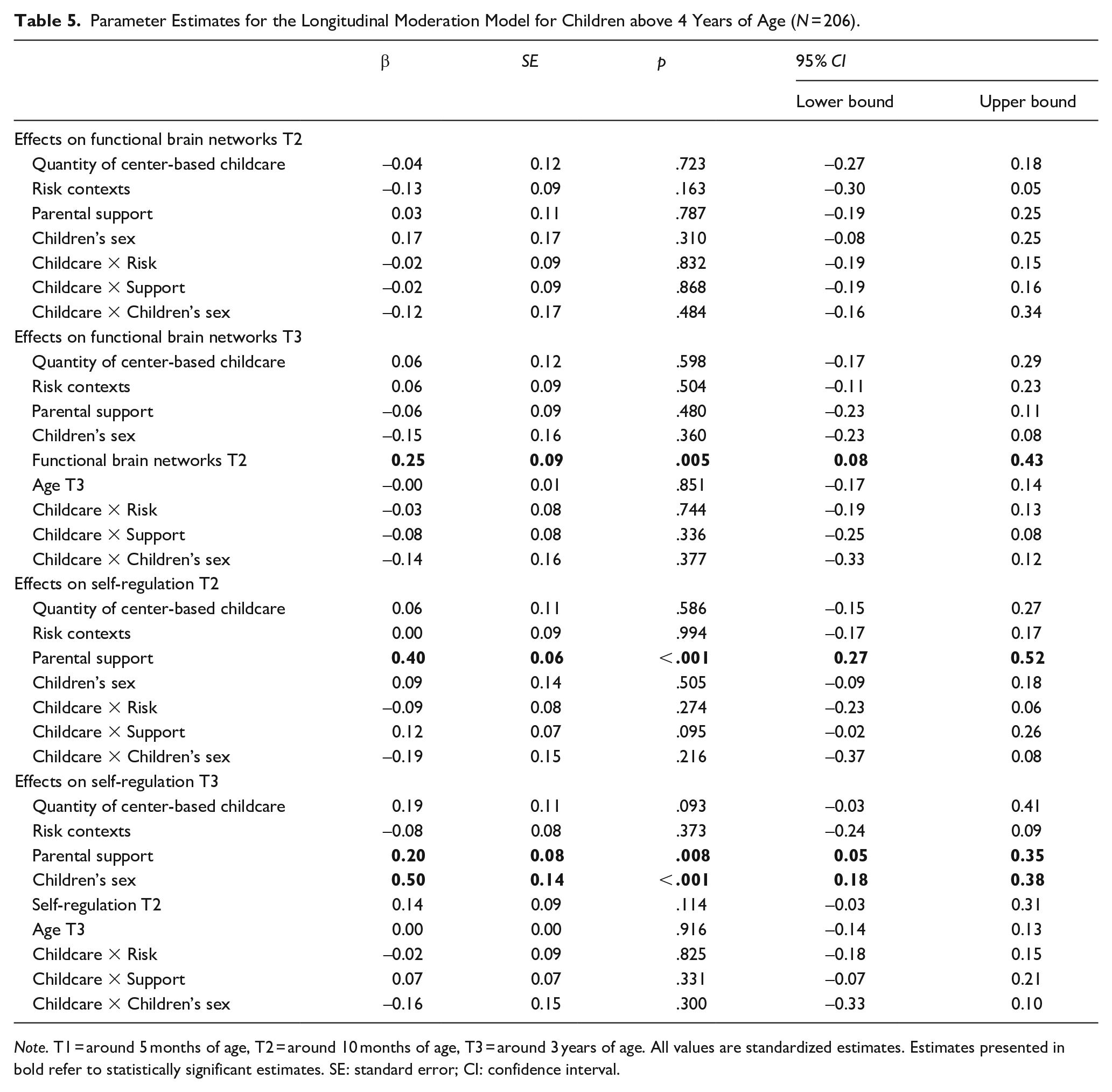
Note. T1 = around 5 months of age, T2 = around 10 months of age, T3 = around 3 years of age. All values are standardized estimates. Estimates presented in bold refer to statistically significant estimates. SE: standard error; CI: confidence interval.
Discussion
As the use of center-based childcare has increased over the past decades (OECD, 2023), so has the attention to the consequences for children’s development. In this study, we examined the relations between quantity of center-based childcare during infancy and variations in functional brain networks and child self-regulation. In line with our hypothesis and previous research (Backer-Grøndahl & Nærde, 2017; Melo et al., 2022; Zysset et al., 2018), this study showed that quantity of center-based childcare during infancy was unrelated to the neurocognitive development of infants around 10 months of age. However, the findings revealed that spending more hours in center-based childcare was related to a greater increase in self-regulation in preschool age children, controlling for self-regulation during infancy. No significant interaction effects were found for exposure to risk, parental support, and children’s sex. Therefore, it appears that the relations between quantity of center-based childcare during infancy and the neurocognitive development of young children do not differ for children from different home environments in a low-risk and high functioning sample, nor for boys and girls. Yet, findings of this study suggest that quantity of center-based childcare during infancy affects self-regulation differently depending on children’s developmental stages.
Center-Based Childcare and Neurocognitive Development in Infants and Preschoolers
The different relations found in infancy (no relationship) and at preschool age (positive relationship) suggest that the positive relation between quantity of center-based care and child self-regulation takes some time to develop and become visible at a later age. High quality center-based childcare settings are characterized by the presence of enriching learning activities and high levels of emotional support from non-parental caregivers (Melhuish et al., 2015). The emergence of self-regulation skills in preschoolers can be positively affected by these early experiences, particularly by supportive and stimulating behaviors of caregivers in the early environment (Bernier et al., 2010; Fay-Stammbach et al., 2014). Here, the more advanced cognitive forms of self-regulation, such as executive functions, typically emerge during the preschool period (Garon et al., 2008; Kopp, 1982). Thus, the positive effect of quantity of center-based childcare on the development of self-regulation in the preschool period may not appear until the age at which more advanced cognitive forms of self-regulation skills have developed over the first years of life.
At the same time, early center-based childcare can represent a rich environment in which young children can practice their social and behavioral skills through interactions with peers and non-parental caregivers, who are likely to encourage following rules and appropriate behaviors (Berger et al., 2021). Given that self-regulation takes some time to develop and continues to rely on such rich environments during early childhood (Fay-Stammbach et al., 2014), the length of attendance in center-based childcare might have played a role as well (Shah et al., 2017). Specifically, a possible explanation for the positive effect of quantity of center-based childcare on the development of self-regulation in the preschool period, but not during infancy, may be that children need a particular “dosage” (e.g., Number of hours × Duration in years) of center-based childcare to experience positive effects on the development of self-regulation (Melo et al., 2022). Therefore, further research should shed light on how quantity of center-based childcare is related to child self-regulation when children attended center-based childcare in different dosages during infancy and the preschool period.
Another explanation for a positive effect of quantity of center-based care on the development of self-regulation in the preschool period, but not during infancy, may be that the positive effects on child self-regulation are a function of greater brain maturation in the first years of life, that comes from exposure to a rich learning environment at an earlier age (Huttenlocher, 2009; Tau & Peterson, 2010). However, despite the importance of environmental experiences in the process of synaptic pruning (Hodel, 2018) and the relations between parenting and functional brain networks found in prior research (Hofstee et al., 2022), this study did not find significant associations between quantity of center-based childcare and individual differences in small-world networks. This indicates that parenting is a stronger and more consistent predictor of children’s brain development than early childcare experiences (Belsky et al., 2007). Yet, small-worldness is only one measure of brain development and further investigation including other brain measures (e.g., power and functional connectivity) is needed to gain more insight in the role of center-based childcare experiences in brain development during infancy and early childhood.
Moderating Effect of Children’s Home Environment
Contrary to our hypotheses, we did not find significant interaction effects for exposure to risk and parental support. However, it should be noted that the current sample consisted of very few children from high-risk families and that mothers in this study generally showed high levels of support toward their children. The lack of variability might result from a combination of convenience sampling and the eligibility criteria, such as proficiency in the Dutch language (Onland-Moret et al., 2020). Moreover, families in rural areas with less accessibility to the lab and adults who are unemployed or from low SES background are less likely to participate in research (Sugden & Moulson, 2015). This might have limited our ability to find significant interaction effects and makes it unclear how well the results generalize to other samples (Jager et al., 2017).
Although children’s home environment was not a significant moderator of the relations between quantity of center-based care and children’s neurocognitive development, its influence is still of crucial importance. Our results showed that maternal support was more strongly related to higher levels of self-regulation than the number of hours per week in center-based childcare. This is in line with previous research, showing that parenting quality was a stronger and more consistent predictor of children’s developmental outcomes (e.g., vocabulary and externalizing behaviors) than quantity of center-based childcare (Belsky, 2006). Importantly, the results of this study also showed a small but significant relation between exposure to risk and maternal support, where exposure to more risk factors in the home environment was related to lower levels of maternal support. Therefore, families from less advantaged home environments may benefit from extra attention and support from non-parental caregivers, as this can promote children’s development (Melhuish et al., 2015).
It might also be that potential negative effects of extensive center-based childcare on children’s neurocognitive development for children from advantaged home environments were attenuated by the compensatory benefits of high quality center-based childcare settings. Some researchers have hypothesized that the potential negative effects of extensive center-based care might only manifest, or be most pronounced, when the quality of the center-based care settings is low (Finch et al., 2015; McCartney et al., 2010). Since 2013, reports of national quality assessments with validated measures have shown a steady increase of process quality of Dutch center-based childcare (Fukkink et al., 2013; Romijn et al., 2023). Therefore, the quality of Dutch center-based childcare might have matched or even exceeded the care that would be provided in children’s home environment, which is shown to foster self-regulation development both in children from advantaged and disadvantaged home environments (Finch et al., 2015; Melo et al., 2022). Yet, more research is needed to further examine the role of the quality of Dutch center-based childcare settings in the relation between quantity of center-based childcare and child self-regulation.
Moderating Effects of Children’s Sex
The relation between quantity of center-based childcare in infancy and variations in children’s neurocognitive development did not differ for boys and girls in this study. A possible explanation for these null findings might be that differential effects of center-based care for boys and girls emerge at a later age than infancy, such as during center-based childcare experiences in the preschool period. For example, during the preschool period, young boys start to show more aggressive behaviors and more rough and physical forms of play, characterized by higher levels of conflict, compared with girls (Endendijk et al., 2017; Votruba-Drzal et al., 2004). The absence of a moderation effect for children’s sex in the association between the quantity of center-based childcare during infancy and child self-regulation may therefore be attributed to the emergence of sex differences in behaviors between boys and girls during the preschool period, and not during infancy.
Notably, self-regulation differences between boys and girls did not emerge either during infancy in this study. This might be due to the emergence of more internalized forms of self-regulation in the preschool period, whereas self-regulation in infants mainly consists of forms of external regulation, as infants cannot yet fully regulate their internal states (Bernier et al., 2010). In line with prior research (Else-Quest et al., 2006; Silverman, 2021), our findings demonstrate that girls show higher levels of self-regulation than boys in the preschool period. Therefore, boys may benefit from extra support and stimulation from non-parental caregivers, to prevent boys for having greater difficulties in regulating their internal states than girls in the preschool period (Ainsworth, 1979; Engel & Gunnar, 2020).
Exploratory Analysis
Previous research demonstrated that children’s experiences with an educational setting and groups in early center-based childcare can play a crucial role in facilitating a smooth transition to elementary school for older preschool age children (Balduzzi et al., 2019; Melhuish et al., 2015). In the Netherlands, children generally enter the kindergarten grades, which are part of Dutch elementary school, around the age of 4. Yet, the results of our exploratory analyses revealed no differences between children under and above 4 years of age in the relation between quantity of center-based childcare and children’s neurocognitive development. As the significant relations between quantity of center-based childcare and variations in child self-regulation in the main analysis lost significance in both subgroups, these null findings might be attributed to less statistical power as a result of smaller subsample sizes in the exploratory analysis. Thus, further research in larger samples of school-aged children is recommended to examine the role of center-based childcare in the transitions to elementary school and the relations with individual differences in self-regulation.
Strengths, Limitations, and Future Directions
This study adds to the limited literature on the relations between quantity of center-based childcare during infancy and variations in children’s functional brain networks and self-regulation. Strengths include the use of a longitudinal design in a large Dutch sample, extending previous research with predominantly US studies. In addition, the longitudinal design allowed for the investigation of variations in functional brain networks and self-regulation and their relationship with the quantity of center-based childcare in different developmental periods. Furthermore, in line with several other studies (e.g., Berry et al., 2014b; NICHD ECCRN, 2003), this study used a cumulative amount of center-based childcare during the first year of life, which may be a more precise measure of infants’ early childcare attendance (Broekhuizen et al., 2017).
However, this study also has some limitations. First, most children came from families with a substantial monthly income and mothers with a high level of education. The relatively advantaged home environments of the children in our sample might limit the generalizability of the results to a broader population. In addition, the homogeneity of our sample may have limited our ability to identify significant interaction effects. Replication of this study in more diverse samples is needed to enhance the generalizability of the findings and to provide a more comprehensive understanding of the effects of quantity of center-based childcare on the neurocognitive development of children from different home environments. For instance, expanding and refining the use of online data collection or home visits, as well as multi-lab collaborations, may positively influence the recruitment of diverse samples (Doebel & Frank, 2023). In addition, recruiter motivation and dedication to gain trust of participants is assumed to increase recruitment of individuals from groups that have traditionally been considered to be hard to recruit (Sugden & Moulson, 2015).
Second, although Dutch childcare is characterized by relatively high quality and high levels of support toward children (Romijn et al., 2023), we could not directly examine the quality of the Dutch center-based childcare settings in this study, as this information was not included in the YOUth cohort study. Previous research demonstrated that the relations between quantity of center-based childcare and child self-regulation are depended on the levels of quality of center-based childcare (Finch et al., 2015; Melo et al., 2022). Thus, future research should take into account the quality of center-based childcare as well, to further elucidate the associations between quantity of center-based childcare and individual differences in children’s neurocognitive development.
Third, given the broad age ranges at T3 and the shift from center-based childcare to elementary school at the age of 4 in the Netherlands, we were unable to take into account the continuity of hours per week in center-based childcare from T2 to T3. Yet, previous research highlights the importance of examining the number of years that children attend center-based childcare during early childhood, beside the number of hours per week (Melo et al., 2022; Shah et al., 2017). Therefore, further research on the consistency in the dosage of center-based childcare, including both the number of hours per week and the number of years of center-based childcare attendance, during infancy and the preschool period is recommended to gain precise insight into the relation of quantity of center-based childcare with children’s development. Here, although a median number of hours in center-based childcare is often used in prior research and seems to reflect the actual quantity of center-based childcare in the Dutch context (e.g., Jacob, 2009; OECD, 2023), an exact measure of the hours spent in center-based childcare is the preferred option.
Finally, this study solely relied on maternal reports of children’s behaviors. Although these parent-reported questionnaires are widely used in the developmental literature (e.g., Putnam et al., 2014; Putnam & Rothbart, 2006), future work should consider supplementing these parent-reported questionnaires with other measures, such as teacher reports of children’s self-regulation in the classroom. This may help to provide a more complete picture of the relations between quantity of center-based childcare and individual differences in child self-regulation, both in the home and classroom environment.
Conclusion
The effects of early and extensive non-parental childcare on children’s development, with a particular emphasis on the negative effects of center-based childcare on socio-emotional development, have been the focus of a long-standing debate over the past three decades (Lamb & Ahnert, 2007). However, findings of this study suggest that quantity of center-based childcare is not negatively associated with self-regulation during infancy. In fact, spending more hours in center-based childcare during infancy promoted the development of self-regulation in preschool age children in a low-risk and high SES sample. More insight into the positive effects of center-based childcare on children’s development can help to encourage a better work–life balance and labor force participation of parents of young children (OECD, 2017). Yet, most importantly, center-based childcare might be an opportunity to invest in positive child outcomes, that may persist into late childhood and beyond (Broekhuizen et al., 2017; Moffitt et al., 2011).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Dutch Ministry of Education, Culture, and Science, and the Netherlands Organization for Scientific Research (NWO): the Gravitation program Consortium on Individual Development (NWO grant number 024.001.003).
Ethical Approval
The research was conducted in accordance with APA ethical standards in the treatment of the study sample. Ethical approval for the YOUth cohort study was provided by the Medical Research Ethics Committee of the University Medical Center Utrecht and informed consent was obtained from both parents at each wave.