
Abstract
Media use and screen time show both positive and negative effects on child development. Parents’ behaviors, perceptions, and regulation of parent and child screen-based device (SBD) use may be critical understudied factors in explaining these mixed effects. We developed the Parent Screen-Based Device Use Survey (PSUS) to assess parental use of multiple SBDs (e.g., computers, phones, and TVs) and tested its factor structure across two United States samples of mothers of children aged 2–6 years (total N = 402). Subscales captured parental SBD use related to Discipline, Limit-Setting, Involvement, Child Care, Family Norms, Self-Regulation, Dysregulation, and Parenting Support, and showed good factor loadings and internal reliability. Validity was tested in relation to parent distress, parent executive function problems, and child behavior problems. Parental limit-setting and involvement were either unrelated to or related to fewer parent and child problems, whereas parental use of SBDs for self-regulation, child care, discipline, support, and family activities, as well as parents’ more dysregulated use, were related to more parent and child problems. The PSUS holds promise in addressing the parental mechanisms that underlie media effects on child development.
Media use and screen time are now normative components of family life with young children. Accordingly, there is a critical need to understand the effects of the use of screen-based devices (SBDs; e.g., TV, tablets, computers, and smartphones) on child development (Elias & Sulkin, 2019). These effects may hold particular influence in early childhood as this is a critical period for neurological and behavioral development and the period in which family rules and routines surrounding media use are first established (Coyne et al., 2017). However, findings on SBD use are inconsistent, with some studies suggesting that SBD use relates to higher parent stress and poorer child behavioral and health outcomes (Golen & Ventura, 2015; Li et al., 2020), whereas others report associations with positive child outcomes (e.g., language development and prosocial behavior; Ostrov et al., 2006) for certain types (e.g., educational programs) and amounts of SBD use (Linebarger & Walker, 2005; Madigan et al., 2020).
Prior mixed findings may be due to a relative lack of attention to parent factors that drive the quantity and quality of child SBD use. We propose that a parent self-regulation perspective could help reveal parental mechanisms underlying SBD use and its effects on child development. In early childhood, parents act as external regulators of children’s emotions and behaviors when children have not yet developed the skills to regulate independently (Vohs & Baumeister, 2004). Parents must also regulate their own emotions and behaviors in response to parenting and child behavior, which can be very challenging (Lunkenheimer et al., 2023). Accordingly, parents may use SBDs as one potential tool with which to regulate themselves and their children, making it crucial to understand how parental self-regulation affects behaviors around SBD use.
To study these processes, new measures may be needed to target parents’ behaviors, perceptions, and regulation of their own and their children’s SBD use (Barr et al., 2010; Coyne et al., 2017). Accordingly, we developed a new, brief measure, the Parent Screen-Based Device Use Survey (PSUS), to assess parents’ regulation of their own SBD use, regulation of and involvement with their children’s use, and use of SBDs as a parenting tool. This measure addresses use of all SBDs and is not limited to one form of media. In this article, we first review parent and child SBD use and address potential parental mechanisms underlying SBD use. Subsequently, we examine the reliability and factor structure of the PSUS as well as its validity via relations with parent and child regulatory functioning, namely, parent distress, parent executive function problems, and children’s behavior problems.
Effects of Children’s SBD Use on Child Development
SBD use may have important implications for child development, especially in sensitive neurobiological stages such as early childhood. Family rules and routines around SBD use are often introduced in early childhood (Coyne et al., 2017) when young children rely on parents for regulation and socialization of developmentally appropriate activities. Furthermore, it is important to understand the impact of SBD use on children given increase in SBD use over the past several decades (Chen & Adler, 2019). Some studies find specific types of SBD use have positive implications for children’s learning outcomes (Barr et al., 2010), prosocial behavior (Ostrov et al., 2006) and language development (Linebarger & Walker, 2005). For example, apps designed to enhance children’s cognitive abilities are associated with positive learning outcomes (Barr et al., 2010). Thus, outcomes may vary by the type of content engaged with and frequency of use.
However, a greater number of studies suggest negative effects of SBD use. The displacement hypothesis posits that time spent engaging with SBDs detracts from other activities that support development, resulting in less positive outcomes (Pagani et al., 2010). Greater childhood SBD use has been associated with poorer health (Li et al., 2020), behavioral (Tamana et al., 2019), and language outcomes (Madigan et al., 2020). Moreover, more SBD use is associated with higher internalizing and externalizing problems, particularly in young children (Tamana et al., 2019), which reflect emotional and behavioral dysregulation and predict longer-term mental health problems (Arslan et al., 2021). Thus, understanding the effects of child SBD use may inform etiology and intervention related to child mental health.
SBD Use in the Context of Parenting
Parents utilize SBDs in numerous ways, including managing children’s screen use (Gentile et al., 2014), engaging in SBD use with children (Sekarasih, 2016), and involving SBDs in discipline (Samaha & Hawi, 2017). In addition, parents employ SBDs to help regulate themselves and manage their own stress (McDaniel & Radesky, 2018). Here, we review some of the primary reasons parents use SBDs, arguing that these functions should be considered in light of prior mixed findings on the impacts of SBD use on child development.
Family Norms Around SBD Use
Parents establish and maintain family norms and rules for children regarding SBD use, reflected in daily family media routines and the total time families engage with screens (Padilla-Walker et al., 2012). SBDs have become commonplace, with families reporting an average of five internet-connected SBDs in the household (Pew Research Center, 2017). One study estimated that more than half of families had the TV on during dinnertime (Jordan et al., 2006); another found that 70% of families watched TV or a movie together at least once a week (Padilla-Walker et al., 2012). Furthermore, family SBD usage appears to be increasing over time (Chen & Adler, 2019). In all, evidence suggests that SBDs are involved in family routines and may be frequently used during time spent together as a family.
Monitoring and Limiting Children’s Screen Time
Parents play a major role in managing children’s SBD use, especially in early and middle childhood, with declining influence in adolescence (Nikken & Jansz, 2006). Types of parental monitoring include active mediation (direct and indirect conversations about the content and intent of media) and restrictive monitoring (rules regarding frequency of SBD use and content; Gentile et al., 2014). Evidence suggests both types of monitoring mitigate negative outcomes in young children (Blum-Ross & Livingstone, 2016). Also, higher monitoring of SBD use is associated with less aggression in children (Collier et al., 2016), with one study finding that evaluative mediation related to aggression (e.g., negative evaluations of violent characters) may be protective for children (Nathanson, 2004).
Discipline, Caregiving, and Parent Involvement
In addition to managing children’s SBD use, parents use screen time as a disciplinary tool, a caregiver, and to promote interaction with their child (He et al., 2005; Padilla-Walker et al., 2012; Sekarasih, 2016). In one study, roughly 70% of families endorsed prohibiting SBD use as a discipline strategy and families were more likely to do so when children’s SBD use was higher on average (Samaha & Hawi, 2017). The use of SBDs as caregivers or “babysitters,” particularly for young children, is also common, with 65% of parents allowing young children to use SBDs to keep quiet in public places and 28% using SBDs to help children fall asleep (Kabali et al., 2015). Parents also report that co-use of SBDs with their children accounts for as much as one third of children’s SBD time (Christakis, 2014). Overall, these rates underscore the need for more scientific attention on SBD use as a parenting tool and its relation to child outcomes.
Parents’ Own SBD Use During Parent–Child Interactions
Parents’ own SBD use influences children through behavior modeling and by impacting or interfering with parent–child interactions. Parents generally agree that SBDs impede the quality of interactions with children (McDaniel & Radesky, 2018). Greater frequency of SBD-caused disruptions to parent–child interactions relates to children’s higher externalizing and internalizing problems (McDaniel & Radesky, 2018), and parents perceive child behavior as more difficult on days when they report their own SBD use as more absorbing and troubling (McDaniel & Radesky, 2017). Parents who use SBDs for personal reasons during interactions with children may be less responsive and engage in fewer positive interactions with their children (Golen & Ventura, 2015), implying that the effects on children may depend on the reasons why parents utilize SBDs.
Mechanisms Underlying Parent SBD Use
When SBDs are used in service of supporting children or strengthening the parent–child relationship, use is associated with more positive child outcomes (Linebarger & Walker, 2005; Madigan et al., 2020; Ostrov et al., 2006). In contrast, when SBD use is centered around parent needs, SBD use may take time away from developmentally appropriate opportunities and meaningful interactions (McDaniel & Radesky, 2018; Pagani et al., 2010). Below, we address reasons for parental SBD use that go beyond SBD use as a parenting tool, using a parent self-regulation perspective to consider how regulatory processes may act as mechanisms underlying positive versus negative effects of SBD use on children.
Stress Management and Coping
The rise in family SBD use has coincided with parents’ concerns about their own usage (Jiang, 2018). SBD use has been identified as a common coping mechanism for adult stress management (Wolfers & Schneider, 2021). Parents use SBDs to manage stress by engaging in self-distraction, information seeking, and active coping (Wolfers, 2021). Research has shown a link between heightened parenting stress and SBD use such that parents were more likely to use SBDs when dealing with more challenging child behaviors (McDaniel & Radesky, 2018).
Self-Regulation
Parent self-regulation may be particularly important for young children’s SBD use since parents act as external regulators of young children whose independent self-regulatory skills are not yet developed (Lunkenheimer et al., 2017). Executive function is one aspect of self-regulation that involves the top-down regulation of thought and behavior via cognitive skills such as inhibition (the ability to inhibit a dominant response), working memory (the ability to maintain and manipulate information in the short term), and cognitive flexibility (the ability to fluidly shift between tasks or rule sets; Diamond, 2013). Positive parenting is effortful and requires executive function; for example, parents must inhibit reactive responses to difficult child behavior and structure socialization and activities in response to children’s changing developmental needs (Distefano et al., 2018; Shaffer & Obradović, 2017). Parenting behaviors associated with executive function skills such as scaffolding, limit-setting, and monitoring are related to children’s greater verbal, cognitive, and prosocial skills (Barr et al., 2010; Linebarger & Walker, 2005; Ostrov et al., 2006). When applied to SBD use, for example, in monitoring and selecting media content for children, higher parental executive function skills may support parenting behaviors that promote more developmentally appropriate SBD use for children.
Conversely, parental executive function problems are associated with greater parenting challenges (Crandall et al., 2015; Sturge-Apple et al., 2014). For example, parents’ inhibitory and working memory problems promote more chaotic household environments, undermine consistent routines, and interfere with maintaining limits (Crandall et al., 2015; Deater-Deckard et al., 2012). These executive functioning challenges may interfere with parents’ monitoring of child SBD use and appropriate use of SBD as a disciplinary tool. Parents’ executive function problems have also been related to parents’ negative child-centered attributions (Deater-Deckard et al., 2010) and reduced affection and support (Curran & Andersen, 2017), which could disrupt parents’ adaptive involvement in and co-use of SBDs with children.
Parenting Support
Another reason parents may engage in SBD use is to communicate with others about parenting experiences, access parenting support, or access information about child health or development. Indeed, parents endorse using social media apps such as Facebook to interact with other parents about the joys and difficulties of parenting and access parenting support (Haslam et al., 2017). Furthermore, many parents use websites and social media to access parenting information, with higher usage reported by parents of younger relative to older children (Baker et al., 2017). However, parental use of SBDs for parenting support remains relatively unstudied. Given its potential to reduce stress and positively impact parenting, we included this aspect of parent SBD use in the development of the PSUS measure.
The COVID-19 Pandemic
This study was conducted during the COVID-19 pandemic. The pandemic and corresponding lockdown and social quarantine periods led to major changes in family lives and functioning, including increased isolation and worsening mental health (de Miranda et al., 2020) and increased parental stress (Seguin et al., 2021). Overall, SBD use increased during the pandemic for both parents and children (Islam et al., 2020; Susilowati et al., 2021). Reported use of SBDs during the pandemic served to combat feelings of distress, boredom, and lack of social interaction for children (de Miranda et al., 2020). Accordingly, the present findings should be interpreted in light of the pandemic context and results may offer information as to how SBD use, parenting, and stress and regulatory processes are interrelated in the context of elevated environmental stressors and social isolation.
Present Study
The present study targeted an improved understanding of the behaviors, perceptions, and regulatory processes involved in parent SBD use to better elucidate the potential mechanisms by which media and SBD use impact outcomes for young children. We developed a new self-report questionnaire, the Parent Screen-Based Device Use Survey (PSUS), to assess parents’ regulation of their own SBD use, regulation of and involvement with their children’s use, and use of SBDs and screen time as a parenting tool. We administered this measure to parents with young children aged 2–6 years to better understand parental SBD use during this critical, early stage of child development. The data used herein was part of a study conducted during the COVID-19 pandemic examining maternal stress and parenting, and thus only parents who identified as mothers were included in the present analysis.
A two-study design was used to develop and test the PSUS. A strength of this design is the ability to iteratively test the factor structure and reliability of the measure across two samples with a larger number of participants. Nine initial subscales were created, including Discipline, Limit-Setting, Involvement, Child Care, Family Norms, Self-Regulation, Dysregulation, Support, and Child-Centeredness. These subscales and their items were novel, developed based on prior research and expectations about what would be the most common and/or meaningful dimensions of parental SBD use, with the exception of two items in the Discipline subscale and two items in the Limit-Setting subscale that were borrowed from Tang et al. (2018).
In Study 1, given the novelty of the measure, exploratory factor analyses were conducted to test the factor structure of the data and whether items mapped onto subscales in expected ways. Based on these results, improvements to the measure were made as edits to existing items/scales or removal of items/scales as appropriate in preparation for Study 2. In Study 2, exploratory factor analyses were conducted again to evaluate subscales of the measure, and then once exploratory analyses supported the number of factors, a confirmatory factor analysis (CFA) was conducted to evaluate the final hypothesized subscales. Finally, concurrent validity was tested in Study 2 via relations between the PSUS subscales and parent distress, parent executive function problems, and child internalizing and externalizing behavior problems given that prior research has demonstrated significant positive relations between these variables and SBD use (McDaniel & Radesky, 2018; Tamana et al., 2019).
Study 1 Method
Study 1 Participants
Study 1 participants included 228 mothers (M age = 35.4 years, SD = 7.0) who had at least one child between two and six years old (M age = 52.3 months, SD = 16.1). Roughly 83.1% of mothers reported their race as White/Caucasian, 7.6% Black or African American, 4.9% Asian, 1.8% Native American, and 2.7% Multiracial. Roughly 5.9% of mothers reported identifying as ethnically Hispanic or Latinx. Median annual family income was between US$60,000 and US$69,999, ranging from under US$4,999 to over US$90,000. Roughly half (51.5%) held a Bachelor’s degree, and 14.1% of participants also held a graduate or professional degree. Most (85.9%) were married or living with a partner. Roughly 27.8% of mothers had one child, 38.8% had two children, 21.1% had three children, and 12.3% had four or more children. Roughly 11% of children had externalizing problems above the clinical threshold as determined by maternal ratings on the Child Behavior Checklist (t ⩾ 63; Achenbach & Rescorla, 2000).
Study 1 Procedure
Study 1 participants were recruited and participated remotely via Amazon Mechanical Turk (MTurk) between July and August 2020 during the COVID-19 pandemic. MTurk is an online platform where users remotely complete paid human intelligence tasks (HITs) posted by researchers (Jensen-Doss et al., 2022). Potential participants could view the study listing if their MTurk accounts indicated (a) residence in the United States, (b) at least 50 successful prior HITs, (c) a minimum 95% HIT approval rating, (d) self-identified female sex, and (e) self-identified parenthood. Interested mothers completed an eligibility screener in Qualtrics. Mothers were eligible if they reported that they (a) were fluent in written English and (b) had at least one child between ages 2 and 6 years. Eligible mothers viewed an implied consent form with study procedures and could download this form for their reference.
After providing implied consent, mothers answered questions about themselves, parenting, and child behavior via Qualtrics, lasting roughly 45–50 min. Participating mothers were asked to answer all items in reference to one “target child,” specifically the mother’s only or youngest child in the 2- to 6-year-old age range. Three attention check questions were included to aid validity of survey responses; these are multiple choice questions where respondents are provided the correct answer, such as “What is the best day of the week? For this question, please answer Tuesday.” Respondents are told during the consent process that these questions will be included to help incentivize attention to all items, and that failure to correctly respond to one or more of these questions results in study removal. Mothers were compensated US$6.00 for study participation via their MTurk accounts. This study was submitted to the Institutional Review Board at Pennsylvania State University and determined to be exempt because only de-identified data were collected.
Study 1 Measures
Parent Screen-Based Device Use
Mothers reported on the frequency of behaviors and perceptions relating to their own, their child’s, and their family’s SBD use, including the use of all cell phones, tablets, laptops, computers, TVs, video games, smart watches, and any other SBDs. Mothers responded to each item on a 5-point Likert-type scale ranging from “Never” (score of 1) to “Often” (score of 5).
The first version of the measure included nine subscales and 31 items. The four-item Discipline subscale targeted the degree to which the parent used screen time as a reward or punishment (e.g., “I take my child’s screen-based device away if they misbehave”). The three-item Limit-Setting subscale targeted the degree to which the parent set limits on child screen time (e.g., “I limit my child’s screen time during weekdays”). The four-item Involvement subscale targeted the degree to which the parent joined or had input in the child’s SBD activities (e.g., “I play games with my child on a screen-based device”). The four-item Child Care subscale targeted the degree to which the parent used screen time to ease the burden of caregiving (e.g., “When my child is using a screen-based device, I can get a break from caregiving”). The four -item Family Norms subscale targeted the degree to which SBD use was an allowed and typical family activity (e.g., “Screen time is a part of our family’s daily schedule”). The 3-item Self-Regulation subscale targeted the degree to which parents used their own screen time to regulate themselves (e.g., “I use my own screen time to help me reduce stress”). The three-item Dysregulation subscale targeted the degree to which the parent perceived difficulty controlling their own SBD use (e.g., “I spend more time on screens than I should”). The three-item Support subscale targeted the degree to which the parent used SBDs to obtain parenting or caregiver support (e.g., “I use a screen-based device to communicate with others about the difficulties of parenting”). The three-item Child-Centeredness subscale targeted the degree to which the parent limited their SBD use specifically to prioritize child needs (e.g., “I stop using my screen-based device when my child needs me”). Item-level responses were averaged to produce subscale scores, which ranged from 1 to 5.
Study 1 Results
Our analytic goal for Study 1 was to explore the degree to which items were interrelated and loaded onto hypothesized subscales. In the early stages of survey development, exploratory factor analysis (EFA) is considered more appropriate than CFA because the latter does not show the degree to which items load onto nonhypothesized subscales nor does it detect misspecification of the number of factors (Kelloway, 1995). Thus, given the novelty of the items and constructs targeted by the newly developed measure, EFA was performed for two to nine factors. Results supported a 9-factor solution, χ²(222) = 346.80, p < .001, comparative fit index (CFI) = .96, root mean square error of approximation (RMSEA) = .05, standardized root mean squared error (SRMR) = .03 (Table 1), offering initial support for the nine subscales originally conceptualized. All individual items loaded onto their respective subscales reasonably well (with highest respective loadings ranging from .45 to .85, p < .001) except for two Child-Centeredness items and one Child Care item. With respect to reliability, Cronbach’s alphas ranged from adequate to good (α = .67–.85) for all subscales, with the exception of two subscales: the Child-Centeredness and Child Care subscales.
Study 1 and Study 2 Exploratory Factor Analysis Results.
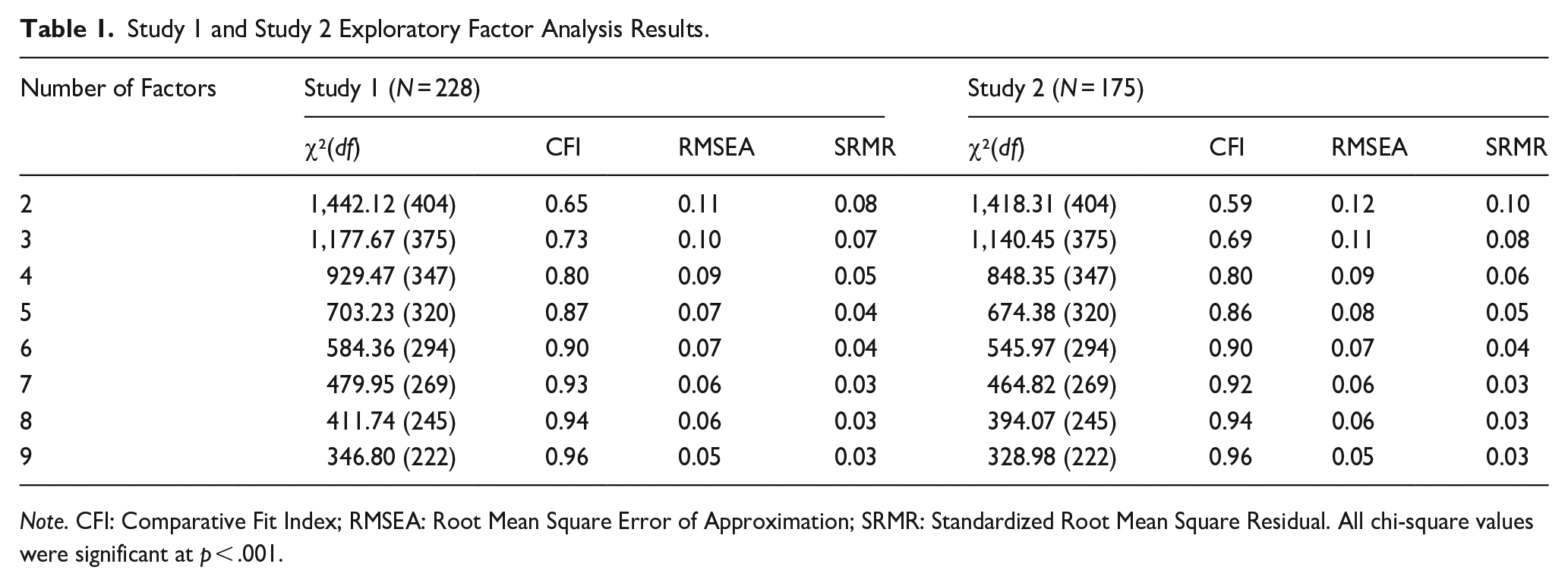
Note. CFI: Comparative Fit Index; RMSEA: Root Mean Square Error of Approximation; SRMR: Standardized Root Mean Square Residual. All chi-square values were significant at p < .001.
Some items loaded onto multiple subscales in ways that could have weakened factor loadings and reliability for the Child-Centeredness and Child Care subscales. For example, the original item, “I try to use my screen-based device less when I am with my child” was designed to reflect Child-Centeredness in terms of prioritizing children’s needs; however, it also loaded onto Self-Regulation, thus could have reflected self-regulation around parents’ SBD use. The most cross-loadings were found for the Family Norms subscale, likely reflecting that when SBD use is a common family activity, it also serves multiple other functions in the family. Bivariate correlations among subscales also suggested some conceptual overlap: the Self-Regulation and Dysregulation subscales showed the highest intercorrelation, r = .58, p < .001, which may have reflected that they captured adaptive and maladaptive dimensions of regulation around SBD use, respectively. In addition, the parent Self-Regulation subscale was intercorrelated with three additional subscales around the r = .40 level, including Family Norms, Discipline, and Support. Remaining intercorrelations among subscales ranged from modest to nonsignificant.
Based on these results, the survey measure was edited and refined in preparation for Study 2. First, items with low inter-item correlations with other items from the same scale were removed from consideration. Second, items with lower factor loadings or that loaded on multiple factors were inspected and wording was edited where necessary to improve clarity of meaning and/or distinction from other items. Third, new items were added to supplement three-item subscales, with the expectation that having at least four items per subscale could improve reliability values. Thus, the revised survey to test in Study 2 had 36 items.
Study 2 Method
Study 2 Procedure
Study 2 participants were recruited and participated remotely via MTurk between December 2020 and January 2021 during the COVID-19 pandemic. All procedures for Study 2 were the same as in Study 1.
Study 2 Participants
Study 2 participants included 175 mothers of at least one child between 2 and 6 years old (M = 46.5 months, SD = 14.2). The average mother was 35.9 years old (SD = 8.7). Roughly 85.6% of mothers reported their race as White/Caucasian, 10.5% Black or African American, 1.3% Asian, 0.7% Native American, and 2.0% Multiracial. Roughly 10.0% of mothers reported identifying as ethnically Hispanic or Latinx. Mothers reported a median annual family income of between US$50,000 and US$59,999, ranging from between US$5,000 and US$9,999 to over US$90,000. Roughly half (51.6%) of mothers held a Bachelor’s degree, and 13.7% of participants also held an advanced graduate or professional degree. Most mothers (77.1%) were married or living with a partner. Roughly 29.6% of mothers had only one child at the time of data collection, 41.4% had two children, 17.8% had three children, and 11.2% had four or more children. Approximately 12.1% of children had externalizing behavior problems above clinical threshold as determined by maternal ratings on the Child Behavior Checklist (t ⩾ 63; Achenbach & Rescorla, 2000).
Study 2 Measures
Parent Screen-Based Device Use (PSUS)
Based on Study 1 results, a revised PSUS was administered. Mothers once again indicated the frequency of behaviors and perceptions related to their own, their child’s, and their family’s SBD use, including the use of all cell phones, tablets, laptops, computers, TVs, video games, smart watches, and any other SBDs. Mothers responded to 36 items, consisting of nine four-item subscales, on a five-point Likert-type scale ranging from “Never” (score of 1) to “Often” (score of 5). Item-level responses on each subscale were averaged such that possible scores on each subscale ranged from 1 to 5. In this second version of the measure, as already noted above, there were changes implemented at the item level such that the number of items per scale was adjusted for some subscales, and certain individual items were altered. However, the nine subscales and their meanings did not change from those described in Study 1.
Parent Distress
Parent distress was measured using the 12-item parental distress subscale of the Parenting Stress Index—Short Form (Abidin, 1997). Mothers rated their agreement with each item on a Likert-type scale ranging from “Strongly Disagree” (score of 1) to “Strongly Agree” (score of 5). Sample items include, “I find myself giving up more of my life to meet my children’s needs than I ever expected,” “I feel trapped by my responsibilities as a parent,” and “Since having this child, I feel that I am almost never able to do things that I like to do.” Item-level responses were summed such that possible scores ranged from 12 to 60. Higher scores indicated higher maternal distress. Cronbach’s alpha reliability was .92.
Parent Executive Function Problems
Maternal executive function problems were measured using the Inhibition, Working Memory, and Shifting subscales of the Behavior Rating Inventory of Executive Function–Adult (BRIEF-A; Gioia et al., 2000). Mothers indicated whether items were “Never a problem” (score of 1), “Sometimes a problem” (score of 2), or “Often a problem” (score of 3) over the preceding month. Sample items on the eight-item Inhibition subscale included, “I have problems waiting my turn,” and “I rush through things.” Sample items on the eight-item Working Memory subscale included, “I have trouble with jobs or tasks that have more than one step,” and “I forget what I am doing in the middle of things.” Sample items on the six-item Shifting subscale included, “I have trouble changing from one activity to the other,” and “I have trouble accepting different ways to solve problems with work, friends, or tasks.” Mothers’ item-level scores on each subscale were summed such that higher scores indicated more executive function problems. Possible scores on the Inhibition and Working Memory subscales ranged from 8 to 24, and possible scores on the Shifting subscale ranged from 6 to 18. Cronbach’s alpha reliabilities for the Inhibition, Working Memory, and Shifting subscales were .86, .89, and .84, respectively.
Child Behavior Problems
Child behavior problems were measured using the Internalizing and Externalizing subscales of the Child Behavior Checklist (CBCL, Achenbach & Rescorla, 2000). Mothers reported whether a series of behavior problems were “Not True” (score of 0), “Somewhat or Sometimes True” (score of 1), or “Very Often or Often True” (score of 2) for their child in the preceding 2 months. The 36-item Internalizing subscale captures child behavior problems related to emotional reactivity, anxiety and depression, somatic complaints, and withdrawal. Sample items include, “Disturbed by any change in routine,” “Clings to adults or too dependent,” and “Avoids looking others in the eye.” The 24-item Externalizing subscale captures child behavior problems related to impulsivity, attention problems, and aggressive behavior. Sample items include, “Can’t concentrate, can’t pay attention for long,” “Easily frustrated,” and “Gets in many fights.” Item-level responses were summed such that possible scores ranged from 0 to 72 on the Internalizing and 0 to 48 on the Externalizing subscales. Cronbach’s alpha reliability for Internalizing and Externalizing subscales were .96 and .93, respectively.
Study 2 Results
PSUS Factor Structure, Reliability, and Intercorrelations
EFA once again supported a nine-factor solution, χ²(222) = 328.98, p < .001, CFI = .96, RMSEA = .05, SRMR = .03, replicating findings from Study 1 in terms of the number of factors (Table 1). Once again, individual items loaded onto their respective subscales reasonably well (estimates ranging from .45 to .85, p < .001), with the exception of two Child-Centeredness items and one Child Care item. With respect to reliability, Cronbach’s alphas ranged from adequate to good (α = .67–.85) for all subscales, with the exception of the Child-Centeredness and Child Care subscales.
Considering that the Child-Centeredness subscale showed similarly poor reliability and fit across both Studies 1 and 2, with problems related to two of the four items, this subscale and its corresponding items was dropped from the questionnaire altogether. With respect to the Child Care subscale, one item was moved from the Child Care to the Family Norms scale based on factor loadings. Finally, one item in the Involvement subscale was dropped due to a low factor loading. After these changes, the resulting survey had a total of 31 items across eight subscales, with each subscale made up of four items with the exception of Child Care (three items), Involvement (three items), and Family Norms (five items) (Figure 1).
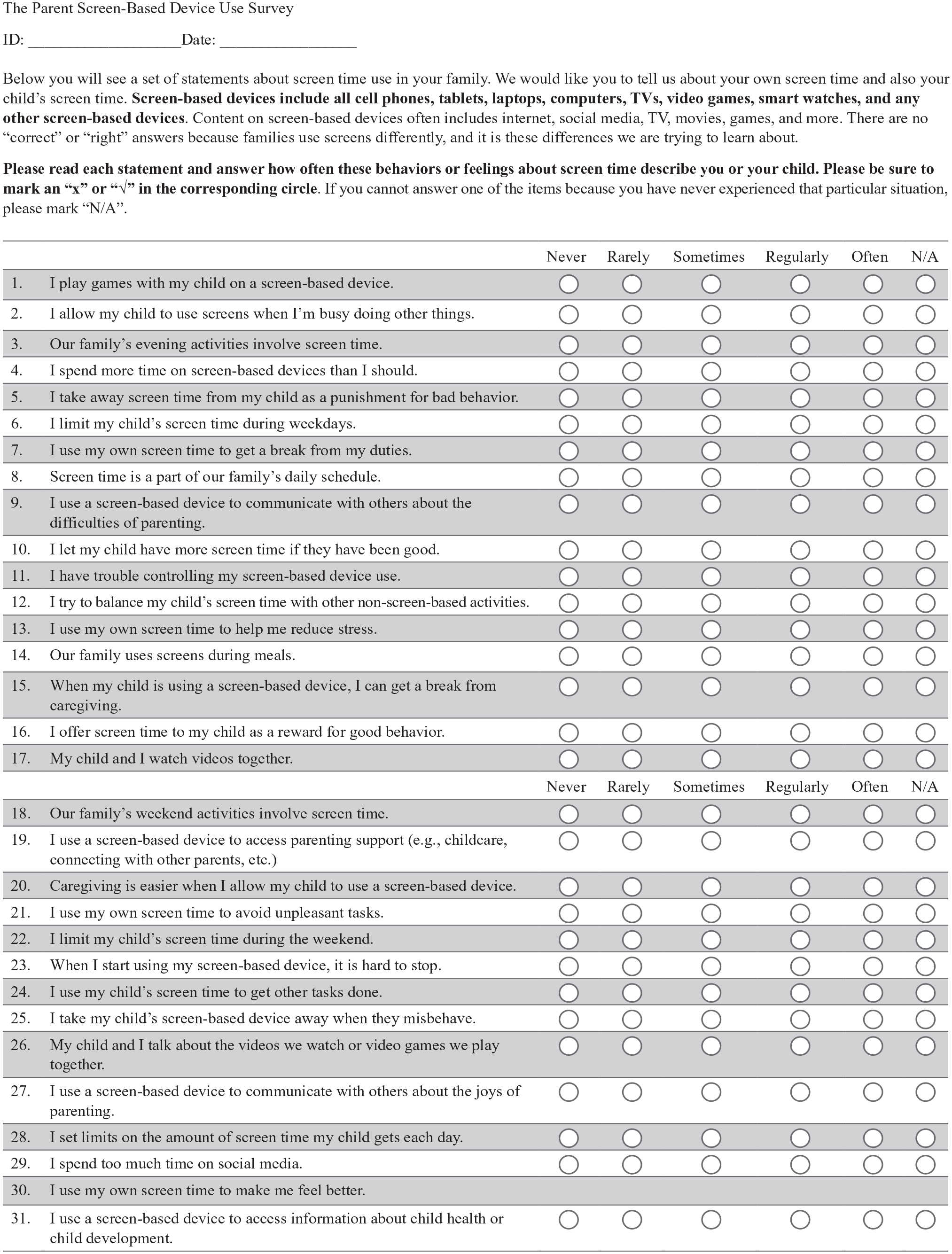
The Parent Screen-Based Device Use Survey.
Once these changes were made, we re-ran the EFA for the revised eight factors, which fit well and was preferable to seven or fewer factors, χ²(245) = 394.07, p < .001, CFI = .94, RMSEA = .06, SRMR = .03. All individual items loaded onto the revised subscales well (Mean loading = .72, range = .48-.89, all p < .001). Cronbach’s alpha reliability for the revised subscales was also good (range = .74–.87). Given the consistency of EFA results across the two studies and that the number of factors was supported by preliminary data, we then performed a CFA to further evaluate the eight hypothesized subscales. Model fit was adequate though did not meet criteria for a good fit across all indices, χ²(409) = 773.10, p < .001, CFI = .85, RMSEA = .07, SRMR = .07. CFA factor loadings for the final subscales are shown in Table 2.
Study 2 Confirmatory Factor Analysis Item Loadings on the Final Eight Subscales of the Parent Screen-Based Device Use Survey.
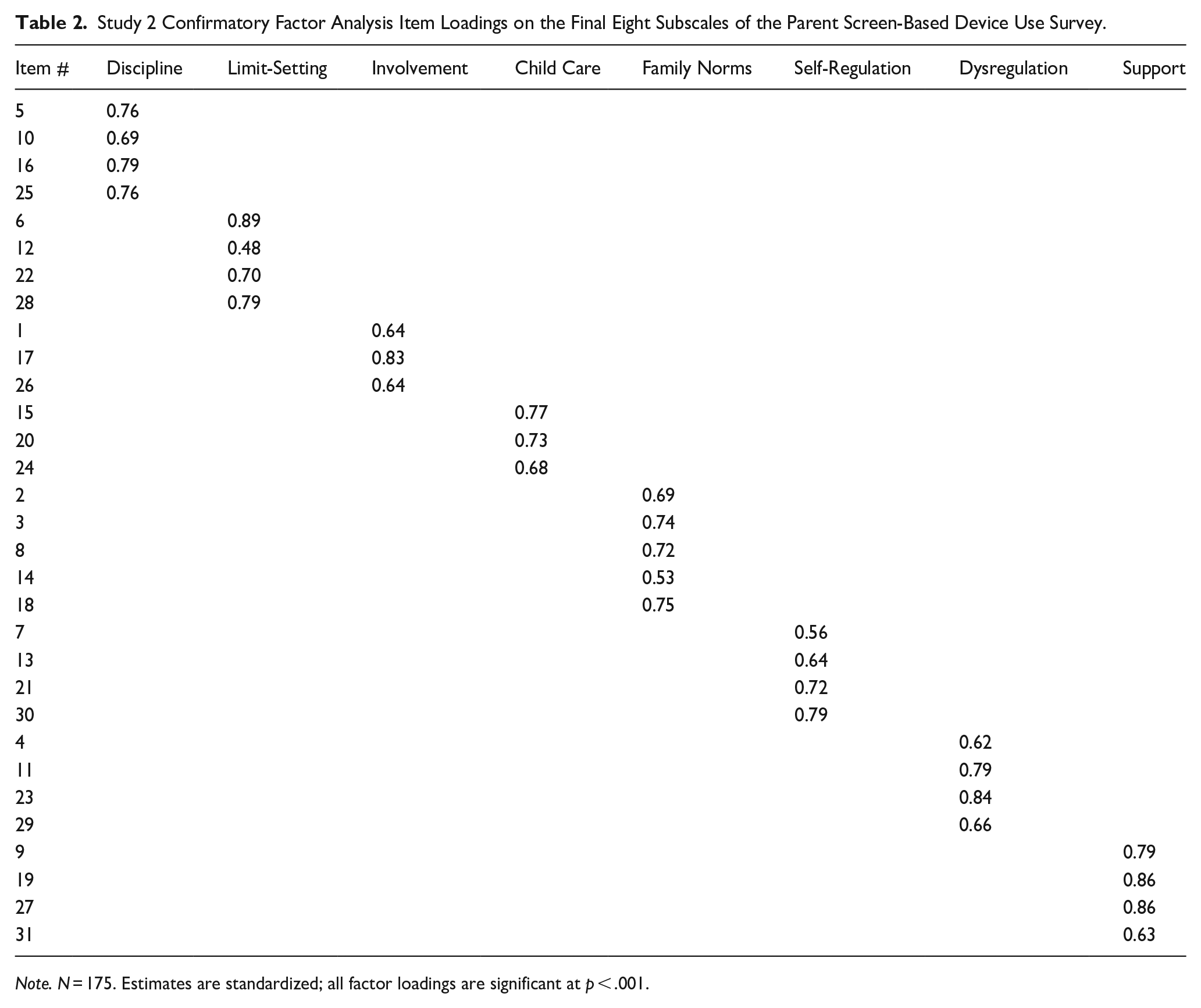
Note. N = 175. Estimates are standardized; all factor loadings are significant at p < .001.
Reliability values and intercorrelations among the final subscales are shown in Table 3. The strongest positive intercorrelations were between Child Care and the subscales of Family Norms, Self-Regulation, and Dysregulation, indicating that child care needs may be an important driver of how and why parents use SBDs with their children. Self-Regulation and Dysregulation were positively intercorrelated, which was not surprising given that they both reflect regulatory capacity in the parent; the fact that they were positively and not negatively intercorrelated suggests the possibility that even when parents positively endorse the use of SBDs to regulate themselves (e.g., to reduce stress), they have concerns about that strategy or that strategy is ineffective.
Study 2 Parent Screen-Based Device Use Survey Subscale Intercorrelations and Reliability.
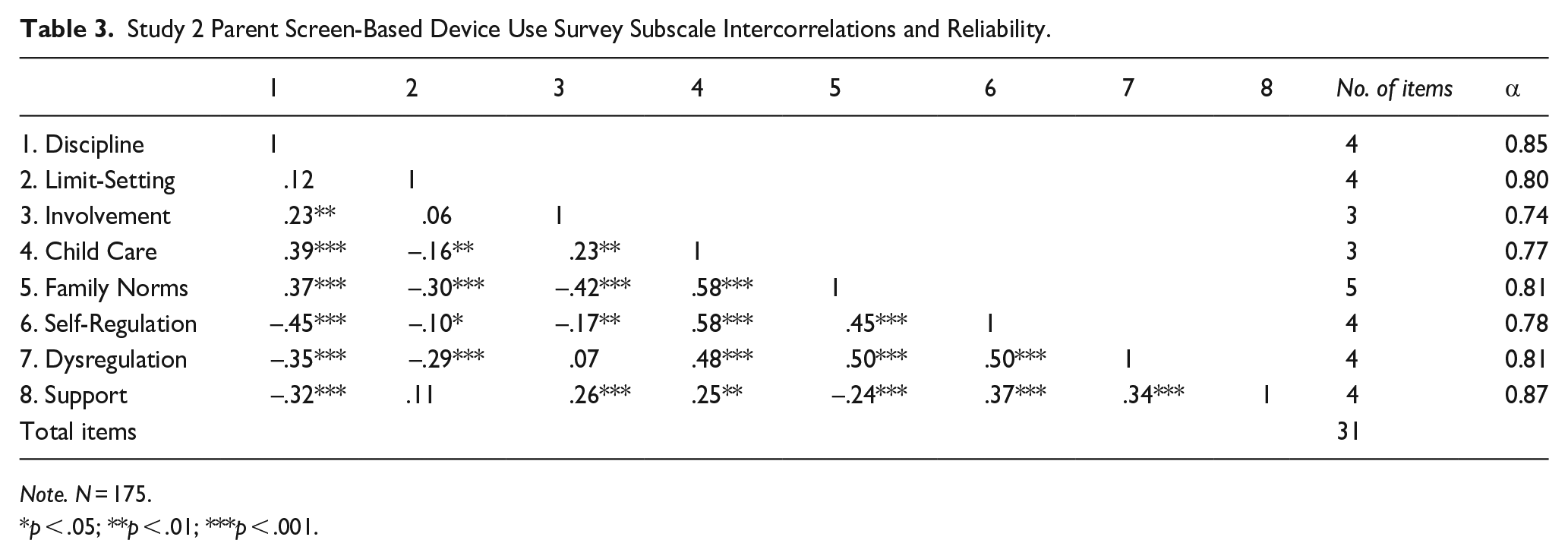
Note. N = 175.
p < .05; **p < .01; ***p < .001.
PSUS Relations with Parent Distress, Parent Executive Function Problems, and Child Behavior Problems
Bivariate correlations were performed to assess validity of this new measure via relations with parent distress and parent and child regulatory difficulties. Descriptive statistics for all study variables are shown in Table 4; bivariate correlations are displayed in Table 5. The subscales of Discipline, Family Norms, Child Care, Self-regulation, Dysregulation, and Support were all significantly and positively associated with parent distress, parent executive function problems, and child behavior problems, ranging from r = .19 to .48. These relations suggest parent distress and parent and child regulatory difficulties are meaningfully positively related to multiple aspects of parent SBD use, including parents’ regulation and dysregulation around SBD use and use of SBDs as a parenting tool or support. The Limit-Setting subscale was modestly negatively related to parental working memory and set-shifting problems, suggesting greater limit-setting around child SBD use was associated with fewer parent executive function problems; limit-setting was not related to parent distress or child behavior problems. Finally, the Involvement subscale was not significantly related to parent distress or parent or child regulatory difficulties.
Study 2 Descriptive Statistics.
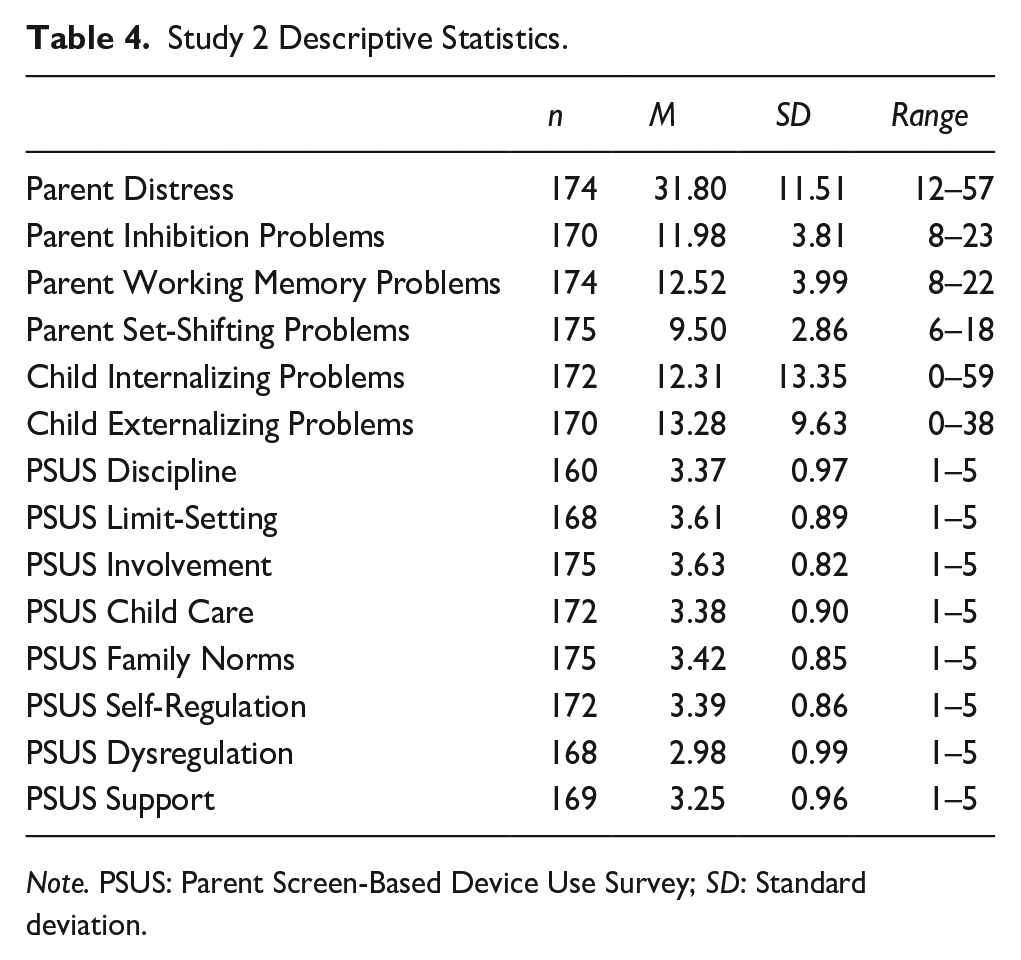
Note. PSUS: Parent Screen-Based Device Use Survey; SD: Standard deviation.
Study 2 Correlations between Parent Screen-Based Device Use Survey Subscales and Parent Distress, Parent Executive Function Problems, and Child Behavior Problems.
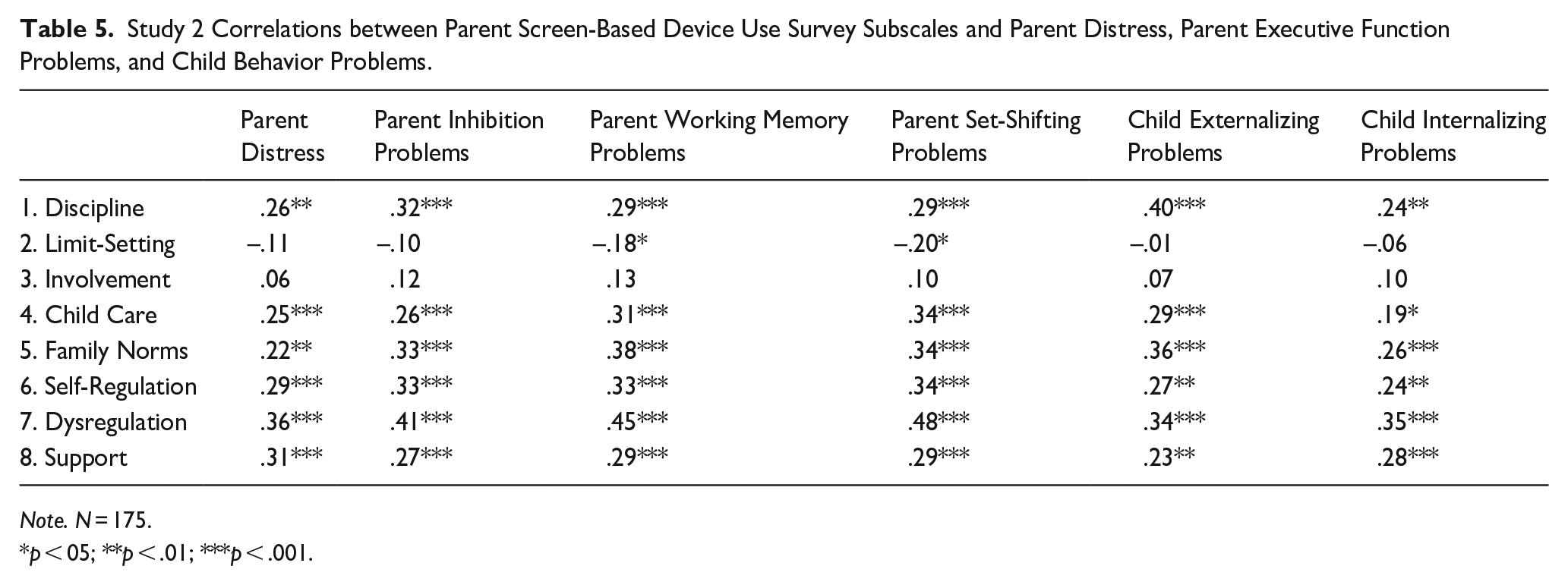
Note. N = 175.
p < 05; **p < .01; ***p < .001.
Discussion
The goal of this study was to develop and validate a new measure capturing parents’ behaviors, perceptions, and regulation of their own and their children’s SBD use. We aimed to acknowledge and better represent the role of parental individual difference factors in child media use, hoping to shed new light on what drives positive versus negative effects of media on child outcomes. We conducted two studies that allowed for the testing and refinement of the PSUS, resulting in a final 31-item questionnaire with good factor analytic structure, good reliability, and validation in the form of relations in expected directions with parent and child regulatory difficulties. Accordingly, we argue that the PSUS offers a useful new tool for researchers interested in capturing parent and parenting effects on child SBD use in the context of the broader family system.
Parent Factors Driving SBD Use: The Role of Parent Self-Regulation
There are likely many reasons parents engage with SBDs, and motivations and behaviors underlying use are likely to change with time and child development. We tested the PSUS in early childhood (ages 2–6 years), a developmental stage in which parents’ scaffolding and external regulation of the child is critical, making the role of parental self-regulation particularly important (Lunkenheimer et al., 2017). This is also the developmental stage during which family rules and routines for media use are typically first established (Coyne et al., 2017). The PSUS targeted parent self-regulation as a potentially central factor in how and why parents’ SBD use affects child outcomes. Results suggested parent SBD-related self-regulation and dysregulation were interrelated and correlated with other aspects of SBD use, suggesting they were in fact central processes underlying parent SBD use.
We found that when parents used SBDs as a tool to help regulate themselves and reduce stress, they were also more likely to use child screen time as a caregiver, report family SBD use as more normative, and perceive their own SBD use as dysregulated. These subscale interrelations were moderately high, ranging from r = .45 to .58. First, these findings suggest that media use in the family is pervasive such that when parents use it for one function (e.g., personal coping), they are more likely to use it for other purposes (e.g., child care and family entertainment). This is not necessarily surprising but offers empirical evidence that media use may be heightened by spilling over from one context to another within the family system (Broderick, 1993). Second, parenting is a common source of stress among parents of young children (Abidin, 1997), and child care in this age range requires the dynamic application of executive function skills to scaffold children and meet their needs (Obradović et al., 2017). Thus, it is likely that parents who use SBDs to regulate themselves and reduce stress in general may also use them to regulate caregiving duties and reduce parenting-related stress.
These robust interrelations may reflect a “slippery slope” of SBD use in families, whereby SBD use for one purpose heightens its use for other purposes. These findings also underscore the difficulty of parents and researchers to distinguish adaptive from maladaptive SBD use when use is frequent. Parents may use SBDs when feeling stressed, which may benefit them and their children by reducing stress in the context of caregiving and otherwise, but they may still perceive their own use as problematic or dysregulated. It may also suggest that using SBDs as a self-regulation tool is ultimately ineffective, for example, that it reduces stress in the short term but at the expense of other longer-term goals, such as optimal support of children’s developmental needs or the quality of the parent–child relationship (McDaniel & Radesky, 2018; Pagani et al., 2010).
Importantly, data used in this study were collected during the height of COVID-19 quarantine and social restrictions, chronic stressors that placed unique demands on parents’ own self-regulatory strategies as well as their role as external regulators for their young children. Indeed, the role of SBDs as a strategy to cope with increased parent stress and mental health challenges (de Miranda et al., 2020; Seguin et al., 2021) is reflected in the increased use of SBDs by both parents and children throughout the COVID-19 pandemic (Islam et al., 2020; Susilowati et al., 2021). Thus, the use of SBDs as a mechanism for regulating both parents and their young children may have been exacerbated by the social restrictions in place due to the COVID-19 pandemic; it will be important to determine in future work if reported variable levels and interrelations are replicated in a nonpandemic context.
SBDs as a Parenting Tool or Source of Parenting Support
Our findings support prior work showing that SBD use pertains to multiple, interrelated aspects of parenting, including discipline (Samaha & Hawi, 2017), limit setting (Gentile et al., 2014), child care (Kabali et al., 2015), and parental involvement in screen use (Christakis, 2014). Parents who used SBDs as a disciplinary strategy with their children were more likely to use SBDs for child care, as a tool to engage with their child, and for parenting support (r = .23–.39). These findings align with previous research but describe more specifically how the use of SBDs for discipline relates to other functions of parental SBD use. They also offer novel information in showing that parents use SBDs to access parenting help, which could have implications for their willingness to consider app-based programming and interventions to support parenting.
Limit-setting was negatively related to parental dysregulation surrounding SBDs (r = –.29), family norms (r = –.30), and use of SBDs for child care (r = –.16), suggesting that parents who employed more limit-setting strategies may have more constructive approaches to parent and child SBD use, as well as less SBD use overall. The benefits of limit-setting indicated here are supported by prior work on parental monitoring of child SBD use being related to more positive child outcomes (Blum-Ross & Livingstone, 2016; Gentile et al., 2014). However, few prior studies have investigated limit-setting as a specific parenting technique for managing child SBD use or in relation to other SBD parenting strategies. Thus, our findings not only add nuance to our understanding of limit-setting in the context of SBD use but also indicate the potential for effective SBD limit-setting to be a positive approach to parent and child media use.
Parental involvement in child SBD use has previously been linked to more positive family attributes such as family connectedness (Padilla-Walker et al., 2012). The present study, however, revealed that higher parental involvement in child SBD use was related to higher use of SBDs for child care, family norms, and self-regulation (r = .30–.57), which have been found to relate to more negative outcomes based on the displacement hypothesis (Pagani et al., 2010). However, it is possible that parental involvement in SBD use with children relates to greater SBD use in general, thus increasing the use of SBDs in both adaptive and maladaptive ways.
PSUS Relations With Distress and Regulatory Problems
Many forms of SBD use were positively related to parent distress, parent executive function problems, and child behavior problems, with dysregulated SBD use showing the most relevance to parent and child regulatory problems. Specifically, parents reported both higher distress and greater executive function problems (in inhibition, working memory, and set-shifting) when they also reported greater SBD use related to discipline, child care, family norms, self-regulation, dysregulation, and support. These findings support the validity of the PSUS from a parent self-regulation perspective and suggest that, on average, the greater use of SBDs for multiple family and parenting purposes may reflect more maladaptive regulatory processes. Conversely, parents who reported more limit-setting surrounding family SBD use also reported fewer executive function problems in working memory and set-shifting (but not inhibition). It is possible that these parents may be more effective, for example, at updating SBD use limits in response to children’s needs or tailoring limits by type of media use.
Generally, findings also align with prior research showing more maladaptive effects of heightened SBD use on children (Li et al., 2020; Tamana et al., 2019). We found that greater SBD use related to family norms, discipline, child care, and parenting support was related to children’s higher internalizing and externalizing problems. It is likely that parents who perceive their children as more challenging enact more discipline and seek more relief from caregiving and support in parenting those children. Children’s greater behavior problems were also related to higher parental use of SBDs for their own self-regulation and more dysregulated SBD use. Limit-setting and involvement in child screen time were not significantly related to behavior problems, suggesting they stood out as forms of parent SBD use that were not maladaptive for children. In this way, findings replicated themes in prior literature (e.g., Elias & Sulkin, 2019), showing that when SBD use is more regulated (via parental limits) and child-centered (via parental involvement) it does not exacerbate children’s problems. In sum, our findings build on prior work showing relations between heightened SBD use and negative outcomes, extending it to parents’ greater distress and executive function problems as well as children’s greater internalizing and externalizing problems (Tamana et al., 2019).
Strengths, Limitations, and Future Directions
The PSUS has multiple strengths. It is unique in offering: (a) an integrated assessment involving various types of SBDs; (b) SBD use as it pertains to the parent, child, and family; and (c) a direct assessment of parent behaviors, perceptions, and regulation of their SBD use, which may act as critical mechanisms of SBD effects on child development. Most prior studies and measures have focused on capturing media-use perspectives and habits regarding single SBD types (e.g., television, cellphones; Pagani et al., 2010; Sekarasih, 2016) and with regard to either parent or child use, but not both (Kabali et al., 2015; McDaniel & Radesky, 2017). By addressing various types of SBD use at multiple levels of the family system, the PSUS may provide a more complete picture of media use in the family context.
The PSUS could supplement other measures of parent self-regulation, stress, parenting, and child behavior in examining how parents cope with stress, how SBDs influence parenting behaviors and challenges, and how SBDs impact children’s adaptive versus maladaptive developmental outcomes. Furthermore, in basic and applied research on parenting, parent self-regulation, coping, and needs for parenting support often go unstudied. The PSUS acts not only as a metric for measuring parenting behaviors but also sheds light on how parents use SBDs to self-regulate and cope with challenges, which could inform potential targets for intervention. This study also adds new information regarding the reasons and the contexts in which parents allow their children to use SBDs and engage in SBD use themselves. We believe this new measure is an exciting and needed contribution to the developmental psychology literature given the increasingly frequent use of SBDs in families and the potential for media-related processes to contribute to individual differences in child development and health.
Our results were drawn from a mostly White, middle-class sample, which appears to be characteristic of English-speaking, U.S.-based MTurk participants (Jensen-Doss et al., 2022). Although a nationwide sample is an advantage, these sample characteristics do not represent the U.S. population as a whole and the field of psychology has a history of developing assessments on predominantly White, Western, educated, middle-income samples, which has contributed to a limited and biased science. Thus, a critical future goal will be to assess the generalizability of the PSUS to other sociodemographic groups, including families of different racial, ethnic, and cultural backgrounds, families who may have less access to SBDs due to socioeconomic disadvantage, and parents and children with varying developmental and clinical profiles.
There were some methodological limitations of the present work. Given the cross-sectional design, nuanced child age-related differences in SBD use could not be explored. Future research could explore age differences within the early childhood period given that toddlers have distinct parenting and socialization needs compared to kindergarteners. Another limitation was a reliance on exclusively maternal self-report measures in the present analysis, which could inflate shared method variance. MTurk participants have been shown to be reliable respondents (Jensen-Doss et al., 2022), however, involvement as a paid research participant in multiple survey-based studies could impact the validity of survey responses. However, attention checks were included for this reason and failing to respond correctly to attention check items resulted in removal from the study, reducing the likelihood of analyzing invalid data.
This study focused on SBD use in early childhood with children aged 2–6 years and thus findings support the use of the PSUS in studies of early childhood. However, items were worded in such a way as to potentially be applicable to school-age children as well. Future research could target the potential reliability and validity of the PSUS with families with school-age children; if valid, its use in later developmental stages could shed light on changes in the effects of parental SBD use on children over time. However, we would not expect the PSUS to adequately capture parental SBD use with adolescents given the qualitatively distinct nature of parenting and media use in childhood versus adolescence. Other future research goals include replication of the PSUS factor structure and reliability; inclusion of fathers and other nonmaternal caregivers; replication in samples collected after the end of COVID-19-related quarantine and social isolation; examining validity in relation to observed data; and testing the longitudinal effects of parent SBD use on child outcomes.
Conclusion
This study offers a new measure targeting the assessment of parental perceptions, behaviors, and regulation around parent and child SBD use. By assessing these behaviors in more nuanced ways and acknowledging the beliefs, norms, and functions they may serve, we hope this measure can supplement future studies aimed at understanding the adaptive versus maladaptive effects of family media use on child development and mental health. Overall, our results suggest that certain types of use, such as limited use and involved co-use, are associated with fewer parent self-regulatory problems, whereas normative family SBD use, using SBDs as a caregiver, disciplinary tool, or support, and parents’ dysregulated use or use of SBDs to regulate themselves are associated with more parent distress, parental regulatory problems, and child behavior problems. With this information, better recommendations can be made to parents about their role in and approaches to media use for themselves and their children to optimize child health and development.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was supported by National Institutes of Health grants R01HD097189 (Lunkenheimer) and T32HD101390 (C.M.D.), as well as an award from the Pennsylvania State University Child Study Center (C.M.D.).
Data Availability
These data are not publicly available.