
Abstract
Medicine is often criticized in science and technology studies (STS) for its dominating measuring practices. To date, the focus has been on two areas of “metric work”: health-care workers and metric infrastructures. In this article, I step back into the training of clinicians, which is important for understanding more about how practices of measurement are developed. I draw on ethnographic fieldwork in a Dutch medical school to look at how a ubiquitous and mundane tool––measuring tapes––is embodied by medical students as they learn to coordinate their sensory knowledge. In doing so, they create their own bodies as the standard or measure of things. Unpacking educational practices concerning this object, I suggest that tracing the making of measuring bodies offers new insights into medical metric work. This also speaks to the growing interest in STS in sensory science, where the body is fashioned as a measuring instrument. Specifically, two interrelated contributions build on and deepen STS scholarship: first, the article shows that learning is an embodied process of inner-scaffold making; second, it suggests that the numerical objectification of sensory knowing is not a calibration to “objectivity machines” but rather to oscillations between bodies and objects that involve sensory-numerical work.
Introduction
Measuring tapes (Figure 1) are remarkably simple, often overlooked objects. Mostly, I use them, as many of you also might, to buy, make, and repair clothes. Home in quarantine during a pandemic, I am writing this article on the same table that I use for sewing. My sewing machine is tucked away in a cupboard and nearby lie a pin cushion, thread, and unraveled measuring tapes. Measuring tapes are used to measure size or distance with linear, standardized, and calibrated markings. Tailors and dressmakers use the softish kind, while the sturdier variety is used (when laser and digital versions are not available) on construction sites and during home repairs. I am most interested here in the tailor’s tape, essentially a band of stiff fabric with markings, able to be carried in one’s pocket, allowing for measuring around curves and corners in a way that the wooden ruler, its material predecessor, does not. The intriguing case I want to explore in this article is how this simple tool is used in the training of doctors.
Measuring tape, fieldwork, Skillslab Maastricht.
I set out to study how doctors learn in digital times, and so, the material measuring tape (like other objects I have ended up writing about with colleagues, like balloons and knitted body parts; Nott and Harris 2020; den Harder and Harris Forthcoming) seemed an unlikely teaching tool to focus on. But they were everywhere, and I could not avoid them. 1 For example, Figure 2 shows a picture from a Dutch medical textbook explaining how to measure lung expansion––that is, how far someone can breathe in and out––by using a measuring tape.
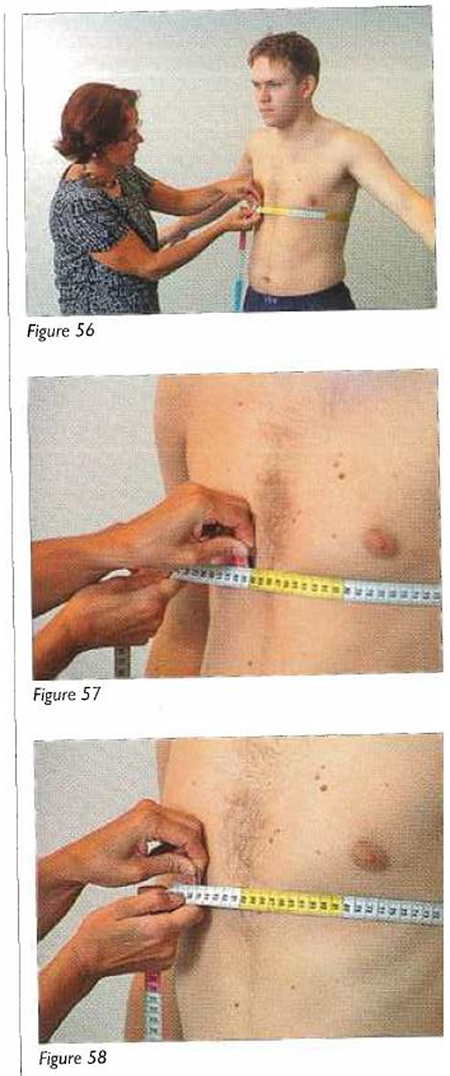
Measuring chest expansion, Skills Laboratory workbook.
Medical students measure the circumferences of arms and legs to learn something about muscle bulk and wasting. They also measure upper arms to find out which blood pressure cuff size to use when learning how to take a blood pressure measurement. There are, in fact, many uses, many other parts of bodies to measure, as I explore later in this article, shaping how students learn about bodies and elicit signs of disease. I could have picked many of these examples from my years of fieldwork in medical schools, but in this article I focus on obstetrics lessons, where students learn to measure mothers and babies to be born. I use these examples because they are often exaggerated moments of measuring and thus helpful for highlighting taken-for-granted aspects of learning measuring practices. And taken together, the obstetric lesson vignettes help to craft a connected narrative about how students engage with the measuring tape. This article is part of my team’s broader research program exploring the role of technologies in how doctors learn with and about bodies, our project called Making Clinical Sense. In essence, I am exploring and attempting to expand through this study of the embodiment of measuring tapes, the materiality of embodied learning. My interest here lies specifically in how medical students craft a “measuring body” (Hoel and Carusi 2018, 47).
Measuring and STS
Measuring tapes are measuring objects par excellence. While STS has long been interested in the histories of measuring instruments (Deringer 2018; Parrinello, Benson, and von Hardenberg 2020), in fields including medicine (Godin 2002; Hiddinga and Blume 1992), it has been more recent scholarship, often at the intersections of STS and anthropology, which has delved into the politics and practices of metric work (Adams 2016; Glasman 2020; Dumit and de Laet 2014). In this literature, medicine is often criticized for its measuring practices. These scholars show how health-care infrastructures are built through counting (Bowker and Star 1999), and how, through quantification and metrification, people’s lives, habits, and practices are turned into numbers. Such numerification has significant effects on individuals’ access to healthcare and how they consider themselves healthy (Yates-Doerr 2015). Some argue that metrics have been used as a tool of medical domination through epidemiology and public health programs (Rhodes and Lancaster 2019; Adams 2016; Nott 2018) and show the long history of damage that measuring has done, through the racist practices of anthropometry, phrenology, and physiognomy. Some of this literature on measuring objects deals with measuring tapes specifically and their role in enacting countable bodies. Such ethnographies show how measuring tapes problematically shape the worlds measured and overshadow alternative narratives (Yates-Doerr and García-Meza 2020) and subjective states such as hunger (Scott-Smith 2013). Scott-Smith (2013) shows that when objects such as measuring tapes are taken for granted, when they become mystified, the objects take on magical authoritarian properties, appearing to be “alive with their own power” (p. 926).
Although in many public and global health narratives numbers are often depicted as transcending contexts, the scholars above point out that numbers are relational beings. The interesting questions they suggest asking, which I incorporate into my own line of questioning in this article, are as follows: How do numbers come about? What work do they do? And, as I want to emphasize most strongly here, what are their material and embodied effects?
To help answer these questions and before turning to my ethnographic explorations of them, I need the insights from another growing and important body of literature in STS on sensory science (see special issue Senses & Society 13 (1) for further key articles). 2 When it comes to numbers, scholars studying sensory science are largely interested in how the sensory is made into measurable objective units, the ways such measuring comes about, and the effects this has on social lives. Within this corpus, some examples include Spackman and Burlingame’s (2018) work on water, Xiao’s (2016) work on tea, and Shapin’s (2016) work on wine. Other scholars focus on how bodies are trained to sense objectively. Take, for example, Butler’s (2019) study of texture profile panels, and the making of “the mouth,” which looks at how human mouths are deployed as test instruments. There are various studies of the perfume industry (Muniesa and Trébuchet-Breitwiller 2010; Teil and Hennion 2004) that discuss the making of “the nose” as measuring instrument. These scholars have deliberately focused on body parts (though Butler [2018] is more expansive in other work) and how bodily instruments are crafted in testing and marketing practices. In this article, I take this line of inquiry in a different direction and look at the role of institutional educational environments, that is, universities, in the making of the sensing, measuring body. Rather than focus on a body part, I focus on a tool and look at how the measured (future patients’ bodies) and the standard of measurements (the students’ bodies) become mutually intertwined with measuring tapes. This provides a parallel case to others’ work that focuses on bodies as disciplined and trained in universities in science classes such as Myers’s (2015) ethnography of the embodied work of protein modelers.
In summary, to date, the STS literature on metrics in medicine has focused mostly on two topics: the health-care worker or medical researcher at work, with their measuring tools to hand, and infrastructures of knowledge production which have metrics at the heart of their logic, mostly in the arena of global health. I build upon this “metric work,” by bringing in insights from STS sensory scholarship, which opens up the politics of measuring and the relationality of numbers into more sensuous, bodily domains. My contribution to both literatures is to take a step back from clinical contexts and look at how individuals who work in and with such metric infrastructures and objects, and who have measuring tools in their hands, are trained to think and, importantly, embody, measurement standards. Rather than look at the sensory politics of governments, companies, or testing facilities, my focus is on the dynamic relations at play in educational environments, specifically, medical education.
Measuring and Medical Education
As many practice theorists show (e.g., Lave and Wenger 1991), studying how novices are incorporated into a system of knowledge production is a highly valuable point of study. Education is about enacting a reality for learners. This enactment becomes a helpful and critical site to study how knowledge is produced and reproduced. School education, however, a classic site of learning, is surprisingly understudied in STS. There are important exceptions, of course. Verran’s (2001) work on mathematics, for example, shows how Yoruba numbers become as bodies, and bodies as numbers, through classroom rituals. Her work moves numbers away from being abstract things in people’s minds to bodily enactments, performed, for example, in the use of a dangling piece of string to teach about one meter. In such instances, Verran (2001) writes, numbers become “figured materiality” (p. 106). STS scholars, such as Barany and MacKenzie (2014), have similarly moved mathematics to a more material place, with observations of how mathematicians use blackboard and chalk in their work.
These two examples are of lessons where numbers are quite central. However, attention to the materiality and sensoriality of numerical work that happens in other lessons, such as with medical students, is also revealing and gives insights into how practices of measurement are developed by those with significant influence on what gets known and understood about health and disease in society. Doctors’ decisions and diagnoses still have much weight in the shaping of conditions and considerations of disease, and this will remain the case despite claims that machines are replacing such embodied skilled practices. I believe that the measuring work happening in medical schools is currently overlooked, yet it is an important place where normalcy and pathology are being actively configured. For as Mol (2002) has beautifully shown in her work on anemia and atherosclerosis, practices, such as measuring, are intimately tied up with what disease is considered to be in the first place.
Medical education becomes a fascinating site of study in STS because of how modifications and transformations of bodies and their abilities, values, affects, and engagements are highlighted when learning clinical skills. The work on medical education to date in STS and anthropology has shown that studying medicine is not only an embodied process of learning about bodies but also an instance of bodily engagements with tools and technologies (Prentice 2013; Johnson 2008; Fenwick 2014). The ethnographic examples in this article are drawn from my own long-term fieldwork in the tradition of the work of these scholars. I have conducted intensive episodes of fieldwork in medical schools and hospitals in the Netherlands and Australia since 2007. Most recently, episodes of fieldwork in the Maastricht medical school were conducted as part of the broader team research project about the role of technologies in learning sensory skills. The project included two other ethnographers and a historian as well as an ecology of local and international collaborators.
As part of this project, I spent one academic year in a place called the Skills Laboratory. The Skills Laboratory is a highly controlled setting where standard set-ups are created and protocols are delivered to teach doctors physical examination techniques before they encounter patients on the wards. This is a model of education in medicine that has been exported to many other countries (Frambach 2014). In the Skills Laboratory, we are seeing the measuring body being made through engagements with the measuring tape, offering a window into understanding more about how numbers get implicated in doctors’ embodied knowledge. Specifically, I suggest that this shows how learning is an embodied process of inner-scaffold making (next section) during which sensory-numerical work is done (the following section).
Measuring Tapes and the Inner Scaffold
Stored in supplies cupboards in the classrooms of the Skills Laboratory, the flexible measuring tapes I found in fieldwork were either in color palettes of white and red (see Figure 1) or the tricolor variety of red, yellow, and green designed for maximum visibility and used frequently in public health programs to measure levels of malnourishment (Scott-Smith 2013). Such measuring tapes were a constant feature in medical school classes, sometimes appearing in unusual ways. In a lesson on cranial nerve examination, for example, in an effort to demonstrate how to examine for nystagmus (a nervous condition of the eye), the teacher stretched out some tape, asked a student to look at a number, then pulled the rolled-up tape quickly through her fingers, asking the other students to assess how the “patient’s” eyes moved back and forth in response to these stimuli. Students also learned how to take baby’s head circumferences on dolls and measure lung capacity as well as the numerous other measurements already mentioned.
In one class I observed during my fieldwork, I saw a lesson that didn’t last more than a few moments where some students were struggling to use the measuring tape to measure a particularly awkward part of the body––it could be any really, for most parts of the body are “awkward” to measure, even if the measuring tape is flexible and made to fit curves and variation. So, the teacher taught them a trick: take the measuring tape and measure three of their fingers together. The teacher showed how this can be a way of measuring the patient’s body, by then using the three fingers put together as an embodied and in-built measuring tape. Her three fingers, she showed, were 6 cm wide. So, these three fingers can then be used as a fleshy measuring tape on their patients. They transmit the measuring information to their own bodies, and they can determine lengths of the patient’s body in 6cm sections; the teacher could use this on a patient without having to get the measuring tape out. She asked the students, “how long are three fingers for you? Let’s get the tape and check.”
Thus, with this soft tape, medical students learned not only how to use this everyday object in a medical way, to obtain information, and to help make a diagnosis by learning what bodies should and should not measure (i.e., constructing specific notions of normalcy and pathology [Canguilhem 2007]), they also learned how to turn their body into a measuring instrument. One way to understand what is happening is that the students are learning how to calibrate what they found in their own measuring to standards and population charts and other statistical curves. But there is more. They are starting to think of bodies, including their own, in terms of numbers. In doing so, they are working at crafting what philosophers Hoel and Carusi (2018) might call an “inner scaffolding of the existential field” (p. 47). Engaging with Maurice Merleau-Ponty’s later work in particular, Hoel and Carusi (2018) unpack his notion of the body as a standard or measure of things and progress this by forwarding the idea of what they call “the measuring body” (p. 47). For Merleau-Ponty, measuring concerns the invisible scaffolding of the perceived, implying complicity between measuring practices and measured phenomena.
In common parlance, scaffolding refers to a temporary structure made from different materials, which supports the making of things, usually buildings. The inner scaffold, in my reading, is an inner support structure for making sense of the world and what is perceived, an invisible connective tissue of “virtual material” (Bennett 2020), built up through medical school, that can be remade to help support different situations. If I turn back to sewing, it is like a dressmaker’s pattern that is adapted for new materials, sizes, and shapes upon which further iterations and variations can be applied. The inner scaffold is made up of an archive of sensory encounters, past, present, and future built up through material engagements in learning settings with students’ own bodies, the bodies of others, and numerical objects (for other related work on technological embodied interactions upon which I also build here, see Harris 2011, 2016). This sensory archive can be resourced, improvised upon, adapted, and tailored as further encounters are made. It is a sensory archive of future bodies, which the doctors-in-training can then (potentially and hypothetically) project onto patients that they might meet in their clinical practice.
Hoel and Carusi (2017) highlight how “technologies are seen as transformative of both perception and phenomena” (p. 74), expanding on Merleau-Ponty’s ideas about how mediating artifacts are integrated into the perceptual complex. Measuring tapes do not exert a force upon the world in and of themselves, they need to be learned as well as used. As Tim Rhodes and Kari Lancaster (2019) write, numbers are afforded life through their entanglements with situated practices, an important part of which is learning with measuring objects that become part of a way of knowing. Looking at making measuring bodies––not only measured bodies––attends to Yates-Doerr’s (2017) plea to engage with studying when, where, and with what effects embodiment matters. It adds insights into how counting gets embodied by medical practitioners as a way of knowing the world and in the crafting of their future patients. The next section explores how this can be thought of as a form of sensory-numerical work.
Sensory-numerical Work
One day I entered a classroom to find the tutorial table filled with strange blue plastic boxes and measuring tapes. Each box was numbered, and if you turned them around, you could see that they contained silicon vaginas. The teacher asked the students how they would feel for cervical dilation. A few of the students held out their thumb and first finger a little apart. She shook her head, no. Several other students held up their first two fingers and she nodded and did the same.
The students then measured varying distances of the space between their fingers with the measuring tape. “You need to know how wide your fingers are at 0 to 10 cm” the teacher said. It was incredibly hard for the students to keep this distance stable because the students’ fingers had already been squished together as they made their way out of the silicon vaginal canal. It was a matter of springing them back into place, where they thought they just were when inside the model. The teacher described how they may lose the width when they brought their fingers outside the simulator but that they needed to learn to know the feeling––she described it as proprioception––of the space between their fingers. They then were taught to constantly measure their fingers against the measuring tape to determine the amount of cervical dilation.
In this way, the students are being taught to build a haptic memory of a fleshy distance, an embodied approximation of a measurement made possible because of the measuring tape (see Parrinello, Benson, and von Hardenberg [2020] for a history of estimated knowledge in science). Measuring the width of a cervix is very difficult to do with a measuring tape itself––access is hard. In order to train their haptic memories, the students were taught to try different models with different centimeter dilations and so in effect were learning differences relative to each other, both in numbers and in sensations. The teacher also felt inside the models to remind herself of the sensation. As the teacher watched a student bring her fingers out of the model tightly bound together, she tried to teach the students how to measure the distance of their fingers by springing them back in place then aligning them on the measuring tape.
It might seem like a simple event, trying to learn the distance between two fingers, but actually, it is a rather extraordinary one, considering how much this knowledge becomes part of birthing decision-making in clinical contexts, where centimeter dilations are important medical facts, for example, when a woman gives birth or her pain is relieved (see the work of Skeide [2019], which shows how this is otherwise in midwifery). The lesson extracts one moment in this process, exaggerates it, isolates it, and plastinates it, highlighting a component of the skills the doctors-in-training learn. The models cannot show other details of labor, such as how effaced the cervix is for example; nor do they attempt to teach the students about the position of the child. It is simply a haptic memory exercise––0–10cm––one that entails doing sensory-numerical work by moving between sensory experience and a numerical figure that can be communicated to others. This emphasizes that the numbers do not necessarily (or only) dominate and reduce but are rather they are part of the encounter, part of the making of distance. The sensory-numerical work matters in the enactments and choreographies of birth, entailing on the doctor’s behalf, a movement back and forth between different ways of assessing and articulating information.
These qualities of the cervix do not precede measuring; they are not objective features of childbirth. They come about because of measuring. There is a back-and-forth between bodies and numbers; the numbers do not only dominate. This relationality and the constant translations that occur constitute sensory-numerical work and transforms the seeming nonsensuous numbers into having sensory effects. Sensory-numerical work can be seen as a kind of “number-sense” that archaeologist Lambros Malafouris (2016) explores as an embodied process developed through engagement with artifacts. It is an oscillation and blurring between bodies and objects, numbers, and sensation.
The somewhat exaggerated examples of measuring bodies that I have presented here so far are insightful because they show how medical measuring and metrics are made not only in classification systems and public health programs and tools but also in the very bodies of clinicians. In sensory-numerical work, skin and plastic, tape and flesh, and numbers and sensations are involved in crafting the medical student’s inner scaffolding in dynamic ways. The measuring device, the measuring body, and the measured do not exist on their own, they are closely related. That is, in the words of Hoel and Carusi (2017, 2018), there is a co-constitution between the measured phenomenon and the standard of measurement or what Mol (2002) may refer to as an enactment of particular kinds of bodies through measuring. Here, everyday (if you are at medical school), measurements come about in the practices of measurement, and they do not precede it. In the process, the medical students’ bodies also become standards of measurement, crafted through inner scaffolding that is made with the measuring tape. In the following section, I explore the collective nature of this endeavor and the working toward a communal and coordinated kind of sensing.
Coordinating Sensing
The first-year medical students move on in the curricula from their cervical measurement class and are now taking their second obstetrics tutorial at the Skills Laboratory, learning how to examine a pregnant woman. Previously, they learned how to take pap smears on truncated (headless, legless, and armless) leather models, but this is their first time with a slightly “more fleshed out” mannequin, the pregnant woman (still no arms or legs, but this time a protruding abdomen). When the students come to class, they find the very same model that is pictured above (see Figure 3) and that also illustrates this lesson in the local textbook. After some chat about the homework and questions, we all go to the mannequin, and the teacher asks the students to take turns examining the model. The first student stands to the left side but then has to move to the right, for she is reminded by her teacher that that is the “right” side for physical examination. By this, the teacher is referring to the tradition that students learn to examine patients from this particular side of the bed. When I asked for some explanation, I heard many different theories for this, including best access to the heart, but my guess is that what it allows for is an easier baseline for later improvisation.
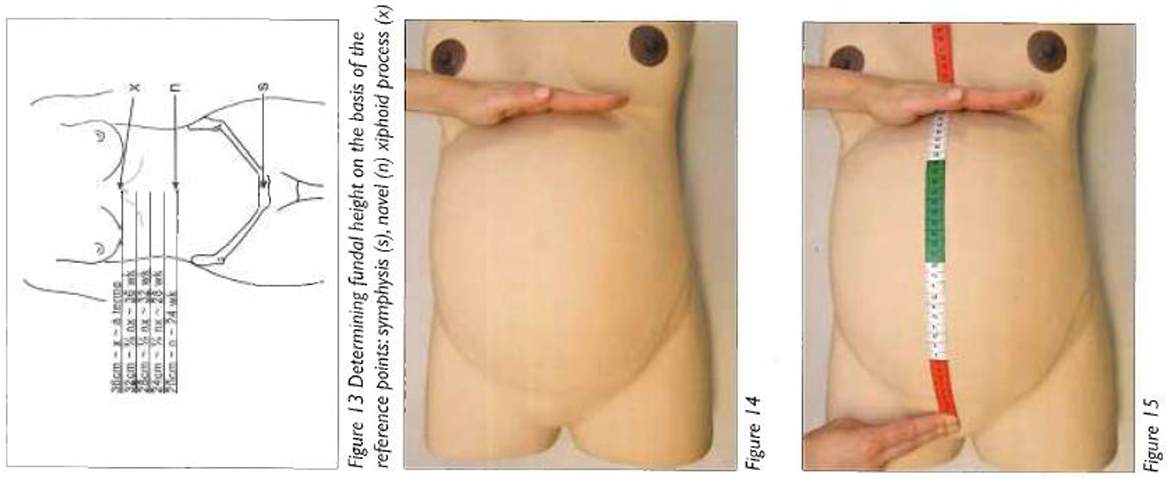
Measuring gestation, Skills Laboratory workbook.
The student takes out the measuring tape and puts the number 0 on top of the bulging belly––a natural inclination, I remember thinking, that they are measuring from top to toe. But no, again: 0 is at the pubis, the teacher tells her. They are measuring “up” the body. The same kind of reorientation happens when medical students learn to read computed tomography scans: they must learn not to look down a body but up a body, as if they are looking up from the feet. When a student asks why you start there at the pubis, the teacher answers that this is a place you can always find, the pubis, a good anatomical orientation point. The student measures up the belly and quickly announces 37.5 cm as the distance. The teacher thinks she has gone too fast: “did you find the top of the uterus?” she asks. “The hard thing at the top?” the student replies. “It’s difficult with the model,” the teacher offers and walks around to the other side of the model and lets out some air. “There, that should make it a bit easier,” as she deflates the model’s pregnant belly slightly. The student measures again and finds the model’s belly from top to pubis to be 35 cm. The teacher asks, “so what does that translate to?” The student stumbles and pauses, “umm 31?” “Well you have the four bit right,” the teacher says, “but you must add four not subtract––so she is thirty-nine weeks.” The students are learning how to turn centimeters into weeks.
Many students start practicing measuring on their own at this point, but they all have the same problem: the pubis bone of the mannequin is made of foam, whereas the underlying structure is harder. So, they keep mismeasuring. The teacher assists them by helping them recalibrate their techniques since the model’s materials are misleading: “the umbilicus should always be 20 cm, so twenty-four weeks,” she says, almost as if to herself. A student asks whether this is the same measurement on all women, and the teacher replies that “no, but more or less.” There is some reduction here to numbers, but also, the measuring practice is shown not to work so well, which students need to start to deal with. The teacher’s technique of helping them with a good “rule of thumb,” that the umbilicus is at 20 cm, is a sensory-numerical tip, a way of making the numbers sensate. This will be built into the inner scaffold, a practice that students can use to understand misleading models, or when there is no measuring tape at hand.
This measuring body is not a static point of reference but is continually crafted in relation to objects such as this model, a model that coordinates collective behavior in and across classes. Coordinated sensing helps to craft corresponding inner scaffolding so that doctors can use their embodied estimates to speak to each other––to let a midwife or obstetrician know over the phone how far dilated a woman is in labor, for example. The novices perform sensory coordination by embodying the object of measurement into their very techniques and descriptions. The measuring tape examples show how knowing is not a simple matter of matching sensory knowledge to the tape. Rather, the tape and the act of measuring are co-constitutive, and it is through the embodiment of the sensory-numerical work that the tape helps create the measuring body. Hoel and Carusi (2018) also point out the importance of technologies as standards in their own right and also, importantly, as ways of coordinating collective behavior––that is, through their ability to create a “shared vision through alignment and repeatability” (p. 62), which is evident in the lesson with the models. What is important to remember is that the measuring body is being made not only with measuring tapes alone but rather with a distributed system of bodies, technologies, environments, and so forth. Found in the Skills Laboratory, that system becomes part of these educational practices that more broadly in medicine attempt individual and communal calibrations.
Examining this sensory-numerical work of coordinating in a distributed system that includes models, homework, tapes, and many other elements ties into insights from the STS literature on intersubjectivity or the study of how subjective sensing can be translated into objective measurement. Sensory science scholars have made similar points about shared vocabulary learning when it comes to making perfumes (Teil and Hennion 2004), or tasting wine (Shapin 2016) or tea (Xiao 2016), or discussing the “intersubjectivity engine” (Shapin 2012) that creates standards against which practices are calibrated. There is a long history of studying attempts at objective measurement in medicine, all of these measuring objects tied into vast networks of skills, objects, and ideas, and all part of the embodied practices of physicians. Some even argue that practices such as auscultation changed the very perceptive abilities and focus of the medical profession (Lachmund 1999). Most of the discussions about such measuring objects in medicine are often around the introduction of what is seen as a radically new technology (e.g., stethoscopes and X-rays; Lachmund 1999; Pasveer 1989)––innovative tools that are viewed as having changed the face of medicine. As in other domains of STS (Oudshoorn 2020), there is less focus on practices concerning humble everyday materials that seem to seep into medical practice, such as the measuring tape. Such objects still work, as the public health work I referred to earlier shows, to coordinate medical practices on huge scales with large effects. In the next section, I speculate on how the concepts that have arisen from fieldwork in medical schools may translate into medical work in clinical settings.
Beyond Medical School
I have focused so far in this article on the sensuous embodiment of the often thought of as nonsensuous––numbers––what philosopher Jane Bennett (2020) may call a form of “influx.” I have not focused on what she might refer to as the “efflux” and on how this measuring body that is made in medical school comes to measure and exert effects on the world. Over the many years I have spent in medical schools and hospitals in Australia and the Netherlands, it seems in fact that the measuring tape almost becomes erased as an object in clinical settings. And though I encountered it frequently during my son’s community health visits, for example (see Figure 4), I have rarely seen clinicians or medical students using measuring tapes in their physical examination of patients in clinical situations.

Measuring head circumference, Skills Laboratory workbook.
Often physical examination practices in “the clinic” only resemble what is taught in the medical schools. Similar to the “artificial set-ups” (Latour 2004) of wine tasting, physical examination classes in the Skills Laboratory are, as Muniesa and Trébuchet-Breitwiller (2010) write in relation to perfume testing, “presented as a preparation for reality, for a reality external to it, but not as its replica. It resembles that reality a little, but it is most of the time quite different––sometimes openly odd” (p. 232). Rather than the choreographed, long, object-filled interactions that happen in medical school lessons, physical examination in the clinic often involves quick assessments, in emergency departments, or in a ward round. A doctor may pull out some instruments, the stethoscope, for example, for a quick listen, but the measuring tapes are reserved for more detailed examinations in other places.
And yet, I saw students and doctors use their fingers, their eyes, and their bodies to measure all the time in the clinic. I saw doctors lay their hands over lumps, spread their fingers across chests, and note “estimated truths” (Parrinello, Benson, and von Hardenberg 2020, p. 3) of distances in their notes in clinical charts. These simple measuring acts were subtle, almost imperceptible, and that underscores my point. Measuring becomes part of an inner scaffold and becomes encompassed in the medical student/doctor-in-training/clinician’s embodied ways of knowing bodies. What mattered in the Skills Laboratory, where I have focused my attention in this article, was that the doctors themselves were becoming measuring bodies. At this point, future clinical interactions are imagined. There is, as Bennett (2020) would put it, “a void between bodies that only a leap of imagination can cross” (p. 28).
Conclusion
How much is a pinch or palmful of salt (Nosrat 2017)? Can you imagine the physical distance of 1.5 m as a kangaroo (Poposki 2020) or a caribou (Cecco 2020)? How do you measure feet and inches across a room––with your feet (Werner n.d.)? Just as bodies have long histories of being measured, so, too, bodies are always being implicated in measuring. Numbers are, as Verran (2001) writes, “uncompleted, partial, and distributed” (p. 106), located in their performance. STS has predominantly focused on the performance of measured bodies and on measuring in sensory science, and in this article, I contribute a different perspective that of the measuring body made in educational settings. It is an attempt to look at how numerical measurements, and, more broadly, technologies, are embodied in one particular site of medical education, where I observed and felt traces of objects in medical learning becoming part of what Hoel and Carusi (2018) refer to as “inner scaffolding” and the “measuring body” (p. 47).
Rather than focus on shiny instruments or infrastructures of science, or the imagined futures of sparkling new technologies, as is often the case in STS, a simple and classic object of measurement in medicine, the humble and ubiquitous measuring tape, takes center stage. Specifically, I looked at how an inner scaffolding is crafted through lessons with this instrument in medical schools. The scaffolding is like a dressmaker’s pattern that is constantly tinkered with for different bodies, a sensory archive that helps to orient the doctor in their work. I suggested that the inner scaffold is crafted through a particular form of sensory-numerical work where calibrated, standardized measuring systems––numbers––are embodied into sensory knowing. I looked at how this work occurs in a distributed ecosystem of objects and bodies, where sensory coordination takes place. In clinical situations, the performance of the measuring tape disappears, but the sensory-numerical work that happened with these tools in medical school has left archival traces, in the form of the inner scaffold, and we can see it in the subtle bodily measuring practices of clinicians. That is, while measuring tapes might only reappear physically at certain moments in doctors’ actual clinical practices, the implication of my argument is that this object may in fact have much more wide-reaching material effects in clinical work than has been previously discussed in STS and anthropology literature: through the making of measuring bodies.
In Hoel and Carusi’s (2018) eyes, measurement is thought of much more broadly than with regard to its quantitative meaning; yet, I stuck close to numerical relations and the very materialization of measurement in everyday life. I considered the measuring tape as a mediating artifact and that medical students create their own bodies as the “standard or measure of things.” In order to make my claims, I drew upon my ethnographic research about how measuring practices are learned and taught in a Dutch medical school, finding visible traces of the making of measuring bodies at work. I focused in the latter half on a series of obstetrics lessons where the measured did not precede the measure but was rather crafted in the acts of learning. My research team has studied different sociomaterial contexts of learning medicine, with different constellations of objects, bodies, curricula, and so forth. These are not discrete configurations; there is overlap through transnational exchanges of ideas, colonial legacies, donated and moving objects, and so forth. There is more to write about from this work about the educational environments that go into making bodies.
How does this particular ethnographically informed piece of writing contribute insights of value to the field of science and technology studies? I suggest that taking a simple educational object, as other STS scholars such as Barany and MacKenzie (2014) demonstrated with chalk in mathematics, for example, reveals something significant about how bodies are enacted through materials and how bodily knowledge is produced and reproduced. For centuries, scholars, Merleau-Ponty included, have grappled with how to consider the complex relationship between things and embodied knowledge, between materials and knowing, with important contributions concerning medicine coming from STS (e.g., Dalibert 2016; Slatman 2014; Oudshoorn 2020).
Recently, sensory scholars have looked at the materiality of sensing bodies as calibrated in sensory science settings such as perfume or food testing. The concerns of these sensory scholars are related and differ from my own. First, they look at a form of bodily transformation where sensory capacities are calibrated, to instruments, standards, and each other, whereas I have offered a more phenomenological understanding of the making process, suggesting that “inner scaffolding” can be thought of as central to this sensory education. And while many STS sensory scholars look at how the body as measuring instrument is trained and calibrated in experimental or tasting sessions, I am concerned with how a measuring body is educated and made in explicitly educational environments. Such settings, particularly those in higher education, have received less attention in STS yet are highly valuable sites for studying knowledge creation. This article extends the existing conversation in STS about the materiality of education beyond primary schools and fields such as mathematics, where most have concentrated their attention so far, to join those looking at other fields of study, specifically medical education.
While Hoel and Carusi (2018) may be correct in their claim that phenomenological theory, and in particular the work of Merleau-Ponty, has not had wide-reaching effects in STS, the body as a topic of study certainly has. As many show in their work, bodies are not static entities, they continue to be modified, transformed (Hoel and Carusi 2018), and enacted (Mol 2002)––whether the bodies of clinicians or those with whom they will work. The worlds created in medical school sites such as in the Skills Laboratories that I spent time in, but also in dissection rooms, microbiology labs, and lecture theaters, are places where future, imagined patients are crafted. These are worlds that “exhibit particular styles or patterns, and in so doing, enact a specific ‘type of organizing’” (Hoel and Carusi 2018, p. 58) knowledge. While many focus on the development of professional identities in educational sites like medical schools (most of the classic but also more recent medical school ethnographies), in this article I show that attention to the measuring body is another way in which to understand the organization of fields of practice such as medicine. The sociomaterial environments of learning have a currently underestimated effect on how students learn to perceive, orientate within, and imagine future patients.
Taking direction from scholars who encourage others to not take embodiment for granted but rather look at how it is made to matter (Yates-Doerr 2017), to not assume concreteness of numbers but rather to see how they are afforded life through their entanglements with situated practices (Rhodes and Lancaster 2019), this article has also contributed to the growing body of literature in STS on metric work. I have contributed to this conversation by taking a step back from clinical work to look at the clinician in the making, looking at how metrics and measurement are ingrained and crafted in educational settings. It is just as important to look at the making of measuring bodies as well as measured bodies. This subsequently offers insights into how systems, infrastructures, and practices of measurement are learned and reproduced over and over again in so many health domains, with serious effects on the lives of individuals and groups via, for example, the diagnosis of disease through physical examination or decisions about whether to order tests. If we are to take seriously the STS claim that things could be otherwise, then we need to look at, and potentially intervene in, this particular stage in the reproduction of medical knowledge. Paying attention to and helping to shape the material conditions of learning in medicine becomes an important and possible site of situated intervention (Zuiderent-Jerak 2015) for STS scholars of medicine.
Insights from this article could be taken in new and refreshing directions, for example, by those studying other numerical-sensory entanglements such as self-tracking or artificial intelligence practices that concern making sense of numbers and complicated relationships between algorithms and embodied knowledge (e.g., Wernimont 2018; Lupton and Maslen 2018). It also relates to work on contemporary cyborgs (Oudshoorn 2020), telemedicine (Pols 2012), and sensor technologies (Gabrys 2019), concerning the dynamic work that numbers do in mundane healthcare practices. These are fields of study where occasionally numbers are seen to be paramount but in fact need to be considered not in opposition to a sensory way of knowing but part of it. These avenues of exploration could also be a way of developing Hoel and Carusi’s (2017, 2018) work further and bringing more phenomenology into STS, in particular their intriguing notion of “style,” acknowledging that different styles can coexist in medical work. It may indeed be the juxtapositions and oscillations of these coexisting styles where we find most value (Verran 2001; Harris and Wojcik 2020). In any case, it will be important not to assume the status of objects in learning, particularly those mundane and taken for granted ones, but rather to take our considerations, as Hoel and Carusi (2018) suggest, “from the middle of things” (p. 64), and to continue our attempts, as Shapiro (2015, 373) puts it so well, to “ethnographically elucidate the ‘somatic modes of attention’ that render [the] minute knowable.”
Footnotes
Acknowledgments
The anonymous reviewers were generous with their time and comments and suggested wonderful ways and literatures to expand and articulate my argument. Thanks to Katie Vann and Edward Hackett at Science, Technology, & Human Values for refining this even further and for suggestions for future work. I am grateful to Ike Kamphof, Andy McDowell, and John Nott who shared comments on much earlier and rougher drafts and Candida Sanchez Burmester for her intellectual and administrative input. Thanks also to the organizers and participants of the 4S 2020 online/Prague panel “Health, care (dis)abilities” for their comments and questions. As ever, I am grateful to the generosity of those I work with in my field sites, for their time and critical ideas, and for the collegial support of the rest of the Making Clinical Sense team. Finally, gratitude for my husband who shared parenting during our various pandemic lockdowns, which meant I could carve out time to write and revise.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: “Making Clinical Sense” is funded by the European Research Council under the European Union’s Horizon 2020 research and innovation programme (grant agreement No. 678390).