
Abstract
When teams in organizations are assembled to perform contingent tasks, team members carry with them experiences of prior interaction with partners in different teams. Focal team members share collaborative experiences to the extent that they worked with common external prior partners. Extending current research on team effectiveness, we investigate how shared collaborative experience (SCE) affects team performance. Consistent with the established understanding of team processes as carrying both a teamwork and a taskwork component, we conceptualize SCE as having two distinct dimensions that we call SCE extent and SCE diversity. We posit that high SCE extent increases the ability of teams to refine their teamwork processes, increasing their performance through enhanced coordination and reflexivity. We argue that high SCE diversity hinders the ability of teams to form a shared understanding of task demands, thus undermining team performance. Furthermore, we investigate the contingent effect of task complexity on the relationship between SCE and performance. We argue that the benefits of implicit coordination and the drawbacks of experience diversity decrease as tasks become more complex and require more explicit coordination and wider repertoires of responses. These predictions find support in an analysis of 1343 robot-assisted surgery operations performed by 114 surgeons during a four-year period in a private university hospital. By explicitly recognizing how team members benefit from the network of their shared prior partners, our study contributes to developing a new approach to study the effectiveness of temporary teams in organizations.
Teams are important in organizations because they enable collaboration among participants with different knowledge, experiences, and cognitions (Cohen & Bailey, 1997; Hackman, 1987; Kilduff, Angelmar, & Mehra, 2000). Building on classic theories of social groups (Homans, 1950: 84-85), teams in organizations are typically understood as stable and clearly bounded subsets of organizational members working interdependently to achieve common goals (Mortensen & Haas, 2018). However, organizations are increasingly relying on temporary action teams whose membership is unstable and drawn from a broader pool of skilled participants to perform contingent or temporary tasks (Bakker, 2010; Klein, Ziegert, Knight, & Xiao, 2006; Wimmer, Backmann, & Hoegl, 2019). Action teams are common in organizations operating in settings such as emergency relief (Klein et al., 2006; Majchrzak, Jarvenpaa, & Hollingshead, 2007), competitive sports (Hüffmeier, Filusch, Mazei, Hertel, Mojzisch, & Krumm, 2017), flight crews (Ishak & Ballard, 2012), and health care (Edmondson, 2003; Vashdi, Bamberger, & Erez, 2013). Typically, action teams disband after completing a set of tasks, and team members eventually reassemble, perhaps with a different composition, around new tasks.
While action teams may benefit from their fluidity and adaptability to dynamic and complex task environments (Mortensen & Haas, 2018), their lack of stability poses challenges for the development of conditions known to be critical for team effectiveness, such as coordination (Valentine & Edmondson, 2015), learning (Reagans, Argote, & Brooks, 2005), experience (Dayan & Di Benedetto, 2011), and shared cognition (Argote, Aven, & Kush, 2018). Extant studies suggest a positive relationship between shared team experiences, such as team familiarity (Huckman, Staats, & Upton, 2009) and team effectiveness (Espinosa, Slaughter, Kraut, & Herbsleb, 2007; Huckman & Staats, 2011), highlighting the importance of elements of “social sharedness” (Tindale & Kameda, 2000) as necessary conditions for team cohesion. Building on the assertion that temporal stability provides a foundation for the accumulation, storage, and retrieval of shared knowledge (Vashdi et al., 2013), studies of teams within organizations examine how shared team experiences may develop in unstable settings, with particular attention paid to the contingent factors through which team familiarity affects team effectiveness (Avgerinos, Fragkos, & Huang, 2020; Luciano, Bartels, D’Innocenzo, Maynard, & Mathieu, 2018).
Given the propensity of individuals working together in teams in transient settings to benefit not only from their own direct experiences of working together, but also from experiences accumulated by working with prior partners in different teams, a recent line of research has examined the role of exposure to multiple prior partners across team boundaries as an alternative to team familiarity (Aksin, Deo, Jónasson, & Ramdas, 2021; Kim, Song, & Valentine, 2023). These studies examine the conditions under which team staffing strategies based on prior partner exposure (aimed at maximizing the experience gained from working with multiple partners across teams over time) may be superior to strategies based on team familiarity (aimed at maximizing the experience gained from working with partners within the same team over time). Research on the conditions making prior partner exposure comparatively more (or less) effective than team familiarity has produced mixed empirical results while leaving two important issues unresolved. First, these two strategies are conceptualized in antagonistic terms: team members who increase their exposure to multiple prior partners do so at the cost of decreased team familiarity. This view neglects the fact that these partners are themselves embedded in a network of dynamic collaborative relationships across different teams over time. In this paper, we argue that when focal team members have prior partners in common, teams can still reap the benefits of “learning from many” (Aksin et al., 2021) without sacrificing elements of familiarity that are important for team functioning. Second, prior studies suggest that as prior partner exposure increases, team members become better able to tap into a more diverse set of task-relevant knowledge by expanding the set of experiences to which they have access (Aksin et al., 2021; Kim et al., 2023). This view fails to recognize that greater prior partner exposure does not necessarily entail access to more diverse knowledge unless those partners increase the diversity of the focal team’s task-related experiences (Bunderson & Sutcliffe, 2002; Huckman & Staats, 2011). In this paper, we amend these limitations by extending the way we think about prior partner exposure by considering: (i) how focal team members may form shared collaborations with these prior partners, thereby preserving elements of social sharedness that are crucial for team functioning, and (ii) how focal team members may leverage these overlapping collaborations to accumulate task-specific experience that is important to react effectively to the task environment.
We refer to this distinctive form of experience as shared collaborative experience (henceforth SCE), which we define as the shared experience that focal team members have accumulated in the past by working with common partners (external to the focal team) across multiple tasks. Consistent with established understanding of team processes as having both a teamwork and a taskwork component (Crawford & LePine, 2013; Marks, Mathieu, & Zaccaro, 2001; Mathieu & Rapp, 2009), we conceptualize SCE as having two distinct dimensions. The first, which we refer to as SCE extent, is defined as the number of prior partners shared by focal team members accumulated over time by collaborating on multiple tasks. SCE extent reflects the teamwork component of shared collaborative experience that focal team members have accumulated through their network of prior collaborations. For example, the SCE extent of a team will be high if focal team members have collaborated with many common partners in multiple tasks over time. The second is SCE diversity, which we define as the aggregate diversity of task experiences that focal team members have been exposed to through shared collaborative experiences across multiple tasks over time. SCE diversity reflects the taskwork component of shared collaborative experience that focal team members access through their network of prior collaborations. For example, the SCE diversity of a team will be high if focal team members and their shared prior collaborators have accumulated heterogeneous experience by performing different types of tasks over time. Conversely, the SCE diversity of a team will be low when its members and their shared prior partners have accumulated homogeneous task experience by performing the same type of tasks.
We argue that the greater the number of shared prior partners among team members, the more teams are able to refine their teamwork processes and enhance their performance through improved coordination and reflexivity (Crawford & LePine, 2013; Marks et al., 2001; Schippers, Den Hartog, & Koopman, 2007). We argue, further, that the more heterogeneous their aggregate task experience, the less likely teams are to develop a shared understanding of the task at hand, thereby hindering team performance (Cronin & Weingart, 2007; Tasheva & Hillman, 2019). Finally, we propose that task complexity is an important boundary condition for the relationship between SCE and team performance. General agreement has been reached that task complexity should be particularly salient when work is distributed among multiple actors, and that high levels of task complexity are challenging for team performance because of the necessity to integrate knowledge, skills, and efforts that are both diverse and highly specialized (Danner-Schröder & Ostermann, 2022; Wood, 1986). Previous research on team processes demonstrates that team functioning is highly contingent on task complexity due to its impact on both teamwork and taskwork (Cannon-Bowers, Salas, & Converse, 1993; Crawford & LePine, 2013; Tasheva & Hillman, 2019). In this study, we examine how task complexity may moderate the relationship between SCE (extent and diversity) and team performance. Specifically, we propose that the benefits of implicit coordination and shared task understanding (Luciano et al., 2018; Rico, Sánchez-Manzanares, Gil, & Gibson, 2008) are more pronounced for less complex tasks, which benefit from the fine-tuning of partners’ well-anticipated actions.
We test our hypotheses using original data collected from surgical teams—a representative form of action teams (Edmondson, 2003; Vashdi et al., 2013)—performing 1343 robot-assisted surgeries in one of the largest and most prominent private university hospitals in Europe. We engage in follow-up qualitative research in order to complement our quantitative data analysis with in-depth insights that add contextual phenomenological evidence to our statistical results. Through detailed fieldwork, we seek to highlight the coherence between our interpretation of the quantitative evidence in support of our hypotheses, and the situated understanding of team processes at play.
Our conceptualization of SCE has important implications for the understanding of team effectiveness under conditions of instability in team membership determined by the nature of the task being performed. Recognizing that the current knowledge of the drivers of performance in traditional teams does not extend automatically to temporary action teams, our study contributes to current theories of team effectiveness and shared team experiences in at least three ways. First, our conceptualization of SCE improves the understanding of the conditions under which shared team experiences affect team performance in temporary settings by recognizing that the benefits of familiarity and social sharedness (Gruenfeld, Mannix, Williams, & Neale, 1996; Tindale & Kameda, 2000) may be obtained, at least in part, through the experience that team members accumulate by being exposed to common prior partners. Second, while the majority of prior studies on shared team experiences neglected the multidimensional content of tasks that increase variation in members’ experience portfolios (Aksin et al., 2021; Luciano et al., 2018), our conceptualization of SCE extent and diversity extends the current literature by shedding light on how the different dimensions of teamwork and taskwork contribute to explain team performance. Third, we add to the debate on the role of task characteristics in team processes (Levesque, Wilson, & Wholey, 2001; Mathieu, Hollenbeck, van Knippenberg, & Ilgen, 2017; Wang, Cheng, Chen, & Leung, 2019) by establishing the role of task complexity as a boundary condition that potentially makes shared team experiences less beneficial or even detrimental to team performance. Task complexity makes partners’ actions more difficult to anticipate. Under these conditions, more explicit forms of coordination are better able to generate effective responses to unexpected demands, and team members are more likely to benefit from team experiences that are not necessarily convergent (Espinosa et al., 2007).
Theoretical Background and Hypotheses
The increasing complexity of work arrangements in contemporary organizations makes teams less stable over time and more dependent on flexible reconfigurations of human and knowledge resources available across team boundaries (Mathieu et al., 2017; Mayo, 2022; Valentine, Retenly, To, Rahmati, Doshi, & Bernstein, 2017; Zappa, Tonellato, & Tasselli, 2023). Research on team effectiveness has examined the limits of effective team functioning in the absence of stable membership. When the duration of membership is limited to the duration of the task to be performed, team members face predictable difficulties in accumulating and transferring experiential learning earned by working together. The reduced familiarity among team members is associated with decreased coordination (Ching, Forti, & Rawley, 2021), less effective transactive memory systems (Hollingshead, 2001), and increased uncertainty about who knows what—and whom—within the team (Faraj & Sproull, 2000; Reagans et al., 2005; Ren, Carley, & Argote, 2006). Prior research has identified several factors that may help stabilize the functioning of short-lived teams. For example, a system of formal roles can reduce uncertainty by providing formal rules for how individuals should work together, regardless of their specific identities (Bechky, 2006). Meso-level structures known as team scaffolds (Valentine & Edmondson, 2015)—which include formal processes, routines, or tools for organizing teamwork—can support coordination by providing “descriptions of and templates for ongoing patterns of action” (Barley & Kunda, 2001: 76) that facilitate the emergence of trustworthiness and accountability in temporally unstable environments.
More generally, because action team members are constantly reassigned to different tasks, research has focused on the relationship between team effectiveness and characteristics that team members share—or social sharedness (Kozlowski & Klein, 2000; Tindale & Kameda, 2000). A recent line of research has highlighted the role of social sharedness in a variety of temporary work settings, ranging from health care (Avgerinos et al., 2020; Luciano et al., 2018) to new ventures (Honoré, 2022), software development (Espinosa, Clark, & Carter, 2018), and crowdsourced production (Deichmann, Gillier, & Tonellato, 2021; Lerner & Lomi, 2019). Most of these efforts have examined how different specifications of shared team experiences—and team familiarity, more specifically—can enhance team effectiveness, highlighting the boundary conditions under which familiarity may, in turn, be beneficial, irrelevant, or even detrimental to performance. For example, Luciano et al. (2018) have shown that the benefits of task-specific shared experience, such as improved synchronization among team members, may be offset by excessive complacency toward each other when tasks are frequently performed and difficult. These findings echo existing evidence on the drawbacks of excessive team familiarity (Berman, Down, & Hill, 2002; Katz, 1982) by showing that, above a given threshold, shared team experience reduces team members’ vigilance and monitoring of the system, which are particularly important antecedents of team effectiveness (Hackman & Morris, 1975).
Building on these findings, recent studies have examined alternatives to team formation strategies based on familiarity. Strategies based on exposure to multiple prior partners have been identified as substitutes for team familiarity (Aksin et al., 2021; Kim et al., 2023). These studies have examined how different composition strategies may generate trade-offs between the benefits of increased coordination that accrue from working with the same partners and the benefits of “learning from many” that accrue from exposure to multiple work partners (Aksin et al., 2021). The evidence produced by this line of research is mixed. For example, Aksin et al. (2021) have shown that higher prior exposure to partners—rather than team familiarity—benefits the performance of emergency relief teams, particularly when they are characterized by conditions of high workload and low standardization of patient pickup tasks. Kim et al. (2023) have extended the debate by showing that, in surgical teams characterized by members at different hierarchical levels (i.e., attending surgeons, resident surgeons, and scrub nurses), prior partner exposure may instead hinder team performance, particularly when decision-executing members have high exposure to decision-making members. The authors suggest that this effect may hold because team leaders “make different decisions even when faced with similar situations and have different preferences and styles,” which “may complicate trainees’ [. . .] ability to generalize from the variation they encounter among team leaders” (Kim et al., 2023: 5). Based on the idea that prior partner exposure brings diverse practices that may be difficult to reconcile, this assertion is at odds with Aksin et al. (2021: 856), who instead suggest that “prior partner exposure broadens the knowledge base of team members” and attribute a more general benefit of partner exposure to increased access to diverse work practices. These inconsistent findings seem to suggest that the extent to which temporary action teams can reap the benefits of “learning from many” is likely to depend on their ability to generate a sufficient level of social sharedness to ensure effective coordination among team members.
Shared Collaborative Experience
How can temporary action teams leverage their members’ exposure to prior partners across multiple tasks over time while preserving the elements of social sharedness necessary to guarantee effectiveness of their current teams? Our attempt to address this question starts by recognizing that when team members “learn from the same many”—that is, when team members collaborate with shared prior partners—they (i) are exposed to the same reference points, thus generating shared team experiences that are critical for effective teamwork, and (ii) access, through their common partners, shared task-specific knowledge that is critical for effective taskwork. We call this specific type of experience shared collaborative experience (SCE).
On the one hand, SCE differs from the concept of prior partner exposure—that is, “the number of distinct partners that a focal team member has worked with during a given time period” (Kim et al., 2023: 3)—by considering that prior partners may be shared among team members. On the other hand, SCE generalizes the notion of team familiarity—that is, the amount of shared experience that team members have accumulated in working together on a focal task—by extending it to the broader concept of “indirect familiarity” accumulated through prior collaborations with shared partners outside the focal team. Figure 1 exemplifies our theoretical construct compared to team familiarity and prior partners’ exposure.
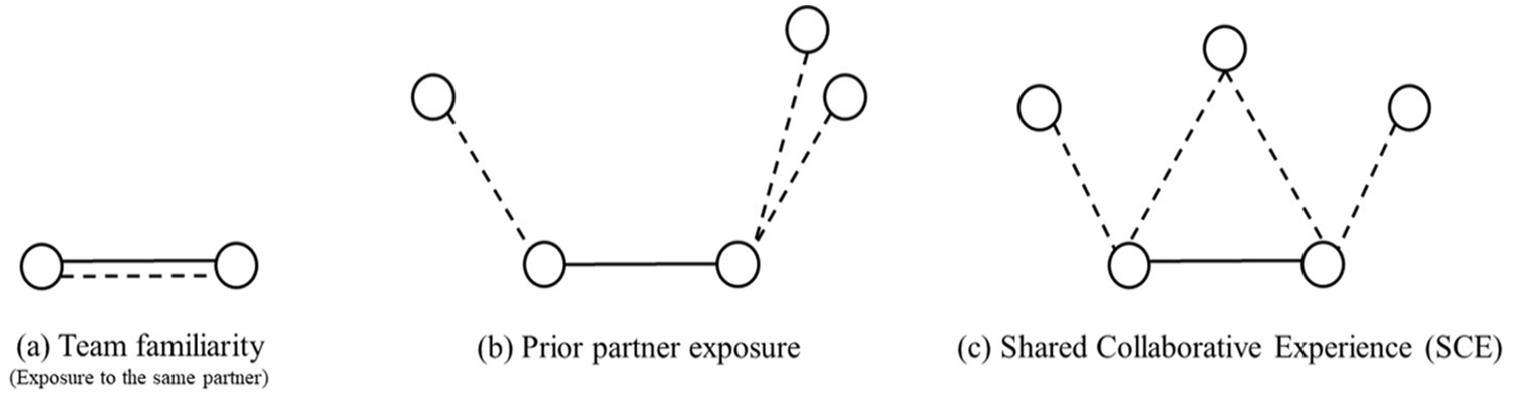
Team Familiarity, Prior Partner Exposure, and Shared Collaborative Experience
Figure 1a depicts a situation in which both current and past collaborations occur between focal team members, increasing their team familiarity. Figure 1b represents a situation in which focal team members have established collaborations with three prior partners, increasing their prior partner exposure. Figure 1c represents a situation in which focal team members have established collaborations with three prior partners (similar to Figure 1b), but only one of these partners is common. Therefore, the focal team members share their collaborative experience with this one prior partner.
In developing hypotheses about the relationship between SCE and team performance, we ground our logic in existing theories of team processes (Marks et al., 2001; Mathieu & Rapp, 2009), which are defined as “members’ interdependent acts that convert inputs to outcomes through cognitive, verbal, and behavioral activities directed toward organizing taskwork to achieve collective goals” (Marks et al., 2001: 357). Following a dynamic view of team processes as defined by a teamwork and taskwork component that develops in both action phases—that is, “activities related directly to goal accomplishment” (Marks et al., 2001: 359)”—and transition phases, that is, activities related to “reflecting on past performance and planning for future action” (Marks et al., 2001: 359), we conceptualize SCE along two distinct dimensions. The first, SCE extent, is related to the teamwork component, which reflects how teams interact to coordinate their cognitive and behavioral activities. This construct—defined as the number of prior partners shared by focal team members accumulated over time by collaborating on multiple tasks—captures the extent to which team members coordinate their activities in “closed” network configurations by means of mutual links to common prior partners. This concept is related to the idea of embeddedness developed by Mark Granovetter and further defined by Scott Feld as “the extent to which [. . .] individuals relate to the same others” (Feld, 1997: 92). However, while the latter is essentially a tie-based social network construct associated with issues of temporal stability and the development of enforceable norms of behavior in dyads (Coleman, 1988; Granovetter, 1985), our construct of SCE extent is based on shared work experiences—and especially temporary collaborative experiences—rather than stable social relationships. We note that our understanding of the consequences of SCE extent is consistent with the argument developed by Coleman (1988: 107-108) about the collective benefits of social capital produced by closed social structures. For example, in the empirical context of our study, a surgical team will score high on SCE extent if the focal surgeons have operated with many common prior partners across multiple tasks.
While team members establish collaborative ties with multiple partners, they not only construct a social structure that may impact how teamwork is conducted but also tap into task-specific knowledge that may affect how taskwork unfolds. The second dimension—SCE diversity—is associated with this taskwork component, which reflects “what it is that teams are doing” (Marks et al., 2001: 357) bringing team members’ experience and knowledge to bear on task demands. Recognizing that reaching out to multiple partners does not automatically imply access to more diverse task experiences, this construct—defined as the aggregate diversity of task experiences that focal team members have been exposed to through shared collaborative experiences across multiple tasks over time—captures how task experience is distributed within the network that connects current team members to their shared prior partners. Previous research has broadly examined the multidimensional nature of task diversity in organizations (Harrison & Klein, 2007; Mannix & Neale, 2005; Tasheva & Hillman, 2019; van Knippenberg & Schippers, 2007). While diversity is generally conceived in terms of differences between individuals (Lerner & Lomi, 2018), we adopt the more focused notion of diversity as “composition of differences in kind, source, or category of relevant knowledge or experience among unit members” (Harrison & Klein, 2007: 1203). Therefore, SCE diversity captures the aggregate intrapersonal variety (Bunderson & Sutcliffe, 2002; Huckman & Staats, 2011) of the collective experience accumulated by focal team members when collaborating with shared prior partners. For example, in the empirical context of the study, two surgeons who solely conduct the same type of surgery—together with their shared prior partners—are representative of a surgical team with low SCE diversity. Conversely, two surgeons whose aggregate task experience accumulated with their shared prior partners spans across a greater number of surgery types are representative of a surgical team with high SCE diversity.
Because both SCE extent and SCE diversity are defined by looking at the extended network of collaborations with previous partners, they are related but distinct concepts, both theoretically and empirically. A focal team may be highly embedded in closed configurations with multiple common partners, but it may lack overall diversity in task experience. Conversely, a focal team may lack a high number of shared partners, but it may still have a diverse set of task experiences (Lerner & Lomi, 2019). Figure 2 graphically illustrates the two different dimensions of shared collaborative experience.
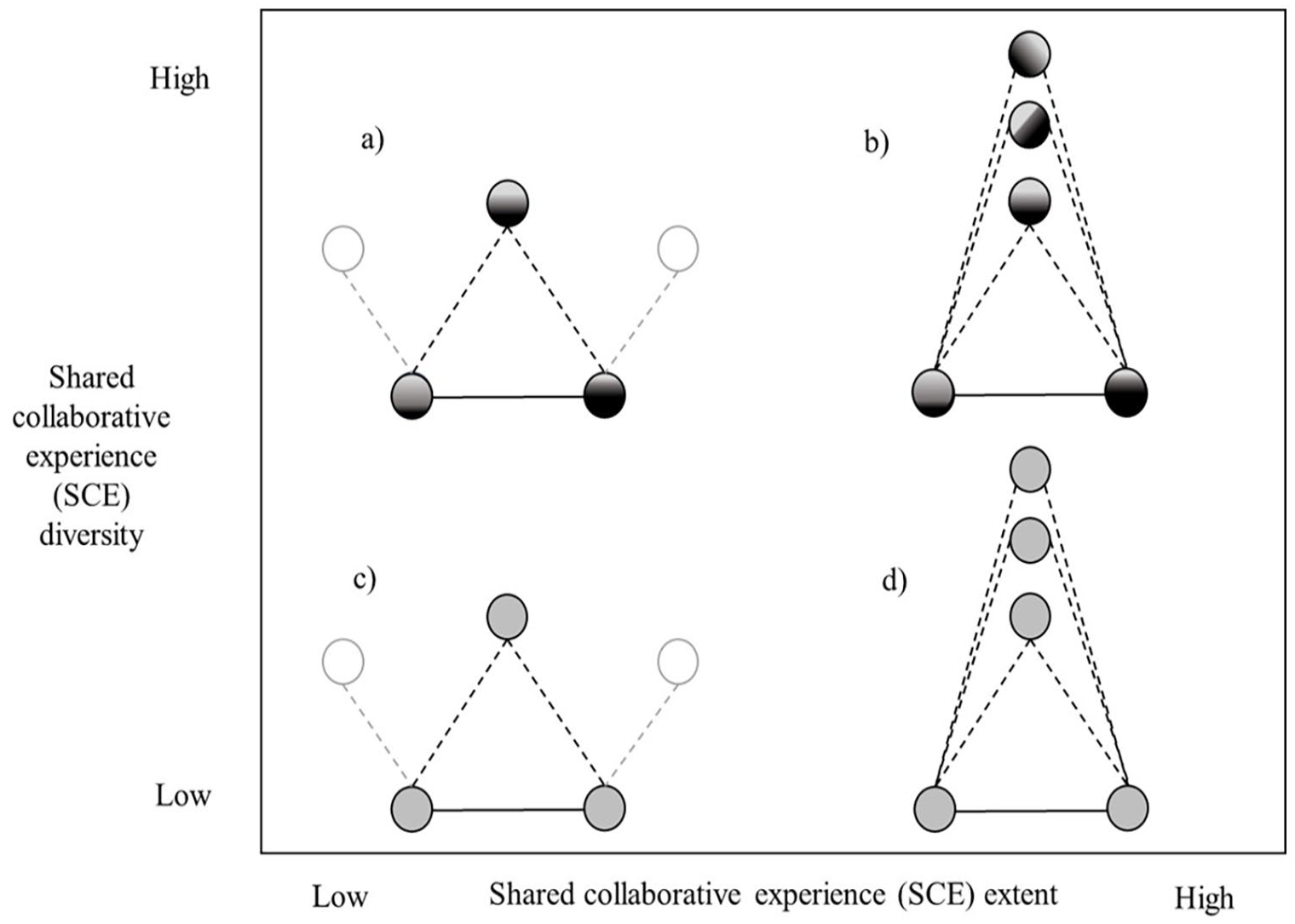
Illustrative Conceptualization of SCE Extent and SCE Diversity
In this figure, all four configurations represent the collaborative experience of focal team members with three different prior partners. Figures 2b and d represent teams with high SCE extent relative to Figures 2a and 2c, as the former have a higher number of shared prior partners than the latter. Figures 2a and 2b represent teams with high SCE diversity, relative to Figures 2c and 2d, as the latter have concentrated their experience in a single task type, while the former have spread their experience more evenly across different task types. As an example, Figure 2d represents a combination of high SCE extent and low SCE diversity: a configuration in which focal team members share collaborative experience with multiple previous partners while always performing tasks of the same type.
Shared Collaborative Experience Extent and Team Performance
We predict that SCE extent will have a positive effect on team performance due to improved teamwork resulting from higher exposure to shared collaborations with the same prior partners (DeChurch & Mesmer-Magnus, 2010; Mohammed, Rico, & Alipour, 2021; van Ginkel & van Knippenberg, 2008). Building on a dynamic view of team process (Marks et al., 2001; Mathieu & Rapp, 2009), or “members’ interdependent acts that convert inputs to outcomes through cognitive, verbal, and behavioral activities directed toward organizing taskwork to achieve collective goals” (Marks et al., 2001: 357), we expect that the extent to which team members leverage the activities by means of interdependent collaborations with their shared prior partners will enhance teamwork through two underlying processes, one occurring during action phases and one occurring during transition phases.
First, we expect SCE extent to increase coordination, or “the process of orchestrating the sequence and timing of interdependent actions” (Marks et al., 2001: 367-68) during action phases because team members experience similar patterns of interaction with shared prior partners. Implicit coordination is generally understood as bearing aspects of anticipation—or “expectations and predictions team members formulate regarding the demands of the task and the actions and needs of others, without being directly notified of these actions” (Rico et al., 2008: 165)—as well as aspects of dynamic adjustment, which entail constant mutual adaptation among team members produced by this anticipation. We argue that SCE extent reflects the tendency of mutual interactions with the same set of prior partners to facilitate the convergence of the team to a common vocabulary and repertoire of actions to align, monitor, and direct the activities of their members. One byproduct of this convergence is that team members are more likely to anticipate their partners’ intentions and are thus better able to coordinate their actions. Luciano et al. (2018) observed a similar dynamic of synchronization in teams with a high level of task-specific (direct) familiarity. We extend this argument to temporary teams with high SCE extent—above and beyond the effect of team familiarity—due to the shared nature of teamwork practices developed within the extended network linking focal team members to shared prior partners.
Second, overlapping collaborative experiences enhance team reflexivity—that is, they facilitate “sharing information and reflecting on experience” (Edmondson, Dillon, & Roloff, 2007: 272) during transition phases. Team reflexivity is understood as a teamwork process occurring during transition phases (Schippers, Edmondson, & West, 2014) whereby team members recollect prior instances of teamwork and reflect on the possibility of altering current routines and activities to improve processes and outcomes (Schippers et al., 2007). In the context of temporary teams, team reflexivity involves individuals who are exposed to collaborative experiences with the same prior partners and thus can bring to a focal team an abundance of shared views and insights from previous task efforts that are resonant with the whole team (Gurtner, Tschan, Semmer, & Nägele, 2007). As action teams’ learning processes may happen across as well as within focal team boundaries (Vashdi et al., 2013), sharing collaborative experience with common prior partners helps focal team members to anchor their representations deriving from action into reflective practices inspired by shared reference points. This process facilitates the convergent recollection of prior teamwork experience, enhances its salience, and assists with the formation of a shared understanding of teamwork-related routines, repertoires, and responses (Konradt, Schippers, Garbers, & Steenfatt, 2015; van Ginkel & van Knippenberg, 2008).
In line with this reasoning, we submit that a higher SCE extent reflects the structural configuration of interactions between members supporting the development of implicit coordination and team reflexivity and ultimately increasing team performance. Specifically, we hypothesize that:
Hypothesis 1 (H1): The extent of shared collaborative experience accumulated by action team members is positively associated with team performance.
Shared Collaborative Experience Diversity and Team Performance
While important, the number of shared prior partners accumulated over time by focal team members is not the only factor affecting the performance of action teams. At least as important is a second dimension of shared collaborative experience—SCE diversity—which reflects the overall composition of task experience accumulated by focal members with shared prior partners over and above the extent of their prior collaborations. Organizational and team scholars have investigated diversity according to several dimensions, including demographic diversity (Reagans & Zuckerman, 2001), functional diversity (Bunderson & Sutcliffe, 2002), cultural diversity (Corritore, Goldberg, & Srivastava, 2020; Wang et al., 2019), and task experience diversity, our focus in this study. Extant research reports mixed evidence on the relation between task experience diversity and team performance (Horwitz & Horwitz, 2007; Lix, Goldberg, Srivastava, & Valentine, 2022; Tasheva & Hillman, 2019; van Knippenberg & Schippers, 2007). A general argument undergirding the expectation that diversity will be beneficial to team performance is rooted in theories of human information processing, highlighting the performance benefits of access to a broader range of prior experiences and unique perspectives (Huckman & Staats, 2011). A countervailing view is rooted in theories of shared cognition and representational gaps (Cannon-Bowers et al., 1993; Cronin & Weingart, 2007), which submit that knowledge diversity within teams may impair performance due to a general lack of common ground (Mannix & Neale, 2005). This view suggests that team coordination is hindered due to the emergence of representational gaps (Cronin & Weingart, 2007) and the inability to form shared understandings or defined courses of action for specific tasks (Boh, Slaughter, & Espinosa, 2007).
Against the backdrop of this debate, in this work we draw on—and further develop—a dynamic view of team processes (Mathieu & Rapp, 2009) to clarify how high levels of SCE diversity may negatively affect team effectiveness in tasks that involve a high level of interdependence, like the ones we analyze in this study. During action phases, taskwork consists primarily of reactive strategy adjustments that are made spontaneously by team members as they interact with each other and adapt to the task environment in real-time. As team members are constantly required to adjust to each other’s actions, we hypothesize that SCE diversity will hinder processes of shared understanding of the task requirements (Cannon-Bowers et al., 1993), trigger representational gaps (Cronin & Weingart, 2007), and be negatively associated with team performance. The real-time processing of diverse experiences accumulated with previous partners requires higher cognitive costs, thus increasing the level of complexity in integrating diverse views and the interpretive ambiguity that team members must manage (Argote & McGrath, 1993; Kilduff et al., 2000). Thus, diverse experiences can hinder group performance during action phases and create problems due to gaps in shared representations of the task at hand and a lack of common ground (Boh et al., 2007; Cronin & Weingart, 2007; Edmondson & Harvey, 2018). In contrast, when teams share a common repertoire of experiences they rely on common language, cues, and symbols that form the basis for teams to function as a “collective mind” (Weick, 1979; Weick & Roberts, 1993).
While action team members react and adapt to the task environment in real-time during action phases, during transition phases, they make deliberate task plans that are developed prior to engagement in the task environment. We posit that higher levels of SCE diversity—that is, greater diversity in team members’ task experience across many types of tasks—are associated with a team’s inability to reap the benefits of group specialization (Crawford & LePine, 2013). Existing research shows that specialized groups are better at developing and articulating “performance strategies” (Mathieu & Rapp, 2009)—that is, coherent plans for achieving task-related goals that are developed during transition phases. Consequently, we argue that high heterogeneity in task experience profiles may complicate the development of coherent performance strategies. Because temporary teams learn through practices that require reflection on previous activities with previous partners (Vashdi et al., 2013), when these activities are heterogeneous, teams may have difficulty agreeing on a coherent course of action that is consistent with task demands. Lack of coherence may result in plans that are inconsistent or full of contingencies, which increases the cognitive costs required for their adoption and implementation (Mathieu & Rapp, 2009). As noted by Crawford and LePine (2013: 40), “the existence of separate thought worlds in the same team can lead to different mental models and a failure to converge on a common set of assumptions about the problems facing the whole team or a shared interpretation of how they should go about solving those problems.” Therefore, we expect that teams with high SCE diversity will be associated with higher task completion times and thus lower performance.
Hypothesis 2 (H2): The diversity of shared collaborative experience accumulated by action team members is negatively associated with team performance.
The Contingent Role of Task Complexity
We have argued that high SCE extent and low SCE diversity benefit action teams by providing the organized knowledge structure that supports smooth team functioning through enhanced teamwork and taskwork processes. However, in line with recent studies on the contextual and contingent effects of shared team experiences on team effectiveness (Avgerinos et al., 2020; Ching et al., 2021; Luciano et al., 2018), we also examine the role of task complexity as a crucial boundary condition within which SCE is likely to operate. Extant research on team processes shows that team functioning is contingent on task complexity, as it affects both teamwork and taskwork (Cannon-Bowers et al., 1993; Crawford & LePine, 2013).
Following closely related studies (Aksin et al., 2021; Luciano et al., 2018), we expect task complexity to be a significant contingency factor in determining when the benefits of social sharedness for team performance are more likely to dissipate—and possibly even turn into liabilities. We draw on existing research (Rico et al., 2008; Vashdi et al., 2013) to conceptualize task complexity along a spectrum where complex tasks contain elements of uncertainty and unpredictability and require explicit processing of multiple informational cues to be successfully managed. Almost by definition, routine tasks tend to be predictable and easily managed through standardized and automated procedures (Weingart, 1992; Wood, 1986; Xiao, Hunter, Mackenzie, Jefferies, Horst, & Group, 1996).
We expect task complexity to moderate the relationship between SCE extent and performance because task complexity reflects a condition under which implicit coordination may pose problems for effective team functioning. Task complexity makes partners’ actions more difficult to anticipate. Uncertain, nonroutine tasks demand increased attention from team members and may require explicit coordination, such as active information seeking, open discussions, and prolonged negotiations (Rico et al., 2008). Insofar as SCE extent is instead associated with reliance on implicit coordination and automatized routines from team members, and that implicit coordination may lead to excessive complacency between team members (Luciano et al., 2018), we may expect that this complacency generated by higher levels of SCE extent will reduce the team’s vigilance, which is crucial for handling complex tasks. This complacency ultimately increases the time needed by team members to adjust to difficult task requirements. Extant research on action teams indicates that as tasks become more complex, teams that rely on more explicit forms of coordination are better able to generate effective responses to unexpected demands than teams that rely on automated responses and shared tacit knowledge (Edmondson, 2003; Xiao et al., 1996). Therefore, we hypothesize:
Hypothesis 3a (H3a): Task complexity attenuates the positive relationship between the extent of shared collaborative experience and team performance. More specifically, the positive relationship between SCE extent and performance will be weaker for more complex tasks.
We also expect task complexity to mitigate the negative relationship between SCE diversity and team performance. Previous research has shown that when teams operate in contexts characterized by uncertain tasks, the specialization induced by a narrower focus on homogeneous tasks becomes less valuable (Ching et al., 2021; Reagans, Miron-Spektor, & Argote, 2016). A broad repertoire of task-based experiences may provide appropriate solutions for tasks that defy easy categorization, or “ideational tasks” (Lix et al., 2022). Diversity of experience in this type of task will provide team members with new ways of interpreting the task demands and allow them to recombine ideas in ways that produce effective solutions. As Kilduff et al. (2000: 23) suggest, the presence of “multiple interpretations in teams is critical for registering complex environments.” Complex tasks may then require a broader repertoire of strategies to draw upon, a concept represented by team members having access to highly diverse shared collaborative experiences. The following hypothesis summarizes our argument:
Hypothesis 3b (H3b): Task complexity mitigates the negative relationship between the diversity of shared collaborative experience and team performance. More specifically, the negative relationship between SCE diversity and performance will be weaker for more complex tasks.
In the empirical part of the paper that follows, we investigate how shared collaborative experience affects the performance of surgical teams involved in robot-assisted surgery operations at a leading European private university hospital. The setting is particularly useful for addressing the theoretical issues that inspire the study because (i) surgeons are recombined into different teams depending on the task at hand, making surgical teams an almost archetypical example of action teams (Edmondson, 2003; Vashdi et al., 2013), and (ii) variations in surgical team performance over time can be measured with considerable accuracy (Pisano, Bohmer, & Edmondson, 2001). As we shall see, this is particularly the case for robot-assisted surgery where operational performance is recorded automatically.
Research Design
Setting
We examine the performance of surgical teams in operations performed using an innovative robotic technology, the da Vinci® Surgical System. Robot-assisted surgery (RAS) is a minimally invasive surgical technology that has gradually gained prominence in the surgical sciences (Hockstein, Gourin, Faust, & Terris, 2007) and is currently attracting considerable popular interest (Max, 2019) and attention from management scholars (Compagni, Mele, & Ravasi, 2015; Iacopino, Mascia, & Cicchetti, 2018; Sergeeva, Faraj, & Huysman, 2020). 1 Since its FDA approval in 2000, RAS has disrupted established work routines, procedures, and flows in operating rooms (ORs) around the world. Despite the significant investment required to acquire the technology (approximately $2.5 million USD), RAS spread rapidly and is now widely accepted as the standard, particularly among gynecologic and urologic surgeons (Singer, 2010).
Two surgeons, identified as main and assistant surgeons, are needed to perform surgical procedures with the da Vinci® robot. Also present in the operating room are an anesthesiologist who is responsible for sedating the patient, a scrub nurse assisting the two surgeons, and a circulating nurse responsible for providing additional support as needed. The lead surgeon and assistant surgeon are located in different areas of the OR with respect to the machine and the patient. The main surgeon stands at a console and views high-resolution 3D images of the patient’s anatomy. Using joysticks and pedals, the main (human) surgeon transmits movements to the arms of the robotic system, which then executes the instructions on the patient. The vision system includes a high-definition 3D endoscope and image processing equipment. The assistant surgeon works close to the operating table and is responsible for the correct positioning and function of the robot’s four arms and endoscopic cameras. The assistant also uses a laparoscopic device to keep the field clear or to help retract tissue while helping the main surgeon better understand what is happening on the operating table. The technology-induced spatial arrangement has important implications for the interdependence and communication between the two surgeons. Given the physical, technological, and sensory barriers in the operating room (Catchpole et al., 2019), the main surgeon is highly dependent on the feedback and stimuli provided by the assistant surgeon (Tiferes et al., 2019). The main surgeon is in a nonsterile field and cannot directly see or touch the patient and therefore relies on the activities performed by the assistant surgeon (Lai & Entin, 2005), who is fully responsible for the laparoscopic steps of the robotic procedure (Sgarbura & Vasilescu, 2010).
To improve our understanding of the technical characteristics of the da Vinci® surgical system and the dynamics of team member interactions during surgical procedures, we negotiated access to the operating theater to observe robot-assisted surgeries directly. Participant observation revealed that despite—or perhaps because of—the physical separation between surgeons imposed by technology, they engaged in intensive and frequent verbal and nonverbal communication during surgical procedures, signaling a high degree of interaction and interdependence as described by Pallotti, Weldon, and Lomi (2022). Our direct observations also clarified the role of support staff in the context of the overall surgical procedure. We observed that while surgeons constitute the strategic core role (Humphrey, Morgeson, & Mannor, 2009; Summers, Humphrey, & Ferris, 2012) responsible for the operational performance of the surgery between the first cut and the last suture on the patient, scrub nurses and anesthesiologists contribute to the surgery mainly by preparing the room for the next operation and managing the process of getting the patient in and out of the room.
Sample and Data
A leading private university hospital in southern Europe provides the empirical opportunity to test the value of the theoretical arguments. The hospital is organized into more than 100 clinical wards with a total capacity of approximately 1500 beds. The hospital community includes more than 4000 members, including physicians, paramedics, nurses, and other health professionals.
Surgical teams are assembled by the directors of the clinical units responsible for specific surgeries. The directors of the clinical units discuss the assignment of surgeons to surgeries among the candidates. The final assignment decision reflects the availability of both technological and human resources, as well as the planned flow of surgeries. For each operation, the main surgeon selects the assistant surgeon. The selection of anesthesiologists and nurses depends on work shifts organized at the ward level, room availability, and more general coordination issues that are not directly related to the specific patient. Nurses work in shifts and are assigned to the OR, not specifically to the surgical team. Approximately 20 RAS nurses are available and work in 8-hour shifts. Unlike nurses, anesthesiologists do not receive specific training in RAS. Their participation is organized around the general flow of surgeries in the hospital.
We collected data on every single RAS operation performed at our research site since the introduction of the da Vinci® technology, from October 2012 to September 2016. This design allowed us to capture the entire history of adoption within the organization and observe the performance of surgical teams from the crucial early period of RAS adoption through the diffusion of experience and eventual routinization. By 2017, experience with the RAS was widespread within the hospital and the device was operating at full capacity. Throughout the observation period, the control software system of the da Vinci® robot recorded data on the duration of each procedure and all information on the surgeons performing the surgeries. We had direct access to the information contained in the database, which we supplemented with data extracted from hospital records about patients and surgeons. The database contains information on daily surgeries, along with a qualitative description of the type of surgery and its classification according to the International Classification of Diseases (ICD-9-CM) and Diagnosed Related Grouping (DRGs) classification systems. In addition, the database contains information about the surgical team involved in each surgery.
Specific time information recorded by the robotic system includes (i) “check-in time,” which indicates when the patient arrives at the surgical facility; (ii) “room-in time,” which indicates when the patient enters the OR for surgery; (iii) “first cut time,” which is performed by the surgeon; (iv) “final suture time,” which indicates when the procedure is completed; and (v) “room-out time,” which indicates when the patient leaves the OR. Our team performance measure is based on this precise timing information.
During the observation period, 114 surgeons were involved in 1671 RAS procedures, which can be grouped into seventeen clinical categories or “types” based on their ICD9-CM codes. 2 Among these categories, hysterectomy and prostatectomy are the most common in our sample, accounting for more than 52% of the cases combined. From the original database, we dropped 328 observations for which we lacked information on the identity of the main or assistant surgeon or the type of surgery performed. The final dataset included 1343 surgeries performed by 106 surgeons between 2012 and 2016. Surgery time was always recorded for each surgery in our sample, but observations are considered incomplete if surgeries are not explicitly associated with a main and an assistant surgeon. A two-tailed t-test was performed to ensure that our dependent variable—surgery time—does not differ significantly due to the drop of incomplete observations (t = 1.3728, p-value = 0.1699). Therefore, we conclude that the surgery time of the two samples being compared (i.e., complete and incomplete observations) are drawn from the same population of surgeries and that we do not incur a significant sampling bias by dropping incomplete observations.
During the first 12 months after adoption, a total of 204 surgeries were performed (1.17 per day, average surgery time: 245.55 minutes). During the last 12 months of observation, a total of 412 procedures were performed, or 1.88 procedures per day (average surgery time: 188.57 minutes). As the OR can be used for eight hours per working day, this figure represents the full capacity of the technology. Thus, the observation period of the study covers the complete cycle of knowledge development, accumulation, and routinization triggered by the introduction of the new robot-assisted surgery technology.
Finally, with the goal of illustrating the logic behind our hypotheses and possibly revealing interesting aspects of the underlying mechanisms, we conducted an exploratory qualitative study by collecting data in the form of semi-structured interviews and direct participant observation of several robot-assisted surgeries. As part of this additional analysis, we conducted 21 semi-structured interviews with key informants (i.e., surgeons involved in RAS operations) and participant observation for a total of 20 hours. Both the interviews and the direct observations of surgical procedures were conducted between September and October 2023. The interviews included in-depth discussions with surgeons to place our statistical findings in the context of their own understanding of the technology and their work. As in previous studies of shared team experience (e.g., Luciano et al., 2018), our goal is to uncover the phenomenology behind the statistical estimates reported and discussed in the quantitative part of the study.
Variables and Measures
Team performance
We use surgery time to measure team performance. We define surgery time for an operation on the ith patient as the time, expressed in minutes, between the first surgical incision and the last suture performed on the patient. This time measure focuses on the duration of the surgery from skin incision to skin suturing and does not include the time prior to the first incision (e.g., time to prepare and anesthetize the patient) or the time from the last suture to the time the patient leaves the OR (e.g., anesthesia recovery time). For similar surgical procedures, the shorter the time of the procedure, the better the performance of the surgical team. We use this operational measure of team performance for several reasons. Surgery time has been routinely used as a proxy for team productivity in the context of surgical teams (Avgerinos et al., 2020; Reagans et al., 2005). Although several different performance measures are available for surgical teams (Hull, Arora, Aggarwal, Darzi, Vincent, & Sevdalis, 2012), procedure completion time is adopted as a technical operational performance measure to capture differences in surgical team knowledge, skills, and abilities across otherwise comparable surgical procedures (O’Connor, Schwaitzberg, & Cao, 2008; Reagans et al., 2005). Surgery time is one of the most critical primary perioperative outcomes, especially in RAS (Talamini, Chapman, Horgan, Melvin, & Academic Robotics Group, 2003).
Surgery time has been widely used in prior research as a measure of both productivity and quality of health outcomes. Faster completion of surgeries indicates that the surgery went well, without complications and errors, as it generally reduces the risk of infection and thus improves the quality of patient outcomes (Katz et al., 2001; Pisano et al., 2001). This is especially true for routine procedures—or procedures where there is relatively little uncertainty about the patient’s condition. This is the typical case for RAS. It has also been shown that the efficiency with which surgeons perform their tasks is significantly associated with the speed of patient recovery and the timeliness of discharge (Catchpole, Mishra, Handa, & McCullock, 2008). The use of other outcome measures, such as mortality or readmissions for surgical complications, does not seem appropriate in our setting. Death is very rare in robot-assisted surgery because the clinical conditions affecting the patients for which it is used normally do not lead to death. Readmissions, although of interest, would pose several problems in our case because complications often occur long after the initial surgery, and follow-up procedures can be treated at another hospital (Ramdas, Saleh, Stern, & Liud, 2018).
In addition, surgery time accurately captures team performance in our context as it takes into account the duration of surgical tasks that are predominantly performed by the two surgeons, thus excluding the time for other activities before the incision or after the final suture in which other clinicians (i.e., the anesthesiologist and nurses) are also involved. Finally, surgery time is the performance metric routinely used by hospitals adopting RAS for the evaluation of the effectiveness of robot-assisted surgery vis-à-vis traditional surgery (Iacopino et al., 2018).
Shared collaborative experience
The main covariates of theoretical interest are shared collaborative experience extent (SCE extent) and shared collaborative experience diversity (SCE diversity). We define them by taking into account information on the sequence of surgeries performed during the observation period. SCE extent for the focal team is defined as the number of surgeons who have worked in the past with both the main surgeon and the assistant surgeon of the focal operation—that is, the number of shared prior partners. We expect that, all else equal, SCE extent will be positively associated with team operative performance (i.e., negatively associated with task completion time). SCE diversity captures the diversity of task experiences that focal team members have access to through their collaboration with shared prior partners. Consistent with prior work on knowledge-based functional diversity (Bunderson & Sutcliffe, 2002; Huckman & Staats, 2011), we conceptualize SCE diversity in terms of experience diversity (Harrison & Klein, 2007). For each team associated with each focal surgery, we reconstruct the full portfolios of experiences that the surgeons developed by working with their common prior partners from the beginning of the observation period to the focal surgery event. These portfolios are vectors composed of seventeen items corresponding to the seventeen different types of procedures, with cumulative counts of surgeries in each specific category, and thus represent the complete record of the surgeons’ composition of experiences accumulated with their common partners up to the focal event. We then aggregate these portfolios at the team level to account for the total experience that team members have access to through their shared collaborative experience and compute the Blau index of variety using the aggregated vector of experiences (Blau, 1977; Harrison & Klein, 2007). The resulting formula is equal to
Task complexity
Task complexity captures the severity of the patient’s clinical condition at the time of surgery and is used to examine how the complexity of the surgical procedure moderates the relationship between shared collaborative experience and team performance. We measure task complexity as the DRG value (in euros) associated with the patient case. The DRG system is an internationally adopted standard costing system used to calculate the cost of medical and clinical services provided to hospitalized patients. DRGs, which are used to determine government reimbursement for hospital care, assign specific codes to groups of patients who receive the same type and amount of care provided by the same specialized personnel using the same type of equipment. Codes are assigned based on specific diagnostic procedures performed on admitted patients. The DRG value reflects the level of complexity and resource absorption associated with a patient as more complex cases are associated with higher treatment costs (Aronow, 1988; Lefèvre, Reboul-Marty, de Vaugrigneuse, & Zeitoun, 2017; Sundaresan, Boysen, & Nerkar, 2023).
Control variables
Our model includes covariates to control for characteristics of (i) individual team members, (ii) teams, and (iii) individual surgeries that may influence the performance of surgical teams and may be related to confounding factors associated with team composition (Avgerinos et al., 2020; Huckman & Staats, 2011; Luciano et al., 2018; Reagans et al., 2005). We include the variables past performance of main surgeon and past performance of assistant surgeon as proxies that capture a surgeon’s ability in the OR. The measure is constructed as the total time gain (or loss) that a surgeon accumulated over time while performing in the operating room, relative to the predicted operating times. To compute this measure, we took—for each surgery—the difference between actual surgery time and predicted surgery time (from our full regression model) and then aggregated the differences over time up to the focal surgery. We also include task experience of main surgeon and task experience of assistant surgeon, measured as the cumulative number of surgical procedures of the same type as the focal procedure performed by the main and assistant surgeons prior to the focal procedure, to control for the dynamics of experiential learning. Team familiarity measures repeated collaboration between the main and assistant surgeons and is intended to control for vicarious learning and enhanced coordination effects (Argote, Ingram, Levine, & Moreland, 2000). It is measured as the number of joint surgical procedures performed by the same two surgeons prior to the focal procedure (Espinosa et al., 2007; Huckman & Staats, 2011; Reagans et al., 2005), capturing how many times the main surgeon chose the assistant surgeon in the past. We include the variable prior partner exposure to control for total exposure to prior partners (Aksin et al., 2021; Kim et al., 2023) so that the extent of SCE is estimated beyond team familiarity and exposure to prior partners. We also include team diversity and prior partner diversity, which consider the experience diversity that characterizes focal team members and the experience diversity of all their prior partners (excluding common partners). Like our approach to measuring SCE extent, these variables are included in the model to test the effect of SCE diversity over and above task experience diversity measured at different levels. Finally, we include room preparation time as a proxy for the role of ancillary staff in the OR, captured by total pre- and post-operative preparation time. To the extent that efficient support staff requires less time on average to prepare the room for surgery (Weinbroum, Ekstein, & Ezri, 2003), and that efficient support staff may help surgeons perform better in the OR (Cassera, Zheng, Martinec, Dunst, & Swanström, 2009), this variable may be considered as a statistical control for the contribution of support staff to the operational performance of the surgical team.
Analytical Strategy
The data analyzed in the empirical part of the study are constructed following an event-based design to account for the fact that, for each surgeon, the stock of accumulated experience changes after each surgery, and teams are constantly assembled and disassembled around contingent tasks, and surgeons are constantly reassigned to different teams. Unlike a panel design, which requires temporal aggregation of events at arbitrary points in time, an event-based design allows us to capture fluid temporal dynamics at a very fine-grained level (Bianchi & Lomi, 2023; Pallotti et al., 2022). For each observation, we update each time-varying variable included in the model (predictors as well as covariates) at the time of the focal surgery by computing covariates using a subset of the dataset trimmed prior to the focal surgery. For each surgery, we focus on the time elapsed between the first surgical cut and the final suture (i.e., “surgery time”) as our main operational measure of team performance. Consistent with previous studies that have examined the effect of experience on surgery time (e.g., Aksin et al., 2021; Edmondson, 2003; Reagans et al., 2005), we employ ordinary least squares (OLS) regression models with a log-linear specification. We also use a log-transformed dependent variable to adjust for its slightly right-skewed distribution, which approximates a normal distribution after the logarithmic transformation. To account for the lack of independence across observations that is typical of dyadic data, we follow an approach developed by Cameron, Gelbach, and Miller (2011) and widely used in empirical studies of organizational networks (e.g., Clough & Piezunka, 2020; Dahlander & McFarland, 2013) that extends the clustering of Hubert-White robust standard errors to more than one variable. Because our data include surgeries performed by teams composed of main and assistant surgeons, we report two-way clustered standard errors computed around both surgeons in our estimates. 4 To account for inherent differences and unobserved heterogeneity across surgery types and years, we include 17 individual dummy variables at the surgery type level and 4 dummy variables at the year level that act as (unconditional) fixed effects. Finally, we standardize our variables to facilitate the comparison of estimates across models.
Results
Hypotheses Testing
Table 1 presents descriptive statistics and correlation coefficients for all variables used in the analysis.
Descriptive Statistics and Pairwise Pearson Correlations among Variables
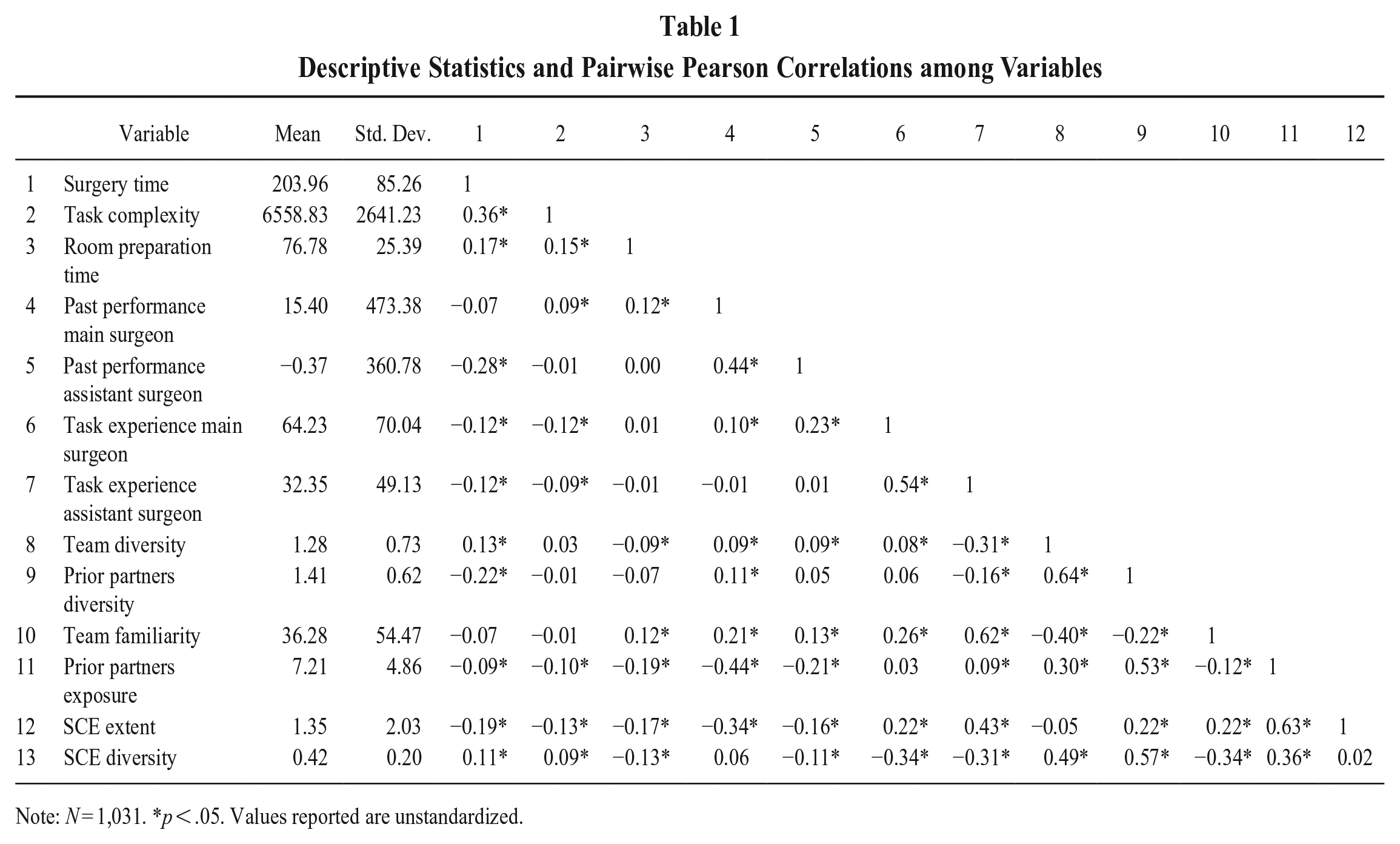
Note: N = 1,031. *p < .05. Values reported are unstandardized.
Given the interdependent nature of our measures, we report moderately high correlations between variables associated with structural features of shared team experiences (such as prior partners exposure and SCE extent) as well as between variables associated with the variety of task experiences at different levels of analysis (such as team diversity, prior partner diversity, and SCE diversity) because surgeons with similar task experience profiles tend to operate together. We further note moderately high correlations between characteristics of main and assistant surgeons (such as past performance and task experience) indicating the tendency of surgeons to collaborate repeatedly over time. Finally, the correlation between SCE extent and SCE diversity indicates a moderate tendency of network configurations linking focal team members to shared partners to encompass a broader variety of task experiences. 5
Table 2 reports the results from a series of pooled OLS regression models. 6 Model 1 is the baseline model, which includes all relevant controls and dummy variables for surgery types and years. Model 2 tests H1 by adding SCE extent to Model 1. Model 3 reveals the direct relationship between SCE diversity and team performance, which corresponds to our H2. Model 4 tests H1 and H2 simultaneously. Models 5 and 6 test H3a and H3b by introducing the interaction terms between our main predictors and task complexity. Finally, Model 7 represents our full model as it includes all individual dummies, controls, main predictors, and both interaction effects. Given our measure of team performance as surgery time, a negative parameter estimate will be associated with a variable having a positive effect on team performance, while a negative effect is associated with a decrease in task completion time and, hence, an increase in performance.
OLS Estimates of Surgery Time (Logged)
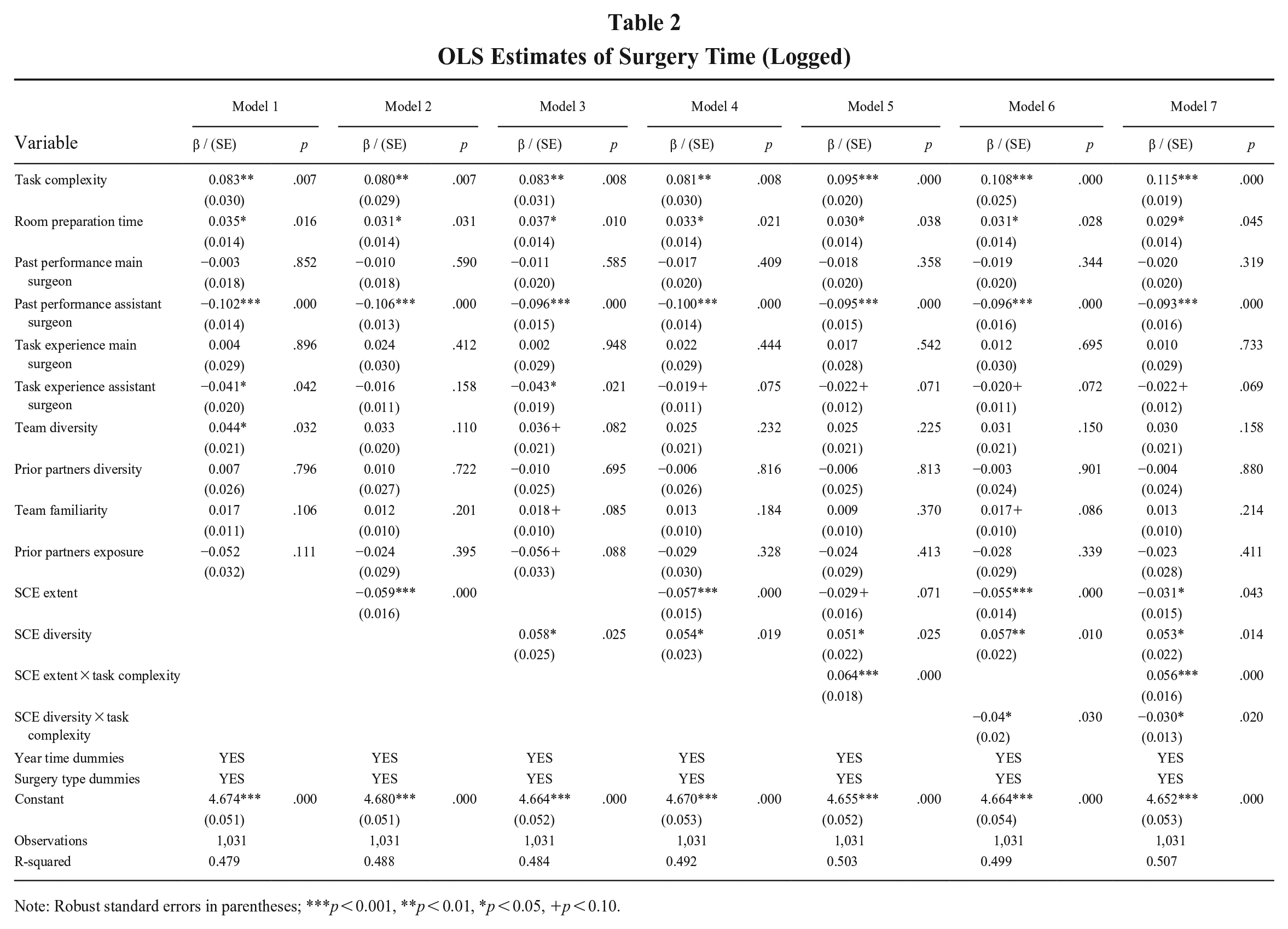
Note: Robust standard errors in parentheses; ***p < 0.001, **p < 0.01, *p < 0.05, +p < 0.10.
We first control for a series of individual and surgery type–level factors that can affect operational performance. As expected, task complexity is positively associated with surgery time, such that an increase of one standard deviation in DRG value (equal to 2641.23 euros) is associated with an increase of [exp(0.083)-1] = 8.65% in surgery time (equal to 17′40″ for the average surgery). This result indicates that complex cases—cases associated with patients’ conditions requiring higher levels of resource absorption as revealed by a higher assigned DRG value—require a longer time in the OR. We find a positive and significant effect—albeit smaller—for room preparation time, our statistical control for the effect of quality of supporting staff on surgery time. Interestingly, both past performance of main surgeon and past performance of assistant surgeon have negative coefficients (i.e., a positive effect on team performance), although only the latter is statistically significant, indicating that surgery time decreases when operations are performed by assistant surgeons who tend to outperform the predicted surgery times. While we find no significant impact of task experience of main surgeon on surgery time, we do report a negative and marginally significant coefficient for task experience of assistant surgeon. Finally, in our sample, neither team familiarity nor prior partner exposure are associated with statistically significant variations in surgery times.
Hypothesis 1 predicts that teams with a large SCE extent (i.e., teams where members share a high number of prior partners) will perform better than teams whose members share fewer common partners. Considering that the duration of an average surgery is almost 204 minutes, with a minimum of 29 and a maximum of 661 minutes, Model 2 shows that—for a typical surgery—an increase of one standard deviation in SCE extent (i.e., an increase in the number of shared common partners by approximately two units) is associated with a [1-exp(−0.059)] = 5.73 percent decrease in surgery time, which corresponds to approximately 11′41″ for the average surgery. This result is significant (p < .001) over and above alternative explanations, including individual experiential learning as measured by individual task experience, team familiarity, or exposure to prior partners. We performed a likelihood ratio test to check the improvement of Model 2 over the baseline of Model 1 (LR χ2(1) = 17.65, p < .001). Overall, this result supports our first hypothesis.
Hypothesis 2 postulates that the diversity of experience profile of team members and their shared prior partners is associated with a higher surgery time and thus lower team performance. The positive and significant parameter estimate of the SCE diversity variable supports our expectation for H2 (p = .025). Model 3 shows that—other conditions being equal—one standard deviation increase in SCE diversity (i.e., an increase of 0.19 in the Blau index of experience variety that focal team members have access to through their shared collaborative experience) is associated with a [1-exp(0.058)] = 5.97 percent increase of surgery time, which corresponds to approximately 12 minutes for the average surgery. The result is significant above and beyond the focal team and prior partners’ diversity. Our Model 3 significantly improves the baseline of Model 1 (LR χ2(1) = 9.06, p < .01), supporting our second hypothesis.
Hypotheses 3a and 3b predict that task complexity moderates the relationships between SCE and team performance. The positive and significant (p < .001) parameter estimate of the interaction term SCE extent × task complexity supports our prediction for H3a, suggesting that the positive impact of shared prior partners on team performance is weakened by the complexity of executed surgeries. The negative and significant (p = .030) parameter of the interaction term SCE diversity × task complexity supports our prediction for H3b, thereby indicating that the negative effect of the experience diversity that team members have access to through their shared prior partners on team performance is also weakened by the complexity of surgeries executed by the focal team. We note that Model 5 and Model 6 improve over Model 4 (respectively, LR χ2(1) = 22.92, p < .001 and LR χ2(1) = 14.45, p < .001).
To examine in greater detail the regions of significance underlying the moderating variables, we employ the Johnson-Neyman technique for marginal effects (Bauer & Curran, 2005). We plot the marginal effects of the main predictors on the outcome variable by computing the margins at many different small intervals of the moderator rather than at a small number of conventional points (e.g., one standard deviation below and above the mean). Marginal effects plots in Figure 3a and 3b provide information about the slope of the marginal effect line (solid line) and the width of the confidence intervals, which depend on the estimated variances and covariances of the independent variable and the moderator (dotted lines). 7 The 95% confidence intervals around the line describe the regions of significance for the hypothesized interaction effect, indicating the range of the moderator within which the effect is significantly different from zero, at 5% significance level. The gray areas in the plots illustrate the regions of statistical significance for the slope of the independent variable (α = 5%). The vertical dotted lines correspond to the cutoff significance values of the independent variables—that is, values at which the entire confidence band remains entirely above or below the zero.
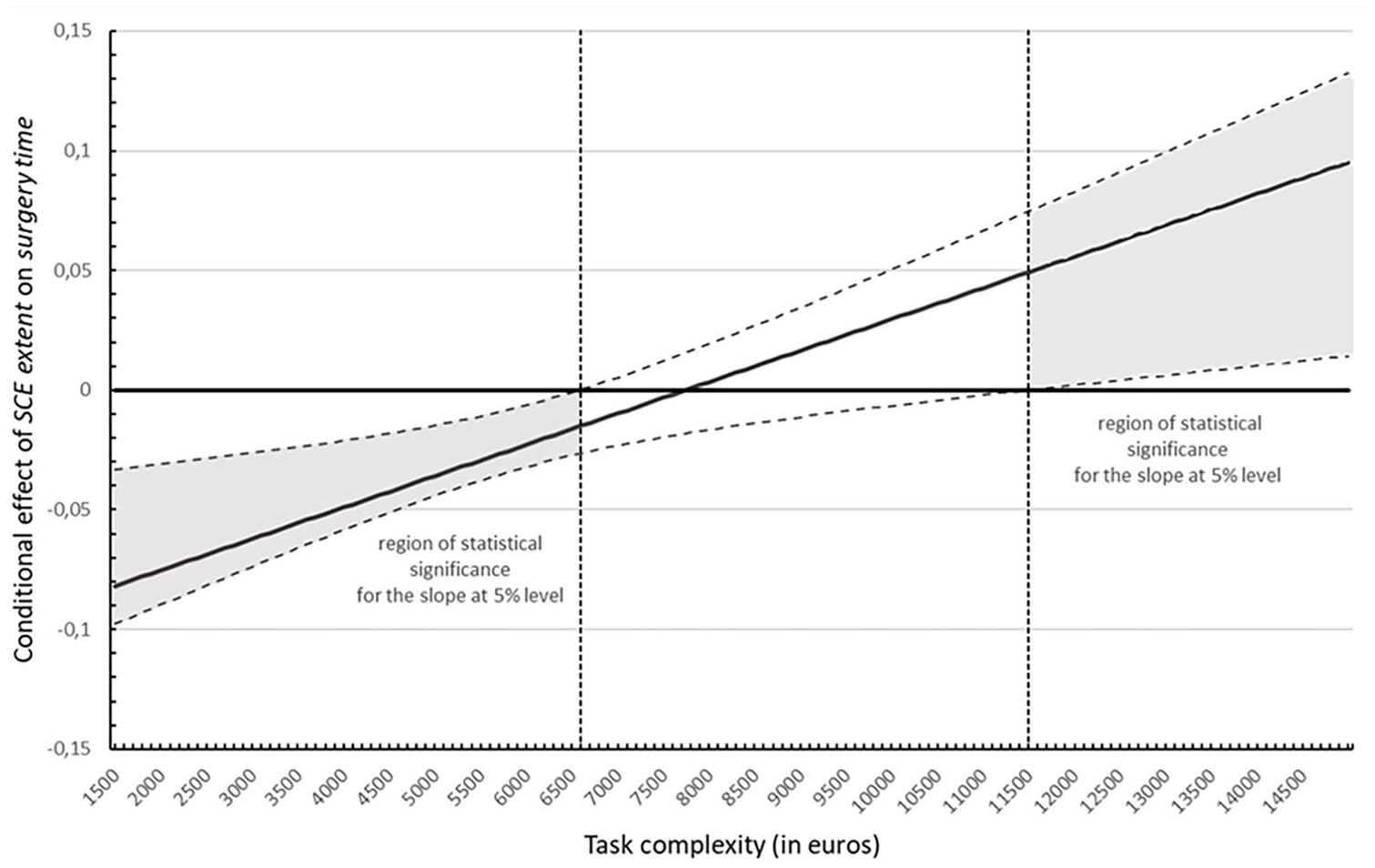
Johnson-Neyman Plot of the Moderating Effect of Task Complexity on the Relationship between SCE Extent and Surgery Time (with 95% Confidence Intervals)
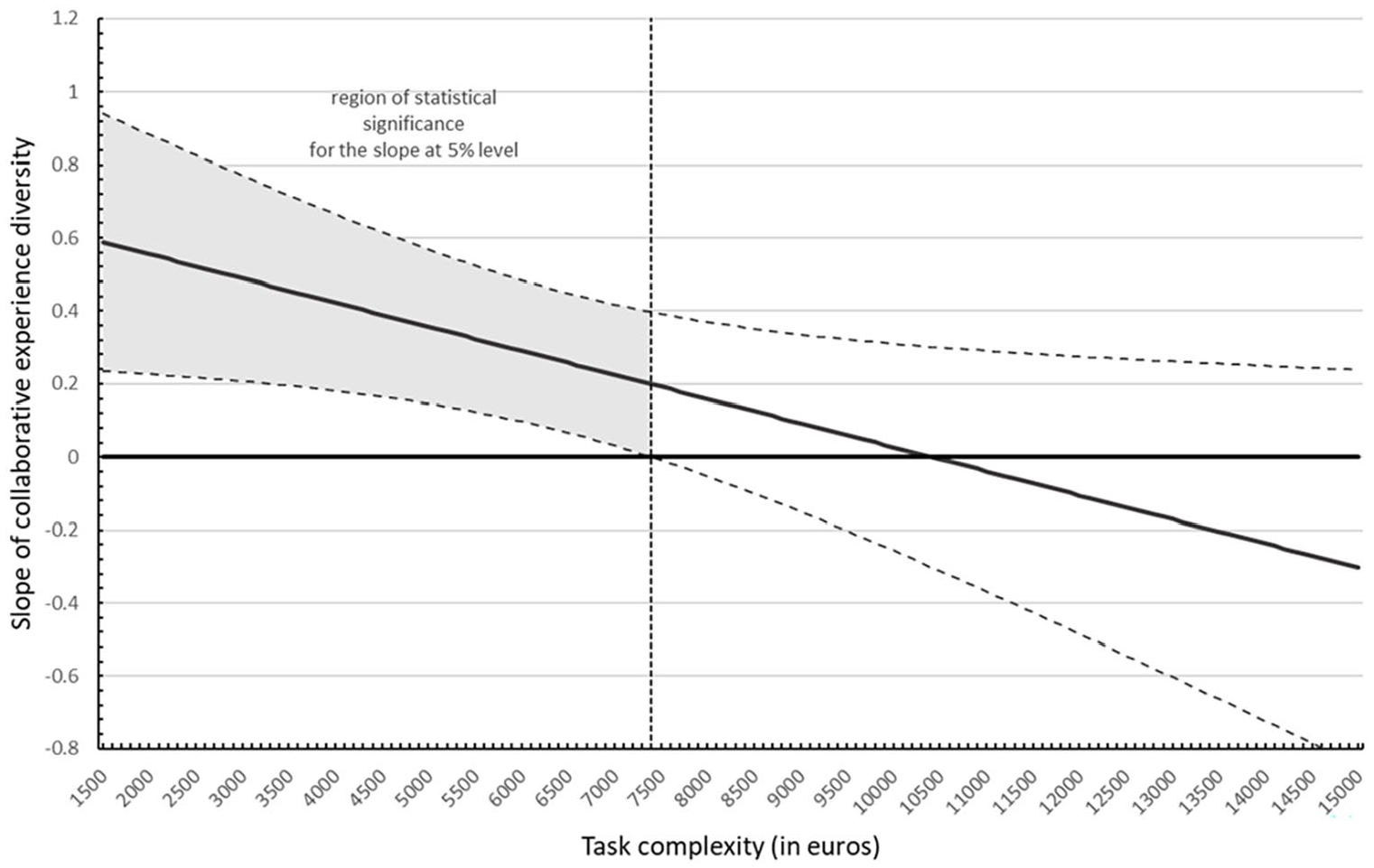
Johnson-Neyman Plot of the Moderating Effect of Task Complexity on the Relationship between SCE Diversity and Surgery Time (with 95% Confidence Intervals)
Our test of the moderation hypothesis between SCE extent and task complexity is summarized in Figure 3a. The horizontal axis represents the different points of the moderator at which the marginal effects were computed (i.e., we selected 100-euro intervals in DRGs between the minimum of 1500 and the maximum of 15000 for the range of task complexity—excluding two outliers—resulting in 136 different points). The vertical axis represents the marginal effect of SCE extent on OR time, conditional on task complexity. The plot shows that the conditional effect of SCE extent on surgery time is negative and statistically significant when the task has a low level of complexity (with the precise cutoff of significance being 6600 euros, which corresponds approximately to the 66th percentile of the DRG). As complexity increases, the effect first becomes insignificant and then becomes positive and significant for extremely high complexity values (i.e., a DRG above 11500 euros, which corresponds to almost the 97th percentile of its distribution). In other words, when tasks are not very complex (i.e., their associated DRG is below the 66th percentile of the observed range), teams whose members share a high degree of prior partners perform better than teams whose members share a lower degree of prior partners, with a range of decrease in surgery time estimated between 1.5% and 7.8% (i.e., approximately 3 to 16 minutes) for each standard deviation increase in SCE extent. However, when tasks are very complex (i.e., have an associated DRG that is around its 97th percentile), teams with high SCE extent tend to perform worse than teams with low SCE extent, suggesting that excessive SCE extent may impair performance when tasks require explicit and complex coordination. Taken together, this evidence supports our hypothesis H3a.
Figure 3b shows the marginal effect of SCE diversity on surgery time, conditional on task complexity. Again, the gray areas in the plot illustrate the range in which the slope of SCE diversity is statistically significant (α = 5%). The plot shows that the conditional effect of SCE diversity on surgery time is positive and statistically significant when the task has a low level of complexity (with the precise cutoff of significance being 7400 euros, which is roughly the 81st percentile of the DRG), indicating that high SCE diversity hurts performance when the task is not very complex. As task complexity increases, the negative relationship between SCE diversity and performance weakens. In contrast to the case of SCE extent, we do not observe a significant change in the sign of the relationship for diversity at very high levels of task complexity. Therefore, we cannot conclude that—within the observed range—teams may benefit from tapping a broader pool of experience for very complex tasks. However, the results support the minimal conclusion that high experience diversity is not detrimental to team performance when tasks are complex.
Qualitative Insights
The results suggested by our statistical analysis demonstrate the existence of relationships between SCE extent, SCE diversity, task complexity, and team performance in the direction we postulated. The additional fieldwork data that we collected allow us to better illustrate the mechanisms underlying these relationships. The goal of our fieldwork was to observe or directly ask the surgeons about actions, behaviors, and practices that support surgical tasks in the operating room. Furthermore, we were able to aggregate and reconnect these practices and behaviors to the processes of teamwork and taskwork that constitute the backbone of our theoretical constructs of (i) SCE extent, (ii) SCE diversity, and (iii) their interaction with task complexity. We refer interested readers to the information on the resulting data structure summarized in Table A1 of online appendix A.
SCE extent
Regarding SCE extent, our results highlight the importance of implicit coordination between surgeons. For example, we report a situation in which surgeons operating in a context characterized by high SCE extent communicate and interact implicitly by waving working instruments to each other as a signal. As a senior urologist explained: “I’m used to coordinat[ing] with [my partners] verbally, but . . . you can also wave the tool you are handling to your partner in a certain way to signal where they have to move quickly to aspirate the blood when needed. . . . If they don’t understand it, you must tell them [explicitly], but this costs more time.” Implicit coordination seems to enable surgeons quickly to update each other and provide partners with relevant information about the task progress. In the words of an expert gynecologist who displayed a high score of SCE extent: “My partner transmits a certain level of reliability that cannot be codified, and we do not need to explicitly communicate what we are going to do next. It is sort of a ‘gut feeling.’ You know at that moment that this person is speaking the same language, so she does everything with much more caution and control. It is a matter of features, gestures, it is an affinity that comes from experience, from working all together as a big team and learning from each other.”
The role of reflexivity in translating SCE extent into team performance also emerged from formal and informal meetings occurring before and after the surgery, which tends to happen more frequently when teams share more partners in common, a configuration labeled by one of the interviewed surgeons with the term “surgical school.” As a senior surgeon explained: “Many of our patients have cancer and for them in our ‘surgical school’ we adopt specific clinical pathways that are shared in the context of multidisciplinary meetings. . . . During these meetings, we discuss such pathways as well as the results of any investigation and clinical data, and then we decide the strategy for the surgery.” Informal debriefings may be held also after surgeries. For example, after a complex prostatectomy, a member of our research team spent one hour in the residents’ room, observing surgeons’ interactions. Once arrived, the main surgeon greeted the residents and commented to the one who served as assistant: “Did you see how badly the patient’s bladder was positioned?!” After that, all surgeons who were present in the room, who also regularly operate together with the main surgeon, joined the discussion about the surgery that was just carried out, considering how to adjust teamwork practices in similar circumstances.
SCE diversity
Our fieldwork also contributes to shed more light on how SCE diversity is converted into team performance. The qualitative evidence we gathered seems to support the negative relationship between diversity and performance in the case of noncomplex tasks. Respondents reported that collaborations with surgeons possessing a more homogenous level of task experience may increase the possibility of establishing common ground and converging to similar representations of the task demands during action and transition phases. As explained by a surgeon we interviewed, “Sharing common surgical experiences can be helpful in reducing the surgery time. If we need to take a certain step that we know well because we both repeatedly have had the same [task] experiences working with others in the past, everything is easier, you know what to do without having to give instructions to each other and you make less mistakes.”
Another important issue emerged during our fieldwork concerning the benefits of deliberate taskwork plans prepared before surgeries associated with groups with specialized task experience, who can more easily match their ability to shared representations of task demands. According to a senior urologist: “Specialization in surgery is used to avoid mistakes, if you have a method that you have experienced several times and the procedure is standardized, you can better prevent troubles. If you work with others having the same knowledge, such specialization makes us understand each other more easily. This doesn’t occur if you work with partners displaying different skills, methods, and approaches.”
Task complexity
Finally, our fieldwork helps illuminate the contingent role that task complexity plays when associated with SCE. Emerging from our qualitative data as a combination of uncertainty and severity in patient’s conditions, task complexity seems to attenuate the relationship between SCE extent and performance as it contributes to decreasing the importance of implicit coordination between team members. A particularly insightful situation emerged during one participant observation. During the intervention, when the main surgeon encountered some critical steps, he started to concentrate more strongly on the surgery, avoiding any verbal and nonverbal communication with the assistant surgeon. Right after the operation, we asked for clarifications about such absence of communication. He told us that during complex surgeries, he tends to speak less, to avoid any distracting issue, and to engage less in any verbal or nonverbal interaction with his assistant surgeon. This testimony revealed a particularly interesting aspect of our story, partly challenging our original expectations, as the main surgeon did not seem to switch from more implicit to more explicit coordination. He is actually engaged in less team coordination overall, taking most of the taskwork upon himself, hence decreasing the relevance of effective teamwork in explaining team performance.
Our fieldwork further illustrates aspects of the relationship between SCE diversity and team performance when tasks are complex. Interviews and observations revealed that, in situations of greater surgical complexity, higher SCE diversity may not be detrimental when dealing with severe and uncertain cases. Diversity in these instances provides the team with a larger pool of potential different solutions to solve less routinary problems. As reported by a thoracic surgeon, “[task experience] diversity may come in handy when patient cases are more complex. If [my partner and I] have worked in the past with others with different skills, we had the chance to see others solving a problem in different ways. In other words, we have more solutions at our disposal.” Being able to access a more diverse repertoire of techniques to solve problems may offset the disadvantage implied by lack of group specialization in situations of higher uncertainty or severity (for instance, in cases of patient co-morbidity) as it broadens the options that surgeons could draw from to complete complex surgical tasks.
Supplementary Analyses
We conducted additional statistical analyses to assess the robustness of our findings to plausible alternative explanations. We focus on three main areas: (i) alternative conceptualizations of shared collaborative experience that may be at play, (ii) possible interaction effects between the teamwork and taskwork components, and (iii) considerations of underlying temporal trends that may confound our results. In all cases, the main substantive patterns of our results remain robust. A full account of the supplementary analyses is available in online appendix B.
Discussion and Conclusions
As organizations increasingly rely on teams characterized by unstable membership to reconfigure individuals around the resolution of transient tasks, researchers and practitioners alike have become increasingly interested in identifying the conditions that sustain collaboration and performance in temporary teams (Mayo, 2022; Valentine & Edmondson, 2015). Our starting point in this paper was the argument proposed by contemporary organizational research on teams that the current understanding of the drivers of effectiveness in traditional teams encircled by stable well-identified boundaries does not extend automatically to action teams with task-dependent boundaries and fluid participation (Tonellato, Tasselli, Conaldi, Lerner, & Lomi, 2024). We identified shared collaborative experience (SCE) extent and diversity as potential factors affecting performance in temporary action teams. While most previous efforts have focused on concurrent overlap in team membership (Mortensen & Hass, 2018; O’Leary, Mortensen, & Woolley, 2011), SCE is based on sequential dynamic interactions that focal team members entertain over time, collaborating with multiple shared partners. Based on a dynamic view of team processes, we have produced statistical results supported by extensive fieldwork showing that action teams associated with higher levels of SCE extent and lower levels of SCE diversity tend to achieve higher levels of operational performance. We have provided clear evidence that task complexity is a statistically significant and substantially important contingency factor affecting team performance. As tasks become more complex, the benefits of high SCE extent diminish and may even reverse to become a liability. As task complexity increases, the negative effect of high SCE diversity on performance also weakens but not enough to reverse the negative relationship between diversity and performance.
Theoretical Contributions
We started our study by observing that what we know about teams in organizations rests on the classic view of social groups as composed of interacting members within clearly defined boundaries (Homans, 1950). How relevant is this time-honored view for our understanding of how teams work and perform in contemporary organizations? Our attempt to address this question in a specific empirical setting allows us to offer at least three broad theoretical contributions to research on team effectiveness within organizations.
First, this study contributes to the debate on the role of shared team experiences in temporary settings subject to frequent reconfigurations (Aksin et al., 2021; Avgerinos et al., 2020; Luciano et al., 2018). Previous studies have questioned the effectiveness of team familiarity, conceptualized as repeated collaboration between members of the same team, in dynamic contexts where team members (Aksin et al., 2021; Avgerinos et al., 2020) and team tasks (Huckman & Staats, 2011; Luciano et al., 2018) are fluid and constantly changing. In general, these conditions require the introduction of stabilizing factors that guarantee effective team functioning despite the constant turnover of individuals and the renewal of tasks (Lomi, Conaldi, & Tonellato, 2012). Consequently, particular attention has been paid to elements of social sharedness (Tindale & Kameda, 2000) that bind individuals into meaningful groupings, for example, by studying the interplay between formal and informal coordination practices (Faraj & Xiao, 2006), role structures (Bechky, 2006; Klein et al., 2006), or team scaffolds (Valentine & Edmondson, 2015). Our study complements and helps articulate these views by proposing a mechanism that extends the notion of shared team experience to the network of shared prior partners in which team members are embedded. In doing so, we respond to calls for the adoption of a network lens in team research (Mohammed et al., 2021; Park, Grosser, Roebuk, & Mathieu, 2020). According to this view: “There are probably lessons to be learned from the network literature and from thinking about team functioning as a series of dyadic exchanges generating network properties” (Mathieu, Maynard, Rapp, & Gilson, 2008: 453). In this study, we examined a fundamental network property generated by a series of dyadic interactions: the degree to which extra-team collaborations are embedded in closed network structures. Taken together, our statistical results provide evidence that team members do not necessarily benefit from repeatedly working with the same partners (i.e., team familiarity) or from always working with different partners (i.e., prior partner exposure) but from sharing collaborative experiences with a network of mutual partners. SCE thus represents a specific type of shared team experience, a “relational” team scaffold (Valentine & Edmondson, 2015), that helps team members coordinate beyond direct team familiarity and prior partners’ exposure (Aksin et al., 2021).
Second, we help reconcile the debate on shared team experiences by advancing a conceptualization of the core construct of SCE along both a team-based as well as a task-based dimension. In doing so, we recognize that “developing a better understanding of the interplay between members’ taskwork and teamwork activities offers great promise for advancing theory and practice concerning current and future team-based organizational designs” (Mathieu & Rapp, 2009: 90). With relatively few notable exceptions (e.g., Crawford & LePine, 2013; Espinosa et al., 2018), the majority of prior studies on shared team experiences focused predominantly on a taskwork dimension, emphasizing the compositional characteristics of the team but neglecting members’ interactions aimed at coordinating and reflecting on taskwork to achieve collective outcomes (Marks et al., 2001). Other studies have focused predominantly on a teamwork dimension, neglecting the multidimensional content of tasks that contribute to variation in members’ experience stocks, and consequently treating team members and their partners as a uniform group of individuals with uniform experience portfolios (e.g., Aksin et al., 2021). Our study helps integrate these prior experiences by explicitly recognizing that members carry both teamwork and taskwork knowledge across different teams and thus understand teams as “multidimensional, fluid entities that need to be treated in a complex, time-dependent fashion” (Hollenbeck, Beersma, & Schouten, 2012; Mathieu et al., 2017: 461). This intuition appears to be consistent with the existing mixed evidence on the effect of prior partner exposure on team performance. For example, Kim et al. (2023) found that in the same temporary teams, attending surgeons’ exposure to multiple nurses increased team performance, whereas nurses’ exposure to multiple attending surgeons instead decreased team performance. While we might expect SCE extent to be constant in these two situations—given the same number of shared prior partners—we might also expect SCE diversity to be significantly different, given a higher expected homogeneity in scrub nurses’ task experience compared to attending surgeons, which may help explain performance differences for the same level of partner exposure. In line with this thinking, we formulated our hypotheses about how two related but distinct dimensions of SCE contribute to explaining team performance (Mohammed et al., 2021).
Finally, heeding the suggestion that “future team researchers should feature task characteristics more prominently than we have in the past” (Mathieu et al., 2017: 461), we extend and test the theory on the contingent role of task complexity for the relationship between SCE and team performance. Our findings add to an existing body of knowledge that views high task complexity as challenging the benefits of team familiarity and other shared team experiences for team performance (Espinosa et al., 2007; Luciano et al., 2018; Vashdi et al., 2013). Complex tasks reveal the limits of excessive embeddedness in clusters of prior partners with homogeneous task experiences. Given the extensive evidence from existing research on the cognitive underpinnings of task complexity (Rico et al., 2008; Xiao et al., 1996), our test of theoretical predictions about the role of task complexity reveals fundamental aspects of the boundary conditions underlying the relationship between SCE and performance. An interesting feature of our results is that—while our theory suggests that complex tasks require more explicit and overt coordination to avoid the dangers typical of excessive complacency (Luciano et al., 2018)—we observed during our fieldwork that surgeons may prefer instead to work in isolation and to focus on their own subtasks, relying on their own expertise and a well-rehearsed system of formal roles and guidelines when making decisions rather than increasing explicit coordination with their teammates. This qualitative evidence seems to suggest that temporary teams rely on different coordination mechanisms at different levels of analysis depending on the specific level of task complexity, as team members may rapidly switch from micro- to meso-level mechanisms, such as team scaffolds (Valentine & Edmondson, 2015) and predefined role structures (Bechky, 2006). Future research could more closely examine the conditions under which teams switch coordination modes to adapt to different levels of task complexity.
Managerial Implications
We believe that our findings have clear relevance for managers involved in team assembly strategies—that is, strategies for staffing high-performing teams (Twyman & Contractor, 2019). Previous research has offered contrasting recommendations for staffing strategies in contexts where teams are dynamically assembled around the performance of contingent tasks. One perspective identifies team familiarity as the ideal team assembly strategy, inviting managers to staff teams that privilege repeated patterns of interactions among team members over time. A rival perspective suggests that team formation strategies that promote greater exposure to previous partners would outperform those that promote team familiarity (Aksin et al., 2021). Our results reconcile these two seemingly incompatible perspectives, highlighting the possibility that managers may be able to balance the positive effects of exposure to prior partners and those of team familiarity by considering a team’s shared collaborative experience. Team-building strategies could leverage prior partner exposure while preserving a sense of commonality through a kind of “indirect familiarity” between focal team members connected through their common partners. On the one hand, our results suggest that when the focal task doesn’t have a high level of complexity, managers would be better off staffing action teams to maximize the amount of shared collaborative experience—by facilitating collaboration among individuals who share a high number of prior partners. On the other hand, when the focal task involves higher levels of complexity, managers responsible for implementing human resource strategies should also consider the extent to which shared prior partners allow focal team members to tap into more diverse experiences, insofar as these experiences provide a repertoire of potentially useful strategies for adapting to heterogeneous task demands. For temporary teams, similarity, competence, and familiarity are no longer the only criteria for assembling a high-performing team (Hinds, Carley, Krackhardt, & Wholey, 2000). Equally important are the experiences that team members have developed and accumulated by interacting with other organizational participants across multiple prior teams. In this study, we argued and demonstrated that these experiences are particularly consequential for team performance when they are developed by team members working with common third parties outside the focal team.
Our findings also have several practical implications for health care managers and administrators. In the specific empirical context of RAS, hospital operations could benefit from our findings in terms of efficiency gains in surgical time. Specifically, better-informed strategies regarding the formation of surgical teams and the organizational conditions under which they perform their surgical tasks (e.g., room preparation time) may help to reduce the duration of surgeries. Although the variables included in our statistical model have an impact quantified in terms of minutes saved per procedure, we emphasize that every minute counts in surgery. For example, our results (Model 7) show that one standard deviation increase in a surgeon’s previous performance helps save 20 minutes (i.e., 10% of the duration of the average procedure). From a clinical perspective, in 60 seconds, surgeons can place a catheter, remove a cyst, stop a bleeding anastomosis, or even resuscitate a patient with chest compressions. We contacted a member of the medical staff at the hospital in the study, who confirmed that: “Saving time in the OR is extremely important to us. First, time has a direct impact on the cost of a surgical procedure. In addition, saving time helps us to add new procedures whenever possible, reduce waiting lists and increase the overall productivity of the hospital.”
Scope, Limitations, and Future Research
Three features concerning the scope of our study deserve special mention in this concluding section as each is associated with a possible direction of future research. First, while the nature of the task we have analyzed allowed us to narrow the focus on individual dyads (the surgeons in our sample), we recognize that teams are typically larger than dyads. In consequence, the generalizability of our results should be considered carefully. Most teams of empirical interest contain multiple dyads, that is, they are networks and should be considered as such (Park et al., 2020). Building on a conceptualization that is widely accepted in studies of work teams (e.g., Kozlowski & Ilgen, 2006; Mathieu et al., 2008), we have considered dyads as a minimal definition of a team. On the one hand, our choice reflects a constitutive feature of robot-assisted surgery (Sergeeva et al., 2020). On the other hand, this choice may affect the extension of our core constructs beyond dyadic teams. We therefore call for further research to explore this issue, following the example of related team constructs that have emerged from the aggregation of originally dyadic constructs and that build on the assumption that team experiences have an “additive” dimension (Gonzalez-Mulé, Cockburn, McCormick, & Zhao, 2020). Groups containing more than two members give rise to dynamic networks of interaction that future research will have to consider more explicitly (Tonellato et al., 2024).
Second, our analysis is limited to teams of surgeons, reflecting their interaction primarily during RAS surgical episodes. Surgeons play a prominent role in the performance of robot-assisted surgery and thus represent the predominant source of variation in team performance (Avgerinos et al., 2020). However, their work in the operating room is supported by ancillary personnel such as anesthesiologists and scrub nurses. While we point out that this facet of our study allowed us to keep possible confounding factors related to formal organizational structure at bay, we invite future research to build on our empirical experience to explore how our findings may be extended to teams with different roles and hierarchical levels. At the same time, surgeons often interact outside the operating room, so our lack of direct and systematic access to this informal interaction may be a limitation of our study. That said, we have no reason to believe that the predictions for SCE in non-peer collaborations would not hold for interactions that occur in non-task-related contexts. For example, if two surgeons had previously collaborated with the same medical director, we would expect to see increased convergence in the representation of teamwork procedures, regardless of the different hierarchical levels of the parties involved or the specificity of the task at hand. While further research in this direction would be clearly useful, we do not see it as invalidating the core results we have reported.
Third, we considered only an operational dimension of team performance in our analyses. Prior research has conceptualized team performance as a multidimensional outcome of team interaction and coordination (Mayo, Myers, & Sutcliffe, 2021). Although different conceptualizations of team performance may be employed, prior research has established that surgery time is a reasonable and contextually appropriate performance dimension of surgical teams (Avgerinos et al., 2020; Casciaro, Lobo, Wilhem, & Wittland, 2022; Reagans et al., 2005), which is particularly appropriate in our context given the absence of life-threatening or particularly serious procedures that would require different performance measures. Surgery time also represents a dimension of performance that relies predominantly on tacit knowledge and for which implicit coordination and mutual adjustment are important in the context of surgical teams (Edmondson, 2003). In addition, we note that a longer duration of surgery typically exposes the patient to a greater risk of infection (Owens & Stoessel, 2008), suggesting that faster completion of surgery tends to be positively associated with other important dimensions of performance, including speed of patient recovery and timeliness of discharge (Catchpole et al., 2008). Finally, our operational performance is measured with considerable accuracy and is proximal to the interaction of the focal members of the surgical teams, thus excluding measurement error related to possible confounding factors such as the role of support staff. Nevertheless, we call for future work to explore the role of SCE in different settings characterized by more ambiguous performance conceptualizations, such as new product development teams, where performance may be based on indicators capturing both operational and creative outcomes (Edmondson & Nembhard, 2009).
Besides the three scope conditions just mentioned, it is worth mentioning as a possible limitation of our study that we did not begin collecting additional fieldwork data until several years after the initial data collection. As a result, some of the surgeons who were part of our original sample—particularly surgeons who had completed their residencies—had already left the hospital by the time we began collecting additional interview and participant observation data. Nevertheless, when we designed the stratified purposeful sampling strategy for our fieldwork, we tried to include as many attending surgeons who were also part of the original sample as possible. We note, in closing, that our quantitative data collection covers several years of data, allowing us to fully capture technology adoption and learning processes that remain stable over time and were still valid during our fieldwork. As a result, although we were not able to reconstruct the original sample perfectly, we were able to elicit multiple perspectives and successfully represent experiences from different areas of the distribution of our theoretically relevant variables.
Conclusion
How can action teams leverage the shared experience accumulated by their members to achieve higher levels of performance under conditions of frequent reconfigurations of team membership? This paper takes a preliminary and yet important step toward addressing this question and advancing the understanding of how shared collaborative experience within networks of prior partners is associated with higher levels of team performance. Our theoretical elaboration and empirical investigation jointly suggest that teams whose members have worked with many common prior partners enjoy considerable teamwork benefits. Teams whose members have accumulated homogeneous task experience with their common prior partners enjoy taskwork benefits. Both teamwork and taskwork benefits, however, diminish and eventually disappear as task complexity increases. For high-complexity tasks, teams whose members share many common partners may even experience a form of liability. A key implication of our study is that configuring high-performing action teams should be based on explicit consideration of team members’ extent and diversity of shared collaborative experience. In other words, the optimal team assembly strategy depends, at least in part, on factors that are external to the team. Similarly important is to recognize that the combination of extent and diversity of shared collaborative experience that is likely to be optimal for team effectiveness depends crucially on the level of complexity of the team task.
Supplemental Material
sj-docx-1-jom-10.1177_01492063241271197 – Supplemental material for The Partners of My Partners: Shared Collaborative Experience and Team Performance in Surgical Teams
Supplemental material, sj-docx-1-jom-10.1177_01492063241271197 for The Partners of My Partners: Shared Collaborative Experience and Team Performance in Surgical Teams by Marco Tonellato, Valentina Iacopino, Daniele Mascia and Alessandro Lomi in Journal of Management
Footnotes
Acknowledgements
We are grateful to action editor Jason Huang and two anonymous reviewers for their thoughtful guidance and constructive criticism throughout the process. We thank Anna Mayo, Jonathan Kush and Alessandro Iorio for their comments on an earlier draft, and Paolo Aversa for his fieldwork advice. We are grateful for the feedback we received at seminars at the University of Trento, LMU Munich, LUISS University, University of Exeter, and Bayes Business School. Financial support received from the Swiss National Science Foundation (grant number 100018_165764, Alessandro Lomi PI) is gratefully acknoweldged.
Supplemental material for this article is available with the manuscript on the JOM website.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.