
Abstract
Current research has reported the beneficial effects of mindfulness-based interventions (MBIs) on general domains of cognition and behavior among children. The present study is the first meta-analysis with controlled studies investigating the pre-post change effects of MBIs on two widely experienced behaviors in childhood education, namely inattentiveness and hyperactivity–impulsivity. With a special developmental focus on the early years, a total of 21 studies with 3- to 12-year-old children were included in the meta-analysis. Results indicated that MBIs decreased children’s overall inattentive and hyperactive–impulsive behavior with a small but significant effect size (k = 21, g + = .38, p < .001). However, this overall positive effect was only significant when teachers rated children’s behavior and nonsignificant when parents and children themselves were the informants. Additionally, MBIs showed a moderate effect in reducing inattentiveness and hyperactivity–impulsivity for children at risk for such behavior. In conclusion, results indicate that MBIs, which are relatively easily applied in educational practice, have the potential to decrease inattentive and hyperactive–impulsive behavior and might contribute to children’s overall better functioning at school.
Keywords
Inattentiveness and hyperactivity–impulsivity have gained substantial interest in behavior change interventions due to their important role in school and social–emotional functioning (Diamantopoulou et al., 2007) as well as future deviance and pathology (Moffitt et al., 2011). As reported by previous meta-analyses, mindfulness-based interventions (MBIs) can be beneficial to self-regulatory skills among youth (Dunning et al., 2018; Klingbeil et al., 2017; Zenner et al., 2014; Zoogman et al., 2015). However, there is still substantial ambiguity pertaining to whether MBIs render specific behavioral effects. As the number of studies with MBIs has been growing, Klingbeil et al. (2017) encouraged future meta-analyses on MBIs with more refined outcome domains, such as inattentive and hyperactive–impulsive behavior. These behaviors are the main symptoms of attention deficit hyperactivity disorder (ADHD) but also pose challenges for non-diagnosed children with subthreshold levels of such behaviors (Schonert-Reichl & Lawlor, 2010).
In the current study, we aimed to address methodological limitations in previous meta-analyses within this topic (Cairncross & Miller, 2016; Chimiklis et al., 2018) and synthesize the available controlled studies with pre-to-post measurement, to assess the potential of mindfulness practices to reduce inattentive and hyperactive–impulsive behaviors in childhood. The significance of this meta-analysis is also supported by the study of Sumner et al. (2018), who stated that the field of behavior change suffers from fragmentation and poor reporting, thus the rigorous systematic synthesis of evidence in behavior change interventions is needed. This meta-analysis would yield evidence-based recommendations about whether school-integrated MBIs could be used to alter these specific behaviors from early childhood. These would be important findings, given that pharmacological treatments for ADHD symptoms are not recommended at an early age, because they often involve unpleasant side effects (Barkley et al., 1990). In addition, it would be important to gain a more in-depth understanding about the potential moderators of the efficacy of MBIs, such as environmental and/or developmental disadvantage of children, which are neglected areas in the previous systematic syntheses.
Attention and Impulse Control in Childhood
Behavior regulation problems, such as impulsive actions and deficient attention control, are often experienced among children in educational and clinical practice (Koch, 2016; Närhi et al., 2017; Schonert-Reichl & Lawlor, 2010). According to the survey of the Primary Sources, teachers reported an increased level of behavior problems, such as inattentiveness and hyperactivity–impulsivity across children (Scholastic and the Bill & Melinda Gates Foundation, 2012), which might have a cascading long-term effect on cognitive and social–emotional functioning from childhood to adulthood (Diamantopoulou et al., 2007; Moffitt et al., 2011). Consequently, it would be important to support practitioners by yielding evidence-based recommendations about whether MBIs could be used to support attention and impulse control from the early years and decrease inattentive and hyperactive–impulsive behavior.
Although attention and impulse control are still developing through the life span, there are some age-appropriate expectations for children to regulate their own actions (Washington State Department of Early Learning, 2012). Early in development, children typically have difficulties with activities requiring sitting and listening, because their attention span is relatively short. From the age of 4–5 years, a child should be able to pay attention for 2–10 min on a task chosen by an adult (e.g., pick up toys, dress up) and 10–15 min on a novel and interesting task. At this age, a child should be able to resist impulses, wait longer to respond in structured settings, and choose an appropriate behavior with little adult direction. Parallel to the maturation of the nervous system, one can expect children to sustain attention in an effortful manner for longer periods and to ignore distractions which simultaneously appear in their environment (Washington State Department of Early Learning, 2012).
Difficulties of attention and impulse control can occur in a child’s life due to various developmental and environmental factors (Eaves et al., 1997). Genetic and biological factors of weak self-regulation are accompanied by a developmental susceptibility to attention and inhibitory control problems (Blair & Diamond, 2008). Psychosocial environmental factors including but not limited to household chaos (Razza et al., 2012), low socioeconomic status (SES) and poverty (Blair, 2010), divorce of the parents (Weaver & Schofield, 2015), early overexposure to electronic media (Cheng et al., 2010), family stress (Becker & McCloskey, 2002), and sleep problems (Gregory & O’Connor, 2002) are all risk factors for attention and impulse control problems and might contribute to the developmental susceptibility of deficient self-regulation. Hackman and colleagues (2010) stated that brain development occurs within a social–economical context, and childhood SES influences neural development. Children from low socioeconomic backgrounds are at increased risk of experiencing stress (Lupien et al., 2000) and show higher rates of attention problems and hyperactive–impulsive behavior (National Institute of Child Health and Human Development Early Child Care Research Network, 2005). Persistent patterns of inattention and hyperactivity–impulsivity are characteristics of ADHD, the most commonly diagnosed neurodevelopmental disorder in childhood that interfere with functioning across multiple settings (American Psychiatric Association, 2000). According to the Diagnostic and Statistical Manual of Mental Health Disorders (DSM-IV), inattentive behavior can be described by behaviors such as failure to listen when spoken to, completely carry out instructions, difficulties with sustaining attention and organization, and off-task behavior (Kofler et al., 2008). Hyperactivity–impulsivity can be described by behaviors like inability to sit still, excessive verbalization and activity, failure to inhibit responses and control behavior, and a tendency to interrupt others. Although 5%–10% of the children population is estimated to be affected by ADHD, it is well-known in clinical practice that a substantially higher number of children and adolescents present subthreshold symptoms (Balázs & Keresztény, 2014).
A potential way to address these behavioral regulation problems can be to implement evidence-based interventions that can improve effective behavior regulation of all children even in the early ages. Based on previous research, MBIs are promising cost-effective avenues to increase physical, social–emotional, and mental health, while reducing self-regulation problems in youth (Carsley et al., 2018; Klingbeil et al., 2017; Takacs & Kassai, 2019; Zenner et al., 2014). Additionally, there are some previous evidence that MBIs can be relatively easily added to the curriculum, and they might be mediated successfully by teachers as well (Meiklejohn et al., 2012).
Mindfulness-Based Interventions
According to John Kabat-Zinn (2003), the founder of the well-known 8-week Mindfulness-Based Stress Reduction program, mindfulness is the act of gently paying attention to the present moment in a nonjudgmental manner. During mindfulness activities, self-regulatory abilities, such as attentional control and emotion regulation, are trained through nonreactive focusing on internal (e.g., thoughts) or external stimuli (e.g., objects, sensations), whereas automatic responding is reduced (Bishop et al., 2004). Mindfulness is rooted in ancient Buddhist philosophy and meditation practice, and in the last several decades clinical and educational practitioners have begun to adopt the concept of mindfulness in the promotion of mental and physical health (Cullen, 2011). MBI is an umbrella term including a wide variety of programs that are based on the theory and practice of mindfulness adopted to different stages of development. In the past 10 years, several programs have been developed and investigated with children, such as the Still Quiet Place (Saltzman, 2014), Paws b (.b Foundations, 2015), MindUP (The Hawn Foundation, 2011), Kindness Curriculum (Flook et al., 2015), Mindful Awareness Practices (Flook et al., 2010), or the YogaKids (Bergen-Cico et al., 2015). Consequently, there is a great heterogeneity between MBIs for youth, relating to dosage, theoretical base, and types of practices used (Emerson et al., 2020). There is no well-grounded consensus about the minimum number of mindfulness sessions that yields sustainable effects, neither from the content nor from the core practices of MBIs. Acute effects on anxiety and attention could be observed even after one short mindfulness exercise (Carsley & Heath, 2018), while enduring changes in attentional and emotional control might occur after long-term and/or more intensive programs (Tarrasch, 2018). The study of Jha et al. (2007) suggested that mindfulness training might improve attention-related behavioral responses by enhancing the functioning of specific subcomponents of attention.
Previous Meta-Analyses
Previous meta-analyses have demonstrated general positive effects of MBIs on cognitive performance (Dunning et al., 2018; Zenner et al., 2014), attention (Klingbeil et al., 2017; Zoogman et al., 2015), and behavioral functioning of the youth population (Dunning et al., 2018; Maynard et al., 2017).
In the existing literature with youth, two meta-analyses synthetized evidence from studies with diagnosed or at-risk samples of ADHD. The meta-analysis of Cairncross and Miller (2016) involved samples diagnosed with ADHD between the ages of 8 and 50 years and showed moderate effects of mindfulness practices in reducing inattentive and hyperactive/impulsive symptoms. This main effect was heterogeneous which could be moderated by the age of the participants, although a moderator analysis of age was not conducted due to the limited number of studies with children. Another limitation of the study was that effect sizes of MBIs were not based on comparisons to control groups, thus positive effects might have been induced by natural maturation or reflect a test–retest effect.
The other meta-analysis by Chimiklis et al. (2018) investigated the effectiveness of MBIs, all kinds of meditation, and yoga on symptom reduction among 5- to 17-year-old children at risk of or diagnosed with ADHD. The effect sizes have demonstrated that MBIs, yoga, and meditation had a significant small to moderate effect with respect to overall decrease in ADHD symptoms based on parents’ and teachers’ reports. The overall effect reported by the parents was heterogeneous, and the moderator analysis revealed that longer sessions of intervention showed significantly larger effect sizes. In case of inattention and hyperactivity separately, the effects were significant but small. The effect on hyperactivity (reported by the parents) was also significantly heterogeneous. The moderator analysis revealed that intervention type (e.g., MBIs, yoga, or meditation) and ADHD diagnosis (formally diagnosed or not) significantly moderated the efficacy of the interventions. MBIs had a larger effect than yoga or the combination of yoga and meditation, and children who were formally diagnosed with ADHD showed greater improvement as compared to the non-diagnosed samples. Conclusions based on this meta-analysis are somewhat limited because of the low number of studies in the moderator analyses (which might lead to low statistical power) and the quality of the included studies because the majority of them were non-randomized trials (82%).
The Present Study
As Klingbeil et al. (2017) pointed out, previous meta-analyses have not intended to identify which specific behaviors can be trained with MBIs in childhood and to elucidate differences in efficacy accounted by moderators such as at-risk status. Hence, an assessment employing rigorous methodology to investigate the effect of MBIs on inattentive and hyperactive–impulsive behavior in early development is warranted. With a special developmental focus on the neglected area of early and middle childhood, this meta-analysis aimed to evaluate the efficacy of MBIs in the reduction of hyperactivity–impulsivity and inattentiveness and explore potential moderators of effectiveness. As previous meta-analyses (Dunning et al., 2018; Klingbeil et al., 2017) proposed to include gray literature in future research to avoid publication selection bias, which arises from the preferential reporting of statistically significant scientific results in peer-reviewed journals, we intended to involve non-peer-reviewed studies also in the present meta-analysis. Furthermore, this is the first meta-analysis that incorporates differences in environmental and developmental background among children as a possible moderator of the perceived benefits of mindfulness.
Consistent with the findings of previous meta-analyses, we expected small but significant effects of MBIs in reducing children’s inattention and hyperactivity–impulsivity. That is, it was hypothesized that children who participated in MBIs would have more pre- to posttest decline in inattentive and hyperactive–impulsive behavior compared to children in the control groups. We also hypothesized that samples at risk for poor attention and impulse control would benefit more from MBIs than non-at-risk samples. Consequently, a stronger positive effect of MBIs on inattention and hyperactivity–impulsivity was expected for samples with a diagnosis related to a neurodevelopmental deficit (e.g., ADHD, learning disorder) and samples with environmental disadvantage (i.e., low SES). In addition, we assessed the effects of other potential moderators of the MBIs used in previous meta-analyses such as age, characteristics of the primary studies, and implemented MBIs.
Method
Search Strategy
A systematic literature search was conducted to identify potential studies that investigated the effect of MBIs on children’s inattentive and hyperactive–impulsive behavior (for the search string, see Appendix A). The comprehensive search was conducted in five electronic databases (PubMed, Scopus, Web of Science, Google Scholar, and ProQuest) for journal articles and unpublished dissertations and theses. The search was conducted up until April 2020. Concurrently, using the snowball method, the reference lists of meta-analyses, review articles, and relevant studies on the efficacy of MBIs were also screened. The PRISMA flow diagram (see Appendix B) demonstrates the process from identification until the inclusion of studies. Finally, 71 studies were assessed for eligibility based on the full-text articles, and 21 met all our inclusion criteria.
Inclusion Criteria
Study design: First of all, the included studies should have implemented a randomized controlled trial (RCT; individual level) or quasi-experimental design (children were not randomly assigned to the conditions but on a group level [e.g., classroom]). Secondly, results of the intervention group were compared to a passive (no treatment) or an active control group (children were assigned to a control activity during the intervention period).
Participants: The age of the sample did not exceed 12 years at the beginning of the study. That is because previous meta-analyses neglected the early ages of development, thus the aim of this study was to apply a special developmental focus on early and middle childhood.
Intervention: The intervention program was primarily based on the concept of mindfulness (e.g., mindfulness meditation, mindfulness-based school curriculum, mindful yoga, etc.), with mindfulness practices such as mindful breathing, mindful movements, enhancement of awareness and/or body scan as core elements of the program. Those studies that were explicitly described by the study’s authors as “mindfulness” interventions were included in the meta-analysis.
Outcome measures: The study reported results on at least one pre- and post-test measurement of inattentive and/or hyperactive–impulsive behavior, which was based on either self-report or the report of parents and/or teachers (e.g., the Hyperactivity subscale from the Strengths and Difficulties Questionnaire). Questionnaires not differentiating between inattention and hyperactivity–impulsivity, but referring both in their items, were included as relevant outcome measures of overall attention and impulse control problems (e.g., BRIEF Global Executive Composite subscale).
Language: The paper was written in English.
Exclusion Criteria
Studies that implemented MBIs which trained solely the parents or the teachers but measured an indirect effect on children’ behavior were excluded from the meta-analysis.
Studies including mindfulness as a subcomponent in the intervention (e.g., Dialectical Behavior Therapy) were also excluded.
Studies that did not report pre- and posttest means with standard deviations were excluded if authors did not reply or could not provide study data when contacted.
Operationalization of Variables and Coding Procedure
Studies that met inclusion criteria were coded by two independent coders. Statistical data for calculating the effect sizes and potential moderator variables were operationalized and coded for each study: (1) sample characteristics (age, whether children were at risk for attention problems and hyperactivity–impulsivity due to low SES or a neurodevelopmental disorder); (2) study design (randomization on an individual level [RCT] or on a group level [quasi-experimental], control condition [active or passive]); (3) characteristics of the MBIs (length of the intervention in hours and in sessions, the instructor [teacher, expert, or both]); (4) type of outcome measure(s) (inattention, hyperactivity–impulsivity, or an overall scale) and the informant/rater (children, parents, or teachers); (5) statistics for calculating effect sizes (sample sizes, means and standard deviations on the pre- and the posttest).
Some questionnaires and/or subscales were not apparently classifiable by the DSM-IV ADHD behavior symptomatology, which we used as a reference point for the categorization of the outcome measures (American Psychiatric Association, 2000). In those cases, we looked through the items of the scale to make a decision. For instance, the subscale of Emotion Regulation from the teacher-rated Social Competence Scale (Flook et al., 2015) was coded as an outcome measure of hyperactive–impulsive behavior based on the content of the items. After inspection of the items, the Youth Self-Regulation Inventory was categorized as a measure of overall inattentive and impulsive behavior.
Samples were considered at risk for inattentive and hyperactive behavior in two cases: (i) the presence of extant psychosocial stress factors in the children’s environment (e.g., low income, household chaos, and disadvantaged living environment) or (ii) the presence of a neurodevelopmental disorder (e.g., ADHD, learning disorders, autistic spectrum disorder, etc.). Any disagreements between the two coders were discussed until a consensus was reached. Inter-rater reliability (percentage of agreement) ranged from 80% (type of outcome measure) to 100% (sample size, diagnosis).
Risk of bias
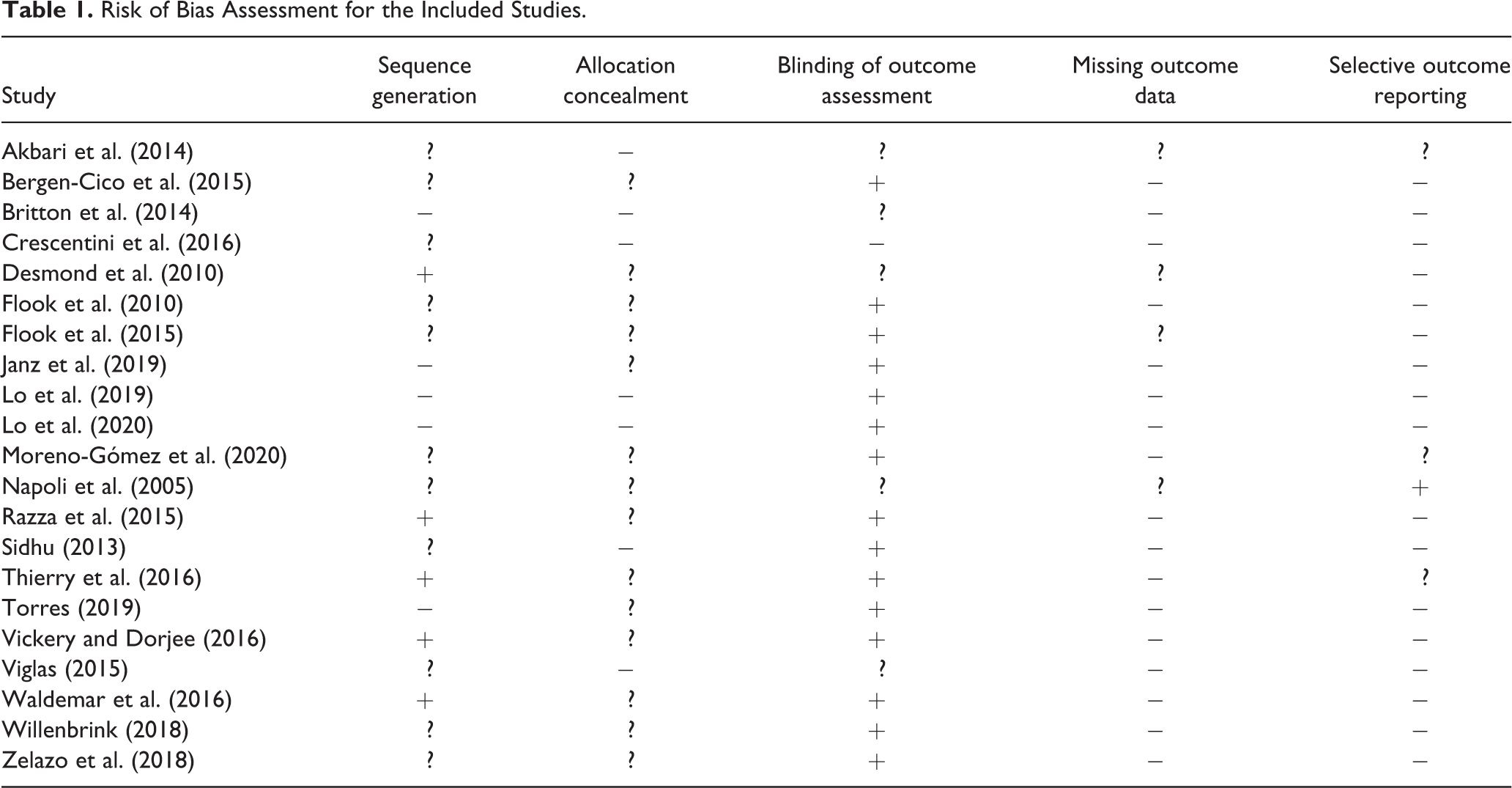
A selected list of items was used from the Cochrane Collaboration’s Risk of Bias Tool and coded by one of the authors to assess the quality of the included studies (Higgins et al., 2011; Pascoe et al., 2017). Risk of bias was coded for the following 5 items: (i) sequence generation (whether the study described how they generated the allocation); (ii) allocation concealment (whether the study described the method they used to conceal the allocation sequence); (iii) blinding of informants who assessed children’s behavior on the outcome measures (whether the informants were aware of the participants’ condition); (iv) missing outcome data (describes the completeness of main outcome data, including attrition and exclusion); (v) selective reporting (of the outcome data in the study). Each study was rated for all categories, by giving “minus” when the risk of bias was low, “plus” indicating a high risk of bias, or “question mark” if the risk of bias was unclear (see Table 1). Risk of bias was used as a moderator variable (RoB index) by calculating a discrete variable: each “minus” was given a value of 1, each “question mark” a value of 0, and each “plus” a value of −1. With this change, individual studies could have a value between −5 and 5, with lower scores indicating higher risk of bias.
Risk of Bias Assessment for the Included Studies.
Data Extraction and Synthesis
In consideration of the relatively small sample sizes in the primary studies, the Hedges’ g standardized mean difference was calculated to estimate the difference between the intervention and the control condition (Hedges, 1983). The Comprehensive Meta-Analysis software (version 3.3; Borenstein et al., 2015) was used for the computation of the individual effect sizes and conducting the analyses. For calculating effect sizes, raw means and standard deviations were entered, but in case of one study that did not report such data (Napoli et al., 2005), the Cohen’s d estimate was utilized and transformed to Hedges’ g. When more than one appropriate outcome metrics were reported in a study, we entered the data on all those and the software used an average of these effect sizes per study before taking the average effect over all the studies. A study with a standardized residual exceeding ±3.29 was considered an outlier (Borenstein et al., 2011).
A positive effect size in the present study suggested less inattentive and hyperactive–impulsive behavior in the MBIs as compared to the control groups. Cohen’s (1988) interpretation of the size of the effect was (a) “small” in magnitude around .20, (b) “medium” around .50, and (c) “large” around or above .80.
Meta-Analytical Procedures
The standardized difference in pre- to posttest change regarding inattentive and hyperactive–impulsive behavior between the MBI and control groups was chosen as the dependent variable, instead of the difference in posttest scores, because quasi-experimental studies were also included that do not ensure equal groups. Effect sizes were standardized using the posttest standard deviations because none of the primary studies reported on the correlation between the pre- and posttest variables (Morris & DeShon, 2002).
The average effect size and the corresponding 95% confidence interval (CI) were calculated using the random-effects model, which incorporate heterogeneity in meta-analyses (Borenstein et al., 2011). The random-effects model was selected instead of the fixed model because there was quite some variation across the included studies (e.g., age, sample size, outcome measures, etc.) and the random-effects model allows between-study differences in addition to sampling error (Hedges & Vevea, 1998). The studies were weighted with the reverse of their variance by the software when calculating the average effect size, so studies with larger samples weighted more in the average than smaller studies (Borenstein et al., 2011).
The heterogeneity of the effect sizes was estimated using the Q-statistic and the I 2 estimate, which signifies the between-study variance caused by systematic differences across the studies beyond sampling error. Small I 2 values, until 25%, represent low variance. Moderate to large (above 50% and 75%) ratios of between-study variance (I 2) suggest substantial heterogeneity and the possibility that the observed heterogeneity may be explained by other factors on the study level (Higgins et al., 2011).
Moderator analyses extend conventional meta-analytical procedures to estimate the extent to which moderators explain heterogeneity in the intervention effect (Hedges & Pigott, 2004). A series of meta-regression and subgroup analyses were conducted with moderator variables regarding characteristics of the studies, children, MBIs, and outcome measures, listed above in the “Operationalization of Variables and Coding Procedure” section. Specifically, a meta-regression analysis indicates whether the effect size is related to the values of moderator variables (Higgins et al., 2011).
Publication bias analyses
Regarding the issue of publication bias, we applied several strategies. First of all, we aimed to include unpublished dissertations, theses, and research reports in an attempt to correct for the tendency of journals to publish studies with significant results (Rosenthal, 1979). Secondly, we assessed the possibility of publication bias in the data set by examining Begg’s funnel plot and Egger’s regression test (Egger et al., 1997). When studies were spread relatively symmetrically around the average effect size on the funnel plot, there were no signs of publication bias (Sterne et al., 2011). Sterne et al. (2011) recommended not to use tests for funnel plot asymmetry when there are fewer than 10 studies, because in that case the statistical power is too low to distinguish chance from real asymmetry. Therefore, the funnel plot was utilized to assess publication bias solely regarding the overall effect size. Additionally, we computed the classic fail-safe number, which reports the hypothetical number of nonsignificant studies that would make the significant average effect nonsignificant (Rosenthal, 1979). When the fail-safe number exceeds 5k + 10, we can consider the average effect robust.
Statistical power analyses
A series of retrospective statistical power analysis was performed for the subgroup effects, and the meta-regressions as suggested by Valentine et al. (2010). When tests for subgroup analysis are retrospectively found to have low power (less than approximately 80% as suggested by Cohen [1988]), nonsignificant effects do not provide a strong evidence for the rejection of a true effect. In most cases in the present meta-analysis, power estimates showed low power for moderator variables, except for publication status and at-risk status of the sample. For underpowered moderator analyses, we decided to report only descriptive information instead of a statistical test of the moderator.
Results
Overall Effect of MBIs on Inattention and Hyperactivity–Impulsivity
A significant, small-sized positive effect of MBIs was found (see Table 2), which was a moderately heterogeneous effect, which is also visible on the forest plot. According to the I 2 statistics, approximately 44% of the variance was attributable to systematic rather than random error. The standardized residuals indicated that there were no outlier studies (see Figure 1).
Average Effects Found Overall and Specifically for Inattentive and Hyperactive–Impulsive Behavior.

Note. CI = confidence interval; SE: standard error.
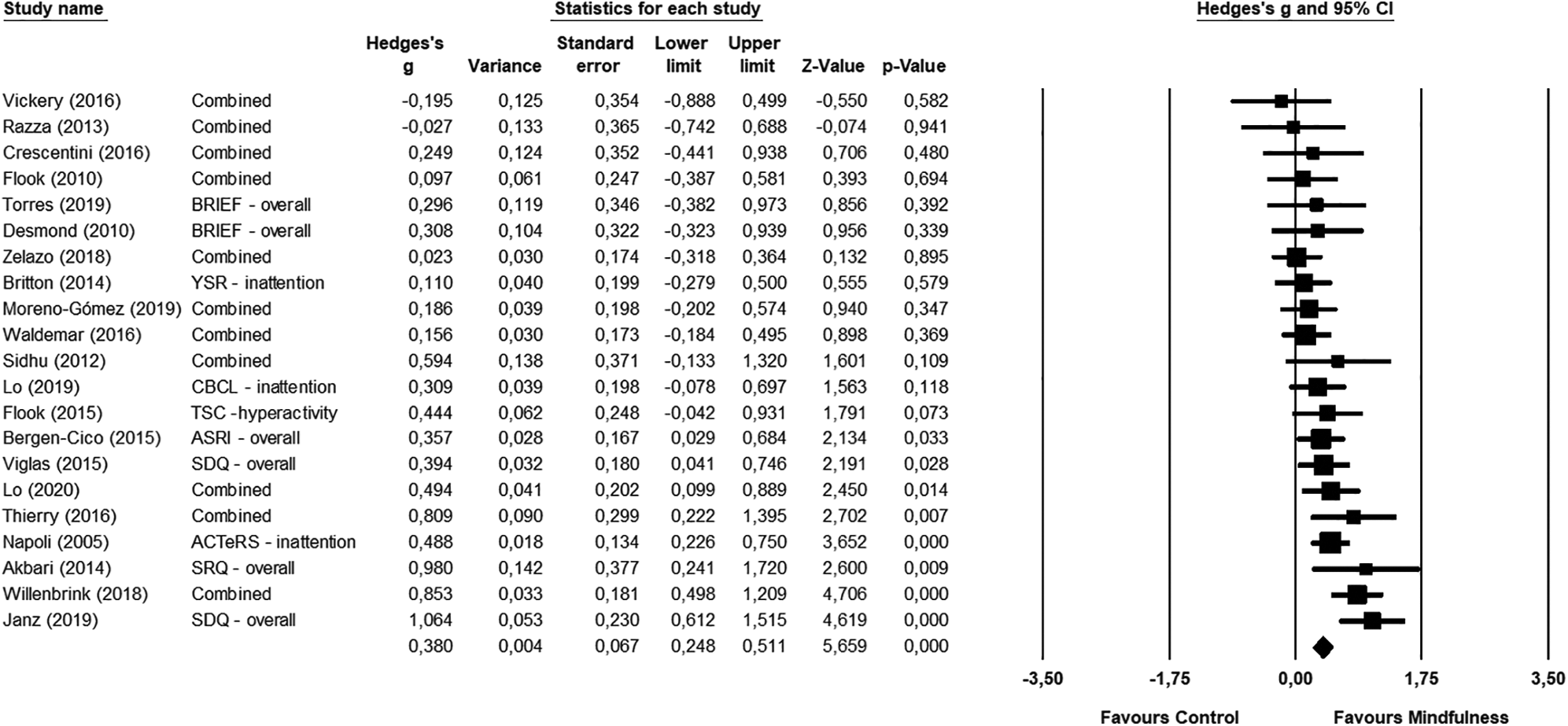
Forest Plot of the Overall Effect Sizes of Included Studies.
Specific Effects
Inattentive behavior effect size
There were nine studies assessing the specific effects of MBIs on inattentiveness. As shown in Table 2, a significant small positive effect of MBIs on inattentiveness was found. However, it should be noted that the 95% CI was quite large, so this estimate does not seem to be very precise. The effect was significant and moderately heterogeneous.
Hyperactive–impulsive behavior effect size
Five studies reported outcomes about the effect of MBIs specifically on hyperactive–impulsive behavior. As shown in Table 2, the effect of MBIs on hyperactive–impulsive behavior was significant, small-sized, positive, and homogeneous.
Moderator Analyses
Age
The meta-regression analysis indicated that the mean age of children did not moderate the efficacy of MBIs on overall inattention and hyperactivity–impulsivity significantly (coefficient = .02, SE = .02, 95% CI [−0.05, 0.05]).
At-risk status
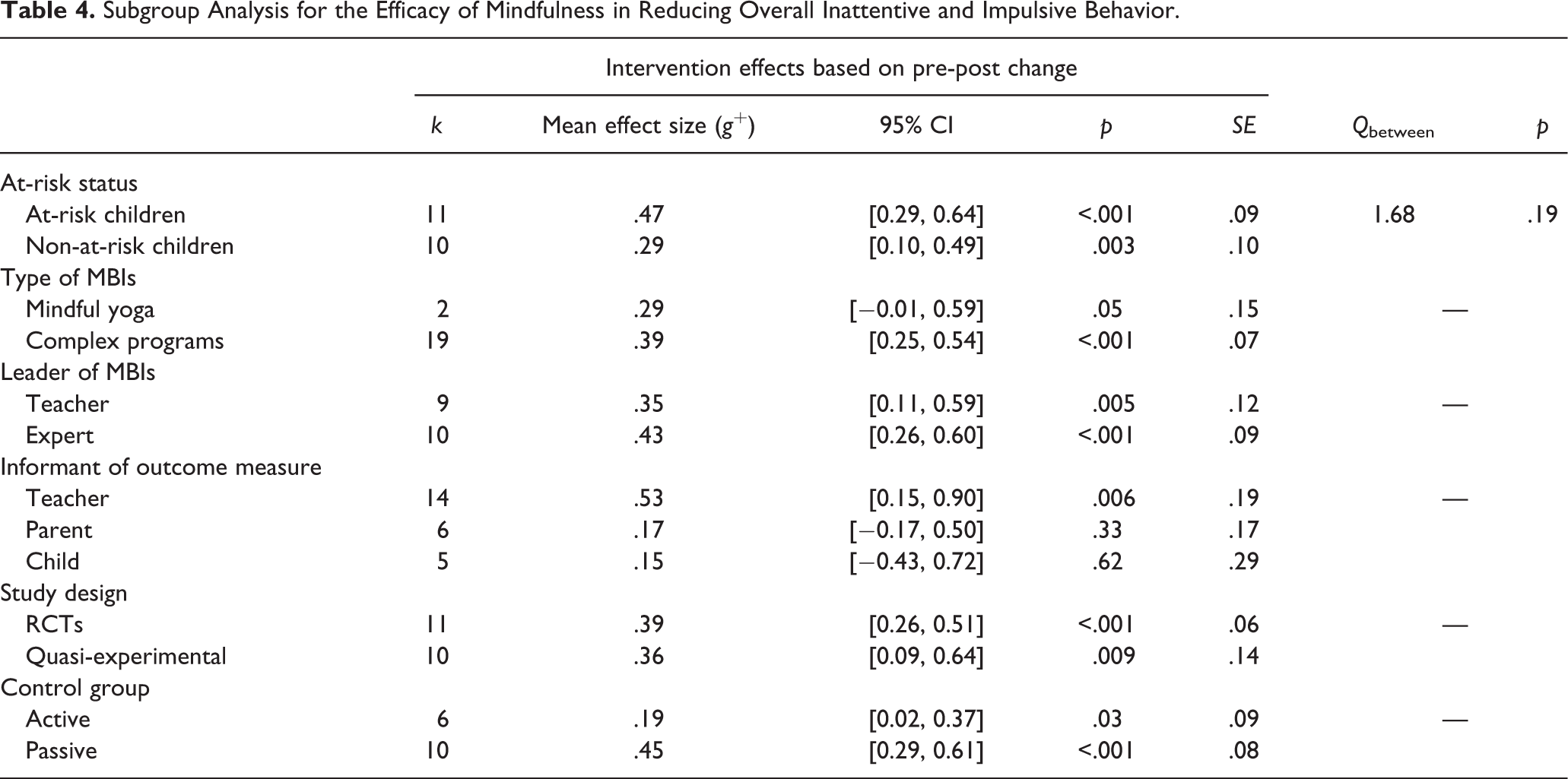
Eleven studies (52%) included samples at risk for attention or impulse control problems (see Table 3). MBIs had a significant medium-sized positive effect on overall attention and impulse control problems of at-risk children and a small significant effect for non-at-risk samples (Table 4). When comparing the two samples, there were no significant differences in efficacy between the two groups. More specifically, the two studies examining children with ADHD showed a significant medium-sized positive effect (k = 2, Hedges’ g = .52, SE = .37, 95% CI [−0.13, 1.32], p = .004), while the one study including children with dyscalculia found a significant large positive effect (k = 1, Hedges’ g = .98, SE = .37, 95% CI [0.24, 1.72], p = .009). Children from low SES background showed a significant, small reduction in inattentive and hyperactive–impulsive behavior (k = 8, g + = .42, SE = .11, 95% CI [0.21, 0.64], p < .001). Similarly, typically developing samples from probably middle and/or high SES showed a small but significant reduction regarding their inattentive and hyperactive–impulsive behavior from MBIs (k = 9, g + = .31, SE = .11, 95% CI [0.09, 0.53], p = .006).
The Characteristic of the Included Studies.
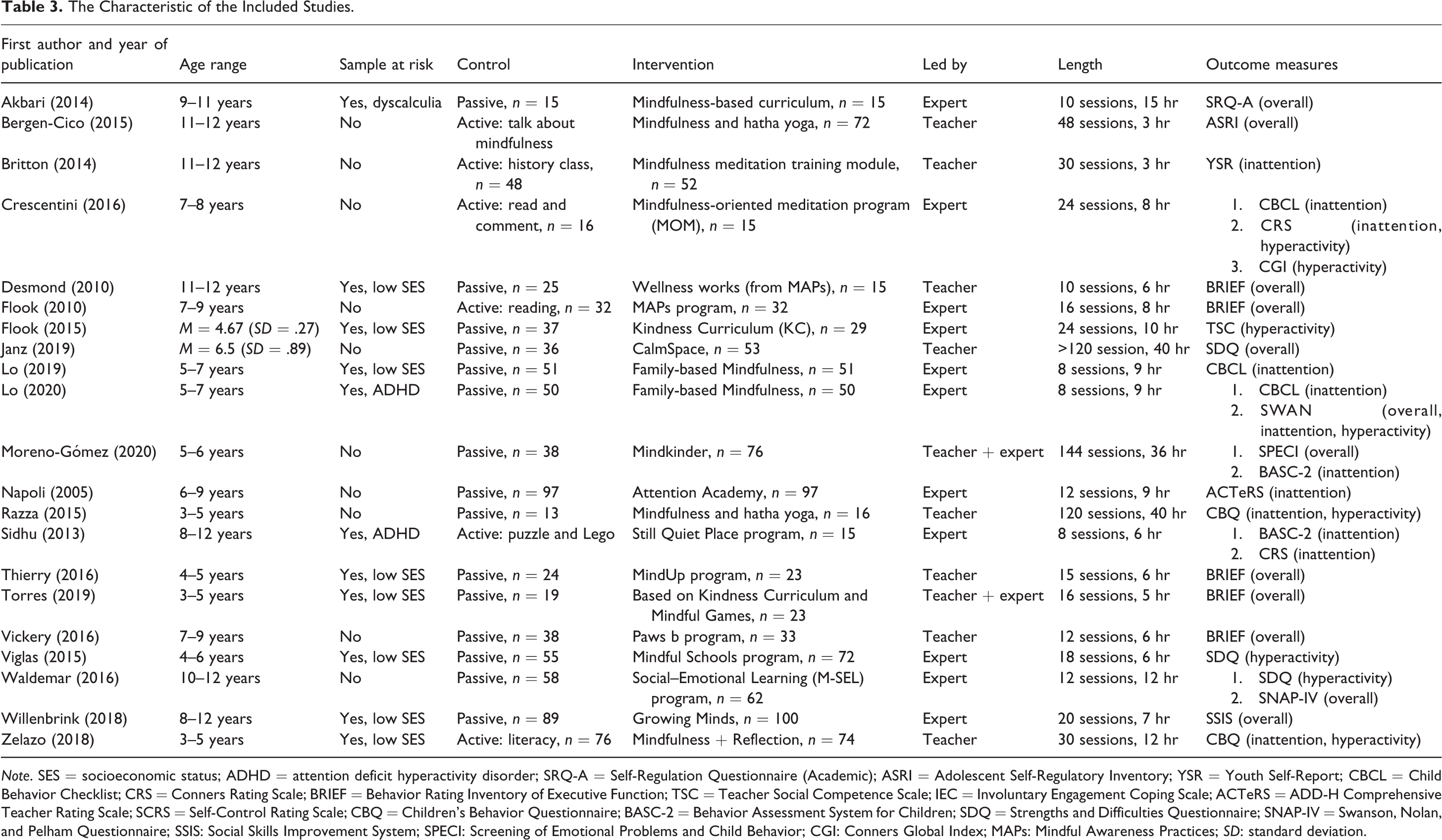
Note. SES = socioeconomic status; ADHD = attention deficit hyperactivity disorder; SRQ-A = Self-Regulation Questionnaire (Academic); ASRI = Adolescent Self-Regulatory Inventory; YSR = Youth Self-Report; CBCL = Child Behavior Checklist; CRS = Conners Rating Scale; BRIEF = Behavior Rating Inventory of Executive Function; TSC = Teacher Social Competence Scale; IEC = Involuntary Engagement Coping Scale; ACTeRS = ADD-H Comprehensive Teacher Rating Scale; SCRS = Self-Control Rating Scale; CBQ = Children’s Behavior Questionnaire; BASC-2 = Behavior Assessment System for Children; SDQ = Strengths and Difficulties Questionnaire; SNAP-IV = Swanson, Nolan, and Pelham Questionnaire; SSIS: Social Skills Improvement System; SPECI: Screening of Emotional Problems and Child Behavior; CGI: Conners Global Index; MAPs: Mindful Awareness Practices; SD: standard deviation.
Subgroup Analysis for the Efficacy of Mindfulness in Reducing Overall Inattentive and Impulsive Behavior.
Leader of intervention
Approximately half of the MBIs were implemented by an expert (52%), two MBIs by teachers and experts together (10%), and the rest were instructed by the teachers (38%). In studies where the teacher was the leader of the MBIs, a small, significant positive effect on impulsivity and inattentiveness was observed. Expert-led MBIs showed a somewhat larger significant positive overall effect (see Table 4).
Informants
MBIs showed a medium-sized, significant effect in reducing inattentiveness and impulsivity when teachers were asked to rate children’s behavior (see Table 4). However, measures based on children’s self-report and parental reports indicated nonsignificant effects (see Table 4). There was only one study which specifically stated using blind raters in respect to group assignment (Crescentini et al., 2016). The effect size found in this study was positive but not significant (Hedges’ g = .23, SE = .35, 95% CI [−0.46, 0.92], p = .51).
Length of intervention
The overall duration of the trainings varied between 3 and 40 hr, including between 8 and 120 sessions, with a median of 6 hr and 10–12 sessions in total. Both total intervention time (coefficient = .004, SE = .01, 95% CI [−0.01, 0.02])) and number of training sessions (coefficient = .003, SE = .03, 95% CI [−0.003, 0.004]) had very small significant positive relationships with the effect size.
Study design
Eleven of the included studies (52%) utilized a quasi-experimental study design, while 10 studies (48%) implemented individually randomized controlled design. In the overall efficacy of MBIs on inattention and hyperactivity–impulsivity, RCTs demonstrated a significant, small-sized positive effect similar to quasi-experimental studies (see Table 4).
Control group
The average effect size in studies utilizing active controls indicated a small-sized significant positive effect size; however, studies with passive control groups showed a medium, significant positive effect size (see Table 4).
Publication bias
As shown in Table 3, the included studies were published between 2005 and 2020 with a steady increase in the number of studies on MBIs for children after 2010. A meta-regression analysis revealed that the year of publication had no significant relationship with the effect size (coefficient = .006, 95% CI [−0.03, 0.04]). Most of the studies (76%) were published in peer-reviewed journals, while there were three dissertations, one thesis, and one unpublished research report. The average effect sizes found in published (k = 16, g + = .34, SE = .08, 95% CI [0.19, 0.49], p < .001) and unpublished reports (k = 5, g + = .54, SE = .12, 95% CI [0.30, 0.78], p < .001) were both significant, positive, and varied from small to medium; however, there was no difference between these average effect sizes (Q between (1) = 2.05, p = .15), which further supports the absence of publication bias.
Risk of bias
Studies with the highest risk of bias (RoB index: −1) indicated a significant medium-sized positive effect (k = 2, g + = .54, SE = .12, 95% CI [0.31, 0.78], p < .001), while studies with the second highest risk of bias (RoB index: 0) showed a small-sized marginally significant positive effect (k = 7, g + = .17, SE = .09, 95% CI [−0.01, 0.35], p = .06). Studies with lower risk of bias demonstrated a significant, small- to medium-sized positive effect (RoB index: 1), k = 4, g + = .50, SE = .22, 95% CI [0.08, 0.93], p = .02; (RoB index: 2), k = 3, g + = .71, SE = .25, 95% CI [0.23, 1.1], p = .004; (RoB index: 3, k = 3, g + = .40, SE = .11, 95% CI [0.18, 0.62], p < .001. Included studies with the lowest risk of bias showed a nonsignificant effect (RoB index: 4) (k = 2, g + = .14, SE = .17, 95% CI [−0.20, 0.48], p = .41).
Discussion
This is the first meta-analysis of rigorously controlled pre- and posttest studies of MBIs applied to improve children’s inattention and hyperactive–impulsive behavior, which are two commonly experienced behavior problems in (pre-)school. By only synthesizing studies with control or comparison groups, the present study addressed limitations of previous meta-analyses including Cairncross and Miller (2016) and Chimiklis et al. (2018). In general, children assigned to MBIs showed small to medium improvements in inattentive and hyperactive–impulsive behavior relative to children in the control groups. By observing these specific behavioral effects of MBIs, this meta-analysis provides a unique contribution to previous meta-analyses (e.g., Dunning et al., 2018; Klingbeil et al., 2017) that observed overall effects of MBIs on comprehensive cognitive and behavioral domains. Furthermore, this is the first meta-analysis that accounted for at-risk status (i.e., neurodevelopmental or socioeconomic risk of self-regulation impairment) as a potential moderator of efficacy of MBIs in reducing inattentive and hyperactive–impulsive behavior.
Including a total of 21 studies, meta-analytic results revealed that MBIs render a significant small positive effect on inattentive and hyperactive–impulsive behaviors. According to these findings, MBIs have a nurturing effect on attention and impulse control of children from 3 to 12 years of age. These benefits may be driven by both bottom-up (e.g., stress reactivity reduction) and top-down processes (e.g., enhancing executive function skills) of self-regulation, trained during mindfulness practices (Zelazo & Lyons, 2012). As Shapiro et al. (2006) assumed, the first process of mindfulness practice is that it leads to a different perspective which results in positive changes regarding targeted outcomes, like better impulse control and less inattention.
Our results are in line with the results of previous meta-analyses, assessing the effect of MBIs on related domains including attention and behavior regulation, which showed small positive effects (Carsley et al., 2018; Dunning et al., 2018; Klingbeil et al., 2017; Maynard et al., 2017; Takacs et al., 2019; Zenner et al., 2014; Zoogman et al., 2015). The meta-analysis of Chimiklis et al. (2018) investigating the effect of MBIs, all kinds of yoga and meditation interventions on inattention and hyperactivity–impulsivity also indicated small to moderate positive effects of these interventions, although it is important to note that most of their included studies implemented a single-subject design (73%) and were not RCTs (82%), unlike in the current meta-analysis. Cairncross and Miller (2016) reported moderate to large positive effects of MBIs on inattentiveness and hyperactivity–impulsivity, also with the majority of studies utilizing a single-subject design. The present study is the first meta-analysis with controlled studies investigating the effect of MBIs on inattentive and hyperactive–impulsive behavior in early and middle childhood with a pre-post change design.
The effect of MBIs on inattentive and hyperactive–impulse behavior was heterogeneous. As suggested by Borenstein et al. (2011), the characteristics of the included study designs were analyzed as moderators. Regarding study designs, results indicated similar small-sized significant positive effects within RCTs allocated on an individual level and quasi-experimental studies (allocated on a group level). Interestingly, Dunning et al. (2018) found that MBIs have a beneficial effect on negative behavior (e.g., aggression, hostility, etc.) and attention (not just inattentive behavior) among youth, but this effect disappeared in the case of negative behavior, and became tendency level in case of attention when they assessed the effects in studies that compared the effect to active control conditions. Our results demonstrated significant small positive effect sizes in studies using active control and medium-sized effects in studies using passive control groups, which tendency is relatively concurrent to the results of the meta-analysis by Dunning et al. (2018).
Moderator analyses about the individual characteristics of children revealed that children at risk for such behavior problems showed a medium-sized effect, while non-at-risk groups indicated a small-sized effect. However, findings revealed that this difference was nonsignificant, thus samples at risk did not benefit significantly more from MBIs than non-at-risk samples. More specifically, studies with socioeconomically disadvantaged children showed a significant moderate-sized positive effect, while studies with typically developing children from middle and/or high SES showed a small positive average effect. In the two studies that tested MBIs with ADHD children, the effect was positive, medium-sized, and significant. Another study including children with dyscalculia, in contrast, found a significant, large positive effect (Akbari et al., 2014). These are promising preliminary results, but further research is warranted regarding the potential of MBIs for children with neurodevelopmental disorders.
From other individual characteristics, the effect of children’s age was also investigated and showed a nonsignificant moderator effect regarding the efficacy of MBIs to decrease inattentiveness and hyperactive–impulsive behavior. This finding showed that MBIs could be efficiently implemented from an early age, such as 3 years, until elementary school. Given that this meta-analysis aimed to fill the gap in previous literature and put a special focus on investigating the efficacy of MBIs from an early age, this is an important finding.
Interestingly, the average effect of MBIs based on teachers’ rating of children’s behavior was significant, positive, and moderate in size, while nonsignificant effects appeared when reports of parents and the children themselves were assessed. Similarly, Klingbeil et al. (2017) also showed a nonsignificant effect size regarding self-reports. Unlikely, Chimiklis et al. (2018) reported a significant effect of MBIs when rated by the parents, whereas this effect was heterogeneous and moderated by the length of the intervention and former ADHD diagnosis, with longer interventions and former ADHD diagnosis indicating a larger effect size. One explanation for the absence of parent- and self-perceived efficacy of MBIs could be that all MBIs from the selected studies were implemented in a (pre-)school setting, and teachers were mostly non-blind for group assessment. Additionally, in approximately half of the MBIs, the teachers were the ones giving children the intervention and reporting on their behavior, which might be a serious source of expectation bias. Furthermore, there might be a chance that MBIs in education provided by teachers are changing teachers’ perceptions of children more than they are changing children’s behaviors. Another possible explanation might be that hyperactivity–impulsivity and inattention can be more striking in the school environment, where high levels of sustained attention, regulation of behavior, and delay of impulses are required. Also, teachers might also be more professional and objective in observing children’s behavior than parents or the children themselves. This is supported by the longitudinal study of Verhulst et al. (1994) where teacher’s reports about behavioral problems were more accurate predictors of poor outcomes in the future than parent’s observations.
Results also indicate that MBIs can be similarly efficiently implemented by regular teachers as long as reducing inattentiveness and hyperactivity–impulsivity is concerned, however, experts showed a somewhat larger effect size comparing to teachers. These findings are in line with the findings of Maynard and colleagues (2017). Another meta-analysis by Carsley et al. (2018) reported that MBIs facilitated by a teacher had a greater effect at posttest of mental health than those delivered by an outside facilitator, while regarding mindfulness outcomes an outside facilitator was more beneficial.
Implications
Due to their cost-effectiveness and feasibility, MBIs have gained a substantial amount of interest in recent years. This meta-analysis reinforces the rationale for the implication of MBIs in an educational context even from the preschool years. Our findings indicated that teachers can effectively implement MBIs following some training and decrease inattentiveness and hyperactivity–impulsivity in their groups. To the best of our knowledge, this is the first meta-analysis that investigated the moderating effect of the samples’ risk status for behavior regulation problems regarding the efficacy of MBIs, and this finding has very important implications for the practical application of MBIs. According to the results, MBIs on a group level are beneficial for all children in school, but for those who are at risk for attention and impulse control problems these benefits seem to be even somewhat larger. Similarly, Diamond and Lee (2011) also found that children with less developed self-control, such as children from low SES or with low executive function skills or ADHD, gain the most from any intervention which train self-control. These findings might indicate that MBIs could potentially reduce the achievement gap between children and support those who underperform because of attention or impulse control problems.
Another important finding about the implication of MBIs was that the length of the programs did not seem to have an effect on the efficacy of MBIs, which means that even a shorter intervention, such as 3–5 hr, can effectively decrease inattention and hyperactivity–impulsivity among 3- to 12-year-old children.
Limitations and Suggestions for Future Research
First of all, unfortunately statistical power was low for many of the subgroup analyses and meta-regressions, except for at-risk status of the samples and publication status, thus a subgroup comparison was conducted only with these moderators. The analyses of other moderator variables (e.g., leader of intervention, length of MBIs, etc.) were limited to effect sizes.
Although this meta-analysis restricted selection criteria to the inclusion of solely controlled studies with pre-post assessment, the included studies still represent some risk of bias due to methodological issues (see Table 1)—for example, (i) the lack of an active control group in some studies might have led to performance bias and nonspecific treatment effects, (ii) two quasi-experimental studies allocated on a group level reported non-equal groups at pretest, thus the risk of selection bias (Lo et al., 2020; Torres, 2019), while four quasi-experimental studies did not report baseline differences, and (iii) non-blind raters might be influenced by expectancy and detection bias (Higgins et al., 2011). It is important to note that most studies with MBIs failed to report the blinding of outcome assessment.
Finally, although the central question of the present meta-analysis was to change behaviors of inattention and hyperactivity–impulsivity, interestingly, there was only two studies that implemented a mindfulness intervention with a diagnosed ADHD sample. Thus, it is questionable whether the present results can be generalized to children with an ADHD diagnosis. At the same time, the present meta-analysis highlights this gap in the literature and encourages future mindfulness RCT investigations with ADHD samples.
Conclusions
MBIs for children resulted in a small- to medium-sized significant decrease in inattention and hyperactivity–impulsivity depending on whether children were at risk for such behavior problems due to neurodevelopmental or environmental disadvantage (e.g., ADHD, low SES) or not at risk. Importantly, the overall effect was significant and moderate when the informants were teachers, but when parents or the children themselves rated their own behavior, the effects were nonsignificant. Despite the limitations, these results provide additional empirical evidence for the inclusion of MBIs in the school curriculum and the consideration of mindfulness practices as a possible support for the development of attention and impulse control in early and middle childhood (both preschool and elementary school). This is further highlighted by the finding that MBIs are beneficial for children at risk for inattentive and hyperactive–impulsive behavior and non-at-risk children as well. Accordingly, MBIs added to the curriculum might serve as an early intervention to reduce the gap in attention and impulse control skills among disadvantaged and non-disadvantaged children.
Overall, the results highlight the potential of MBIs as classroom interventions, which can be relatively easily added to the curriculum, and can serve as a tool for educators to constructively reduce the widely reported attention and impulse control problems. In the future, further research is needed to investigate the effect of MBIs on other specific behaviors in childhood (e.g., subtypes of anxiety, compulsion, aggressive behavior). These findings would have an important practical relevance especially for interventions embedded in education to decrease behavior problems.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Loránd Eötvös Research Network (project number: LP-2018-21/2018) and the Faculty of Education and Psychology, ELTE Eötvös Loránd University. Zsofia K. Takacs was funded by the Hungarian National Research, Development and Innovation Office [grant number: PD121297].