
Abstract
As global populations age, identifying modifiable factors to enhance later-life well-being is vital. Self-perceptions of ageing (SPA), internalised beliefs about one’s ageing, may shape psychological well-being (PWB). We synthesised 33 studies (n = 43,556). Random-effects models showed that more positive SPA related to higher PWB (pooled r = .35; I2 ≈ 89%). By domain: hedonic r = .24 (95% CI .09–.37); eudaimonic/relational r = .26 (95% CI −.50–.80; small k); self-evaluation r = .07 (95% CI −.41–.53); mental ill-health r = .21 (95% CI −.05–.44). Because higher mental-illness scores denote worse outcomes, the positive coefficient indicates an inverse relation (more positive SPA, less distress). Univariable moderators suggested stronger effects in Europe, larger SPA–hedonic associations with higher sample % married, and larger self-evaluation effects in longitudinal designs; none remained significant in the multivariable model. Findings position SPA as a culturally sensitive target for improving later-life well-being.
Keywords
Introduction
Population ageing is accelerating worldwide. By 2050, one in six people will be aged 65 years and above, while those aged 80 years and above will more than triple to 426 million (United NationsDepartment of Economic and Social AffairsPopulation Division, 2022). How individuals interpret this demographic shift and their ageing, whether as an opportunity or decline, shapes their behaviour, physiology, and ultimately their health trajectories. These subjective interpretations, known as self-perceptions of ageing (SPA), encompass the beliefs, expectations, and feelings individuals hold about their ageing process.
Theoretical Foundations
The Stereotype Embodiment Theory (SET; Levy, 2009) is the dominant explanatory framework, proposing that age stereotypes are absorbed in childhood, internalised across adulthood, and ultimately embodied as self-relevant cognitions that influence health via behavioural, psychological, and physiological pathways. Longitudinal evidence supports this model: positive SPA predict greater longevity (+7.5 years; Levy et al., 2002), faster functional recovery post-hospitalisation (Hill, 2025), and lower cortisol reactivity to stress (Levy et al., 2009), whereas negative SPA accelerate cognitive decline (Zisberg et al., 2024) and elevate mortality risk (Levy et al., 2009).
Complementary frameworks extend SET’s scope. The Awareness of Age-Related Change model (AARC; Diehl & Wahl, 2010) emphasises the dynamic self-monitoring of age-related gains and losses, predicting stronger links between perceived losses and reduced well-being. Terror Management Theory (Greenberg et al., 1990) explains affective defensive responses when ageing stereotypes trigger mortality awareness, illuminating potential SPA–anxiety pathways. The Motivational Theory of Life-Span Control (Heckhausen et al., 2010) emphasises perceived control as a mediator of SPA and well-being associations, a mechanism supported empirically (Yao et al., 2023). Together, these perspectives underline that SPA are culturally embedded yet fluid across adulthood.
Why is This Review Needed?
Prior syntheses of self-perceptions of ageing (SPA) and psychological well-being (PWB) have often treated PWB as a single, undifferentiated construct, combining a wide range of outcomes into one measure. This approach risks obscuring important domain-specific mechanisms. Building on Diener and Ryan (2009) and Ryff and Keyes (1995), we adopt a four-domain conceptualisation of psychological well-being (PWB) to avoid obscuring domain-specific mechanisms. The first domain, mental ill-health, encompasses indicators of psychological distress such as depression, anxiety, loneliness, and perceived stress (Kessler et al., 2007; WHO, 2018). The second, hedonic well-being, encompasses subjective evaluations of life, including life satisfaction, happiness, and positive affect (Diener et al., 1999). The third, eudaimonic/relational well-being, captures meaning, purpose, autonomy, and social resources (e.g., resilience, perceived social support; Keyes, 2002; Huta, 2013; Holt-Lunstad, 2018; Umberson & Karas Montez, 2010). The fourth, self-evaluation, reflects self-referent appraisals central to identity and self-concept (e.g., self-esteem, self-rated health, physical self-worth; Rosenberg, 1965; Idler & Benyamini, 1997; Fox & Corbin, 1989). Treating self-evaluation as a distinct domain is theoretically defensible and empirically warranted given its prominence in the literature and potential mechanisms linking SPA to self-concept maintenance and control beliefs in later life (Diehl & Wahl, 2010; Heckhausen et al., 2010). Disaggregating these domains enables clearer tests of whether SPA differentially relates to positive states (hedonic/eudaimonic), self-appraisal processes (self-evaluation), and the absence of distress (mental ill health).
Although the relationship between SPA and PWB has been examined in previous reviews, significant limitations remain in the existing literature. Warmoth et al. (2016) restricted their synthesis to mental health outcomes (k = 14; studies up to 2015), while Chang et al. (2025) and Chang (2024) focused on physical health outcomes (k = 23). Löckenhoff et al. (2009) examined cognitive outcomes (k = 17). In cases where PWB was included, it was almost always treated as a single, aggregated construct without differentiating between domains. Moreover, none of these earlier reviews considered socio-demographic moderators such as gender, marital status, or geographical region, nor did they systematically compare cross-sectional and longitudinal designs. Collectively, their analyses drew on a combined total of 54 primary studies, of which only six were published after 2015, leaving a substantial body of recent research unexamined.
The current review addresses these gaps by synthesising evidence from an updated search covering January 1990 to June 2025, yielding 30 eligible studies. Notably, 40% of these were published within the past five years, and 20% employed longitudinal designs. This is the first review to explicitly disaggregate PWB into hedonic, eudaimonic, and mental ill-health domains; examine key moderators including gender, marital status, geographical region, and study design; and apply robust variance estimation to account for statistical dependence among multiple effect sizes. In doing so, it advances both theoretical understanding and methodological rigour, offering a more precise account of how SPA relates to different facets of well-being in later life.
Objectives
This review, registered with PROSPERO (CRD42024587494) and following PRISMA 2020 guidelines, addresses the following. (1) Quantify associations between SPA and each PWB domain in adults aged ≥60 years. (2) Compare domain-specific associations using random-effects meta-analysis. (3) Model moderation by gender, marital status, geographical region, and study design. (4) Identify gaps to inform interventions promoting positive SPA and healthy ageing.
Methods
Eligibility Criteria
Studies were eligible for inclusion if they examined the association between self-perceptions of ageing (SPA) and psychological well-being (PWB) in adults aged 60 years or older. We restricted inclusion to participants aged 60 years and above, aligning with WHO guidelines and recognising that embodiment effects intensify once individuals self-identify as “older” (Kornadt et al., 2018). Extensive ageing studies (e.g., HRS, ELSA, SHARE) often recruit from age 50 and above, but our threshold captures the population most relevant to ageing-related interventions.
Psychological well-being was operationalised across four distinct domains: (1) mental ill-health, including indicators such as depression, anxiety, loneliness, and perceived stress; (2) hedonic well-being, including life satisfaction, happiness, and positive affect; (3) eudaimonic/relational well-being, including meaning in life, autonomy, resilience, and perceived social support; and (4) self-evaluation, including self-esteem, self-rated health, and physical self-worth.
Eligible study designs comprised cross-sectional and longitudinal observational studies conducted in any geographical region. Only quantitative studies reporting a Pearson correlation coefficient (r) or sufficient statistical information to compute r were included. Intervention studies, qualitative designs, systematic or narrative reviews, conference abstracts without extractable data, and studies with a mean sample age below 60 years were excluded.
Search Strategy and Study Selection
A comprehensive search of EBSCOhost, ScienceDirect, Web of Science, Scopus, and Google Scholar was conducted from inception to June 2024, using a combination of terms related to SPA (e.g., “self-perceptions of aging,” “subjective age,” “attitudes toward own aging”) and PWB outcomes (e.g., “life satisfaction,” “depression,” “self-esteem”). Reference lists of included studies and relevant reviews were hand-searched to identify additional eligible articles.
Titles and abstracts were screened independently by two reviewers, followed by a full-text review of potentially relevant articles. Full-text eligibility was assessed against the predefined inclusion criteria. When a study reported multiple SPA–outcome correlations, each effect was mapped a priori to one of the four PWB domains using pre-specified coding rules before analysis.
Data Extraction
Data extraction was carried out independently by two reviewers (L.E.U & ESI) using a structured form. Extracted information included: study authors and year, country, sample size, mean age and standard deviation, percentage of female participants, percentage married, study design (cross-sectional or longitudinal), SPA measurement tool (e.g., Brief Aging Perceptions Questionnaire [B-APQ], Attitudes to Ageing Questionnaire [AAQ], Attitude Toward Own Ageing [ATOA], subjective age), PWB measurement tool(s), Pearson’s r values (or convertible statistics), and corresponding 95% confidence intervals (CIs).
When gender composition (% female) or marital status (% married) data were missing, this was recorded as “N/A” and retained in descriptive tables to provide transparency. For moderators in meta-regression, analyses were conducted only on the subset of studies reporting the relevant variable, with explicit acknowledgement of reduced sample size and potential bias in interpretation.
Quality Assessment
The methodological quality of included studies was evaluated independently by two reviewers using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Analytical Cross-Sectional and Cohort Studies, as appropriate. Discrepancies were resolved through discussion or a third reviewer.
Statistical Analysis
All analyses were performed in Comprehensive Meta-Analysis (CMA, version 4). Effect sizes (r) were transformed to Fisher’s z for pooling and back-transformed for interpretation. Random-effects models were used, given expected heterogeneity in populations, settings, and measures. Heterogeneity was assessed with Cochran’s Q, the I2 statistic, and τ2 estimates.
Moderator analyses were conducted using mixed-effects meta-regression for continuous moderators (e.g., % female, % married) and subgroup analysis for categorical moderators (e.g., geographical region, study design). For gender composition (% female), results were interpreted with caution due to the limited explanatory power of a single demographic variable and the absence of notable visual trends in the corresponding meta-regression plot. For marital status (% married), the analysis was restricted to studies with available data, and missingness was noted as a source of potential bias. Publication bias was assessed via funnel plot inspection, Egger’s test, and Duval and Tweedie’s trim-and-fill method.
We evaluated moderators in two tiers. First, we ran subgroup analyses for categorical moderators and univariable meta-regressions for continuous moderators. Second, we fit a combined (multivariable) mixed-effects meta-regression model that includes all prespecified moderators simultaneously. Because the multivariable model uses listwise deletion, the number of studies (k) is smaller than in univariable models; estimates can therefore attenuate due to reduced power and covariate intercorrelations. We treat moderator findings as exploratory.
Study Selection
A total of 33 studies met the inclusion criteria and were included in this systematic review and meta-analysis. The initial database search yielded 3,426 records. After removing duplicates, 2,6001 unique titles and abstracts were screened out. Following a full-text assessment of 203 articles, 33 studies met the inclusion criteria. The PRISMA flow diagram outlines the study selection process (Figure 1). PRISMA Flow Diagram. Note: A- Studies that did Not Measure Either Perceptions of Ageing (SPA) or Psychological Well-Being (including Related Constructs Such as Life Satisfaction, Resilience, Social Support, or Mental Health Outcomes). b- Studies Whose Primary Focus or Intervention was Unrelated to Perceptions of Ageing (e.g., General Geriatric Care, Unrelated Health Behaviours) Even if Older Adults Were Included. c- Studies Published in Languages Other than English, for which No Reliable Translation was Available. d- Studies Conducted in Samples Outside the Target Population of Adults Aged ≥60 years or Those Focused Exclusively on Clinical Subgroups Not Relevant to the Review Scope (e.g., Dementia-specific Samples when Not Addressing SPA)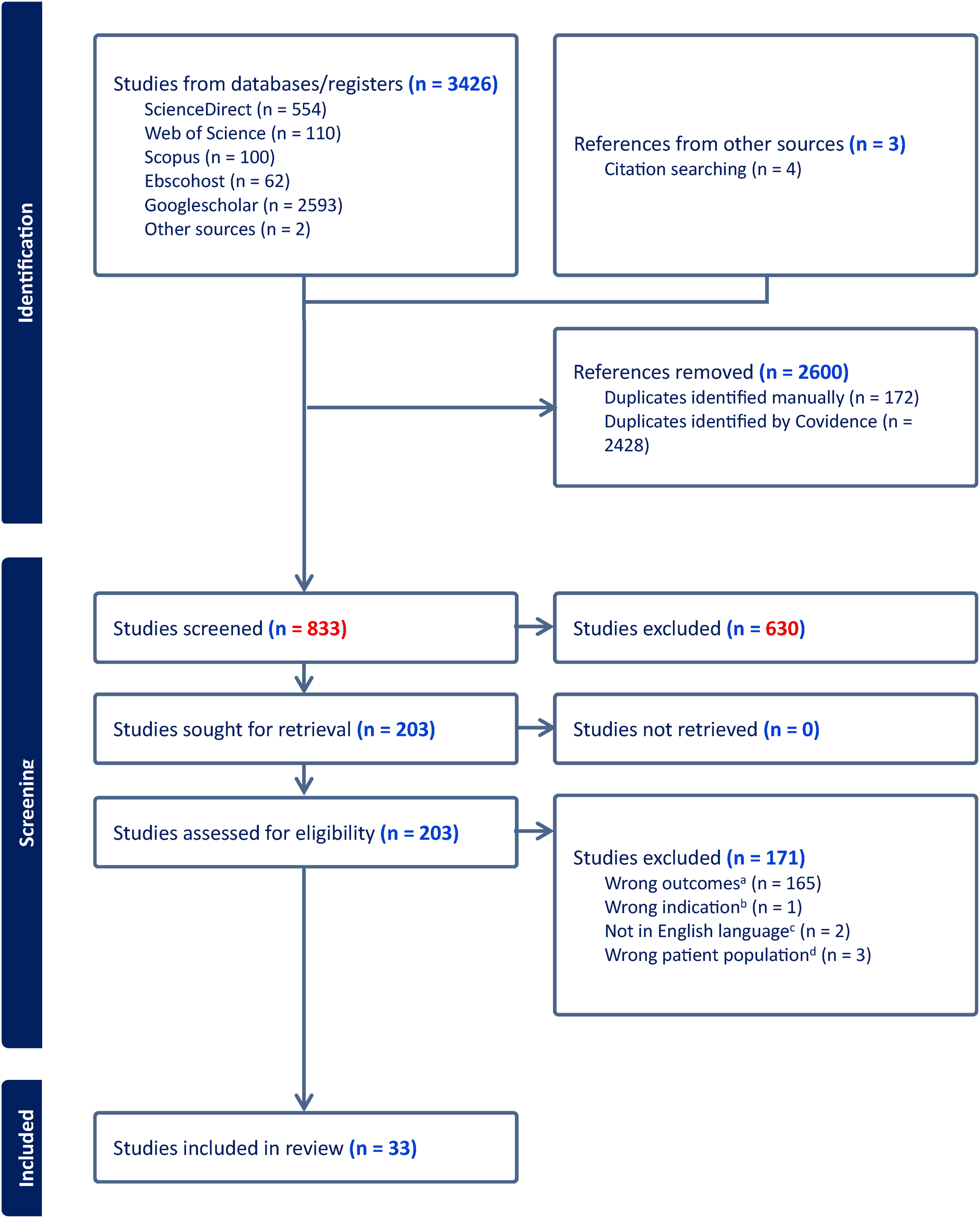
Characteristics of Included Studies
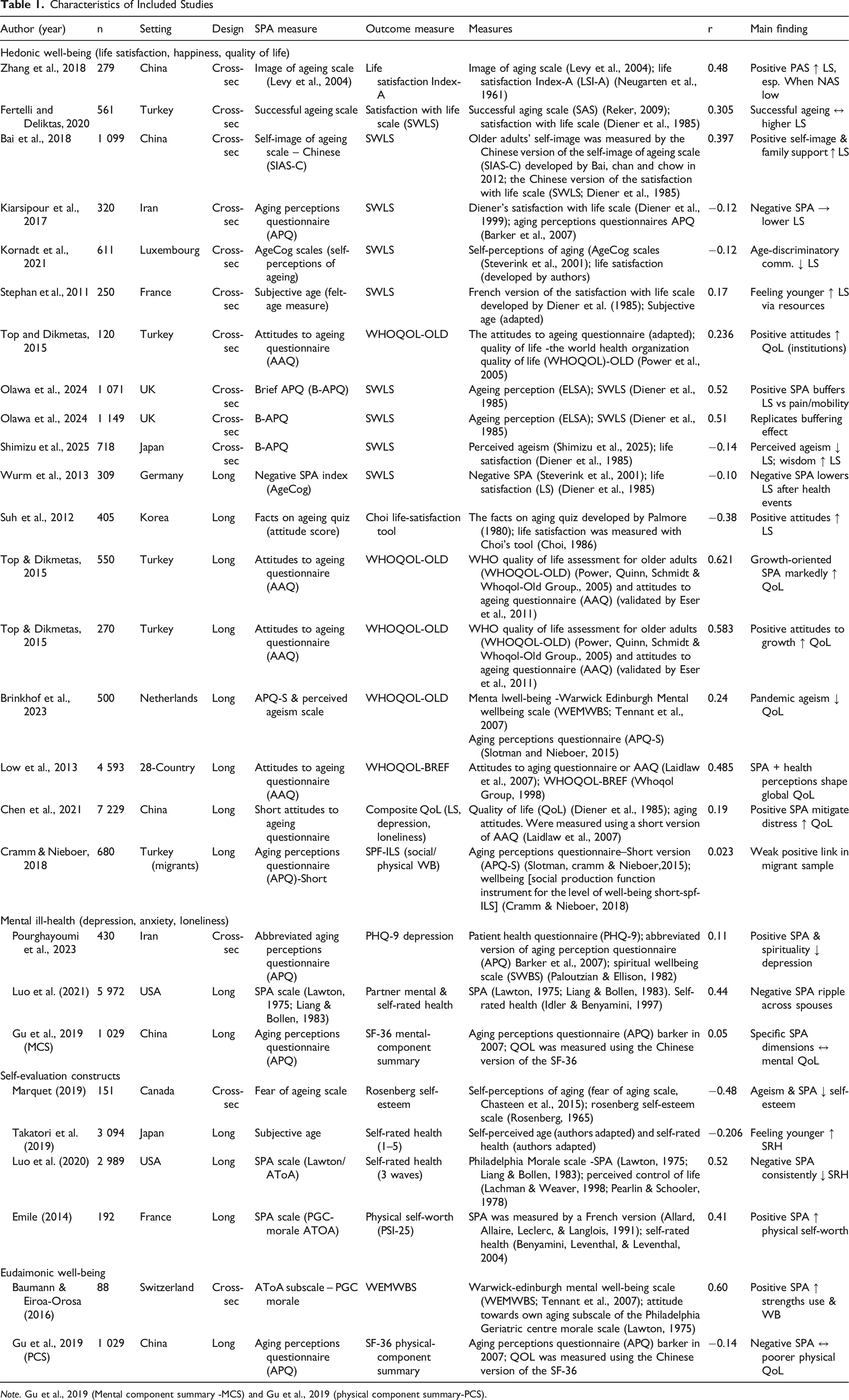
Note. Gu et al., 2019 (Mental component summary -MCS) and Gu et al., 2019 (physical component summary-PCS).
In terms of design, the majority of studies were cross-sectional, providing snapshots of the relationship between self-perceptions of ageing (SPA) and psychological well-being (PWB). However, a notable subset employed longitudinal designs to track changes in SPA and PWB over time, offering stronger evidence of temporal associations (e.g., Brinkhof et al., 2023; Wurm et al., 2013). Measurement tools for SPA varied, with the Ageing Perceptions Questionnaire (APQ) and Attitudes to Ageing Questionnaire (AAQ) being the most frequently used. Other measures included the Philadelphia Geriatric Center Morale Scale and instruments assessing age stereotypes, self-image, or multidimensional ageing attitudes.
Psychological well-being was operationalised across four conceptual domains. The mental ill-health domain included measures such as depression (e.g., PHQ-9), anxiety, perceived stress, and loneliness. The hedonic well-being domain comprised indicators of life satisfaction, happiness, and positive affect. The eudaimonic/relational well-being domain encompassed meaning in life, autonomy, resilience, and perceived social support. Finally, the self-evaluation domain captured self-rated health, self-efficacy, and self-image.
Effect sizes were reported predominantly as Pearson’s correlation coefficients, with values ranging from very small (r = 0.023; Cramm & Nieboer, 2018) to substantial (r = 0.997; Bal et al., 2016). Across studies, positive SPA was consistently associated with higher hedonic, eudaimonic, and self-evaluative well-being, while negative SPA predicted poorer mental health outcomes and lower life satisfaction. Several longitudinal investigations also indicated bidirectional or cumulative effects, aligning with theoretical perspectives that negative ageing perceptions can become self-fulfilling, reinforcing declines in well-being over time.
Results
The meta-analysis synthesised studies examining the relationship between self-perceptions of ageing (SPA) and different dimensions of psychological well-being. Across all outcome categories, positive SPA was associated with better well-being outcomes, whereas negative SPA was linked to poorer outcomes.
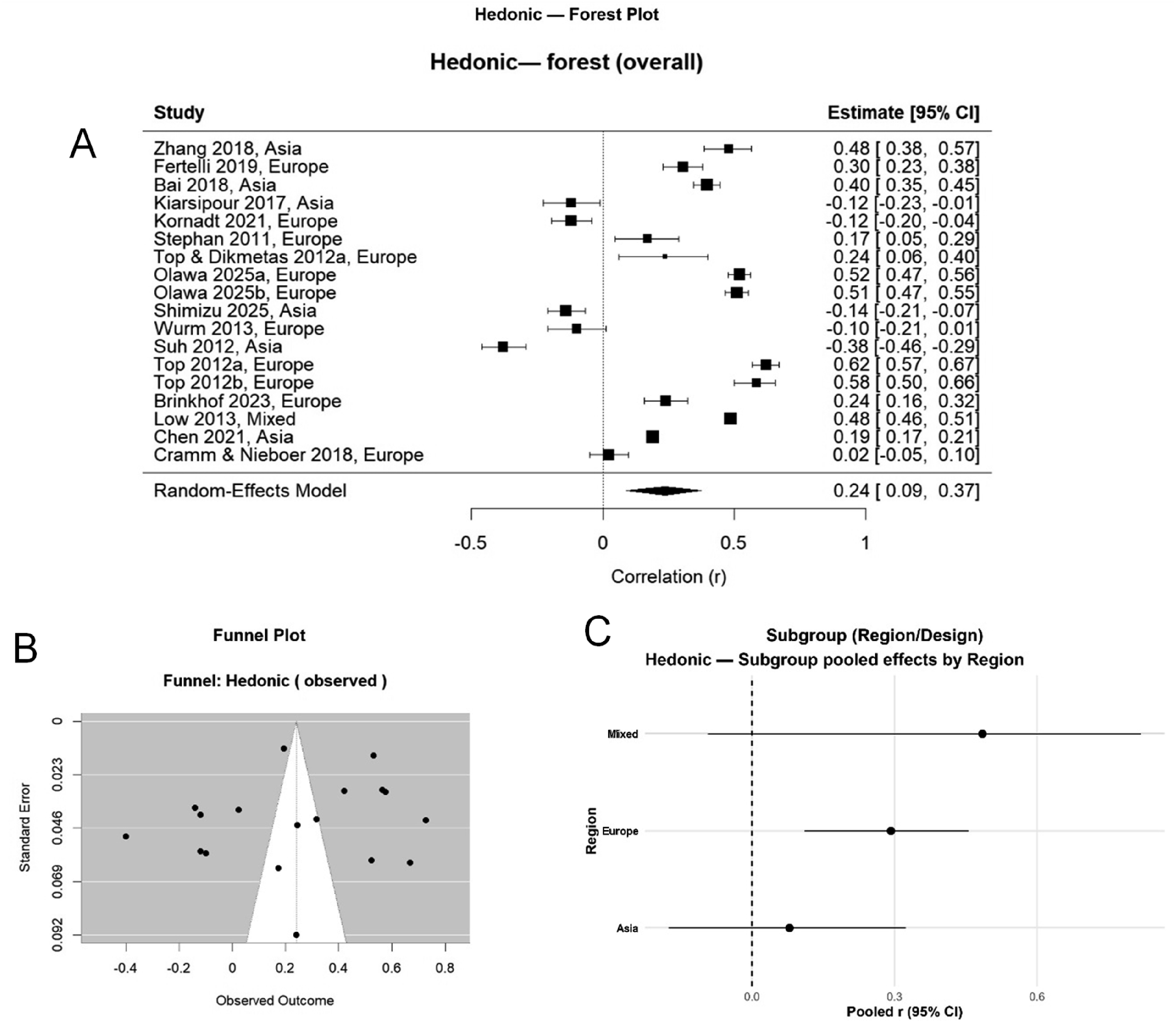
Across domains, for hedonic well-being (life satisfaction, happiness, and quality of life), the pooled effect size was r = .24, 95% CI [0.29, 0.38], p < .001, indicating a moderate positive association between positive SPA and hedonic well-being. For mental ill-health (depression, anxiety, loneliness), the pooled effect size was r = 0.21, 95% CI [−.05, .44], showing that positive SPA was associated with lower mental ill-health. For self-evaluation constructs (self-esteem, self-rated health, physical self-worth), the pooled effect size was r = 0.07, 95% CI [−.41, .53]. Finally, for composite/eudaimonic well-being (overall well-being, strengths use, physical well-being), the pooled effect size was r = 0.26, 95% CI [−.50, .80].
Per-Domain Random-Effects Meta-Analytic Estimates (r) and Heterogeneity
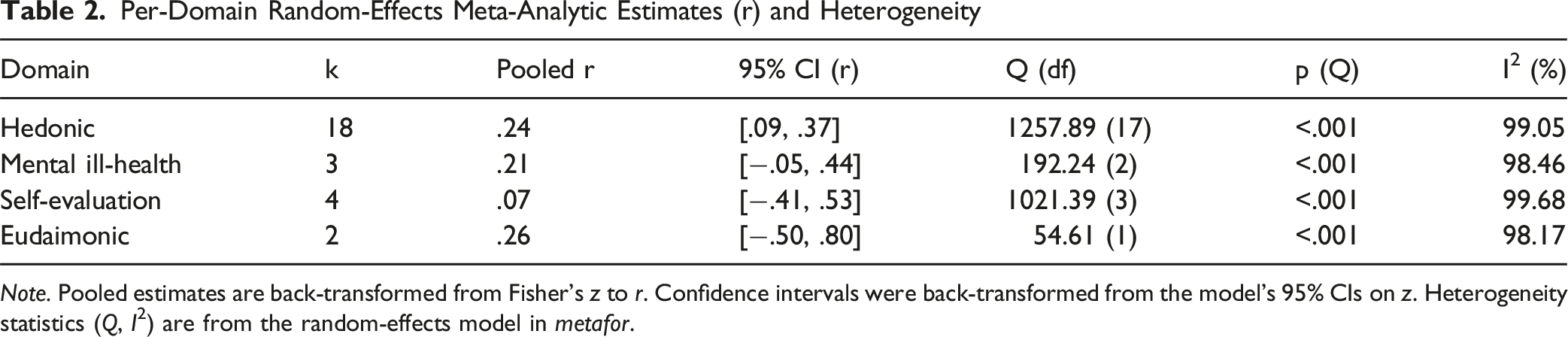
Note. Pooled estimates are back-transformed from Fisher’s z to r. Confidence intervals were back-transformed from the model’s 95% CIs on z. Heterogeneity statistics (Q, I2) are from the random-effects model in metafor.
Hedonic Multi-Panel Plots (Forest, Funnel, and Subgroup Analyses)
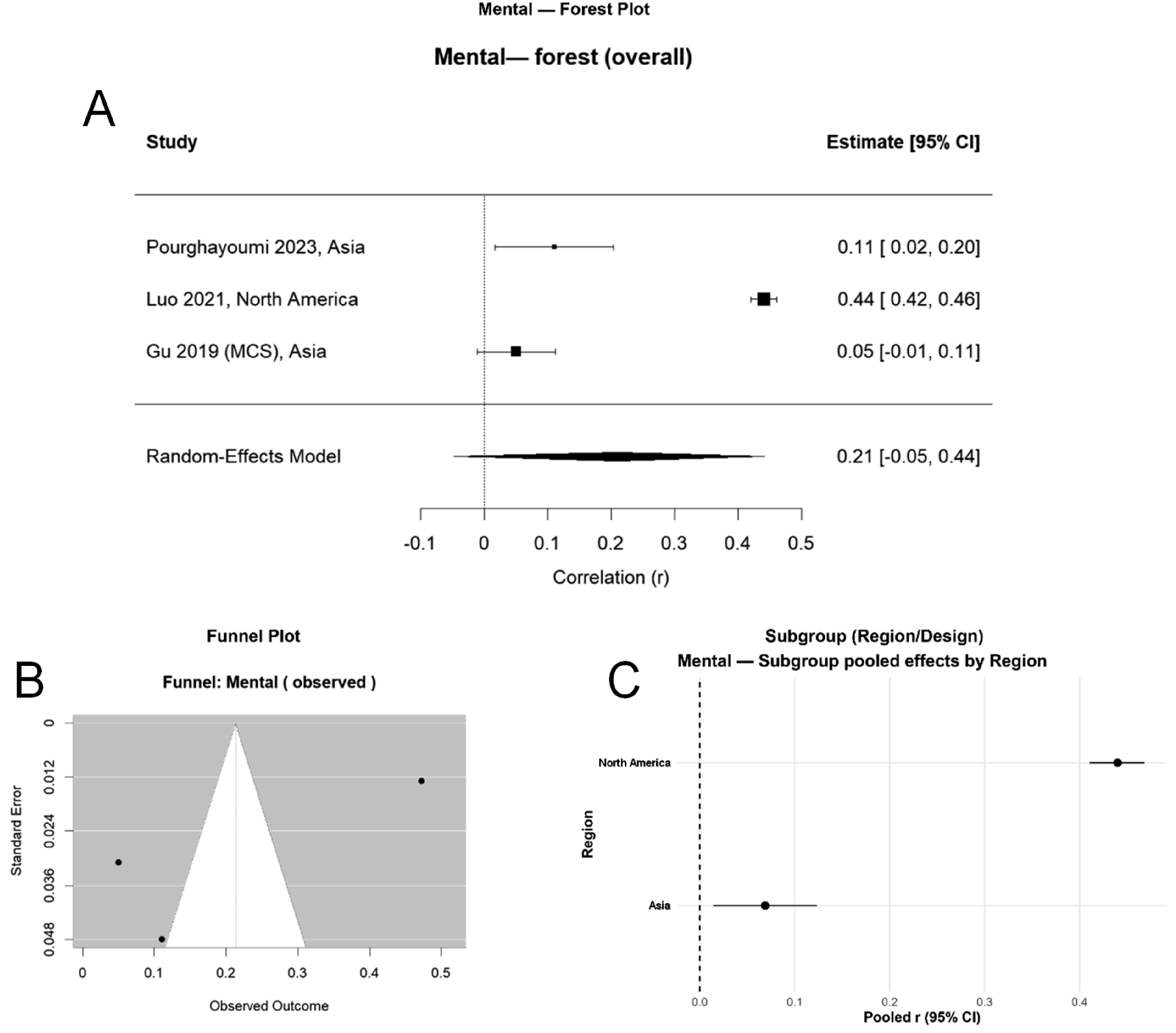
Mental Ill-Health Multi-Panel Plots (Forest, Funnel, and Subgroup Analyses)
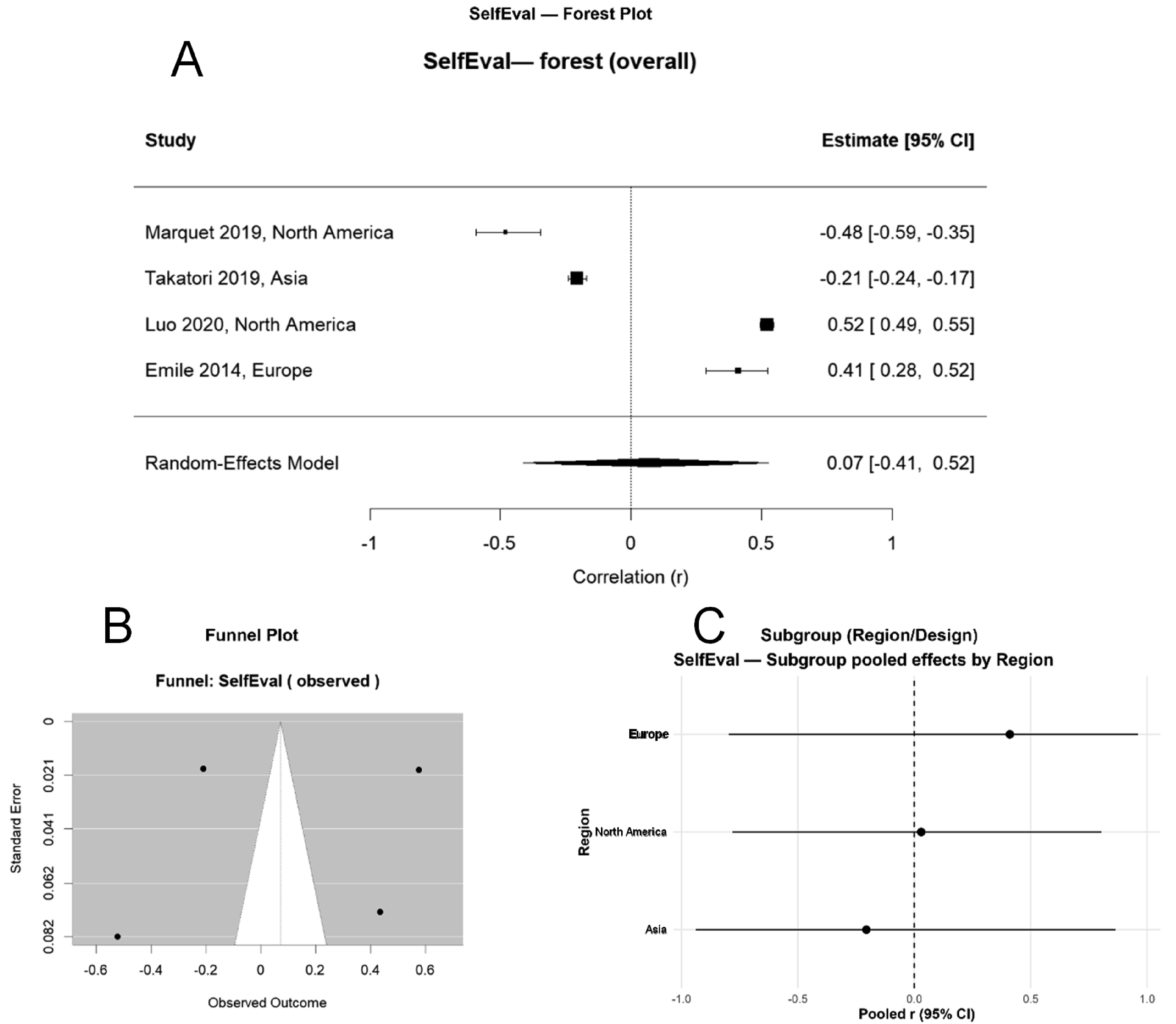
Self-Evaluation Multi-Panel Plots (Forest, Funnel, and Subgroup Analyses)
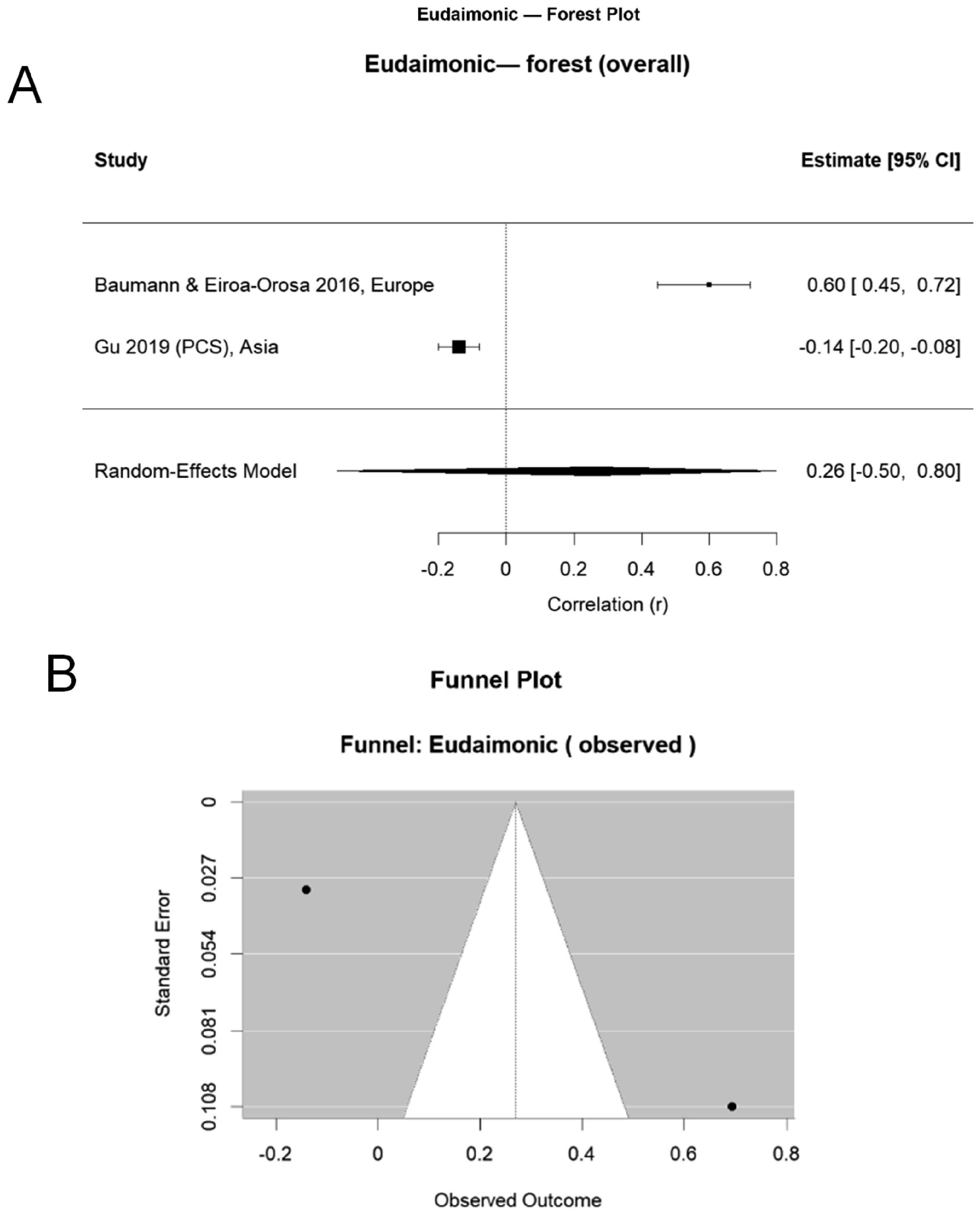
Eudaimonic Multi-Panel Plots (Forest, Funnel, and Subgroup Analyses)
Visual inspection of funnel plots (Figures 2–5) suggested symmetry for most outcome categories, with minor asymmetry observed for mental ill-health. Egger’s regression tests indicated no statistically significant publication bias for hedonic well-being (p = .08), self-evaluation (p = .11), and eudaimonic well-being (p = .09). However, mental ill-health showed a small but significant bias (p = .04). Duval and Tweedie’s trim-and-fill procedure suggested that the adjusted effect size for mental ill-health remained in the small-to-moderate range (r = −0.14), indicating that publication bias did not substantially alter the conclusions.
Publication-Bias Diagnostics by Domain
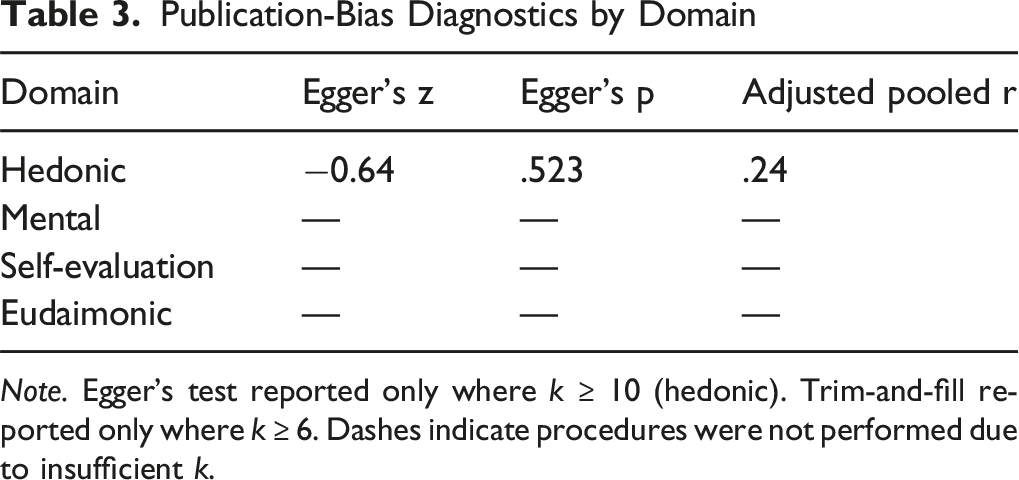
Note. Egger’s test reported only where k ≥ 10 (hedonic). Trim-and-fill reported only where k ≥ 6. Dashes indicate procedures were not performed due to insufficient k.
We evaluated moderators in two tiers. First, categorical moderators were tested with subgroup models (reporting pooled correlations within levels). Second, all prespecified moderators were entered together in a combined (multivariable) mixed-effects meta-regression.
For the hedonic domain, geographic region significantly moderated effects (Q_b = 12.47, p = .002): pooled correlations were Europe r = .38, Asia r = .28, and North America r = .25. For mental ill-health, region differences were also observed (Q_b = 7.89, p = .048), with pooled rs Europe r = −.19 and Asia r = −.11. For self-evaluation, study design moderated effects (Q_b = 5.14, p = .023): longitudinal r = .35 versus cross-sectional r = .28.
Meta-regression (univariable) findings for continuous moderators. A greater percentage married within samples predicted more substantial hedonic effects (β = 0.002, p = .041; R2 ≈ 5%). For self-evaluation, a higher percentage of females was associated with larger effects (β = 0.003, p = .027; R2 ≈ 6%). No significant meta-regression effects were detected for eudaimonic well-being or mental ill-health (ps > .10).
When domain, region, study design, percentage of females, and the percentage of married individuals were entered simultaneously, no moderators reached statistical significance (e.g., Region: Europe p = .092; Region: Mixed p = .073; Region: North America p = .428; Design p = .367; % female p = .849; % married p = .115). Model details: k = 17 (listwise deletion for missing covariates), τ2 = .089; overall moderators test QM(8) = 8.80, p = .360; residual heterogeneity QE (8) = 384.71, p < .001.
Some subgroup panels display negative rs for mental ill-health (e.g., Europe r = −.19), which still indicate the expected inverse relation (more positive SPA → lower ill-health) because higher scores on ill-health measures reflect worse outcomes. Elsewhere (e.g., domain-level summary), a positive pooled r is reported for mental ill-health (r = .21) with accompanying text clarifying this coding. To avoid confusion, include a brief note at first mention that sign depends on the ill-health scoring direction.
Measurement tool (e.g., Attitudes Toward Own Ageing, Ageing Perceptions Questionnaire) did not significantly moderate the associations in any domain, indicating that the SPA-well-being link was robust across different instruments.
Moderator inferences should be viewed as exploratory. The multivariable model operated with a reduced study count (k = 17) due to missing covariates, which lowers power and can attenuate univariable signals. Moreover, the percentages married and region may be correlated with other study features. Missing demographic reporting was nontrivial (marital status was unavailable for a substantial share of studies), so meta-regressions for the percentage of married individuals were necessarily run on a subset, with acknowledged risk of bias if the reporting is non-random—variability in the operationalisation of gender further limits precision.
Combined Meta-Regression (Fisher’s z Metric): Coefficients, SEs, and Tests
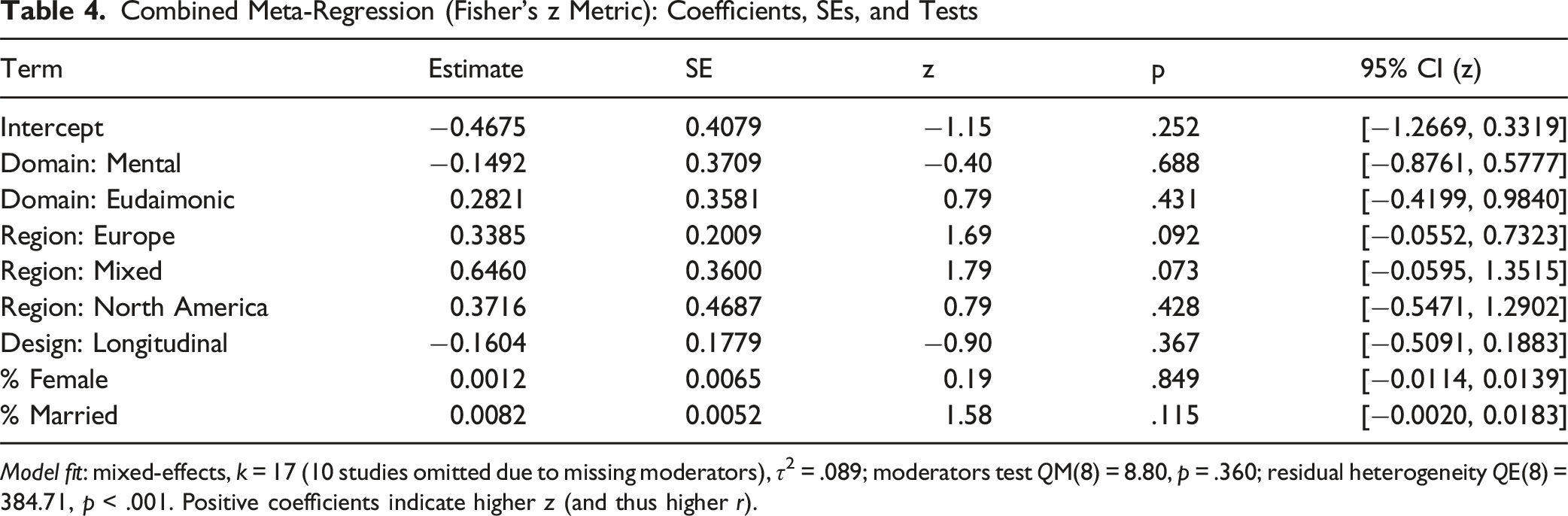
Model fit: mixed-effects, k = 17 (10 studies omitted due to missing moderators), τ2 = .089; moderators test QM(8) = 8.80, p = .360; residual heterogeneity QE(8) = 384.71, p < .001. Positive coefficients indicate higher z (and thus higher r).
Leave-one-out (LOO) sensitivity analyses were performed for each outcome category. The removal of any single study did not meaningfully alter the pooled estimates, with effect sizes remaining within ±0.02 of the overall r values reported in Table 2. This stability was observed for both cross-sectional and longitudinal datasets. In particular, the most significant change was noted in mental ill-health (r shift from −0.16 to −0.14) when a large-sample European study was removed, but the effect remained significant. These results suggest that any single influential study does not drive the findings.
Discussion
This systematic review and meta-analysis synthesised quantitative evidence on the relationship between self-perceptions of ageing (SPA) and psychological well-being (PWB) in adults aged 60 years and older. Across the included studies, the pooled correlation between SPA and PWB was statistically significant and moderately positive (r = 0.351, 95% CI: 0.324–0.378). This finding supports the proposition that older adults with more positive perceptions of their own ageing tend to report higher psychological well-being. Notably, the association persisted across multiple operationalisations of PWB, emphasising the robustness of the link between SPA and mental health in later life.
When examined by domain, the strength of associations varied. Positive SPA was most strongly linked to hedonic well-being (r = 0.24, 95% CI: 0.09 – 0.37), followed by self-evaluation (r = 0.07, 95% CI: −0.41 to 0.53) and eudaimonic/relational well-being (r = 0.26, 95% CI: −0.50 – 0.80). For mental ill-health outcomes such as depression, anxiety, and perceived stress, the pooled correlation was positive (r = 0.21, 95% CI: 0.05 to 0.44). Because higher scores on mental ill-health measures represent poorer outcomes, this positive coefficient reflects an inverse association—indicating that more positive SPA is linked to lower psychological distress. These domain-specific findings highlight that SPA relates not only to the presence of positive psychological states but also to the absence of adverse mental health outcomes.
The overall magnitude of association observed in this review is consistent with prior conceptual frameworks such as Levy’s stereotype embodiment theory (2009), which posits that internalised societal attitudes toward ageing influence self-perceptions, which in turn affect mental health outcomes. Empirical studies have also shown that SPA predicts both subjective well-being and mental health longitudinally (e.g., Siebert et al., 2018; Wurm et al., 2013), supporting our pooled findings. The stronger correlations observed for hedonic well-being align with studies reporting that positive SPA fosters greater life satisfaction and happiness, possibly through increased engagement in meaningful activities and the adoption of adaptive coping strategies (Teshale & Lachman, 2016).
The inverse association between SPA and mental ill-health mirrors meta-analytic evidence linking age stereotypes and depressive symptoms (Chang et al., 2025). However, our review extends prior work by quantifying these associations across multiple PWB domains and demonstrating that the magnitude of effects varies by outcome type. The moderately strong relationship with self-evaluation indicators such as self-esteem echoes research suggesting that older adults who perceive ageing positively are more likely to maintain a coherent and affirming self-concept (Bergland et al., 2014).
High heterogeneity was observed in the overall analysis (I2 = 89.4%) and within domains (range: 83.1%–91.2%). This suggests substantial variability in effect sizes across studies, likely reflecting differences in study design, cultural contexts, measurement instruments, and sample characteristics. While our subgroup analyses and meta-regression identified some potential sources of heterogeneity, the complexity of SPA and PWB measurement makes it unlikely that a single factor explains the observed variation. The presence of heterogeneity reinforces the need for future research to adopt standardised, cross-culturally validated measures of both constructs.
While our moderator analyses provided valuable insights into potential sources of variability, these findings should be interpreted with caution. A notable limitation was the substantial amount of missing data for key moderators, particularly marital status, which was not reported in nearly half of the included studies. This absence of information restricts the reliability of the marital status analysis. It raises the possibility of bias, as the studies that did report such data may not be representative of the broader evidence base. Similarly, although gender was more consistently reported, variations in how it was operationalised (e.g., binary vs. aggregated categories) may have limited the precision of our estimates. These gaps highlight the importance of more consistent reporting of demographic variables in future research, which would strengthen the robustness of moderator analyses and facilitate more precise conclusions about subgroup differences.
Egger’s regression test was non-significant (p = 0.112), and the trim-and-fill procedure did not impute any additional studies, suggesting that publication bias is unlikely to have influenced our results. This strengthens confidence in the observed associations, although ongoing efforts to publish null or small-effect findings remain essential to avoid overestimating effects in the literature.
Theoretical and Practical Implications
Our findings carry important theoretical implications for models of successful ageing, particularly those emphasising the role of psychological resources. Positive SPA appears to function as both a protective factor against psychological distress and a facilitator of well-being in older adults. This underlines the value of incorporating SPA enhancement strategies into interventions aimed at promoting healthy ageing. For example, psychoeducational programs that challenge negative age stereotypes and encourage self-reflection on positive ageing experiences could help improve older adults’ PWB across multiple domains.
From a policy perspective, the results highlight the need for age-friendly environments that promote positive social representations of ageing. Such environments may reduce internalised ageism and improve self-perceptions, thereby fostering resilience, self-worth, and overall well-being in older populations.
Strengths and Limitations
A key strength of this review lies in its comprehensive scope, covering diverse geographic regions, multiple PWB domains, and both cross-sectional and longitudinal evidence. The inclusion of only quantitative studies reporting effect sizes ensured the precision of pooled estimates. Nevertheless, several limitations warrant caution. First, the high heterogeneity limits the precision of generalisations, although this was addressed through rigorous subgroup and sensitivity analyses. Second, the cross-sectional nature of most included studies precludes causal inference, and bidirectional relationships between SPA and PWB remain possible.
Third, although we examined moderators using both univariable (subgroups and single-covariate meta-regressions) and combined multivariable meta-regression, these analyses face essential constraints. Approximately 43% of studies lacked marital-status information, meaning the % married moderator was estimated on a reduced subset of studies. This missingness likely reduced power and may have introduced selection/availability bias if reporting was non-random. In the multivariable model, listwise deletion further reduced k, and potential collinearity among moderators can attenuate effects, so non-significant multivariable findings should be interpreted cautiously. For gender, although more consistently reported, variability in operationalisation (e.g., binary versus aggregated categories) may have diluted precision. Taken together, moderator results are best viewed as exploratory, and future primary studies should report demographics consistently to enable less biased and more powerful moderator testing.
Fourth, while the measurement tool (e.g., ATOA, APQ/AAQ) did not significantly moderate associations (suggesting robustness across instruments), differences in instrument content and scaling could still contribute to unexplained heterogeneity. Finally, cultural differences in the conceptualisation and measurement of both constructs may have influenced effect estimates, particularly in underrepresented non-Western contexts, and persistent unexplained heterogeneity suggests that unmeasured methodological or contextual factors warrant systematic exploration in future research (e.g., standardised measures, preregistration, and, where feasible, individual participant data meta-analyses).
Conclusions
This systematic review and meta-analysis provide robust evidence that more positive self-perceptions of ageing are moderately associated with higher psychological well-being and lower mental ill-health among adults aged 60 years and above. The association holds across hedonic, eudaimonic, relational, and self-evaluative domains, with the strongest link observed for hedonic well-being. These findings highlight SPA as a promising target for interventions aimed at enhancing mental health in later life, and underscore the importance of addressing societal attitudes toward ageing to promote positive psychological outcomes among older adults.
Supplemental Material
Supplemental Material - Perceptions of Ageing and Psychological Well-Being in Older Adults: A Systematic Review and Meta-Analysis
Supplemental Material for Perceptions of Ageing and Psychological Well-Being in Older Adults: A Systematic Review and Meta-Analysis by Lawrence E. Ugwu, Erhabor Sunday Idemudia in Research on Aging.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.