
Abstract
Research on psychological resilience in the workplace is on the rise, aiming to better understand how to successfully manage adverse events. Although scholars have started to explore the concept of team resilience, the focus of the theory on team resilience has been largely on cognitive mechanisms. However, neglecting the role of relational mechanisms discounts the collaboration and social interaction that are necessary for successful teamwork, especially in the face of adverse events. To address this research gap, we conducted a qualitative study with a palliative care team that experienced work-related adverse events. Based on our data and applying conservation of resources theory, we develop a process model of team resilience. This model specifies the experience of adverse events as loss events and illustrates how teams can counteract these losses and enact team resilience through the relational process of caring. Caring in teams can be enacted through four dimensions, which we refer to as understanding, being with, doing for, and enabling. By enacting these caring dimensions, teams can heal social safety and collective action capabilities and can moreover build valuable resources, which may buffer resource loss and fuel resource growth in subsequent team resilience episodes. Our findings provide a better understanding of the role of relational processes in team resilience enactment and specify caring as a core relational mechanism that enables team resilient outcomes. Overall, we provide a nuanced understanding of the different elements within a team resilience process.
Keywords
Many organizations and their employees struggle with responding to adverse events, as these events are often complex and handling them requires collaboration across disciplinary boundaries (Smith, Rondi, De Massis, & Nordqvist, 2024; Williams, Gruber, Sutcliffe, Shepherd, & Zhao, 2017). Accordingly, research on the concept of psychological resilience is on the rise, as it addresses the question of how to successfully manage adversity (Hartmann, Weiss, Newman, & Hoegl, 2020b; Luthans & Youssef, 2007; Raetze, Duchek, Maynard, & Wohlgemuth, 2022).
Work in contexts that entail substantial adversity and therefore make resilience particularly relevant is predominantly organized in teams, as teams are well suited to address complex and challenging problems (Maloney, Bresman, Zellmer-Bruhn, & Beaver, 2016; Mathieu, Maynard, Rapp, & Gilson, 2008). For example, healthcare, firefighting, or emergency response teams often face adverse events (Maynard, Kennedy, & Resick, 2018), as do teams in less dangerous but still failure-prone work environments, such as start-up teams (Preller, Breugst, Patzelt, & Dibbern, 2023) or innovation project teams (Todt, Weiss, & Hoegl, 2018). Thus, it is important to understand how teams can collectively develop resilience—that is, team resilience.
Scholars have highlighted that theory on team resilience has focused primarily on operational tensions and cognitive resources (Barton & Kahn, 2019). However, successful teamwork relies heavily on relational processes, such as mutual support or affect management (Driskell, Salas, & Driskell, 2018a; Hoegl & Gemuenden, 2001). Especially in the face of adverse events, relational processes are of high importance because the experience of adverse events may create negative emotions and anxiety (Maitlis, 2020), which may harm collaboration and support, thus limiting the potential to successfully deal with adverse events (Barton & Kahn, 2019; Driskell, Salas, & Driskell, 2018b). This argument is consistent with conservation of resources (COR) theory, which highlights relational processes as key resources that may explain resilient functioning in organizations in the face of adverse events (Hobfoll, Freedy, Lane, & Geller, 1990; Hobfoll, Halbesleben, Neveu, & Westman, 2018). In fact, neglecting the role of relational mechanisms discounts the collaboration that is necessary for successful teamwork. Thus, to advance our understanding of the team resilience process, it is important to uncover the relational processes team members engage in to enact team resilience and demonstrate resilient outcomes. In our study, we aim to address this issue by investigating the following research question: How can relational processes enable team resilience enactment in the face of an adverse event?
To investigate this research question, we conducted a qualitative study with a multidisciplinary palliative care team. On the basis of a broad variety of data sources, including site visits, interviews, team members’ written reflections, periodic short surveys, and documentary data, we investigated how the team drew on relational processes to manage two adverse events the team experienced. In our analysis, we uncovered caring as a central relational process enabling team resilience. Building on our findings and integrating tenets of COR theory, we developed a processual understanding of team resilience that captures the role of caring for the enactment of team resilience in the face of adverse events.
Our study contributes to research on team resilience in two major ways. First, we uncover the relational process of caring as a key mechanism that explains how teams can enact resilience in the face of adverse events. We specify and conceptualize four mechanisms of caring and illuminate how caring as understanding and being with can heal social safety and how caring as doing for and enabling can heal collective action capabilities, which can be harmed through loss experiences triggered by adverse events. Doing so, we contribute to a better understanding of the relational processes that are conducive to teams enacting resilience. This contribution is important, as teamwork is likely to suffer from the loss of safe spaces in the face of adverse events, and cognitive mechanisms might not be functional enough to restore these safe spaces. By elucidating the role of caring in the team resilience process, we connect the discourse on team resilience (e.g., Hartmann, Weiss, Hoegl, & Carmeli, 2021; Hartwig, Clarke, Johnson, & Willis, 2020; Stoverink, Kirkman, Mistry, & Rosen, 2020) with the discourse on care in organizations (e.g., Arnold & Ross, 2023; George, 2014; Tsui, 2013). Furthermore, we address scholarly calls to enhance our understanding of how to practice care in organizations (Antoni & Beer, 2024).
Second, we develop theory on team resilience as a dynamic process and elucidate the interplay of the experience of adverse events and mechanisms of positive adjustment, as called for by prior research (Caza, Barton, Christianson, & Sutcliffe, 2020; Chapman et al., 2020; Gucciardi et al., 2018; Hartmann et al., 2020b; Raetze et al., 2022). In this regard, and building on COR theory (Hobfoll, 1989; Hobfoll et al., 2018), we illustrate how the experience of adverse events can be understood as loss events, which explains how the experience of adverse events becomes meaningful and impactful for teams and teamwork. We illuminate how caring can counteract losses of safe social spaces and safe spaces for action and, thus, enables the enactment of team resilience fueling team resilient outcomes. Acknowledging intertemporal effects, we further theorize how the outcome of one resilience episode influences the subsequent resilience episode when the team experiences another adversity. In sum, our process perspective allows for (1) understanding how adverse events affect team functioning, (2) how teams enact team resilience through relational mechanisms in the face of adverse events, (3) how teams subsequently produce resilient responses, and (4) how such resilience episodes feed into the handling of subsequent adverse events. This fine-grained processual understanding of the team resilience process complements and extends prior work on team resilience as a capacity (e.g., Brykman & King, 2021; Carmeli, Friedman, & Tishler, 2013; Stoverink et al., 2020) and enriches the nascent conversation on the team resilience process (Preller et al., 2023).
Theoretical Background
Psychological Resilience in Organizations
Psychological resilience is a core concept of positive organizational behavior (Luthans & Youssef, 2007) and is defined as positive adjustment amid adversity (Sutcliffe & Vogus, 2003). Psychological resilience encompasses two defining elements: first, the experience of adversity, understood as “an unfortunate event or circumstance or the state of serious and continued difficulty” (Tian & Fan, 2014: 252), and second, adjustment to or beyond a steady state of well-being or performance (King, Newman, & Luthans, 2016; Kossek & Perrigino, 2016). Research on psychological resilience in organizations has investigated the concept as a stable trait, a developable capacity, an outcome, or a process (Hartmann et al., 2020b). On the basis of their integrative review, Raetze et al. (2022) concluded that scholars have only recently started to understand resilience as a process. Thus, in this study, we take a process perspective on resilience. Building on Fisher, LeNoble, and Vanhove (2023: 1047), we define the resilience process as an “iterative process activated by the experience of adversity, in which existing resources (i.e., capacity) are mobilized via response strategies (i.e., enactment) that result in positive adaptation (i.e., demonstration).”
Adversity—that is, the experience of adverse events—refers to highly challenging experiences that threaten an entity’s identity, well-being, and performance (Hoegl & Hartmann, 2021). The enactment of resilience encompasses the mechanisms used to handle adverse events (Fisher, Ragsdale, & Fisher, 2019). During the enactment of resilience, actors may draw on preexisting resources—for example, the capacity for resilience—or may build and restore them (Williams et al., 2017). Ultimately, positive outcomes, such as recovery in performance, mark the demonstration of resilience as an outcome (Gucciardi et al., 2018). The outcome of this process episode may impact subsequent process episodes of resilience when a subsequent adverse event is experienced and a new resilience episode starts, leading to interepisode effects (Hartmann, Weiss, & Hoegl, 2020a; Moenkemeyer, Hoegl, & Weiss, 2012; Sutcliffe & Vogus, 2003).
Team Resilience
While research on employees’ individual psychological resilience has flourished over the past decades, “research on team resilience is still in its infancy” (Chapman et al., 2020: 61). According to recent literature reviews, there is limited empirical research on team resilience (Chapman et al., 2020; Hartmann et al., 2020b; Hartwig et al., 2020; Raetze, Duchek, Maynard, & Kirkman, 2021; Raetze et al., 2022), but attention to this construct has increased in recent years (e.g., Adler, Bliese, Barsade, & Sowden, 2022; Dierdorff & Fisher, 2022; Li & Tangirala, 2022). While psychological team resilience shares conceptual similarities with psychological resilience at the individual level of analysis, team resilience is different, particularly because of high task interdependence, which requires the coordination and collaboration of team members to allow team functioning at the collective level (Stoverink et al., 2020).
Teams are defined as “collectives who exist to perform organizationally relevant tasks, share one or more common goals, interact socially, exhibit task interdependencies, maintain and manage boundaries, and are embedded in an organizational context that sets boundaries, constrains the team, and influences exchanges with other units in the broader entity” (Mathieu et al., 2008: 411). Stoverink et al.’s (2020) pioneering theoretical work on team resilience capacity underlined the role of cognitive aspects, such as information sharing and processing, in developing team resilience. In line with this, empirical research has shown that cognition-focused states are positively related to team resilience capacity (Brykman & King, 2021; Vera, Rodriguez-Sanchez, & Salanova, 2017). For example, team bricolage was positively related to team resilience capacity in cases of high task interdependence (Talat & Riaz, 2020). Similarly, access to knowledge and experiential learning (Carmeli, Levi, & Peccei, 2021) as well as voice climate (Brykman & King, 2021) were positively related to team resilience capacity. Specifically, Li and Tangirala (2022) revealed that prohibitive voice hindered performance loss via error management during disruption stages, while promotive voice fostered positive outcomes via process innovation in recovery stages. However, research examining different pathways to team resilience capacity suggests that beyond cognitive processes, relational processes might play a crucial role in building team resilience capacity (Hartmann et al., 2021). To theorize about the role of these relational processes in the team resilience process, we draw on COR theory (Hobfoll, 1989) and the literature on caring in organizations (e.g., Arnold & Ross, 2023; Lawrence & Maitlis, 2012).
Conservation of Resources (COR) Theory
A prominent theory that has been applied in research on psychological resilience in the workplace (see Hartmann et al., 2020b) and on how to address adverse events (see Gregg, Restubog, Dasborough, Xu, Deen, & He, 2022) is COR theory (Hobfoll, 1989). COR theory provides a theoretical foundation for “the processes most relevant to stress and adaptational responding” (Hobfoll, 2001: 358) as well as for “resource gain and loss processes” (Hobfoll et al., 2018: 114) and discusses how to establish resilience in the workplace (Hobfoll et al., 2018). It posits that entities make use of resources to cope with stressful situations and strive to build resource reservoirs for times of future needs (Hobfoll, 2001). Although COR theory has mostly been used in research on individuals, it may also be applied to the study of teams (Fisher et al., 2023; Hobfoll et al., 2018; Stoverink et al., 2020), as crossover processes can explain how affective states and resources can be transmitted and become shared in teams (Westman, 2001).
COR theory underscores that adverse events may jeopardize entities’ reservoirs of resources and, thus, their functioning (Hobfoll et al., 2018). However, according to Corollary 1 of COR theory, entities “with greater resources are less vulnerable to resource loss and more capable of orchestrating resource gain” (Hobfoll, 2012: 229). Specifically, COR theory highlights the integral role of interpersonal relations for resilience (Hobfoll, 2011b), as interpersonal relations provide a multitude of different resources that are conducive to building resilience (Hobfoll, 2001; see page 342, Table 1). Specifically, nurturing and caring relationships have been highlighted as key promoters of well-being and resilience (Hobfoll, 2001, 2002, 2011b; Hobfoll et al., 1990) and are conducive to developing resilience in teams (Hobfoll et al., 2018).
List of Interviews
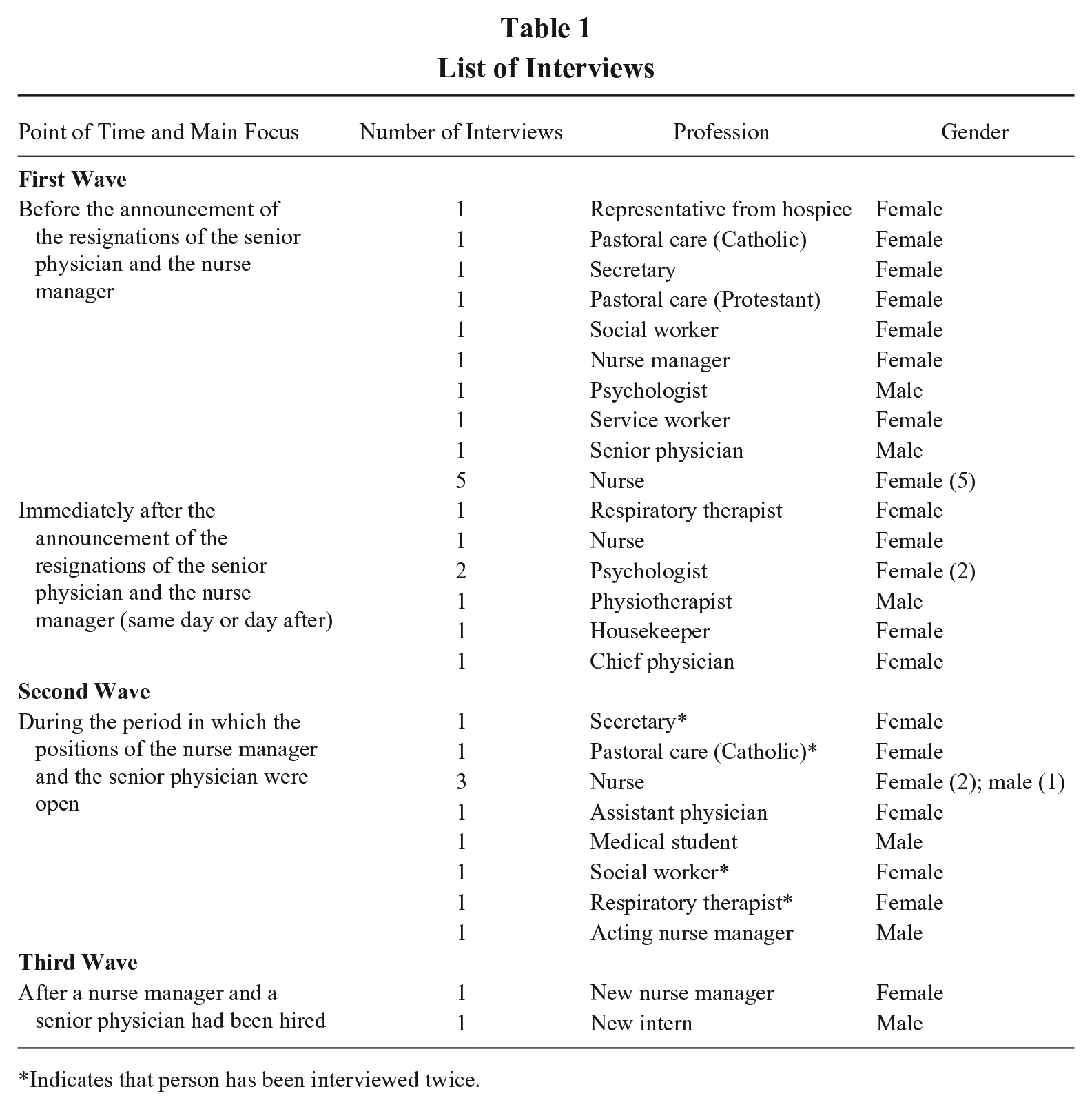
Indicates that person has been interviewed twice.
The Role of Caring
According to Carmeli, Jones, and Binyamin (2016), the essence and main building block of a positive human relationship is captured in the concept of caring. Caring “is a particular form of interrelating between people” (Carmeli et al., 2016: 49) and encompasses both the feeling of concern for others and acting upon this concern (Saks, 2021; Tronto, 1998). Gilligan (1993: 62) suggested that “the ideal of care is thus an activity of relationship, of seeing and responding to need, taking care of the world by sustaining the web of connection so that no one is left alone.” Caring has been argued to be central to human flourishing (Tsui, 2013) and at the core of collective functioning (Held, 2015). It involves caring about another person and becoming aware of their needs, as well as providing care by actually performing specific actions. As caring is a form of interrelating, it involves receiving care and responding to care (Tronto, 1998). Thus, when caring for one another, people have a genuine interest in one another, show empathy, and act in the interest of enabling others to thrive (Carmeli et al., 2016; Kahn, 1993). Moreover, people not only need to be accessible to others and enable perspective but also need to be open to receiving care from others (Kahn, 2001). Through this mutuality in the relationship, a social bond is formed, which makes caring not only important for caregiver–client relationships, as discussed by prior research (e.g., Kahn, 1993; Swanson, 1991), but also underscores the importance of caring as a relational connection in team environments (Carmeli et al., 2016).
In a team context, caring includes “how a team cares for itself as a team, as well as how the team cares for its individual members” (Lawrence & Maitlis, 2012: 656). To engage in caring, team members must understand each other as relational and interdependent (Arnold & Ross, 2023; Held, 2005). When caring for one another, team members can build a space with a sense of meaning, belongingness, and safety, which have been described as essential for a holding team environment (Kahn, 2001). Overall, Tronto (1998: 16) argued that “caring is greatly undervalued in our culture,” which is unfortunate given the potential positive effects of caring for various actors (Arnold & Ross, 2023). Thus, Tsui (2013) underscored the importance of a better understanding of care for organizational scholarship. Hence, to address recent calls to better understand the underlying relational processes that fuel team resilience in the face of adversity (Barton & Kahn, 2019; Caza et al., 2020), we connect to the relatively recent discourse on care in organizations (Arnold & Ross, 2023; Lawrence & Maitlis, 2012; Tsui, 2013).
Method
We selected a qualitative approach for our study, given the nascent stage of research on team resilience processes and given that qualitative methods have been recommended for studying how teams can successfully manage adversity over time (Edmondson & McManus, 2007; Gregg et al., 2022). Specifically, recent literature reviews on resilience have recommended leveraging the opportunities of qualitative research for creating a better understanding of how adverse events unfold and how actors can enact resilience and successfully deal with adversity (Hartmann et al., 2020b; Raetze et al., 2021, 2022).
Research Context and Sample
In this study, we accompanied a palliative care team over the course of two years. According to the World Health Organization (2020), palliative care “is an approach that improves the quality of life of patients (adults and children) and their families who are facing problems associated with life-threatening illness. It prevents and relieves suffering through the early identification, correct assessment and treatment of pain and other problems, whether physical, psychosocial or spiritual.” The palliative care team we accompanied was organized as a ward of a municipally owned hospital in Germany. We gained access to the research site via the hospital’s ethics committee, which supported our research endeavor and established contact with the chief physician of the ward for palliative care. The ward for palliative care was interested in collaborating with us, as the team was then experiencing an adverse event. The ward could hold up to eleven patients simultaneously, which is a common capacity, as the focus of palliative care is intensive care. Each year, the ward cared for approximately 300 patients, who stayed there for ten days on average. While 60% of the patients stabilized and could then move home again or to hospice, 40% of the patients died on the ward.
The investigated palliative care team was a highly suitable subject for studying team resilience for three reasons. First, during our study, the focal team experienced two adverse events: Several relatives of the palliative team had severe medical issues and were treated as patients and subsequently died on the ward. Following this event, the senior physician and the nurse manager, two central figures on the team, announced that they were resigning and leaving the ward. Although palliative care teams generally face high work demands as they must handle suffering and death daily, these two events were experienced as adverse, as indicated by the chief physician and the whole team. Thus, this case allowed us to study how the team coped with these adverse events. Second, palliative care teams are a revelatory subject for the study of team phenomena, as palliative work is explicitly based on a team approach (Hanks, Cherny, Christakis, Fallon, Kassa, & Portenoy, 2010). Palliative care aims to take care of various needs of patients and their relatives, and to achieve this goal, different competencies are needed (Goldsmith, Wittenberg-Lyles, Rodriguez, & Sanchez-Reilly, 2010). Therefore, palliative care relies on multiprofessional teams (Simon & Higginson, 2009). Third, palliative care teams experience unique and extreme work demands since they work with terminally ill patients (Cooper & Mitchell, 1990). Surprisingly, several studies have shown that despite these work demands, the stress levels of palliative care workers are generally below those of workers from other professions (Vachon, 1995). It seems that, because of these specific work situations, palliative care teams are well trained and equipped to develop successful coping responses, which might serve as a foundation to develop resilience against adverse events. Thus, although the course of events was unknown to us at the beginning of the study, we were confident that relevant insights into how teams deal with adverse events at work could be revealed by accompanying the palliative care team.
The Palliative Care Team
At the beginning of the study, the palliative care team we investigated consisted of 34 employees from 11 different professions: 2 physicians, 16 nurses, 2 physiotherapists, 1 music therapist, 1 respiratory therapist, 3 pastoral care employees (Catholic and Protestant), 1 secretary, 3 service employees, 1 housekeeper, 1 social worker, and 3 psychologists. The two physicians, the nurses, the secretary, the housekeeper, the social worker, and the service employees worked only in palliative care, whereas the other employees assumed additional responsibilities in the hospital or worked as freelancers.
Working Procedures
The work on the ward was structured as follows: Between 9 and 10 a.m., team members held a joint breakfast. On weekdays, at 10 a.m., both the doctors and the nurses in charge (and on Thursday, one of the psychologists) conducted a ward round during which they visited every patient and discussed the patient’s status. In the evening, the team members held a short dinner. Every Thursday, the team had a large team meeting that followed a predefined structure. First, for every patient who had died during the week, candles were lit, and the team observed a minute of silence. Next, the team discussed each patient for a few minutes. Moreover, clinical supervision guided by an external counselor was conducted approximately every two months, during which team members could address the emotions, relevant issues, or experiences that had been stressful or extraordinarily memorable for them. In addition to these “large” team meetings, every subteam held meetings at varying intervals. The nurses, for example, exchanged information twice a day between working shifts, whereas the therapeutic team, including the therapists, psychologists, and pastoral care subteam, met approximately every three months to exchange information and discuss new approaches.
Data Collection
Our data collection started while the first adverse event unfolded. We conducted site visits and interviews and collected team members’ written reflections, short self-report surveys, and documentary data over two years. An overview of our data collection efforts in the context of the unfolding events is provided in Figure 1. Our site visits and interviews were centered on the two adverse events. We established regular contact with the chief physician during the first adverse event. Site visits and structured interviews commenced while the team recovered from this adverse event. We also visited the team and conducted interviews when the second adverse event started, which was with the announcement of the resignation of two key team members. We collected additional data while the team recovered from this adverse event. At the end of this second wave of site visits and interviews, no new narratives emerged. To validate our findings, we collected additional written reflections and short surveys in the following weeks. Half a year after the second adverse event, we conducted a third period of intense and frequent site visits and interviews to explore longer-term effects and probe our analysis. After thirteen months of data collection, two of the authors discussed and reflected on the preliminary research results with the palliative care team in a group discussion. Overall, our data combines retrospective and real-time accounts. All the data were collected before the COVID-19 pandemic. Thus, the COVID-19 pandemic did not influence our research.
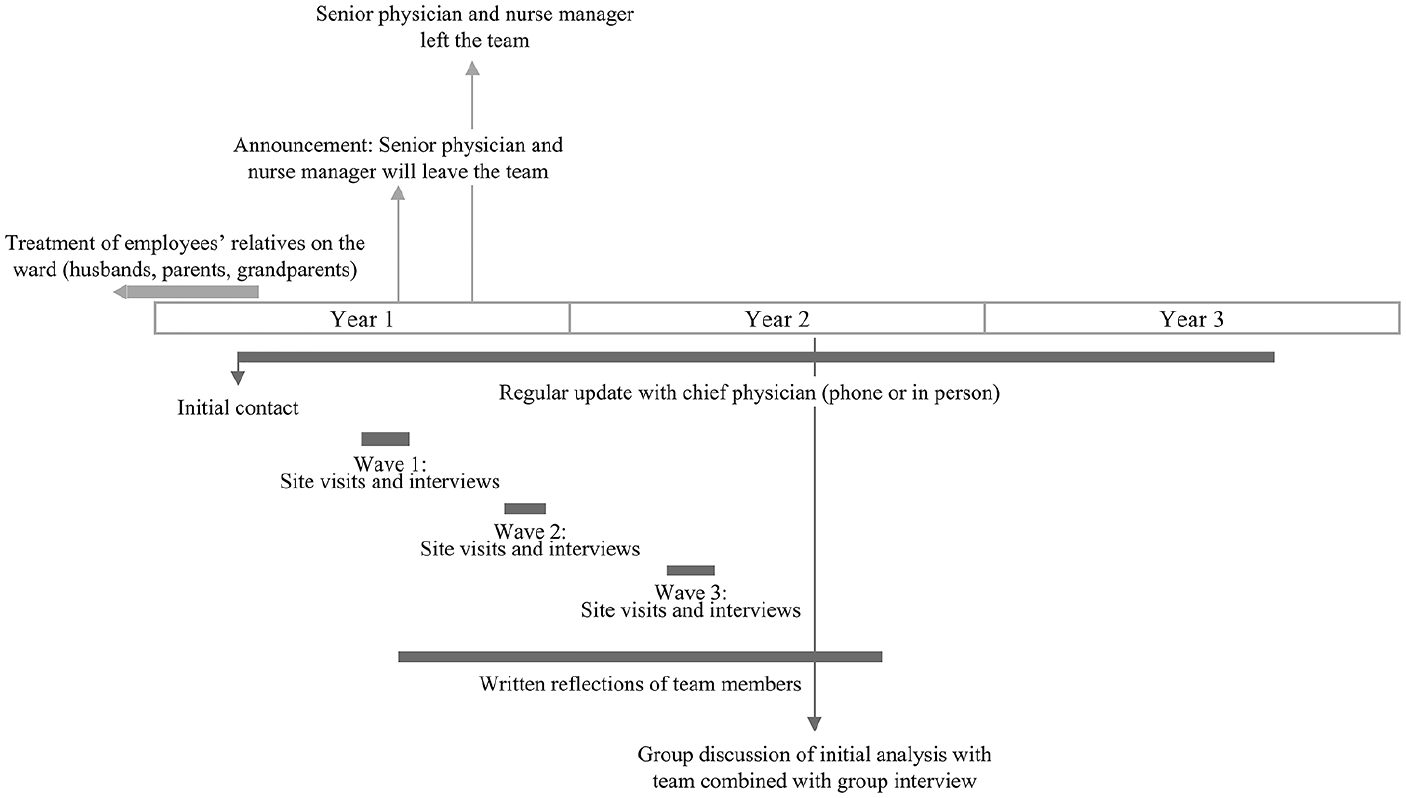
Timeline
Site Visits
The first author conducted multiple site visits to grasp the everyday working reality of the palliative care team. In sum, the first author spent fourteen days in the palliative care ward, which corresponds to more than 140 hours of observations. During these site visits, the author dressed like the physicians and the nurses—that is, in a green lab coat. The author observed the work of the different professionals and the collaboration among the team members and talked to the employees, patients, and relatives. The site visits were conducted en bloc in different phases of the adverse events. During and after each site visit, the first author took extensive field notes.
Narrative Interviews
As soon as she had built rapport with team members, the first author began conducting 33 in-depth narrative interviews with 29 team members from all eleven professions and with an assistant physician and an intern who had an outsider perspective on the team. The interviews were conducted in German. Table 1 provides an overview of the interviews that were conducted. The interviews lasted between 15 and 80 minutes and were 28 minutes on average. Owing to the firm integration in the field setting and the solid background information, we could focus on key events during the interviews. We used a semi-structured interview guide following the critical incident technique (Flanagan, 1954) and focused on how the team dealt with the two adverse events. As the study developed, the interview guide was slightly adapted to address the current events. Of the 33 interviews, 30 were recorded and transcribed; two team members (one of whom was interviewed twice) asked not to be recorded. In these cases, the interviewer took extensive notes during and after the interviews. Whenever team members were interviewed twice, the second interview was shorter than the first interview.
Written Reflections
We asked the team members to provide anonymous written reflections beginning on the day of the senior physician’s and nurse manager’s resignation announcement. Throughout the study, team members had the opportunity to complete a written reflection whenever they wanted to share their experiences. We asked the team members to reflect on the work week, describe a situation that was salient in their minds, and explain why it was salient. In addition, the team members were asked to complete a short survey and assess their personal emotional state based on Lang’s (1980) Self-Assessment Manikin (SAM). We initially measured the team members’ emotional states following the termination announcement, collected self-assessments during the following month, and then again roughly four months later. In total, we collected 37 handwritten reflections.
Short Surveys
At three time points—that is, directly after the announcement that two key team members were leaving the team and four and seven months later—the team members were asked to evaluate the team’s participative safety (Anderson & West, 1994) and to assess their personal resilience and the team’s resilience based on the Connor-Davidson Resilience Scale (Campbell-Sills & Stein, 2007) using a 5-point Likert scale.
Documentary Data
We collected articles about the examined palliative care team published in local newspapers and included an introductory movie about this team, which was publicly available on the hospital’s website, in our analysis. In addition, we searched the hospital’s webpage to enrich our understanding of the organization. Moreover, to gain a sound understanding of the research context, we collected information about palliative care, about the palliative care market, and about the treatment of cancer. These additional data sources were primarily used to triangulate our analysis and improve our understanding of the research context, while this information was not used as a key source to develop our theoretical model.
Qualitative Analysis
We relied on abductive forms of analysis (Timmermans & Tavory, 2012) and aimed to construct a theory on team resilience. We were guided by the methodology outlined by Gioia, Corley, and Hamilton (2013). As such, at the beginning of the analytic process, we tried to be ignorant of the literature but relied on the raw data for analysis. After a first analysis of the data through memos and in-vivo coding, we started to cycle “between emergent data, themes, concepts, and dimensions and the relevant literature” (Gioia et al., 2013: 21). As such, our “research process might be viewed as transitioning from ‘inductive’ to a form of ‘abductive’ research, in that data and existing theory [were then] considered in tandem (Alvesson & Kärreman, 2007)” (Gioia et al., 2013: 21).
We started our analysis process during the data collection to guide our data collection efforts. We wrote memos to capture our impressions and created narratives based on our field notes. Throughout the process of our study, we kept returning and updating our memos to record our evolving ideas and produce different versions of our theoretical model. Given the sensitive setting of our study context, we interacted with our study objects with respect and a sense of responsibility.
To follow a rigorous qualitative research process, we implemented an insider and outsider approach (Strike & Rerup, 2016). The first author, who had experience with palliative care and similar forms of treatment and who had emerged in the field, acted as an insider, and the second author acted as an outsider who was never present at the data collection site. The insider gave updates on the data collection and discussed the initial findings with the outsider. The outsider offered inspiration for additional questions to explore during the data collection. Moreover, the outsider acted as a devil’s advocate who “relentlessly pushed for clarification and elaboration, asked critical questions, and identified themes that the first author either agreed with or found additional support for in the data” (Strike & Rerup, 2016: 888). The third author built a bridge between the insider and the outsider, as the third author visited the site during the data collection but was less involved in the data collection process. All the authors were involved in developing the process model and iteratively discussed the model while it was emerging.
Data Coding
We were guided by recommendations for coding data by Saldana (2013) and Locke, Feldman, and Golden-Biddle (2022). On the basis of our pre-analysis, we concluded that our data were suited for elucidating the team resilience process. We progressed our analysis by coding our field notes from our site visits. We focused on how the team made sense of adverse events, how they dealt with these events, and how they demonstrated resilience. Our initial analysis revealed that caring was integral to how the team interacted and related. Thus, in the process of coding and analyzing all our data, we aimed to refine the role of caring in the team resilience process.
We consulted the literature on COR theory (Hobfoll, 2001; Hobfoll et al., 2018), the literature on (team) resilience processes (e.g., Fisher et al., 2023; Moenkemeyer et al., 2012; Sutcliffe & Vogus, 2003), and the literature on care in organizations (e.g., Arnold & Ross, 2023) to structure our coding steps. We decided to focus on the different elements of the resilience process (i.e., the experience of adverse events, enactment of resilience, resilient outcomes—that is, demonstration of resilience—and interepisode effects; Fisher et al., 2023; Hartmann et al., 2020a). Our data structure is provided in Figure 2.
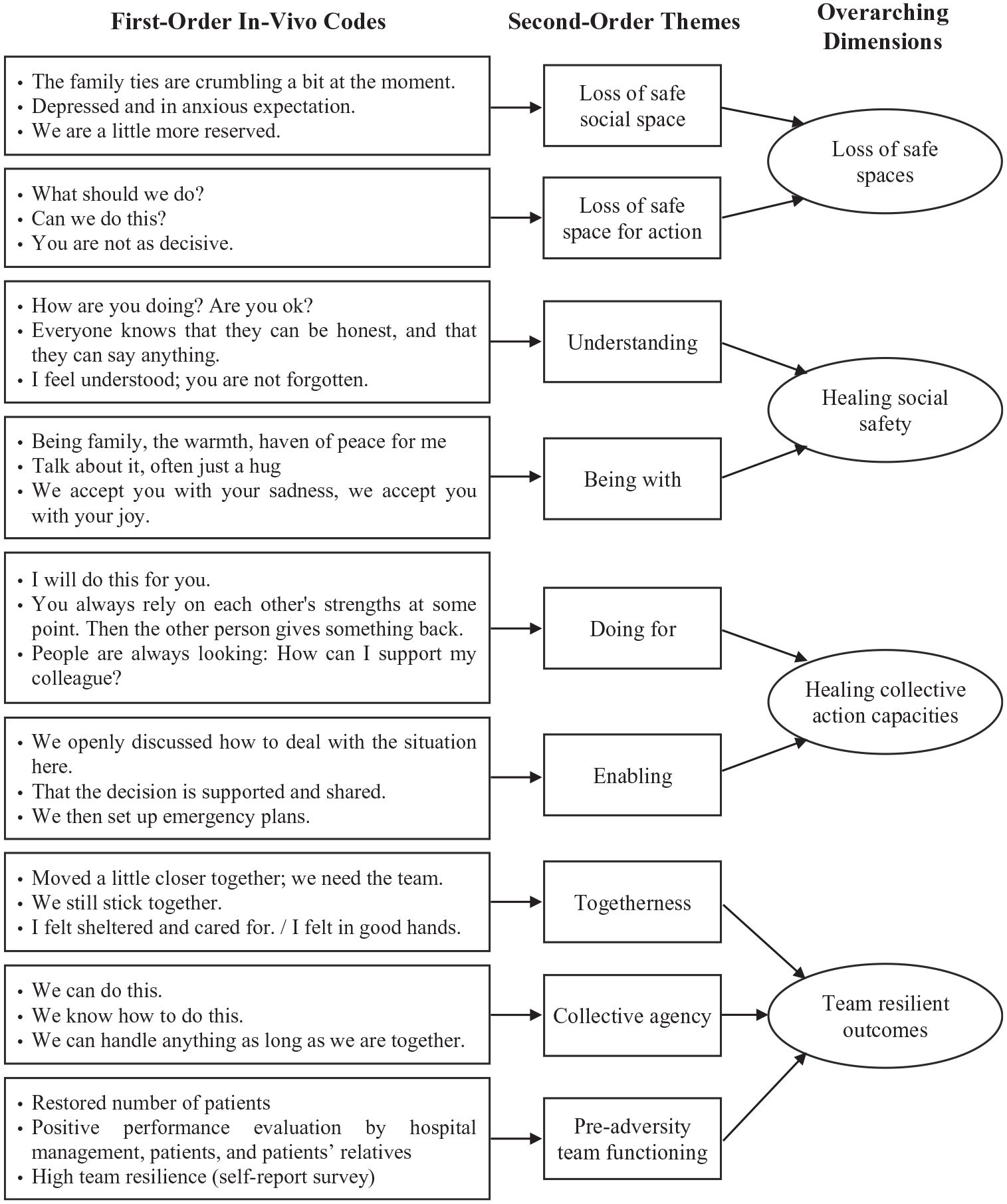
Data Structure
First, we started to code the field notes and interviews, focusing on how the team made sense of the adverse events. Our in vivo coding revealed that the adverse events triggered collective perceptions of loss, which were partly team-related and partly action-related. To organize these codes and arrive at patterns, we connected our findings with insights from COR theory to form two different second-order themes related to the overarching concept of loss.
Second, we applied in vivo coding to analyze how the team coped with these adverse events and enacted resilience. It became obvious that relational processes were key to coping with the adverse events. Upon closer examination, we identified caring as a key mechanism of team resilience enactment. To structure our in vivo coding, we consulted the literature on care in organizations. Swanson (1991) provides a categorization of caring interactions in caregiver–patient relationships, which we used as inspiration but refined further to organize our in vivo codes. By combining patterns (Locke et al., 2022), we analyzed how the team engaged in care. Moreover, we analyzed the effects of these mechanisms, which led us to focus on team outcomes.
To better understand how the team demonstrated resilience, we returned to the narratives on how team members described their handling of the two adverse events and how they perceived or had perceived their teamwork. Resilience theory argues that judgment is needed regarding which developmental outcome is evaluated as good or positive (Masten, 2001). Although initial organizational resilience theory focuses on performance as the key determinant of resilience, our in vivo coding revealed that the team referred to additional criteria to assess their functioning. It became obvious that only through the development of togetherness and collective agency could the team restore functioning, not only in the short term but also in the longer term, accounting for temporal considerations in team resilience research (Gucciardi et al., 2018).
Finally, considering juxtaposing patterns and building on resilience process theory, COR theory, and the literature on care in organizations, we analyzed how the first resilience episode influenced the second resilience episode. We analyzed how the resilience outcomes fulfilled a buffering and a fueling role, which influenced the unfolding of the second resilience episode. We embedded our analysis in a process model of team resilience.
We probed our emerging theorizing with the data from the written reflections and the short surveys, which provided further confidence in our theorizing. Although the description of our analysis might suggest a linear process, it can be better understood as an iterative form of analysis. Throughout the process, we discussed the analysis and probed and questioned our initial results and the underlying mechanisms that were sought to connect the different categories. Because of this iterative process, our theoretical model was constantly revised and refined (Gioia et al., 2013; Locke et al., 2022). Finally, as suggested by Gioia et al. (2013), we derived propositions based on our process model of resilience.
Findings
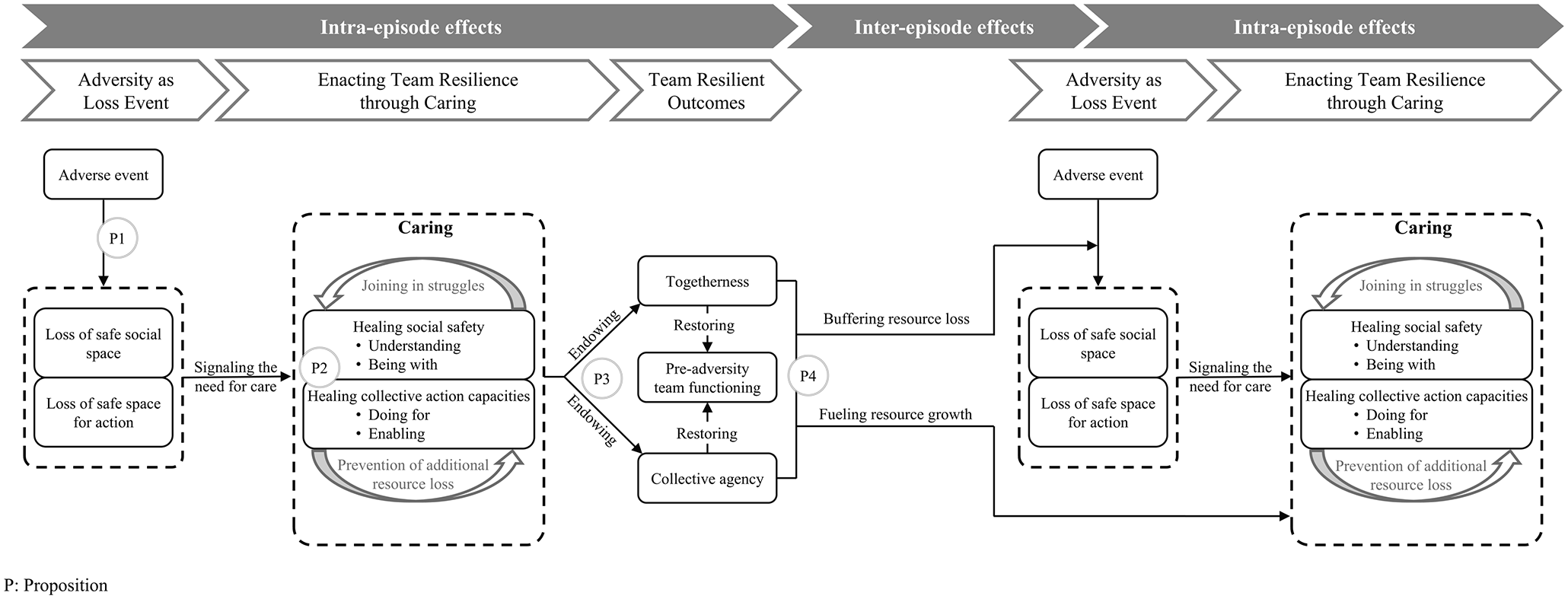
In this section, we present our findings and illustrate them with exemplary data. To specify the origins of the data, we replicate verbatim quotes, as spoken by the team members in the field, in quotation marks. We label the interview quotes as “Int.” and the quotes from written reflections as “Ref.” The data that originated from our observations during site visits are labeled as “Obs.” On the basis of our analysis, we developed a conceptual model of the team resilience process and the role of caring in this process. The model illustrates the team resilience process and pinpoints (1) the experience of adverse events as a loss event, (2) the enactment of team resilience through caring, (3) team resilient outcomes, and (4) interepisode effects that illustrate how one resilience episode influences a subsequent resilience episode. We develop propositions that are positioned within our conceptual model, which is displayed in Figure 3.
Conceptual Framework of the Team Resilience Process
Experience of Adverse Events as Loss Events
The examined palliative care team experienced two adverse events. During the first adverse event, several palliative care team members’ relatives were treated, and some eventually died, on the ward so that “there was constantly somebody [a relative] on the ward.” During that time, “there were just so many deaths,” team members “went from one funeral to the other,” and “it felt like the team had been cursed.” Although the death of a human is a significant event, palliative care teams are experienced in frequently handling death. As such, a week in which none of the patients died was the exception for the team. What made this situation special was that the patients were related to the team members. Thus, the situation “was simply more stressful for everyone” (Int. Psychologist A), as “we were all somehow relatives” (Int. Chief Physician).
Approximately three months after this first adverse event, the senior physician and the nurse manager announced their resignations. They left the ward two months later because they had good opportunities for professional development elsewhere. Their resignations were “all-around catastrophic and devastating news” (Ref.) and critical to the team, which became evident when they announced the change during the Thursday formal team meeting: During the team meeting, first the nurse manager and then the senior physician explain that they will be leaving the team on October 1st. The atmosphere is still and tense. The team members glance at each other: Some are shocked, some look concerned, and some look very miserable. Marie says “That is a shame, that really is bad news”. Helena and Silke begin to quietly cry. Lena asks “Where is the booze”? Dr. Petersen raises her voice “Hopefully we will . . . no . . . we
Team members were “shocked” (Ref.) and emphasized that the senior physician and the nurse manager were “a mainstay on the team” (Ref.) and had “a central role on the team—both functional and personal” (Ref.).
These two events marked the first defining element of a resilience process episode: the experience of an adverse event, which produces high levels of stress and threatens a team’s identity, well-being, and performance (Sutcliffe & Vogus, 2003). According to COR theory, loss events and the loss of resources are the central drivers of experiencing threat and stress (Hobfoll, 1989). During the adverse events, team members indicated that they experienced “heavy losses.” Thus, adverse events were understood as loss events. Specifically, our findings suggest that the team experienced two different forms of loss. We elaborate on these forms of loss with representative quotations in the section below and in Table 2.
Adversity as Loss Experiences
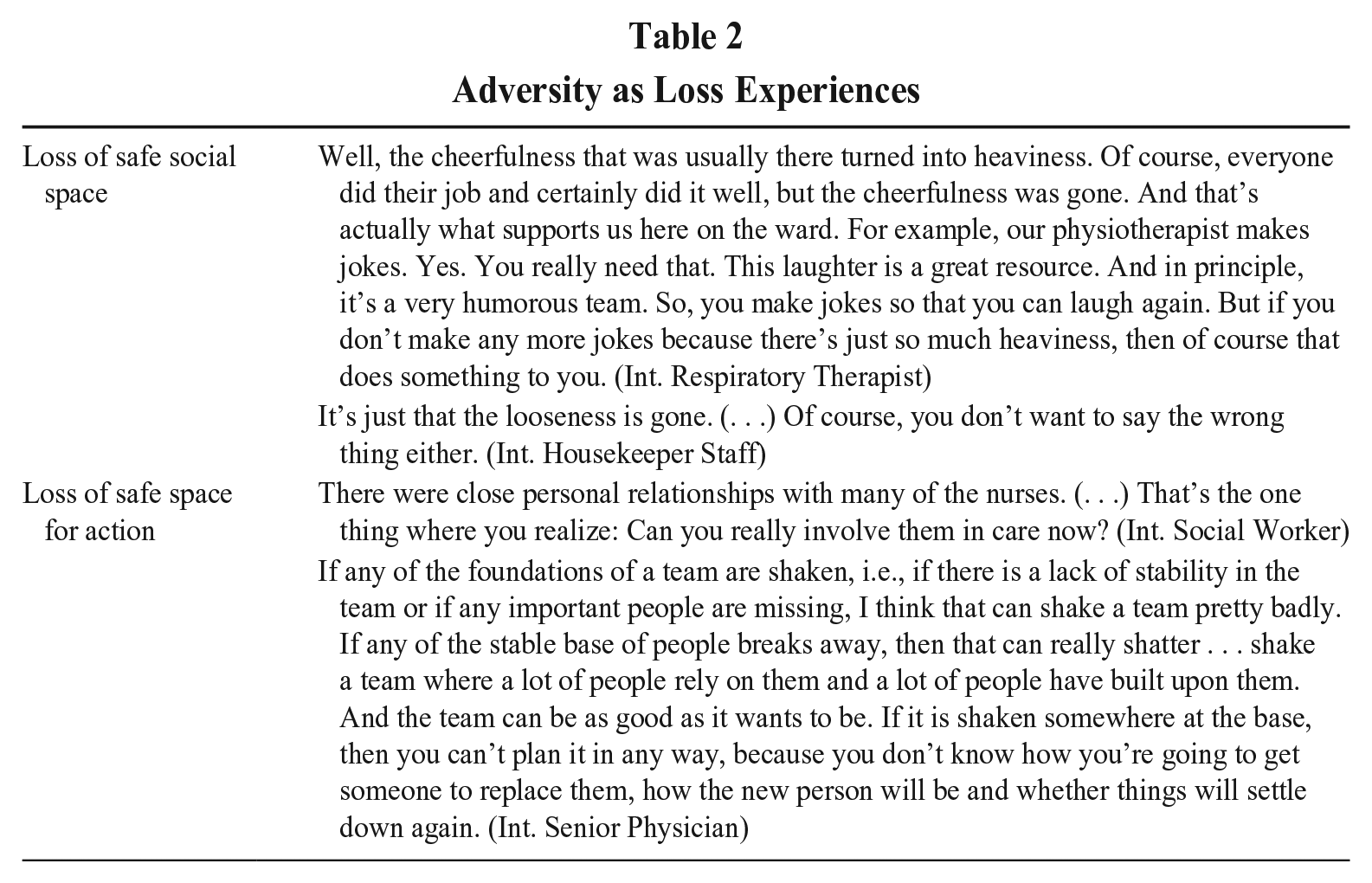
Loss of Safe Social Space
We refer to the first loss experience as the loss of a safe social space. A safe social space refers to a psychological, relational space in which people feel a sense of security and safety and feel safe to interact with each other. During the adverse events, the “stable social fabric developed large cracks” (Ref.) and the team experienced “emptiness,” “sadness,” “anxiety,” and “speechlessness” (Ref.). These social tensions made it difficult for team members to interact with each other, as they felt insecure in their interactions. Thus, team members were more cautious in their interactions, as they did not want to do something wrong. Conversations and interactions between team members changed, as explained by different team members: Yes, you can tell from the meetings that it’s not so easy, I’d say, to approach things. So, it’s never easy; that may sound wrong, but you’re really personally involved in a different way. (Int. Social Worker) You’re a bit more reserved so that you don’t become encroaching in what you say. (Int. Nurse Manager) And I said: “I don’t know what’s going on. When I come into the room, the conversations stop. There’s just so much tension. I want to know what’s going on now.” (Int. Housekeeper)
This loss of a safe social space was problematic and hampered teamwork, as, especially in these difficult situations, “the need for conversations was higher” (Int. Nurse C).
Overall, we observed how the experiences of adverse events disrupted relational patterns. These disruptions hurt the social fabric of the team and, in turn, triggered social isolation, which harmed team cohesion. Ultimately, this threatened the team’s identity and its ability to cope with stress as a unit. We present further quotes on the loss of safe social spaces in Table 2.
Loss of Safe Space for Action
As a second loss dimension, team members also felt a loss of a safe space for action. This label describes the absence of scripts and behavioral guidance, which can guide interdependent collective behavior toward task accomplishment. In the face of the adverse events, the team had to make sense of what was happening, how it was impacting the team, and what should be done to successfully manage the situations toward resilient outcomes. As such, at the beginning of the adverse event, “there [was] a lack of security” (Ref.) such that team members had many open questions, such as “How will we go on?” (Ref.), “How do we behave?”, and “How should we deal with it as a team?” (Ref.). Overall, this action-related insecurity “was a powerful undertow” (Ref.), which affected the whole team. The team did not have any routines on how to cope with such adverse events. Yet, a high need for guidance and direction existed: Normally, they don’t need such clear rules. And I don’t want them either . . . because they should do their job. They do their job well, and if something swims a little in the other direction, then that’s just the way it is. Because I know that they always try to get the best out of the day for the patients and out of the processes. But I’ve already noticed that they need someone who clearly speaks and leads. (Int Nurse Manager)
However, developing the needed guidance and routines to enable task-related action was difficult because, in that situation, team members were “less decisive” than usual. Overall, the loss of a safe space for action triggered rumination about the current problems. Theory suggests that collective rumination impairs resilience, as it questions feelings of control and hampers joint action (Knipfer & Kump, 2022). Moreover, the absence of routines and scripts harmed agency (Kahn & Rouse, 2021), hindering coordination and synergistic work on the task (Bandura, 2001). Based on our analysis, we make our first proposition:
Enacting Team Resilience Through Caring
Together, the loss of a safe social space and the loss of a safe space for action were stressful and threatened the team’s successful coping with adverse events. However, COR theory argues that entities may “employ other resources to offset net loss” (Hobfoll, 1989: 518). In other words, the resource investment principle (Principle 2) in COR theory states that people must invest resources to recover from loss (Hobfoll et al., 2018). Thus, a resilient response must counteract the loss of resources (Hobfoll, 2011b). The literature on organizational healing argues that the experience of adverse events may activate resources that are specific to so-called wound sites (Powley, 2013). In particular, social relations can be used to address situational needs connected to stress (Hobfoll, 1989). Prior research highlights that human distress is a crucial trigger for collective responses characterized by care and concern (Dutton, Worline, Frost, & Lilius, 2006). Consistent with this research, we found that the main mechanism through which the team was endogenously equipped to successfully cope with the adverse events and enact resilience was the collective process of caring.
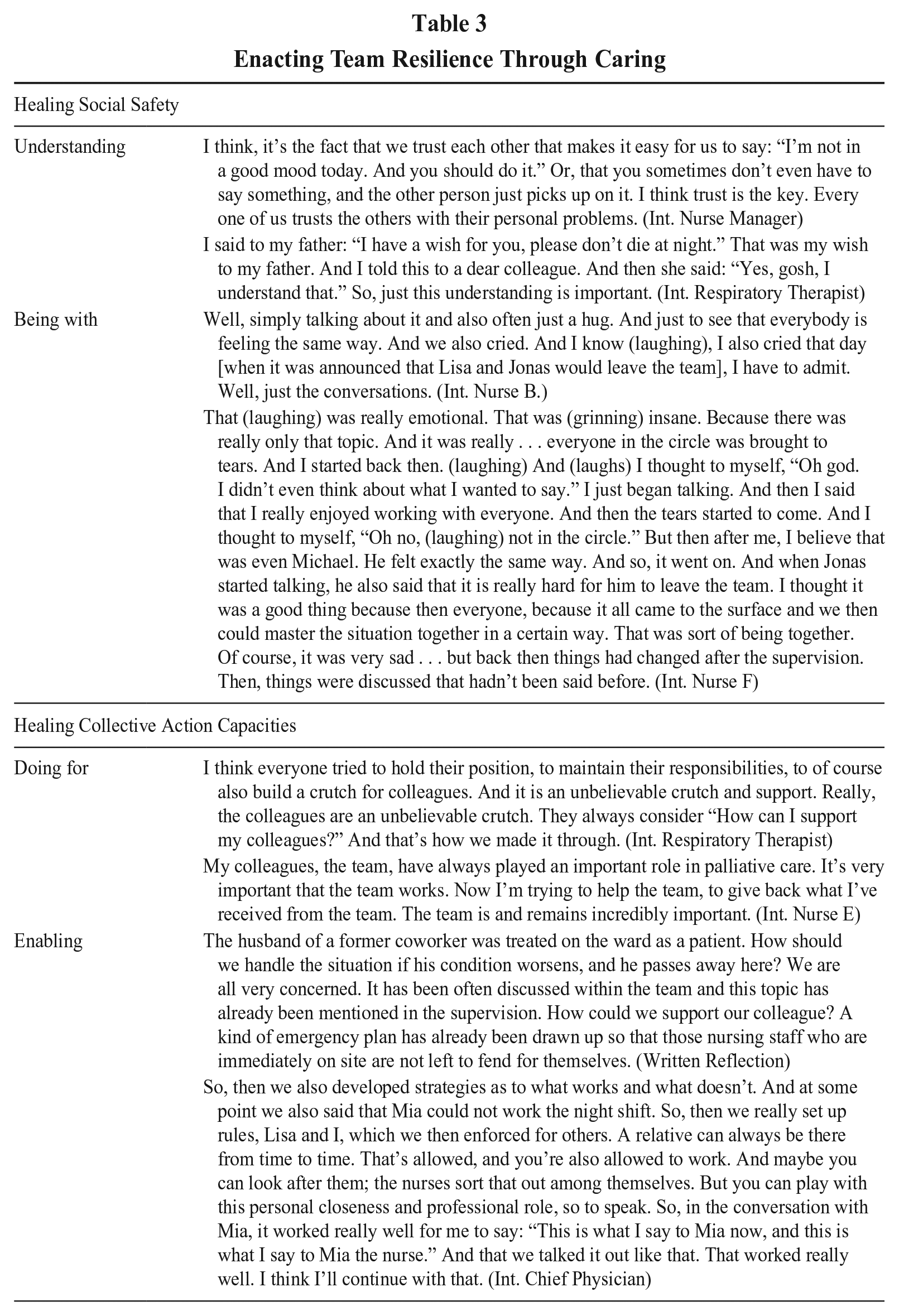
We observed how the team members engaged in caring to handle adverse events. As caring is an other-oriented process, it embraces an understanding of the self as being interdependent with others and as being connected to the social environment (Markus & Kitayama, 1991). Thus, engaging in caring fostered the construction of joint struggles, which were separate from those of individual team members and considered team struggles. Instead of blaming individual team members for causing difficulties, team members developed an attitude of “we are in this together” and framed the adversities as created by the situation, not by the team members. This finding is important because the theory on teams’ experience of adversity suggests that if difficulties are perceived to be triggered endogenously by individual team members, this perception may jeopardize team cohesion and, consequently, team coping (Razinskas, 2021). As such, joining in the struggles enabled the team to face and handle the adverse events by building on the team’s capacities. Consequently, caring allowed the team to heal relationships within the team and the team’s functioning (Olekalns, Caza, & Vogus, 2020; Powley, 2013). We identified mechanisms of caring that were primarily used to heal social safety and mechanisms of caring that were primarily used to heal collective action capacities. We illustrate the different caring mechanisms with representative quotations in the section below and in Table 3.
Enacting Team Resilience Through Caring
Healing the Social Safety
Due to the experience of loss during both adverse events, the team faced cracks in its social fabric, which we labeled as the loss of safe social space. To heal these relational wounds, the team engaged in two separate processes of caring, which we labeled understanding and being with.
Caring as understanding describes the desire of one person to understand the personal reality of the one cared for (Swanson, 1991). This dimension of caring included perspective-taking as well as the feeling of being understood, which was borne by concern for the other. Team members described how they were concerned about each other’s and the team’s well-being. A nurse who lost her husband on the ward explained: [I experienced the team] as very supportive. So, I didn’t see it as imposing something on me, but rather . . . You prefer to give in this profession, or that’s how I feel. So, I’d rather give and step in and do, than take. And in this phase, I actually took a lot. And I was always afraid that I was taking too much from the team. How long can they even put up with me? Am I asking too much of them? That was actually my fear: To what extent can they cope? (Int. Nurse E)
Because of the ongoing feeling of “speechlessness,” these tensions were difficult to resolve. To counteract these problems and address these issues, team members noted that they engaged in seemingly small actions to signal interest in colleagues’ social realities, such as by sincerely asking “How are you?” These caring actions helped create an understanding of the different lived experiences and constituted inclusive acts that reopened social spaces. As soon as these social spaces were reopened, team members described that they felt that they could “speak to everybody” and “about everything”: Because there is a basis of trust. And everyone actually knows that they can be honest and that they can say anything. (Int. Physiotherapist) You notice that everyone trusts each other. So, everyone talks, even when we have our supervision . . . It’s not just about patients or cases, but everyone also talks privately about their private problems. And that really means something when you confide in people privately in such a large group. (Int. Nurse C)
When sharing these personal perspectives, team members highlighted a space of deep understanding. This understanding was described as a major resource for handling adverse events, as “it provides a good feeling, when you are understood” and “everyone succeeds when they are understood” (Int. Secretary).
Complementing understanding as caring to heal the team, the team engaged mechanisms that we labeled as being with. Caring as being with refers to being emotionally present to the other (Swanson, 1991), which reflects a deeply embedded care for each other and includes reciprocal sharing of both positive and negative feelings, such as joy and companionate love or anxiety. Team members described the team as “loving,” “family,” or a “haven of peace.” As such, the team provided a holding environment for team members, in which they felt “sheltered” and “cared for.” This holding environment allowed team members to be together in their negative feelings and share their strains and sadness. As the respiratory therapist explained: This sympathetic way. For example, when my father was there [as a dying patient on the ward], they joked with me like before, you see? It was such honesty. A tender honesty. This is what our team is, I think. And there was an acceptance; you can be as you are. We accept you with your sadness; we accept you with your joy. And we also accept you if you make a silly joke (smiling). (Int. Respiratory Therapist)
Team members also noticed that “what the team does for those affected is received with such gratitude that it has lifted some of the tension” (Int. Pastoral Care), which underscored the role of receiving and responding to this receiving. Moreover, those who were affected opened up, which repaired the social spaces within the team: The remarkable thing is that she simply gave you a hug, on her own initiative. She was actually in a situation where her husband was lying there. And she often . . . just gave us a hug or something. And (takes a deep breath) somehow she just talked to us about other things when she went out of the room. (Int. Service Worker)
This practice of being with each other in the face of adverse events and joining together in sadness allowed the team to reestablish a social space in which all the team members felt connected. This process helped the team cope with the adverse experiences: (exhaling) What helped the team? What we normally never do, but what we did then: We all went to the funeral together as a team . . . Or whoever wanted; it wasn’t a mandatory event, but rather whoever wanted to go. It was important to be there for many of us. [. . .] And we talked about it a lot. Tears were also shed. So, it’s all part of the process. (Int. Senior Physician) And somehow you realized that we weren’t just work colleagues. Well, we are work colleagues, but it’s just very cordial between us. And that you just like the others, and of course you want them to stay. And it was nice to feel that somehow. And I also think that, for me, something changed after the supervision, that this grief was simply lived and that it was talked about. (Int. Nurse F)
Joint processing of strains and negative emotions opened up the space for positive interactions that were future-oriented. To heal the team, its members came up with creative and joyful ideas of being with each other, which provided meaning and conveyed the worth of individual team members to the whole team. In some cases, these joyful ideas of being with had a ritual pattern, which allowed the team members to let go of strain.
What helped me in particular, for example, was that we formed a music band to say goodbye to these three persons; with very different people from the nursing staff, then the social services, music therapy, and me as a respiratory therapist. We formed a music band and we wrote and sang farewell songs together. We released these three persons with these songs, or we let go of them. And that’s what supported me personally the most, to say it again in these songs: “Hey, you were really great as humans, as forces here on the ward, but now we’re releasing you, and that’s okay.” We also did a ritual, which was quite funny. We made them walk on split logs and then said, as a punishment, because they’re leaving, they have to walk on split logs. But we release them and let them go. So, they were practically knighted. And that was the saying: “Take your split log and go!” (Int. Respiratory Therapist)
Overall, the caring processes of understanding and being with can be characterized as active forms of connecting. These connective actions healed the social fabric within the team (Olekalns et al., 2020), helped redistribute individual strains across the team, and opened spaces for feelings of safety and shelter (Kahn, 2001).
Healing Collective Action Capacities
Due to the experiences of loss, the team felt a lack of security concerning how to act and to successfully perform their work. To heal these task-related wounds, the team engaged in processes of caring, which were described as doing for and enabling.
Caring as doing for refers to comforting actions that are intended to help others, to reduce their burden, and to preserve their needs and dignity (Swanson, 1991). Team members explained that it is natural to support colleagues, especially when they are strained: With things as difficult as her situation [a nurse losing her husband], it goes without saying that you’re there for each other and that you help each other out. You don’t really mind because you’re actually happy to do it. Yes. (Int. Nurse B)
During the adverse events, colleagues supported and helped each other with their daily work tasks, and they moreover overtook specific tasks to lighten the burden of their colleagues: During that time, I was supposed to hold a training course about dyspnea for students at the nursing school. But there was my father on his deathbed. And then I told Lisa, and she said, “You stay with your father. I’ll take over the training,” without preparation. “I don’t have to work tomorrow; I’ll take it on for you.” It’s simply the feeling of being looked after. (Int. Respiratory Therapist)
Doing for each other was understood as a mutual process of giving and receiving. It was not only directed to lift the burden of individual team members but also intended to keep the team’s level of performance high by making use of each team member’s strengths and covering for temporary weaknesses. Team members focused on individual and collective well-being to enable successful collective functioning in the long term: You always rely on each other’s strengths at some point. And then, the other person gives something back. And I think you can’t just rely on the strength of the individual, but it really is a team. And you always have to make sure that you don’t exhaust the individual in any way. [. . .] So, you always have to dose it well as a team. That we support each other. Support and strengthen. And in turbulent times, we try to bring out the strengths of the individual again through discussions. Sometimes you have phases when you’re not feeling well. Then, you support that person again, and the person gives back to you in phases when the other person needs it. But you always keep an eye on the team and look at the entirety. (Int, Nurse E)
The consciousness of individual states and the potential strength of teamwork endogenously equipped the team to open up possibilities for actions while accounting for temporary limitations.
As a second mechanism to heal the team’s action capacities, the team engaged in caring practices that we labelled as enabling. As a collective caring process, enabling describes actions to facilitate the team’s transition and its capabilities to adapt and grow. It involves the sharing of perspectives and information, the validation of different perspectives, and discussing ways of looking at or acting on a situation (Swanson, 1991). Enabling was developing the competence to engage in effective actions to handle adverse events. These actions had the goal of achieving the collective capacity to act, as the team “needs to be capable of acting” (Int. Chief Physician).
During the adverse events, the team lacked routines and well-established best practices. Thus, it was discussed whether and how the team could handle the situation: I think we got off to a good start right from the beginning. We thought about it very, very early on, when we found out that our colleague’s husband was ill, that we knew what could happen and asked ourselves the question: Can we, as a team, make it possible for him to pass away here? (Int. Nurse Manager)
When discussing different options, it was “important to hear from all team members” and to “value the different perspectives.” As caring is a “value-expressive attitude that confirms the worth or importance of the persons who are the objects of care” (Arnold & Ross, 2023: 622), this type of information and perspective sharing can be considered a caring act. As such, everybody was involved in discussing perspectives and options for acting: I think this open communication is very important here. It doesn’t matter what the problem is; it only matters that you simply talk openly about how you’re feeling or how you experience it. And that you simply talk openly and try to find a solution. (Int. Social Worker) I think we deal with it quite openly. It works. We then said, “This is how it has to be. We have these boundaries now. And we won’t go beyond them.” (Int. Secretary)
The team’s capabilities to act were the highest priority, as “it always matters that it is feasible” (Int. Housekeeper). Thus, caring as enabling also served the function of creating guidelines for actions, helping to recreate feelings of security in acting: That happened a year and a half earlier, so we were already asking ourselves the question. He arrived once in a very poor condition but stabilized again. And then I simply asked the team whether it would be possible at all, if he came at some point, for us to look after him here until he passed away. And I think that led to this always being a topic in supervision, a topic in handovers and simply a topic between people. Some people just meet up for a coffee. And most of the things are discussed in the smokers’ corner, even though nobody smokes here, but a lot of change is initiated over coffee. I think—thank God—it’s been well structured from an early age. And they knew that there are people who ask critical questions, and they knew, I’m interested in how they want to deal with this. Because, to be honest, I wouldn’t have had a solution to this problem at the time. And so, the door was open for the other relatives of our colleagues, because we knew that if we did it for one person, it wouldn’t be a question for another relative. And we simply created firm rules about what happens when a relative comes in and said immediately, “This shift, which is alone, is the night shift, and with my consent, which I have also obtained from the nursing service management, one can immediately bring in an additional person” so that the person is no longer alone and doesn’t have to make any decisions on their own. (Int. Nurse Manager)
Beyond considering current capabilities for action, the process of enabling also ensured future capabilities for acting, as it allowed the team to “pinpoint difficult situations and process them.” Thus, enabling prevented the accumulation of mental and emotional load, which could impede long-term functioning and long-term mental health (Schabram & Maitlis, 2017): And I think it was also important for the team to experience this, to talk about it in advance during supervision and to discuss the whole thing again afterward during supervision. Is there anything else? Is there anything to work through? Is there anything to discuss about the whole thing? How is everyone coping? Or is there anything else that needs to be discussed together so that everyone is on the same page? (Int. Nurse E)
In summary, the caring processes of doing for and enabling endogenously equipped the team with resources to act, which is consistent with theory on high-quality connections (Dutton & Heaphy, 2003). The two processes enabled the integration of different perspectives to identify new and feasible opportunities. This approach accounted for the interdependencies that are inherent in a team setting, especially in interdisciplinary teams (Mathieu et al., 2008; Stoverink et al., 2020). Overall, engaging in doing for and enabling allowed the development of action strategies as well as effective adaptation. Consequently, we propose the following proposition:
Team Resilient Outcomes
Since the experience of adverse events threatens a team’s identity, well-being, and performance, a team resilient outcome is established if the team demonstrates that it can recover its identity, well-being, and performance (Hartmann et al., 2020a; Sutcliffe & Vogus, 2003). We observed how engaging in caring helped to build resources and endogenously endowed the team to develop team resilient outcomes. We detail the team resilient outcomes with representative quotations in the following section and in Table 4.
Team Resilient Outcomes
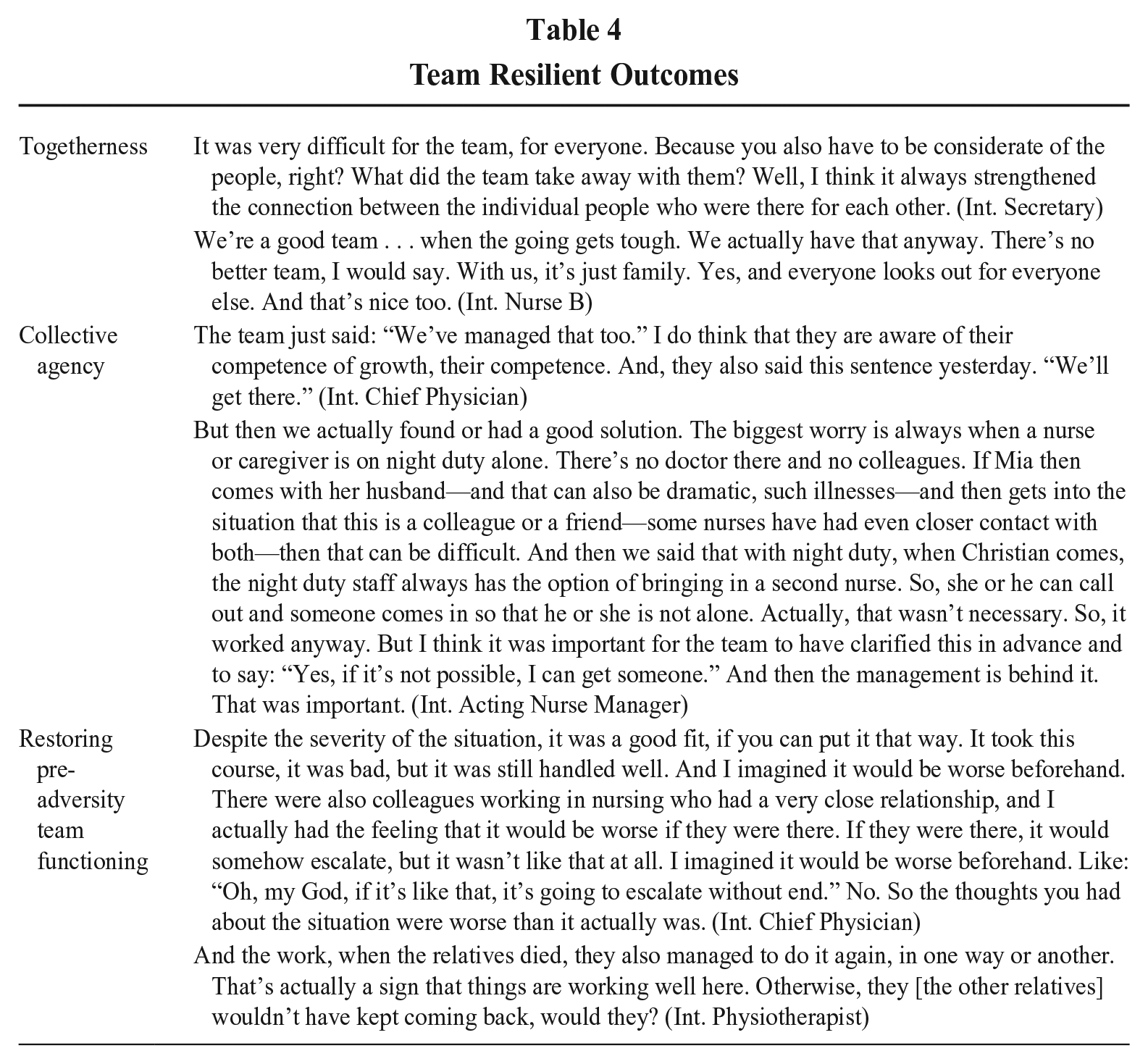
Togetherness
First, engaging in caring fostered the team’s feeling of togetherness. The feeling of togetherness reflects a strong sense of belonging and connection to the team, understood as a higher-level social unit. Experiencing the mechanisms of caring signaled to team members how important the team was to the individual team members: [We learned] that you can really get through crises like this. And I believe that we also learned how important we are to each other. (Int. Nurse Manager)
Moreover, caring for each other in a mutual process made team members feel and experience that the team was more than the sum of individuals or individual actions. As such, through caring, the team was endowed with a feeling of wholeness, a capacity that could only exist on a collective level and by the entirety of the team: [The team has learned as a whole, that] we simply feel like a team. So that’s really cohesion. Or even with our parties or when we have the festival of flowers, that’s just such cohesion with the team. [. . .] I’ve also sought help from the respiratory therapist, one time. You can approach anyone and get support. And you actually feel good because it really is a big team, and you know you can go to anyone and get help from anyone. (Int. Nurse A) Everyone is a piece of the puzzle. And every piece of the puzzle is equally important. (Int. Social Worker)
Having this sense of belonging and wholeness was a relief for the team, as it created safe social spaces again. In these spaces, team members felt valued, close to each other, and secure again. As different team members explained: No situation is difficult enough that you can’t get through it, right? You can get through everything. The more you are with one another, the easier it gets. A sorrow shared is a sorrow halved. (Int. Physiotherapist) And you are not alone. So, we are not alone. We are still a team, and we stick together. This provides security and support. (Int. Nurse C)
Overall, the feeling of togetherness endowed the team with security concerning who the team members were and what they belonged to. These feelings of security and safety provided anchoring in the face of uncertainty and unburdened the team by preventing additional resource losses and, consequently, accumulating strain.
Collective Agency
Second, engaging in caring also fostered the team’s collective agency. Collective agency describes the team members’ understanding “that they have the capacity to act together to try to influence the problem they face” (Lawrence & Maitlis, 2012: 652-653). As such, collective agency provides a team and its members with the feeling that they can be successful together, heal and renew themselves, and accomplish good outcomes, even in the face of hardship (Bandura, 2001). By engaging in caring, team members became aware of their team as a resource, which strengthened their beliefs in their capabilities to act: What initially appeared to be a positive development (staff replacement) then caused unrest in the team, but we managed to overcome this together. (Ref.)
The team learned to make use of the team as a resource to handle difficult situations: I’ve learned that it always goes on, no matter what. But that you keep going, even if something throws you off track. And also, that you have to keep going as a team. It doesn’t help, does it? Actually, Christian was such a link for us or the other relatives. Because when there was a party, the relatives were also there. But we need to move on . . . and we need to support them [those, who lost a relative on the ward] and take them with us. (Int. Nurse D)
Endowing faith in the team’s capabilities for action helped establish new guidelines for collective action. It enabled the team to develop opportunities and establish boundaries: Firstly, it has changed because we have learned how important communication is. I don’t think anyone was so aware of that with the patients or in the team. And that has changed. They talk to each other more. That it’s also about priorities. So, they do not avoid the issues anymore. (Int. Nurse Manager)
This better understanding of action capabilities provided the team with safety for action: Simply the knowledge that you can deal with something like that. Perhaps also knowing your limits: You can take on something like this, but in that kind of situation you might rather say no. But I think, on the whole, it’s more the feeling that you can pull something like that off well. (Int. Pastoral Care)
As such, by using collective agency, the team could unburden itself from the strain of the loss of safety for action. The consideration of current capabilities allowed the team to make decisions jointly and reestablish safe spaces for action.
The team also said, “Yes, that’s how it works, that’s how it is.” It’s simply “spreading the load over several shoulders,” this burden, and saying: “They’re all in this together.” And it’s not the case that just because I’m the doctor or the senior doctor and she’s the boss, that we’re now above them. Of course, we have to make the decisions. I don’t want to dismiss that at all. But to also see from the nursing side that the decision is supported, that it fits, that it’s good as it is, and that it’s also coherent. (Int. Senior Physician)
Consistent with Principle 2 of COR theory (Hobfoll et al., 2018), the team invested resources of caring to recover from the loss of safe spaces and to endow resources of togetherness and collective agency. Furthermore, through successful coping based on caring, the team could protect itself from additional resource losses and strengthen its resource reservoirs. This result underscores the COR theory notion that “although stressful events often involve diminishment of resources, reversing resource loss is likely to restore well-being” (Hobfoll, 2002: 314).
Restoring Pre-Adversity Team Functioning
By making use of the gained resources of togetherness and collective agency, the team was able to demonstrate restored functioning despite adverse experiences. The positive feedback from patients and their relatives expressed during conversations and in thank-you cards served as evidence that the team’s quality of service recovered quickly. Furthermore, although the team leaders tried to limit the intake of patients on specific days of the adverse events (for example, on the days when relatives died on the ward), on average, the number of treated patients remained the same, indicating that the quantity of work performed recovered. Finally, the chief physician and the team members evaluated the team’s handling of the situation as “competent, caring and affectionate” and felt that their performance recovered well.
Our analysis suggests that the demonstration of team functioning was fueled by the resources of togetherness and collective agency. For example, togetherness fostered joint effort and balanced team members’ contributions. This effect was important, as interdisciplinary teams can only perform at the highest level if all team members contribute their specified skill sets. As a medical intern explained: Here, it is a different kind of working together. Dr. Petersen takes the lead, and she says from the beginning, “We are one team, and we all work together.” And she includes everybody, but she also expects that everybody will join in. And that’s the reason things work so well here. (Int. Medical Intern)
Moreover, team members were aware of their togetherness as a resource, because a team, not individual efforts, is needed to achieve certain things: And in our work, in particular, we need the team. Because every individual is lost here, I think. Because it’s simply difficult. (Int. Secretary) I simply realize that if the team didn’t work together as well as it does, from my perspective, the work would be much more difficult. You often have the feeling that you’re actually looking forward to coming here and to working together. And that simply makes a lot of things easier. (Int. Social Worker)
High levels of functioning were also enabled through the experience of collective agency. Knowing that the team has the capacity to address the problems at hand provided the confidence needed to perform at high levels despite obstacles: We decided as a team what we could do to provide support when the time comes, but we didn’t actually need those plans. We discussed that we could leave Marie out of the shift. But it was good for Marie that she was there. So, we didn’t really need that at all. There were already thoughts of “if, in case,” but we didn’t really need that. As strange as that sounds, but it was good, actually. (Int. Nurse B)
As the interview excerpt exemplifies, what helped the team perform was not the strategy per se but rather knowing that the team felt competent to act and could exercise influence—that is, collective agency. On the basis of our analysis, we make the following proposition:
Interepisode Effects
The process perspective on psychological resilience argues that “early experience shapes later experience” (Sutcliffe & Vogus, 2003: 97). The experience that a team has gained in one resilience episode influences the feelings, cognitions, and behaviors in a subsequent resilience episode and helps determine how a team copes with adverse events—that is, resilience enactment (Bandura, 1986). We also identified this interepisode effect in our data. We observed how the team enacted and demonstrated resilience in the face of the first adverse event and built valuable resources. These resource reservoirs positively influenced the team’s enactment of resilience when facing the second adverse event, which is consistent with Corollary 1 of COR theory: “Those with greater resources are less vulnerable to resource loss and more capable of resource gain” (Hobfoll et al., 2018: 106). We elaborate on these inter-episode effects—that is, the effects that connect one resilience episode with a subsequent resilience episode–with representative quotations in the following section and in Table 5.
Interepisode Effects
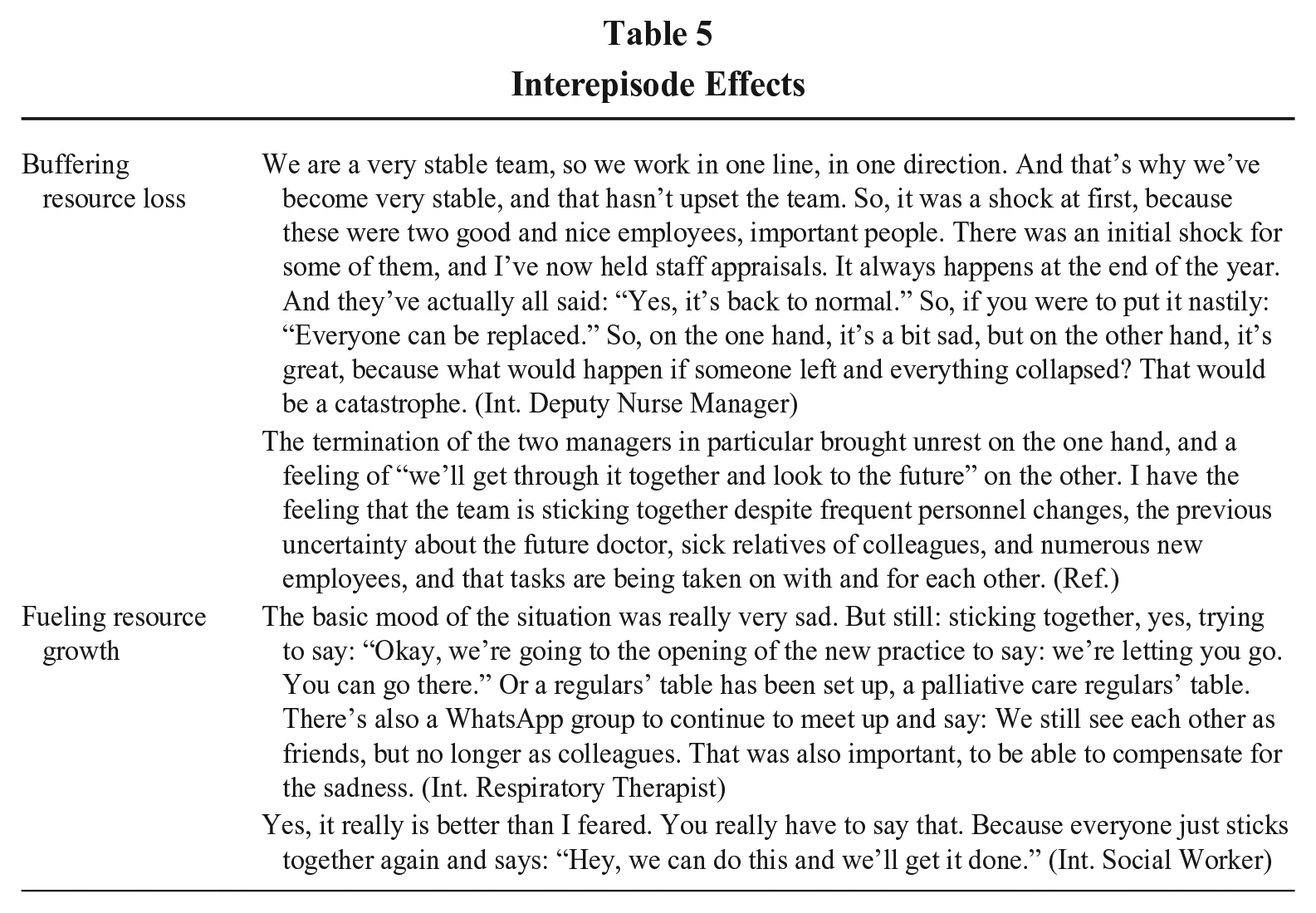
Buffering Resource Loss
The team developed togetherness and collective agency through caring during the first adverse event. When experiencing the second adverse event, the team could draw on these resources to prevent resource loss, as suggested by COR theory (Hobfoll et al., 2018). Although different, the second adverse event was experienced as severe as the first adverse event. However, during the process of enacting resilience in the first experience of adversity, the team experienced that they were together and capable of addressing obstacles. This experience provided the team with strong confidence and realistic optimism (Swanson, 1991), which acknowledged not only the severity of the situation but also the team’s resources. Although the specific outcome of the situation was unknown, this knowledge about collective capabilities was comforting and provided hope, which buffered against the resource loss of safe social spaces and the resource loss of safe spaces for action: At the hospital summer party, the palliative team sits together at a table and shares a drink. Team members talk and joke with each other. Some team members playfully tease Jonas about his intentions to leave the team. He replies with a smile on his face but is clearly sad. Leaving the team seems to be difficult for him. Dr. Petersen looks tired. She talks with each of the team members, asking how they feel about the situation. Marie approaches her and states, “Well, that news was . . . kind of heavy.” She then adds confidently, “But we have already overcome so many hurdles this year, and this is not going to knock us out, right? I mean, the rest of us are not going to leave the team. We will stick together!” (Obs.) It’s similar; it’s sadness again. But it’s like this: We’ve been there, right? We already know, we’ve been through it before, a situation like this. We got through it then, and we’ll get through it again this time. This time it is almost easier because we have already developed a strategy to deal with it. So, we already know: What supports us? We do a lot together, we support each other again, we write each other cards again, we write each other letters again. We know where we can go. And we’ve known that from the beginning, we’ve already known that. And that’s why it isn’t so bad now, I think. (Int. Respiratory Therapist)
Fueling Resource Growth
In addition to its buffering effect, the knowledge of the gained resources of togetherness and collective agency also fueled resource growth by endogenously equipping the mechanisms of caring as a form of enactment of resilience. Moreover, the knowledge that caring was a successful form of enacting resilience and the training in exercising caring strengthened the different mechanisms of caring. As such, the team invested resources to fuel additional resource growth (Hobfoll et al., 2018): Well, I think that the situation at the beginning of the year actually strengthened our team. I do think that. Because the team spirit has simply improved. It was already good before. But now, because of all the tragic stories, it has actually become even closer. And of course when someone leaves, that’s when it’s really difficult, isn’t it? But as I said, you can always call them. They’re still there in person, they’re still there. You can still call them. We now also have a palliative care WhatsApp group. And they still all write in there. (Int. Secretary)
The finding that resource gains of prior resilience episodes can fuel connected resource growth in the face of subsequent adverse events can be interpreted considering Principle 3 of COR theory, which states that “resource gain increases in salience in the context of resource loss” (Hobfoll et al., 2018: 106). As such, when additional resource loss is experienced, the gain of resources accelerates and can have increasing effects on coping, as actors may experience hope, which fuels goal-directed effort (Hobfoll, 2011b). Thus, the development of these so-called resource gain spirals can explain how resilience may unfold over time and may fuel long-term and healthy team functioning. Furthermore, experiencing adverse events may function as a restriction on Corollary 3 of COR theory, which states that resource gain spirals are weak and develop slowly (Hobfoll et al., 2018). In fact, the experience of adverse events seems to speed up the development. Thus, the interdependencies between the experience of adverse events and the enactment of resilience must be considered. Consequently, we make the following proposition:
Discussion
Our study contributes to the understanding of team resilience by highlighting the important role of the relational process of caring for teams to enact resilience in the face of adverse events and by identifying and relating core elements of the team resilience process. Specifically, we found that adverse events can be conceptualized as experiences of loss, creating a loss of safe social spaces and a loss of safe spaces for action. We explored how teams can enact team resilience through the relational process of caring and specified that caring in teams can be established through four dimensions that serve different purposes. Engaging in the caring dimensions of understanding and being with seems conducive to healing social spaces, while engaging in the caring dimensions of doing for, and enabling helps heal collective action capabilities. Ultimately, caring can build the resources of togetherness and collective agency, which are conducive to restoring a team’s functioning. Finally, the resources of togetherness and collective agency can buffer and restore resource loss and fuel resource growth in subsequent team resilience episodes. These findings expand our understanding of the team resilience process to explain how teams can effectively respond to adverse events by drawing on relational mechanisms. Our findings are of great relevance for the many teams prone to facing adverse events (Maynard et al., 2018), especially given the ever-increasing levels of uncertainty and dynamism in today’s workplaces (Schmutz, Bienefeld, Maynard, & Rico, 2023).
The Role of Caring as a Relational Mechanism for Team Resilience
We offer a theoretical model explaining how team resilience is developed and enacted through relational mechanisms in the face of adverse events. We pinpoint caring, which is a positive form of connecting and interrelating (Saks, 2021), as a key relational behavior for developing team resilience. Although caring is a fundamental element in humanity, it has received little attention in management research (Saks & Gruman, 2024). This oversight is unfortunate, as caring might be of growing importance, especially in an environment that is changing fast and is prone to adverse events (Gibson, 2020). In fact, prior research has shown that a sole focus on task completion and avoidance of social and emotional realities in the face of adverse events is likely to increase distress rather than resolve it (Kahn, 2018), which likely inhibits high-level performance (Barnes, Wagner, Schabram, & Boncoeur, 2023). Our research suggests that caring as a key resource of teams might nurture positive and healthy functioning, especially when facing adverse events. Thus, our research challenges the common narrative that a concern for others cannot be reconciled with a focus on organizational functioning or high performance and echoes the call for acknowledging the importance of caring (George, 2014; Lawrence & Maitlis, 2012).
Specifically, our research highlights how caring enables team resilience. We identify four dimensions of caring and specify how these dimensions fulfill different functions in the team resilience process. First, with the start of a team resilience episode marked by an adverse event, caring seems to be an important prerequisite for engaging in a collective coping process, as caring in teams is a reciprocal act and forms social bonds of mutuality. Thus, caring fosters the construction of joint struggles, which fuels the synchronization and coordination of coping efforts toward collective action targeting joint goals (Kahn, Barton, Fisher, Heaphy, Reid, & Rouse, 2018).
Second, caring matters as a relational process to reduce the impact of adverse events as loss events and to foster healing from adverse events. Engaging in caring can stop and even reverse the resource-draining effect in teams triggered by adverse events. Specifically, the caring dimensions of understanding and being with can create holding environments (Kahn, 2001) that shield against additional loss of safe social spaces. By creating a sense of security and safety, relational wounds can heal so that team members feel a strong sense of connection. Moreover, the caring dimensions of doing for is important to realize the potential of teamwork (which builds on the competencies of multiple actors) through mutual support and an acceptance of current limitations. Simultaneously, enabling can help create feasible scripts for action on which the whole team agrees. Developing such scripts counteracts the feeling of the loss of safe spaces for action and nurtures opportunities for action as well as the team’s collective efficacy. Overall, caring helps to process strain and anxiety collectively and allows psychological closure (Barton & Sutcliffe, 2023). Thus, we argue that caring is an important mechanism for breaking resource loss spirals. This implication extends our understanding of COR theory and team resilience, as Hobfoll et al. (2018) highlighted that understanding how to break resource loss spirals is key to our understanding of resilience.
However, teams engaging in caring not only break loss spirals but also trigger regaining functionality and improve it through resource gain spirals. Caring represents a process of active connecting through which team members can endogenously equip the team with resources. Through its different dimensions, caring helps team members grow closer together and develop a feeling of togetherness. Moreover, by caring for each other, team members can combine physical and cognitive resources in novel ways and develop effective strategies for action that can leverage existing capabilities and even build new capabilities. Doing so fuels collective agency, which produces a shared belief among team members that they have the collective power to achieve the desired results (Bandura, 2001). Both of these resources—that is, togetherness and collective agency—enable future-oriented coping. As such, caring can be understood as both a loss-oriented resource that prevents future loss and a gain-promoted resource that promotes future gains.
Thus, from a COR theory perspective, we argue that caring functions as a key resource (Hobfoll, 2002), which is particularly important for the resource gain cycle, as key resources have the potential to nurture and grow connected resources (Sonnentag & Meier, 2024). For example, through caring, teams are likely to grow connected resources—that is, develop team resilience outcomes. Hobfoll (2002) explains that in contrast to entity-based resources, some key resources function as processes, which also applies to caring, as caring is a relational process. However, caring combines many important resources, such as “the presence of intimate others who can be confided in” (Hobfoll, 2002: 310), feeling valuable to others, intimacy, companionship, affection, or help (Hobfoll, 2001), among others. In this regard, our research extends COR theory, which has primarily been applied to individuals, as we identify a collective key resource that applies to teams. Integrating caring into team interactions may help teams to build powerful resource caravan passageways, specifically nurturing conditions, which foster resource-fueling processes and trigger resource gain spirals that endogenously equip teams with resource caravans—that is, an aggregation of connected resources (Hobfoll, 2001, 2011a, 2011b; Hobfoll et al., 2018).
By highlighting caring as a key mechanism for developing team resilience, we not only contribute to resilience theory but also enrich the research on caring in organizations. Our analysis provides a more granular understanding of the process of caring and its dimensions. Our identification of four caring dimensions illustrates the facets of caring and might serve as a starting point for a more granular conceptualization and operationalization of the phenomenon of caring in work relationships.
Team Resilience as a Dynamic Process
Our model takes a process view of team resilience. We theorize about the interplay of adverse events, resilience enactment, and the development of resilient outcomes, and we elucidate interepisode effects through which one resilience episode influences a subsequent resilience episode.
Adversity as a Loss Event
We theorize about the concept, meaning, and impact of adversity or adverse events. Although adversity is a defining element of the resilience process, it has rarely been part of the actual investigation in prior empirical studies on resilience (Raetze et al., 2021). Fisher et al. (2023: 1070) even stated that “the adversity component is arguably the biggest ‘black box’ in theory and research regarding the resilience process.” Building on COR theory, we conceptualize the experience of adverse events as loss events to explain how adverse events negatively affect teams and their members. According to COR theory, “items that clearly reflect loss are the most psychologically threatening” (Hobfoll, 1989: 518). This perspective can explain how adverse events create strain and stress, as, from a COR perspective, stress can be defined as “a reaction to the environment in which there is (a) the threat of a net loss of resources, (b) the net loss of resources, or (c) a lack of resource gain following the investment of resources” (Hobfoll, 1989: 516). Importantly, loss is not only a part of bereavement but is also inherent to a variety of other undesirable events (Hobfoll, 1989). Hence, such a perspective can help to better understand how adversity as a loss event unfolds its effects. In our study, we specified two forms of loss resulting from the adverse events—that is, loss of safe social spaces and loss of safe spaces for actions. The loss of safe social spaces may threaten a team’s identity and collaboration (Hobfoll et al., 1990), while the loss of safe spaces for action jeopardizes a team’s performance. Hence, illuminating this loss of felt safety explains how adverse events are threatening a team’s identity, well-being, and performance and elucidates why and how relational team processes are essential in collectively dealing with adversity. Hence, we echo Hobfoll’s (2001: 345) claim that events “must be unpacked into the losses and gains that they contain” to better understand their impact.
Enactment of Team Resilience Through Caring
Another debate revolves around how and why resilience emerges. In this regard, scholars have called for a better understanding of the mechanisms of resilience or the nature of resilience enactment (Caza et al., 2020). We extend this debate by identifying caring as a relational mechanism and form of enactment of team resilience.
Our focus on relational mechanisms extends the discussion on team resilience, which has focused on cognitive and task-focused mechanisms. However, forms of connections are of crucial importance, especially in the face of adverse events, as these experiences might shatter deep-seated beliefs about security (Maitlis, 2020). Active forms of interrelating, such as caring, can create a new space of comfort and security and are thus important to enable functioning despite such adverse events. Especially at the team level of analysis, active forms of connecting are relevant to prevent a team from falling apart and instead allow coordinated joint efforts, which are needed to tackle complex tasks. Moreover, the social, relational mechanism of caring can explain how resource reservoirs are widened beyond the naturally limited reservoir of resources that are contained within individual team members to establish collective resource pools (Hobfoll et al., 1990). Possessing relational resources can prevent the depletion of personal individual resources, which explains how the relational mechanism of caring fosters gain spirals in subsequent resilience episodes. Thus, our theorizing suggests that social relational mechanisms might be key to team resilience as a collective construct. By focusing on what team members do to establish relational mechanisms, we extend our understanding of the interpersonal dynamics inherent in team resilience and create a better understanding of team resilience as a collective enactment.
Team Resilient Outcomes
In resilience research, clarity is required regarding what can be classified as a positive outcome (Masten, 2001). Most of the prior research has highlighted the importance of team performance as a marker of a team resilient outcome. However, scholars have recently started to argue that a narrow, often short-term focus on performance might be inadequate for making judgments about resilient outcomes (Hartmann et al., 2020a; Raetze et al., 2022). For example, a team that manages to bounce back in performance shortly after an adverse event might still suffer from emotional breakdowns and fall apart later. Accordingly, in terms of COR theory, a team might exhaust its resources to meet short-term performance goals and enter a defensive state afterward, lacking any resource pools. Such a scenario does not reflect a sustainable form of team resilience (Barnes et al., 2023).
Thus, we provide a more comprehensive understanding of team resilience outcomes and depict the relevance of three different markers. First, we pinpoint togetherness as a team resilient outcome. Togetherness may secure a holding environment and can endogenously equip a team with a strong sense of connection (Barton & Kahn, 2019). Second, we identified collective agency as a team resilient outcome. Collective agency provides a team with a feeling of competence and shared intentions (Makowski, 2024). Both these resources are needed for future-oriented functioning and enable a gain-oriented focus. As such, togetherness and collective agency reflect healthy team states that restore pre-adversity functioning, which we highlighted as a third marker of a team resilient outcome. In addition to restoring team functioning, healthy team states of togetherness and collective agency also influence how the team handles subsequent adverse events. Thus, our theorizing underlines the importance of considering team resilience markers beyond narrow, short-term task performance.
Interepisode Effects
A further field of inquiry addresses how resilience processes unfold over time and, specifically, how facing and dealing with adverse events will affect the experience and management of subsequent adverse events (Caza et al., 2020; Hartmann et al., 2020a; Raetze et al., 2022). In this regard, scholars have clarified that studying the effects of different resilience episodes is difficult and may require longitudinal methods that capture the experience of different adverse events and how actors deal with these events (Caza et al., 2020). On the basis of our data, we were able to theorize about intraepisode effects, which occur within one resilience episode, and interepisode effects, which connect different resilience episodes.
Specifically, the team resilient outcomes of togetherness and collective agency influenced the subsequent resilience episode in two ways. On the one hand, they fueled a maintaining belief in the team and its capabilities and, thus, buffered the loss of resources, which was triggered by the adverse event. Consequently, the team experienced reduced loss of safe social space and reduced loss of safe space for action compared to the experiences in the first resilience episode. On the other hand, the resources of togetherness and collective agency fueled additional resource growth and strengthened the enactment of caring to handle the loss of safe spaces. Our findings resonate with Corollary 1 of COR theory in that those resources gained by successfully handling the loss triggered by the experience of the first adverse event made the team less vulnerable to resource loss when facing a second adverse event (Hobfoll et al., 2018). Moreover, the fueling of additional resource growth illustrates how resource gain spirals are created. Therefore, our study pinpoints how adverse events can be handled to allow for long-term growth and thriving. Although prior research has focused on the trajectories up to the point of bouncing back, we consider the trajectory that follows one episode of resilience. Our findings may also be interpreted in terms of human sustainability, which investigates how employees can perform at a high level without subverting their psychological or physiological well-being (Barnes et al., 2023). The literature on human sustainability underscores a long-term focus and highlights a sustained ability to perform (Barnes & Wagner, 2023). To sustain this long-term functioning at the team level of analysis, markers such as togetherness and collective agency seem crucial.
Practical Recommendations
Our research suggests that teams can develop resilience through caring. Several mechanisms can help develop capacities for caring, which can be activated if and when adverse events strike. First, teams can benefit by building an ethic of caring, which highlights the value of relationships and caring for connected others (Lawrence & Maitlis, 2012). Our findings also showed that allowing for team members’ voice can foster caring. If their perspectives are heard and considered, team members feel valued and important to the team. As such, team meetings on important topics or decisions could be implemented such that each team member is asked to share their own perspectives at the beginning of the meeting. Moreover, rituals can be a powerful tool for establishing caring practices (Saks & Gruman, 2024). Rituals can help reduce anxiety and uncertainty and enable shared emotions by providing shared attentional direction and a locus of control (Lepisto, 2022; Metiu & Rothbard, 2013). Moreover, they can boost confidence and strengthen relational bonds (Hobson, Schroeder, Risen, Xygalatas, & Inzlicht, 2018; Slavova & Metiu, 2022). Although rituals can be learned and trained in the absence of adverse events, they can become especially powerful during adverse events.
Limitations and Future Research
As with all empirical work, our study has limitations. First, we derived our findings from studying team resilience in a multidisciplinary palliative care team. We thoughtfully selected our research context because unconventional contexts offer an opportunity to better understand understudied processes (Bamberger & Pratt, 2010; Bell, Fisher, Brown, & Mann, 2018). In other words, we purposefully build on the extreme setting of palliative care to elucidate the different elements of the team resilience process. As explained by Hymer and Smith (2024: 8), harnessing this extreme setting allowed us to “illuminate patterns that may be difficult to detect in more ordinary organizational contexts.” Nevertheless, the natural question may arise as to whether the implications of our findings can be transferred to teams in other contexts.
We selected the context of palliative care because we were confident that palliative care teams are highly likely to develop effective responses to adverse events, as they are well trained to cope with high daily work demands, as explained in the Methods section. However, other types of teams are also likely to experience such adverse events and such responses to adverse events. For example, the illnesses of relatives, or even the illness or death of a team member, are circumstances that teams in all types of organizations may face and that may severely harm team functioning (Kahn, Barton, & Fellows, 2013). Moreover, the loss of team members is a critical challenge, especially if these team members have a special role, such as in interdisciplinary teams, which need the different competencies in the team. As our theorizing is general in nature—that is, not specific to the healthcare context—and is anchored in COR theory, we suggest that our general propositions and the identified mechanisms will be transferable to other organizational contexts. However, how these mechanisms are enacted might vary. For example, in our case, the caring mechanisms of being with involved physical contact, such as hugging. In other contexts, these forms of relating might not feel appropriate. In these cases, the mechanisms of being with might be more strongly enacted through narrative practices (Lawrence & Maitlis, 2012). Hence, although we do not (of course) claim statistical generalizability based on our qualitative analyses, the conceptual model developed in this study offers analytical transferability—that is, the transfer from our specific empirical findings to general theory—which, in turn, can be applied to other contexts (Hymer & Smith, 2024; Pratt, Lepisto, & Dane, 2019). Thus, the adverse events that teams experience and the specific ways in which teams from other contexts engage in the four highlighted caring processes might differ, but we expect the role of adverse events as a loss event, the role of caring in the team resilience process, and the process of interepisode effects to be conceptually transferable across contexts. Nonetheless, future research on the team resilience process in different professional contexts would help to probe the transferability our research implies. Our propositions might offer a starting point for such research.
Second, we collected different forms of data—that is, field notes from site visits, interviews, written reflections, short surveys, and secondary data. We acknowledge that each of these forms of data has its own limitations. We tried to address these limitations by triangulating our findings across data sources. Moreover, an important hurdle in research on resilience is the frequent unexpectedness of adverse events. Therefore, in field research that is based on primary data, rich data are difficult to collect before, during, and after adverse events. In our case, as soon as we established contact with the palliative care ward and heard about the current adverse event, we tried to collect as much information as soon as possible. We were also lucky to be in the palliative care ward and could collect data when the second adverse event hit. To extend our research, future empirical research that provides an even more granular understanding of the interplay of the experience of adverse events and processes of recovery in establishing resilience would be useful. For example, future research could investigate whether different forms of adverse events, such as people- vs. task-related adverse events or endogenous vs. exogenous adverse events, might influence the team resilience process differently.
Third, although our study did not focus on the role of leadership, team members highlighted that their chief physician was important as a role model, as exemplified, for example, by the quote from the medical intern. This importance has also been highlighted by prior theory and research on the interplay between resilience and leadership (e.g., Barton & Kahn, 2019; Todt, Weiss, & Hoegl, 2019). Moreover, scholars suggest that leaders can act as role models to establish caring cultures in organizations (Saks & Gruman, 2024). We recommend that future research develops a better understanding of how leaders can facilitate or inhibit the resilience process.
Finally, we provide a conceptualization and analysis of caring in teams and of caring as a mechanism of resilience enactment. Our coding built on, extended, and refined Swanson’s (1991) perspective on caring. Her analysis argued that facilitating others to maintain belief could be considered a dimension of caring. On the basis of our data, we did not find that maintaining belief is an element of the caring process. Our data suggest that maintaining hope plays an important role in interepisode effects. Future research on our second proposition would be valuable to validate the different dimensions of the caring process.
Overall, we are still in the early stages of the research on the team resilience process. Therefore, we hope that the conceptual model developed in this study provides fertile ground for future studies to further advance, refine, and contextualize the theory on the team resilience process.
Footnotes
Acknowledgements
We are deeply grateful to our study participants who shared their stories with us and allowed us to immerse ourselves in this sensitive work context. We would like to thank our editor Nicky Dries and the anonymous reviewers for their insightful comments for improving our manuscript throughout the review process. Moreover, we would like to thank Sally Maitlis, Marlys Christianson, and Paula Jarzabkowski for their valuable feedback on prior versions of this manuscript. We wish to acknowledge financial support from the Bavarian research consortium ForChange and the Joachim Herz Foundation.