
Abstract
The objective of the study was to assess the consistency between self-reported demographic characteristics, health conditions, and healthcare use, and administrative healthcare records, in a sample of enrollees of an Indigenous health organization in Colombia. We conducted a phone survey of a random sample of 2113 enrollees September-2020/February-2021. Administrative health records were obtained for the sample. Using ICD-10 diagnostic codes, we identified individuals who had healthcare visits for diabetes, hypertension, and/or pregnancy. Using unique identifiers, we linked their survey data to the administrative dataset. Agreement percentages and Cohen’s Kappa coefficients were calculated. Logistic regressions were performed for each health condition/state. Results showed high degree of agreement between data sources for sex and age, similar rates for diabetes and hypertension, 10% variation for pregnancy. Kappa statistics were in the moderate range. Age was significantly associated with agreement between data sources. Sex, language, and self-rated health were significant for diabetes. This is the first study with data from an Indigenous population assessing the consistency between self-reported data and administrative health records. Survey and administrative data produced similar results, suggesting that Anas Wauu can be confident in using their data for planning and research purposes, as part of the movement toward data sovereignty.
Keywords
Introduction
Broadly speaking, the two main types of data sources in population health and health services research are surveys and administrative/clinical records. As is the case with other fields of research, the main challenge is to ensure the reliability and validity of the data. Since earlier years of health and sociological research, methodological studies of survey research have dealt “with the many possible sources of bias to be found in… surveys” (Suchman, 1962). Furthermore, given that self-reporting “is often used to estimate health care utilization … the accuracy of such data is of paramount concern” (Bhandari & Wagner, 2006). Studying the consistency between self-reported and administrative health records is of value for health services research, due to their respective strengths and weaknesses, as well as advantages and disadvantages. It has been suggested that linking administrative data with primary data complements the unique strengths of each type of data (Roos et al., 1993). Furthermore, the consistency between self-reported and administrative health records may substantially vary across different types of illnesses, population groups, contexts, and countries. Thus, a better understanding of their levels of trustworthiness can provide evidence for methodological decision-making in health research. To our knowledge, despite the numerous studies assessing this consistency (Al-Azazi et al., 2019; Brown & Adams, 1992; Clifasefi et al., 2011; Lix et al., 2008; Lix et al., 2010; Okura et al., 2004; Rhodes & Fung, 2004; Robinson et al., 1997), none has been conducted with Indigenous populations. In a two-year study with a large Indigenous health organization in Colombia, we assessed the role of intercultural hostels and bilingual guides in relation to access to health care, utilizing self-reported survey data and administrative data (Mignone et al., 2021). This provided a unique opportunity to assess the consistency between administrative health records and self-reported data from the Indigenous Wayuu population of Colombia.
The Wayuu are the largest of the 115 Indigenous ethnic groups in Colombia (Departamento Administrativo Nacional de Estadística, 2019). Living in the northeast region of Colombia, La Guajira, in 2018 the Wayuu population consisted of 380,460 people (Departamento Administrativo Nacional de Estadística, 2019). For livelihood, the Wayuu raise small livestock, produce, and sell hand-woven items such as hammocks and handbags, aside from relying on other informal income sources. A majority of the Wayuu live in small rural villages and hamlets, some closer to urban centres and some in remote areas (Mignone et al., 2021). From an epidemiological perspective, frequent pathologies include malnutrition, respiratory and gastrointestinal infections among children less than five years of age (Hernández Bello et al., 2017), sexually transmitted infections, hypertension, uterine/cervical cancer, injuries, and dental problems (Mignone et al., 2021).
In 1993, the Colombian government passed Law 100 creating Health Promoting Enterprises (Empresas Promotoras de Salud [EPS]) (Restrepo & Valencia, 2002), which in essence are health insurance organizations. Some EPSs are for-profit and others not-for-profit. Anas Wayuu is a non-profit Indigenous led EPS created in early 2000 by two Indigenous associations representing 120 Wayuu communities. At the time of our study, Anas Wayuu was providing health care coverage to 220,000 people, 71% Indigenous Wayuu. To provide coverage, Anas Wayuu contracts with a health care network of 27 Indigenous Health Service Provider Institutions and 65 non-Indigenous Health Service Provider Institutions privately owned or from the public sector such as State Social Enterprises. The coverage includes health promotion and disease prevention services, and primary, secondary, and tertiary health care (Mignone & Gómez Vargas, 2015). As the single payer of health services, Anas Wayuu relies on a vast information system of administrative data for all health care encounters.
For the main study (assessing Anas Wayuu’s intercultural health initiatives and their role in access to health care) (Mignone et al., 2021), we utilized data from the administrative health records information system, as well as survey data. The purpose of the present study was to examine the consistency between survey responses and administrative health records among Indigenous Wayuu health insurance enrollees in relation to health conditions/states and use of healthcare services, and to determine the factors associated with the consistency of responses.
Method
Cohort
The sampling frame, consisting of 34,961 Wayuu individuals 18 years of age and older, was created from Anas Wayuu’s lists of current (90%) and former (10%) enrollees. During the data collection phase of the study (September 2020 to February 2021), four bilingual surveyors attempted to contact 25,025 individuals by phone. Of those, 22,719 were unreachable (phones turned off, numbers changed, etc.), and 371 declined to participate. A total of 2160 surveys were completed. After removing duplicates and poorly completed surveys, the final sample consisted of 2113 individuals.
Study Period
The study period was 2017 to 2020. We chose this period because it closely aligned to the three years prior to the survey, which was the timeframe that the survey questionnaire asked about.
Data Sources
The 34-item survey was jointly developed among researchers, Anas Wayuu staff, and a Wayuu Knowledge Keeper. The questions asked about demographic characteristics (e.g., sex, age, region of residence), languages spoken (Spanish, Wayuunaiki), self-rated health (poor to excellent), diagnosed physical health conditions, and receipt of healthcare in the past three years. Sex was dichotomous male/female as per advice of Anas Wayuu, which also matches the two categories used for administrative data. The survey was translated from Spanish to Wayuunaiki so it could be administered in the participants’ preferred language.
The study used administrative data collected by Anas Wayuu which in Colombia are called “Registros Individuales de Prestación de Servicios” (RIPS) [Individual Records of Service Provision]. The RIPS data contains information on aspects of medical service delivery, such as hospital discharge summaries, emergency visits, medical claims, prescription drug therapies, and birth registrations. The RIPS also contain demographic and identifying information, such as age, gender, area of residence, and user type. The RIPS structure has been unified and standardized for all health institutions in the country. Health institutions must provide monthly health records to a regional state entity. According to an official data quality report, when comparing the RIPS to patients’ clinical history, there was 95% agreement between the data sources for patient demographic characteristics and 83.4% agreement for diagnostic coding (Martínez & Pacheco, 2013).
As an entity that manages public resources, Anas Wayuu relies on this healthcare data to pay healthcare providers and to manage resources. Additionally, RIPS are the primary data source used to estimate the prevalence and incidence of diseases among the enrolled population (Martínez & Pacheco, 2013). Although administrative data is not intended for research purposes, it is a rich source of information for studying enrollee utilization of healthcare resources, as well as other evaluation and research purposes (MCHP, 2007).
Variables
The survey demographic question included sex, languages spoken, and region of residence. Age was determined as the difference between the interview date and birthdate recorded in the information system of Anas Wayuu enrollees. The languages question asked if participants could “entiendo” (understand) and/or “hablo” (speak) Castellano (Spanish) and/or Wayuunaiki. The self-rated health question was worded as follows: “¿En general, diría que su salud es?” (In general, would you say your health is?). Respondents could answer “excelente”, “muy buena”, “buena”, “regular”, or “pobre” (excellent, very good, good, regular, poor).
The health conditions question in the questionnaire asked about ever having cardiovascular diseases, respiratory diseases, stomach issues, cancer, diabetes, infectious diseases, and being pregnant. We focused on three conditions/states: hypertension, diabetes, and pregnancy. We selected these three conditions/states because we hypothesized that individuals would seek healthcare for these conditions/states. In fact, hypertensive diseases are one of the leading causes of medical consultation in La Guajira (Ministerio de Salud de Colombia, 2012). We also hypothesized that since hypertension and diabetes require treatment and monitoring, people would know if they had these conditions and would accurately self-report them. We also figured that women would accurately self-report pregnancy. We hypothesized that the degree of agreement would vary across the health conditions. We did not choose cancer because too few survey participants self-reported having a cancer diagnosis. We did not select respiratory diseases, stomach issues, or infectious diseases because they are general categories of conditions that people may not seek healthcare for. The survey question about healthcare use asked about using or trying to use health services (e.g., doctor, nurse, treatment) in the past three years. Individuals responded either “Si” or “No” (yes or no) to the health conditions and healthcare use questions.
Enrollment records were linked to RIPS to consolidate patient history of use of health services and clinical and demographic information. The four-digit ICD-10 disease diagnosis code and date of visit were used to identify patients with diabetes, hypertension, and those who were pregnant during the study period. “Cases” were defined as survey participants with at least one visit to the doctor or hospital with the ICD-10 diagnostic code for the health condition/state. The ICD-10 codes were chosen based on a review of how other studies defined these conditions/states using administrative data (Chen et al., 2010; Khokhar et al., 2016; Robinson et al., 1997).
Data Linkage
Anas Wayuu provided a file of medical visits of 1,442,399 consultation records and 70,973 hospitalizations for years 2017 to 2020. The administrative data and survey data files were linked via a unique user identifier. Thus, the joined dataset only included records for the 2113 survey participants. The medical visits and hospitalization data were structured in a way that the number of visits per patient, diagnoses, and year could be determined. Survey participants who were in the Anas Wayuu user registry, but did not have any healthcare visits, were assumed to not have used health services during the study period.
Statistical Analysis
We calculated basic descriptive statistics (i.e., means, standard deviations, frequencies, percentages) for the demographic variables (e.g., age, sex), health conditions/states, and the pattern of contact with the health care system (e.g., number of hospital admissions and physician visits). The prevalence of the health conditions/states was calculated from each data source. The degree of agreement between the two data sources was determined by calculating the percent agreement, and the Cohen’s Kappa coefficient (a chance-corrected measure of agreement) and corresponding 95% confidence intervals. According to Landis and Koch (1977), a kappa value less than 0.40 is considered poor-to-fair agreement, a kappa value between 0.41 and 0.60 is considered moderate agreement, a kappa value of 0.61 and 0.80 is considered substantial agreement, and a kappa value of 0.81 and 1.00 is considered excellent agreement. Logistic regression was performed for each health condition/state to determine if any of the demographic factors could explain the (in)consistency between the data sources.
Results
Consistency Between Self-Reported Demographic Characteristics and Administrative Records
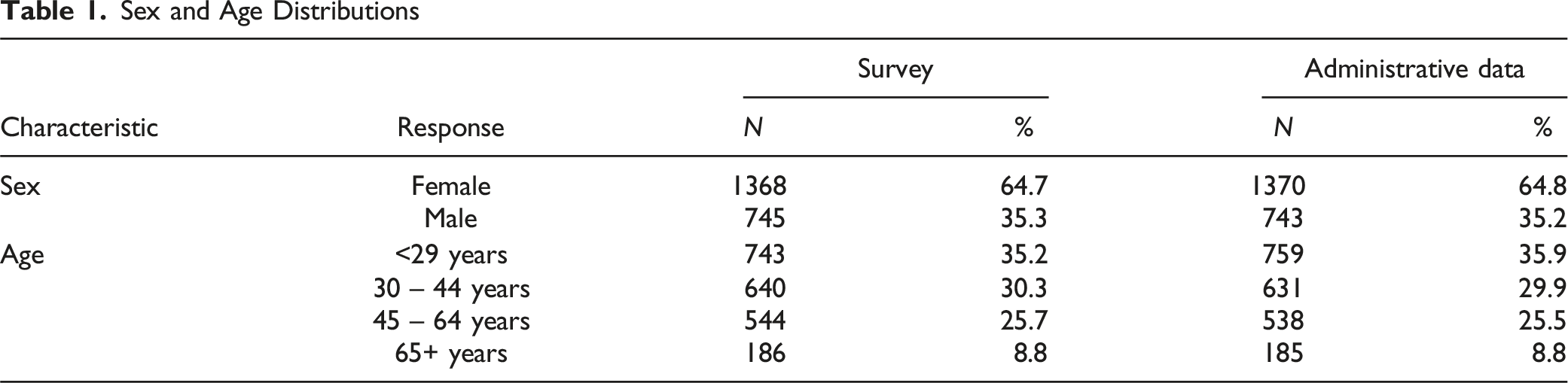
Sex and Age Distributions
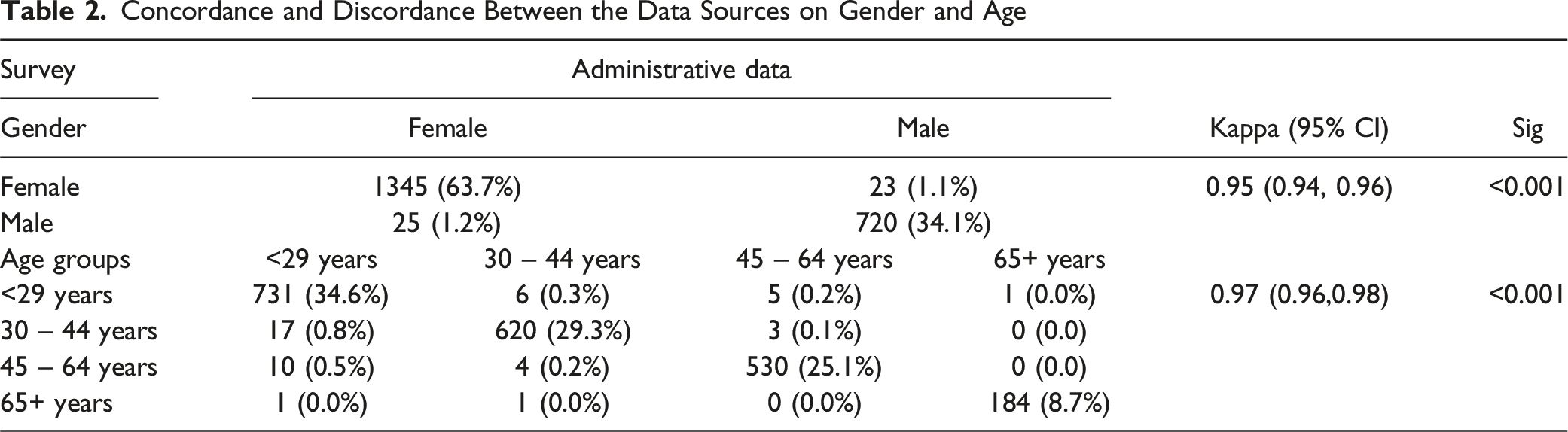
Concordance and Discordance Between the Data Sources on Gender and Age
Consistency Between Self-Reported Healthcare Use and Administrative Records
Concordance and Discordance Between the Data Sources with Respect to Healthcare Use

Consistency Between Self-Reported Health Conditions and Administrative Records
Prevalence of the Health Conditions/States by Data Source (N = 2113)

Concordance and Discordance Between the Two Data Sources for the Health Conditions/States

Logistic Regression Results
Logistic regression was performed to determine if agreement between the two data sources for the three health conditions/states could be explained by the demographic characteristics (sex, age, language) and health status. These demographic and self-rated health variables were obtained from the survey. The sample was limited to survey participants who were current enrollees at the time of the survey and used healthcare in the three years prior to their survey date. The Hosmer-Lemeshow test was not significant for any of the models suggesting the models fit the data well (diabetes: χ(8)2 = 13.292, p = .102; hypertension: χ(8)2 = 8.882, p = .180; pregnancy: χ(6)2 = 3.622, p = .728). The Nagelkerke R2 was 0.07 for the diabetes model, 0.095 for the hypertension model, and 0.16 for the pregnancy model, suggesting the models did not explain much of the variation.
Age was significantly associated with agreement for all three health conditions/states. For diabetes and hypertension, the odds of agreement were lower for the two middle age groups (30–64 years) than the oldest age group (65+ years). Language was only significantly associated with agreement for diabetes; specifically, individuals who spoke Wayuunaiki had lower odds of agreement between the data sources than individuals who did not speak Wayuunaiki. Sex and self-rated health were significantly associated with agreement between the data sources for diabetes. That is, male sex and having better health had lower odds of the data sources agreeing relative to female sex and having poorer health, respectively. Age was the only variable significantly associated with the data sources agreeing for pregnancy; the odds that the two data sources agreed was significantly higher for 30- to 44-year-olds relative to 45- to 49-year-olds.
Discussion
A primary concern when using administrative data for research is the accuracy and completeness of information (Peabody et al., 2004), while recall bias is a key concern for self-reported data (Lix et al., 2010). Given that the consistency between self-reported and administrative health records is likely to vary across different population groups, contexts and countries, the lack of such studies among Indigenous populations is a significant gap in the literature. The data from our broader study (Mignone et al., 2021) provided us with the opportunity to examine the consistency between survey responses and administrative health records among Indigenous Wayuu health insurance enrollees. This assessment was done in relation to demographic information, health conditions/states, and use of healthcare services, while seeking to determine the factors associated with consistent responses.
The sex and age distributions derived from the survey and administrative data were almost identical and there was a high degree of agreement between them, suggesting both data sources are accurate and reliable with respect to these characteristics. This was expected since sex and age are unambiguous. A similar percentage of survey respondents self-reported using or trying to use healthcare in the three years prior to the survey (84%) as actually used healthcare according to Anas Wayuu’s records (88%); however, the kappa statistic was in the poor range, because the observed agreement (79%) was similar to the chance agreement (76%). As well, the kappa statistic is influenced by prevalence; that is, the level of agreement will be lower when the prevalence is high (in this case, a high percentage of the sample used health care) (Zec et al., 2017). The discrepancy between the data sources may be partly due to how the survey question was asked (i.e., used or tried to use healthcare); however, we would have expected the percentage of healthcare users to be higher based on the survey than the administrative data. The agreement between the data sources in relation to healthcare utilization (88% for administrative and 84% for survey) seems to conform with the results from other studies (Short et al., 2009) and somewhat differ from others (Beebe et al., 2006). Thus, at a population-level, Anas Wayuu can be relatively confident in reporting on the healthcare use of its enrollees.
The prevalence of diabetes and hypertension were almost identical between the data sources; however, there was only a moderate degree of agreement. Interestingly, agreement between the data sources was significantly associated with some of the characteristics of the sample, meaning that agreement was better for certain subgroups than others. Specifically, there tended to be better agreement for women, older adults, individuals who did not speak Wayuunaiki, and individuals in poorer health.
There was approximately a 10% difference among women of reproductive age who self-reported being pregnant in the three years prior to the survey (34%) and the administrative case definition (44%), and the kappa statistic was in the moderate range. Our administrative case definition may have been too sensitive, “detecting” cases of pregnancy when a woman had not been pregnant (e.g., we included ICD-10 code Z40.0 -problems related to an unwanted pregnancy-) or respondents may have answered the question negatively if their pregnancy did not result in a live birth. Some of the misclassification may have also occurred due to inaccuracies in sex and age (the variables used to subset the sample), though this misclassification is likely minimal. In contrast to the diabetes and hypertension results, agreement between the data sources tended to be better for younger women and women in better health. Our findings in general are consistent with factors that affect the accuracy of self-reporting of health care utilization identified in a systematic review of the literature: sample population and cognitive abilities; recall time frame; type of utilization; utilization frequency; questionnaire design; mode of data collection; and memory aids and probes (Bhandari & Wagner, 2006).
There were limitations to the study. The survey was not conducted face-to-face but over cell phones. Furthermore, it was administered during a time of uncertainty such as the COVID pandemic. It is difficult to ascertain if the results would have been different if the survey had been conducted before or after the pandemic.
Conclusion
At a population-level, our study showed that survey and administrative data tell essentially the same story, suggesting that Anas Wayuu can be relatively confident in using their administrative data for planning and research purposes with respect to these health conditions. However, subgroup analyses based on identity characteristics, particularly age, should be interpreted with caution. The study addressed a significant gap in the literature, as it relates to health care utilization data of Indigenous peoples. Given the increasing relevance of addressing the rights of Indigenous Peoples across the world to strengthen and implement their data sovereignty (Mashford-Pringle et al., 2019; Hayward et al., 2021; Walter & Suina, 2019), the research reported here is also of value in supporting that agenda.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Inter-American Development Bank.