
Abstract
Abstract
Background:
Research and policy emphasize that attending school every day is critical, yet the reasons why students miss school remain less understood. With growing concern over absenteeism, it's essential to develop a more nuanced understanding, especially regarding absences related to preventive health care. To exemplify this issue, this study focuses on whether students miss school for reasons such as routine dental care.
Research Question:
To what extent are children missing more days of school or experiencing a higher likelihood of chronic absenteeism due to preventive dental care (i.e., 6-month dental visits)? We also explore whether dental visits serve as a proxy for socioeconomic advantages, such as income or insurance coverage, and whether those factors explain attendance patterns.
Research Design:
Using data from the Early Childhood Longitudinal Study, Kindergarten Class of 2010–11, we examined the association between going to the dentist and children’s absences in the earliest years of schooling. Using a sample of 23,470 student-by-year observations, we used several regressions with a student-level fixed effect approach to examine the relationship between preventive dental visits and missing school. We also tested what student characteristics predicted both dental visits and attendance outcomes.
Conclusions:
We found that regular dental visits are more common among students with higher income and insurance coverage, yet these socioeconomic indicators do not predict absenteeism when dental visits are used as the predictor. Preventive dental care is associated with only minimal school absences and not with chronic absenteeism. These findings suggest the need for more targeted attendance messaging and raise the potential value of school-based health services, especially for families less likely to access preventive care.
Even before the COVID-19 pandemic started, data showed that students were missing copious amounts of school days (Gee et al., 2023). In fact, the term “chronic absenteeism,” most often defined as missing 10% or more of the school year, was used at least as far back as the early 2000s (Epstein & Sheldon, 2002), long before COVID-19 emerged. Hence, attention paid to monitoring students’ absences has been well established. And this attention is well justified—a growing body of interdisciplinary research now supports that missing school is associated with deleterious outcomes (Ansari, 2022; Ansari et al., 2023; Aucejo & Romano, 2016; Gershenson et al., 2017; Childs & Grooms, 2018; Childs & Lofton, 2021; Gottfried, 2009, 2011, 2014; Liu et al., 2021; Singer et al., 2021). Given this ubiquitous and unambiguous stance from within the research base, it appears justified that policy has encouraged students to attend school as frequently as possible (California Office of the Attorney General, 2014; Ely & Fermanich, 2013; Ujifusa, 2016).
In practice, school and district leaders have been responding to the calls from research and policy to address chronic absenteeism. For instance, schools have increasingly adopted programs that incentivize attendance by either rewarding or punishing students and their families (Robinson et al., 2021). Aside from school programs, the legal system has also been involved in addressing absenteeism. These laws often require schools to report students with excessive absences to local authorities, potentially resulting in legal action against parents or guardians. The intent behind such laws is to hold families accountable and underscore the importance of consistent school attendance. As an aside, the effectiveness and fairness of these programs and laws continue to be discussed (Keppens & Spruyt, 2020).
Therefore, from numerous stakeholder perspectives—academic, policy, practice, and legal—school attendance has been framed as essential, and any deviation from that has been perceived as a problematic. For all of the cross-disciplinary and cross-institutional conversations about having children present in school as much as possible, why and when students miss school is less understood—as has been the case for decades (Gottfried, 2009). Most often, we have details on whether students’ absences are excused or unexcused (Gottfried, 2009). This is helpful as a baseline because this distinction helps schools most often distinguish between illness and disengagement (Gottfried, 2009). Yet, both excused and unexcused absences count toward becoming chronically absent because chronic absenteeism is a measure of total days missed. Without a clearer understanding of more specific reasons why students miss school, it becomes difficult to assess the relative importance of being in school versus not on a given day, making it challenging to understand the meaning of what contributes to being absent. That is, it is challenging to assess how to understand why students are absent and whether those absences may be necessary, legitimate, or desirable.
To this aim, in this study, we exemplify one instance (of many) in which students are missing school for what we believe are legitimate and desirable reasons: namely, dental health care. Prior research has demonstrated that student health directly links to absenteeism, where students with poorer health are more likely to be absent (Allen, 2003; Bloom et al., 2006; Gottfried, 2017; Graves et al., 2019). Absences in the domain of illness and poor health issues certainly fall into the excused category of absences (Gottfried, 2009). These are absences that are likely unexpected and are often out of the control of students and their parents—for example, it is unlikely anyone plans on getting the flu. Yet, these absences are counted toward students’ total counts of absenteeism, contributing to how students’ educational progress is tracked, monitored, and evaluated. At the same time, it would be difficult to find supporters of sending ill children to school.
That said, other forms of excused absences pertaining to health also count toward students’ absences: missing school for preventive health care. We know very little about the link between preventive health care and missing school—that is, absences that are in students’ (or parents’) control but still pertain to health. In this study, we focus going to the dentist as an example of preventive health care. A focus on dental care is valuable because tooth decay and cavities are among the most common chronic disease among children (Padung et al., 2022). To avoid these issues, the American Academy of Pediatric Dentistry generally recommends a 6-month interval for preventive dental care visits for school-age children (American Academy of Pediatric Dentistry [AAPD], 2023–2024). Therefore, in this study, we define preventive dental health care as this 6-month interval, and then we explore the link between regular 6-month interval checkups and missing school.
Regular 6-month dental checkups for children are essential for maintaining optimal oral health and preventing issues such as cavities, gum disease, and tooth decay. These visits also offer opportunities for education on proper oral hygiene practices and the importance of a balanced diet. Early detection and treatment of dental problems during these checkups can prevent them from worsening and becoming more costly to address later (AAPD, 2023–2024). Clearly, prioritizing routine dental visits contributes to overall well-being.
However, preventive dental health visits pose a conundrum in light of how we process and understand what it means to miss school. On one hand, Ruff et al. (2019) found that poor oral health was associated with more absenteeism. In their meta-analysis, these authors found that going to the dentist on a regular basis is associated with better school attendance in the long run. Children who went to the dentist more frequently were able to attend school more frequently because of less mouth pain (Seirawan et al., 2012). Unsurprisingly, students in pain do not want to attend school. In turn, regular routine checkups with dentists could increase general oral health, implying that students will attend school more regularly and in turn be experience higher academic outcomes (Blumenshine et al., 2008; Detty & Oza-Frank, 2014; Seirawan et al., 2012).
On the other hand, with some exceptions (i.e., a school-based health center; Graves et al., 2019), most children in the United States receive dental care at off-site locations, such as dental clinics or private dental offices. In fact, a Google search of the number of pediatric dentists open Monday through Friday showed that these far outweigh the number of pediatric dentists open on weekends. Although dentists’ work schedules vary, many work fewer than 40 hours a week and during standard business hours, with weekends and evenings typically reserved for emergencies (U.S. Bureau of Labor Statistics, 2025). For families to follow the AAPD recommendation to take their children to the dentist for preventive action, children mostly likely must be absent from school. This seems to run counter to the messaging from research, policy, and practice that every school day matters. Therefore, in this study, we asked: To what extent do children miss school for preventive dental care?
The tension that parents must face between the necessity of preventive dental care and the prevailing educational discourse on school absenteeism raises significant questions about how we understand how to process the reasons why children are absent. Although the imperative to maintain consistent school attendance is well supported by research linking frequent absences to negative academic and socioemotional outcomes, the benefits of routine health care, particularly dental care, cannot be overlooked (AAPD, 2023–2024). Preventive health actions, such as 6-month dental visits, are essential for long-term well-being—especially in early childhood—yet they can be perceived as at odds with the dialogue of 100% school attendance policies. This disconnect suggests a need to reconsider how absences are understood within the broader context of a child's overall health and development.
Moreover, the current educational policies and practices that emphasize reducing absenteeism may inadvertently discourage parents from scheduling necessary health appointments during school hours; therefore, we need a better understanding of the extent to which preventive care links to missing school. If preventive health care, such as dental checkups, is viewed merely as a minor interruption to schooling rather than an integral component of a child's academic development, we can better understand when it is important to miss school. It is crucial, therefore, that policymakers and educators collaborate to develop more nuanced approaches to absenteeism that recognize the legitimacy of health-related absences while still promoting regular school attendance.
In light of these complexities, there is a pressing need for further research to explore the specific links between health-related absences on both academic outcomes and long-term well-being. Research should aim to differentiate between absences that are truly detrimental to a child's education and those that, while resulting in missed school days, are crucial for maintaining overall health. By doing so, we can better inform policies that strike a balance between minimizing absenteeism and ensuring that students' health needs are adequately met, ultimately fostering a more supportive approach to promoting school attendance.
Methods
To explore the link between preventive dental health and missing school, we relied on data from the Early Childhood Longitudinal Study, Kindergarten Class of 2010–11 (ECLS-K: 2011). Conducted by the National Center for Education Statistics (NCES) at the U.S. Department of Education, ECLS-K used a sampling design to create a nationally representative sample of kindergarten students. The first round of data collection was in the fall and spring of the 2010–2011 school year and continued once annually through elementary school. The data include information on children and their families, teachers, administrators, and schools.
In total, there were 23,470 student-by-year observations in our sample. The percentage of missing data among the variables used in our study ranged from 0% to 9.4%. We used conventional multiple imputation methods to handle missing data in our study, specifically multiple imputation via chained equations, generating 20 sets of plausible values for observations with missing data (Kontopantelis et al., 2017; Royston, 2004). Consistent with NCES reporting guidelines, sample sizes were then rounded to the nearest 10. We ensured the national representativeness of our findings by using the appropriate probability weights provided by ECLS-K to account for differential patterns of response and nonresponse.
Six-Month Dental Care Visits
In the spring of each kindergarten, first-, and second-grade year of data collection, parents were asked about their children’s dental visits: “How long has it been since your child’s last visit to a dentist or dental hygienist for dental care?” To align with the AAPD definition of preventive dental care, we coded responses into whether or not a child had visited the dentist within this recommended period of 6 months. Overall, 66% of our total sample had gone to the dentist within the past 6 months. Given that our data are nationally representative, this statistic understandably aligns with descriptive data in other studies. For instance, Blackburn et al. (2022) found that approximately 70% of children in Alabama had seen a dentist for a regular checkup in the previous 6 months.
Absenteeism
We used two measures of absenteeism taken from the yearly teacher survey in the spring of each academic year. First, we used teacher-reported absences reported by six discrete categories: zero absences, 1–4, 5–7, 8–10, 11–19, and 20 or more absences. To improve the interpretation of coefficients, previous studies using the same dataset have recoded these categories to the midpoint of response options; students who were never absent were coded as having 0 absences, and students who were absent 20 or more days were coded as missing 20 days (Ansari & Gottfried, 2021; Gottfried, 2017; Gottfried et al., 2016; Gottfried & Kirksey, 2021). We also used a measure of chronic absenteeism, which we classified students missing 11 or more days. Our classification directly aligns with the measure used for prior research on chronic absenteeism, using data from ECLS-K: 2011 (Gee, 2019).
Control Variables
Table 1 provides a list of independent covariates used in the current study. These variables were derived from survey items on either the teacher or the parent surveys. Given our analytic strategy that follows, we rely only on variables that change over time. First, we included a set of child and family characteristics; these are listed in the table as having a disability, English language learner status, health rating by parents, BMI score, whether the student’s family had insurance coverage, and whether the child lived with both biological parents. Although the dataset did include other child and family characteristics, they did not vary each year and thus would drop out of our analysis, as described in the next section.
Descriptive Statistics for Main Study Variables.
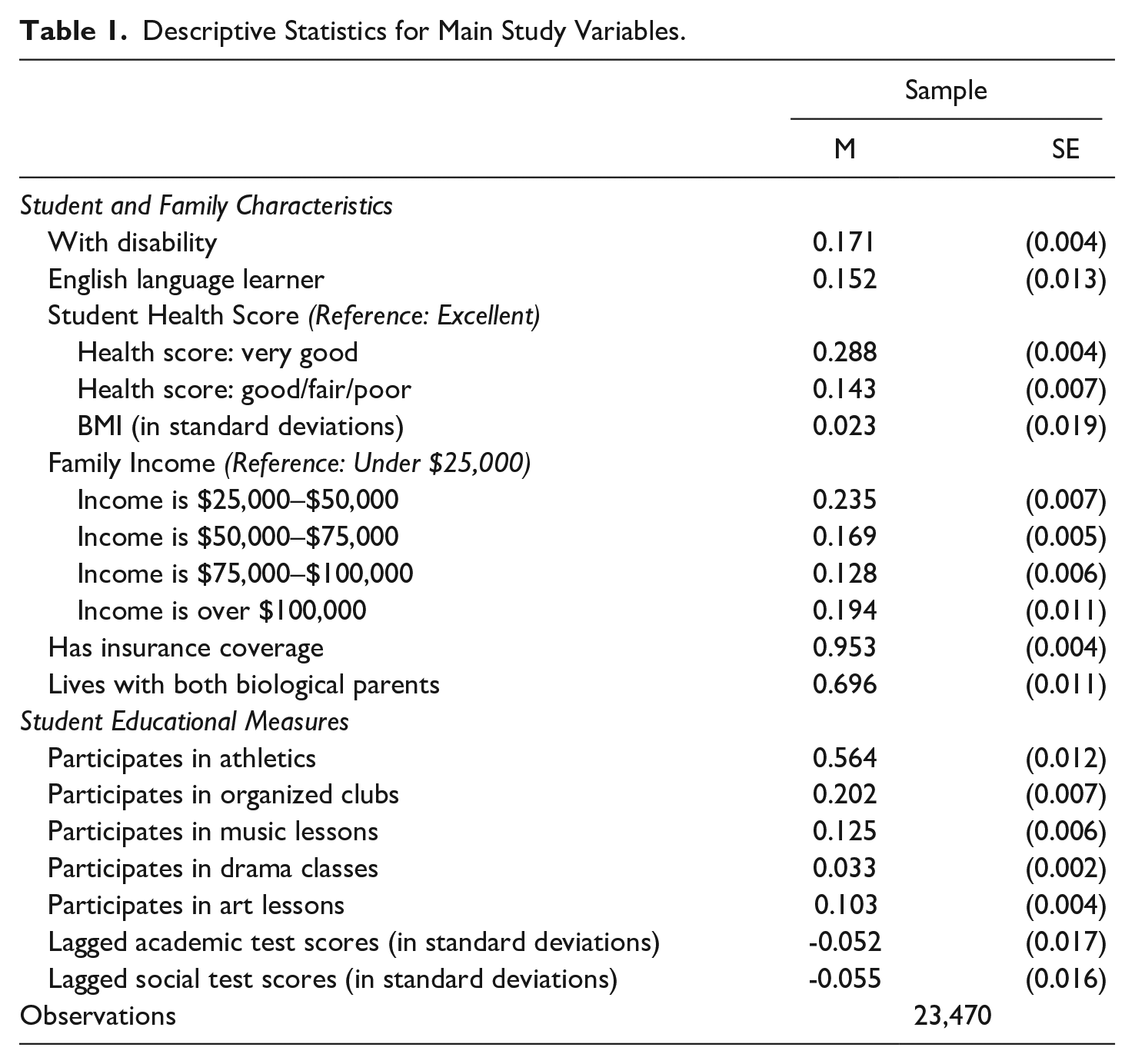
In the second section of Table 1, we list measures that we used that pertain to a student’s educational characteristics. For instance, we included a series of indicator variables to notate what a student participated in before or after school, which might have ramifications for propensity to be more or less likely to be at school (Gottfried, 2019). We also included two measures of a student’s academic ability and developmental outcomes. For academic ability, students had their literacy and math skills assessed each year. Teachers also reported on students’ socioemotional skills using the Social Skills Rating System. From these independent measures, we created two scales: one for student academic achievement (α = .92) and the other for student socioemotional skills (α = .86). We used a lagged index from the previous year for both achievement and socioemotional skills.
Analysis Plan
Before examining the relationship between dental visits and absenteeism, we first explored what factors predicted whether a student regularly attended dental checkups. Specifically, we estimated the probability that a student had visited the dentist in the past 6 months as a function of their background characteristics. The following regression model was used for student i at school s in year t:

In this equation,
Importantly, the longitudinal nature of ECLS-K allows us to observe the same student for multiple years. Thus, we can use student fixed effects (i.e., indicators for student ID code). The inclusion of student fixed effects holds constant all unmeasured time-invariant student characteristics, which explains why we can only rely on time-varying factors that were included in the ECLS-K dataset. What remains are time-varying measures, such as changes in going to the dentist over time. We examined whether children’s going to the dentist at a 6-month mark could predict student absenteeism by looking at within-child changes in dentist-going. To do so, we began with a baseline model in the following equation for student i at school s in year t:

In this equation,
Given this model structure, in which we compared students with themselves over time, we were less concerned about individual-level differences that would have been influencing going to the dentist or absenteeism. For example, highly involved parents might send their children to school and might ensure that they go to the dentist at 6-month intervals. It would be unreasonable to compare this student with a student who has parents who are not involved and thus may not be as vigilant about sending their child to school or going to the dentist. Thus, the benefit of the fixed effect specification is that we compared the same child across the years of our dataset. In some years, the child had the 6-month checkup, and in other years they did not. That is, our model relied on the variation in 6-month dental checkups; in this way, each student becomes their own comparison group.
Results
First, we wanted to assess which students were more likely to have regular dental visits. Table 2 displays the results for Equation 1, where school fixed effects were included. There are some observable differences in which students regularly visit the dentist. Students in better health are slightly more likely to go, as are those from higher income households. Insurance coverage also shows a strong positive association, though this is less surprising given that nearly 95% of the sample had coverage. We also saw some notable patterns with extracurricular participation, where students involved in athletics or organized clubs appeared more likely to have had a dental visit. This relationship may reflect underlying socioeconomic status. Importantly, the inclusion of these variables also slightly attenuated the magnitude of the income coefficients, further suggesting potential confounding. These patterns underscore the importance of using student fixed effects to account for stable individual differences and better isolate within-student changes over time. In this way, Table 2 certainly motivates our analytic strategy to adopt student fixed effects.
Predicting Regular Dental Checkups by Student Characteristics.
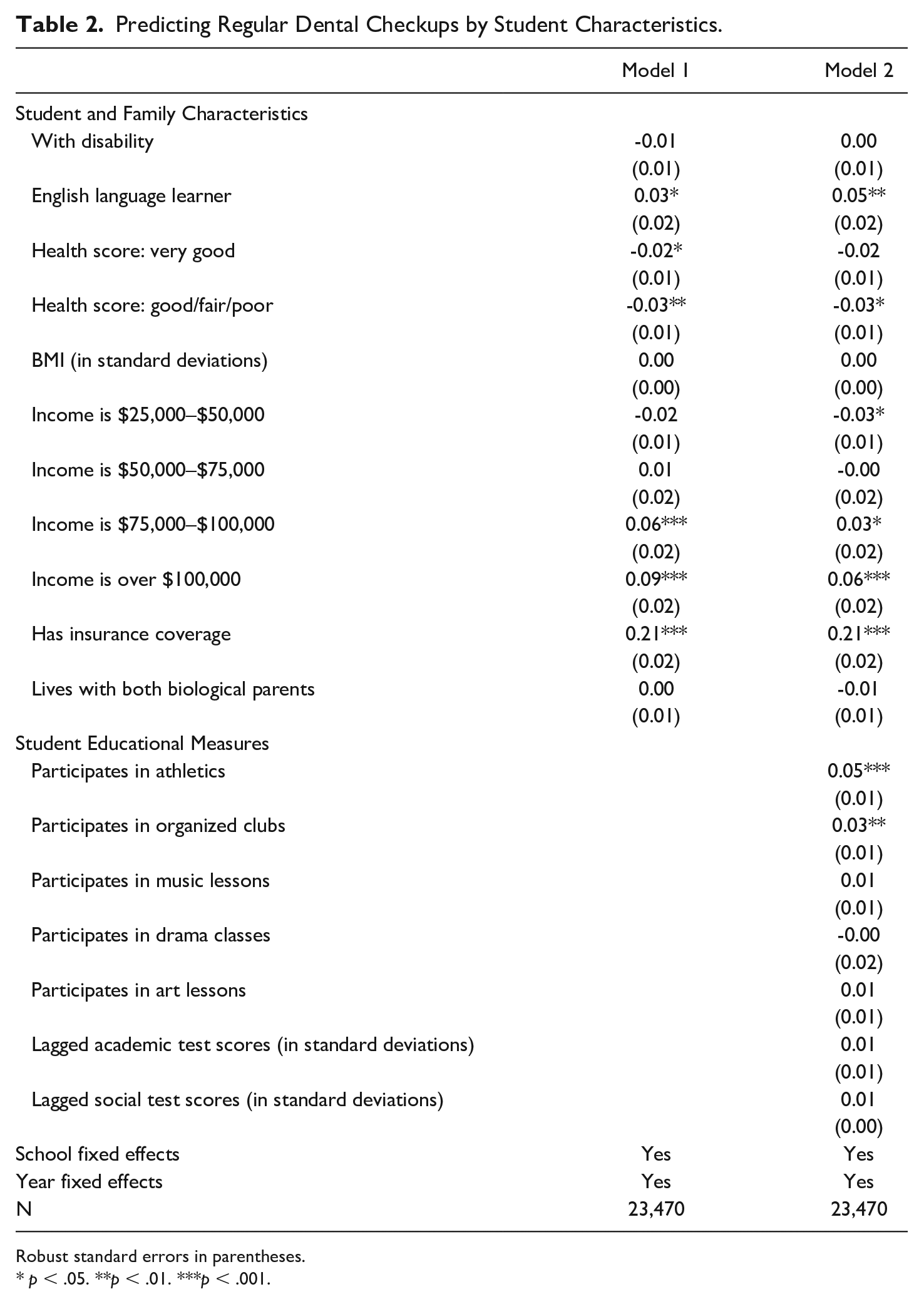
Robust standard errors in parentheses.
p< .05. **p < .01. ***p < .001.
Next, we examined the number of days a student missed depending on whether they had a preventive dental visit. Table 3 presents the results from Equation 2, which includes student fixed effects. Because the outcome here is the number of days absent, the coefficients reflect average within-student differences across years. As discussed earlier, our model includes only covariates that can plausibly vary over time. Standard errors, clustered at the school level, are reported in parentheses.
Estimates of Regular Dental Checkups on Number of Days Absent.
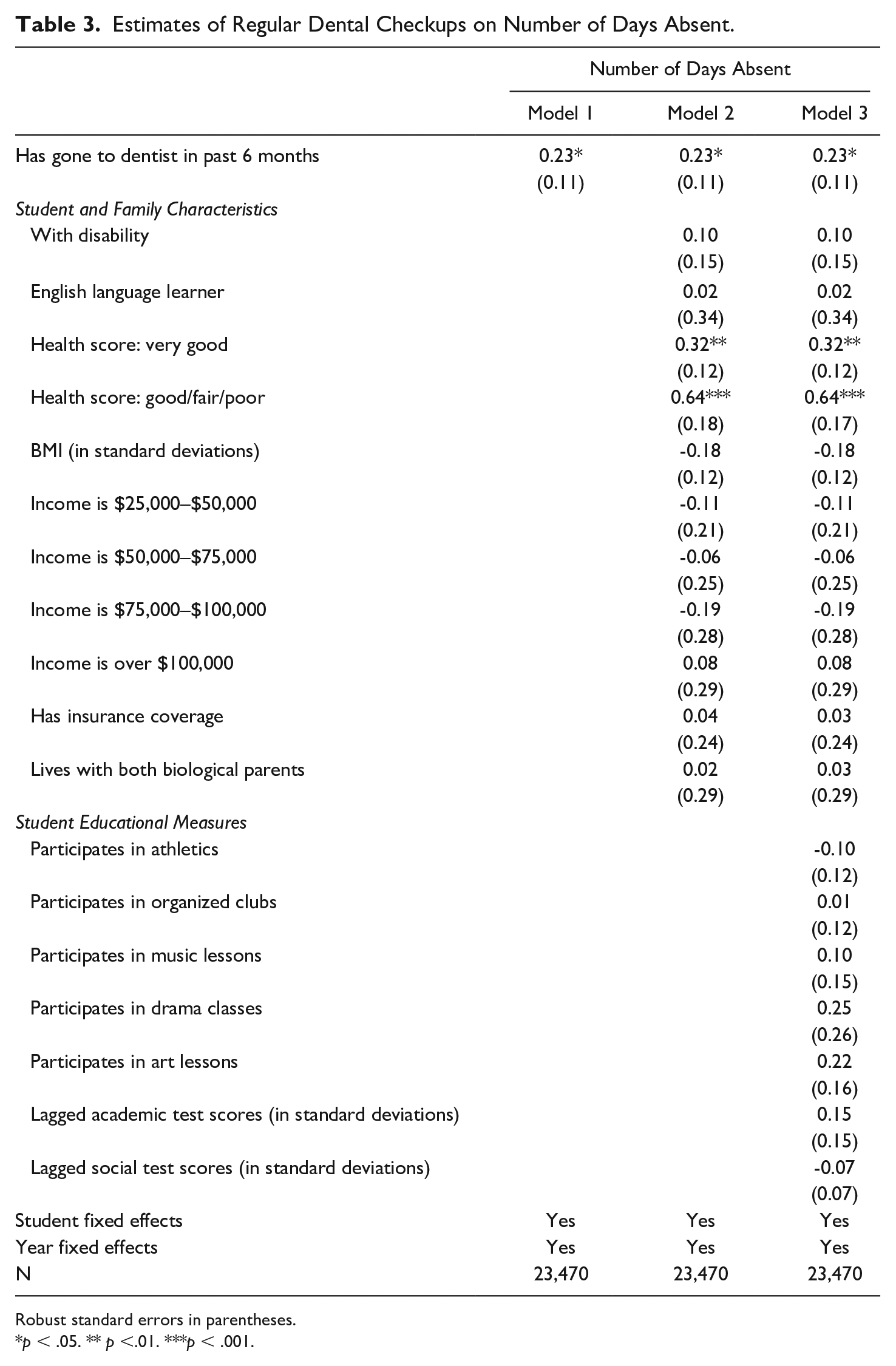
Robust standard errors in parentheses.
p < .05. ** p <.01. ***p < .001.
We began with a model that simply compared students who went to the dentist in the previous 6 months with those who did not. As shown in the first row, students who had a recent dental visit missed slightly more school than those who had not. This finding held even after adjusting for child and family characteristics in Model 2 and adding educational variables in Model 3. Across all specifications, the pattern remained consistent: Going to the dentist within the previous 6 months is associated with slightly higher school absences.
The coefficient in Table 3 is approximately 0.23, or about one quarter of a school day. This finding is reasonable when considering that a routine 6-month dental visit typically lasts 30–45 minutes (Stanford Medical School, n.d.). When accounting for travel time and potential delays, it is plausible that the entire appointment process could result in missing roughly a quarter of the school day, suggesting that the magnitude of the coefficient aligns with the expected time cost of a dental visit. Given the policy relevance of chronic absenteeism, usually defined as missing 10% or more of instructional days, and its links to academic and developmental outcomes, we also investigated whether having a 6-month dental visit was associated with chronic absence.
Table 3 also includes coefficients for parental reports of their child’s general health, offering additional insight into how broader student health may relate to school absences. Relative to students whose parents described their health as “excellent” (roughly 60% of the sample), students rated as having “very good” health missed an average of 0.32 more days of school. This effect is even stronger among the 13% of students whose health was described as “good,” “fair,” or “poor,” who missed about 0.64 more days. These differences are statistically significant and highlight that even small gradations in perceived health can meaningfully affect school attendance. This broader health context helps frame our interest in dental care as one specific, tangible dimension of a child’s overall health. While routine dental visits may seem minor, they reflect a family’s access to and engagement with preventive health services—factors that can influence, and be influenced by, patterns of school attendance.
Table 4 presents the findings for chronic absenteeism, using models that mirror those in Table 3, all estimated with student fixed effects. Across all three models, the first row of coefficients shows that having a dental visit in the previous 6 months is not associated with an increased likelihood of being chronically absent. This result aligns with expectations: Routine dental visits are infrequent, occurring only twice a year, and are not akin to recurring issues such as chronic illness or school disengagement. Moreover, as noted earlier, a dental appointment typically results in missing only about a quarter of a school day—far less than the cumulative absences required to meet the threshold for chronic absenteeism.
Estimates of Regular Dental Checkups on Chronic Absenteeism.
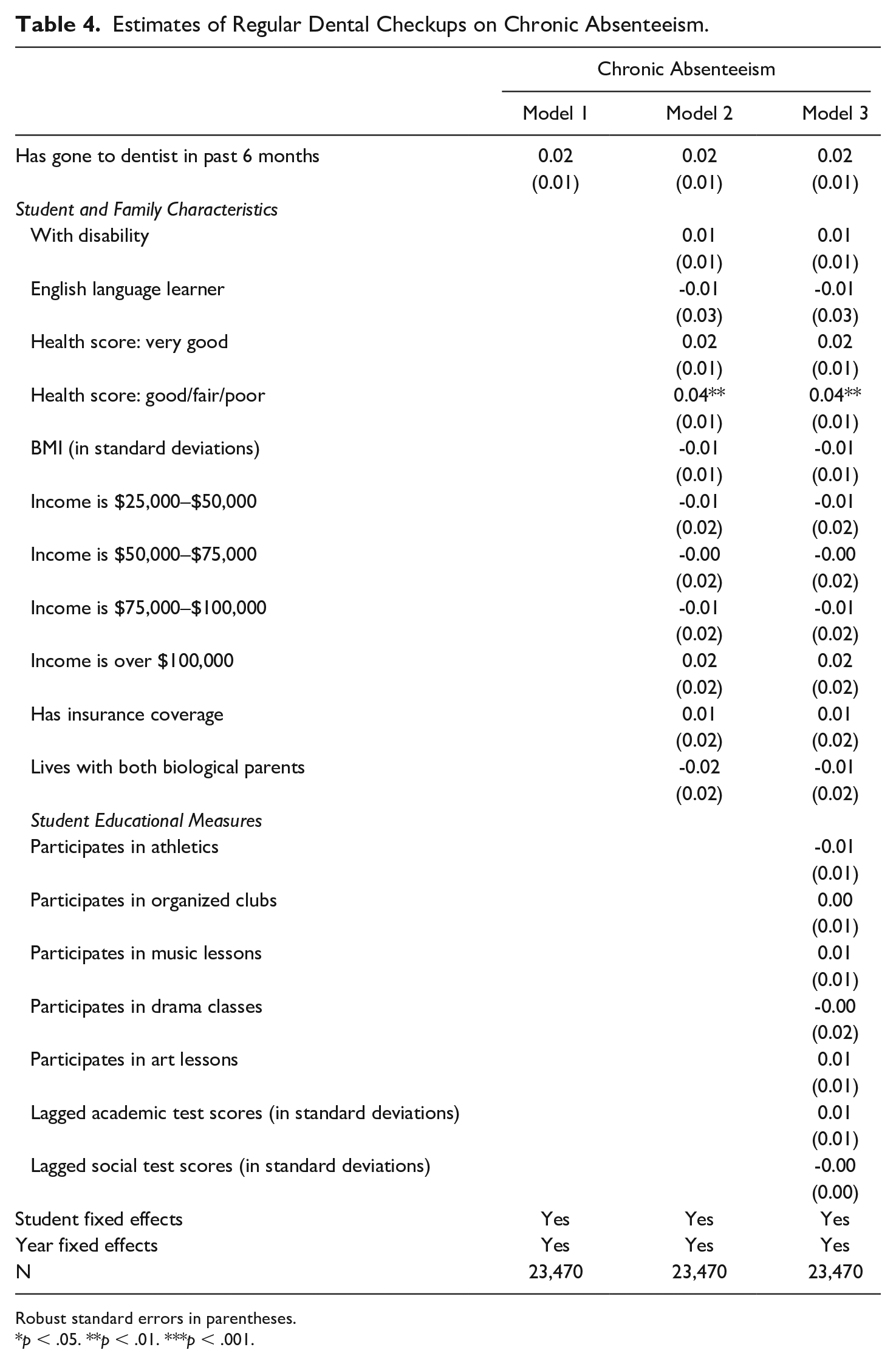
Robust standard errors in parentheses.
p < .05. **p < .01. ***p < .001.
In this way, our main findings here show that preventive dental care was not indicative of chronic absence. An important finding, however, was that going to the dentist did not indicate some sort of larger illness or issue, given that it was not linked to an outcome measure that would have picked up significant bouts of missing school. Instead, given Tables 2 and 3, it appears from our findings that going to the dentist every 6 months maps directly onto missing a small amount of school for exactly that purpose.
Sensitivity Tests
We tested the robustness in our findings in several ways. For instance, students who rode the bus to school may not have parents who could easily pull them out of school for a dentist visit. Therefore, we examined bus riders, who have less flexibility, versus students who went to school in other ways (carpool, walk). Table 5 presents our regressions when we split the sample out for these two groups. The results suggest that only non–bus riders missed school for a dentist visit. Again, these students might have had flexible transportation options (i.e., parents driving them to and from school, as mentioned earlier), which may explain why this group would have been absent for a regular dentist visit.
Sensitivity Analyses.
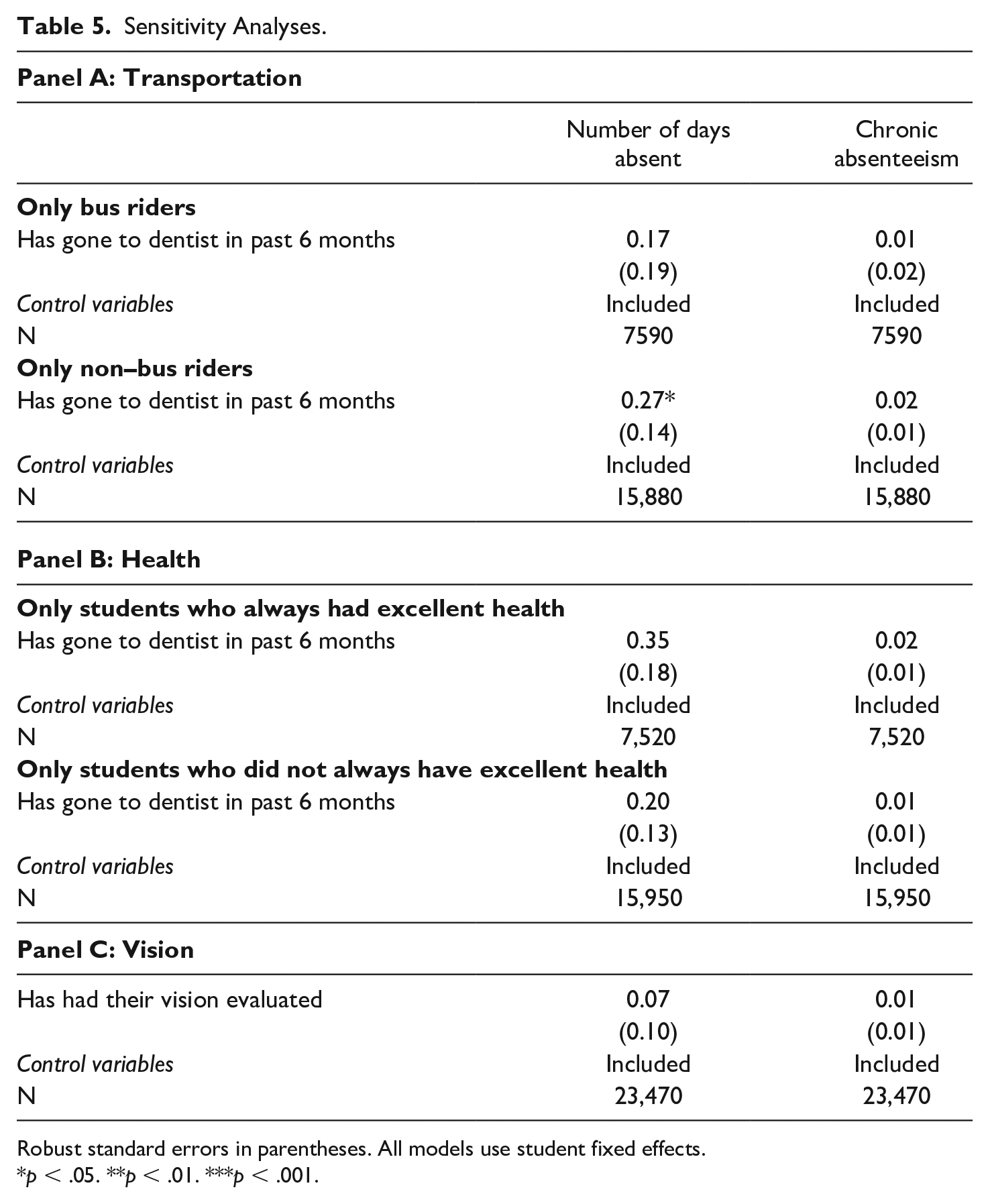
Robust standard errors in parentheses. All models use student fixed effects.
p < .05. **p < .01. ***p < .001.
Next, we examined two groups: healthy versus less healthy. It might be the case that children who are less healthy might be making more frequent dental visits as part of an overall less healthy individual profile. Once again, we divided the sample and ran the regressions. We did not find that different student groups were related to different relationships between going to the dentist and absenteeism. This underscores that the 6-month dental visit is preventive, not due to illness or health issues, and hence supports our main findings.
Finally, we investigated whether students who had their vision evaluated showed differences in attendance. The results can be seen in Panel C of Table 5. The models do not show that there is any link between vision checkups and absenteeism. Although this study cannot pinpoint reasons why, it is often the case that vision tests occur at school itself, whereas dental appointments require visiting an office. In fact, 40 U.S. states and Washington, DC, require vision screening at school (Wahl et al., 2021). Therefore, the lack of findings for vision screening is logical and in line with where students would receive these preventive services.
Although not shown for the sake of clarity, we also examined whether going to the dentist in one year would predict absences in future years. That is, we wanted to test whether missing school for the dentist was just symptomatic of underlying frequent missing-school behavior. The findings were null. In other words, missing school for a 6-month checkup in one year did not have any influence on students’ absences in a future year; going to the dentist this year was related only to missing school this year.
Discussion
Understanding and measuring absenteeism are complex tasks. Although reducing student absences is a clear goal, the reality is that some missed school days are inevitable, whether for necessary or avoidable reasons. To explore how students miss school in practice, this study examined the relationship between preventive dental care and school absenteeism, focusing on whether regular dental checkups contributed to absenteeism among our nation’s youngest elementary school students. The analysis, which relied on nationally representative data of children over time, revealed that although children who had attended dental checkup appointments within the past 6 months were slightly more likely to miss school, these absences did not predict chronic absenteeism. This suggests that although dental visits resulted in missed school days, they did not contribute to the more severe issue of chronic absenteeism, which is associated with significantly higher levels of missed school and negative academic outcomes.
A growing body of research demonstrates that the reasons students miss school matter. Excused absences, for instance, have been shown to have a weaker association with negative academic outcomes than unexcused absences (Gershenson et al., 2017; Gottfried, 2009, 2011, 2014). Ehrlich et al. (2014), examining preschool absenteeism in Chicago Public Schools, found that chronic absenteeism was often driven by health and logistical barriers, with racial disparities in the reasons that children missed school. Similarly, Klein and colleagues (2022), using the Scottish Longitudinal Study, found that most types of absences were negatively associated with high-stakes exam performance, albeit to varying degrees—highlighting that the impact of absenteeism operates through multiple pathways beyond lost instruction. In short, the reasons behind student absences matter deeply for understanding their consequences. As researchers begin to disentangle health-related absences from other types, it is essential not to treat all health absences as the same. Differentiating between preventive care, chronic illness, and acute illness could offer valuable nuance in how absences are tracked, interpreted, and potentially addressed through policy or intervention.
Limitations
Although this study provides important insights into the relationship between preventive dental care and school absenteeism, several limitations should be noted. First, the use of secondary data from the ECLS-K limits the scope of variables available for analysis. Although the dataset is rich, it does not capture all potential factors that could influence both dental visits and absenteeism, such as changes to parental work schedules, school schedules, or access to transportation. It does also does not include reasons for choosing a specific dentist, the distance of the dental office from school, or the appointment time.
Second, the measure of dental visits is based on parent-reported data, which could introduce recall bias. Parents may not accurately remember the exact timing of their child’s last dental visit. Certainly, having a school record measure of dental visit would be preferred, though this would require educational systems to be linked to health systems. Related to parents, we also do not have parental-reported reasons as to why they would choose to schedule a dental appointment during school hours.
Third, the study focuses on a nationally representative sample, which is a strength in terms of generalizability. However, this broad approach may overlook important regional or demographic differences in how preventive dental care is accessed and its impact on school attendance. For example, differences in state policies regarding dental care, or variations in access to dental care providers in urban versus rural areas, could influence the findings. In addition, policies and practices may have changed since the pandemic, both within and across states. Though the data remain relevant and nationally representative, certainly the context of the data being from 2010–13 should be taken into account when considering how to design current policy.
Finally, the study’s focus on dental visits as a specific form of preventive health care may limit the applicability of findings to other types of health-related absences. Despite these limitations, the study provides valuable evidence on the complex relationship between health care practices and educational outcomes, underscoring the need for further research and policy on the reasons why students miss school.
Implications
The findings of this study highlight that unpacking why and how students miss school is complex. Namely, we found that children are missing school for 6-month dental checkups, but this is not indicative of being chronically absent. On the one hand, this is desirable. The AAPD (2023–2024) has found that regular dental checkups at 6 months for children can prevent oral disease, which would exacerbate absenteeism in the future. On the other hand, policy has emphasized that being in school every day is essential and the only solution to combatting chronic absenteeism (Attendance Works, 2023). Thus, it becomes understandably challenging to make sense of these messages.
As such, we offer implications from our work to help untangle this predicament. Being in school is certainly essential; students miss numerous opportunities when they are absent (Gottfried, 2017). However, we need a better conceptualization of why students are missing school. First, we need to update our measures of absenteeism. Going to the dentist for preventive health care is a positive, healthy behavior. Therefore, we need our absence measures to reflect all types of healthy behaviors so that we can identify when children and their families are making investments in health; as mentioned, long-term attendance patterns are impacted when children remain healthy (Ruff et al., 2019). We need to identify these instances of absenteeism and consider how they should be integrated into our understanding of student absenteeism and into accountability metrics.
Additionally, we can update messaging to parents. Although we want policy to underscore that missing school may be harmful (Gottfried, 2009), it may not always be “bad.” We certainly would not want parents to reduce preventive health visits, given their long-term importance to children’s well-being. Thus, nuance from policymakers and practitioners is required. Perhaps we need a new way of coding absences: excused-illness, unexcused, and excused-preventive. Certainly, the AAPD would argue that dental health is essential and a clear measure to prevent future problems, yet policy messaging does not make this clear in its current rhetoric around attendance.
Our findings underscore the importance of distinguishing between types of absences, particularly those stemming from preventive health care, and how they relate to broader patterns of attendance and student well-being. Although routine dental visits were not linked to chronic absenteeism, they were more common among students with higher income and insurance coverage, suggesting that they may signal broader family capacity to prioritize preventive care and overall child flourishing. Future research should examine whether the same socioeconomic variables that predict regular dental care also correlate with stronger overall attendance, potentially revealing a constellation of protective factors. Moreover, understanding absenteeism among children less likely to access routine checkups, such as those with limited transportation options or lacking consistent health care access, could help identify subgroups that might benefit most from school-based health interventions. By highlighting how routine care and structural barriers intersect with school attendance, this work reinforces the value of holistic approaches to addressing absenteeism.
This work also has implications for establishing systems that enable researchers, practitioners, and policymakers to access detailed information about the reasons for student absences. The differences we highlighted in preventive health visits, such as dental checkups versus in-school vision screenings, illustrate the complexity behind absenteeism. If educational systems were equipped with data on the specific reasons why students are absent, targeted interventions could be developed to address the root causes more effectively. Future research could then consider whether similar patterns hold for other forms of preventive care that were not in the dataset, such as such as doctor visits for vaccinations versus whether vaccinations being provided at school. These data could inform the development of tailored programs that provide in-school services for common health needs, reducing the need for students to miss school. This is the hypothesis that we can generate from our results that suggest a null association between in-school vision screenings and absenteeism.
Moreover, understanding the underlying reasons for absenteeism could help policymakers refine attendance policies to focus on preventing detrimental absences without penalizing necessary ones. This was made even more clear by the fact that only non–bus riders were missing school for dental visits. This may have arisen due to differences in transportation access and scheduling flexibility, which in itself has implications for student absenteeism (Gottfried, 2017). Therefore, when we consider how to build better data systems and support systems to improve attendance, doing so might have multiple implications. First, such a system would enable researchers to study patterns in absenteeism more accurately, leading to insights that could shape more effective attendance interventions and policies. Second, these systems themselves might improve access. If bus riders were not leaving school to see the dentist, then bringing the dentist to school could improve health access in addition to school attendance. Therefore, having comprehensive data on reasons for absenteeism would facilitate a more informed and equitable approach to building systems that improve student attendance and educational and health outcomes.
Finally, if the goal is truly to minimize the number of student absences, then a viable solution would be to provide essential services at school, particularly for students in families who are less likely to access preventive care or have comprehensive insurance coverage. As noted earlier, dental visits typically occur offsite. However, our ancillary results show that students do not miss school for vision checkups because these often occur at school. If the solution to chronic absenteeism is that every student must attend every day, we must find ways to ensure that children can access the supports and resources they need at school, minimizing the need for them to miss school. Achieving the goal of “every student, every day” requires a more holistic approach.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.