
Abstract
This study investigated the relationship between traumatic life stress, trust, and prosocial behavior as a positive mental health outcome in Syrian refugee children in Canada. Trust is a resilience factor shown to promote adjustment after resettlement. The specific goals of the study were to test the influence of refugee children’s traumatic life stress on their prosocial behavior and the mediating role of trust in this link. Five- to 12-year-old Syrian refugee children (N = 124) and their caregivers (N = 51) who recently resettled in Canada participated in this study. Children retrospectively reported their experiences of traumatic life stressors, and caregivers reported their children’s current level of trust and prosocial behavior using questionnaires. Traumatic life stress (e.g., witnessing violence and conflict, separation from family, death of family members) was negatively related to refugee children’s trust in others, while trust was related to more prosocial behaviors, confirming its mediating role. These results suggest that experiencing more traumatic life stressors is associated with less prosocial behaviors as a positive mental health outcome through lower levels of trust. The current findings suggest that fostering trust may be a promising avenue for intervention to promote prosocial behavior and resilience in refugee children who are resettling in a new society.
Amid the largest refugee crisis since World War II, numerous children and families worldwide have been uprooted from their homes and countries every day during the past decade. According to the United Nations Refugee Agency (The UN Refugee Agency, 2023), 108.4 million people have fled and were displaced worldwide by the end of 2022. Forty percent of the refugees are children below 18 years of age, and the largest group is from Syria. Painful experiences of adversity often characterize the displacement experiences of Syrian refugees. For instance, in a recent review of refugee mental health (Scoglio & Salhi, 2020), the prevalence of exposure to violence (e.g., witnessing murder, torture, or combat) ranged from 25% to 93% among adolescents. Also, during displacement, refugees often live in precarious conditions, such as refugee camps and shelters, with limited resources and support from the host country. Researchers have suspected that exposure to adverse experiences is a key risk for refugee youths’ adjustment after resettling in a new country (Eloranta et al., 2017; Panter-Brick et al., 2011).
Meanwhile, scholars have identified individual-level strengths such as prosocial behavior as an antidote for the harmful effects of adversity and a promotive factor for minority children’s sense of well-being, mental health, and positive social relationships (Aydinli-Karakulak et al., 2019; Haroz et al., 2013). However, despite prosocial behavior’s importance as a resilience factor for refugee children, there is a lack of empirical testing on the specific psychological mechanism through which adversity links to prosocial behavior. Although a few previous studies have investigated the mediating mechanisms through which adversity affects prosociality (e.g., Chaitin & Steinberg, 2008; Staub & Vollhardt, 2008), there is very limited research with children and especially in refugee populations. Considering the importance of trust as a psychological foundation for establishing and maintaining prosocial attitudes toward others (Carlo et al., 2010), the present study investigates trust as a potential mechanism linking exposure to traumatic stressors and prosocial behavior in Syrian refugee children who have resettled in Canada.
Displacement Experience, Resettlement, and Mental Health
The displacement experience is a complex process, including the preflight phase in the place of origin, the flight from home and living in transitory placements, and the resettlement phase in a new location or returning home (Lustig et al., 2004). Researchers have identified the displacement experience characterized by uncertainty, chaos, and exposure to war-related stressors as risk factors for mental health problems in refugee children (e.g., Panter-Brick et al., 2011). A systematic review estimated the rates of mental health problems among refugee children and youth as high as 54% for post-traumatic stress disorder and 30% for depression. These rates are higher than those for general children and adolescent populations (for a review, see Bronstein & Montgomery, 2011).
As such, in understanding the mental health issues of refugee children, research (e.g., Betancourt et al., 2016; Eloranta et al., 2017) has predominantly adopted a deficit model (Yaylaci, 2018), which argues that psychopathology arises from an individual’s distress and dysfunction. However, one limitation of this approach is that alleviating mental health problems does not necessarily predict higher life satisfaction or thriving (Suldo & Shaffer, 2008). For instance, Malti (2020) took a humanistic developmental psychopathology perspective and argued that positive mental health, such as prosocial functioning and thriving, are independent of the absence of mental health issues and meaningful outcomes for every child. As such, the antecedents of such positive thriving factors must be better understood and targeted in prevention and intervention efforts. Furthermore, our understanding of resilience—the ability to overcome adversity and achieve positive outcomes despite exposure (Rutter, 2012) also illustrates the pivotal role of protective factors that mitigate the negative effects of adversity. For instance, with similar levels of exposure to devastating war experiences, some children show more healthy psychological functioning compared with their peers (Pacione et al., 2013). Moreover, adaptation to trauma is a dynamic process involving multiple systems within and surrounding the individual, and vulnerability factors as well as promotive and protective factors moderate or mediate the effects of adversities on children’s adjustment (Masten & Narayan, 2012). In line with these ideas, scholars have emphasized the importance of adopting a positive developmental perspective in understanding mental health challenges within an ecological system among refugee populations (e.g., Frounfelker et al., 2020; Yaylaci, 2018).
Prosocial Behavior and Adjustment
Children’s prosocial development is a crucial mental health outcome in fostering resilience in refugee children and adolescents since prosociality is a consistent marker for positive development (Bell et al., 2013; Griese & Buhs, 2014). Developmentally, prosocial behavior is vital in promoting a personal sense of well-being, social cohesion, and inclusion. For example, empirical evidence has shown that peers prefer those who are highly prosocial (Caprara et al., 2000) and prosocial behaviors play a crucial role in creating high-quality friendships and affectionate behaviors toward friends (Markiewicz et al., 2001). In addition, children’s prosociality has been associated with better academic achievement (Caprara et al., 2000) and positive social and behavioral self-perception (Chung-Hall & Chen, 2010).
Although sparse, some research suggests a link between prosociality and better adjustment in refugees. For instance, war-exposed refugee adolescents who reported higher prosocial behaviors during displacement were more likely to report improvements in anxiety symptoms 6 months later (Haroz et al., 2013). Similarly, school-age refugee children in Sweden showed better adjustment with fewer mental health difficulties when they displayed more prosocial behaviors (Daud et al., 2008). Besides the positive implications for children and adolescents’ mental health, some studies suggest that refugees’ prosocial behaviors may improve nonrefugee attitudes toward refugees. For example, a neuroimaging study with adults found that empathy toward outgroup members (e.g., refugees) increased when people learned that they had received help from an outgroup member (Hein et al., 2016).
These findings collectively point to the possibility that refugee children’s prosocial behaviors may help their social–emotional adjustment and improve the inclusive ethos of reception among nonrefugee children in the host country. However, few studies have addressed the importance of prosocial behavior as a positive mental health outcome or considered it a target of intervention (e.g., Ehntholt et al., 2005).
Exposure to Traumatic Stress and Prosocial Behavior
It is important to consider traumatic stressors in understanding the development of prosocial behaviors in refugee children. Stress comprises events that are positive or negative and traumatic or nontraumatic (Willard et al., 2016). Meanwhile, DSM-5 specifies that “exposure to actual or threatened death, serious injury or sexual violence” (DSM-5 A criteria; American Psychiatric Association, 2013, p. 271) is a clinical requirement for diagnosing post-traumatic stress disorder (PTSD). Therefore, based on these criteria, we can categorize the exposure to war and violence experienced by refugee children as traumatic life stress.
While scholars have linked traumatic life stress to increased aggression (Kitzmann et al., 2003), the research findings on prosocial behaviors remain inconsistent. The perspective of “altruism born of suffering” emphasizes that traumatic life experiences boost prosocial behaviors due to post-traumatic growth (Staub & Vollhardt, 2008). However, Chaitin and Steinberg (2008) argue that individuals exposed to massive traumatization, such as war, have difficulties connecting to others’ suffering and empathizing with them. These characteristics may contribute to low levels of prosocial behavior. Notably, in a sample of children and adolescents, early war-related life stress temporarily increased prosocial behaviors among in-group members but not toward outgroup members and did not transfer to later prosocial behaviors in the long term (Bauer et al., 2016). There is also evidence that children who experience early adversity, such as domestic violence, are more likely to experience delays in prosocial development (Mejia et al., 2006). The idea that chronic stress leads to self-focused avoidant behaviors rather than other-oriented prosocial behaviors might explain the negative association between war-related stress and prosocial behavior or the lack thereof (Eisenberg et al., 2014).
However, Syrian refugee children generally experience much higher levels of traumatic life stressors than community samples, associated with higher PTSD symptoms (Macksoud & Aber, 1996). Thus, we focus on the effects of experiencing traumatic stress caused by stressors such as witnessing interpersonal violence or family loss and separation that are common during a war. War-related traumas tend to be interpersonal and can be more destructive as they include intentional attacks by another person and the loss of connections to significant others. These experiences shape one’s view of safety, intimacy, and trustworthiness (Janoff-Bulman, 1992). Understanding whether and how traumatic life stress negatively affects prosocial development will contribute to finding ways to promote refugee children’s prosocial behaviors.
The Role of Trust in the Traumatic Life Stress-Prosocial Behavior Link
One promising mechanism underlying the relationship between traumatic life stress and prosocial behaviors is one’s sense of trust. Trust is the generalized expectation that another individual can be consistently relied upon and that they are honest (Rotenberg, 2010). Developmental psychology has stressed the importance of trust for a long time. For example, psychosocial theory (Erikson, 1963) argues that establishing trust versus mistrust is the basic developmental task in early childhood for building healthy interpersonal relationships and for children’s social–emotional adjustment across their lifespan. In addition, empirical evidence has shown that children with high trust are more helpful to classmates and have better peer relationships (Rotenberg, 2010). Similarly, researchers found an association between higher trust and a higher likelihood of expressed prosociality while controlling for other social–emotional factors (e.g., sympathy) during early to middle childhood (Song et al., 2018). However, despite the role of trust in positive outcomes, there is scant research on adjustment outcomes related to trust in the refugee literature (e.g., Eide et al., 2018).
Trust and mistrust have been identified as key themes as refugees go through the entire process of becoming a refugee even prior to arriving in the host country in refugee camps (Hynes, 2003). Refugees often leave their country of origin to escape war and persecution, and such a dire environment and unpredictability may contribute to a sense of mistrust (Majumder et al., 2015; Ní Raghallaigh, 2014). Also, the degrees of violence and conflict that they experienced in the displacement process can negatively affect refugees’ ability to trust others (Daniel & Knudsen, 1995). This is not surprising given that experiencing trauma characterized by betrayal in social relationships can disrupt one’s ability to detect the trustworthiness of others, which may result in a lower sense of relational trust (Gobin & Freyd, 2014). According to a review on trust of refugees (Essex et al., 2022), it seems that trust and mistrust are main issues among refugees regardless of nationality, cultural backgrounds, and countries where they resettled. In addition, there is evidence of a positive association between trust and prosocial behavior (Carlo et al., 2010; Song et al., 2018). Here we study the role of trust in refugee children’s development of prosociality concerning their traumatic life stress.
Current Study
The general aim of this study is to examine the relationship between traumatic life stress and prosocial behaviors in Syrian refugee children resettling in Canada. Specifically, we asked whether (1) experiencing traumatic life stress has a direct effect on lower prosocial behavior and (2) whether traumatic life stress has an indirect effect on prosociality via trust. We examine these questions in Syrian refugee children between ages 5 and 12 because early to middle childhood is the critical period to extend trust and prosocial behaviors from family members toward nonfamilial targets (Abrams et al., 2015; Eisenberg et al., 2006; Rotenberg, 2010). Moreover, childhood traumatic stress is a potent risk factor for developing serious long-term mental health problems (Chapman et al., 2004).
Method
Participants
Participants included 124 five- to 12-year-old Syrian refugee children (51.6% female, Mage = 8.99 years, SD = 2.26) and their primary caregivers (N = 51) resettling in an urban area of Canada within the past two-and-one-half years. The average number of children was 2.43 per family (range = 1–5). We invited participants to engage through community events (e.g., mosque events or Saturday school) and schools. Settlement workers provided a brief explanation, and our research team contacted families who expressed interest in participating in the study. For data collection, our research team visited participants’ homes or the mosque, depending on each family’s preference. The median education level of parents was middle school for fathers (33.1% elementary school, 24.6% middle school, 14.4% high school, 6.8% college, and 21.2% university) and mothers (40% elementary school, 20.9% middle school, 12.2% high school, 7% college, and 20% university). On average, participants and their families had lived in Canada for 14.35 months.
Procedure
This study was part of an ongoing longitudinal study on Syrian refugee children’s social–emotional development and mental health after resettlement; the research ethics board at the University of Toronto approved this study (protocol reference #33501). Before participating in the research, caregivers provided verbal assent (for illiterate caregivers) or written consent (for literate caregivers), and children agreed verbally. Well-trained research assistants who were bilingual speakers of English and Arabic conducted the interviews. Bilingual research assistants and primary investigators translated questionnaires to Arabic from English and back-translated them to English. The researchers interviewed all caregivers and most children in Arabic based on their preferences. The interview using questionnaires including a retrospective measure of life stress took approximately 1 hr for caregivers and 50 min for children at the families’ preferred locations, either at their homes or at a mosque. After the interview, we gave the caregivers a gift card and small treats (e.g., a small toy) to the children after debriefing.
Measures
Prosocial Behaviors
Caregivers reported on children’s prosocial behavior using the five-item prosocial behavior subscale of the Strength and Difficulties Questionnaire (SDQ, Goodman, 1997; for example, “Helpful if someone is hurt, upset, or feeling ill”). Caregivers reported on a four-point Likert-type scale (0 = Not at all true, 3 = Almost always true). Higher scores imply that parents reported their children as more prosocial. This scale is a well-validated measure used for different age groups and ethnicities (e.g., Hemdi & Daley, 2017). Cronbach’s α of prosocial behavior was .62.
Traumatic Life Stress
We measured children’s life stress experiences using selected Traumatic Stress Questionnaire items (Bean et al., 2006). We chose five items that describe stressful life events that may be particularly relevant to the refugee experience. Children responded dichotomously to each item describing different life events to indicate whether they had happened in the past (e.g., “Have you been separated from your family?”). We used the sum score of this scale for this study because the responses were binary (Yes = 1 or No = 0). Higher scores mean that participants had experienced more traumatic life-stress events.
Trust
Caregivers reported children’s level of trust using the Holistic Student Assessment (HSA, Malti et al., 2018). Among seven subscales of the HSA, we only used the trust scale (three items, e.g., “Trusts other people”) for this study. Caregivers responded on a four-point Likert-type scale (0 = Not at all true, 3 = Almost always true). Higher scores indicate that parents reported their children as more trusting and thus showed a higher level of trust. Cronbach’s α of the trust scale was .68.
Data Analysis Strategy
First, we used SPSS 26 to examine the descriptive statistics, correlation, and independent t-test for gender differences. Next, we tested the direct effect of life stress on prosocial behavior and the mediating effect of trust in the link between life stress and prosocial behavior in a path analysis with Mplus 8.4, using maximum likelihood estimation. Model fits were evaluated based on multiple indices together (i.e.,
Results
Descriptive Statistics
As shown in Table 1, there is a negative correlation between traumatic life stress, prosocial behavior, and trust. As expected, trust and prosocial behavior were positively correlated. Traumatic life stress, however, was negatively related to trust and prosocial behavior. We conducted an independent t-test to test the mean differences by gender. The results indicated that although there was no significant difference in traumatic life stress and trust, girls showed significantly higher prosocial behavior levels than boys. Also, older children were more prosocial than younger children. We analyzed the percentages of each life stressor to examine the frequencies of specific types of traumatic life stressors that children experienced. As shown in Figure 1, more than half of our sample reported experiencing separation from their family (55.6%) and witnessing physical violence (56.4%). Less common traumatic life stressors were the death of a close family member (26.3%) and personal injury or illness (13.3%). The least common stressor was the death of a friend (3%). Approximately half of our participants (49.5%) experienced two types of traumatic life stressors, and 17.2% reported that they experienced at least one of them.
Descriptive Statistics and Bivariate Correlations Between Study Variables.
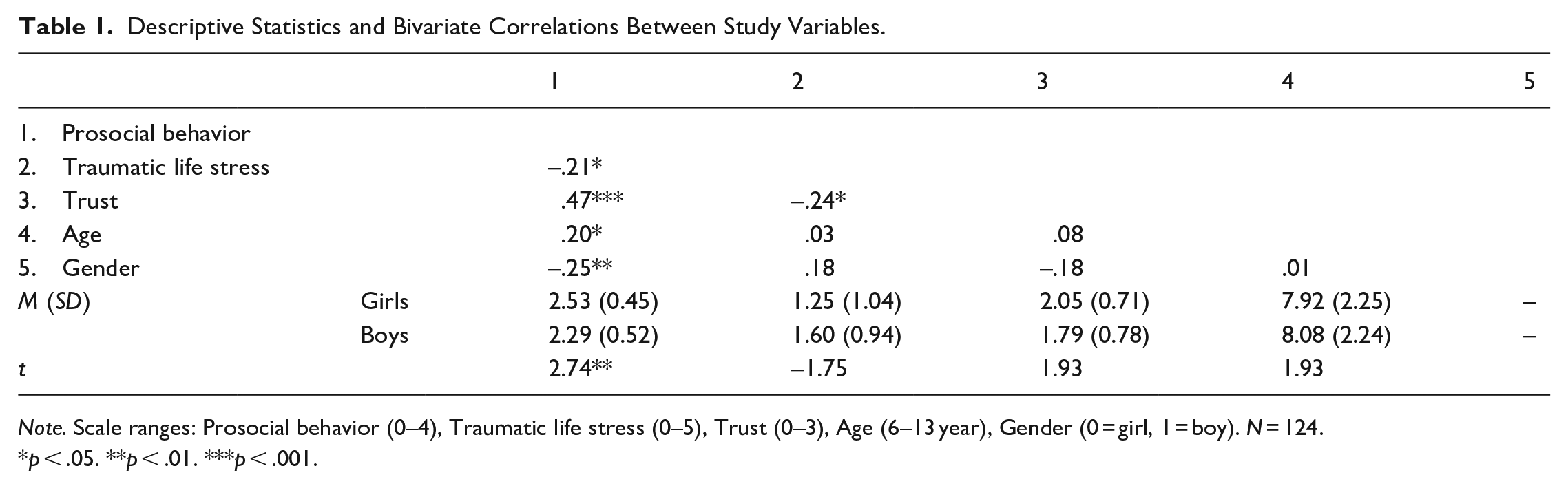
Note. Scale ranges: Prosocial behavior (0–4), Traumatic life stress (0–5), Trust (0–3), Age (6–13 year), Gender (0 = girl, 1 = boy). N = 124.
p < .05. **p < .01. ***p < .001.
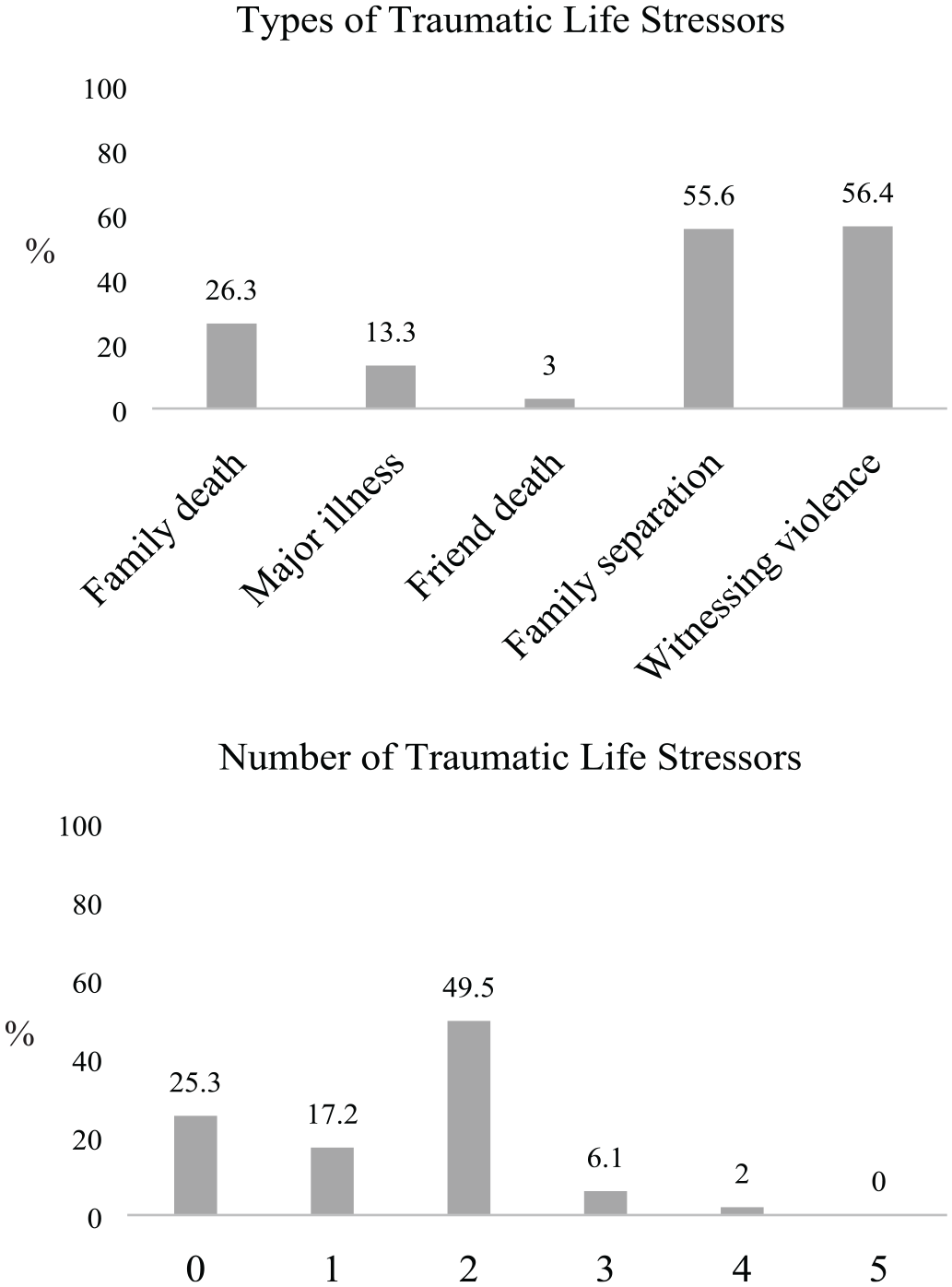
Percentages of Children Who Experienced Traumatic Life Stressors by Type and Number (N = 124). The Five Stressors Were Chosen From the Traumatic Stress Questionnaire.
Trust as a Mediator of the Link Between Traumatic Life Stress–Prosocial Behavior
To test the direct effect of traumatic life stress on prosocial behavior, and to understand the mechanism underlying the link between traumatic life stress and prosocial behavior among Syrian refugee children, we tested a simple mediation model using path analysis. Our research model had an acceptable fit to the data,
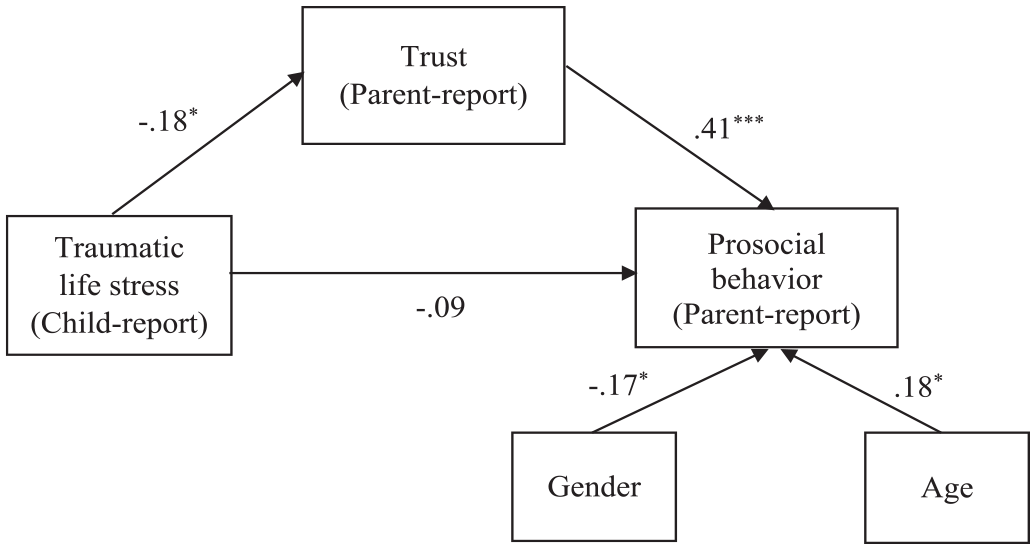
A Path Model Examining the Mediating Effect of Trust in the Link Between Traumatic Life Stress and Prosocial Behavior (N = 124).
The direct effect of traumatic life stress on prosocial behavior was not significant. However, we found a negative relationship between traumatic life stress and trust, and in turn, trust was positively related to prosocial behavior. As expected, the indirect effect of traumatic life stress on prosocial behavior through trust was significant (b = −.05, 95% CI = [−.111, −.005]). These results suggest an association between experiencing more traumatic life stressors and less prosocial behaviors through lower levels of trust. The moderated mediation analyses with child age as a moderator yielded a poor model fit or an insignificant moderating effect.
Discussion
This study focused on children’s prosocial behavior as a positive mental health outcome for Syrian refugee children’s successful resettlement. Unlike most studies focusing on refugee children’s mental health problems and deficits, this study contributes to the relatively limited literature on refugee children’s resilience and thriving. The aim of this study was twofold: First, to investigate the effect of traumatic stress on prosocial behaviors, and second, to examine the role of trust in the link between life stress and prosocial behaviors.
We found a link between traumatic life stress and lower prosocial behavior, but the link disappeared when we considered trust. This result implies that the link between traumatic life stress and low levels of prosocial behavior is not robust. Previous research on Syrian refugee children in Turkey also found that compared with nonrefugee children, refugee children reported similar levels of prosocial behaviors despite having increased psychological and behavioral difficulties (Alsayed & Wildes, 2018). Other evidence has shown no relation between war-related trauma and prosocial behaviors in Palestinian children and adolescents in the Gaza Strip (El-Khodary & Samara, 2019). However, as illustrated in the concept of “altruism born of suffering,” some research has reported increased prosocial behaviors and altruism after traumatic stress (Staub & Vollhardt, 2008). These inconsistent results imply refugee children’s potential resilience in facing trauma, especially given that many children, including our participants, reported witnessing violence or separation from a family member, both events closely related to children’s engagement in social interactions. Therefore, it was essential to illuminate the psychological mechanisms underlying the influences of traumatic stress on prosocial behavior, such as trust.
As predicted, traumatic life stress (e.g., witnessing violence and conflict, separation from family, death of family members) was inversely related to refugee children’s trust in others, while trust was related to more prosocial behaviors. That is, low trust mediated the link between higher traumatic life stress and lower prosocial behaviors. A study with Syrian refugee children (Özer et al., 2013) found that the loss of a family member or loved one (74%) was the most commonly experienced stressor, and 60% of Syrian refugee children reported that their lives were in danger, suggesting that traumatic life events are not uncommon in refugee families. Indeed, of the children who participated in our study, more than half reported experiencing interpersonal traumatic stressors such as witnessing violence or separation from a family member, and more than a quarter had lost a family member. Moreover, among the five types of traumatic events we investigated, more than half of our sample reported experiencing at least two. Our findings expand on existing literature (e.g., Janoff-Bulman, 1992; Wu et al., 2020) on the link between traumatic life stress and trust in refugee and nonrefugee samples. These findings corroborate the idea that adverse life events, such as witnessing violence and being separated from family, could contribute to lower trust in refugee children since trust is an emotion which children develop through daily social interactions (e.g., Daniel & Knudsen, 1995).
A refugee family’s journey, including experiencing a temporary campground, frequent displacement, an unsafe environment, and suspicion directed toward refugee populations, may erode children’s trust in other people, the community, and the world (e.g., Lyytinen, 2017). From a developmental perspective, children can judge another person as reliable or unreliable by age 5 (Vanderbilt et al., 2011). However, losing family members who sometimes are their attachment figures and experiencing adversities can increase children’s uncertainties in life. Also, unlike losing family members due to a natural disaster, the death of loved ones due to violence increases the possibility of PTSD and long-term depression (Kaltman & Bonanno, 2003). These mental health difficulties are a factor that interferes with building trusting relationships as well as maintaining healthy psychological functioning (Nickerson et al., 2014).
Moreover, such contexts involve many serious interpersonal conflicts, which can increase children’s sensitivity to interpersonal threats. Therefore, children would not be able to learn that the world is secure and that other people are reliable, which would interfere with building trustful relationships.
It is not only the processes of becoming a refugee that affect refugees’ trust or mistrust but also how refugees are being perceived and treated by others in the new environment. The social milieu in the host country where Syrian families are resettling are affected by multiple layers of ecological systems including the country’s political and cultural climates, which vary at national and regional levels. Considering our sample, at the macro-level, Canada is considered as one of the countries with the most inclusive refugee policy and the government has been implementing multiculturalism-related policies (Costigan et al., 2010). As a consequence, Canada might be more tolerant of outgroup members and willing to participate in multicultural education (Maharaj & Connolly, 1994), which, in turn, has positive influences on refugee families’ impressions of the host country. Although Canada is well-positioned to support Syrian refugee children as one of the advanced countries that welcomed a large number of refugees, there are still preexisting racialized prejudices that shape how others perceive and behave toward refugee families (Matthews, 2008; Walker & Zuberi, 2020). In a qualitative study in Winnipeg, interviewing refugee students, racism and discrimination were found as ongoing challenges for refugee students, whether actual or perceived (Stewart, 2011). Therefore, researchers and interventionists should keep in mind that even highly inclusive countries may not be completely free of biases against refugees who are a visible minority.
Experiencing discrimination as a visible minority may hinder refugee children to build trust in the new society and further exacerbate existing trauma symptoms. Opportunities for active and safe interactions between refugees and original members of the host country might reduce intergroup discrimination, while boosting intergroup trust. However, Syrian refugee adults found that they favored in-group members compared with outgroup members (El-Bialy et al., 2022). Such an attitude may be helpful for promoting in-group coherence, but an extreme preference for in-group members might hinder their integration into the host society. To avoid this potential separation from the society, refugee families would need to be provided with sufficient opportunities to build trust toward the new society through interactions with the local community. Based on a case of Norway, Vårheim (2014) suggests the idea of utilizing local libraries to provide various programs for refugee families to participate. As a targeted intervention for trust, using a social game with peers in which children can learn when and how much to trust others could be a possible intervention to foster optimal trust (Song et al., 2020). Such community-based interventions can provide a structured environment that is accessible for everyone, where refugees and nonrefugees can informally interact, and build intimate intergroup trust.
Trust was positively related to prosocial behaviors in Syrian refugee children even after controlling for the effects of gender and age. Consistent with the literature, older children and girls were more likely to engage in prosocial behaviors. Trustful children are more prone to interpret the distress or suffering of others as genuine (Carlo et al., 2010), which may encourage them to engage in prosocial behaviors. Similarly, to protect themselves from additional harm, refugee children who have lower trust toward others might exercise more caution in contexts where they have options to help others. Therefore, continuous exposure to traumatic events may contribute to Syrian refugee children’s lower levels of trust, decreasing the chance of helping others.
Indeed, trust mediated the link between traumatic life events and prosocial behavior. Refugee children’s experiences of being separated from their parents or losing loved ones might interrupt their development of reliable and trustworthy internal representations of others. In a study with Syrian refugees (Halasa et al., 2020), children and adolescents reported the highest levels of social anxiety (e.g., “I worry about what others say about me,” “I feel nervous when I am around certain people”) compared with other anxiety symptoms, implying that they may have negative internal schemas about interpersonal relationships. Secure relationships with parents and parental support may prevent the development of negative social schemas. However, even if children are still living with their parents, parents are also traumatized by war experiences, which may limit their emotional availability to support their children’s distress regulation. For example, Thabet and colleagues (2008), most refugee parents showed high levels of PTSD. They found a relationship between the parents’ poor emotional responses to their children and their children’s PTSD and anxiety.
Considering refugee parents’ own challenges, the role of community becomes more important. Promoting a sense of safety, a sense of self- and collective efficacy, connectedness, and hope are important targets to consider as broad intervention principles for helping refugees overcome trauma (Hobfoll et al., 2007). To target these goals, schools and local communities could play crucial roles in promoting adaptation among refugee families. Academic achievements, valuing education, and experiencing positive school life have been identified as important predictors of newcomer children’s adjustment (Drury & Williams, 2012; Montgomery, 2010). Also, middle Eastern refugees who were living in Denmark adjusted better over time (Montgomery, 2010) and overcame their trauma from war and terrorism better if they perceived school as a safe place (Masten & Narayan, 2012). Schools are where refugee children spend most of their time on a daily basis, and thus they can provide a stabilizing space for the sense of safety and inclusion and intellectual growth (Matthews, 2008). Moreover, teacher preparedness (e.g., inclusive and culturally competent teaching techniques for classroom instruction), mental health services will help meet the unique needs of refugee students (Walker & Zuberi, 2020). Therefore, making a school a safe place for refugee children may be the important first step for intervention. To foster children’s school adjustment, both micro-level interventions as well as macro-level campaigns to improve deeper understanding and inclusive social climate among the members of the society will be important.
Interventions should consider how best to support refugee children’s resilience at multiple levels to protect from psychological trauma. Previous research on intervention programs for refugee children report that tiered programs have been successful for increasing community engagement, reducing stigma, and providing help to children, which were also cost effective (Rousseau et al., 2013). For example, a Canadian program implemented a tiered program including community health clinics for providing psychosocial support for refugee children and families, while providing culturally adapted community based mental health treatment for children who are in need of more significant psychiatric care. A school program in Canada used artistic expression techniques to help refugee children explore the meaning of hope, which increased children’s hopefulness as well as positively affecting hopefulness in children’s families and refugee community as children shared their hope projects with others (Yohani, 2008). These systems (i.e., schools and communities) are perceived to be fundamental for affording resilience capacity as they appear to promote a sense of safety and connectedness, perceived agency, and optimistic thinking in facing threats and disturbances in life of refugee families (Masten & Narayan, 2012).
Meanwhile, we did not find any developmental differences among early and middle childhood refugee children in the associations between traumatic stress, trust, and prosocial behaviors, despite the expected age differences in the levels of prosocial behavior. These findings suggest that the mechanism through which traumatic stress affects the development of trust and prosocial behaviors may be consistent throughout childhood. Alternatively, the methods we used to assess children’s level of trust and prosocial behavior may not have been sensitive enough to capture developmental variations because they were all caregiver reports.
The uniqueness of the results of this study might need to be interpreted while considering some relevant characteristics of the sample. For the present study we only included children who were from intact families to control for family composition. Thus, our findings may not be applicable to other family structures such as unaccompanied refugee minors. In a case study of unaccompanied refugee minors who are resettling in the United States, Carlson and colleagues (2012) found that cultural identity, religiosity, school performance, and reasonably well-functioning families before emigration were key buffering factors for overcoming their trauma. Also, beliefs and faith might have functioned as a protective factor in our sample of Syrian refugee families, which might have moderated families’ interaction with trauma and resettling experiences (Masten & Narayan, 2012).
This study is not without limitations. First, we relied on caregivers’ reports for children’s trust and prosocial behaviors. We made this decision based on the notion that when children are traumatized, parents may be a more reliable source of information for their children’s changes in behavior, mood, and overall functioning (El-Khani et al., 2016). In future studies, first, researchers might benefit from considering self-reported trust to gauge children’s internal emotional states and beliefs. Second, the concurrent measurement of the mediator and the dependent variable–mothers reported their children’s trust and prosocial behavior concurrently, which limits the directionality of the relation between the two variables. Using a longitudinal design will be important to confirm the role of trust as a mediating mechanism. Third, focusing on more specific types of trust and targets of prosocial behaviors would be valuable for delving into the inner world of refugee children. Fourth, examining post-migratory contextual factors (e.g., parenting, peer relationships) in conjunction with children’s social–emotional and social–cognitive characteristics would be important for understanding their overall adjustment after resettlement. Finally, it would be important to examine developmental specificity of the current findings by investigating different age groups such as refugee adolescents. Developmental timing of exposure to adversity can have important implications for future adaptation, and older youth may be more protected in one way but more vulnerable in another way due to their cognitive maturity and awareness compared with younger children (Masten & Narayan, 2012).
Despite its limitations, this study provides evidence for the role of trust in children’s prosocial behaviors in the context of exposure to war-related trauma. Our results add to the literature by proposing that traumatic life stress impacts prosocial behaviors in refugee children through their psychological process of trusting others. Interventions that focus on building trust among traumatized children who are neglected and separated from their families also indicate that safe and predictable relationships and environments can provide opportunities for children to learn to engage in trust-based behaviors (Knight et al., 2004; Purvis et al., 2013). These results suggest that a promising avenue of intervention involves promoting refugee children’s abilities to trust others in mitigating the ill effects of traumatic life stress and nurturing positive mental health and thriving. In addition, those working with refugee children should consider creating reliable and stable relationships, which is an important goal. For instance, a qualitative study of refugee children and adolescents showed that having older adults in a community who supported and encouraged them to learn effective coping strategies and have hopes for the future immensely helped them deal with their parents’ loss (Luster et al., 2009). Moreover, evidence suggests that trust supports refugee children to effectively manage conflicts in relationships, establish reliable interactions, and recover from trauma regardless of cultures (e.g., Bermudez et al., 2018; Chouliara et al., 2017). Thus, even if refugee children develop mistrust due to traumatic life stress, they may be able to recover their impaired trust through healthy relationships during the resettlement process if given opportunities to rebuild and maintain trusting relationships.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Grant #1920-HQ-0001151920-HQ-000115 from the Public Health Agency of Canada (PHAC) to the third author, and the 2022 research grant of Yonsei University (2022-22-0298) to the corresponding author.