
Abstract
Objective:
Emerging research suggests that the Covid-19 pandemic has disproportionately and adversely affected children with Attention-Deficit/Hyperactivity Disorder (ADHD). The purpose of this meta-analysis is to consolidate the findings from studies that examined changes in ADHD symptoms from before to during the pandemic.
Method:
Database searches of PsycINFO, ERIC, PubMed, and ProQuest were used to identify relevant studies, theses, and dissertations.
Results:
A total of 18 studies met specific inclusion criteria and were coded based on various study characteristics. Twelve studies examined ADHD symptoms longitudinally and six studies assessed ADHD symptoms retroactively and during the pandemic. Data from 6,491 participants from 10 countries were included. Results indicated that many children and/or their caregivers reported an increase in child ADHD symptoms during the Covid-19 pandemic.
Conclusions:
This review points to a global increase in ADHD symptoms and has implications for the prevalence and management of ADHD during the post-pandemic recovery.
Since the declaration of the Covid-19 pandemic in 2020, global reports abound of increased mental health problems among the world’s children and youth. In the early days of the pandemic, mental health experts expressed concern about their observations of children and families in distress (e.g., Dubicka & Carlson, 2020). As empirical studies ensued, albeit mostly cross-sectional, some early data suggested heightened mental health needs among children and youth in the wake of the Covid-19 pandemic (e.g., Liang et al., 2020; Marques de Miranda et al., 2020; Xie et al., 2020), while other findings pointed to improved child mental health in some domains (e.g., Cost et al., 2022). Over the past 2 years, research examining the impact of Covid-19 on child and youth mental health has been mounting, including longitudinal designs (e.g., Creswell et al., 2021).
Accordingly, researchers have begun to synthesize the findings via systematic reviews and quantitative meta-analyses as more studies have been published. Racine et al. (2021) conducted a meta-analysis on the global prevalence of internalizing symptoms in children and adolescents and found increases in clinically elevated depressive and anxiety symptoms during the first year of the pandemic. Likewise, meta-analytic results by Bussières et al. (2021) showed that child and youth internalizing and externalizing symptoms increased as a result of the pandemic. Meta-analytic findings from early in the pandemic have linked school closures with weakened mental health for students (Viner et al., 2022). The meta-analysis by Ma et al. (2021) using Chinese data suggested that the mental health of girls (compared to boys) and adolescents (compared to younger children) was most adversely affected. Based on the results of their rapid systematic review, Meherali et al. (2021) speculate that, compared to adults, the pandemic is likely to have long-term consequences on children’s and adolescents’ mental health, and point to the need for increased service access.
Simultaneously, studies about the pandemic’s apparent impact on the functioning of children and youth with disabilities, such as those with Attention-Deficit/Hyperactivity Disorder (ADHD), have been emerging from research teams around the globe. Sibley et al. (2021) found that American youth with ADHD reported exacerbated problems with depressive behaviors and school avoidance in the early days of the pandemic. Shuai et al. (2021) studied digital media use in Chinese children with ADHD during quarantine and reported connections with several social-emotional risk factors, such as increased symptom severity, motivational difficulties, executive functioning problems, and family environment problems. Researchers in Italy and Canada found that youth with ADHD struggled more with online learning than their neurotypical peers (Hai et al., 2021; Tessarollo et al., 2022), although researchers in the US did not find this effect (Lupas et al., 2021). Canadian caregivers of children with ADHD reported less healthy lifestyle habits and increased mental health symptoms in their children during the first year of the pandemic (Swansburg et al., 2021). A diagnosis of ADHD in childhood has even been linked with increased likelihood of Covid infection and medical complications from the virus (Merzon et al., 2022).
Despite some studies pointing to a disproportionate impact of the pandemic on children with ADHD, and the recent systematic reviews about its impact on child and youth well-being more broadly, we do not yet know if the prevalence of ADHD symptoms—namely inattention, hyperactivity, and impulsivity—have in fact changed during the past 3 years. In order to inform clinical practice regarding the diagnosis and management of ADHD, trends in symptom presentation need to be statistically explored, particularly using studies that measured symptoms prior to the onset of the pandemic. To that end, the present study employed a meta-analysis to examine changes in ADHD symptoms due to the pandemic. This quantitative review included studies that examined changes in children and adolescents with subclinical and/or clinical levels of ADHD symptoms from before to during the Covid-19 pandemic.
Methods
Literature Search
A systematic literature search was conducted in three databases: PsycINFO, ERIC, PubMed, and ProQuest Theses and Dissertations. Search terms included a variety of medical subject heading (MeSH) terms and keywords. See Appendix for the complete search strategy. The systematic literature search was conducted in November 2022. A total of 803 studies were located, with 517 remaining after duplicates were removed. Articles were uploaded onto Covidence, a systematic review management software.
Study Selection
See Figure 1 for the Prisma flow diagram of the study selection process. Study titles and abstracts were screened using predetermined inclusion and exclusion criteria. The second phase of screening required a full-text review of the 180 remaining studies, and 18 studies met all inclusion and exclusion criteria and remained for the final sample of studies.
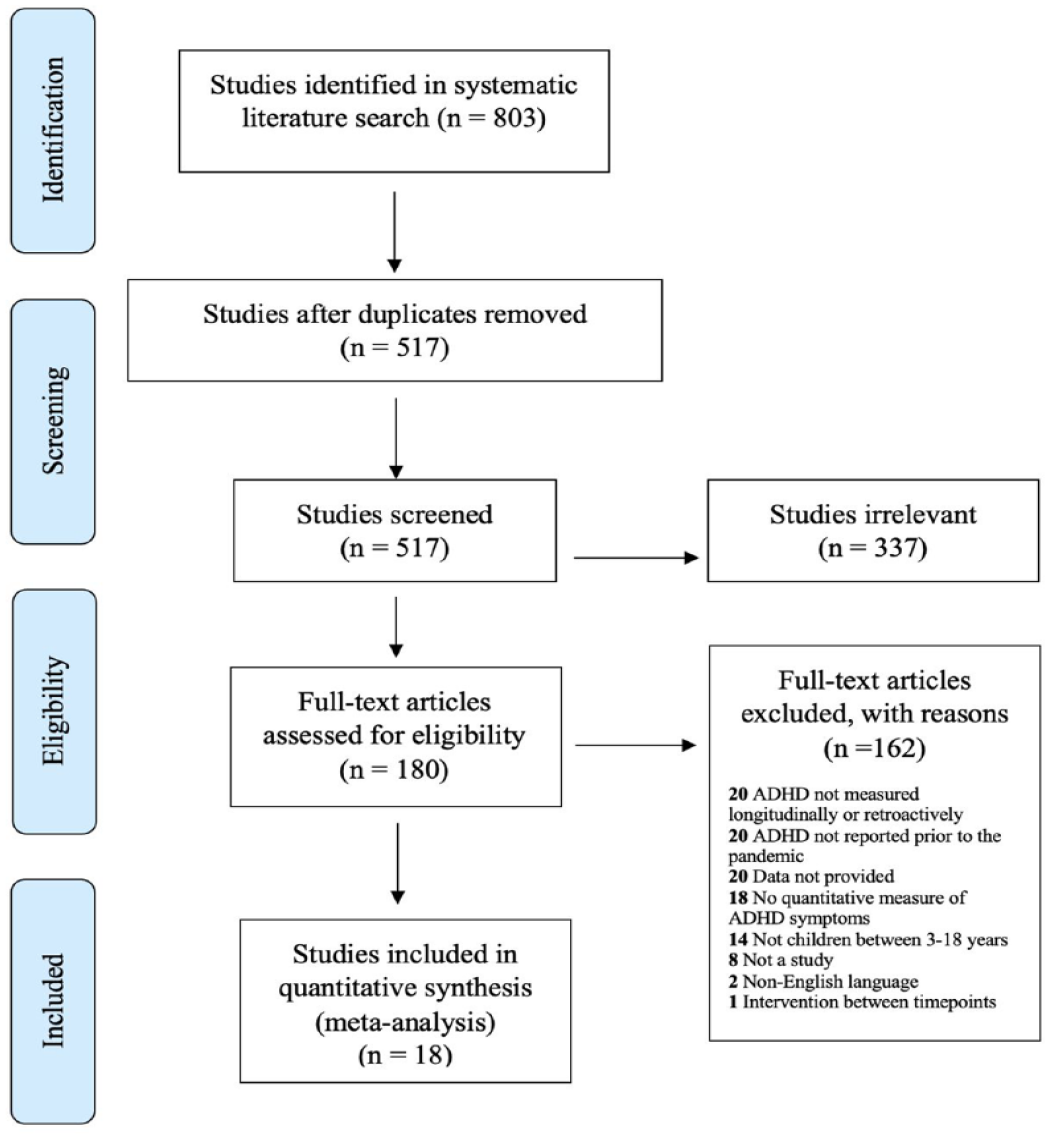
Selection process of studies using the PRISMA flow diagram.
Inclusion/Exclusion Criteria
Study must report on child hyperactivity and/or inattention symptoms with a quantitative measure from at least one informant (i.e., child, parent).
- Study must include at least one timepoint reporting ADHD symptoms prior to the start of pandemic (prior to March 2020) OR include a retroactive report of ADHD symptoms from before the pandemic (prior to March 2020).
- Study must include at least one timepoint reporting ADHD symptoms after the start of the pandemic (after March 2020).
- Study participants must be children between the ages of 3 and 18 years old (i.e., pre-school level to grade 12).
- Study must provide appropriate statistical information (i.e., means, standard deviations, sample size) or other sufficient data to calculate the chosen effect size.
- Study must be written in the English language.
- Study must be an empirical, primary source (manuscripts, dissertations and theses only).
Study Coding
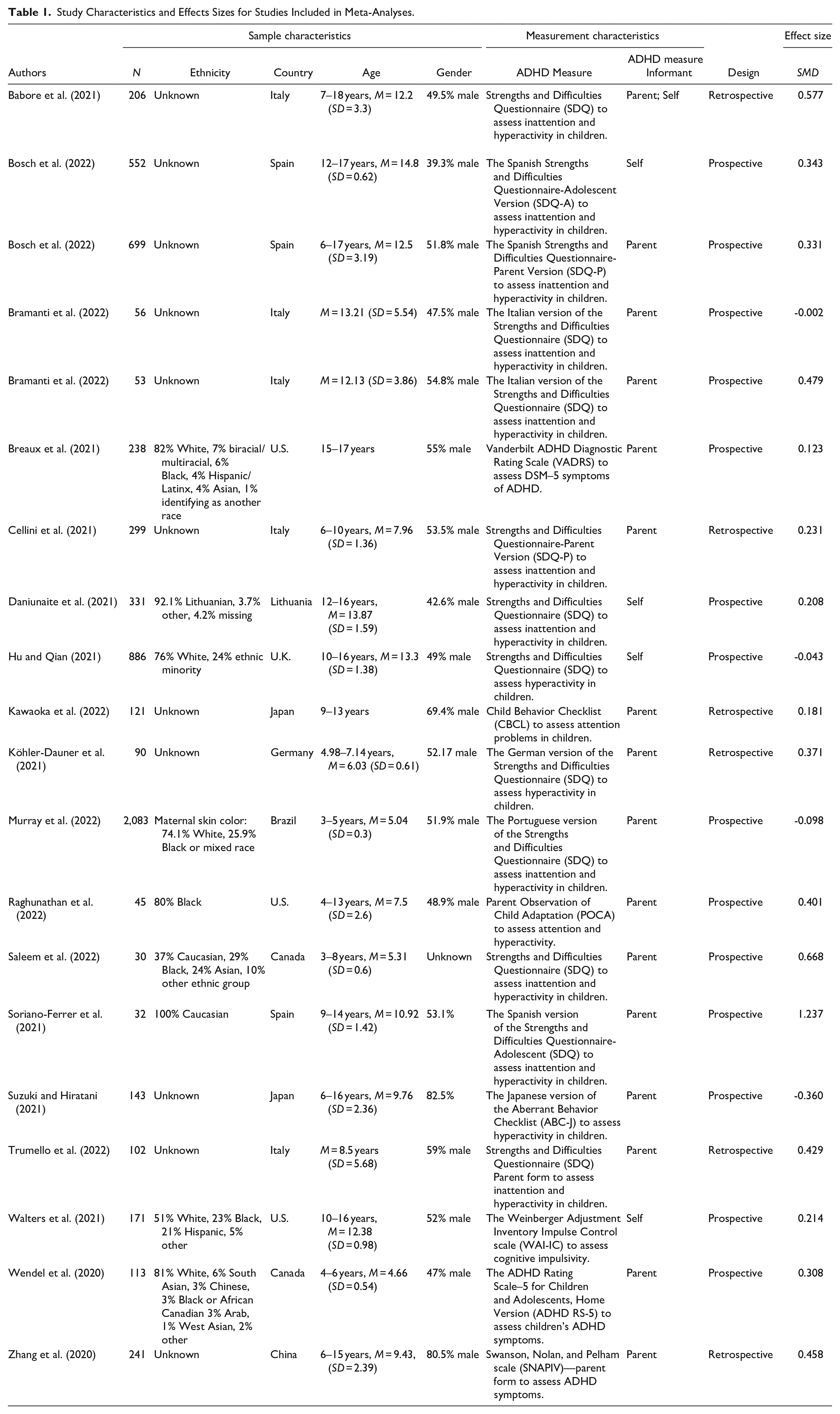
See Table 1 for study characteristics. The final set of studies was coded for a variety of sample and methodological characteristics. Studies were coded across five categories, these include: sample characteristics (e.g., gender, sample size), measurement characteristics (e.g., measure used, informant), design characteristics (e.g., cross-sectional vs. longitudinal), source characteristics (e.g., publication status, year of publication), and study quality (i.e., three items extracted from the Quality Assessment Tool for Diverse Designs; Sirriyeh et al., 2012). To establish inter-rater reliability, a research assistant coded a subset of studies (<20%). There was excellent inter-rater reliability (98%), indicating high agreement between raters.
Study Characteristics and Effects Sizes for Studies Included in Meta-Analyses.
Sample Characteristics
The final sample of studies included 18 published studies and a total of 6,491 participants. Twelve studies measured ADHD symptoms longitudinally and six studies measured ADHD symptoms retrospectively. Two studies (Bosch et al., 2022; Bramanti et al., 2022) each included two separate samples of children, resulting in a total of 20 effect sizes for analysis. Sample sizes ranged from 30 children to 2,083 children and the mean sample size across all studies was 325 children. Each study was coded to determine the reporting quality using three items (i.e., clear description of research setting, detailed description of data collection procedure, statistical assessment of reliability and validity of measurement tools). Ten studies (55%) met all three criteria for study quality indicating high-quality reporting and the remaining eight studies (45%) met two out of three criteria.
Meta-Analytic Procedure
One meta-analysis was conducted using the third version of the Comprehensive Meta- Analysis (CMA) software (Borenstein et al., 2013). The Standardized Mean Difference (SMD), also known as Cohen’s d, was selected as the effect size of choice. This is because the final set of studies reported data pertaining to the difference in means (i.e., pre and post means and measures of variance, t-test results), reducing the need to transform data for other types of effect sizes. SMD’s are interpreted as small if d = 0.2 to 0.5, medium if d = 0.5 to 0.8, and large if d > 0.8 as per Cohen’s (1988) recommendations.
One study (Zhang et al., 2020) provided paired sample t-test results, three studies (Bosch et al., 2022; Daniunaite et al., 2021; Murray et al., 2022) provided pre and post means with associated correlations, and 14 studies provided pre and post means with paired sample t-test results. All data from studies was transformed into the SMD using the CMA software. A random effects model was used for the meta-analysis since we assumed that the variability between studies is a result of sampling error and other influencing factors (e.g., age, gender, types of measures; Borenstein et al., 2010; Card, 2011). Additionally, results computed from random effects models are more generalizable since the model assumes that effect sizes are distributed normally, rather than assuming there is one true effect for all studies. Studies are also weighted more evenly in random effects models (Borenstein et al., 2010). To meet the assumption of independence of effect size, each study sample was only represented once by averaging and combining data within studies (Card, 2011). For example, when a study provided mean differences for both inattention and hyperactivity scores (i.e., Wendel et al., 2020), we used the CMA software to combine these effect sizes and ensure the study sample provided only one effect size in the meta-analysis. This process was required for three studies.
Publication Bias
Literature indicates that studies with large effect sizes are more likely to be published than studies presenting smaller or non-significant effect sizes (Borenstein et al., 2011; Card, 2011). To avoid publication bias, a systematic search of Proquest Theses and Dissertations was conducted to access unpublished works; however, no unpublished manuscripts remained in the final sample of studies.
Publication bias was addressed using two methods: Egger’s regression test (Egger et al., 1997) and Rosenthal (1979). Egger’s regression test measures the association between effect size estimates and sample sizes, relative to statistical power (Card, 2011). Rosenthal’s Failsafe N assesses the robustness of the meta-analysis by providing the number of studies (with effect sizes of zero) required to lower the overall effect size to a non-significant level (Card, 2011). Rosenthal’s failsafe N must be equal to 5(k) + 10 (k = number of studies) to be confident no publication bias exists.
Moderator Analyses
Moderator analyses examined gender and age of study participants to evaluate any moderation of the potential change in ADHD symptoms. These individual characteristics warrant further investigation because extant research documents important differences in behavior. That is, boys tend to display more hyperactive ADHD presentations (Slobodin & Davidovitch, 2019), whereas girls tend to experience more inattentive presentations and their symptoms are often less apparent. Moreover, ADHD symptoms in young children typically involve more hyperactivity and conduct problems, whereas older children tend to experience a decrease in severity of symptoms but experience more comorbid issues (Young & Amarasinghe, 2010). To assess potential methodological effects, report informant and study design are included as moderators. Existing literature indicates key differences in terms of reporting ADHD symptoms (parent vs. self-report; Achenbach et al., 1987). Retrospective recall studies introduce concerns in terms of reliability of reporting and it is important to identify any differences found between studies using this method and longitudinal reporting. Finally, sample types present potential method effects if studies are only reporting ADHD symptoms for children diagnosed with ADHD rather than populations that include children with and without ADHD. Importantly, most included studies consisted of children with a range of ADHD symptoms (community samples). There were not enough studies that included other types of samples (clinical samples) to include sample type as a moderator.
Four moderator analyses were conducted, and each moderator level included at least three studies (Borenstein et al., 2011). A fixed-effects model was selected for one moderator analysis (i.e., report informant) because there were fewer than five studies in the self-report level of the moderator (Hedges & Vevea, 1998). While the small number of studies included in this specific moderator lowers the power of the analysis, using a fixed-effects model amplifies the power but presents limitations in terms of generalizability (Borenstein et al., 2010). A mixed-effects model was used for the other three moderator analyses.
Results
Figure 2 includes the full distribution of computed effect sizes and the summary effect (located at the bottom of the figure). The 20 effect sizes ranged from −.360 to 1.237. The summary effect is listed on the final row of the figure and indicates a small, significant and positive SMD for ADHD symptoms from before to during the pandemic [d = 0.270 (95% Cl. 0.158 < d < 0.382), Z = 4.723, p < .001]. That is, children experienced an increase in ADHD symptoms during the pandemic.
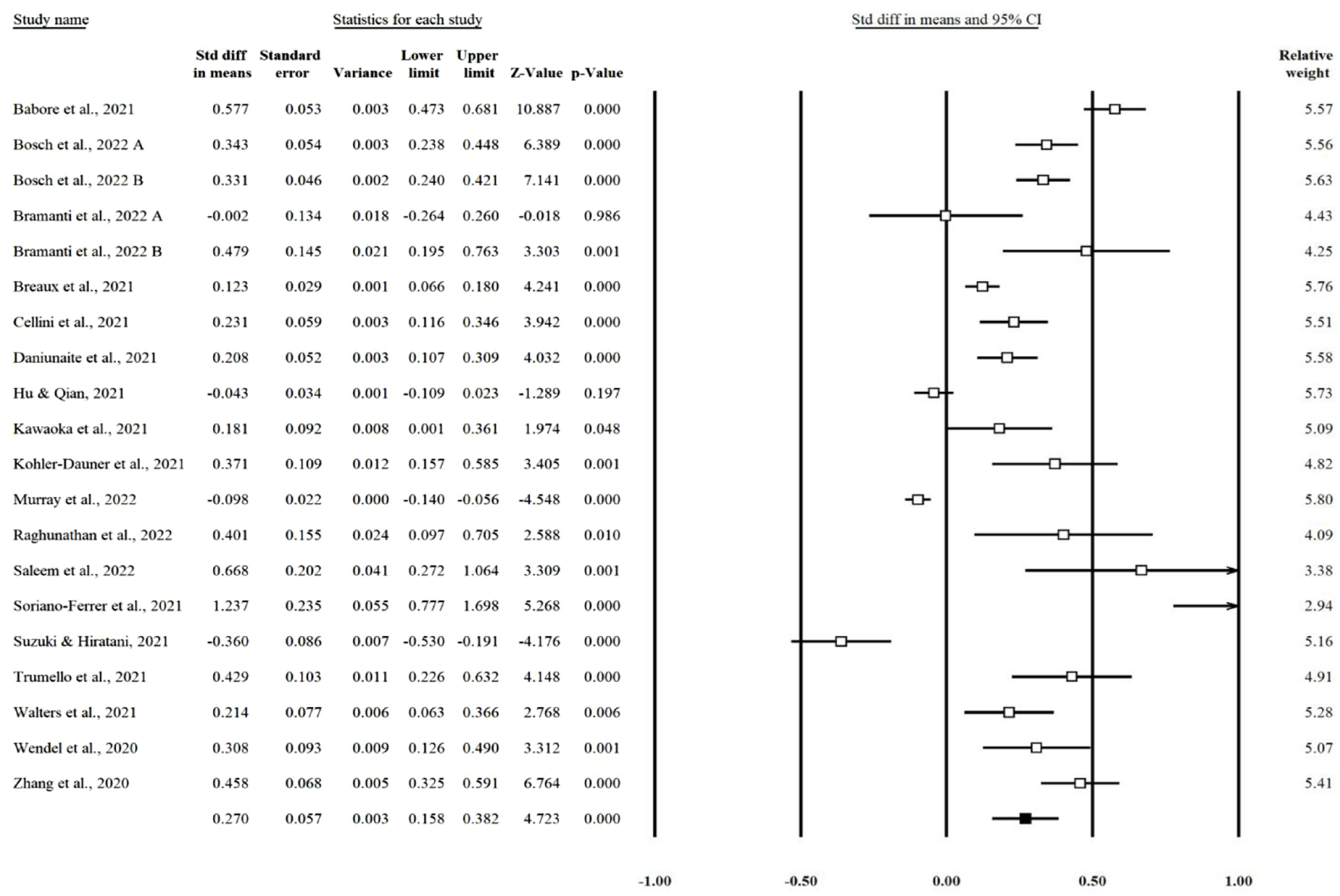
Distribution of effect sizes and summary effect for the meta-analysis.
There was true variability between study effect sizes as indicated by the significant test for homogeneity of variance [Q (19) = 361.005, p < .001]. The I2 index was 94.737%, which suggests that the sample of studies had a large proportion of variance due to factors other than sampling error.
Publication Bias
Egger’s linear regression was significant (p = .004), which indicates that publication bias may be present in the final sample of studies. However, Rosenthal’s Failsafe N was 162, above the threshold of 100 studies and does not indicate compelling evidence for publication bias.
Moderator Analyses
Gender
A meta-regression moderator analysis was used to assess whether gender moderates the change in ADHD symptoms. The proportion of males in each study sample was used and did not have a significant moderating effect (β = –.5303, p = .3137; Q = 1.02).
Age
Given the large range of ages within the included studies, age was entered as a moderator to assess its potential effect on the change in ADHD symptoms. Age was separated into three categories: below 10 years old, above 10 years old and all ages. We categorized age in this way to account for developmental differences that occur when children shift into adolescence (American Psychiatric Association [APA], 2013) and because of how the included studies grouped students together (i.e., 6–10, 12–17, 4–13 years). The results showed no significant moderating effect for age (Q = 1.612, p = .447).
Study Design
Study design was entered as a moderator to identify a potential methodological effect. Studies were categorized as prospective (e.g., longitudinal) if they included two separate reports (one timepoint prior to the pandemic and one timepoint during the pandemic), and retrospective (e.g., cross-sectional) if the study included a recall report of ADHD symptoms prior to the pandemic and a report during the pandemic. No moderating effect was found for ADHD symptoms (Q = 2.421, p = .120) between prospective and retrospective studies.
Report Informant
Informant for ADHD symptoms was entered as a moderator to assess another potential methodological effect on the change in ADHD symptoms. We divided report informants into two categories: caregiver informant and self-report. No moderating effect was found for the increase in ADHD symptoms (Q = 1.009, p = .315) between caregiver informants and self-reports.
Discussion
Through a meta-analysis of extant studies, this study aimed to identify patterns of change in ADHD symptomology for children and youth from before to during the Covid-19 pandemic. Results from an amalgamation of 6,491 participants suggest that the pandemic has had a significant and exacerbating effect on the presentation of inattention, hyperactivity and/or impulsivity in children and adolescents, but the overall size of this effect was small. To an extent, these findings support the large body of emerging evidence that children’s mental health and behavioral functioning has been adversely impacted during the Covid-19 pandemic.
Due to the time-sensitive nature of the studies included in this review, 18 published studies were included. Nonetheless, there are several methodological strengths of this timely review that permit confidence in the conclusions. First, the review included data with ratings of pre-pandemic and mid-pandemic reports of ADHD symptoms—either via longitudinal data collection or through retrospective reports—as well as a statistical change score. This helps address the known shortcomings of many Covid-related cross-sectional studies (Vaillancourt et al., 2021) which have limited conclusions about change. Despite the inclusion of retrospective reports, an examination of 12 longitudinal studies (i.e., with pre-pandemic data collection) with 5,432 children showed an increase in the ADHD symptoms measured. Interestingly, three longitudinal studies (Hu & Qian, 2021; Murray et al., 2022; Suzuki & Hiratani, 2021) did not report an increase in ADHD symptoms. Thus, despite the inclusion of studies with discrepant findings, the results still indicate a significant effect overall. Further, the moderator results for study design type indicated no significant differences between studies that used longitudinal reports and retrospective reports.
This meta-analysis included data from several regions around the world using diverse samples: USA, Canada, Italy, Spain, Brazil, Lithuania, Germany, China, Japan, and the United Kingdom. Moreover, the sample consisted of data about a diverse group of children—although nine studies did not include ethnicity data, the remaining studies included data from families self-identifying as White, Black, Hispanic, European, Chinese, South Asian, Arab, West Asian, biracial, multiracial, or other ethnic minorities. Unfortunately, sufficient data was not reported in the studies to conduct moderator analyses for ethnicity or minority status. Nonetheless, the inclusion of a heterogenous sample suggests that the findings may apply to a broad group of children from differing backgrounds.
In order to draw conclusions from meta-analyses, it is important that study quality is carefully evaluated. Our three-pronged approach to assessing study quality for inclusion (i.e., clear description of research setting, detailed description of data collection procedure, statistical assessment of reliability and validity of measurement tools) revealed that 55% of the included studies met all three criteria, and the remaining 45% met two out of three criteria for quality. Importantly, all the included studies used a well-validated measure of ADHD symptoms, such as the Strengths and Difficulties Questionnaire (SDQ), and two time points or retroactive reports. While the included studies did not report on their attrition rates, many of the studies only included participants who completed both time points. Finally, the included studies had large sample sizes with diverse socio-demographic characteristics, resulting in a heterogenous sample of over 6,000 children from different regions around the world. It is evident that the studies included in this meta-analysis were methodologically rigorous and include a diverse population of participants.
The results from this meta-analysis suggest that the increase in ADHD symptoms was not affected by child gender or child age. It will be important to further explore these differences in future research, given the limitations of our moderator analyses. The moderator analyses assessing methodological aspects (i.e., study design, report informant) were also not significant, indicating that the increase in ADHD symptoms remains consistent regardless of study design or informants used in this samples.
Limitations
The majority of studies included in this meta-analysis had limited demographic information available (e.g., sample ethnicity, ADHD presentation, age groupings, attrition rates) which limits the ability to identify factors that may be contributing to the increase in ADHD symptoms. It will be important that future studies provide more detailed information about their samples to permit in-depth systematic reviews. While four moderator analyses were conducted, a significant amount of heterogeneity among effect sizes remains unexplained. Lastly, although steps were taken to eliminate publication bias, Egger’s linear regression was significant, indicating the possibility of publication bias within the final set of studies. There is a risk of publication bias in any meta-analysis (Borenstein et al., 2011) and this bias can lead to overestimating the size of the summary effect (Borenstein et al., 2011; Card, 2011).
Despite these limitations, given the high-quality studies included in this meta-analysis, and the statistical effect sizes observed, we can conclude that there appears to be a global increase in ADHD symptoms as a result of the Covid-19 pandemic. Decades of pre-pandemic research have illustrated adverse effects of childhood ADHD symptoms on social (i.e., Ros & Graziano, 2018), familial (i.e., Zhao et al., 2019), and academic functioning (i.e., Lawrence et al., 2021). We may indeed see an increase in prevalence rates of ADHD diagnoses in the coming years, which will have direct impacts on service delivery. Given the known risks associated with an ADHD diagnosis, it is important the clinicians working with children and youth and ADHD researchers are aware of this global increase resulting from the Covid-19 pandemic.
Supplemental Material
sj-docx-1-jad-10.1177_10870547231158750 – Supplemental material for ADHD Symptoms Increased During the Covid-19 Pandemic: A Meta-Analysis
Supplemental material, sj-docx-1-jad-10.1177_10870547231158750 for ADHD Symptoms Increased During the Covid-19 Pandemic: A Meta-Analysis by Maria A. Rogers and Jaidon MacLean in Journal of Attention Disorders
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.