
Abstract
The aim of this scoping review is to outline the existing landscape of how real patients participate in the workplace-based assessment of trainees across diverse healthcare professions. In 2019–2020, the authors searched MEDLINE, EMBASE, CINAHL, PsycINFO, ERIC, and Web of Science databases for studies that included descriptions of experiences whereby patients received care from a health professional trainee and participated in workplace-based assessments of that trainee. Full-text articles published in English from 2009 to 2020 were included in the search. Of the 8770 studies screened; 77 full-text articles were included. Analysis showed that strategies for patient participation in workplace-based assessment varied widely. Aspects studied ranged from validation of an assessment tool to evaluation of the impact of an educational intervention on trainees’ performance. Assessment of patient satisfaction was the most common approach to patient involvement. The majority of studies were conducted in North America and in the context of physician training. Formal patient participation in the assessment of health professional trainees appears heterogeneous across health professions. Gaps in the literature are evident; therefore, this review points to an inclusive approach to workplace-based assessment to ensure patient feedback of the trainees who care for them is represented.
Keywords
Introduction
Training health professionals who are ready to meet the challenges of current and changing societal needs is necessary for quality healthcare delivery (Frank et al., 2010; Suikkala et al., 2018; Touchie & ten Cate, 2016). Given the emphasis on patient-centred care, educational programs must equip trainees with competencies to address patients’ individual values, needs, and preferences. Involvement of patients in the training process can transform how health professional trainees ultimately communicate and practice safe patient care. (Lehane et al., 2019). Despite continuous efforts to provide patient-centred care, incorporation of patients in the assessment of health professional trainees appears to be lagging. The patient voice is noticeably absent from competency-based assessments even though patient participation throughout the educational spectrum aligns with true patient-centred health professions education and increased patient feedback opportunities would enhance trainee social accountability (Regan de Bere & Nunn, 2016).
Active patient participation in health professions education at undergraduate, postgraduate, and continuing professional development levels has increased dramatically during the last 20 years (Suikkala et al., 2018). Real patients play critical roles in health professional trainee learning experience as standardized patients (SPs), simulated patients, patient volunteers, virtual patients, patient partners, patient tutors, and real patients (Hudson & Ratnapalan, 2014; Towle, 2006). A “real” patient is defined as “someone who has a direct lived experience with the disease and/or condition they sought to display” (Rowland et al., 2019). This description distinguishes real patients from individuals who do not actually have a condition or a disease and who have been trained to represent it or “role-play” (Towle et al., 2010). Various contributions of real patients to health professions education, such as their role in curriculum development (Towle, 2006) and delivery (Bollard et al., 2012), storytelling of lived experiences (Rowland & Kumagai, 2018), and bedside teaching (Monrouxe et al., 2009) have been explored. However, in our view, research demonstrating patient involvement workplace-based assessment (WBA) of health professional trainees has been neglected.
Workplace-based assessment encompasses different assessment techniques of trainee performance (e.g., case-based discussions, direct observation of procedural skills, and mini-clinical evaluation exercises) in a clinical learning environment combined with feedback (Guraya, 2015; Moreau et al., 2019) provided by a supervisor, in some disciplines known as a clinical educator, preceptor, or field advisor. (Bridge et al., 2014). Fostering reflective practice of trainees through the observation of trainee performance together with pertinent feedback, is a hallmark of WBA (Guraya, 2015). In conventional WBA, the patient’s perspective is proxied by the trainee’s supervisor (Bridge et al., 2014). The supervisor observes the-trainee-patient interaction and provides performance feedback to the trainee which may not fully represent the patient’s own experience. We argue that patients themselves are able to bring insightful perspectives on the trainee’s performance owing to their direct interactions with them.
Providing patients with opportunities to offer feedback regarding the care trainees provide can promote the provision of holistic patient-centred care (Bowe & Armstrong, 2017; Carraccio et al., 2016; Kogan & Holmboe, 2013). A patient-generated perspective would be a valuable supplement to existing assessment strategies and serve as a potential patient-focused means of identifying areas of future improvement for trainees (McMahon-Parkes et al., 2016). Feedback in health professional WBA is also facilitates trainee transition into practices committed to patient-centred health care using patient knowledge and lived experiences in clinical settings (Suikkala et al., 2018). Prior research illustrates the variety of ways patients participate in health professions education, but real patients' perspectives on the care they receive or their involvement in non-physician trainee assessment is understudied (Suikkala et al., 2018). Khalife et al. (2022) have recently explored the literature on patient involvement in the assessment of medical trainees and found that patients may take part either as a stand-alone group or as part of a multi-source feedback process. Moreover, patients made comments about the professional conduct and communication skills they witnessed, as opposed to assessments by physicians who focused on the trainee’s medical knowledge (Khalife et al., 2022). Unfortunately, the review by Khalife and team (2022) was limited to evidence on the ways patient participate in competency-based assessment of post-graduate physician trainees (e.g., medical residents and fellows). However, we argue that the need for understanding patient perspectives on trainee performance is required across all health professions education. Accordingly, we conducted this scoping review which is guided by the following broad research question, “What published experiences exist regarding active participation by real patients in the workplace-based assessment of health professional trainees?”
Methods
We chose to perform a scoping review as it seeks to identify a body of emerging evidence (Munn et al., 2018) and offer a broad perspective of a topic in question (Pham et al., 2014). We conducted a comprehensive, structured literature review utilizing the expertise of a medical librarian (VK) to map the evidence and gauge the state of the published experiences regarding real patients’ involvement in the education and, in particular, the assessment of a learner in training across diverse health care professions. Our scoping review was conducted using a framework initially proposed by Arksey and O’Malley (2005) then adapted by Levac and team (2010). This framework consists of a five-step process: (1) composing the research question; (2) identifying potentially eligible studies; (3) selecting relevant studies according to a predefined criterion; (4) charting the data; and (5) collating, summarizing, and reporting the findings.
Search Strategy
A search strategy was developed using the PICO format (Population, Intervention, Comparison, and Outcome) (Schardt et al., 2007) to identify published studies and conference proceedings using the electronic databases MEDLINE, EMBASE, CINAHL, ERIC, Web of Science, and PsycINFO (see Supplemental Digital Appendix A). An initial search was performed in Medline (Ovid), the results of which went through a Peer Review of Electronic Search Strategies (PRESS) (McGowan et al., 2016) (see Supplemental Digital Appendix A) for search submission and peer review assessment form). Once the PRESS was completed, the search strategy was applied to all other databases, with adaptions to keywords, subject headings, and index terms as needed to align with the characteristics and properties of each database (see Supplemental Digital Appendix B for search terms used). Two searches were conducted, one for medicine and nursing and a one for various other health professions, including pharmacy, dentistry, physical therapy, occupational therapy, dietetics/nutrition, emergency medical technician (EMT)/paramedic, respiratory therapy, and social work. Our rationale for conducting two separate searches was to account for the variety and relevance of subject coverage in specific bibliographic databases as well as the need to differentiate themes arising in each health profession. The searches were carried out between January 2020 and May 2020 without applying any geographical limits. To ensure that the search was as exhaustive as possible, additional studies were identified by hand-searching and screening the reference lists of the full-text articles selected and included in the review.
Citation Management
All the references were exported into RefWorks ProQuest. Articles were grouped according to the database and health profession, either medicine + nursing or other health professions. Duplicates were removed manually and using the deduplication feature in RefWorks ProQuest.
Study Screening and Selection
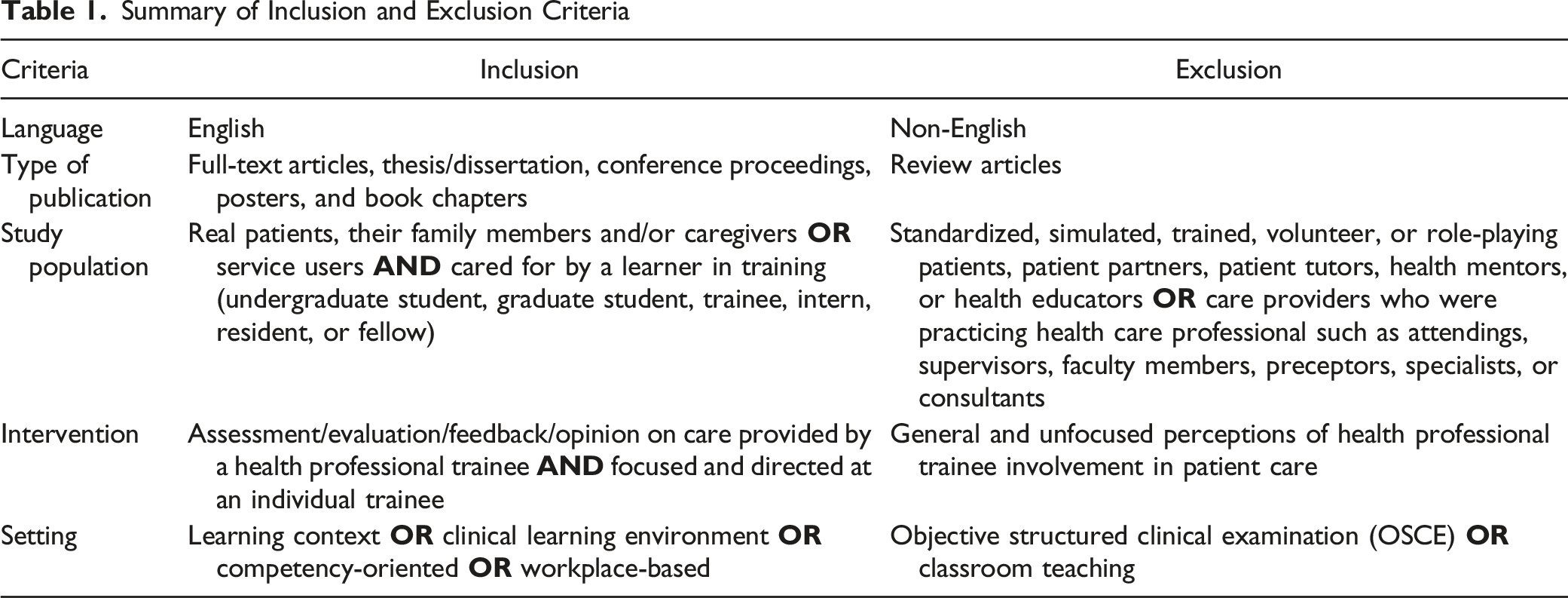
Summary of Inclusion and Exclusion Criteria
Data Extraction
Relevant data from eligible papers was collected using a predesigned data extraction form (see Supplemental Digital Appendix C) on which following information was collected: 1) citation; 2) study location/country; 3) study setting (discipline, site/context, study participants and inclusion criteria); 4) study objectives; 5) methods (study design, theoretical framework, data collection tools, and analysis); 6) outcomes; 7) results; and 8) conclusion.
Data Synthesis and Analysis
We conducted content analysis for the included studies. Because our analysis is of descriptive nature, we combined qualitative, quantitative, and mixed-methods in the same analysis (Suikkala et al., 2018) and categorized the included studies based on their objectives and/or aims. We did not perform risk of bias or quality assessments of the selected studies because, unlike systematic reviews, such assessments are not typically conducted for scoping reviews since the former are frequently carried out to give an overview of the available evidence, regardless of the methodological quality or risk of bias (Tricco et al., 2018).
Results
Overview of Included Studies
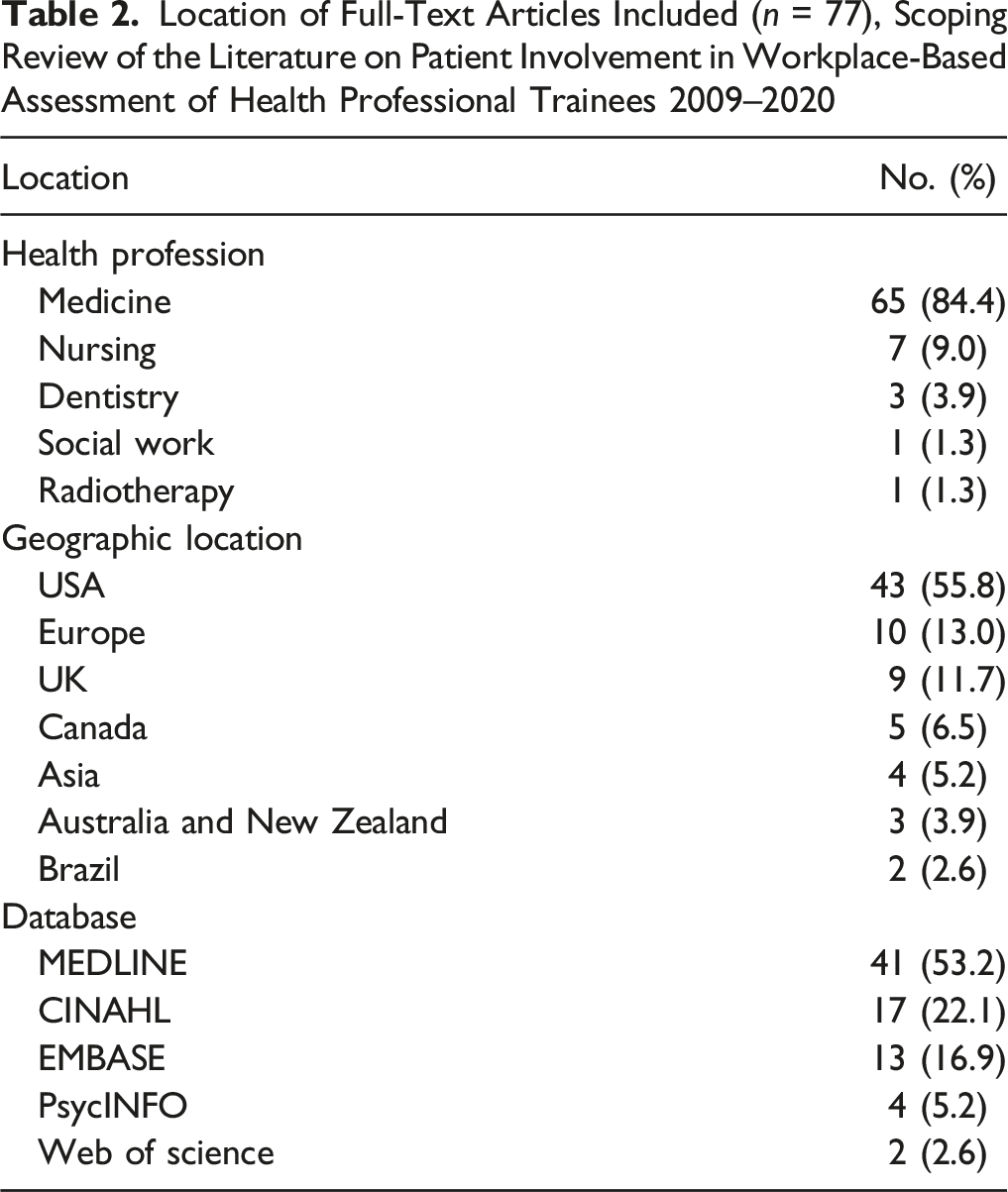
We included 77 articles in this scoping review after screening and the exclusion of 8693 articles (Figure 1). The majority of published experiences describing patient involvement in WBA is found within physician training programs (n = 65; 84.4%) followed distantly by nursing education (n = 7; 9%). More than half of the articles identified were situated in the United States (n= 43; 55.8%) (Table 2). We organized these study objectives and subsequent findings into six specific categories of patient participation in the WBA of health professional trainees which include; 1) patient satisfaction with trainee care; 2) patient feedback using an assessment tool; 3) patients as contributors to multi-source feedback systems; 4) patient feedback to evaluate an educational intervention (such as a workshop, curriculum, or module) on trainee performance and skills.; 5) patient feedback and influence on trainee learning; and 6) factors influencing patient feedback. Some studies had several objectives that were organized into more than one of the categories discussed below (see Supplemental Digital Appendix D for characteristics of included studies). In many studies, patients were asked to provide feedback not on overall trainee performance but instead on specific skills and behaviour such as communication, empathy levels, interpersonal skills, and professionalism by completing questionnaires and/or participating in interviews. PRISMA Flow Diagram for the Scoping Review Process Location of Full-Text Articles Included (n = 77), Scoping Review of the Literature on Patient Involvement in Workplace-Based Assessment of Health Professional Trainees 2009–2020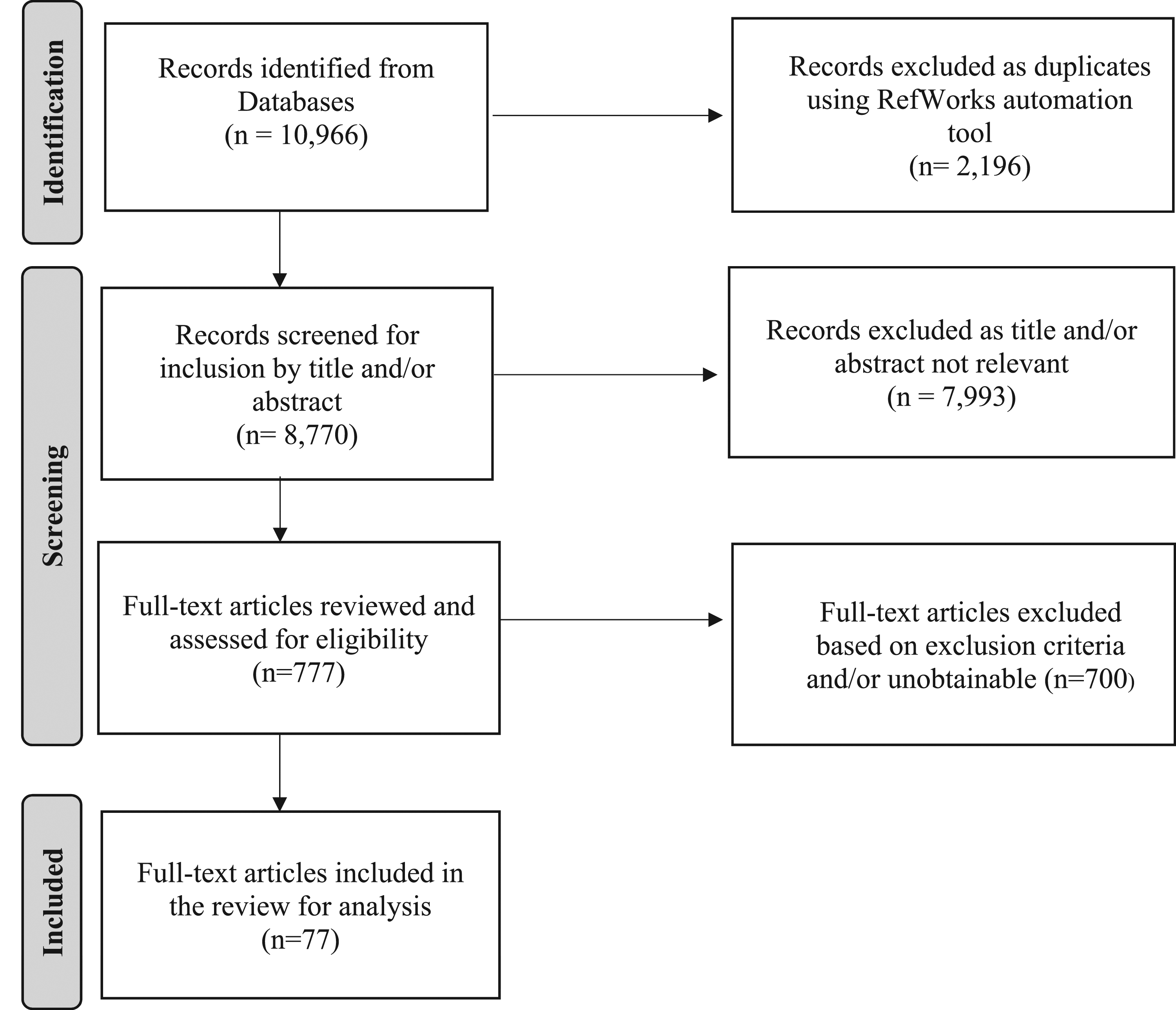
Patient Satisfaction with Trainee Care
Among the most common aspects of patient involvement in the WBA of health professional trainees is examining patient satisfaction with care provided by trainees (Canales et al., 2019; Dalia & Schiffman, 2010; Sherbuk & Barakat, 2019). Patients and/or their families and caregivers were asked to characterize their satisfaction with the quality of their care encounter with a trainee alone (Oskay et al., 2015; Turner et al., 2016) or when the trainee joined the care provided by a clinical supervisor (Beard et al., 2020; Li et al., 2018). Patients views on trainee performance and competency in aspects of care such as professionalism (Niedermier, 2017), communication (Niedermier, 2017; Oda et al., 2014; Stewart et al., 2011), and interpersonal skills (Niedermier, 2017; Oda et al., 2014) were gathered, sometimes using a standard tool such as the patient satisfaction questionnaire (PSQ) (Nouri et al., 2018). Patient satisfaction was also examined in relation to other factors such as training level (Dudas et al., 2010; Nadkarni et al., 2014), trainee self-satisfaction (Kamangar et al., 2016; Francis et al., 2014), quality of care, or workload (Francis et al., 2014). Other researchers used survey questionnaires to measure patient satisfaction with care provided by a health professional trainee within a trainee-run clinic (Riddle et al., 2014; Witherspoon et al., 2019).
Patient Feedback using an Assessment Tool
The objective of some studies was to test the feasibility and/or value of collecting assessment data from patients using an assessment tool to gain insight into patients’ perspectives on their involvement in trainee assessment process (Bridge et al., 2014), capture the patient experience of trainee care by examining the facilitators and barriers to obtaining feedback from patients (Mahoney et al., 2019) or develop and validate a new patient feedback tool (Debyser et al., 2020; Dine et al., 2014; Reinders et al., 2009; Sripada et al., 2011). Diachun and colleagues (2012) studied patients’ and caregivers’ ability to complete a performance evaluation following trainee care. Ward and Benbow (Ward & Benbow, 2016) also sought to collect information about trainee performance through the patients’ own words using a feedback form. In the same study, researchers also examined how patient feedback would reflect the qualities patients value when receiving care from a health professional trainee (Ward & Benbow, 2016). Le Comte and colleagues (2016) used a standard tool (patient surveys) to assess patient perceptions of the health professional trainees care including respect, listening, understanding the patient concerns and confidentiality. In other more specific circumstances, patients were asked about their perceptions of certain aspects of trainees’ communication skills (Khan et al., 2016; Newcomb et al., 2017; Wen et al., 2012), shared understanding between patients and trainees (Khan et al., 2016), and trainee knowledge and the clinical care patients received, (Pecha et al., 2015) using questionnaires, patient opinions of the education they received during challenging consultations by trainees was compared to that of their supervisors (Wouda & van de Wiel, 2015). Schoenborn and team (2017) aimed to gain an insight into patient perspectives of the communication and clinical decisions made by trainees during primary care. In another study, Wiggins et al. (Wiggins et al., 2009) solicited patient perceptions on whether trainees demonstrated professionalism through certain behavioral, communicative and personal characteristics. Scheffer and colleagues (2013) adopted existing questionnaires to examine patient experiences with trainee empathy, patient-centredness, and patient enablement in an education ward, where health professional trainees were involved in direct patient care. The researchers also compared the patient experience in an educational ward with a regular non-education ward (Scheffer et al., 2013).
The Communication Assessment Tool (CAT), a validated instrument developed for patient assessment of the interpersonal communication skills of physicians (Makoul et al., 2007) was used by several researchers. For example, patients were asked to complete the CAT to evaluate the effectiveness of a specific educational intervention (e.g., history-taking) received by health professional trainees (Yu et al., 2018) or to assess the impact of a curriculum on trainees’ performance using patient feedback (DeBlasio et al., 2019; Dubosh et al., 2019). In other circumstances, the CAT was used to solicit patient feedback on trainees’ communication and confidence (Newcomb et al., 2018) or to examine whether trainee-related characteristics influence patient ratings of communication (Myerholtz et al., 2010). Newcomb and team (2017) also elicited SPs’ and real patients’ perceptions using CAT to develop and validate a feasible process for assessing trainees’ communication.
Patients as Contributors to Multi-Source Feedback Systems
Patient assessment of health professional trainees was sought as part of MSF initiatives which also included patients’ families and caregivers, trainee preceptors and mentors, health care site administrators, nurses, physicians, peers, and/or trainee self-assessment (Bernardo et al., 2019; Braend et al., 2010; Garra et al., 2011; Kamangar et al., 2016; McMahon-Parkes et al., 2016; Riveros et al., 2016; Tiao et al., 2013). Patient feedback was triangulated with trainee self-assessment (Braend et al., 2010; Persson et al., 2013), assessment from trainee and faculty (Keister et al., 2017), clinician and non-clinician (Murphy et al., 2009), faculty and non-faculty evaluators (Warm et al., 2010), or grades assigned by the trainee’s tutor (Santiago & Neto, 2016). Speers and Lathlean (Speers & Lathlean, 2015) designed, evaluated, and examined a multisource feedback system that helped trainees seek patient perspective of trainee interpersonal skills on their own, independent of their supervisors.
Other purposes for obtaining patient input as part of wider stakeholder feedback in WBA included: 1) developing and implementing a multi-source assessment method (Sharma et al., 2012; Wener et al., 2011); 2) examining the reliability and/or feasibility of a validated MSF tool (Garra et al., 2011; Murphy et al., 2009); or adapting an existing MSF instrument (LaMantia et al., 2017); 3) associating patient feedback on trainee communication skills with trainee self-perception (Ford et al., 2014); 4) evaluating the feasibility and acceptability of video supervision of patient care (Groener et al., 2015); or 5) assessing the degree of patient-centredness in a clinic (Mazanec et al., 2015). Noordman and colleagues (2019) specifically evaluated trainee patient-centred skills such as communication and empathy from a trifocal point of view through feedback offered by patients, observers, and the trainees themselves. Hall et al., (2019) also examined the correlation between trainees’ scores on standardized video interviews with faculty- and patient-rated scores of communication, professionalism, and interpersonal skills. Another study compared perspectives of SPs with that of actual patients to see how closely they agreed on rating trainee communication skills and professionalism (Sattler et al., 2017). Similarly, Debyser and team (2011) examined how patient feedback on trainee performance was consistent with feedback solicited from the trainee and their educators. In one study, the researchers compared how patients and their families perceived bad news delivered by health professional trainees with how the bad news was perceived by physicians (Toutin-Dias et al., 2016).
Patient Feedback to Evaluate an Educational Intervention
In some instances, patient feedback was collected to assess the impact of an educational intervention on health professional trainees’ competencies and skills, sometimes using a validated assessment tool or a patient satisfaction questionnaire (Oda et al., 2014). Educational interventions involved the creation and delivery of an educational experience of a coaching experience (Rassbach et al., 2019), a new curriculum (Canales et al., 2019; DeBlasio et al., 2019; Dubosh et al., 2019; Mitchell et al., 2016; Niedermier, 2017; Oda et al., 2014), training program (Bylund et al., 2018; Latta et al., 2013; Schutte et al., 2018; Yu et al., 2018), or an educational module (Lin et al., 2013; McElroy et al., 2014) where patient perspectives were collected to determine changes in specific in trainee performance such as patient history-taking, communication, confidence, interpersonal skills, and professionalism.
Patient Feedback and Influence on Learning
Patient responses to questions about trainee communication were elicited to determine its nature, its value as a means of providing feedback for trainees (Gharib et al., 2017), and how trainees perceived it (Grieveson et al., 2011). Davies and Lunn (2009) recruited patients to offer their formative assessment and examined the potential role of patients in participating in trainee assessment from the trainees’ point of view. Other researchers explored the process of collecting feedback from patients and how it could be used as a potential learning opportunity for future practice (Masters & Forrest, 2010; Pearl et al., 2018) and whether patient feedback contributed to trainees passing or failing (Pearl et al., 2018).
Factors Influencing Patient Feedback
In one study, the demographics of patients and their families such as socioeconomic status or race/ethnicity were assessed in relation to patient ratings of the care they received from a health professional trainee to examine the potential contextual influences on patient feedback (Long et al., 2014). Other studies examined the correlation of patients’ and/or caregivers’ attitudes towards trainees with trainee-related characteristics such as level of training (Dudas et al., 2010; Myerholtz et al., 2010; Nadkarni et al., 2014), trainee gender and first language (Myerholtz et al., 2010), or patient and trainee demographics (Persson et al., 2013). Ratelle and team (2020) refined an existing tool to examine the correlation between patient assessment of trainee professionalism with patient demographic data such as sex, race/ethnicity, and education level and resident characteristics like sex, age, and previous medical training.
Discussion
To our knowledge and to this date, this is the first scoping review to locate published experiences describing real patient participation in the WBA of health professional trainees. Specifically, our review broadens the perspective on the existing landscape of patient participation in WBA of trainees in important ways: the inclusion of diverse health professions and the assessment methods employed. Yet aside from assessment of physicians- and nurses -in-training, this scoping review discouragingly found no published experiences of the patient role in WBA of other health professional trainees. Our synthesis aligns with other scholars who also underlined the abundance of research on real patient participation in the clinical learning of medical trainees compared to trainees from other disciplines such as pharmacy and dentistry (Bing-You et al., 2017; Suikkala et al., 2018).
The lack of evidence on patient participation in the WBA of a broader health professional trainee population is alarming and warrants a prompt action. If health professional training programs claim to be educating future patient-centred practitioners, patients must be offered more accountability, specifically by having an active voice in the trainee assessment process. Our review suggests that medicine and nursing professions have a more diverse, yet still scattered and unsystematic means for patient assessment of trainees compared to other health professions. Correspondingly, a more concerted effort and collaboration is needed to understand how to better incorporate patients within our assessment systems. Although students in other health professions programs are typically outnumbered by medical and nursing trainees (U.S. Bureau of Labor Statistics, 2020), these curricula often share a mutual competency-based approach to education (Gruppen et al., 2012; Lucey et al., 2018) and in fact have overlapping professional training needs such as communication, professionalism, and interpersonal skills. We strongly encourage health professions educators from different backgrounds and disciplines to take a step towards an inclusive patient-centred education by borrowing from the experiences of the health professions highlighted in our review. For example, the data assessment methods used such as the CAT and aspects of trainee performance and skills assessed by patients. The CAT has the advantage of being a pre-existing and validated assessment tool which was used by multiple researchers included in this review and could be readily adopted by any health profession to collect patient feedback on trainee communication (Makoul et al., 2007). Less is known how the perspectives of patients’ family members or caregivers could be incorporated in MSF provision (Moreau et al., 2019). The experiences and views of the patient’s family member or caregiver are vital to enrich health professional trainees’ learning as they might hold additional opinions of trainees’ performance owing to the prominent role, they sometimes play in the patient’s health care journey. Another area that is worth navigating is the feasibility and value of having trainees directly solicit the patient perspective as we highlighted earlier in the work undertaken by Speers and Lathlean (2015).
There are specific patient-centred ethical aspects worth emphasizing in the process of patient involvement in the WBA of trainees (Suikkala et al., 2018). In particular, some patients might have certain concerns or reservations with respect to how sharing their perspectives on trainees might impact the quality of care they receive; therefore, it is of crucial importance that the patient’s right to self-determination is acknowledged and respected. Correspondingly, ethical aspects which should be considered when requesting patient feedback include honouring the patient’s preferences on their anonymity, confidentiality, and vulnerability along with feedback timing and patient’s capability and availability when requesting their feedback (Suikkala et al., 2018). Our review also proposes some aspirational avenues for future research in which the position of the health professional trainee in the patient assessment interface including their role, perspectives, and receptiveness of patient feedback, is considered. For instance, coaching feedback has been extensively used in medical education in which trainees are trained with a coach to process feedback by analyzing and reflecting on it to define goals and build a strategy to achieve them (Armson et al., 2019; Khalife et al., 2022). We believe that understanding how coaching feedback based on patient input may promote trainee professional growth, learning, and practice improvements that ultimately enhance patient care and outcome warrants future research (Khalife et al., 2022).
Research reveals several benefits of involving patients in health professional trainees’ assessment, including enhancing trainees’ partnership, advocacy, and communication, and detecting potential areas of improvement in the teaching and learning process (Crawley & Frazer, 2015; Khalife et al., 2022). The responsibility of teaching health professional trainees the value and benefits of involving patients in their assessment is mostly shouldered by health professions educational institutions and programs. The use of patient-centred approaches to health professions education is continuously evolving and health professions curricula are the best place to start incorporating more patient perspectives. Health professions educators must adjust their curricula to meet the dynamic and critical changes in the health care environment. Incorporating the patient voice into the processes for assessment of experiential and workplace-based learning would be a valuable addition to the curriculum. In rapidly changing clinical and educational settings, patient input would also be an asset in curriculum design, evaluation, and improvement to maintain course quality and promote trainees learning outcomes. The notion of involving patients in the WBA of health professional trainees was found to be welcomed and well-received by both trainees and patients. Several studies examined the potential for involving patients in the assessment of medical (Davies & Lunn, 2009; Grujich et al., 2012) and nursing (Duygulu & Abaan, 2013) trainees by soliciting trainees’ perspectives on having patients be part of the trainee WBA. Some trainees reported feeling at ease with having patients assess their performance and some trainees stated that receiving patient feedback boosted their confidence (Davies & Lunn, 2009), others favored the involvement patients in their assessment process and thought that it would be beneficial to have patients as part of the assessment during clinical placements (Duygulu & Abaan, 2013). Students justified their preferences by stating that patients spend considerable time with them in the practice setting (Duygulu & Abaan, 2013). Research also shows that patients deem their contribution to trainee educational experience as an altruistic means of giving back to their community (Morgan et al., 2013; Suikkala et al., 2018; Wykurz & Kelly, 2002).
Strengths and Limitations
Strengths and limitations of this scoping review warrant discussion. Having three researchers working independently screen and synthesize articles helped ensure reliability. However, the search strategy was limited to studies published in English language; therefore, we may not have located all available evidence regarding real patients’ active participation in the WBA of health professional trainees. Over 50% of the included studies were conducted in the United States and therefore our findings are contextualized for a North American training and assessment landscape. In addition, our review did not incorporate any grey literature that may have reported anecdotal experiences. As educational scholarship is an evolving field, it is possible that reports exploring patient involvement in health professional trainee assessment are limited. Academic programs may be incorporating patient input into their curricula without disseminating their research findings or publishing their experiences.
Conclusion
Although real patient perspectives are valuable in trainees’ skill development and professional growth, research on formalized patient roles in WBA of health professional trainees is lacking. Overall, there is limited evidence of patient participation in competency-based feedback of trainees in medicine and nursing fields and even less evidence that patients’ perspectives are incorporated in the feedback process for other health professional trainees. Published experiences from medicine and nursing educational contexts indicate that both professions have more diverse and concrete means for patient assessment of trainees than other health professions. This review also reveals that formal patient roles in health professional trainee assessment are inconsistent in the ways patient feedback is elicited and the outcomes that are assessed. This gap in the literature points to the need to change the existing pedagogical techniques of WBA by incorporating the patient voice into trainees’ assessment processes.
Supplemental Material
Supplemental Material - Real Patient Participation in Workplace-Based Assessment of Health Professional Trainees: A Scoping Review
Supplemental Material for Real Patient Participation in Workplace-Based Assessment of Health Professional Trainees: A Scoping Review by Arwa Nemir, Marion Pearson, Vanessa Kitchin, and Kerry Wilbur in Evaluation & the Health Professions
Footnotes
Acknowledgments
We acknowledge the hard work, time, and dedication of all the included authors in this scoping review.
Authors’ Contributions
Arwa Nemir, Marion Pearson, Vanessa Kitchin, and Kerry Wilbur made significant contributions to the conception of this scoping review, including being responsible for all the key decisions regarding the study design, database screening, data acquisition, abstraction, analysis, and interpretation of the data, writing of the review, and presentation of results. All authors granted final approval of the version to be published and agreed to be responsible for all elements of the work, including ensuring that any issues about the work’s accuracy or integrity are properly investigated and addressed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.