
Abstract

ICRP Publication 150 Guest Editorial
Risks from Plutonium and Uranium Exposure
In its 2007 Recommendations, the International Commission on Radiological Protection (ICRP) outlined several operational quantities for use in radiological protection. Amongst these was the radiation weighting factor, wR, defined as ‘a dimensionless factor by which the organ or tissue absorbed dose is multiplied to reflect the higher biological effectiveness of high-LET (linear energy transfer) radiations compared with low-LET radiations’ and used to calculate equivalent dose and effective dose (ICRP, 2007). The Commission selected values for wR by judgement, using data on the relative biological effectiveness (RBE) of different types of radiation in inducing stochastic effects, specifically cancer.
For alpha particles, the Commission concluded in 2007 that ‘despite substantial uncertainties in estimates of dose and risk from intakes of alpha-emitting radionuclides, the available human and animal data indicate that the RBE depends on the biological end-point under consideration’. Specifically, the Commission judged that ‘the limited human data that allow estimation of alpha particle RBE values suggest values of around 10–20 for lung and liver cancer and lower values for bone cancer and leukaemia’. As the data available did not provide ‘compelling evidence for a change of the radiation weighting factor for alpha particles’, the Commission retained the wR value of 20 adopted in Publication 60 (ICRP, 1991).
How have things changed since 2007? Radon and its progeny constitute the major source of exposure to alpha emitters for the public and for groups of hard-rock underground miners. During the past decade or so, the Commission has published several reports on radon doses, risks, and protective measures (ICRP, 2010, 2014, 2017). A key strength of the assessment of radon risks was the availability of epidemiological data from studies of miners and of people exposed to radon at home (ICRP, 2010). The present publication presents an assessment of the risk of cancer from plutonium and uranium exposure. As with radon, this assessment has benefited from epidemiological data published since the start of the millennium, although earlier findings have also been considered. Furthermore, the notable dosimetric input to this publication is highly commendable.
Let us start with plutonium. We know much more now about the risks from occupational exposure to plutonium, particularly from extensive long-term health studies of workers at the Mayak plant in Russia who received a wide range of exposures. At lower levels of exposure, the Mayak findings are complemented by results from studies of groups of workers in Europe and North America (in particular, plutonium workers at the Sellafield plant in the UK). The authors of this publication refer to a ‘lack of consistency of results across the range of studies of workers exposed to plutonium’; however, these results might be more consistent once account is taken of uncertainties due to relatively small numbers of exposed workers in some studies and difficulties in estimating organ-/tissue-specific doses. The strongest findings come from a combined analysis of the Mayak worker cohort and the Sellafield worker cohort using a unified dosimetry methodology (Gillies et al., 2017). As is pointed out in this publication, estimates of the risk of lung cancer from plutonium exposure are compatible for the two cohorts, although the power of the Sellafield study is limited. Furthermore, analysis of data for Mayak workers also suggests associations between plutonium exposure and risk of liver and bone cancers, whereas there is no consistent evidence from occupational studies for increased risk of leukaemia.
For uranium, the picture is less clear. Epidemiological studies of workers are limited by low statistical power and difficulties in estimating historical doses. Consequently, it is not possible to quantify the risk of cancer in relation to organ-/tissue-specific doses from uranium.
Based on data on lung cancer deaths among Mayak plutonium workers, miners exposed to radon, and the Japanese atomic bomb survivors, this publication estimates a biological effectiveness of alpha particles relative to high-energy photons of approximately 14–16. Given the various assumptions that underpin this calculation, it is amazing that these RBE estimates are so close to the Commission’s wR value of 20 for alpha particles. Nevertheless, the range of uncertainty for these RBE estimates is likely to be wide, given the different exposure scenarios and epidemiological designs, and the challenges in assessing organ-/tissue-specific doses. Also, this comparison depends largely on data for male smokers, although it is notable that increased risk of lung cancer has also been seen among female plutonium workers at Mayak, most of whom were non-smokers. Furthermore, it has not been possible using these epidemiological data to assess the RBE for cancers of the liver or bone, or any other type of cancer, or to draw firm conclusions about possible associations with non-cancer diseases such as circulatory diseases.
It should be emphasised that the RBE estimates derived in this publication relate to occupational exposures. For radon, there is good evidence from studies of exposure in homes to suggest that the risk of lung cancer is consistent with that estimated from studies of miners exposed at low levels (ICRP, 2010). In contrast, epidemiological studies of environmental exposure to plutonium and uranium do not indicate increased risk of cancer overall, and do not provide a basis for assessing RBE related to exposure of the general population.
To have reached the stage where it is possible to make direct estimates of lung cancer alpha-particle RBEs from epidemiological studies of radon- and plutonium-exposed workers is highly impressive, and is testament to the efforts of the researchers involved and to the cooperation of workers and worker organisations. The fact that these RBE estimates are close to the wR value of 20 for alpha particles is reassuring. That said, questions remain regarding the appropriateness of using this wR value in all protection scenarios involving alpha particles. In particular, for exposures to uranium, the current epidemiological knowledge base is insufficient to draw conclusions. Ongoing work to conduct large-scale epidemiological studies of workers exposed to uranium, improve estimates of organ-/tissue-specific doses, and better understand the impact of uncertainties will be challenging. Nevertheless, based on advances made previously, there is reason to hope that this multi-disciplinary research will further enhance the RBE assessments that underpin protection from alpha emitters.
COLIN R. MUIRHEAD
ICRP COMMITTEE 1 MEMBER (1997–2009)
References
Cancer Risk from Exposure to Plutonium and Uranium
ICRP PUBLICATION 150
Approved by the Commission in May 2021
Abstract–The objective of this publication is to provide a detailed review of results from recent epidemiological studies on the risk of cancer from exposure to plutonium and uranium, and how these results relate to the assumptions currently used for protection against alpha radiation. For plutonium, the two main studies are of the cohorts of workers employed at the nuclear installations at Mayak in the Russian Federation and at Sellafield in the UK. The analysis of the Mayak worker cohort provides an estimate of the slope of the dose–response curve for the risk of lung cancer, while at lower levels of plutonium exposure, the Sellafield worker cohort provides results that, within relatively large confidence intervals, are consistent with those for the Mayak worker cohort. Results from the Mayak worker cohort also show an association between plutonium exposure and the risk of liver and bone cancers, but not the risk of leukaemia. Lifetime excess risk of lung cancer mortality has been calculated for scenarios of acute and chronic inhalation of plutonium nitrate and plutonium oxide, similar to work performed previously for radon and its decay products in ICRP Publication 115. Estimated lifetime excess risk of lung cancer mortality per unit absorbed dose is close to that derived from miner studies for exposure to radon and its progeny, and is compatible with the assumption of a radiation weighting factor of 20 for alpha particles. Epidemiological studies of the risk of cancer associated with uranium exposure have been conducted among cohorts of European and North American workers involved in the nuclear fuel cycle. Current results do not allow the reliable derivation of dose–risk models for uranium for any cancer type. Continuation of efforts to improve dose assessment associated with plutonium and uranium exposure is recommended for future research.
© 2021 ICRP. Published by SAGE.
Plutonium; Uranium; Alpha emitter; Epidemiology; Cancer; Health risk
MAIN POINTS
EXECUTIVE SUMMARY
1. Objectives
(a) In the current radiological protection system, estimation of radiation risk and detriment is primarily based on the risks observed in the Life Span Study cohort of the Japanese atomic bomb survivors, who were exposed at a high dose rate, mainly to an external source of gamma rays. It is assumed that these observed risk estimates can also be applied to different situations of exposure, such as internal contamination by radionuclides emitting alpha radiation, leading to protracted and heterogeneous irradiation, once account is taken of the relative biological effectiveness of alpha particles compared with low-level exposure to gamma rays, and of the organs/tissues irradiated. (b) The results of several epidemiological studies reported over the last two decades allow the direct estimation of the risk of cancer related to exposure to alpha-particle-emitting radionuclides. A critical analysis of these results can be used to evaluate the validity of the assumptions applied to protection against alpha emitters. (c) This publication provides a detailed review of results from recent epidemiological studies of the risk of cancer and occupational exposure to isotopes of plutonium (mainly 238Pu, 239Pu, and 240Pu) and uranium (mainly 234U, 235U, and 238U). It updates previous reviews published by national and international organisations, specifically the Fourth Committee on Biological Effects of Ionizing Radiation (BEIR IV) Report of the US National Research Council (NRC, 1988), the International Agency for Research on Cancer monograph on internal emitters (IARC, 2012), and the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) 2016 Report on the biological effects of uranium (UNSCEAR, 2017). The present publication constitutes the first comprehensive review of health risks associated with plutonium exposure to be published in over 30 years. (d) This publication presents calculations of the lifetime excess risk of lung cancer mortality associated with example scenarios of plutonium inhalation, similar to those performed previously for radon and its decay products in Publication 115 (ICRP, 2010). It discusses the uncertainties associated with these results, and their potential impact for radiological protection.
2. Methodology used
(e) This publication focuses essentially on epidemiological studies published since 2000 in which organ-/tissue-specific dose estimates are based on individual monitoring of internal exposure to plutonium or uranium. Individual annual exposure data, long duration of health surveillance in the cohort, and validation of the dosimetric models used for individual organ-/tissue-specific dose assessment were the major criteria considered for inclusion of a study in the analysis of lifetime risk. Consequently, results contributing to this analysis derive from a limited number of cohorts. (f) For plutonium, several studies have been performed in North America, Europe, and Russia. One joint case–control study has been performed in Europe, but was limited by its size. The two main studies are the cohorts of workers employed at the nuclear installations at Mayak in the Russian Federation and at Sellafield in the UK. Assessments of intakes and organ-/tissue-specific doses for Mayak workers arising from the inhalation of plutonium have been based primarily on the interpretation of measurements of urinary excretion, taking account of workers’ occupational histories and the physicochemical forms of the inhaled plutonium aerosols. Results from autopsy data have also been used to determine model parameter values. There has been a progression of biokinetic and dosimetric models used for this purpose over the last 20 years, most recently applying the methodology of the Commission. This publication details the recent Mayak Worker Dosimetry Systems (MWDS-2008 and MWDS-2013) and the system developed for the joint analysis of Mayak and Sellafield plutonium workers as part of a European Union SOLO (epidemiological studies of exposed (g) The assessment of uranium-specific doses for workers employed in the nuclear fuel cycle (processing, concentration, enrichment, and reprocessing operations) is difficult due to the relatively fast clearance of uranium from blood circulation, variability of exposure to uranium compounds, and differences in the methods used to monitor internal exposure. The solubility of the uranium compounds to which workers are exposed is a particularly important parameter in determining lung doses from bioassay data. Cohorts of uranium miners were not considered in this publication, as they were discussed extensively in Publication 115 (ICRP, 2010), and the major risk of lung cancer identified in these cohorts is due to radon and its decay products.
3. Review of epidemiological results
(h) The epidemiological evidence on risks associated with plutonium is less extensive than that for radon and its progeny. Indeed, the first epidemiological results from underground hard-rock miner studies were published at the end of the 1960s, whereas most of the results related to plutonium were published after the 1990s. Furthermore, the number of studies providing results on risks associated with plutonium exposure is more limited than for radon progeny. In addition, the assessment of doses due to plutonium exposure is more complicated due to the chemical nature of plutonium compounds, and the retrospective reconstruction of plutonium doses from bioassay measurements. (i) Risk of lung cancer resulting from plutonium exposure has been quantified through extensive study of the Russian Mayak workers, which includes a wide range of exposure levels. Risks at lower levels of plutonium exposure can be complemented by analysing other cohorts in Europe and North America. One of the major risks related to plutonium exposure is lung cancer. Several successive analyses of the Mayak worker cohort, based on different dosimetry systems and periods of follow-up, have provided estimates of the dose–response relationship. Estimates of the risk of lung cancer for Mayak workers are compatible with estimates obtained in two European studies published in 2017, but which have relatively wide confidence intervals. Much of the evidence derives from male smokers. The impact of statistical power, uncertainty in dose estimates, and co-factors (e.g. tobacco smoking) that may influence cancer development are considered, together with alternative dosimetric approaches. (j) Results from the Mayak worker cohort also suggest an association between plutonium exposure and risks of liver and bone cancers, although data are limited. There is no consistent evidence of a positive dose–response relationship between the risk of leukaemia and plutonium exposure. (k) Epidemiological studies of the risk of cancer associated with uranium exposure are primarily of cohorts of workers exposed to different chemical forms of uranium. Published studies are collated and evaluated, but most do not provide information that fulfils all the criteria mentioned above for the estimation of risks specific to uranium exposure. In recent years, several studies have been published using improved organ-/tissue-specific dose calculations, but they remain inconclusive because statistical power was limited and some of the information needed to reconstruct doses was not recorded in the past. Therefore, at present, it is not possible to quantify the risk of cancer per organ-/tissue-specific dose of uranium on the basis of the published studies. (l) A few recently published studies have also considered possible health effects other than cancer, mainly circulatory diseases (Annex A). Some results are suggestive of an association between plutonium or uranium exposure and increased risk of circulatory diseases, especially results from the Mayak worker cohort. However, at present, these studies do not permit definitive conclusions on the existence of non-cancer diseases associated with internal exposure to plutonium or uranium.
4. Quantification of the lifetime risk of lung cancer associated with plutonium exposure
(m) It is now possible to estimate the lifetime excess risk of lung cancer following inhalation of plutonium directly from epidemiological studies of plutonium workers. Calculations have been performed for illustrative scenarios with a total plutonium intake of 1 Bq, assuming either an acute inhalation event at 20 years of age or chronic inhalation at 20–29 years of age of either insoluble plutonium oxide or soluble plutonium nitrate. Lung doses were calculated using models from Publication 141 (ICRP, 2019). Lifetime risk was calculated using ICRP baseline rates for a composite Euro-American male population, as provided in Publication 103 (2007), and the risk model derived from the SOLO project analysis of Gillies et al. (2017). These unitary intake scenarios should be considered as examples, ignoring the impact of variations in important factors such as smoking, to provide an estimated order of magnitude of risk and to illustrate variations in dose and risk for the inhalation of plutonium. (n) For the same intake, the cumulative doses to lung tissues from plutonium oxide are higher than those from plutonium nitrate, but the lifetime excess risk of lung cancer mortality per mGy varies little, with estimates between 1.4 and 1.7 per 10,000 persons, depending on the solubility (plutonium oxide or plutonium nitrate) and exposure rate (acute or chronic intake). In comparison, the lifetime baseline risk of lung cancer mortality is 631 per 10,000 persons for a Euro-American male population. (o) For comparison, exposure to 222Rn progeny under the scenario considered in Publication 115 (ICRP, 2010) of 7.1 mJ h m−3 (2 working-level months) per year from 18 to 64 years of age, when converted to lung dose, leads to a lifetime excess risk of lung cancer mortality per mGy of 1.6 per 10,000 persons.
5. Implications for radiological protection and future research
(p) A comparison of the lifetime excess risk of lung cancer mortality from exposure to an external source of gamma radiation (based on the Life Span Study of the Japanese atomic bomb survivors) and from internal exposure to plutonium (based on the Mayak workers study) indicates that, for the same absorbed dose to the lung and dose distribution, the risks from plutonium exposure are larger than those from external gamma exposure by a factor of approximately 16. The risk for radon progeny exposure appears to be consistent with that from plutonium exposure, and larger than that from external gamma exposure by a factor of approximately 14, despite the very different distribution of alpha-particle dose within the lung. (q) These comparisons suggest a biological effectiveness of alpha particles relative to high-energy photons of approximately 14–16 for lung cancer. These values are compatible with the current radiation weighting factor, wR, of 20 used by ICRP for alpha particles in the calculation of equivalent and effective doses (ICRP, 2007). (r) It should be noted that this comparison is based on lung absorbed dose and lifetime excess risk of lung cancer mortality, with application of a dose and dose-rate effectiveness factor (DDREF) of 2 to the risk derived from the Japanese Life Span Study. Not applying a DDREF would lead to relative biological effectiveness of approximately 7–8 for lung cancer. Also, care has to be taken in making comparisons with wR as the latter is intended to embrace the risk of all stochastic effects, whereas lung cancer mortality alone is considered in the present calculations. Further, it was considered premature to quantify lifetime excess risks for bone and liver cancers, for which associations have also been demonstrated for plutonium, and different relative biological effectiveness values for alpha radiation may apply for these cancer types. (s) Further research is needed to improve the assessment of health risks associated with plutonium or uranium exposure in epidemiology, dosimetry, and risk modelling. Uncertainties associated with plutonium and uranium exposure and dose reconstruction are substantial, and inhalation of different chemical forms leads to very different cumulative organ-/tissue-specific absorbed doses. For lung cancer, a better determination of the distribution in the different parts of the lung is important. Important efforts have been made in recent years to improve dose assessment and to consider the potential impact of uncertainties on risk estimates, and should be maintained in the future. Also, extension of existing cohorts and combined analyses of data are needed to increase power, and allow improved estimation of the risks associated with plutonium and uranium exposures. In addition, better consideration of the effect of smoking in future analyses is highly desirable. For uranium, more information on the intake of different chemical forms is required. Future research may better characterise the risks associated with alpha particles emitted by plutonium for cancer induction in organs/tissues other than the lung.
1. INTRODUCTION
1.1. Risk of cancer from exposure to alpha emitters
(1) Estimates of the excess risk of cancer following exposure to ionising radiation are largely derived from epidemiological studies of people acutely exposed to moderate and high doses of gamma rays, primarily the Life Span Study (LSS) of the Japanese survivors of the atomic bombings of Hiroshima and Nagasaki in 1945. To obtain risks that would apply at low doses and low dose rates of exposure to low-linear energy transfer (low-LET) radiation (i.e. gamma ray, x ray, and beta radiation), the Commission reduces the risk determined at moderate-to-high doses and high dose rates by a dose and dose-rate effectiveness factor (DDREF). (2) The System of Radiological Protection recommended by the Commission applies not only to such circumstances of exposure to low-LET radiation, but also to all other situations including intakes of alpha-particle-emitting radionuclides that deposit energy heterogeneously between and within organs/tissues of the body, and continue to irradiate these organs/tissues with short-range alpha particles over a prolonged period, often many years. In addressing these exposure conditions using risk estimates derived from the LSS, a number of assumptions are made regarding the equivalence and additivity of external and internal exposures (particularly for radionuclides emitting short-range radiations distributed inhomogeneously within the body), the relative biological effectiveness (RBE) of alpha particles compared with gamma rays, and the effect of protracted exposure in comparison with acute exposure. (3) These assumptions can be tested using appropriate epidemiological studies of those exposed to internally deposited alpha emitters. There are good data obtained over several decades on lung cancer in underground hard-rock (e.g. uranium) miners who inhaled 222Rn and its radioactive alpha-particle-emitting decay products. Risks, doses, and protection against exposure to radon and its progeny have been considered by the Commission in several publications [Publications 115, 126, and 137 (ICRP, 2010, 2014, 2017)]. (4) Over the past two decades or so, studies have been published of those exposed to isotopes of plutonium and uranium. These radionuclides distribute in the body, specifically in the lung, differently from radon and its progeny. In particular, radon and its decay products deliver doses primarily to the upper lung (bronchi) for a brief period, whereas plutonium and uranium deliver doses throughout the lung and over a protracted period, especially plutonium. In this publication, these epidemiological studies of plutonium and uranium exposures will be reviewed and the implications of the findings for radiological protection will be discussed. This publication provides a detailed review of results from epidemiological studies considering the risk of cancer from occupational exposure to plutonium and uranium published over the last 20 years. It aims to update previous reviews published by national and international organisations, especially the Fourth Committee on the Biological Effects of Ionizing Radiation (BEIR IV) Report (NRC, 1988), the International Agency for Research on Cancer (IARC) monograph on internal emitters (IARC, 2012), and the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) 2016 Report on the biological effects of uranium (UNSCEAR, 2017). The present publication constitutes the first comprehensive review of health risks associated with plutonium exposure. (5) This publication is concerned with epidemiological studies able to provide information on the dose–response relationship with the risk of cancer. Experimental studies are thus not considered here. However, IARC (2001, 2012) and the United States Agency for Toxic Substances and Disease Registry (ATSDR, 2010, 2013) reviewed evidence from experimental data on animals exposed to internalised plutonium and uranium. Such information has been used to infer the risk of cancer in humans (Bijwaard and Dekkers, 2007). (6) This publication focuses on recent epidemiological studies in which organ-/tissue-specific dose estimates are used, based on individual monitoring of internal exposure to plutonium or uranium. The dosimetric methodology for the calculation of organ-/tissue-specific doses from internally deposited plutonium and uranium is reviewed and discussed, and the importance of obtaining accurate doses for use in epidemiological studies is emphasised. (7) For plutonium, the two main studies are the cohorts of workers employed at the nuclear installations at Mayak in the Russian Federation and at Sellafield in the UK. The risk of lung cancer resulting from plutonium inhalation has been quantified through an extensive study of the Mayak workers, which includes a wide range of exposure levels. Risks at lower levels of plutonium exposure are complemented by analysing other cohorts in Europe and North America, although the cohort of Sellafield plutonium workers remains of principal importance among these studies. Recent studies of the Sellafield workforce have provided estimates of the dose–response relationship for lung cancer that are comparable with those obtained in several successive analyses of the Mayak worker cohort (MWC), based on different dosimetry systems and periods of follow-up. (8) Calculations of the lifetime excess risk of lung cancer mortality following inhalation of plutonium may be performed for unitary intake scenarios using dosimetric models from Publication 141 (ICRP, 2019), baseline mortality rates for a composite Euro-American male population (ICRP, 2007), and the risk model from the latest analysis of the MWC (Gillies et al., 2017). This provides an estimated order of magnitude of the risk, and can illustrate variations in the lung dose and consequent risk for the inhalation of plutonium under different conditions of exposure. The results may be compared with the lifetime excess risk of lung cancer mortality per unit lung dose from inhalation of 222Rn and its progeny, under the scenario considered in Publication 115 (ICRP, 2010), and with that following exposure to external gamma radiation, based on the experience of the Japanese atomic bomb survivors. With respect to lung cancer, these comparisons provide information on the biological effectiveness of alpha particles emitted from plutonium and radon progeny relative to high-energy gamma radiation, which is relevant to the radiation weighting factor, wR, for alpha particles used for the purposes of radiological protection. (9) Epidemiological studies of the risk of cancer associated with uranium exposure have been conducted among cohorts of European and North American workers exposed to different chemical forms of uranium in the nuclear fuel cycle. These studies have been reviewed in the UNSCEAR 2016 Report (UNSCEAR, 2017), and the present publication updates the UNSCEAR review. Evidence from studies of uranium workers, however, remains limited.
1.2. Exposure to plutonium
(10) Plutonium is an actinide element formed in nuclear reactors, mainly as the 238Pu, 239Pu, 240Pu, 241Pu, and 242Pu isotopes; and 239Pu is the principal fissile material used for the production of nuclear weapons. 239Pu, with a radioactive half-life of 24,065 years, was first produced artificially and identified in 1941 in Berkeley, California, USA. It exists naturally on Earth in minute quantities when 238U nuclei absorb neutrons generated by the spontaneous fission of uranium isotopes, and was first separated by Seaborg and Perlman in 1949. 239Pu is produced in nuclear reactors when 238U captures a neutron, with the 239Np (half-life 2.356 days) so-formed undergoing beta decay to 239Pu. The longer that uranium fuel is irradiated in a reactor, the greater the proportion of other isotopes of plutonium that are formed, as the plutonium isotopes capture neutrons. For example, when 239Pu captures a neutron, 240Pu is created (half-life 6561 years), and 238Pu is formed from various neutron absorption reactions in uranium and neptunium isotopes. 238Pu has a relatively short half-life of 87.7 years, and a correspondingly high specific activity and decay heat: 1 g of 238Pu generates approximately 0.6 W of thermal power. Pure 238Pu is produced by neutron irradiation of 237Np, recovered from spent nuclear fuel. It produces little hazardous penetrating radiation, and so has found industrial applications in radioisotope thermoelectric generators (RTGs) used, for example, in cardiac pacemakers, spacecraft, and radioisotope heater units (RHUs) used in spacecraft to heat critical components. 241Pu is produced in higher ‘burn-up’ nuclear fuel as more neutron capture reactions occur, and decays by beta transformation (half-life 14.35 years) to 241Am, an alpha emitter with a half-life of 432 years. The longest-lived isotope of plutonium is 244Pu with a half-life of 81 million years. The behaviour of plutonium in the human body depends on its chemistry, and this has been discussed in previous publications (ICRP, 1972, 1986, 1993, 2019). (11) Plutonium was first separated on an industrial scale from irradiated nuclear fuel in 1945 at the Hanford site in Washington State, USA. It was there that the plutonium was produced for the atomic bombs detonated in the Trinity Test in New Mexico, USA on 16 July 1945, and over Nagasaki, Japan on 9 August 1945. Plutonium continued to be produced at Hanford to build up the nuclear weapons arsenal of the USA with the last plutonium production reactor closing in 1987. Other sites reprocessing irradiated uranium fuel were also constructed, and were operated in the USA to produce weapons-grade plutonium (with a high 239Pu content), such as the sites at Savannah River, South Carolina and Rocky Flats, Colorado. (12) Efforts to produce plutonium in the former USSR started shortly after the end of the Second World War. The first Russian nuclear complex, currently known as the ‘Mayak Production Association (PA)’, was built for this purpose in the Southern Urals of Russia, Chelyabinsk Province. This complex included nuclear reactors, a radiochemical plant, a plutonium production plant, and a number of auxiliary facilities; the only facilities with potential for significant plutonium exposures were the radiochemical reprocessing plant and the plutonium production plant. The first reactor commenced operation in 1948, and the radiochemical and plutonium plants were completed 1 year later. The first 10 years (1948–1958) of Mayak PA operations were the period of development of industrial-scale technology for producing plutonium. (13) Exposures at the Mayak radiochemical plant involved substantial exposures to external radiation from short-lived fission products and to aerosols containing mostly plutonium nitrate, whereas exposures at the plutonium production plant involved intake of aerosols containing plutonium dioxide or mixtures of plutonium-containing salts, combined with comparatively low doses of external radiation. The levels of exposure to plutonium were dependent on the workplace, period of employment, work undertaken, and whether workers used individual respirators that protected the airways. The highest exposures occurred between 1948 and 1958 before respirators were introduced. The highest exposures among workers employed during this period of time were among chemical engineers and chemical technicians employed in jobs related to enrichment of plutonium solutions, extraction of plutonium from these solutions, and processing of plutonium in metal or dioxide form. (14) Plutonium for the nuclear weapons programme of the UK was first produced at Windscale Works, Sellafield in north-west England in 1952. Like the plutonium production sites in the USA and then in the USSR, Windscale Works consisted of nuclear reactors, a chemical reprocessing plant, and a plutonium finishing plant. Exposures to plutonium at Sellafield in the early years of production were greater than in later years, but did not reach the levels experienced in the early years of operation at Mayak. Later, weapons-grade plutonium was also produced in France and China. (15) In addition to nuclear weapons programmes, plutonium has also been separated from irradiated nuclear fuel in reprocessing plants for civil purposes, primarily for use as a fuel in nuclear power stations. Civil plutonium is usually derived from fuel with a higher ‘burn-up’ – the uranium fuel has been kept in a reactor for longer periods and has a higher content of plutonium isotopes other than 239Pu (e.g. 240Pu and 238Pu). This change in the ‘spectrum’ of alpha-emitting radioisotopes and their chemical forms leads to potential exposure to aerosols with increased contributions from 238Pu and 241Am to the total alpha activity, and smaller aerosol particle size due to particle fragmentation attributed to nuclear recoil during radioactive decay of 238Pu. (16) Environmental exposure to plutonium arises mainly from fallout from atmospheric nuclear weapons testing and discharges from nuclear installations, principally from nuclear fuel reprocessing plants. Doses are predominantly small and difficult to estimate accurately, although special investigations (e.g. autopsy studies) have confirmed the (generally) very low levels of exposure of members of the public.
1.3. Exposure to uranium
(17) Uranium is an actinide metal, and is the most massive element (atomic number 92) to be present in any quantity in the Earth’s crust. Uranium has no stable isotope, but two isotopes are sufficiently long-lived for primordial uranium nuclei to be present on Earth today: 238U has a half-life of 4.47 × 109 years, and 235U has a half-life of 7.04 × 108 years. 234U also has a relatively long half-life of 2.46 × 105 years, but is only present on Earth because it is part of the radioactive decay chain of 238U. The uranium presently found on Earth consists of 99.27% 238U and 0.72% 235U (and 0.01% 234U as a result of the presence of 238U); approximately half of the 238U that was initially present on Earth has now decayed, whereas only approximately 1% of the original 235U now remains. (18) Uranium is naturally present in varying concentrations in soil, rocks, and in surface and ground water (UNSCEAR, 2000). A large portion of natural background radiation in the environment originates from radionuclides in the radioactive decay chains of 238U and 235U. With the isotopes in equilibrium, 238U and 234U each contribute approximately 48.9% of the total activity content of natural uranium, with 235U contributing the remaining 2.2% (ATSDR, 2013). When the content of 235U or 234U is greater than that in natural uranium, the material is referred to as ‘enriched’ uranium, while uranium with a 235U or 234U content less than naturally occurring uranium is referred to as ‘depleted’ uranium. Enriched uranium is produced in specialist uranium enrichment plants for use in fuel for commercial nuclear reactors, typically at a 235U enrichment of 3–5%, and at higher 235U enrichments for use in research, military reactors, and weapons. A by-product of the enrichment process is depleted uranium. (19) Uranium exhibits both chemical and radiological effects. The chemical effects are independent of the isotopic make-up of the uranium compound. These effects are non-carcinogenic and are assumed not to occur below a certain concentration. Uranium compounds vary greatly in solubility, which can lead to differences in the bioavailability of the compound after inhalation or ingestion. Solubility of the compound varies according to valence, with the tetravalent form being less soluble than the hexavalent form. (20) In addition to the chemical toxicity of uranium, all uranium isotopes emit alpha particles on radioactive decay, which are classified as carcinogenic to humans by IARC (2001, 2012). Although 238U is the most abundant naturally occurring isotope, many other isotopes, ranging from 232U to 237U, continue to be handled to varying extents within the nuclear fuel cycle. Some of them, for instance 232U (an alpha emitter with a half-life of 72 years), produce progeny that emit alpha particles, beta particles, and gamma rays. (21) The potential for uranium exposure occurs throughout the nuclear fuel cycle: mining and milling of uranium; uranium conversion and enrichment; reactor fuel fabrication; reactor operation; nuclear fuel reprocessing; waste handling and disposal; and research and development. Inhalation is the principal means of intake of uranium in the uranium fuel cycle, and the chemical form of intake is important in determining the organ-/tissue-specific doses received, in particular, by the lung, with insoluble forms of uranium residing for a longer time in the lung and giving a higher cumulative dose. (22) In addition to ubiquitous exposure to naturally occurring sources of uranium, such as intakes from foodstuffs and drinking water, small additional exposures to members of the public occur from operations of the nuclear fuel cycle, such as uranium mining and processing. Doses from these additional exposures are typically very low.
1.4. Assessment of internal exposure to radionuclides
(23) Doses from intakes of radionuclides cannot be measured directly. Intakes are estimated from measurements of activity in the body or in excreta using biokinetic models. Most alpha-particle-emitting radionuclides cannot be measured directly in vivo, unless the alpha decay is accompanied by a reasonably high-energy gamma ray that can be detected outside the body, as in the case of 241Am. They are therefore usually monitored by urine bioassay, and more rarely by faecal bioassay. Biokinetic models are constructed to provide a mathematical description of the uptake and retention of radionuclides in body organs and tissues, and their excretion over time after intake by inhalation or ingestion (and occasionally, wounds). Such models are also used to determine the number of radioactive transformations occurring in different organs and tissues over specified time periods, and absorbed doses are then calculated using dosimetric models (ICRP, 2015a). Incorporated long-lived radionuclides such as isotopes of plutonium and uranium, which can be retained tenaciously in the body, may continue to irradiate tissue for many years after intake. (24) Inhalation is a common route of occupational intake. Large uncertainty is usually associated with estimated internal doses following inhalation. The reliability of estimated intakes and doses depends notably on the quality of measurements; characteristics of the inhaled material, particularly its solubility and rate of absorption from the lungs to blood; variations in individual physiological characteristics; and the time between exposure and measurement. Generally, these factors are not well known, and estimates of internal doses are subject to substantial uncertainties. (25) The most commonly used biokinetic and dosimetric models are those of the Commission, as described in previous publications. The Human Respiratory Tract Model (HRTM) of Publication 66 (ICRP, 1994a), revised in Publication 130 (ICRP, 2015a), considers both the extrathoracic and the thoracic airways, and the interstitial tissues of the lungs. The thoracic airways (lung) are divided into three regions for which doses are calculated separately: the bronchial region (BB), the bronchiolar region (bb), and the alveolar-interstitial (AI) region. The fraction of inhaled activity that is deposited in those regions mainly depends on the particle size distribution of the inhaled aerosol, which is characterised by the activity median aerodynamic diameter and the associated geometric standard deviation (GSD). The HRTM treats clearance as a competitive process between absorption into blood, which depends on the solubility of the inhaled material, and particle transport to the alimentary tract and lymph nodes. It is assumed that particle transport rates are the same for all materials, whereas absorption into blood is material-specific. Different solubilities of chemical forms of plutonium and uranium lead to substantially different retention times in the lungs, and hence substantially different magnitude and duration of dose delivery. (26) In the HRTM, absorption is treated as a two-stage process: dissociation of the particles into a material that can be absorbed into blood (dissolution); and absorption of soluble material and material dissociated from particles into blood (uptake). To represent time-dependent dissolution, a fraction fr of the deposited particles is assumed to dissolve rapidly at a rate sr, while the remaining fraction (1-fr) is assumed to dissolve more slowly at a rate ss. Dissolution depends upon the chemical form of the inhaled material, whereas subsequent uptake to blood depends on the element. Uptake is usually assumed to be instantaneous unless the dissolved ions become bound to respiratory tract tissues. To represent time-dependent uptake, a fraction fb of the dissolved material may be considered to be retained in a ‘bound state’, from which it is transferred into blood at a rate sb and is not subject to particle transport (ICRP, 1994a, 2015a). (27) The Human Alimentary Tract Model (HATM) of Publication 100 (ICRP, 2006), replacing the former Gastrointestinal (GI) Tract Model of Publication 30 (ICRP, 1979), describes the intake of radionuclides by ingestion, their absorption to blood, and excretion into faeces. It also deals with activity transferred from the respiratory tract or from the systemic circulation, mainly through the liver. Absorption from the alimentary tract to blood is quantified by the fraction fA of ingested activity. (28) The biokinetics of an inhaled radionuclide after absorption from the lungs to blood depends on the element. Direct information on the biokinetics of systemic plutonium and uranium comes from studies of human subjects injected with isotopes of the elements, and autopsy data of exposed subjects. Studies of a variety of laboratory animals fill the gaps in information for humans (ICRP, 2017, 2019). (29) For adults, following uptake to blood, approximately 80% of plutonium is transferred to the liver and skeleton, and the remainder is transferred to the kidneys and other soft tissues. A significant proportion of plutonium is retained tenaciously in the skeleton, while limited urinary and faecal excretion takes place. From the liver, a small proportion of the activity is transferred to the alimentary tract via bile, and the remainder is recycled back to blood (ICRP, 1993, 2019). (30) For adults, following uptake to blood, approximately 75% of uranium is excreted in urine over the following few days and approximately 15% is deposited on bone surfaces. The remaining 10% of uranium is transferred to the liver, red blood cells, and other soft tissues, while limited faecal excretion takes place (ICRP, 1995, 2017). The biokinetics of uranium in the skeleton is similar to that of calcium, but only a small proportion is retained over the long term because of bone remodelling and continuing urinary excretion. (31) The skeleton is composed of compact cortical bone, including medullary cavities, and spongiosa, made of a lattice of thin trabecular bone and marrow (ICRP, 1996). Plutonium and uranium from the bloodstream deposit on bone surfaces, and may be buried in bone volume by formation of new bone, or released from bone surfaces by resorption and returned to the bone marrow and blood (ICRP, 1989).
2. RISK OF CANCER FROM EXPOSURE TO PLUTONIUM
2.1. Introduction
(32) Production of plutonium on a large scale requires several technological stages including:
irradiation of uranium fuel in nuclear reactors; chemical dissolution of irradiated uranium fuel; chemical separation of plutonium from untransmuted uranium, transplutonium, and other actinide elements and fission products; and chemical extraction of plutonium from the resulting solution and its purification. (33) These stages are usually subdivided into three specific components: nuclear reactors, radiochemical cycle, and plutonium production cycle. Workers from radiochemical and plutonium production plants have the greatest potential for exposure to plutonium. (34) Following inhalation and deposition in the respiratory tract, plutonium is cleared by particle transport to the alimentary tract and lymph nodes, and by absorption to blood. The rate of clearance to blood depends on the chemical form of the inhaled plutonium; for example, plutonium is absorbed to blood at a higher rate when inhaled as the nitrate rather than the oxide. After absorption to blood, plutonium distributes in organs and tissues, primarily the liver and skeleton. (35) The risk of cancer resulting from plutonium exposure has been quantified through extensive studies of the Russian Mayak workers, who experienced a wide range of exposure levels. Estimates of risk at lower levels of plutonium exposure are complemented by analyses of other worker cohorts in Europe and North America, mainly the workers at Sellafield in the UK. One of the major risks related to plutonium inhalation is lung cancer, but plutonium also deposits on bone surfaces and in the liver, giving rise to risk of bone and liver cancers. Epidemiological studies of Mayak workers and other worker cohorts informing on the risk of cancer from plutonium are reviewed in this section, and lifetime risk of death due to lung cancer is calculated.
2.2. Dosimetric aspects
(36) Assessments of internal dose have been carried out for plutonium workers at Mayak PA, at Sellafield, and at some other European and US sites. The methodologies and assumptions made in these calculations are described below. The dosimetry performed for the main epidemiological studies of the MWC and the joint Sellafield worker cohort (SWC) and MWC is explained first, and then the dosimetry applied in other European and US studies is described. The most recent ICRP models (ICRP, 2015a, 2017, 2019) are used for the most recent Mayak and Sellafield analyses; previous versions of the ICRP models have been used in earlier analyses. Alternative modelling approaches have also been used to estimate lung dose and urinary excretion.
2.2.1. Dosimetry for the Mayak worker cohort
(37) Assessments of intakes and organ/tissue doses of the Mayak workers arising from the inhalation of 239Pu have been primarily based on the interpretation of urine bioassay data. The biokinetic and dosimetric models used for this purpose have been updated over the years (Khokhryakov et al., 2000, 2002, 2005). For interpretation of the measurement results, the dosimetry systems also used information on occupational history, exposure history, and physicochemical properties of plutonium aerosols. Studies conducted from 2000 used the dosimetry system Doses-2000, updated to Doses-2005 in 2007. The corresponding estimates of dose were based on a modified version of the HRTM (ICRP, 1994a), and the absorption characteristics of different chemical forms of plutonium were classified according to in-vitro solubility analysis of air samples from workplaces. The absorbed dose to the lung was averaged over the entire organ. (38) In Doses-2005, a fixation depot was introduced in the respiratory tract model from which no plutonium clearance took place (Khokhryakov et al., 2005). Another change was that in Doses-2000, the systemic burden was estimated with a modified Durbin excretion function (Durbin, 1972), and a fixed systemic distribution was assumed based on autopsy data, whereas the plutonium systemic model described by Leggett et al. (2005) was introduced in Doses-2005. Doses-2005 was developed further into the Mayak Worker Dosimetry System 2008 (MWDS-2008).
2.2.2. Mayak Worker Dosimetry System 2008
(39) MWDS-2008 was developed as a collaborative effort between Russian, UK, and US dosimetrists, and implements a modified version of the HRTM (ICRP, 1994a), the Publication 30 GI Tract Model (ICRP, 1979), and the systemic biokinetic model for plutonium described by Leggett et al. (2005), which was later adopted by the Commission in Publication 141 (ICRP, 2019). MWDS-2008 is described in detail by Khokhryakov et al. (2013), and the principal characteristics of this system are described below. (40) The autopsy data of Mayak workers showed greater retention of insoluble forms of plutonium in the pulmonary tissues of smokers compared with non-smokers. Consequently, smokers and non-smokers were treated separately, and the default HRTM particle transport rates were modified for smokers, as described in Publication 66 (ICRP, 1994a). When the smoking status was unknown, it was assumed that males were smokers and females were non-smokers. Aerosols of plutonium were divided into three categories according to their absorption characteristics (i.e. their chemical properties). These categories were:
plutonium nitrates; plutonium oxides; and a mixture of plutonium compounds (nitrates, chlorides, oxalates, oxides, and dioxides). (41) Absorption parameter values were derived for each category by fitting model predictions to autopsy data. The autopsy data showed a higher-than-expected plutonium burden in the respiratory tract relative to that in systemic tissues at extended times after intake. To model this, the bound state of the HRTM was used to represent a fixed deposit of plutonium activity in the respiratory tract, which is not subject to particle transport or absorption (Khokhryakov et al., 2005). For non-smokers, values for the bound fraction were approximately 0.3 for oxides and 0.04 for nitrates. The assumed fixed deposit may actually represent particulate material deposited in the AI region that is sequestered in the interstitium, or material that has become encapsulated in fibrous scar tissue. (42) The autopsy data also showed that the ratio of plutonium in the pulmonary lymph nodes and in the lung parenchyma was higher than predicted by the HRTM. To reflect this, the particle transport rate from the AI region to the thoracic lymph nodes was modified by fitting model predictions to the autopsy data (ratio of the lymph node burden to systemic burden) (Khokhryakov et al., 2013). (43) The intake regime for each worker was based on their exposure history, with the exposure pattern assumed to be chronic but decreasing exponentially with time. The rate of decline was estimated for each type of workplace. However, if a worker had been exposed inadvertently to an acute intake because of an accident, they were excluded from the cohort. The size distribution of the inhaled aerosols was assumed to be lognormal with an activity median aerodynamic diameter of 5 µm and GSD of 2.5, which are the ICRP default values for occupational exposures (ICRP, 1994a). (44) Before the late 1970s, many workers were given DTPA (a chelating agent) prior to their urine sample to enhance their excretion. This improved the detection capabilities. It was estimated that, on average, Ca-DTPA increased the urinary excretion of plutonium by a factor of approximately 62. This factor was uniformly applied to estimate the ‘natural’ urinary excretion rate (i.e. the excretion rate if DTPA had not been administered). This enhancement factor is consistent with other values from 1 to 130 reported in the literature (Davesne et al., 2016), most being approximately 50, but it introduces an additional source of uncertainty in the estimated urinary excretion rate that Vostrotin et al. (2017) quantified with GSD of 1.85. (45) The intakes were estimated by fitting model predictions to the urinary excretion data by applying the maximum likelihood method (ISO, 2011; EURADOS, 2013). It was assumed that the uncertainty associated with the urinary excretion data could be described by a lognormal distribution with a given GSD. However, for simplicity, each data point was assumed to have the same GSD, in which case the estimated intake is independent of the GSD. If the measurement was below the decision threshold (DT), the value was set equal to DT/2. (46) The absorbed dose to the lung was calculated by dividing the energy deposited in the lung (excluding the lymph nodes) by the total mass of the lung. This is approximately equal to the absorbed dose to the AI region, and it assumes that the sensitivity per unit mass of the central airways (BB and bb regions of the lungs) is the same as that of the AI region. The energy deposited due to alpha recoil was excluded in the calculation. If the body mass was known, the estimated absorbed dose to the lung (and to other organs) was adjusted by multiplying the dose by the ratio of body mass for the reference worker to the actual body mass. This may have introduced some biases in lung doses as the masses of the radiosensitive regions of the lung are not necessarily proportional to the body mass. When the individual body mass was unknown, an assumption was made that the lung mass was 1.1 kg for a male worker and 0.904 kg for a female worker. (47) The MWDS-2008 analysis assumes that all the alpha activity arises from 239Pu. The exact radionuclide composition of the inhaled material was not considered. However, other nuclides, such as 238Pu, 241Pu, and 241Am, would also be present in the source term and, furthermore, the activity composition would change with time. In-vivo measurements with a whole-body counter showed that the fraction of 241Am in the total body relative to the sum of actinides was sometimes as high as 15% (Khokhryakov and Yefimov, 2007). Taking account of the radionuclide composition of the source term will affect the individual’s dose assessment, and neglecting it is an additional source of uncertainty. (48) Although approximately one-third of workers employed in plutonium production or radiochemistry in the early 1950s were monitored for plutonium by urinalysis (Shilnikova et al., 2003), a systematic urine monitoring programme did not begin until approximately 1970. As a result, only approximately 40% of workers in the radiochemical and plutonium plants had internal dose assessments based on urine monitoring. Of these 40%, only approximately one-third had more than two urine measurements. However, for the workers with lung absorbed doses exceeding 0.2 Gy, approximately half had more than two urine measurements. For approximately 73% of workers, their first plutonium measurement in urine was taken during the second half of their career.
2.2.3. Mayak Worker Dosimetry System 2013
(49) MWDS was further developed in 2013 by the same international group. The revised system (MWDS-2013) used to assess doses to the lung and other organs/tissues of the plutonium workers at Mayak PA was based on the revised HRTM that was later adopted in Publication 130 (ICRP, 2015a). New absorption parameter values for plutonium oxides and nitrates have also been derived. As with MWDS-2008, the Publication 30 GI Tract Model (ICRP, 1979) and the systemic biokinetic model for plutonium described by Leggett et al. (2005) were implemented. In addition, uncertainties associated with dose estimates were calculated, taking account of uncertainties in both the urine measurement data and the model parameters. In a Bayesian approach, the uncertain quantities are represented as random variables following probability distributions. Prior distributions are first assigned based on initial knowledge. Next, the prior distributions are updated to incorporate information from measurement data. The updated probability distributions are called ‘posterior distributions’, and are updated by applying Bayes’ theorem, an elementary result of probability theory (NCRP, 2010). Bayesian techniques were applied in MWDS-2013 to calculate posterior distributions on doses derived from urinary data. A description of the dosimetry system is given by Birchall et al. (2017a). The main differences between this system (MWDS-2013) and the previous system (MWDS-2008) are described below.
2.2.3.1. Respiratory tract model parameter values
(50) Prior distributions were assigned to respiratory model parameter values, including aerosol size parameters, breathing parameters, deposition efficiency parameters, particle transport parameters, and absorption parameters (Birchall et al., 2017a). Most of the prior distributions were derived and justified by Puncher et al. (2011) for a European worker study (Tirmarche et al., 2010). However, notable exceptions are the absorption parameters associated with the assumed bound state (fb and sb), and the slow dissolution rate (ss) for plutonium nitrates and oxides. (51) The revised HRTM of Publication 130 (ICRP, 2015a) has adopted a new particle clearance model for the AI region which models observations of greater long-term retention in the AI region than assumed previously for insoluble particles. Approximately 33% of the alveolar deposit of insoluble particles is assumed to be sequestered in the interstitium, and as such is not subject to particle transport other than very slow clearance to lymph nodes. Sequestration to the interstitium of relatively insoluble forms of plutonium is consistent with observed long-term retention in the lungs of Mayak workers. (52) Circumstantial evidence of a bound state for plutonium comes from a re-analysis of historic beagle dog data where dogs were exposed to plutonium nitrate and followed for 15 years (Puncher et al., 2017b); and autopsy data of a US Trans-Uranium and Uranium Registries (USTUR) whole-body donor (Case 0269), a plutonium worker who inhaled plutonium nitrate (Puncher et al., 2017a; Tolmachev et al., 2017). In both cases, a bound state was required to fit the late retention data. For USTUR Case 0269, Tolmachev et al. (2017) measured plutonium activity in the upper and central airways of the respiratory tract (i.e. in ET2, BB, and bb) 38 years after acute exposure. Given that this activity would have been cleared by mucociliary clearance if in particulate form, these measurements provide evidence for binding (bound material is assumed not to be subject to particle clearance). Furthermore, the ratio of the measured activity in the thoracic lymph nodes to total lung activity at autopsy was lower than expected, indicating that material had been bound to lung tissue (Puncher et al., 2017a). However, it is not known whether the plutonium present in the upper and central airways was associated with the epithelium, as assumed in the dosimetric model for the bound fraction, or in underlying tissues, such as lymphatic channels (ICRP, 2019). The uncertainties associated with the assumption of binding are discussed further in Paras 103–105. (53) Assuming that some plutonium was retained in a bound state, autopsy data from 20 Mayak workers, exposed to nitrates alone, were analysed to determine values of fb and ss (Puncher et al., 2017c). Using a Bayesian approach with the revised Publication 130 HRTM (ICRP, 2015a), the mean value of fb was determined as 0.0014 [95% confidence interval (CI) 1.1 × 10−4 to 3.0 × 10−3]. There was no evidence for an sb value other than zero. Based mainly on this data set and taking account of the fb estimates from USTUR Case 0269 and the beagle dog data, MWDS-2013 assumed a uniform prior distribution between 0 and 0.004 with a representative fb value of 0.002 (Birchall et al., 2017a, 2019). The median value determined for ss for plutonium nitrate was 2.5 × 10−4 day−1 with GSD of 1.08. Puncher et al. (2017d) also carried out a similar analysis on autopsy data from 20 Mayak workers exposed to oxides alone. The median value determined for ss for plutonium oxide was 4.7 × 10−5 day−1 with GSD of 1.07.
2.2.3.2. Dosimetry assumptions
(54) Radiosensitive cells in each of the three regions of the lung have been identified for the purposes of the HRTM (ICRP, 1994a). These are basal (BBbas) and secretory (BBsec) cells in the bronchial epithelium; Clara cells (a type of secretory cell) in the bronchiolar epithelium; and endothelial cells such as those of capillary walls and type II epithelial cells in the AI region. The radiosensitive targets of the BB and bb regions are assumed to be restricted to tissue layers of given depths and thicknesses, whereas in the AI region, it is assumed that the sensitive cells are distributed homogenously throughout its mass. In MWDS-2013, the absorbed dose to each target region was calculated:
bronchial basal cells, Dbas; bronchial secretory cells, Dsec; bronchiolar region, Dbb; and alveolar region, DAI. (55) Where a single quantity is required to represent lung dose, a weighted absorbed dose to the lung was calculated in MWDS-2013 with the weighting scheme of the HRTM (ICRP, 1994a, 2015a) for equivalent dose to the lung:

Due to the much smaller mass of the target regions in the BB and bb regions than in the AI region, this apportionment assumes a substantially greater sensitivity per unit mass of the central airways than the lung tissue represented as AI. Calculating this weighted absorbed dose with equal regional weights, as opposed to the mass-weighted absorbed dose that was used in MWDS-2008, is preferable because the evidence on risks from radon progeny shows that the dose to central airways can result in lung cancer. Calculating lung dose as a mass-weighted absorbed dose would result in the prediction of incidence of lung cancer in miner study groups exposed to radon that is lower than observed. Equal apportionment for the three regions of the lung provides much better consistency with the observed incidence (Marsh et al., 2014; Birchall and Marsh, 2017).
(56) No correction factor was applied to the lung dose to account for the variation in lung mass between subjects (Birchall and Sokolova, 2017). However, separate doses to males and females were calculated with the ICRP reference organ masses for males and females (ICRP, 2002).
(57) In the revised HRTM of Publication 130 (ICRP, 2015a), there are no modifying factors for particle transport rates for smokers because long-term lung retention studies of insoluble particles show no clear difference between smokers and non-smokers (Gregoratto et al., 2010). The dose calculations for MWDS-2013 did not distinguish between smokers and non-smokers.
2.2.3.3. Urine measurement assumptions
(58) Workers stayed at an inpatient hospital for 72 h in order to provide three consecutive 24-h urine samples. The urine measurements were used to provide an estimate of workers’ average excretion rate over a 24-h period. If incomplete samples were collected, they were normalised to an equivalent 24-h value by considering either the volume of the sample or the amount of creatinine in the sample. Before 2008, urine samples were normalised by volume if the volume collected was small (<0.5 L), while after 2008, all urine samples were normalised by creatinine concentration measurements. As explained above for MWDS-2008 (Para. 44), for those workers who were given DTPA prior to their urine sample, a correction was made to account for the enhanced excretion due to DTPA. (59) Uncertainties associated with urine measurements were estimated by Vostrotin et al. (2017) and expressed as GSD. These uncertainties included: (i) measurement uncertainties due to counting statistics; (ii) uncertainties associated with the collection period; and (iii) variability in the enhancement factor for those workers given DTPA. These uncertainties were also applied to the urine data below the DT, but the contributions due to counting statistics were ignored. Likelihood functions were derived for urine data above and below the DT, which can be used in a Bayesian analysis. Approximately half of the urine measurements were below the DT.
2.2.3.4. Exposure assumptions
(60) Based on personal or static air sampling data, three separate time periods were identified during which average air concentrations were expected to be different (Sokolova et al., 2017). These were before 1958, between 1958 and 1970, and after 1970, with median values of annual volumetric activity of alpha-emitting radionuclides in workplace air assumed to be 3.2, 0.32, and 6.4 × 10−3 Bq m−3, respectively. The exposure pattern was therefore simplified to a stepwise function corresponding to three levels of constant chronic intake with relative concentrations of 1:0.1:0.002. A relatively uninformative prior distribution was assigned to the total intake, described by a lognormal distribution with GSD of 6 (Birchall et al., 2017a). The median value, M, of this prior distribution was assumed to be proportional to the number of years of exposure. It was shown that the dose estimates were not overly sensitive to the value of M (Puncher et al., 2014). (61) Where there was direct evidence of additional acute intakes, the worker was excluded from the cohort.
2.2.4. Dosimetry for the joint cohort of plutonium workers from the Russian Federation and the UK
(62) A joint epidemiological analysis of Russian and British plutonium worker cohorts was undertaken to investigate potential associations between occupational exposures to plutonium and lung cancer or leukaemia mortality and incidence, or cardiovascular disease mortality (Gillies et al., 2017). The study combined the MWC and SWC. The dosimetry system used was similar to MWDS-2013, which implemented the revised HRTM that was later adopted in Publication 130 (ICRP, 2015a), the Publication 30 GI Tract Model (ICRP, 1979), and the systemic biokinetic model for plutonium described by Leggett et al. (2005). A Bayesian approach was adopted where uncertainties on model parameter values and intakes were first derived as prior probability distributions. However, absorbed tissue doses for the Mayak and Sellafield workers were provided as point estimates (i.e. single estimates without uncertainties). These point estimates were calculated for each worker based on their urinalysis data as follows (Puncher and Riddell, 2016): a Bayesian posterior distribution of intake was calculated using an assumed prior distribution of intake with the model parameter values fixed at their prior means. The best estimate of intake was taken as the mean of the posterior distribution, which was then used to calculate absorbed doses to the lung and other tissues/organs. This approach is also applicable to cases where all the urinalysis data are censored below the detection limit (DL), and leads to unbiased estimates of doses. This is important because 45% of the monitored workers in the pooled cohort only had urine measurements that were below the DL. Puncher and Riddell (2016) reported that the point estimates of dose produced for the epidemiological study were unbiased. (63) A relatively uninformative prior distribution was assigned to the total intake described by a lognormal distribution with GSD of 6. For the Sellafield workers, a constant chronic exposure over the exposure history was assumed, with additional acute intakes if direct evidence was available. The median value of the total intake prior distribution was calculated for each Sellafield worker, assuming 20 Bq year−1 and 20 Bq per acute intake. These values were derived from analysis of historical personal air sampler data (Puncher et al., 2014). The exposure pattern assumed for the Mayak workers was a stepwise function consisting of three separate constant chronic intake regimes, as described above for MWDS-2013 (Para. 60). (64) The prior distributions assumed for the model parameters were the same as those for MWDS-2013 apart from the slow dissolution rate, ss, for plutonium nitrate (Puncher and Riddell, 2016; Birchall et al., 2017a). Different studies of humans inhaling plutonium nitrate suggested significantly different solubility in terms of the level of slow dissolution. For example, Puncher and Etherington (2016) re-analysed the lung, urine, and systemic data from two volunteers who inhaled 237Pu/244Pu nitrate (Etherington et al., 2003) and estimated an ss value of 2.2 × 10−3 day−1 using a Bayesian analysis (Birchall et al., 2017a; ICRP, 2019). This value is significantly higher than the value assumed for MWDS-2013 (ss = 2.5 × 10−4 day−1), which was based on autopsy data of 20 Mayak workers exposed to plutonium nitrates alone (Puncher et al., 2017c). It was noted that the value derived from the volunteer experiment (ss = 2.2 × 10−3 day−1) was similar to that derived from rat studies of Sellafield plutonium-bearing materials (Moody et al., 1993). As there was no consensus on which value to use, for the purposes of dose reconstruction, two sets of dose estimates were produced: one set based on a normal prior distribution for ss with a mean of 2.2 × 10−3 day−1 (referred to as the ‘Sellafield prior distribution’) and the other based on the ‘Mayak prior distribution’ of MWDS-2013 for plutonium nitrates. Thus, the Mayak prior for plutonium nitrate assumes lower solubility than the corresponding Sellafield prior. (65) On average, the lung doses calculated for each worker of the SWC using the ‘Mayak prior distribution’ are approximately three times higher than those calculated using the ‘Sellafield prior distribution’ with a variation characterised by GSD of 1.4. As expected, there is little or no effect on systemic doses [liver and red bone marrow (RBM)], and a small effect on intake. (66) It was not clear whether the observed difference in long-term dissolution was due to differences in chemical processes (e.g. causing partial oxidisation of the nitrate material) at Mayak and Sellafield, different levels of exposure, or a difference in interpretation between an experimental study and autopsy results. Recently, ICRP (2019) has reviewed human and animal studies following inhalation of plutonium nitrate to derive specific absorption parameter values. An ss value of 2.0 × 10−3 day−1 was recommended based on:
long-term monkey and dog studies with follow-up periods of 8 years and 15 years, respectively (Brooks et al., 1992; Dagle et al., 1993; Puncher et al., 2017b; Pellow et al., 2019); analysis of autopsy and bioassay data of USTUR Case 0269, a plutonium worker who inhaled plutonium nitrate (James et al., 2007; Puncher et al., 2017a; Tolmachev et al., 2017); and the volunteer experiment discussed above (Puncher and Etherington, 2016). (67) It was noted that a large fraction dissolving at a slow rate (ss = 2.5 × 10−4 day−1), as reported for the MWC based on autopsy data, was inconsistent with the results of the USTUR and the long-term dog and monkey studies, but it was considered that a slow rate could apply to higher levels of exposures (ICRP, 2019). The data available suggest that the different time scales of the volunteer study (approximately 4 months) and the Mayak autopsy data (>5 years) cannot explain the discrepancy in the assessed ss values for the SWC and MWC. The discrepancy likely reflects different exposure conditions in the two cohorts in terms of industrial chemical processes, with the possible presence of residual insoluble material in some plutonium nitrate, and involved masses, with higher mass of plutonium nitrate inducing greater polymerisation of hydrolysed plutonium in the lung (ICRP, 1986; Nolibé et al., 1989). (68) Recently, Bull and Puncher (2019) considered three approaches to reconcile the discrepancy in the assessed ss values for the MWC and SWC. These were: (i) a slower dissolution rate in the interstitium compared with other regions of the lung; (ii) a three-component dissolution model for nitrates; and (iii) an oxide component in Mayak ‘nitrate’ exposures. The authors concluded that the latter assumption best describes the Mayak dissolution rate as the other two variants were inconsistent with the long-term dog studies. Assuming an oxide component in Mayak ‘nitrate’ exposures gave lung doses that were approximately 30% lower, on average, than those calculated with MWDS-2013 (Bull and Puncher, 2019). (69) Urine sampling procedures at the Sellafield site changed after 1970 because of the discovery of a problem involving the adventitious contamination of urine samples arising from the re-use of glass sample bottles. By 1971, disposable plastic bottles were introduced. To take account of this, pre-1971 urine data were divided by 3 and were assigned a larger measurement uncertainty (GSD = 2.8) compared with post-1970 data (GSD = 1.6) (Riddell et al., 2000; Puncher and Riddell, 2016) (see Section 2.2.5). Workers who only had pre-1963 urine results that were all recorded as ‘less than the reporting level’ were excluded from the SWC. (70) For the Sellafield workers, the dose arising from intakes of 241Pu was included in the dose calculation (Para. 83). This was inferred from the expected activity ratio of 241Pu to plutonium alpha emitters in the plant material on an annual basis. In comparison, the dosimetry for the Mayak workers assumed that all the alpha activity arose from 239Pu and did not take account of intakes of 241Pu or 241Am (Para. 47).
2.2.5. Dosimetry systems for other worker studies
2.2.5.1. European combined analysis of plutonium workers (Alpha-Risk project)
(71) Grellier et al. (2017) investigated the effects of internal exposure to plutonium and uranium for workers in the British [Atomic Weapons Establishment (AWE), UK Atomic Energy Authority (UKAEA), and British Nuclear Fuels Ltd (BNFL) cohorts], Belgian [SCK•CEN/Belgonucléaire/Belgoprocess (SCK•CEN/BN) cohort], and French [Commissariat à l’Energie Atomique-Compagnie Genérale des Matières Nucléaires (CEA-COGEMA) cohort] nuclear industries in a case–control study of lung cancer and leukaemia mortality, nested within appropriate cohorts from the study by Cardis et al. (2007). The nested case–control design allowed detailed dose reconstruction as well as the collection of individual data on potential confounders. Bingham et al. (2017) described the dosimetry in detail, which is summarised below. (72) The systemic biokinetic model for plutonium described by Leggett et al. (2005) and the Publication 66 HRTM (ICRP, 1994a) were used to generate point estimates of lung dose. Transport through the GI tract was based on the Publication 30 model (ICRP, 1979). Doses were calculated using reference organ/tissue masses from Publication 23 (ICRP, 1975) and radionuclide transformation data from Publication 38 (ICRP, 1983). (73) Bioassay data obtained for controls after the date of cancer diagnosis of the matched case were excluded. This ensured that the dose assessments for controls were not biased by the availability of more accurate bioassay results compared with the cases. A maximum likelihood method was applied to provide an estimate of the intake(s) based on the best fit between the observed bioassay data and that predicted from the estimated intake regimes. For the AWE cohort, subjects with measurements that were all below the reporting level were excluded from the study. For the UKAEA and CEA-COGEMA cohorts, a Bayesian fitting was used to provide a central estimate of the intake for such workers by extracting the median from the posterior probability distribution. For the BNFL cohort, the approach taken was that the last measurement result in the exposure period was set as positive at the limit of detection, and chronic intake was assumed over the period. (74) The individual alpha-particle doses to the BB region, bb region, AI region, thoracic lymph nodes, and RBM were estimated. For the main epidemiological analysis, the dose to the lung was calculated as the arithmetic mean of the doses to the BB, bb, and AI regions. The alpha-radiation dose from 241Am ingrowing from 241Pu in the exposure material was included in the plutonium dose for the UKAEA, BNFL, CEA-COGEMA, and SCK•CEN/BN cohorts. (75) Dose assessment was essentially based on urine measurements, with variable numbers per subject. A small number of faecal and lung monitoring (CEA-COGEMA) results were also used. (76) Chronic intakes were assumed for any period of a worker’s career that involved a potential risk of internal exposure by plutonium. The start and end dates of chronic intakes were determined from records of work history for the UKAEA and AWE cohorts, and from exposure files for the CEA-COGEMA cohort. Where these data were not available or did not align with the monitoring data, start and end dates were adjusted based on monitoring intervals and known periods of employment. By default, for BNFL workers, chronic exposure periods were started 6 months prior to the first sample for plutonium bioassay, as this was the usual monitoring interval. Evidence for acute intakes came from reports of incidents, from air-sampling data, from nose-blow results, and from post-incident monitoring. (77) An aerosol particle size of 5 µm activity median aerodynamic diameter was chosen as the most typical of workplaces. The lung solubility of the exposure material was based on information available on the materials used or known to be present in the workplaces (buildings) in which individuals had worked. The lung solubility parameter values used were derived by assigning the material to the appropriate HRTM default absorption type (ICRP, 1994b), or from experimental evidence, or by re-evaluating historical intake assessments to obtain specific HRTM absorption parameters.
2.2.5.2. Sellafield workers
(78) Cohort studies of the plutonium workers employed at the Sellafield plant in north-west England have been reported by Omar et al. (1999) and McGeoghegan et al. (2003). For these studies, annual doses to tissues/organs of individual workers arising from the inhalation of plutonium were calculated based on measurements of plutonium in urine. These older studies made use of older versions of the ICRP biokinetic models, and alternative modelling approaches have also been used to estimate lung dose and urinary excretion. Details of the calculations are given by Riddell et al. (2000) and are briefly discussed here. (79) For the majority of the assessments, a single constant chronic exposure was assumed. Assessments of systemic uptake of plutonium (i.e. activity transferred to blood) were obtained from urine measurements by applying the Jones urinary excretion function (Jones, 1985). From the assessed uptake rate, the dose to the lungs, GI tract, and systemic organs were calculated by implementing the ICRP biokinetic and dosimetric models available at the time of calculation. For the analysis carried out by Omar et al. (1999), these were the respiratory tract model and the GI tract model described in Publication 30 (ICRP, 1979), and the systemic biokinetic model for plutonium described in Publication 48 (ICRP, 1986). (80) The Publication 30 respiratory tract model (ICRP, 1979) classified material according to its solubility in terms of retention times in lung: Class D, retained for days; Class W, retained for weeks; and Class Y, retained for years. The results presented by Omar et al. (1999) were for Class Y materials alone as measurements made on the solubility of plutonium compounds commonly found at Sellafield showed that the majority exhibit behaviour closest to Class Y. Compared with the current HRTM (ICRP, 2015a) applied to the pooled MWC and SWC (Section 2.2.4), Class Y roughly translates to Type S, including plutonium oxide. (81) The organ dose calculations carried out for the cohort study of female plutonium workers at the Sellafield plant (McGeoghegan et al., 2003) used updated biokinetic and dosimetric models, namely the Publication 66 HRTM (ICRP, 1994a) and the Publication 67 biokinetic model for plutonium (ICRP, 1993). However, a separate urinary excretion function (Jones, 1985) was still applied to assess the uptake of plutonium as the function was derived using Sellafield worker data. (82) The uptake rate assessed from urine data with the Jones (1985) urinary excretion function was higher than expected when compared with uptake estimates obtained from autopsy data. Consequently, the calculated organ doses were reduced by a factor of 3, as it was judged that the autopsy data would provide a more accurate estimate of true uptake (Riddell et al., 2000). They were reduced by an overall factor of 9 when based on pre-1971 urine data alone due to substantial adventitious contamination of urine samples mentioned in Para. 69. Since the actual bias introduced by both the use of the Jones (1985) function and the contaminated pre-1971 glass sample bottles was not quantified accurately, it led to large uncertainty in historical Sellafield dose assessment. For workers with both pre-1971 and post-1970 urine data, only the post-1970 data were used in the assessment. (83) In addition to the doses from ‘Pu alpha’ (i.e. from 239Pu, 238Pu, and 240Pu), the dose from 241Pu intake and from its decay product, 241Am, was also estimated. 241Pu intake was inferred from the expected activity ratio of 241Pu to ‘Pu alpha’ of the plant material. The expected activity ratio changed annually to reflect changes in the prevailing plant conditions and the average recorded burn-up of the fuel reprocessed each year (Riddell et al., 2000).
2.2.5.3. US nuclear workers
(84) The potential health hazards of internal exposure to plutonium have been recognised in the USA since the early 1940s because it is an alpha emitter like radium, to which New Jersey dial painters were exposed previously (Rowland, 1994). Consequently, a Health Group was established in the Manhattan Project to implement occupational radiation safety that prevented workers from receiving significant plutonium intakes. Notably, in 1944, Wright Langham instituted a programme for the collection of daily urine samples from Los Alamos National Laboratory employees handling plutonium. The plutonium content of those samples was extracted with an iron carrier by cupferron in chloroform, and measured with gas-flow proportional counters and a background of approximately 30 counts min−1. From 1945, urine samples were collected on holiday away from Los Alamos to avoid cross-contamination, and the measurement background was decreased to approximately 0.1 counts min−1 (Campbell et al., 1972; Miller et al., 2008). (85) The dosimetric interpretation of the plutonium bioassay results was made possible by data collected in experimental studies (ICRP, 2019). For instance, biomedical studies began in 1944 with studies on rodents that indicated translocation of plutonium from blood to the liver and skeleton, with a long retention half-life in the skeleton (Durbin, 1975, 2011). Moreover, from 1945 to 1948, 18 seriously ill persons were injected with tracer amounts of plutonium citrate or nitrate to investigate the relation of the systemic burden and excretion rate of plutonium (Langham et al., 1950; Langham, 1959). The life expectancies of the subjects were judged to be short at the time of injection, but eight were still alive after 8 years, and four survived for at least three decades (Rowland and Durbin, 1976). Thus, both the results of human injections and the Los Alamos worker data were used by Langham et al. (1950) to determine urinary and faecal excretion curves for plutonium. (86) In practice, approximately 6000 urine analyses were conducted on Los Alamos workers between 1944 and 1950. Twenty-seven workers excreted measurable amounts of plutonium. Their health was followed first by Langham et al. (1962) and Hempelmann et al. (1973), and later by Voelz et al. (1979, 1997). More recently, Miller et al. (2008) estimated their doses and those of an expanded group of 210 former Los Alamos workers from the years 1944–1945; the median effective dose was 75 mSv with GSD of 1.62. (87) Schubauer-Berigan et al. (2007) carried out a nested case–control study of leukaemia excluding chronic lymphocytic leukaemia [non-chronic lymphocytic leukaemia (CLL) leukaemia] among workers at five US nuclear facilities. Both external and internal exposures were considered. Equivalent doses to RBM arising from exposures to plutonium were calculated from urine measurements by implementing ICRP biokinetic and dosimetric models (Daniels et al., 2006). These included the Publication 66 HRTM (ICRP, 1994a), the Publication 30 GI Tract Model (ICRP, 1979), and the Publication 67 biokinetic model for plutonium (ICRP, 1993). Evaluations were carried out only for those workers who had detectable plutonium in urinary excretion (≥1.7 mBq day−1). Occupational, dosimetry, medical, and site records were reviewed to obtain information regarding date and route of exposure, isotopic composition of source term, and plutonium solubility. Unless information was available to suggest otherwise, the following assumptions were made:
route of intake was inhalation; intakes occurred 3 days prior to the first ‘positive’ bioassay sample; solubility of material was 50% Type M (moderately soluble) and 50% Type S (slow absorption); and source term consisted of 239Pu alone. (88) Lung doses arising from inhalation of plutonium and uranium have also been calculated for a case–control study of workers employed at the Rocky Flats Plant in Colorado (Brown et al., 2004). These assessments were based on urine measurements of plutonium and uranium, and on in-vivo lung measurements. Intakes of 241Am were inferred from the assessed 239Pu intakes and the isotopic ratios of the nuclear materials processed at Rocky Flats. The biokinetic and dosimetric models described in Publication 30 were used in the calculations (ICRP, 1979). For cases and controls, 98% and 96% of the collective internal lung dose, respectively, was due to a combination of plutonium and 241Am. (89) An earlier cohort study of Rocky Flats workers (Wilkinson et al., 1987) had used cumulative systemic plutonium deposition as calculated from urinalysis results, but tissue-specific doses were not estimated. (90) A cohort study of Los Alamos workers (Wiggs et al., 1994) used cumulative systemic plutonium deposition based on urinalysis results, and did not estimate tissue-specific doses. However, for a subset of 26 Manhattan Project workers (Voelz et al., 1997), annual tissue-specific doses were calculated using the Publication 30 models (ICRP, 1979). (91) A cohort study of Hanford workers (Wing et al., 2004) did not use available bioassay results for plutonium, but preferred to use exposures derived from a job-exposure matrix.
2.2.6. Uncertainties in plutonium dose estimates
(92) The uncertainty in an internal dose assessment based on bioassay data, such as urinary measurements, arises from many sources:
uncertainty in the bioassay measurements; uncertainties in the route, time, and pattern of intake; uncertainties associated with the chemical and physical form of the deposited radionuclide(s), such as the activity size distribution and the absorption characteristics of the inhaled material; uncertainties in the identity of radionuclides and their relative abundances in the source term; and uncertainties in the biokinetic and dosimetric models used to interpret the bioassay measurements. (93) The US National Council on Radiation Protection and Measurements (NCRP, 2010) reviewed these uncertainties, and the methods used to evaluate them, extensively. In MWDS-2013, a multiple realisation approach was applied to assess uncertainty on dose in a Bayasian inference framework (Birchall et al., 2017c). Uncertainties in internal dose assessments based on bioassay data can be quite large. This is illustrated by the work of Puncher and Riddell (2016). Using Bayesian inference techniques, they calculated posterior distributions of absorbed doses to the lung for plutonium workers of the Sellafield plant based on urinary measurements. The analysis took account of uncertainties in the biokinetic models, measurements of urinary excretion, and estimates of intakes. The parameter values for each worker were assumed to be independent. The geometric mean values of the ratio of the 97.5%:2.5% posterior values were a factor of 100 for lung dose, and 30 for doses to the liver and RBM. It was inferred that the most important sources of uncertainty in lung dose were uncertainties in the rapid absorption parameters (fr, sr) and uncertainties in the pre-1970 urine measurement data (Para. 69). (94) While Bayesian inference techniques have been used to calculate posterior distributions of internal plutonium doses based on urine data for epidemiological studies of plutonium workers from the Mayak and Sellafield plants (Puncher and Birchall, 2008; Tirmarche et al., 2010; Puncher and Riddell, 2016; Birchall et al., 2017c; Birchall and Puncher, 2017), further research is required to determine the appropriate methods of analysis of these data. Such an analysis will need to take account of shared and unshared errors. Shared errors are uncertainties that are 100% correlated between different workers, whereas unshared errors assume no correlation between workers. Statistical techniques to estimate uncertainty in risk that reflects statistical sampling error and uncertainty in dose including shared errors have been described by Stayner et al. (2007). Generally, the error associated with internal doses can be considered as Berkson type (error independent of observation, same dose assigned to a group of individuals) because of the inability of biokinetic and dosimetric models to predict the individual’s true dose for a given exposure. It is noteworthy that the mean value of the posterior distribution of dose is generally greater than the point estimate of dose calculated with the best-estimate values of the input model parameters. This difference arises because the biokinetic and dosimetric models are non-linear with respect to most of their parameters. (95) Typically, non-incident-specific intakes (i.e. background intakes) of actinides are modelled by assuming a constant chronic intake. However, truly chronic intakes are rare, and plutonium workers may be exposed to a series of acute intakes. The uncertainty in the estimated intake associated with assuming a constant chronic intake was investigated by Wilson and Bull (2007). Artificial 239Pu urinary datasets were created, consisting of four urine samples per year over a 10-year period arising from two random acute intakes per year. Assuming a constant chronic intake over a 10-year period resulted in an average systematic uncertainty in the estimated intake of approximately 4%. In comparison, the authors noted that the uncertainty associated with the solubility characteristics of the inhaled material can be a major source of uncertainty in dose assessments that are based on excretion data. (96) The uncertainty in biokinetic models used to interpret bioassay measurements not only arises from uncertainties associated with model parameter values, but also uncertainty associated with the structure of the model. Such uncertainties may arise because the structure of the model provides an oversimplification of the known processes, because the model cannot account for unknown processes, or because part of the model structure is based on mathematical convenience rather than the actual processes. For example, a volunteer study suggested that the early urinary excretion rate following inhalation of plutonium nitrate might be enhanced compared with that following intravenous injection (Etherington et al., 2003). The uncertainty in the biokinetic approach used may result in biased estimates of intakes and doses based on bioassay data. For instance, the evaluation of data for UK plutonium workers gave estimates of organ retention of 239Pu that were significantly higher when based on urinary data with the Jones urinary excretion function compared with direct measurements of concentrations in systemic tissues obtained at autopsy (Para. 82; Jones, 1985; Lawson et al., 1989; Bailey et al., 1996; Riddell et al., 2000). The Jones function substantially underestimated urinary plutonium data from recent injection studies, while the more recent plutonium models used in Publications 67 and 141 (ICRP, 1993, 2019) model urinary excretion in accordance with these data. (97) Comparisons of estimates of intake of plutonium for the Mayak workers based on either urine or autopsy data showed good agreement using the plutonium biokinetic model of Publication 141 (Leggett et al., 2005; Birchall et al., 2017b; ICRP, 2019). The geometric mean ratio of the intake estimates (urine:autopsy) ranged from 0.92 to 1.14 depending on the assumed exposure regime. (98) As described earlier, the HRTM divides the lung into three regions: the BB region, the bb region, and the AI region. Where a single quantity is required to represent lung dose, a weighted absorbed dose to the lung was calculated in MWDS-2013 with the weighting scheme of the HRTM (ICRP, 1994a, 2015a) (see Para. 55). In deriving apportionment factors representing the region’s estimated sensitivity relative to that of the whole lung, Publication 66 (ICRP, 1994a) considered applying the relative risk concept. In this concept, it is assumed that the induction of cancer by radiation exposure is proportional to the background lung cancer rates. Current information on the relative distribution of the major histological types of lung cancer in populations of smokers and non-smokers suggests a higher incidence of cancer in the central airways (BB and bb) compared with the AI region. The regional distribution of lung cancer types in the general population was considered in Publication 66 (ICRP, 1994a). Values of 0.6 for the BB region, 0.3 for the bb region, and 0.1 for the AI region were obtained for a population of non-smokers and smokers. Results from experimental animal studies also generally indicate that uniform irradiation of the lung is more likely to lead to the induction of cancer in the BB and bb regions than the AI region. However, in animal studies in which inhaled insoluble alpha emitters delivered most of the dose to the deep lung, carcinomas appeared to originate in the lung periphery, corresponding to the AI region (ICRP, 1994a). The Commission concluded that there is no quantitative basis for deriving factors, with any acceptable degree of confidence, to represent regional differences in radiation sensitivity among the BB, bb, and AI rgions. In the absence of such adequate quantitative information, Publication 66 (ICRP, 1994a) recommended that the BB, bb, and AI regions should each be assigned one-third of the total radiation detriment in the lung. As the mass of the target tissues in the BB (approximately 1 g) and bb (approximately 2 g) regions is much smaller than the mass of the AI region (1100 g), this implies far greater sensitivity per unit mass for the central airways than the lung tissue of the AI region. The identification and localisation of radiosensitive target cells in each region of the lung, as well as the combination of regional lung doses into a single dose quantity, are additional sources of uncertainty in lung dosimetry. (99) Saccomanno et al. (1996) measured the distribution of tumours in the bronchial tree for a cohort of 467 miners and 311 non-miners. All subjects were male with positive smoking histories. The results showed tumour distribution in the BB:bb:AI regions to be 0.68:0.15:0.16 for miners and 0.59:0.18:0.23 for non-miners. Winkler-Heil et al. (2015) also estimated values of apportionment factors by comparing different radon and thoron exposures, which produce different regional dose distributions, with observed regional cancer distributions. The authors concluded that apportionment factors of approximately 0.65, 0.30, and 0.05 for the BB, bb, and AI regions may represent a realistic estimate. (100) Table 2.1 shows the regional absorbed doses and the weighted absorbed dose to the lung arising from the inhalation of 239Pu for nitrates and oxides. These values were calculated using MWDS-2013 assuming the Commission’s default apportionment factor (ABB:Abb:AAI) values of ⅓:⅓:⅓ and the default model parameter values given by Birchall et al. (2017a). However, assuming apportionment factors of approximately 0.6:0.3:0.1 instead of the Commission default values (⅓:⅓:⅓) decreases the weighted absorbed dose to the lung per unit intake by approximately 1.5 and 2.2 for plutonium nitrates and oxides, respectively. (101) The radiosensitive cells in the central airways are considered to be basal (BBbas) and secretory (BBsec) cells in the bronchial epithelium, and Clara cells (a type of secretory cell) in the bronchiolar epithelium (ICRP, 1994a, 2015b). Based primarily on the histological measurements of Mercer et al. (1991), these radiosensitive targets of the BB and bb regions are assumed to be restricted to tissue layers of given depths and thicknesses. For example, in the BB region, the secretory cells are assumed to be uniformly distributed within the depth range of 10–40 µm and the basal cells are assumed to be uniformly distributed within the range of 35–50 µm from the lumen. In contrast, the histological measurements of Robbins et al. (1990) showed smaller cell depths, with average secretory and basal cell depths of 19 µm and 27 µm, respectively (ICRU, 2012). Mercer et al. (1991) also showed that the cell nuclei were not uniformly distributed, but exhibited a distinct maximum within the reported ranges. Thus, the assumed cell depth distribution of the target cells in the central airways is a source of uncertainty. (102) For plutonium oxide, the dose to the basal cell layer mainly arises from the activity sequestered by macrophages in the lamina propria of the BB region (Birchall et al., 2010, Table 2.1). Thus, the sequestered activity is assumed to be physically closer to the basal cell layer compared with activity deposited on the surface of the epithelium which is cleared quickly by mucociliary action. For plutonium nitrates, the dose to the basal cells arises mainly from both the sequestered activity and the bound activity that is assumed to be uniformly distributed throughout the epithelium. If basal cells were assumed to be located at smaller depth than they are, then the estimated dose they receive from alpha radiation emitted by activity deposited on the epithelial surface would increase. However, because this lumenal activity is cleared relatively rapidly, the cell depth distribution of the target cells in the central airways is not a major source of uncertainty for plutonium dosimetry. (103) Assumptions regarding the bound fraction, fb, can have a significant effect on the lung dose for inhaled nitrates, mainly affecting dose to the central airways. For example, assuming an fb of 0.008 as opposed to no binding increases the lung dose by a factor of approximately 1.6 following the inhalation of 239Pu nitrate. The default fb value of 0.002 assumed in MWDS-2013 was based on re-analysis of historic beagle dog data, autopsy data of USTUR Case 0269, and autopsy data of Mayak workers following inhalation of plutonium nitrate (Birchall et al., 2017a, 2019) (see Para. 52). Mean values of fb ranged from 0.001 to 0.008, with extreme values ranging from 0.0001 to 0.011. (104) Measurements of activity in the upper and central airways of USTUR Case 0269 provided evidence of binding because particulate material would have been cleared by mucociliary transport (Para. 52). However, it is not known if the activity assumed to be bound is uniformly distributed throughout the epithelium, as assumed in the dosimetric model, or is in the underlying subepithelial tissue (ICRP, 2019). Lower doses would be obtained if bound activity was located within the subepithelial layer. The assumption that it is uniformly distributed in the epithelium is based on the premise that chemical binding has occurred in which dissolved ions bind to lung tissue. Measurements of the activity concentration in the BB, bb, and AI regions of the lung of Case 0269 showed uniform distribution between the three regions; the activity concentration in each region was not statistically different from the average lung concentration (Tolmachev et al., 2017). However, autoradiographs of selected lung tissue sections obtained from this donor showed that the microdistribution was non-uniform (Nielsen et al., 2012). An alpha ‘star’ aggregate of plutonium was measured in the connective tissue of the bronchioles, which indicates that the plutonium was localised rather than diffused within the region. This suggests that the activity is retained by an alternative or additional mechanism to chemical binding. For example, physical binding could occur in which particulate material has become immobilised as a result of encapsulation in some type of biological matrix (Puncher et al., 2017a). (105) More recently, urine and autopsy data from a further two USTUR registrants (Cases 0631 and 0745) have been analysed in studies of plutonium retention in lung tissues (Poudel et al., 2021). The solubility of the inhaled material was assessed to be between that of plutonium nitrates and oxides. These cases show significant plutonium activity remaining in the upper and central respiratory tract in addition to the AI region and the thoracic lymph nodes. Estimated values of fb were 0.01 and 0.04 for Cases 0631 and 0745, respectively. The authors discussed mechanisms other than chemical binding that may account for the long-term retention of plutonium in the upper and central airways. These included encapsulation of particulates in scar tissue (i.e. physical binding) and possible systemic uptake into the lungs. Not knowing the exact mechanism and location of retained material introduces further uncertainty in the lung dose estimates. (106) Any difference between the actual microdistribution of plutonium in human organs and that assumed by dosimetric models can be a significant source of uncertainty. For the Mayak workers, a high plutonium burden was observed in the respiratory tract relative to that in systemic tissues at long times after intake. Hahn et al. (2004) used autoradiography to investigate the distribution of plutonium in the lungs of 24 autopsied Mayak workers. The concentration of plutonium activity was not uniform in the various lung regions, but was significantly less than the average lung concentration in the bronchovascular interstitial tissue of the bronchi and the lumen of the conducting airway, and significantly higher in parenchymal and non-parenchymal scars, with a density of particles approximately 14 times the average of the lung. Similarly, Nielsen et al. (2012) observed long-term retention of plutonium in an autopsied Hanford worker (USTUR Case 0269 mentioned above) to be concentrated in parenchymal scar tissue. Some of the fixed deposit of plutonium in the respiratory tract may therefore correspond to plutonium encapsulated in scar tissue. When this occurs, it introduces another source of uncertainty as the HRTM does not take account of such a process. Furthermore, it is not known whether plutonium encapsulated in scar tissue plays a part in lung carcinogenesis. However, lung cancer may develop from scars and fibrosis resulting from injuries in the AI region (Spencer, 1982, 1985; Yu et al., 2008; Kato et al., 2018). In rats, pulmonary fibrosis also appeared to prolong the retention of plutonium dioxide in the lung, without noticeably changing the risk of the incidence of lung cancer per unit of dose (Lundgren et al., 1991). Regional doses were weighted by their relative sensitivity to radiation-induced cancer (i.e. by their apportionment factors: ABB = 1/3, Abb = 1/3, AAI = 1/3). Calculations were carried out with Mayak Worker Dosimetry System-2013 with the default model parameter values given by Birchall et al. (2017a). Fractional contribution to weighted absorbed lung dose. Doses committed over 50 years.

2.3. Epidemiological studies
(107) The most important cohort regarding the health effects of plutonium exposure is the MWC because of the numbers of workers exposed and the magnitude of the exposures. This cohort and the results obtained are detailed in Section 2.3.1. Several other studies have been conducted, mainly in the UK and the USA. These studies and the results obtained are detailed in Section 2.3.2. (108) Most of the analyses considered the risk of lung cancer specifically, so particular attention is given to lung cancer; however, results related to bone cancer, liver cancer, leukaemia, and other cancers are also considered.
2.3.1. Mayak workers
2.3.1.1. Description of the cohort
(109) The Mayak nuclear complex began operations in 1948 aiming to produce plutonium for the Soviet Union’s nuclear weapons programme. Workers at the Mayak facility were exposed to both external radiation and plutonium (and some other radionuclides), and received doses that were considerably higher than those from similar operations in other countries. (110) The Mayak Worker Registry was established in the mid-1980s and initially included workers in the reactors, the radiochemical plant, and the plutonium production plant hired between 1948 and 1972. The cohort has subsequently been expanded to include workers hired between 1973 and 1982, and workers in auxiliary plants (water treatment and mechanical repair) who were added to increase the number of workers with relatively low doses. The Mayak Worker Registry includes 25,757 workers with data on occupational history, date and place of birth, vital status (known for 94% of workers), and date and cause of death (Koshurnikova et al., 1999). By the end of 2008, 12,338 workers had died. (111) The Mayak Worker Registry includes estimates of annual doses to several organs/tissues of the body from external gamma irradiation, based on film badge data, and from internally deposited plutonium, based on urine measurements. A limitation of the cohort is that only approximately 40% of those who worked in the radiochemical and plutonium plants (and thus had potential for non-trivial plutonium exposure) have the urine measurements needed for internal dose estimation. Since the Mayak Worker Registry was established, both external and internal dose estimates have been improved substantially, resulting in several dosimetry systems as discussed in Section 2.2. The mean estimated lung dose among 6540 workers with positive plutonium exposures (plutonium detected in urine samples) was 0.12 Gy (Gilbert et al., 2013). (112) The plutonium dose–response relationship has been evaluated for cancers of the lung, liver, and bone (i.e. the principal organs/tissues of plutonium deposition), and for leukaemia, originating in RBM adjacent to bone surfaces.
2.3.1.2. Statistical methods
(113) The Mayak Worker Study is a cohort study, and most analyses have been cohort-based with workers followed from the date of their initial employment at Mayak through to the selected end-of-follow-up date. Variables such as attained age, time since exposure, and cumulative doses are allowed to change as workers are followed over time, and are thus considered as time-dependent variables. Analyses rely on internal comparisons in which the risk of lung cancer is compared by levels of external and internal cumulative dose to the lung, rather than comparisons with an external group, such as the Russian general population. Cumulative lung doses are typically lagged by 5 years; that is, at a time t, doses received in the preceding 5 years are excluded to account for the minimum latent period for lung cancer. Most analyses are based on an excess relative risk (ERR) model, with the effects of both external dose and plutonium dose evaluated simultaneously. The ERR model is expressed as follows:
(114) ERR and EAR were commonly expressed as linear functions of dose, although other functions, such as linear-quadratic and linear-exponential, have also been explored. The baseline risk was either modelled as a function of sex, attained age, and other variables (e.g. smoking); or was handled non-parametrically with separate baseline parameters for each stratum defined by these variables. Most recent analyses have assumed a multiplicative relationship for radiation exposure and smoking by including smoking as part of the baseline risk, but departures from a multiplicative relationship have been explored. Models were fitted with either Poisson regression (using the AMFIT module of Epicure) or Cox regression. (115) Dose–response analyses for plutonium have been based solely on that portion of the data for which plutonium doses could be estimated. Thus, in order to contribute to plutonium dose–response analyses, a worker must either have a plutonium urine measurement or have worked solely in the reactor or auxiliary plants with little potential for plutonium exposure; these latter workers were considered as unexposed, and assigned plutonium doses of zero. Primarily for the purpose of obtaining stable estimates of risk from external dose, some analyses have used a plutonium surrogate based on place and time of employment for workers who were not monitored for plutonium but who had potential for non-trivial exposure, possibly substantial; however, this portion of the data does not contribute to the investigation of the plutonium dose–response relationship.


2.3.1.3. Results by site of cancer
(a) Lung cancer
(116) During the past decade, the risk of lung cancer from plutonium exposure has been evaluated by several investigators. The results published since 1998 are summarised in Table 2.2. The earlier lung cancer mortality analyses were based on the Doses-2000 system or earlier dose estimates (Koshurnikova et al., 1998; Kreisheimer et al., 2000, 2003; Gilbert et al., 2004), while more recent analyses have been based on Doses-2005 (Jacob et al., 2007; Sokolnikov et al., 2008), MWDS-2008 (Gilbert et al., 2013; Labutina et al., 2013; Zöllner et al., 2015), or MWDS-2013 (Gillies et al., 2017). Labutina et al. (2013) studied the incidence of lung cancer among workers who were resident at diagnosis in the closed city of Ozyorsk, adjacent to Mayak. The follow-up period for the most recent mortality analysis (Gillies et al., 2017) extends through 2008 (through 2005 for workers who emigrated from Ozyorsk). Historical variations in the number of workers considered in a study are due to different inclusion criteria related to the plant (with or without auxiliary plants) and to the period of exposure (including or not including workers hired before 1973). Analyses by Kreisheimer et al. (2003) and Jacob et al. (2007) were restricted to males with smoking data. The most recent analyses excluded workers followed for less than 5 years as many of these workers were lost to follow-up; however, as no deaths due to lung cancer occurred in this period, this mainly affects the total number of workers reported as contributing to the analysis. Due to differences in the selection of workers, in the follow-up periods, and in the consideration of modifying factors of the dose–risk relationship (recent results are presented for an attained age of 60 years), it is difficult to compare estimated ERR Gy−1 from various analyses. (117) Gilbert et al. (2004) studied lung cancer mortality between 1955 and 2000 among Mayak workers employed between 1948 and 1972, and used early estimates of lung doses from plutonium determined using the methodology of Krahenbuhl et al. (2002), with doses lagged by 10 years (although supplementary analyses were also performed with 5- and 15-year dose lags). ERR Gy−1 estimates for lung cancer mortality and internal dose at an attained age of 60 years, after adjusting for external dose, were 4.7 [95% confidence interval (CI) 3.3–6.7] for males and 19 (95% CI 9.5–39) for females. Adjustment for smoking had little impact on ERR Gy−1 estimates. A highly significant trend of lung cancer mortality ERR was also found using categories of increasing predicted likelihood of inhalation of plutonium for those workers without plutonium monitoring data. (118) The lung cancer mortality analysis of Gilbert et al. (2013) used MWDS-2008 estimates for both internal doses and external doses to the lung. These analyses excluded 1084 workers who either died or were lost to follow-up in the first 5 years, and 10,052 workers (355 lung cancer deaths) who had potential for plutonium exposure but were not monitored for this exposure. The characteristics of the remaining 14,621 workers (10,918 males and 3703 females) are shown in Table 2.3. (119) The mean plutonium dose to the lung among exposed females was higher (0.17 Gy) than that for exposed males (0.09 Gy). Of the 9545 males with smoking data, 74% reported smoking, whereas only 3.5% of the 3163 female workers with smoking data reported smoking. Of the 486 lung cancers that had occurred by the end of 2008, 401 were in male smokers. The dose distribution among the 6540 workers with positive plutonium lung doses is shown in Table 2.4. Only 9% of these workers had plutonium doses exceeding 0.2 Gy, and only approximately 2% had doses exceeding 1 Gy. Nevertheless, the fact that it is not possible to measure the pattern of dose accumulation in individual workers limited the ability to evaluate the potential effects of time since exposure in the MWC. (120) Lung cancer mortality was evaluated using ERR models for lung doses from both internal (plutonium) and external exposure with adjustment for attained age, sex, birth cohort, calendar year period, and smoking, with both internal and external doses lagged for 5 years. Fig. 2.1 shows ERR for lung cancer by plutonium dose category. ERR for lung cancer was reasonably described by a linear function of internal and external doses. The internal dose ERR was higher for females than males, and declined strongly with attained age. At attained age of 60 years, ERR Gy−1 for plutonium dose was 7.4 (95% CI 5.0–11) for males and 24 (95% CI 11–56) for females. A significant dose–response relationship was observed when analyses were restricted to plutonium doses to the lung <0.2 Gy (P < 0.001), with an estimated ERR Gy−1 for males at 60 years of age of 7.0 (95% CI 2.5–13). This estimate was very similar to that for the full dose range, although the CI was wider. (121) Analyses of 12,708 workers with information on smoking indicated that the interaction of plutonium exposure and smoking was greater than additive (P < 0.001) and likely to be submultiplicative (P = 0.011). The estimated ERR Gy−1 for smokers was 6.9 (95% CI 4.6–10), while that for non-smokers was 29 (95% CI 9.8–83). The estimate for non-smokers was based on only 43 lung cancer deaths, and thus was highly uncertain. With modification by smoking accounted for, estimated ERR Gy−1 values for males and females were nearly identical. (122) Labutina et al. (2013) evaluated the incidence of lung cancer among workers employed at Mayak between 1948 and 1982 who were registered as diagnosed with lung cancer before 2005 while residing in Ozyorsk. Doses were based on MWDS-2008, with a dose lag of 10 years. Significant risk-modifying effects were found for attained age and smoking status, but not for sex. For non-smokers at an attained age of 60 years, the modelled ERR Gy−1 was 24 (95% CI <14–>36) for males and 33 (95% CI <22–72) for females. Importantly, data on histological type of lung cancer were available. Significant dose–response relationships were found for male workers for adenocarcinoma, squamous cell carcinoma, and other epithelial lung cancers, with a much larger ERR Gy−1 estimate for adenocarcinomas [33 (95% CI 16–72), when no modifying factors were taken into account] than ERR Gy−1 estimates for other types of lung cancer (Table 2.2). Summary of Mayak lung cancer plutonium dose–response analyses published since 1998. MWDS, Mayak Worker Dosimetry System; ERR, excess relative risk; CI, confidence interval. Workers were either monitored for plutonium or worked solely in the reactor or auxiliary plants with little potential for plutonium exposure. Except for Kreisheimer et al., workers with potential for plutonium exposure had to have been monitored for at least 2 years before the end of follow-up. Little potential for plutonium exposure. Potential exposure to plutonium. ERR Gy−1 is for all ages. Number with plutonium doses of 0, including a few workers in the radiochemical and plutonium plants. Number with positive plutonium doses, including a few workers in the reactor and auxiliary plants. Based on cancer incidence data for workers who were diagnosed with lung cancer in the city of Ozyorsk. ERR Gy−1 estimates are unadjusted for risk-modifying factors. The number of workers contributing to these analyses is not given in the paper. Number of Mayak workers included in analyses of Gilbert et al. (2013) (percentage in parentheses), mean plutonium lung dose, mean external lung dose, and number of lung cancers by sex and smoking status. Based on cumulative dose up to 5 years before the end of follow-up. Distribution of plutonium doses to the lung among 6540 workers with positive doses.
*
Based on cumulative lung dose up to 5 years before the end of follow-up. Excess relative risk (with 95% confidence intervals) of lung cancer and number of lung cancer deaths by categories of plutonium dose to the lung (black points and vertical bars) and fitted linear function for males at 60 years of age (Gilbert et al., 2013).




Analysis performed in the SOLO project
(123) As part of the European Union’s FP7 SOLO (epidemiological studies of exposed (124) The MWC consisted of 22,374 radiation workers first employed at the main plants between 1948 and 1982, of whom 6989 were monitored for exposure to plutonium and 10,397 were potentially exposed to plutonium (possibly heavily) but were not monitored for this exposure; monitoring for exposure to plutonium at Mayak through urinalysis started in approximately 1970. The period of follow-up was terminated at the end of 2008 for Mayak workers who were residents of Ozyorsk, and at the end of 2005 for Mayak workers who had emigrated from Ozyorsk. (125) Overall, there were 789 deaths from lung cancer in the MWC, but only 509 cases of lung cancer were observed due to restriction of the incidence analysis to residents of Ozyorsk. Among those monitored for plutonium exposure, there were 267 cases and 253 deaths from lung cancer (when workers diagnosed with lung cancer within 2 years of first monitoring for plutonium were excluded because of the possibility that monitoring may have occurred because of concerns about the health of a worker). Information on smoking status was not available for this analysis due to the lack of information for Sellafield workers comparable with that available for Mayak workers. (126) ERR with respect to radiation dose to the lung from both external gamma radiation and internal alpha radiation from plutonium was estimated, taking into account all of the available non-radiation factors. Factors affecting background rates were sex, attained age, and birth cohort, and factors affecting the radiation risk estimates were sex and attained age. A dose lag of 10 years was adopted. (127) Uncertainty surrounding the choice of the slow dissolution rate (ss) for plutonium nitrate in the lung meant that two sets of lung doses from plutonium were generated for use in the analyses: those derived from Mayak autopsy cases (ss = 2.5 × 10−4 day−1) and those derived from UK volunteer experiments (ss = 2.2 × 10−3 day−1) (see Section 2.2.4). (128) Lung cancer mortality and incidence from plutonium were found to be significantly increased at relatively high lung doses (for mortality, >200 mGy using ss = 2.5 × 10−4 day−1 and >100 mGy using ss = 2.2 × 10−3 day−1; for incidence, >200 mGy using ss = 2.5 × 10−4 day−1 and >50 mGy using ss = 2.2 × 10−3 day−1). As in previous studies of Mayak workers, the plutonium dose–response relationship for the incidence of lung cancer among male Mayak workers was found to be linear across the whole dose range with ERR Gy−1 estimates of 7.88 (90% CI 5.73–10.65) using ss = 2.2 × 10−3 day−1 and 5.27 (90% CI 3.83–7.12) using ss = 2.5 × 10−4 day−1 at an attained age of 60 years, while for lung cancer mortality among male Mayak workers, estimated ERR Gy−1 values were 7.02 (90% CI 5.23–9.23) using ss = 2.2 × 10−3 day−1 and 4.74 (90% CI 3.53–9.23) using ss = 2.5 × 10−4 day−1 at an attained age of 60 years. ERR Gy−1 point estimates were found to be consistent down to a relatively low lung dose when restricting the range of plutonium dose included in the analysis. For example, in the incidence analysis for Mayak males, a significant ERR Gy−1 estimate was detectable down to 0.05 Gy, and for the mortality analysis for Mayak males, a significant ERR Gy−1 estimate was detectable down to 0.1 Gy, these estimates being positive and consistent with those for the full dose range. (129) For Mayak female workers, ERR Gy−1 at 60 years of age in terms of lung dose from plutonium was 11.62 (90% CI 6.93–18.78) for ss = 2.5 × 10−4 day−1 and 16.11 (90% CI 9.60–26.02) for ss = 2.2 × 10−3 day−1 for lung cancer mortality, and 20.41 (90% CI 11.47–36.04) for ss = 2.5 × 10−4 day−1 and 27.55 (90% CI 15.44–48.61) for ss = 2.2 × 10−3 day−1 for the incidence of lung cancer. (130) Gillies et al. (2017) examined the effect of external irradiation on the risk of lung cancer in the Mayak workforce. For deaths due to lung cancer, ERR Gy−1 (using the ss = 2.5 × 10−4 day −1 solubility assumption) was 0.38 (90% CI 0.22–0.58), while it was 0.30 (90% CI 0.12–0.54) for the incidence of lung cancer; the risk estimates obtained using the ss = 2.2 × 10−3 day−1 solubility assumption were very similar.
(b) Liver cancer
(131) Gilbert et al. (2000) conducted a study of liver cancer mortality before 1997 among Mayak workers employed between 1948 and 1958. Analyses were in terms of plutonium body burden (lagged by 10 years) as organ doses could not be estimated reliably. A highly significant trend of increasing risk of liver cancer mortality with increasing plutonium body burden was reported (based on 36 deaths). Liver cancer mortality risk was also significantly higher for workers from the plutonium production plant who were unmonitored for exposure to plutonium (14 deaths). (132) Dose–response analyses for liver cancer mortality prior to 2004 among workers employed between 1948 and 1972, utilising the Mayak Doses-2005 system (with a dose lag of 5 years), were reported by Sokolnikov et al. (2008) with a linear function providing an adequate fit. ERR Gy−1 for plutonium dose to the liver differed significantly by sex, and was 2.6 (95% CI 0.7–6.9) for males (based on 14 deaths with a non-zero dose estimate) and 29 (95% CI 9.8–95) for females (based on 12 deaths with a non-zero dose estimate), but did not depend on attained age. The association was only apparent for plutonium liver doses in excess of 3 Gy. There was no evidence that ERR Gy−1 depended on attained age. (133) The incidence of liver cancer between 1948 and 2004 was studied by Labutina et al. (2013) using the MWDS-2008 plutonium doses for workers employed between 1948 and 1982, with a dose lag of 10 years. Cases were workers who lived in Ozyorsk at diagnosis. A linear dose–response model gave ERR Gy−1 for plutonium liver dose of 10.6 (95% CI 4.7–30.0) for both sexes combined (32 cases), but a linear-quadratic model provided a significantly better fit, which was due to a marked increase in risk for estimated liver doses >4 Gy. Hepatocellular was the most common type of liver cancer (18 cases) and reflected the notably increased risk at doses >4 Gy that was found for all liver cancers combined, but this pattern of cases by dose group was also present for haemangiosarcoma (eight cases) while none of the six cases of cholangiocarcinoma had a liver dose >0.5 Gy.
(c) Bone cancer
(134) Koshurnikova et al. (2000) studied bone cancer mortality prior to 1997 among Mayak workers employed between 1948 and 1958. Analyses were in terms of plutonium body burden as organ doses could not be estimated reliably, and a 2-year lag period was used. A highly significant increase in bone cancer mortality with increasing plutonium body burden was reported (based on 10 deaths). A highly significant excess of bone cancer deaths occurred among workers in the plutonium production plant who were not monitored for exposure to plutonium (seven deaths). (135) Sokolnikov et al. (2008) reported a significant dose–response relationship for bone cancer deaths before 2004 for workers employed between 1948 and 1972, and based on bone surface doses from Doses-2005 with a 5-year dose lag. ERR Gy−1 did not differ significantly by sex, and for both sexes combined was 1.6 (95% CI 0.3–6.8) based on six deaths with a non-zero dose estimate. However, the evidence for a bone cancer mortality dose–response relationship relied on only three deaths with doses >10 Gy under the Mayak Doses-2005 system: the bone surface doses for these workers were 18 Gy (male), 31 Gy (female), and 69 Gy (female). There was a significant decline in ERR with attained age, with all three deaths occurring before 55 years of age. (136) Labutina et al. (2013) studied the incidence of bone cancer before 2005 in Mayak workers employed between 1948 and 1982 who were resident in Ozyorsk at diagnosis, using plutonium doses to the bone surface given by MWDS-2008 with a 10-year dose lag. Based on 10 cases, there was an indication of increasing risk with increasing plutonium dose, but the trend was not significant with only two cases having doses >1 Gy (one of which had a dose >10 Gy).
(d) Leukaemia and other lymphatic and haematopoietic cancers
(137) Shilnikova et al. (2003) conducted analyses of leukaemia mortality before 1998 in the cohort of 21,557 Mayak workers hired at the main and auxiliary plants between 1948 and 1972 (66 deaths from leukaemia other than CLL). Doses-2000 were used with a 2-year dose lag. Plutonium body burden estimates were used for monitored workers, and a surrogate index of plutonium exposure was used for unmonitored workers. The analyses for non-CLL leukaemia mortality indicated a clear dose–response relationship for external dose with the increased risk notably larger for doses received 3–5 years before death, but there was no evidence of a dose–response relationship for plutonium dose. (138) The incidence of leukaemia between 1948 and 2004 among 22,373 Mayak workers employed between 1948 and 1982 was analysed by Kuznetsova et al. (2016). Doses to RBM were from MWDS-2008 with a 2-year dose lag. For external radiation exposure, ERR Gy−1 for leukaemia excluding CLL (56 cases), after adjustment for the dose from plutonium, was 3.57 (90% CI 1.55–8.22), predominantly due to the risk of acute myeloid leukaemia, with the excess risk concentrated within 5 years of exposure. The preferred dose–response model for leukaemia excluding CLL was quadratic in dose, and included modifying factors to account for increased risk at younger ages at exposure and a decreasing risk with increasing time since exposure; the model gives ERR at 1 Gy of 0.52 (90% CI 0.16–1.26) 25 years after exposure for an age at first exposure of 25 years. In contrast, for plutonium exposure, there was no clear increase in the risk of leukaemia excluding CLL, after adjustment for the dose from external radiation, with ERR Gy−1 of 3.63 (90% CI <0–15.85). No significant increase in risk was found for workers who were unmonitored for exposure to plutonium but who were employed in the early years of operation at Mayak in those facilities in which exposure to substantial quantities of plutonium was most likely. There was little indication of excess risk of lymphoma or multiple myeloma associated with exposure to either external radiation or plutonium. (139) Although leukaemia mortality and incidence in the Mayak and Sellafield workforces was part of the SOLO study, the results of the leukaemia component of this study have yet to be published.
(e) Other cancers
(140) Shilnikova et al. (2003) studied 1062 deaths from solid cancers other than cancers of the lung, liver, and bone (sites of major plutonium deposition) before 1998 among 21,557 Mayak workers employed between 1948 and 1972. Doses-2000 was used with a 5-year dose lag. For external dose, a significant downward curvature in the dose–response relationship was found with ERR Gy−1 at low doses, adjusted for plutonium exposure, of 0.21 (90% CI 0.06–0.37). Some evidence was found for an effect of plutonium exposure on the risk of other solid cancer mortality when a combination of body burden data for monitored workers and surrogate exposure categories for unmonitored workers was used. (141) Cancer incidence data were analysed to investigate the association between doses from external gamma-ray and internal plutonium exposures and the risk of solid cancers other than lung, liver, and bone (Hunter et al., 2013). Included were 22,366 Mayak workers first employed between 1948 and 1982. MWDS-2008 was used with various lag periods, although most results were presented for no lag. A total of 1447 cases of other solid cancers were registered in the follow-up period until 2004. A weak association was found between cumulative dose from external gamma rays and the incidence of solid cancers other than lung, liver, and bone [ERR Gy−1 = 0.07 (95% CI 0.01–0.15)], but this association lost its significance after adjusting for internal plutonium dose [ERR Gy−1 = 0.06 (95% CI −0.01 to 0.14)]. There was no significant association with plutonium liver dose [ERR Gy−1 = 0.10 (95% CI −0.02 to 0.26)] or with potential plutonium exposure in unmonitored workers. The study provides only weak evidence of an increased risk of plutonium exposure for solid cancers other than lung, liver, and bone (Hunter et al., 2013). (142) Mortality from solid cancers other than lung, liver, and bone was analysed by Sokolnikov et al. (2015a). The cohort under study included 25,757 workers from the main (reactor, radiochemical, and plutonium production) as well as auxiliary (water treatment and mechanical repair) plants employed between 1948 and 1982. The analyses used MWDS-2008 (with colon doses lagged by 5 years) and an extended follow-up until 2008, and included 1825 deaths from other solid cancers. A linear dose–response relationship with exposure to external gamma rays provided the best fit to the data: ERR Gy−1 = 0.16 (95% CI 0.07–0.26) when unadjusted for plutonium exposure and ERR Gy−1 = 0.12 (95% CI 0.03–0.21) when adjusted for plutonium dose and monitoring status. Cancer of the oesophagus was notably raised in relation to external dose: ERR Gy−1 = 1.26 (95% CI 0.36–3.27). The background mortality rate for other solid cancers was significantly higher among those who had been monitored for plutonium [relative risk (RR) 1.16, 95% CI 1.11–1.39] compared with workers not monitored for plutonium, and when this difference with respect to monitoring status was taken into account, the dose–response relationship using plutonium liver dose had a positive slope that was not significant. The authors concluded that while there was some evidence of an excess risk associated with inhalation of 239Pu for mortality from solid cancers other than lung, liver, or bone, this may have been largely due to factors related to the selection of subjects for plutonium monitoring (Sokolnikov et al., 2015a). A subsequent study (Sokolnikov et al., 2017) examined groups of Mayak workers with different likelihoods of exposure to substantial quantities of plutonium, and found no evidence that plutonium exposure affected the risk of other solid cancers or the risk of these cancers associated with external exposure.
2.3.2. Other plutonium worker cohorts
2.3.2.1. Description of epidemiological studies
(143) Table 2.5 summarises the characteristics of the cohort and case–control studies allowing quantification of the risk of cancer based on individual estimates of plutonium exposure using measurements or job-exposure matrices. Summary of studies of occupational exposure to plutonium and cancer among workers other than the Mayak workforce. AWE, Atomic Weapons Establishment; BNFL, British Nuclear Fuels Ltd; CEA, Commissariat à l’Energie Atomique; CLL, chronic lymphocytic leukaemia; n.a., not available; UKAEA, UK Atomic Energy Authority; MoS, Ministry of Supply; WBC, whole-body counting; Y, yes; N, no.

UK studies
(144) The studies of Omar et al. (1999), McGeoghegan et al. (2003), and Gillies and Haylock (2014) reported on cancer mortality and incidence among Sellafield workers. Omar et al. (1999) included 14,319 male and female workers. They classified 5203 workers as plutonium workers because urine samples for plutonium monitoring were available for them, among which there were 839 females. Two methods were used to assess plutonium uptake for these workers: individual assessments and standard assessments. For the 993 workers involved in an exposure incident or compensation claim, individual assessments were performed by a health physicist using urine assays, full work history records, and the circumstances of known acute exposure incidents. Standard assessments were performed for 3616 workers using urine assays, and assuming plutonium exposure started 6 months prior to the date of first urine sampling and ended on the date of the last sampling. No assessment was performed for the remaining 594 workers who were known to have been potentially exposed to plutonium but had limited or no usable urine data. Organ/tissue doses were calculated for the 4609 workers with adequate plutonium urine monitoring records; these plutonium doses were added to external doses in the analyses of trends of risk with cumulative dose, but separate analyses in terms of plutonium dose alone were not conducted. McGeoghegan et al. (2003) restricted their study to 5618 female workers, of whom 837 were identified as plutonium workers. Among these 837 females, 643 had at least five urine samples so that estimates of assessed organ-/tissue-specific plutonium doses could be calculated. Detectable plutonium burdens were found for 360 workers. A detailed description of how the organ-/tissue-specific plutonium doses were calculated for the Sellafield workers can be found in Section 2.2.5. Gillies and Haylock (2014) calculated standardised mortality ratios (SMRs) for 12,272 Sellafield workers monitored for exposure to plutonium and followed-up to the end of 2005. For these Sellafield worker studies, the SMRs for plutonium workers were calculated and compared with those for other Sellafield workers. (145) Atkinson et al. (2004) studied mortality among 51,397 UKAEA workers. The effect of plutonium exposure was evaluated by stratifying workers into ever/never monitored for plutonium based on the presence or absence of records documenting a worker being monitored for plutonium exposure. Cumulative external radiation exposure included exposure at the study site plus other sites when the exposure was known and occurred prior to employment at the site. In addition, the external exposure measures included tritium and neutron exposures, and were adjusted for subthreshold and missing readings. Plutonium-specific doses were not calculated. (146) The SWC has also been analysed in the framework of the European Union SOLO project (Gillies et al., 2017) to study lung cancer and leukaemia mortality and incidence, and circulatory disease mortality, in the Mayak and Sellafield workforces. The SWC consisted of 23,443 radiation workers first employed between 1947 and 2002, of whom 12,192 had ever been monitored for exposure to plutonium, including 1815 females. The period of follow-up was terminated at the end of 2005. Overall, there were 384 cases of lung cancer and 406 deaths from lung cancer in the SWC. Among those monitored for plutonium exposure, there were 220 cases of lung cancer and 225 deaths from lung cancer. ERR with respect to radiation dose from both external gamma radiation and internal alpha radiation to the lung from plutonium was estimated, taking into account all of the available non-radiation factors: factors affecting background rates were sex, attained age, and birth cohort; and factors affecting the radiation risk estimates were sex and attained age. Uncertainty surrounding the choice of the lung solubility parameter for plutonium nitrate led to two sets of lung doses from plutonium being generated for use in the analyses: those derived from Mayak autopsy cases (ss = 2.5 × 10−4 day−1) and those derived from UK volunteer experiments (ss = 2.2 × 10−3 day−1).
US studies
(147) The cohort study of 26,389 Hanford workers employed for at least 6 months between 1944 and 1978 (Wing et al., 2004) focused on mortality and length of employment in jobs with potential for plutonium exposure. Deaths before 1995 were identified. A job-exposure matrix was used to stratify each year of a worker’s employment into one of three categories of potential for plutonium exposure: minimal, non-routine, and routine. The three-dimensional matrix was developed using facility information on job title, area/process, and time period. The records for the 377 workers (1.4% of the workers studied) with documented systemic plutonium deposition were used to test the ability of the matrix to identify workers with documented contamination. The average length of follow-up exceeded 22 years for the three groups where this information was available. Although these three groups were relatively large, the number of workers identified as exposed to plutonium was considerably less: 3065 and 8266 individuals were identified as routinely exposed and non-routinely exposed, respectively. (148) Wiggs et al. (1994) studied 15,727 white males employed for any length of time at Los Alamos between 1943 and 1977, and examined mortality rates to the end of 1990, particularly in relation to cumulative systemic plutonium deposition calculated from urinalysis results. The 303 workers with cumulative systemic plutonium deposition ≥74 Bq (when lagged by 10 years) were compared with 3472 workers with plutonium deposition <74 Bq. Voelz et al. (1997) studied 26 workers who were employed in the Manhattan Project at Los Alamos between 1944 and 1945, and were highly exposed to plutonium. (149) Wilkinson et al. (1987) studied 5413 white males employed for at least 2 years at Rocky Flats between 1952 and 1979. They examined mortality to the end of 1979, particularly in relation to cumulative systemic plutonium deposition calculated from urinalysis results. Mortality rates for workers with cumulative systemic plutonium deposition (lagged by 10 years, or 2 years for leukaemia) <74 Bq were compared with rates for workers with deposition ≥74 Bq, and for all cancers and lung cancer for depositions of 74–184 Bq and ≥185 Bq. (150) Three case–control studies conducted in the USA considered various cancer outcomes. Wing et al. (2000) studied 98 cases (and 391 matched controls) of multiple myeloma mortality among workers hired before 1979 at four US nuclear facilities (Hanford, Los Alamos, Oak Ridge, and Savannah River) with a potential for external exposure and an absence of major radioactive dust exposure. Cause of death before 1991 (1987 for Hanford) was identified in a total of 115,143 workers. Bioassays of urine and faecal samples, and whole-body counting records were used to stratify workers according to monitoring for internal radiation exposure, which included plutonium, uranium, strontium, and tritium. External exposure estimates included tritium and neutrons. (151) Schubauer-Berigan et al. (2007) conducted a case–control study of non-CLL leukaemia mortality (206 cases and 823 controls) among workers at the same four US nuclear facilities as Wing et al. (2000), plus the Portsmouth Naval Shipyard. Cause of death before 1995 (1997 for Portsmouth) was identified among a total of 94,517 workers employed for at least 30 days before 1979 or 1978 (1975 for Savannah River), and monitored for exposure to radiation. Bone marrow doses were determined for each study member using external radiation exposure to photons, neutrons, and tritium; occupational medical x rays; and plutonium urine measurements. Urinary excretion data were used to estimate potential systemic plutonium deposition. Four categories were defined based on the highest reading of plutonium excretion measured in mBq day−1. Over half of the cases (58%) and controls (54%) had no available bioassay records. Bone marrow doses were calculated using current ICRP biokinetic models and default parameters. Three assumptions were made: inhalation was the route of entry; intakes occurred 3 days before the first associated positive bioassay sample; and the solubility of the inhaled material was 50% Type M and 50% type Y (Daniels et al., 2006). (152) In their lung cancer mortality nested case–control study of 180 cases and 720 matched controls among 16,258 Rocky Flats workers employed for at least 6 months between 1952 and 1989, Brown et al. (2004) calculated dose to the lung using recorded external exposure to gamma radiation and neutrons; urine bioassays for plutonium and uranium; lung count data for plutonium, uranium, and their decay products; and inferred doses from 241Am based on estimated intake of 241Pu (Ruttenber et al., 2001). For external doses, gamma and neutron doses were recorded as a combined dose. Missing doses for 1 year or more were imputed for 51.7% of cases and 58.9% of controls. For internal doses, effective intakes and annual equivalent doses were estimated using the Code for Internal Dosimetry, Version 1.3 which was based on Publication 30 (ICRP, 1979). Smoking histories were obtained from interviewing relatives (80% of histories) and co-workers, and medical records; smoking information was obtained for 68% of cases and 84% of controls.
Combined analysis of Mayak and Sellafield plutonium workers (European Union SOLO project)
(153) To date, evidence of the risk of lung cancer and other cancers in relation to plutonium exposure has been mostly based on findings from the MWC. However, the scale of the exposures and the different dose assessment methodology used in the MWC meant that there was considerable uncertainty about whether the risks derived from this cohort could be extrapolated to low doses and were applicable to other cohorts. The SWC represents one of the few available companion cohorts with individual plutonium monitoring data available over a long follow-up period, with approximately 500,000 urine sample results available for over 12,000 plutonium-monitored workers covering the low dose range. The MWC and SWC therefore represent complementary resources for studying the health effects associated with plutonium exposure. The combination of these cohorts using a unified dosimetry methodology has enabled the study of plutonium risks over a wider dose range than could be managed in the MWC alone (Gillies et al., 2017). (154) The combined MWC and SWC includes 45,817 workers hired in the main facilities of Mayak PA (i.e. reactor, radiochemical, and plutonium production plants) in 1948–1982 or at Sellafield in 1947–2002. The pooled cohort includes a total of 1195 lung cancer deaths. Levels of plutonium intake in the MWC were much higher, with the SWC data contributing mainly to the lower dose range. (155) Analyses in terms of both lung cancer mortality and incidence were conducted (Gillies et al., 2017). One particular feature of these analyses is that the alpha-particle dose to the lung was calculated twice, using different parameter values describing the rate of plutonium absorption from the lung (see Section 2.2.4). This is due to dosimetric differences between the MWC and the SWC that could not be resolved in the timescale required for the epidemiological analyses. (156) Smoking information was available for the MWC alone, and so could not be used in the combined analysis. However, from analysis of the background (i.e. in the absence of radiation exposure) lung cancer mortality rates, it was clear that smoking rates in the SWC were lower than in the MWC.
European combined analysis of plutonium workers (Alpha-Risk project)
(157) In the Alpha-Risk project (Bingham et al., 2017; Grellier et al., 2017), funded by the European Union (EU), lung cancer and leukaemia mortality risks associated with internal exposure to plutonium and uranium were investigated through a case–control study nested within radiation worker cohorts in the UK (AWE, UKAEA, and BNFL cohorts), Belgium (SCK•CEN/BN cohort), and France (CEA-COGEMA cohort). The case–control design allowed detailed dose reconstruction as well as the collection of individual data on potential confounders (Grellier et al., 2017).
2.3.2.2. Results by site of cancer
Lung cancer
(158) Studies of the risk of lung cancer associated with plutonium exposure (other than Mayak workers) are summarised in Table 2.6. Summary of results of epidemiological studies of plutonium-exposed populations (other than Mayak workers) for the risk of lung cancer. n.a., not available; ERR, excess risk ratio; EOR, excess odds ratio; SE, standard error; SIR, standardized incidence ratio; SMR, standardized mortality ratio; CI, confidence interval. At 60 years of age.

UK studies
(159) In the studies of Sellafield workers, the ‘healthy worker effect’ was seen for both lung cancer mortality and incidence (Omar et al., 1999; McGeoghegan et al., 2003; Gillies and Haylock, 2014). The average lung dose from plutonium was 194 mSv and from external radiation was 196.7 mSv. No dose–response relationship was observed with cumulative plutonium dose plus external radiation for lung cancer mortality or incidence among plutonium workers (Omar et al., 1999). McGeoghegan et al. (2003) failed to find a dose–response relationship with cumulative plutonium dose among female workers, although the numbers were small. (160) The EU SOLO project examined lung cancer mortality and incidence in Sellafield workers (Gillies et al., 2017); there were 384 cases of lung cancer and 406 deaths from lung cancer. (161) For lung cancer mortality and incidence, there was no consistent pattern of significantly increased risk by plutonium lung dose group for either ss = 2.5 × 10−4 day−1 or ss = 2.2 × 10−3 day−1 dissolution rate, although point estimates of lung cancer ERR were positive for all dose groups for both mortality and incidence for both solubility assumptions. Estimates of ERR Gy−1 of lung dose from plutonium at 60 years of age were non-significantly positive for both lung cancer mortality and incidence: for mortality, ERR Gy−1 was 6.34 (90% CI <−1.6 to 18.8) for ss = 2.5 × 10−4 day−1 and 20.60 (90% CI <−1.5 to 58.6) for ss = 2.2 × 10−3 day−1; and for incidence, ERR Gy−1 was 8.14 (90% CI <−1.21 to 21.17) for ss = 2.5 × 10−4 day−1 and 27.00 (90% CI <−2.06 to 67.6) for ss = 2.2 × 10−3 day−1 (Gillies et al., 2017). (162) Lung cancer mortality and incidence were also examined with respect to external exposure. For lung cancer mortality, ERR Gy−1 was 0.22 (90% CI −0.25 to 0.82) for ss = 2.5 × 10−4 day−1 and 0.18 (90% CI −0.27 to 0.78) for ss = 2.2 × 10−3 day−1, while for incidence, ERR Gy−1 was 0.25 (90% CI −0.23 to 0.88) for ss = 2.5 × 10−4 day−1 and 0.22 (90% CI −0.26 to 0.84) for ss = 2.2 × 10−3. The pattern of these risk estimates was consistent with that obtained for the plutonium alpha-particle dose to the lung in the Sellafield workers (see above); ERR Gy−1 estimates were positive, but not significantly so (Gillies et al., 2017).
US studies
(163) In their study of Hanford workers, Wing et al. (2004) focused on workers in jobs with routine potential for plutonium exposure. They found a positive relationship between such jobs and risk of lung cancer: the increase in lung cancer mortality was 2.0% [standard error (SE) = 1.8] for each year employed in a job with routine potential for plutonium exposure. The risk for age <50 years was −1.0% (SE = 2.7), while the risk for age ≥50 years was 7.1% (SE = 3.4). (164) Wiggs et al. (1994) studied workers at Los Alamos, particularly in relation to cumulative systemic plutonium deposition. For 303 workers with cumulative systemic plutonium deposition ≥74 Bq (when lagged by 10 years), the mortality rate ratio (RR) for lung cancer with respect to 3472 workers with plutonium deposition <74 Bq was 1.78 (95% CI 0.79–3.99). Voelz et al. (1997) found one lung cancer death in the 26 Manhattan Project workers highly exposed to plutonium during the Second World War, which was less than that expected from national rates; RR when compared with the lung cancer mortality rate among 876 unexposed Los Alamos male workers employed between 1944 and 1945 was 3.31 (95% CI 0.44–25). (165) Wilkinson et al. (1987) reported a significantly low SMR for lung cancer in the Rocky Flats workforce [SMR = 0.64 (95% CI 0.46–0.87)]. The RR when the lung cancer mortality rate in plutonium-exposed workers (≥74 Bq systemic deposition) was compared with that for unexposed workers (<74 Bq), with a lag period of 10 years, was 1.43 (95% CI 0.33–4.65), but the RR for the highest exposed group (≥185 Bq) was 0.63 (CI not given). (166) Brown et al. (2004) and Brown and Ruttenber (2005) presented results from a lung cancer mortality nested case–control study of Rocky Flats workers. The risk of lung cancer with respect to internal lung dose (lagged by 10 years) was reported. Odds ratios (ORs) (adjusted for cumulative external dose, period of joining, and duration of employment) were elevated for all five non-zero categories of cumulative internal lung dose, with ORs being greatest for intermediate dose groups and significant for the middle 21–32-mGy category. There was a significant reduction in OR with duration of employment. The ORs for two non-zero external dose categories were non-significantly less than 1.0. With a further adjustment for the number of years of non-zero internal lung dose (to address uncertainties in the dosimetry methodology), significantly elevated ORs were found for all five internal lung dose categories; there was a significant reduction in OR with increasing number of years of non-zero internal lung dose. Additionally, adjusting for age at first estimate of lung dose for those workers with a non-zero internal lung dose reduced the ORs so that none were significant, but the effect of age at first internal lung dose was significant [observed deaths (O) = 98; OR = 1.05, 95% CI 1.01–1.10]; this adjustment for age at first internal lung dose had the effect of notably increasing the ORs for the external dose categories, but no OR was significantly different from 1.0. A significant positive linear trend with internal lung dose was found for workers employed for 15–25 years (P < 0.001), but for those workers employed for <15 years or for >25 years, ORs for most internal lung dose categories were <1.0 and none were significant. Brown et al. (2004) stated that the inclusion of smoking data for 730 subjects with such information ‘did not confound by 10 percent or greater the relation between cumulative lung dose and lung cancer’, but gave no details, so smoking histories were not included in the final models (Brown and Ruttenber, 2005).
Combined analysis of Mayak and Sellafield plutonium workers (European Union SOLO project)
(167) The EU SOLO project conducted a joint analysis of the SWC and MWC. Analyses in terms of both lung cancer mortality and incidence demonstrated a clear effect of exposure to alpha particles emitted by plutonium on both outcomes with the incidence ERR Gy−1 being somewhat higher than the mortality ERR Gy−1. The pattern of the dose–response relationship showed no indication of non-linearity or significant differences between cohorts, although the results were clearly dominated by the MWC data. (168) Trends in background age-related rates of lung cancer morbidity and mortality were comparable between the SWC and MWC, but a difference was observed in variation in background by year of birth or the calendar period. However, information about smoking status was not available in the framework of this analysis, and the differing smoking habits in the UK and the Russian Federation may well explain these differences in birth cohort effects. (169) ERR associated with radiation dose of both external gamma radiation and internal alpha radiation from plutonium was estimated, taking into account all of the available non-radiation factors: factors affecting background rates were cohort (i.e. MWC and SWC), sex, attained age, and birth cohort; and factors affecting the radiation risk estimates were sex and attained age. The pooled radiation risk analysis, in terms of the cumulative internal alpha-radiation dose to the lung from plutonium, revealed compatible ERR Gy−1 estimates to those obtained for the two cohorts separately. (170) Examination of the plutonium dose–response relationship for the incidence of lung cancer found significantly increased risks at relatively low doses for the SWC of 2–5 and 5–10 mGy using the Mayak lung solubility assumption (ss = 2.5 × 10−4 day−1), and 1–2, 10–20, and ≥20 mGy using the Sellafield lung solubility assumption (ss = 2.2 × 10−3 day−1). In the MWC, an increased risk was only observed at relatively high doses (200–500 mGy using ss = 2.5 × 10−4 day−1 and 50–100 mGy using ss = 2.2 × 10−3 day−1). As in previous MWC studies, the plutonium dose–response relationship was found to be linear across the whole dose range, and ERR Gy−1 point estimates were found to be consistent down to relatively low doses when restricting the range of plutonium dose included in the analysis. For example, in the incidence analysis, a significant pooled ERR Gy−1 estimate was detectable at relatively low levels (0.2 Gy when using ss = 2.5 × 10−4 day−1 and 0.1 Gy when using ss = 2.2 × 10−3 day−1), with positive ERR Gy−1 point estimates down to 0.05 Gy and consistent with the overall estimate. (171) Study of potential effect modifiers on the plutonium ERR Gy−1, such as attained age, sex, and age at first plutonium exposure, was hampered by the lack of power in the SWC. For the MWC and, as a consequence, for the pooled cohort, it was found that sex and attained age were significant factors affecting the value of estimated ERR Gy−1. Sex significantly modified the plutonium ERR Gy−1 estimate in the MWC, with the risk of incidence being four times higher in Mayak females than Mayak males, and the risk of mortality being two to three times higher in Mayak females than Mayak males. The SWC male ERR Gy−1 estimate was compatible with that of the MWC males, but the number of female lung cancers was very low (10 deaths, eight incident cases) in the SWC, and models that allowed estimated ERR Gy−1 to vary by sex within the SWC converged poorly. In relation to attained age, a declining pattern in the plutonium ERR Gy−1 estimate with increasing attained age was observed in both cohorts, and although the power to detect this effect in the SWC was lower, the scale of this effect was very similar in both cohorts {e.g. for the incidence of lung cancer using ss = 2.2 × 10−3 day−1, the age effect was Exp[−3.04 × log(age/60)] for the MWC and Exp[−5.85 × log(age/60)] for the SWC}.
Combined analysis of European plutonium workers (Alpha-Risk project)
(172) Grellier et al. (2017) obtained a lung cancer mortality excess odds ratio (EOR) Gy−1 of lung dose from plutonium for the BNFL workforce (median lung dose in 232 controls of 0.85 mGy) of 48.8 (90% CI <0–195); these BNFL workers received their plutonium exposures at Sellafield. In comparison, in the SOLO project, Gillies et al. (2017) reported a lung cancer mortality ERR Gy−1 for Sellafield workers at an attained age of 60 years, using the ss = 2.2 × 10−3 day−1 solubility assumption, of 20.6 (90% CI <−1.5 to 58.6). ERR Gy−1 point estimates for the Sellafield workforce obtained from the SOLO and Alpha-Risk studies differ by a factor of >2, although it should be noted that lung doses will have been estimated on the basis of different dosimetry systems. These estimates are statistically compatible and also have wide CIs that include 0 (i.e. are statistically consistent with no excess risk). (173) Grellier et al. (2017) found a lung cancer mortality EOR Gy−1 of lung dose from plutonium for all workers included in the Alpha-Risk study (median lung dose in 463 controls of 1.25 mGy) of 49 (90% CI 16–106). There was little variation in estimated EOR Gy−1 when each contributing cohort was removed from the analysis: when the BNFL workforce was excluded, EOR Gy−1 was 50 (90% CI 15–117), and the lowest estimated EOR Gy−1 was obtained when the AWE cohort (median lung dose in 133 controls of 6.06 mGy) was removed [37 (90% CI 0.18–121)]. (174) An unusual finding of Grellier et al. (2017) was that lung cancer mortality associated with external dose for the BNFL workforce (median dose in 960 controls of 38.84 mGy) was borderline significantly negative, with EOR Gy−1 of −0.46 (90% CI <0–0.16). This compares with the equivalent external exposure ERR Gy−1 for the Sellafield workforce (all attained ages) obtained by Gillies et al. (2017) in the SOLO project using the ss = 2.2 × 10−3 day−1 solubility assumption (median external dose of 16.2 mGy) of 0.18 (90% CI −0.27 to 0.78). For all workers included in the Alpha-Risk study, the estimated risk of lung cancer associated with gamma radiation dose (median dose in 1264 controls of 33.86 mGy) was EOR Gy−1 of −0.44 (90% CI −0.6 to 0.04), which contrasts with the strong positive association estimated with the plutonium alpha-particle lung dose [49 (90% CI 16–106) (median lung absorbed dose of 1.25 mGy)] (Grellier et al., 2017).
Liver cancer
(175) Other studies (apart from the Mayak studies) have reported results related to liver cancer and plutonium exposure. Among 5203 Sellafield plutonium workers employed between 1947 and 1975 and followed-up to 1992, Omar et al. (1999) found one death from liver and gallbladder cancer when 5.08 deaths were expected from national rates (SMR = 0.19, P < 0.01). No incident cases (between 1971 and 1986) were reported while 3.13 were expected. In a later study, Gillies and Haylock (2014) found 15 deaths from, and 30 cases of, liver and gallbladder cancer among 12,272 plutonium workers employed at Sellafield between 1947 and 2002 and followed-up to 2005, generating a non-significantly raised SMR of 102 and a standardised incidence ratio (SIR) of 108. The ratio of the SMR with respect to that for workers monitored for exposure to external sources of radiation alone was significantly raised (P < 0.05) at 2.49, but the ratio of SIRs was non-significantly increased at 1.81. (176) In the USA, Wiggs et al. (1994) found 15 liver cancer deaths among 15,727 white male workers employed at Los Alamos, which was below the number expected from national rates, and none of these deaths occurred among 303 highly exposed plutonium workers. Of 5413 white male workers at Rocky Flats, three deaths from liver and gallbladder cancer were found (a non-significantly raised SMR of 139), but none of these deaths occurred among plutonium workers with estimated cumulative systemic deposition (lagged by 10 years) of ≥74 Bq (Wilkinson et al., 1987).
Bone cancer
(177) Omar et al. (1999), McGeoghegan et al. (2003), and Gillies and Haylock (2014) reported results for bone cancer, and found no deaths among Sellafield plutonium workers. Omar et al. (1999) and McGeoghegan et al. (2003) found no cases of bone cancer, and Gillies and Haylock (2014) reported two cases. As this is a relatively rare cancer, no deaths or cases were expected among the females included in the study of McGeoghegan et al. (2003), and only 1.1 deaths and less than one case were expected among the Sellafield workers included in the study of Omar et al. (1999). The two cases included in the study of Gillies and Haylock (2014) gave a SIR of 94. (178) In the USA, Voelz et al. (1997) reported a single death from bone cancer among 26 white males who had been highly exposed to plutonium during the Manhattan Project at Los Alamos during the Second World War. However, the number of deaths expected from national rates among such a small number of males was very small, so that even one death represented a highly significant excess (P < 0.01). The cumulative dose to the bone surface from plutonium for this man was calculated to be 0.44 Gy. Wiggs et al. (1994) reported that this death from bone cancer was the only death before 1991 among 303 highly exposed plutonium workers from Los Alamos. Wilkinson et al. (1987) found no deaths from bone cancer in 5413 white male workers at Rocky Flats.
Leukaemia and other lymphatic and haematopoietic cancers
(179) For Sellafield, Omar et al. (1999) and McGeoghegan et al. (2003) found that plutonium workers had fewer deaths from, and incident cases of, leukaemia than expected compared with the national population, although Gillies and Haylock (2014) found that the rates of leukaemia deaths or cases in Sellafield plutonium workers were approximately the same as those of the national population. With a 2-year lag, Omar et al. (1999) found no significant dose–response relationship between non-CLL leukaemia mortality or incidence and total (external plus plutonium) RBM dose, which averaged 51 mSv for plutonium workers. Among females, McGeoghegan et al. (2003) also failed to find a dose–response relationship for the risk of leukaemia, with an average cumulative external dose of 23.3 mSv and an assessed internal lung dose of 3.45 mSv (taken as a surrogate for RBM dose from plutonium, which was not given). (180) Only one significant result was reported, which was that for combined lymphatic and haematopoietic cancers. Contrary to what they found for leukaemia, Omar et al. (1999) found a significant trend with cumulative plutonium plus external radiation dose for incidence of all lymphatic and haematopoietic cancers among plutonium workers using a lag of 0, 10, or 20 years. Omar et al. (1999) reported that the association was also present for plutonium dose alone; this positive trend was due largely to two cases with cumulative plutonium doses >400 mSv, one case of Hodgkin’s lymphoma and one of multiple myeloma. (181) Leukaemia mortality and incidence in the Sellafield workforce was also a subject of study in the EU SOLO project examining the combined MWC and SWC. However, the leukaemia component of the SOLO study has yet to be reported. (182) In the USA, in their case–control study of non-CLL leukaemia, Schubauer-Berigan et al. (2007) found a positive relationship between the risk of leukaemia and total dose to RBM [ERR = 4.0 Sv−1 (95% CI −1.0 to 9.4)], but it was not significant. The average cumulative RBM dose of 30.6 mSv among cases was only slightly higher than that of 24.9 mSv among controls. (183) The component of the EU Alpha-Risk case–control study that examined leukaemia mortality has yet to be published.
Other cancers
(184) Apart from lung cancer, the only other noteworthy result for respiratory cancers was reported for pleural cancer. Among British UKAEA workers monitored for plutonium, the SMR for pleural cancer when exposure was lagged by 10 years was 392 (95% CI 106–768), and the mortality rate was significantly higher than that for other radiation workers (RR = 6.7; 95% CI 1.5–28.5), but there was a (non-significant) negative trend with external radiation dose (Atkinson et al., 2004). Omar et al. (1999) found a significant SMR of 471 [P < 0.001; O = 8, expected deaths (E) = 1.70] for plutonium workers at Sellafield, but RR when this SMR was compared with the significantly (P < 0.05) raised SMR of 390 for other radiation workers at Sellafield was 1.15 (not significant); no dose–response relationship was found for pleural cancer mortality and cumulative plutonium dose combined with external radiation exposure. The average dose to soft tissue for plutonium workers was 1.7 mSv. Given the strong association between pleural cancer and exposure to asbestos, it seems likely that the increased SMRs are due to asbestos exposure rather than plutonium exposure (Omar et al., 1999; Atkinson et al., 2004). (185) Among the UKAEA workers, Atkinson et al. (2004) reported an increased SMR for uterine cancer among female workers monitored for plutonium (SMR = 669, 95% CI 134–1955). Restricting the uterine cancers to those of the endometrium increased SMR to 1538 (95% CI 173–5555) and RR to 56.6 (95% CI 8.3–infinity) when compared with other radiation workers; the number of deaths was three and two, respectively. There was a (non-significant) negative trend with external dose. (186) For all Sellafield workers, Omar et al. (1999) reported a negative trend of all cancer mortality with cumulative plutonium effective dose plus external radiation dose assuming W class for plutonium. They found an elevated SMR of 144 (P < 0.05) compared with the general population, and RR of 1.90 (P < 0.05) among plutonium workers compared with other radiation workers for mortality from ill-defined and secondary cancers; no dose–response relationship was found for cumulative combined plutonium and external dose. Omar et al. (1999) reported a significant positive association between the incidence of pancreatic cancer and cumulative plutonium dose alone when the dose was lagged by 10 years. Among female Sellafield workers, McGeoghegan et al. (2003) found a significantly increased RR for mortality from all cancers in plutonium workers compared with other radiation workers. With the SMR for plutonium workers only slightly, and non-significantly, elevated (SMR = 113), this excess was attributed to a deficit of cancers among the other radiation workers (SMR = 51). Neither the standardised registration ratio (SRR) for all cancer incidence nor the RR when compared with the SRR for other radiation workers differed significantly from the null. No significant dose–response relationship was found with either cumulative plutonium dose or external radiation dose. (187) An increase in breast cancer among Sellafield workers was reported by both Omar et al. (1999) and McGeoghegan et al. (2003). Omar et al. (1999) found a significant increase in mortality among plutonium workers based on six deaths, with SMR of 236 (P < 0.05) compared with the general population and RR of 7.66 (P < 0.01) compared with other radiation workers. This elevated RR was driven by a deficit of breast cancer deaths among radiation workers (SMR = 34, O = 2, E = 5.92, P < 0.05). Mortality risk among plutonium workers did not vary significantly with cumulative plutonium dose to soft tissues plus external radiation dose. No significant excess was found for cancer incidence (SRR = 121, O = 4, E = 3.32). In the study by McGeoghegan et al. (2003) of female Sellafield workers, similar results were found: SMR was 197 (O = 7, E = 3.50) among plutonium workers, while RR decreased to 3.77 (P < 0.05) but remained significant. As in the study of Omar et al. (1999), there was a deficit of breast cancer deaths among the other radiation workers (SMR = 54, O = 5, E = 9.3). For incidence, SRR was 144 (O = 10, E = 6.9) and RR was 3.34 (P = 0.013), which again was driven by a deficit of incident cases among other radiation workers (SRR = 69, O = 12, E = 17.3); no dose–response relationship was seen with cumulative plutonium dose. McGeoghegan et al. (2003) noted that for one of the breast cancer deaths included in the study of Omar et al. (1999) as occurring in a plutonium worker, urine samples were only taken after the diagnosis (and were found to be below the detection limit); if this death was excluded, the SMR was no longer significantly elevated (O = 5, E = 1.15).
Environmental exposure to plutonium
(188) Doses received from the presence of plutonium in the environment, largely from atmospheric nuclear weapons testing but also locally from discharges from nuclear fuel reprocessing plants, are small, and epidemiological studies of the effects of such low doses cannot plausibly produce meaningful results relating to the risk from exposure to plutonium. Studies have been carried out examining the possibility that the risk of certain cancers from plutonium exposure have been seriously underestimated, such as mortality in the closed city of Ozyorsk adjacent to Mayak (Deltour et al., 2015), or the incidence of childhood leukaemia following the peak of fallout from atmospheric nuclear weapons testing (Wakeford et al., 2010), without indications of an effect of plutonium exposure.
2.4. Calculation of lifetime risk of lung cancer
2.4.1. Method of calculation of lifetime risk
(189) Due to variations in the characteristics of the study populations (such as attained age, duration of follow-up, and baseline rates), a direct comparison of ERR estimates obtained from different cohorts may be misleading. The calculation of the individual cumulated risk up to a given age in a specific exposure scenario can take such variations into account (Thomas et al., 1992). The cumulated risk over a lifetime, often called the ‘lifetime excess risk’, is obtained using:
A risk model derived from a representative epidemiological study, with or without modifying factors (such as attained age, age at exposure, or time since exposure). Use of such a model enables estimation of risk for other populations, including extrapolations outside the range considered by the epidemiological study (exposure level, sex, duration of follow-up, attained age), once appropriate account is taken of the transfer of risk models between populations with different baseline rates. Baseline reference rates for all-cause and lung cancer mortality or incidence. This allows calculation of the baseline lifetime risk of lung cancer in the absence of exposure. Baseline rates are also part of the lifetime risk calculation when the risk model is expressed on a relative basis (i.e. ERR-based model). A scenario of exposure based on hypothetical intake conditions. (190) Lifetime excess risks can be estimated for either cancer incidence or mortality. It is considered that the evidence reviewed in this publication provides all elements needed to calculate lifetime risk of lung cancer mortality associated with plutonium exposure. (191) For the purposes of illustration, the lifetime risk of lung cancer mortality associated with a scenario of exposure to plutonium was calculated for a male worker. The lifetime duration is taken to be 90 years, as is generally considered for workers by the Commission. The method used is the calculation of the lifetime attributable risk as described in NRC (2005) and Thomas et al. (1992). Lifetime attributable risk is calculated using the survival function for a population unexposed to radiation, and is a close approximation to the more general risk of exposure-induced death, which is calculated using a survival function that accounts for deaths due to the same exposure to radiation for which risk is estimated. (192) Calculation of lifetime excess risk of lung cancer death was conducted by Sokolnikov et al. (2015b, 2017), using parameters presented by Gilbert et al. (2013), for a population of Russian males of working age (18–70 years) exposed to particularly high doses. A similar approach was used in the present publication, consistent with methods described by Thomas et al. (1992) and NRC (2005), using updated dosimetric models and risk coefficients, based on unitary scenarios of plutonium exposure and Euro-American baseline mortality data as a reference.
2.4.1.1. Risk models
(193) The most recent risk model derived from the MWC was selected, quantifying the relationship between the radiation dose delivered to the lung due to plutonium intake and ERR of lung cancer death. The model considers a linear relationship between dose and risk, with a strong decrease in this association (modifying effect) with increasing attained age. The model equation is:
(194) The model has been published by Gillies et al. (2017), and is based on plutonium lung dose estimated using MWDS-2013 (ss = 2.5 × 10−4 day−1). In this model, the estimated ERR for males at attained age of 60 years was 4.74 Gy−1 (90% CI 3.53–6.24), with modifying effect of attained age α = −2.74 (95% CI −4.51 to −1.04). A 10-year lag time was considered between lung dose and lung cancer death. (195) The variation of ERR Gy−1 with attained age for the Gillies model is illustrated in Fig. 2.2, and compared with ERR Gy−1 obtained using a previous model obtained from the MWC analyses published by Gilbert et al. (2013). The Gilbert model was based on plutonium lung dose (lagged by 5 years) estimated using the older dosimetry system (MWDS-2008). In that model, estimated ERR for males at attained age of 60 years was 7.4 Gy−1 (95% CI 5–11), with modifying effect of attained age α = −3.1 (95% CI −5.4 to −0.8). Variation of the excess relative risk (ERR) coefficient per Gy of plutonium lung dose with attained age for males, according to Gilbert et al. (2013) and Gillies et al. (2017).


2.4.1.2. Reference rates
(196) The reference baseline rates used are those provided in Publication 103 (ICRP, 2007) for both general mortality and lung cancer mortality for a composite Euro-American male population. Euro-American male reference mortality rates were used to be coherent with the risk models that were derived for Mayak workers. Fig. 2.3 shows the evolution of lung cancer baseline rates with age; rates increase sharply after 40–44 years of age (7.19 deaths per 100,000 per year) up to 80–84 years of age (464.57 per 100,000 per year) and then decrease. Based on these rates, the cumulated baseline risk from 20 to 89 years of age is 631 per 10,000 (Fig. 2.4). Age-specific lung cancer mortality baseline rates for adult Euro-American males, according to ICRP (2007). Age-specific cumulative lung cancer mortality baseline risk, weighted by the probability of survival, for adult Euro-American males.


2.4.2. Unitary plutonium intake scenarios
(197) To allow comparison of estimated lifetime risk values among different exposure situations, four exposure scenarios were considered, corresponding to a total intake of 1 Bq of 239Pu as nitrate (moderately soluble) or oxide (relatively insoluble) forms, assuming either an acute intake or a chronic intake over 10 years. Plutonium intake was considered to occur at the age of 20 years for the acute scenario and from 20 years to 29 years for the chronic scenario. Annual absorbed doses to the lung were calculated from the time of intake to 89 years of age. These were calculated using Publication 141 (ICRP, 2019) dosimetry. Characteristics of the scenarios are detailed in Table 2.7. (198) These scenarios for unit intake provide a basis for the estimation of lung doses for different levels of exposure. For example, to calculate the dose for an acute intake of 1000 Bq at 20 years of age, the cumulated dose given in Table 2.7 is multiplied by 1000. (199) Figs 2.5 and 2.6 present the distribution of annual lung dose by age for both acute and chronic plutonium intake, for plutonium nitrate or plutonium oxide, based on Publication 141 (ICRP, 2019) dosimetry. Characteristics of plutonium exposure scenarios for a total intake of 1 Bq of 239Pu assuming either an acute intake or a chronic intake over 10 years. The absorbed dose to the lung committed over 70 years (i.e. from 20 to 89 years of age) was calculated for plutonium nitrate or plutonium oxide based on Publication 141 (ICRP, 2019). Total dose cumulated from 20 to 89 years of age (i.e. >70 years). Annual lung dose as a function of attained age for acute intake of 1 Bq of 239Pu at 20 years of age, for plutonium nitrate or plutonium oxide, calculated based on Publication 141 (ICRP, 2019). Annual lung dose as a function of attained age for a total chronic intake of 1 Bq of 239Pu, for plutonium nitrate or plutonium oxide, calculated based on Publication 141 (ICRP, 2019). The exposure period is 10 years from 20 to 29 years of age.



2.4.3. Results of estimates of lifetime risk for unitary plutonium intake scenarios
(200) Lifetime risk of lung cancer mortality for each plutonium exposure scenario (acute vs chronic intakes and oxide vs nitrate; Table 2.8) has been estimated using the most recent risk model derived from the epidemiological studies of Mayak workers described above (Gillies et al., 2017), and based on lung doses derived using Publication 141 (ICRP, 2019) dosimetry. The risk in each year of life was obtained by multiplying the estimated ERR using Gillies et al.’s risk model (based on 10-year lagged cumulated dose) by the age-appropriate baseline rate of lung cancer mortality and survival function (ICRP, 2007). Lifetime risk has been integrated from the beginning of exposure at 20 years of age up to 89 years of age (i.e. 70 years). (201) For a fixed total intake of 1 Bq, the cumulated doses to lung tissue from low solubility compounds (e.g. plutonium oxide) are higher than doses from compounds with higher solubility (e.g. plutonium nitrate). In the scenarios described in this section (Table 2.7), doses vary by more than a factor of 2 between the lower and higher solubility compounds. (202) The lifetime risk estimates for plutonium oxide and nitrate (Table 2.8) differ by a factor of 2 or less. Gillies et al.’s (2017) risk model is linear with dose, but it also accounts for the dependency of risk on attained age. As lung doses vary with age (Figs 2.5 and 2.6), differences between risks for different compounds do not entirely reflect the differences between total cumulated doses. (203) It is concluded that it is now possible to estimate the lifetime risk of lung cancer attributable to plutonium exposure. Uncertainties associated with exposure reconstruction are very important, and different types of plutonium compounds can lead to very different cumulated doses (Section 2.2.6). Reliable lifetime risk estimates can be achieved by good characterisation of intake conditions (duration, timing, activity levels, and chemical form of compound). Lifetime risk of lung cancer mortality for scenarios with a total plutonium intake of 1 Bq, assuming either acute intake or chronic intake, of either plutonium nitrate or plutonium oxide, calculated for the ICRP Euro-American male population (ICRP, 2007). The risk model from Gillies et al. (2017) was applied, and Publication 141 (ICRP, 2019) dosimetry was used to calculate lung dose distribution (Fig. 2.5). Euro-American males (ICRP, 2007).

2.5. Discussion
2.5.1. Summary of risk estimation
(204) Strengths of the MWC include over 50 years of follow-up, reasonably complete mortality data, incidence data for workers resident in the adjacent closed city of Ozyorsk, estimates of annual plutonium and external doses for individual workers, and a wide range of doses. (205) An important limitation of the Mayak data is that despite extensive efforts by dosimetrists, plutonium dose estimates are subject to large uncertainties. As noted in Section 2.2.2, for approximately two-thirds of the workers who had plutonium monitoring data and were included in the most recent analyses, plutonium dose estimates were based on only one or two bioassay measurements. Thus, plutonium doses are subject to large measurement errors, which are known to bias estimated risk coefficients towards zero if no adjustment is made. Additional sources of uncertainty in plutonium doses are discussed in Section 2.2.6. It is hoped that in future, these uncertainties will be quantified in a way that allows them to be accounted for in dose–response analyses. Further, plutonium monitoring was only carried out for approximately 40% of workers who could have potentially been exposed to significant quantities of plutonium, so surrogate measures of plutonium exposure have had to be developed for these workers. (206) Most plutonium risk estimates were based on a mix of males and females and of smokers and non-smokers. As most Mayak worker lung cancers occurred in male smokers, risk estimates for females and non-smokers are very imprecise, limiting the usefulness of the Mayak data for estimating risks in other populations. Even for estimating risks in male smokers, estimates may not be fully appropriate as smoking data for the MWC do not include data on rate (cigarettes per day) or duration of smoking. (207) Despite these limitations, the MWC is unique in providing reasonably precise estimates of the plutonium dose–response relationship for lung cancer, and an opportunity to evaluate the dose–response relationship for other types of cancer, particularly liver and bone cancers as plutonium deposits in the liver and on bone surfaces. There are indications of excess risks of liver and bone cancers among Mayak workers in relation to organ/tissue doses from plutonium, which are stronger for liver cancer, but limited numbers of deaths and cases restrict firm inferences for estimating ERR Gy−1 for these cancers, including the shape of the dose–response curves and any risk-modifying factors. (208) To date, the results from studies of plutonium workers other than the MWC have not provided any consistent indication of an increased risk for the target organs/tissues of interest in respect of plutonium deposition, although the data are limited. (209) Analysis of the SWC by Gillies et al. (2017) demonstrated no consistent pattern of significantly increased risk of lung cancer by plutonium lung dose, although point estimates of lung cancer ERR were positive for all dose groups for both mortality and incidence for both lung solubility assumptions. Further, the study of plutonium workers from the EU by Grellier et al. (2017) found a significant positive association between lung dose from plutonium alpha particles and lung cancer mortality.
2.5.2. Comparison of studies
(210) Patterns of risk in the MWC can be compared with those identified in underground hard-rock miners exposed to radon progeny (Marsh et al., 2014). For lung cancer, the magnitude of the decline in ERR Gy−1 with attained age observed in Mayak workers was very similar to that based on 11 cohorts of underground miners analysed by the BEIR VI Committee (NRC, 1999). In contrast to data on the 11 cohorts evaluated in BEIR VI and to more recent data from the Czech, French, and German miner cohorts (Tomasek et al., 2008; ICRP, 2010; Kreuzer et al., 2018), there was no evidence of a decline in risk with time since exposure. (211) Parallel analyses of data for the MWC and the LSS cohort of Japanese atomic bomb survivors who were aged 15–60 years at exposure were conducted by Gilbert et al. (2013). The MWC ERR estimates for plutonium exposure for males at 60 years of age, expressed per Sv of equivalent dose to the lung (i.e. using wR for alpha particles of 20), was 0.35 (95% CI 0.24–0.50), nearly identical to an estimate of 0.36 (95% CI 0.04–0.78) based on LSS mortality data or an estimate of 0.34 (95% CI 0.05–0.72) based on LSS incidence data (Gilbert et al., 2013; Marsh et al., 2014). The ratios of female and male ERR estimates were also similar in the MWC and LSS cohort. However, CIs for LSS-based estimates were wide and compatible with much smaller or larger quality factors. ERR in the LSS cohort, unlike that in the MWC, did not show a decline with attained age. The above comparisons of the MWC and LSS ERRs were based on analyses that included an attained age parameter that was intermediate between estimates for the MWC and LSS cohort. (212) For lung cancer mortality at an attained age of 60 years in the male Mayak workforce, ERR Gy−1 of lung dose from plutonium using the ss = 2.5 × 10−4 day−1 solubility assumption was 4.74 (90% CI 3.53–6.24) (Gillies et al., 2017). This compares with the equivalent ERR Gy−1 estimate obtained by Gilbert et al. (2013) of 7.4 (90% CI 5.0–11), although it should be noted that Gilbert et al. (2013) lagged doses by 5 years whereas Gillies et al. (2017) lagged doses by 10 years, and that the lung dose estimates used by Gillies et al. (2017) were based on an updated dosimetry system. (213) For the incidence of lung cancer at an attained age of 60 years in the male MWC, ERR Gy−1 of lung dose from plutonium using the ss = 2.5 × 10−4 day−1 solubility assumption was 5.27 (90% CI 3.83–7.12) (Gillies et al., 2017). This compares with the equivalent ERR Gy−1 estimates obtained by Labutina et al. (2013) of 7.1 (95% CI 4.5–10.9), although the lung dose estimates used by Gillies et al. (2017) relative to those of Labutina et al. (2013) were based on an updated dosimetry system; both studies used a dose lag of 10 years. (214) The final estimates for the risk of lung cancer associated with plutonium lung dose derived from the pooled MWC and SWC analysis of Gillies et al. (2017) were within the range ERR = 5–8 Gy−1 for males at 60 years of age for both mortality and incidence, and using both lung solubility assumptions. These risk estimates are very similar in magnitude to those obtained in previous studies of the Mayak workers. (215) Further, the lung cancer ERR Gy−1 estimated from the pooled MWC and SWC in relation to external gamma was in the range of 0.2–0.4 Gy−1 gamma dose to the lung, which is similar to the results of past investigations of Mayak and Sellafield workers, and of other groups of persons exposed to low-LET radiation. (216) Most studies of lung cancer and plutonium exposure have used a dose lag of 5 or 10 years to address the latent period between exposure and effect. Gilbert et al. (2013) lagged doses by 5 years, whereas Gillies et al. (2017) lagged doses by 10 years; Gillies et al. (2017) stated that a dose lag of 5 years was considered in a supplementary analysis, but results were not presented. These dose lags are coherent with the literature: a 5-year lag is now generally considered appropriate for lung cancer and radon exposure in studies of miners (ICRP, 2010), while a 10-year lag was used in earlier studies of all solid cancers although a 5-year lag is now more commonly adopted (NRC, 2006; UNSCEAR, 2008).
2.5.3. Advantages and limitations
(217) The lack of consistency of results across the range of studies of workers exposed to plutonium is not surprising given the relatively small number of workers identified as plutonium workers in each study. With an average length of follow-up in excess of 20 years for the cohort studies, there is adequate latency to identify cancers related to occupational exposure, but the small number of workers identified as plutonium workers coupled with the relatively low percentage of deaths in the cohorts diminishes the power of the studies. (218) The different studies used standard methods for analysis. Several considered mortality data alone (Brown et al., 2004; Wing and Richardson, 2005; Grellier et al., 2017), but others also considered incidence (Omar et al., 1999; McGeoghegan et al., 2003). (219) Several studies did not provide estimates of a dose–risk relationship for plutonium organ/tissue doses (Omar et al., 1999; McGeoghegan et al., 2003; Wing et al., 2004). Omar et al. (1999) and McGeoghegan et al. (2003) calculated organ/tissue dose estimates based on monitoring for plutonium and from external radiation exposure, but did not present any risk estimates based on these plutonium dose estimates alone. Instead, results from the analysis of trends with plutonium dose combined with external dose were presented. The remaining studies by Wing et al. (2000, 2004) and Atkinson et al. (2004) stratified the worker cohort based on the presence or absence of monitoring for plutonium exposure. Most of these studies estimated risks for plutonium workers in terms of external radiation doses, although the relevance of these estimates with respect to plutonium exposures is questionable given the noteworthy differences in the data and methods used to determine external radiation exposure. (220) The estimates of ERR Gy−1 for lung cancer for both external exposure and internal plutonium exposure obtained by Gillies et al. (2017) in the pooled MWC and SWC show comparability of risks between those cohorts; this suggests that the pooling of cohorts is acceptable, which leads to increased statistical power and allows the study of a wider range of doses. (221) To date, the only firm evidence for the risk of cancer in relation to plutonium exposure has been based on findings from studies of the MWC. However, the scale of the exposures and the different dose assessment methodology used in the MWC mean that there is considerable uncertainty about whether the risks derived from this cohort could be extrapolated to low doses and are applicable to other cohorts. The SWC represents one of the few available companion cohorts with individual plutonium monitoring data available over a long period: approximately 500,000 urine sample results available for over 12,000 plutonium-monitored workers covering the low dose range. The MWC and SWC therefore represent complimentary resources for studying the health effects associated with plutonium exposure. The combination of these cohorts within a unified dosimetry methodology has enabled the study of plutonium risks over a wider dose range than could be managed using the MWC alone. (222) The results obtained in the pooled MWC and SWC suggest that the estimated risk of lung cancer is applicable to other cohorts, as comparable risks associated with plutonium exposure were found in the two contributing cohorts. However, at the present time, the power to detect risks in the SWC is relatively low and is hampered by the large uncertainty surrounding dose assessments based on early urine sample results. In the MWC, the power to detect effects is high across the mid to high dose range, but the power to detect effects at low doses is hampered by the relatively high limit of detection in place in the MWC for a large proportion of follow-up. For the MWC, the power to detect effects at low doses could potentially be improved by the addition of post-1982 workers into the cohort, or by the reconstruction of doses for those workers who were potentially exposed to substantial levels of plutonium but were not monitored. The power to detect effects in the SWC could be improved by extending follow-up, which would increase the data for the subcohort of Sellafield workers whose dose assessments are based on high-quality sample results, and by efforts to improve the dose assessments for early Sellafield workers, and through the creation of a plutonium job-exposure matrix (de Vocht et al., 2019; Riddell et al., 2019).
2.5.4. Relative biological effectiveness of plutonium for lung cancer
(223) RBE of different types of ionising radiation, the ratio of the absorbed doses of two types of radiation that produce the same level of a specified effect as estimated largely from experimental studies on cells or animals, are the basis for the wR values recommended by the Commission (ICRP, 2007) for the purposes of radiological protection. The recently published Mayak studies on risk from plutonium exposures, and the lifetime risk estimates presented in Section 2.4, can be used to gauge the RBE of alpha particles emitted by plutonium, in particular, and of alpha particles, in general. For alpha particles, Publication 103 (ICRP, 2007) recommends a wR of 20 for the calculation of equivalent and effective doses for radiological protection purposes. (224) ERR Gy−1 values obtained by Gillies et al. (2017) in the pooled MWC and SWC for both external exposure and internal plutonium exposure allow an estimation of RBE for alpha particles emitted from plutonium and the resulting risk of lung cancer: the point estimate obtained from this investigation is within the range of 10–30, which can be considered, in view of uncertainties in both the estimation of risk itself and of dose measurements and estimation, as a broad confirmation of the appropriateness of the value currently adopted in radiological protection as wR for alpha particles of 20. (225) This section investigates the biological effectiveness of plutonium alpha particles relative to high-energy photons by comparing the lifetime risk of lung cancer mortality for plutonium exposures estimated using the Gillies et al. (2017) risk models from the Mayak workers (Section 2.4.1) with lifetime risk of lung cancer mortality based on risk models derived from the LSS of the Japanese atomic bomb survivors. In this exercise, the reference radiation for comparing the health effects of plutonium is high-energy photons (i.e. alpha particles relative to gamma rays) and the health endpoint is lung cancer mortality. The biological effectiveness of alpha particles is estimated as the ratio of the lifetime risk from exposure to plutonium to the lifetime risk from exposure to high-energy photons described by annual absorbed doses to the lung (Gy), identical to those estimated for each of the plutonium intake scenarios described in Section 2.4.2. (226) The lifetime risk from exposure to high-energy photons has been estimated using the risk model for lung cancer mortality for the LSS cohort reported by Ozasa et al. (2012). The LSS included 86,611 subjects with a follow-up period from 1950 to 2003. Weighted doses to LSS cohort members were estimated using the DS02 dosimetric system, based on the gamma dose plus a small contribution from exposure to neutrons. The dose–response relationship for lung cancer mortality has been derived using estimates of lung absorbed dose (in Gy), based on a total of 1558 lung cancer deaths. (227) ERR and EAR models have been derived for lung cancer mortality in the LSS cohort. The models indicate a response linear in dose, adjusted by age and sex modifiers:
(228) For the ERR model, β represents the sex-averaged ERR per unit dose (Gy) at attained age of 70 years after exposure at 30 years of age. For the EAR model, β represents the sex-averaged EAR per unit dose (per 104 person-year Gy) at attained age of 70 years after exposure at 30 years of age. (229) Lifetime attributable risks (Thomas et al., 1992; NRC, 2005) from exposures to high-energy photons have been estimated based on the ERR and EAR models from Ozasa et al. (2012) separately by using: (i) lung doses corresponding to exposure scenarios described in Section 2.4.2; (ii) baseline rates of lung cancer mortality and survival functions for a Publication 103 composite Euro-American male population (ICRP, 2007); and (iii) a 10-year lag representing the minimum latency period [as in the main analyses in Gillies et al. (2017)]. Risks in each year of life were derived by summing the risks from annual doses in all previous years of exposure, except those during the last 10 years (i.e. 10-year lag), calculated either from the EAR model (EAR risk projection) or by multiplying ERR by the baseline rate of lung cancer mortality at that age (ERR risk projection). Both risk projections were weighted by the survival function (ICRP, 2007). Lifetime risk was integrated from the beginning of exposure at 20 years of age up to 89 years of age. (230) Lifetime risk obtained from the Japanese LSS was divided by a DDREF of 2, as recommended in Publication 103 (ICRP, 2007), for the application of risk models derived from a cohort acutely exposed to gamma rays to a chronic exposure situation relevant for comparison with the plutonium intake scenarios described in Section 2.4.2. (231) Results of the lifetime risk calculation are presented in Table 2.10. The lung cancer mortality risks from exposures to alpha particles are larger than the risks from low-level exposure to high-energy photons by a factor of approximately 15–22, depending on the exposure scenario and choice of model (ERR vs EAR). (232) The above results suggest RBE of plutonium alpha particles relative to high-energy photons of approximately 15–16 when based on the ERR model, and 19–22 when based on the EAR model. Note that without the application of a DDREF of 2 to the lifetime risk estimate derived from the LSS models, the estimated RBE would be a factor of 2 lower (indicating values of 7–11). Parameter values and effect modifiers of the excess relative risk (ERR) and excess absolute risk (EAR) models for lung cancer mortality from the Life Span Study (Ozasa et al., 2012). Best estimate and 95% confidence interval. Comparison of lifetime risk of lung cancer estimated for exposures to plutonium alpha particles and high-energy photons assuming the same lung dose distribution. Lung dose distribution obtained for a total intake of 1 Bq of 239Pu. LSS, Life Span Study; ERR, excess relative risk; EAR, excess absolute risk. Reduced by a dose and dose-rate effectiveness factor of 2. Composite Euro-American male population. Reported values represent ratios of lifetime risk before rounding to two digits (ratio of unrounded lifetime attributable risk estimates).



2.5.5. Comparison with the relative biological effectiveness of radon for lung cancer
(233) In Publication 115 (ICRP, 2010), a nominal risk coefficient of 5 × 10−4 per working-level month (WLM) (1.4 × 10−4 per mJh m−3) was adopted for the lung detriment per unit exposure to radon and its progeny, on the basis of a review of epidemiological studies of underground miners, including studies with relatively low levels of exposure. Risk models used for the calculation of lifetime risk were ERR models derived from miner studies, considering a modifying effect of exposure rate and time since exposure, and with a minimal lag time of 5 years between exposure and lung cancer death (ICRP, 2010). Lung cancer baseline rates were reference rates averaged over males and females, and over composite Euro-American and Asian populations of Publication 103 (ICRP, 2007). The exposure scenario considered was a constant low-level exposure to 2 WLM per year during adulthood from 18 to 64 years of age, and the risk was estimated up to 90 years of age. Repeating the calculation using only the baseline rates for Euro-American males instead of the reference rates averaged over males and females and over Euro-American and Asian populations gives a lifetime risk estimate of approximately 7 × 10−4 per WLM (ICRP, 2010). (234) A lung equivalent dose of 24.3 mSv per mJh m−3 (86 mSv per WLM) of exposure to radon progeny for male miners was calculated in Publication 137 (ICRP, 2017), with a wR of 20 for alpha particles (ICRP, 2007). This corresponds to a weighted absorbed dose to the lung, as defined in Section 2.2.3, of 4.3 mGy per WLM. (235) The scenario of radon exposure considered in Publication 115 (ICRP, 2010) therefore corresponds to an absorbed dose rate to the lung of 8.6 mGy year−1 from 18 to 64 years of age, with a total exposure of 94 WLM corresponding to a total lung absorbed dose of 0.40 Gy. The lifetime EAR value of 7 × 10−4 per WLM for Euro-American males (ICRP, 2010) and a weighted absorbed dose to the lung of 4.3 mGy per WLM (ICRP, 2017) gives a corresponding lifetime risk of lung cancer per lung dose of 1628 deaths per 104 per Gy (i.e. 0.16 Gy−1). (236) For comparison, under the same scenario of exposure, a lifetime attributable risk, integrated up to 90 years of age, was estimated from exposure to high-energy photons, using the ERR model from Ozasa et al. (2012) presented in Table 2.9. The same estimate of annual absorbed doses to the lung of 8.6 mGy year−1 from 18 to 64 years of age was used. Also, the baseline rates of lung cancer mortality and survival functions of Publication 103 (ICRP, 2007) for Euro-American males were used, with a 5-year lag representing the minimum latency period, as in Publication 115 (ICRP, 2010). A DDREF of 2 was applied to derive the excess risk from the LSS ERR model, and an excess of 113 deaths per 104 per Gy (1.13 × 10−2 Gy−1) was obtained. (237) Table 2.11 compares the lifetime excess risk of lung cancer death per unit lung dose for exposure to plutonium, radon progeny, and high-energy photons. The risk from exposure to alpha particles emitted by radon progeny is greater than the risk from exposure to high-energy photons by a factor of approximately 14, which is consistent with the factor of approximately 15–16 between risks from exposure to plutonium and photons. These figures would suggest biological effectiveness for lung cancer mortality of alpha particles relative to photons of approximately 14–16. Comparison of lifetime excess risk per lung dose of 1 Gy from exposure to plutonium (four exposure scenarios), radon, and high-energy photons for Euro-American males. ERR, excess relative risk; LSS, Life Span Study; DDREF, dose and dose-rate effectiveness factor.
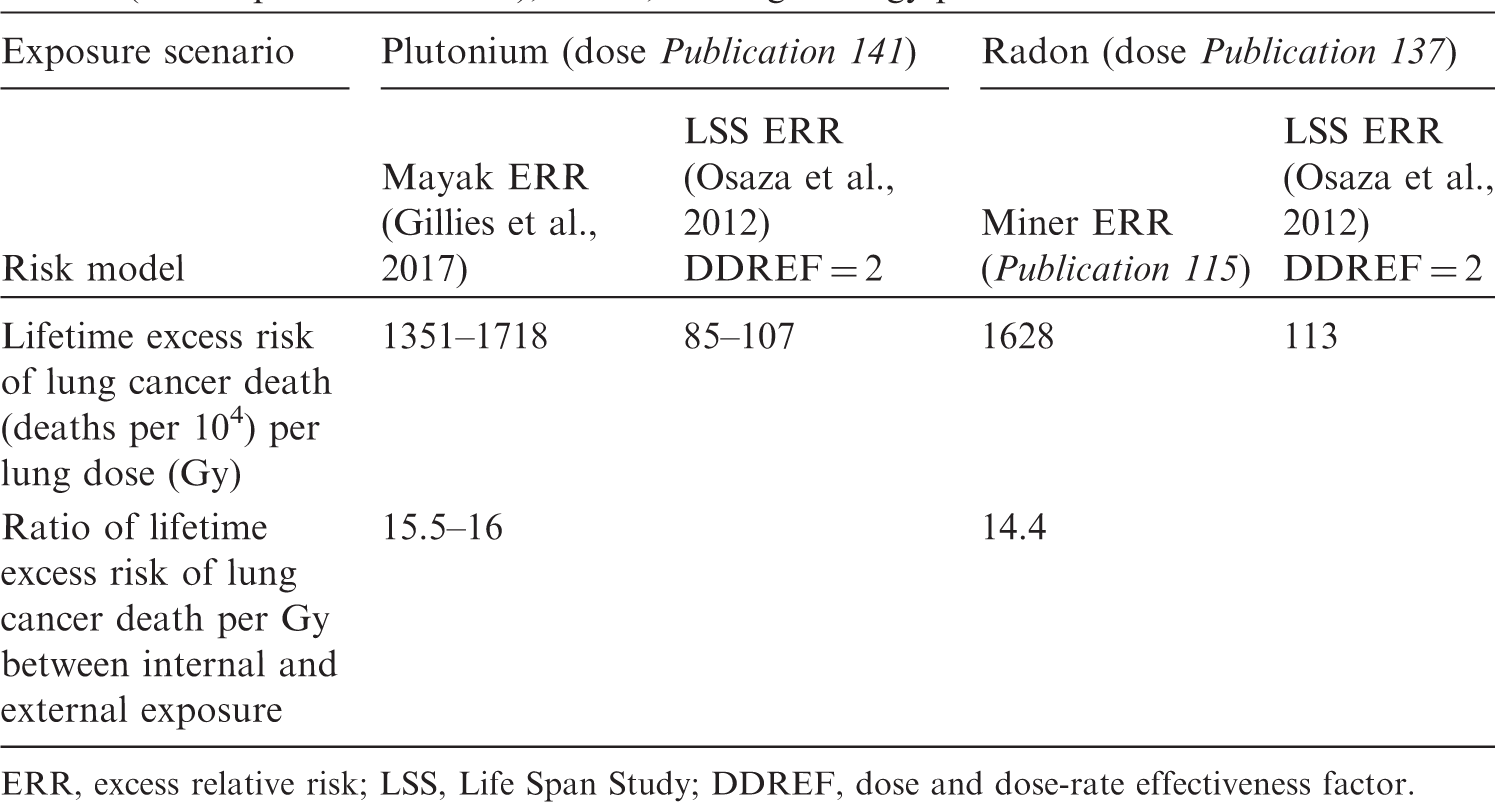
2.5.6. Interpretation of the estimated relative biological effectiveness values
(238) RBE values estimated for plutonium and radon progeny are comparable with the wR value recommended by ICRP for alpha particles. However, while most inferences about the biological effectiveness of alpha particles have been based on studies of cancers in animals or studies of transformation in cells (NCRP, 1990; Muirhead et al., 1993), the results presented here are based on human epidemiological data. Such an approach of ‘equivalence in risk’ has already been used by ICRP for radon (ICRP, 1993), but equivalence was in terms of detriment and not for a single organ as is the case here. (239) Therefore, caution is needed when interpreting the values of RBE derived in this publication, especially when comparing with other radionuclides or when discussing wR, as the wR value is intended to embrace all effects from all sources of alpha emission, whereas only lung cancer mortality for specific alpha-particle emitters is considered in the present calculations. For example, plutonium-related risk of cancer has been observed for liver and bone (Section 2.3.1), for which different RBEs for alpha radiation may apply. (240) Also, important uncertainties are associated with the derived biological effectiveness, including statistical uncertainties in the parameter values of the risk models, uncertainties related to dosimetry, uncertainties related to the transfer of risk (ERR vs EAR risk models) and DDREF, and uncertainties related to the effects of smoking (Section 2.5.1). For example, applying the LSS EAR model to the miner scenario of exposure would yield a lower estimate of 80 deaths per 104 Gy−1 (instead of 85–107 deaths, Table 2.11). In the same way, considering a lag time of 10 years (instead of 5 years) would have led to slightly lower values. The choice of energy for the reference photon radiation, either x rays or high-energy gamma rays, is another factor possibly influencing any estimation of RBE. (241) Therefore, it should be kept in mind that the value of RBE estimated here for alpha particles emitted by plutonium and radon progeny concerns the risk of fatal lung cancer alone, and corresponds to specific scenarios of exposure, while wR is a judgement value for radiological protection purposes and applies to all effects of alpha radiation, including other types of cancer. Finally, the contribution of lung dose from internal emitters of alpha particles to effective dose is directly proportional to the value assigned to the tissue weighting factor wT for lung.
2.5.7. Potential impact of uncertainties
(242) As discussed in Section 2.2.6, uncertainties associated with internal dose assessments based on bioassay data can be quite large. Even so, epidemiological studies that evaluate site-specific cancers from occupational exposure to plutonium have generally not considered the uncertainties in the dose assessment. At best, the impact of these uncertainties has only been discussed qualitatively. Generally, only point estimates of doses are available, without any estimate of uncertainty. (243) In addition to dose uncertainties, other limitations can exist that are related to the epidemiological design (e.g. selection and ascertainment bias, loss to follow-up, statistical power, confounding) and the modelling of the relationship between radiation exposure and risk (e.g. the shape of the dose–risk relationship, modifiers of the dose–risk relationship) (UNSCEAR, 2018). (244) MDWS-2013 and the Gillies et al. (2017) risk model apply for a mixed population of both smokers and never smokers. The risks of lung cancer death have been estimated for the composite Euro-American male population, which also represents a population that includes both smokers and never smokers. However, the prevalence and level of smoking could be different in the MWC and in the Euro-American male population for which the risks were estimated. (245) Calculations of the distribution of annual lung doses over age for the given exposure scenarios presented in Section 2.4.2 have also been performed using MWDS-2013 instead of Publication 141 (ICRP, 2019) for the lifetime lung cancer mortality risk calculations. Using MWDS-2013, lung doses would have been approximately 25% lower for oxide and approximately a factor of 2 higher for nitrate than the doses presented in Table 2.7. The impact of the dosimetry system on lifetime risk per unit intake would have been similar to the impact on the magnitude of doses, with lifetime risk being 20% lower for oxide and approximately twice as high for nitrate if using MWDS-2013 (compared with results presented in Table 2.7). However, the lifetime risk per Gy for both dosimetry systems is similar with values of 0.15–0.19 Gy−1 for MWDS-2013 and 0.14–0.17 Gy−1 for Publication 141 (ICRP, 2019) dosimetry. Likewise, the ratio of risk of lung cancer mortality of exposures to plutonium alpha particles and exposure to high-energy photons using ERR models would have been approximately 16 using MWDS-2013 [similar to the range of 15–16 using Publication 141 (ICRP, 2019), as presented in Table 2.8]. These results indicate that the choice of dosimetry system used to calculate the distribution of annual lung doses over age for the given exposure scenarios is not a very sensitive factor in calculation of the lifetime lung cancer mortality risk per Gy. However, the dosimetry system used to calculate the Mayak worker doses for the epidemiological analysis is an important factor. (246) The absorbed dose to each target region of the lung is calculated separately. The lung dose (or the weighted absorbed dose to the lung) considered in Table 2.7 is the arithmetic mean of the absorbed doses to the BB, bb, and AI regions of the lung, consistent with the equal apportionment of the detriment applied in Publication 130 (ICRP, 2015a) for calculation of the equivalent dose to the lung. However, apportionment factor (ABB:Abb:AAI) values of approximately 0.6:0.3:0.1 are consistent with regional distribution of lung cancer types in the general population of smokers and non-smokers (Para. 98). Assuming these values instead of the Commission’s default values (⅓:⅓:⅓) decreases the weighted absorbed dose to the lung per unit intake by approximately 1.5 and 2.2 for plutonium nitrates and oxides, respectively (Para. 100). It is difficult to infer the effect of different apportionment factors on estimated lifetime risk per Gy without repeating the dosimetric calculations and the epidemiological analysis itself. However, it is likely that estimated lifetime risk per Gy would be approximately a factor of 1.5–2 greater with apportionment factors of approximately 0.6:0.3:0.1. Correspondingly, the estimated RBE would be approximately a factor of 1.5–2 higher. (247) The lifetime risk of death due to lung cancer was also calculated for the composite Euro-American male population based on exposure to radon progeny (Section 2.5.5). Assuming apportionment factor (ABB:Abb:AAI) values of approximately 0.6:0.3:0.1 instead of the Commission’s default values (⅓:⅓:⅓) increases the weighted absorbed dose to the lung per unit exposure by approximately a factor of 1.2 (ICRP, 2017). Consequently, estimated lifetime risk of death due to lung cancer per Gy and estimated RBE based on radon progeny exposure would be approximately 1.2 times lower with apportionment factors of approximately 0.6:0.3:0.1. (248) The comparison of risk per lung dose between protracted irradiation by alpha particles from plutonium or radon progeny and acute exposure at moderate-to-high gamma-ray doses in the LSS cohort is performed with the application of a DDREF to the LSS risk estimates. As a ratio of these risks, the value of RBE estimated here for alpha irradiation of the lung is proportional to the assumed value of DDREF because wR is based on RBE values with respect to low-level gamma-ray exposures. A value of 2 is used by the Commission to derive risk coefficients for all types of solid cancer. The choice of a DDREF of 2 by the Commission is based upon dose–response features of experimental data and upon the epidemiological data of the LSS available in the 1990s ICRP, 1991. Recommendations of the International Commission on Radiological Protection. ICRP Publication 60. Ann. ICRP 21(1-3). Its magnitude is uncertain as highlighted by different analyses (Kocher et al., 2005, 2018, 2019; NAS/NRC, 2006; Wakeford et al., 2019), and this uncertainty propagates to that of the present RBE estimation for plutonium alpha particles and lung cancer mortality. A reappraisal of the validity of the DDREF regarding current scientific knowledge is ongoing in the framework of an ICRP task group (Rühm et al., 2015, 2016, 2018; Shore et al., 2017; Tran and Little, 2017). Applying no DDREF to the lifetime risk derived from the LSS ERR model would suggest an RBE value of approximately 7–8 instead of 14–16.
3. RISK OF Cancer from exposure to uranium
3.1. Introduction
(249) Given the weak evidence for the risk of cancer consequent to ingestion of uranium and to inhalation of uranium in the environment (see Section 3.4.4.2), the quantitative evaluation of uranium carcinogenicity undertaken in this section is limited to occupational exposure to uranium through inhalation resulting from the processing of uranium ore through milling and refining, chemical conversion, enrichment, fuel fabrication, and spent fuel reprocessing. Although increased risk of lung cancer has been found among underground uranium miners, this excess has been attributed to inhalation of radon and its decay products released from the ore, and exposure of the lung to radon progeny. The relationship between radon and its progeny and lung cancer is discussed in Publication 115 (ICRP, 2010), and is not considered in detail in this publication. (250) The likelihood of internal radiation exposure from occupational intakes of uranium varies throughout the nuclear fuel cycle and is dependent upon the processes, the techniques used, and the chemical characteristics of uranium exposure. Subsequent to the mining of raw uranium ore, milling consists of crushing and grinding ore followed by chemical leaching, separation of uranium from the leachate, and precipitation as ‘yellowcake’ – a chemically complex mixture of diuranates, basic uranyl sulphate, and hydrated uranium oxides – which contains 70–90% uranium. During uranium conversion, U3O8, the main component of yellowcake, is reduced to UO2 using hydrogen, then to UF4 by addition of hydrofluoric acid, and finally to UF6 by exposure to fluorine. Gaseous diffusion or gas centrifuge plants may be used to enrich the 235U in the uranium in UF6 for commercial purposes from 0.72% 235U to approximately 3–5% 235U, and to higher enrichments for research and military purposes. After enrichment, UF6 is reconverted into metallic uranium or UO2 for fuel fabrication. Spent fuel reprocessing involves dissolution of the irradiated fuel elements in acid, followed by chemical separation of plutonium and uranium from the solution. (251) In 2012, IARC concluded that there was sufficient evidence of the carcinogenicity of uranium from studies using experimental animals, but that evidence was limited in humans exposed to mixtures of natural, enriched, and depleted uranium (IARC, 2012). Recently, in its 2016 Report, UNSCEAR (2017) published an extensive review focusing on biological effects of uranium in experimental studies of laboratory animals, and in epidemiological studies of workers and the general population. (252) The present publication provides a critical summary of the UNSCEAR 2016 Report (UNSCEAR, 2017) and discusses the impact of recent epidemiological studies. The focus here is on studies of workers that provide information on the specific effect of exposure to uranium; studies of uranium miners are excluded because their primary exposure is to radon and its progeny.
3.2. Dosimetric and toxicological aspects
(253) Due to variations in the type and size of airborne uranium particles and the chemical form of uranium contained in particles, the solubility and resulting biokinetic distribution of uranium in the human body differ significantly (ICRP, 2017). Inhalation of soluble uranium compounds leads to ready absorption from the lungs to blood, leading to organ retention and principally urinary excretion. Insoluble uranium, however, is retained in the lungs to a larger extent, with a greater proportion being transported to tracheobronchial or other thoracic lymph nodes, or escalated from the lungs and swallowed. Consequently, health hazards are likely to vary across the nuclear fuel cycle because of the different forms of uranium present at each stage (Ansoborlo et al., 2002). (254) Depending on the chemical compound, uranium may display any reference absorption type from the respiratory tract [fast (F), moderate (M), slow (S), intermediate, F/M or M/S] and approximately 0.2–2% is absorbed from the small intestine (ICRP, 2017). For example, the relatively insoluble materials uranium octoxide and dioxide used to be assigned to Type S (ICRP, 1994b) until their absorption kinetics were more precisely characterised as intermediate between those of Types M and S (M/S). (255) The ICRP biokinetic and dosimetric models applicable to uranium, and material-specific absorption parameter values, are presented in Publication 137 (ICRP, 2017). To estimate internal uranium exposure in a cohort of US enrichment workers, Anderson et al. (2013) implemented the former models of Publications 66 (ICRP, 1994a) and 69 (ICRP, 1995) in the InDEP computer code. Intakes were evaluated from bioassay data using either a least-square method or a Bayesian method. Uncertainties on biokinetic models, dose coefficients, and bioassay data were quantified by lognormal probability distributions based on literature and expert judgement, and propagated by Monte Carlo calculation. (256) As a heavy metal, uranium displays chemical toxicity in addition to delivery of radiation dose. Inhalation of uranium hexafluoride induces irritation at high doses; some uranium compounds may cause pulmonary effects at relatively high inhalation exposures. However, long-term exposure to lower concentrations (generally <10 mg m−3) has not usually resulted in pulmonary toxicity (WHO, 2001). Biological effects of uranium in the skeleton, liver, gonads, central nervous system, and immune system have been observed in rodents at concentrations substantially above those to which humans are exposed, but did not lead to pathologies except for an indication of impaired bone metabolism and suggestions of some negative effects on the behaviour of animals (UNSCEAR, 2016). Report to the General Assembly, Annexe B. United Nations Scientific Committee on the Effects of Atomic Radiation, New York). In a human study of environmental exposure, effects of chronic ingestion of uranium in drinking water on bone metabolism were studied among 146 males and 142 females aged 26–83 years who, for an average of 13 years, had used drinking water originating from wells drilled in bedrock in areas with naturally high uranium content (Kurttio et al., 2005). There was some suggestion that elevation of CTx, a marker for bone resorption (P = 0.05), as well as osteocalcin, an indicator of bone formation (P = 0.19), could be associated with increased uranium exposure (uranium in water and intakes) in males, but no similar relationship was found in females. No clinically significant pathologies have been found in veterans exposed to depleted uranium (Hines et al., 2013; McDiarmid et al., 2013). (257) The main target organ to be considered for uranium toxicity is the kidney (WHO, 2001; ATSDR, 2013; UNSCEAR, 2016). In the kidney, proximal tubules are considered to be the main target. There is limited information from human studies indicating that the severity of effects on kidney function and the time taken for renal function to return to normal both increase with the level of uranium exposure. Currently, uranium is regarded as a less potent nephrotoxin than the classical nephrotoxic metals (cadmium, lead, mercury). A cohort of veterans exposed to depleted uranium has been followed since 1994. They were divided into two groups: low exposure (urine uranium levels <0.1 µg g−1 creatinine) and high exposure (urine uranium levels ≥0.1 µg g−1 creatinine and usually bearing embedded fragments of depleted uranium). No significant differences in the parameters of kidney function were observed between the two groups, and the values were in normal ranges. However, some parameter changes were close to significance (McDiarmid et al., 2009, 2011). Effects of chronic ingestion of uranium in drinking water on kidney function were studied in Canada (Limson Zamora et al., 1998) and in Finland (Kurttio et al., 2006a). In both studies, uranium intake was associated with increased glucose excretion in urine, and the study in Finland also showed a small effect on blood pressure; however, no damage to glomerular function was observed. Renal effects have been observed in animals exposed to aerosols of soluble uranium compounds at concentrations of at least 0.13 mg U m−3 for intermediate durations. However, no renal effects were observed in animals exposed to 1.1 mg U m−3 as insoluble compounds; the lowest level that has been observed to cause adverse effects was 8.2 mg U m−3 (ATSDR, 2013). (258) On the basis of animal experiments and human data, ATSDR calculated minimum risk levels (MRLs) for chemical toxicity of uranium under some situations of exposure. An MRL is defined as an estimate of daily human exposure to a substance that is likely to be without an appreciable risk of adverse effects (acute kidney damage) over a specified duration of exposure. MRLs of 0.002 mg U m−3 and 0.0008 mg U m−3 have been derived for intermediate-duration inhalation exposure (15– 364 days) to insoluble and soluble compounds of uranium, respectively. MRLs of 0.0008 mg U m−3 and 0.00004 mg U m−3 have been derived for chronic inhalation exposure (≥365 days) to insoluble and soluble compounds of uranium, MRLs of 0.002 mg U kg−1 day−1 and 0.0002 mg U kg−1 day−1 have been derived for acute-duration (≤15 days) and intermediate-duration (15–364 days), oral exposure to soluble compounds of uranium, respectively. The database was considered inadequate for derivation of a chronic oral MRL (ATSDR, 2013). (259) From available biological and health effects data, the World Health Organization (WHO) has adopted a tolerable intake (TI) approach to derive a guideline value for the chemical toxicity of depleted uranium. WHO (2001) concluded that limitations on public intake of soluble depleted uranium compounds (Types F and M) should be based on a TI value of 0.5 µg per kg of body weight per day, and limitations on public intake of insoluble (Type S) depleted uranium compounds should be based on a TI value of 5 µg per kg of body weight per day. The TI value of 0.5 µg per kg of body weight per day leads to a limitation on public inhalation of soluble depleted uranium compounds to 1 µg m−3 depleted uranium in air; the same guideline air concentration of 1 µg m−3 depleted uranium in air for insoluble depleted uranium compounds comes from the dose limit of 1 mSv year−1 for the public. The 8-h time-weighted average limitation on worker inhalation of soluble and insoluble depleted uranium compounds is 50 µg m−3 depleted uranium in air. For assessment of drinking-water quality, WHO (2017) adopted a provisional guideline value of 30 µg L−1 below which there is no clear evidence of effects in human populations. A report of the UK Royal Society assessed the health hazards associated with the use of depleted uranium munitions following the military conflicts in the Persian Gulf and the Balkans (Royal Society, 2001, 2002). Part II of the report considered the chemical toxicity effects of uranium on the kidney (Royal Society, 2002). Based on the limited human exposure data, it was reported that adverse effects can be detected at chronic intakes that result in kidney levels of 0.1–0.5 µg U g−1 kidney, or acute intakes resulting in approximately 1 µg U g−1 kidney. However, the long-term effects (if any) of these elevated uranium levels are not clear. These toxicity reference values were supported by a further review of the scientific literature including several human studies that were not considered by the Royal Society Working Group (Hodgson et al., 2007). It was also noted that, for humans, the ratio of uranium urinary excretion to kidney concentration shows no obvious change up to kidney concentrations of at least 3 µg U g−1 kidney (Hodgson et al., 2007). (260) The Royal Society Working Group noted that the kidney is a resilient organ, and that approximately two-thirds of kidney function can be impaired without obvious clinical signs of disease. It was also noted that normal kidney function can be restored even after a large acute intake of uranium, although some abnormalities may remain detectable for several years. The long-term effects of acute uranium poisoning in humans are not well known, but there could be kidney failure in later life (Royal Society, 2002). (261) A US National Research Council committee concluded that transient adverse renal effects of uranium including proteinuria and glucosuria may occur at peak kidney concentrations as low as 1.0 µg U g−1 kidney (NRC, 2008). Following this conclusion, Leggett et al. (2012) reviewed the literature on the chemical toxicity of uranium, and applied ICRP biokinetic models (ICRP, 1994a, 1995, 2006) to adopt a reference primary guidance for prevention of chemical toxicity from intake of uranium; they concluded that the concentration of uranium in the kidneys should not exceed 1.0 µg U g−1 kidney at any time. (262) The UNSCEAR 2016 Report (UNSCEAR, 2017) concluded that, in rodent studies, injury to the kidney occurred from 0.1 mg kg−1 whole body and renal concentrations >3 µg U g−1 kidney, which have been used as the basis for occupational exposure limits. However, the limited human studies suggest that damage to the kidneys can be detected following chronic exposure that results in uranium concentrations as low as 0.1 µg U g−1 kidney, and that acute intake which leads to a peak uranium level of approximately 1 µg U g−1 kidney can lead to detectable kidney dysfunction. As noted by Leggett (1989), the apparent discrepancies between studies addressing the chemical toxicity threshold of renal uranium may be due largely to differences in perceptions or definitions of toxicity, sensitivity of the measurements of kidney damage or dysfunction, patterns of exposure (e.g. acute vs chronic), and sensitivity to renal uranium in different species.
3.3. Epidemiological studies
3.3.1. Description of studies
(263) The relationship between exposure to internally deposited uranium and cancer in nuclear fuel cycle workers has been the subject of several extensive literature reviews and meta-analyses (Guseva Canu et al., 2008; Zhivin et al., 2014; Stammler et al., 2016), and was also addressed in the UNSCEAR 2016 Report (UNSCEAR, 2017). Table 3.1 summarises these data and includes the seven most recent studies (Grellier et al., 2017; Yiin et al., 2017, 2018; Bouet et al., 2018, 2019; Zablotska et al., 2018; Golden et al., 2019) published after the completion of the UNSCEAR 2016 Report (UNSCEAR, 2017). Studies are grouped by type of uranium work (e.g. uranium milling, uranium conversion) and then ordered alphabetically by author within each work category. (264) From the 21 cohort studies and six case–control studies of uranium workers summarised in Table 3.1, several specific steps in the uranium nuclear cycle are covered: uranium milling and refining (Pinkerton et al., 2004; Boice et al., 2007, 2008; Zablotska et al., 2013, 2018; Kreuzer et al., 2015; Bouet et al., 2018); uranium enrichment via gaseous diffusion (McGeoghegan and Binks, 2000a; Yiin et al., 2009, 2017, 2018; Chan et al., 2010; Figgs, 2013; Zhivin et al., 2016); chemical conversion and fuel fabrication (Dupree-Ellis et al., 2000; McGeoghegan and Binks, 2000b; Richardson and Wing, 2006; Guseva Canu et al., 2011a; Silver et al., 2013; Bouet et al., 2019; Golden et al., 2019); and research and development of nuclear reactors and fuel fabrication (Ritz et al., 2000; Boice et al., 2011). Three studies covered all steps of the nuclear fuel cycle (Fournier et al., 2016; Samson et al., 2016; Grellier et al., 2017). The solubility of the uranium used in these different activities varied from predominantly soluble uranium in uranium enrichment to insoluble uranium in uranium processing. (265) Very few studies provided information on uranium-specific health risks due to missing (or sparse) uranium-specific exposure estimates because of absent or incomplete historical recording of individual information (Table 3.1). The present publication focuses on studies that reported uranium-specific risks for the three most plausible cancer outcomes following uranium exposure: lung cancer (organ of entry following inhalation); kidney cancer (organ of accumulation and elimination); and leukaemia and other lympho-haematopoietic malignancies (outcome of interest after general radiation exposure). The more recent studies add little to the evidence on other cancers reviewed in the UNSCEAR 2016 Report (UNSCEAR, 2017), and so are not considered further in this publication. With the potential exception of lung doses following inhalation of insoluble forms of uranium, in the studies considered in this publication, organ/tissue doses from uranium tend to be very low, and this should be borne in mind when interpreting the resulting risks per unit uranium-specific dose. (266) Studies of uranium millers are not informative with respect to the risk of cancer linked specifically to uranium-bearing dust (see Table 3.1), and so do not contribute to the evidence on uranium-specific health effects reviewed in this publication. Description of studies of workers where uranium was a major source of exposure. SMR, standardised mortality ratio; R&D, research and development; BNFL, British Nuclear Fuels Ltd; CEA, Commissariat à l’Energie Atomique; AWE, Atomic Weapons Establishment; UKAEA, UK Atomic Energy Authority; FBFC, Franco-Belge de Fabrication du Combustible.
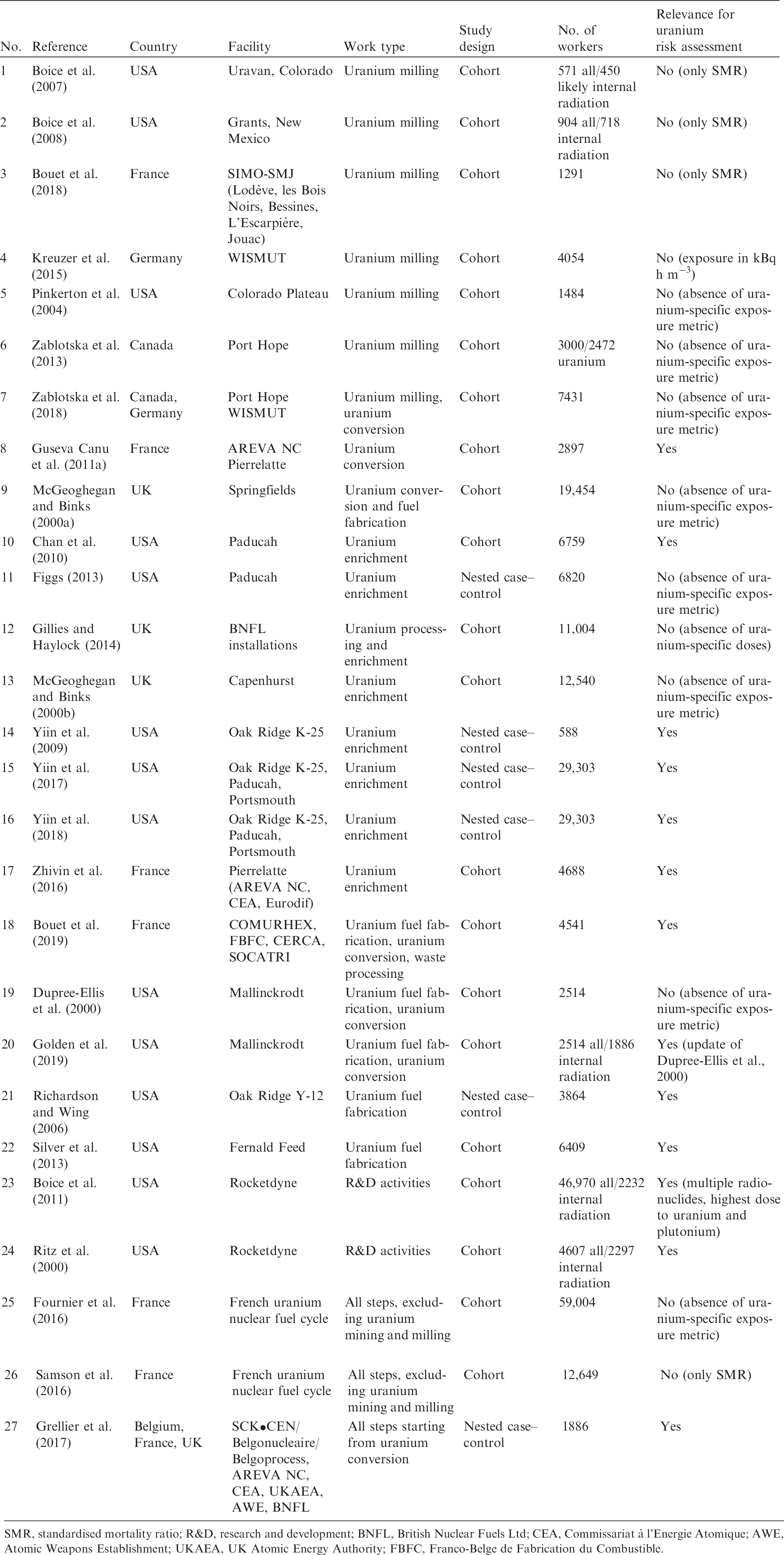
The Alpha-Risk study
(267) In the EU-funded Alpha-Risk project (Grellier et al., 2017), internal exposure to plutonium and uranium for workers in the British (AWE, UKAEA, and BNFL cohorts), Belgian (SCK•CEN/BN cohort), and French (CEA-COGEMA cohort) nuclear industries was investigated through a case–control study of lung cancer and leukaemia mortality, nested within appropriate cohorts from the International Collaborative Study of Cancer Risk Among Radiation Workers in the Nuclear Industry. The nested case–control design allowed detailed dose reconstruction as well as the collection of individual data on potential confounders. (268) Grellier et al. (2017) found a lung cancer mortality EOR Gy−1 of lung dose from uranium alpha particles for all workers included in the Alpha-Risk study (median lung dose in 1011 controls of 2.22 mGy) of 4.2 (90% CI −2.5 to 17). There is notable variation in estimated EOR Gy−1 when each contributing cohort is removed from the analysis: the highest EOR Gy−1 was obtained when the BNFL workforce (median lung dose in 781 controls of 2.38 mGy) was excluded [26 (90% CI 2.5–80)], while the lowest EOR Gy−1 was obtained when the AWE cohort (median lung dose in 125 controls of 3.25 mGy) was removed [−0.1 (90% CI −3.3 to 9.3)]. (269) As indicated in Section 2.3.2, EOR Gy−1 of lung dose from plutonium for all workers included in the Alpha-Risk study (median lung dose in 463 controls of 1.25 mGy) was 49 (90% CI 16–106), which is approximately 10 times higher than that for the dose to the lung from uranium, while the estimated risk of lung cancer associated with gamma radiation (median dose in 1264 controls of 33.86 mGy) was in the opposite direction [EOR Gy−1 = −0.44 (90% CI −0.6 to 0.04)] (Grellier et al., 2017). (270) The results from the Alpha-Risk study for leukaemia mortality have yet to be published.
3.3.2. Statistical methods
(271) The cohort and case–control studies summarised in Table 3.1 were mainly based on causes of death information obtained from death records, although a few also used cancer incidence registration data. All the cohort studies reported SMRs and some also reported SRRs. (272) In the majority of studies, the referent was the national population, although in some studies, both national and regional referent rates were used. The expected numbers of deaths (or cancer registrations) were generally calculated adjusting for age, sex, race, and calendar period. (273) For intracohort analyses, three analytic approaches were used: conditional logistic regression; Poisson modelling; and Cox proportional hazards modelling. As examples, Ritz et al. (2000) used conditional logistic regression to estimate RRs adjusting for age at risk, pay status (as an indicator of socio-economic status), time since first exposure, and external radiation dose; Poisson modelling was used to estimate ERR or RR. In their studies, Boice et al. (2011), Guseva Canu et al. (2011), and Golden et al. (2019) calculated risk estimates based on Cox proportional hazards modelling including age, sex, calendar time, and socio-economic status in the model; the referent group was unexposed workers. Chan et al. (2010) calculated standardised RRs using the direct standardisation method with the lowest exposed group as the referent. Zhivin et al. (2016) and Bouet et al. (2019) used grouped Poisson regression adjusted for sex, age, calendar period, socio-economic status, subcohort, and concomitant exposures to trichloroethene, heat, and noise. (274) Three of the case–control studies used conditional logistic regression to estimate risk (Richardson and Wing, 2006; Yiin et al., 2009; Grellier et al., 2017). Risk sets were formed using incidence density matching with replacement based on attained age of the case. Richardson and Wing (2006) matched controls to cases on birth year, sex, race, socio-economic status, length of employment, and employment status at the attained age at death of the case. Yiin et al. (2009) selected five controls from the risk set for each case matched on sex, race, and living as long as the case; and Grellier et al. (2017) selected one to three controls matched on age, sex, and facility. Yiin et al. (2017, 2018) used Cox proportional hazards analysis to estimate risk. For each outcome, risk sets were drawn from the cohort using incidence density matching on sex, race, attained age, birth date, and plant of the case.
3.3.3. Results by organ system
3.4.3.1. Lung cancer
(275) Studies of occupational exposure to uranium do not generate reliable findings unless the risk of cancer can be expressed in terms of organ-/tissue-specific doses from internally deposited uranium. Many studies that include uranium workers do not use uranium-specific doses, but 11 studies that have examined the association between lung cancer have employed uranium internal doses or dose proxies (Richardson et al., 2006; Chan et al., 2010; Guseva Canu et al., 2010; Boice et al., 2011; Silver et al., 2013; Zhivin et al., 2016; Grellier et al., 2017; Yiin et al., 2017; Bouet et al., 2019). These quantitative results are presented in Table 3.2. (276) The majority of selected studies have shown no significant increase in the risk of lung cancer with lung dose from uranium. A single French study (Guseva Canu et al., 2011a) found significant increases for exposure to reprocessed but not unirradiated uranium. Studies of cohorts of uranium enrichment workers in France (Zhivin et al., 2016) and in the USA (Yiin et al., 2017), exposed mainly to rapidly soluble uranium compounds, did not find a significant risk of lung cancer. The study by Ritz et al. (2000) is the only study to find a significant dose–response relationship; this cohort was exposed to a mixture of uranium and fission products. (277) The studies of Grellier et al. (2017) and Silver et al. (2013) indicate a positive dose–response relationship, but both with large CIs that cannot exclude the absence of a trend with uranium dose. In the Alpha-Risk study of Grellier et al. (2017), when testing the influence of specific employer groups, the risk coefficients for AWE and BNFL were in opposite directions. (278) For most of the workers included in these studies, the estimates of mean lung dose from uranium were very low. In the study by Yiin et al. (2017), the average absorbed lung dose linked to uranium exposure was 0.07 mGy, while the cumulative external gamma dose to the lung was 40 mGy. In the case–control study of Grellier et al. (2017), the median lung dose from uranium was 2.2 mGy (with a maximum value of 301.5 mGy), while the mean dose from gamma radiation was 33.9 mGy (with a maximum value of 308 mGy). The study by Golden et al. (2019) reported a median lung dose from uranium of 33.1 mGy, with a maximum value of 885.2 mGy. The study by Bouet et al. (2019) reported a mean lung dose from uranium of 4.22 – 10.9 mGy, depending on modelling hypotheses, while the cumulative external gamma dose to the lung was 11.12 mGy. (279) In order to increase statistical power and take into account uncertainty linked to the estimated individual doses from uranium exposure, a large international effort with a common protocol for data collection, organ dose calculations focusing on those uranium oxide components that may contribute substantially to the lung dose, and appropriate analysis of results is necessary to achieve a better estimate of the risk of lung cancer from uranium exposure. Dose–response analyses of uranium-specific lung doses and risk of lung cancer. RR, relative risk; ERR, excess relative risk; HR, hazard ratio; SRR, standardised rate ratio; CI, confidence interval.

3.4.3.2. Kidney cancer
(280) Toxicological data show that uranium causes damage to the kidneys after acute high-level exposure to uranium, which is a heavy metal that preferentially accumulates in, and is eliminated from the body via, the kidneys. The organ-specific doses received from uranium in the studies that have considered kidney cancer are very low. The studies presented in Table 3.3 cannot clearly confirm a carcinogenic effect at low chronic exposure; although some studies indicate a positive trend, the large CIs include the possibility of the absence of an effect. (281) A single study by Golden et al. (2019) revealed a significantly positive dose–response relationship, where the dose to the kidneys was from combined external and internal exposures and not specifically from uranium exposure. When the toxicological effect of uranium was considered by controlling for the level of dust exposure encountered by the workers, the risk increased with a hazard ratio (HR) of 1.85 (95% CI 1.09–3.14) at 100 mGy; the dose–response relationship over cumulative dust exposure categories was not significant. Of the 17 deaths from kidney cancer included in the study by Golden et al. (2019), 16 were from cancer of the renal parenchyma, and one was from cancer of the ureter (no deaths from cancer of the renal pelvis were observed). In contrast, kidney cancers linked to radiation exposure are sited in the renal pelvis and ureter (primarily transitional cell carcinomas), and not in the renal parenchyma, except at very high therapeutic doses. (282) Improvement should be possible in future through consideration of the heterogeneity of the distribution of uranium in the different parts of the kidney, and identifying the part of the kidney where the cancer occurs, as these may differ for radiation vs chemically associated effects. Dose–response analyses of uranium exposure and risk of kidney cancer. CI, confidence interval; ERR, excess relative risk; HR, hazard ratio; RR, relative risk.

3.4.3.3. Lymphatic and haematopoietic cancers
(283) Results related to uranium-specific doses and risk of lymphatic and haematopoietic cancers are presented in Table 3.4. Among the 16 selected studies, results are presented using the malignant disease groupings of leukaemia, other lympho-haematopoietic cancers – Hodgkin’s lymphoma, non-Hodgkin’s lymphoma, and multiple myeloma – and all lympho-haematopoietic cancers combined. Three studies by Yiin et al. (2009, 2017, 2018) of US uranium enrichment plant workers have consistently reported a significantly increased uranium-associated risk of multiple myeloma, although the SMR for multiple myeloma was slightly less than unity (Yiin et al., 2017). Such an association has not been reported from other studies of uranium workers, although investigation of the subject has been limited. Chan et al. (2010) found an indication of an effect of uranium exposure upon the risk of non-Hodgkin’s lymphoma, but with no apparent trend with level of exposure. For the other lympho-haematopoietic cancer groupings, no increase in risk with exposure to uranium was observed. (284) The issues considered above for the lung cancer and kidney cancer studies apply to these studies of lympho-haematopoietic cancers as well, in particular that the organ-/tissue-specific doses received from exposure to uranium are very low. An additional difficulty in comparing these studies is the grouping of outcomes in multiple ways: all lympho-haematopoietic cancers, non-Hodgkin’s lymphoma, multiple myeloma, and others. Not only are there multiple groupings but the International Classification of Diseases codes used to define each grouping may not be the same across studies. Dose–response analyses of uranium exposure and risk of lymphatic and haematopoietic cancer. CI, confidence interval; ERR, excess relative risk; HR, hazard ratio; LHP, all lympho-haematopoietic cancers; MM, multiple myeloma; NHL, non-Hodgkin’s lymphoma; OR, odds ratio; RR, relative risk; SRR, standardised rate ratio.
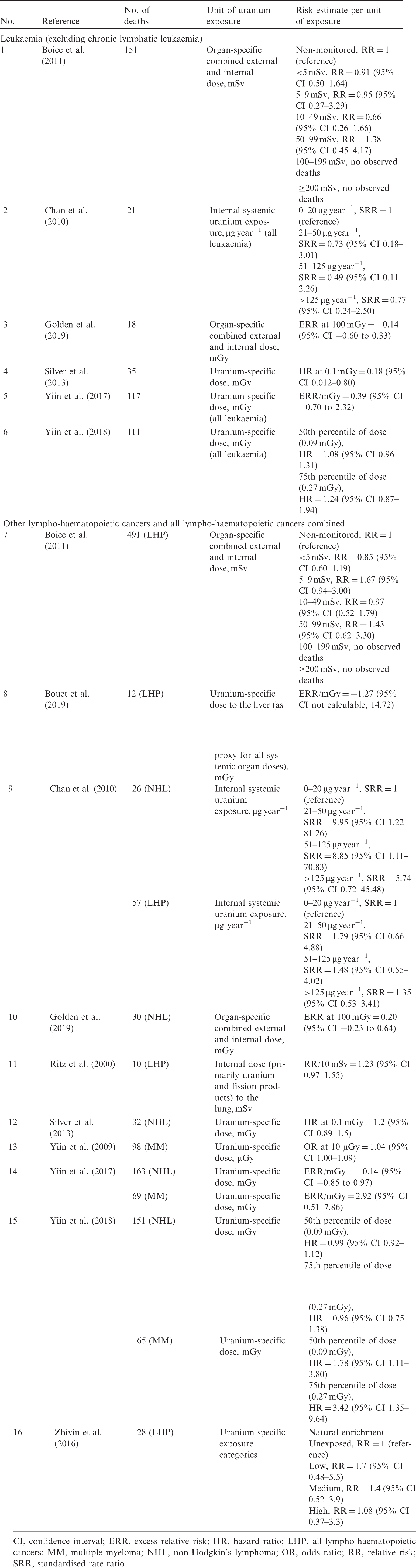
3.4.4.2. Environmental exposure to uranium
(285) Studies of people living near uranium processing facilities have not provided evidence for any increased risk of cancers related to uranium exposure (UNSCEAR, 2017). (286) The evidence for uranium carcinogenicity linked to ingestion remains limited. In a review of epidemiological studies of possible health effects after ingesting naturally occurring radionuclides through drinking water, Guseva Canu et al. (2011b) considered 27 peer-reviewed articles published between 1970 and 2009 reporting original results, including studies of uranium, radium, and radon in drinking water. Among these, five individually based studies provided results on a potential association between the risk of cancer and uranium concentration. A case–control study of non-Hodgkin’s lymphoma in Saskatchewan (Canada) found higher uranium concentrations in the drinking water of cases than of controls (Witmans et al., 2008). A leukaemia case–control study in Fallon (USA) found no significant differences in well-water uranium or radon concentrations between cases and controls (Seiler, 2004). The only cohort study was conducted among Finnish individuals using bedrock well-water. On the basis of this cohort, three case–cohort studies were conducted, using individual-level exposure assessments, of 35 leukaemia cases (Auvinen et al., 2002), 107 stomach cancer cases (Auvinen et al., 2005), and 112 urinary cancer cases, including kidney cancer (Kurttio et al., 2006b). No significant associations were reported, either with radionuclide concentrations in well-water (uranium, radium, and radon) or with cumulative radiation doses when estimated. (287) Weak but significant associations between uranium concentration in drinking water and cancers have been observed in ecological studies in Bavaria (Banning and Benfer, 2017) and South Carolina (Wagner et al., 2011). (288) Overall, the available results do not demonstrate convincing evidence for an association between uranium in drinking water and risk of cancer. However, only a few studies have been conducted to date, and methodological limitations (poor exposure measurement methods, no control for confounding, small sample size) affect most of them. (289) The effects of exposure to depleted uranium have received attention in extensive reviews of the health of Gulf War veterans (Harley et al., 1999; Royal Society, 2001, 2002; Depleted Uranium Oversight Board, 2007; Committee on Gulf War and Health, 2008; IARC, 2012). The issue of health effects following exposure to depleted uranium was examined in the UNSCEAR 2016 Report (UNSCEAR, 2017), and no excess risk of cancer has been identified among those individuals exposed to depleted uranium.
3.3.4. Discussion
3.4.4.1. Summary of results from studies of workers
(290) At present, there is only weak epidemiological evidence to suggest an association between internal organ-/tissue-specific radiation dose resulting from exposure to uranium and risk of cancers that have been studied. However, the size of the study populations limits the statistical power to detect an association, and the organ/tissue doses are relatively low in most studies. The main limitation is the lack of precise estimates of internal uranium-specific dose to the individuals included in studies. (291) Contrary to the situation for plutonium, present knowledge of risk of cancer associated with uranium exposure does not permit calculation of lifetime risk of cancer. (292) One study suggested a positive association between insoluble forms of reprocessed uranium and lung cancer (Guseva Canu et al., 2011a) on the basis of a job-exposure matrix. Grellier et al. (2017) and Silver et al. (2013) showed a positive trend between the lung dose estimated from chronic uranium exposure and risk of lung cancer, but the CIs of these positive trends did not exclude the absence of a trend. In future, research into the risk of lung cancer should focus primarily on workers being exposed to insoluble uranium compounds as these workers will have received the largest lung doses. Smoking habits should also be taken into account if information is available, and chemical exposures during uranium processing also need to be considered (Ritz, 1999). (293) Positive results have been reported for kidney cancer in various parts of the nuclear fuel cycle. Golden et al. (2019) reported a significant dose–response relationship, but for the combined doses to the kidneys from external and internal exposures and not just uranium exposure. Silver et al. (2013) and Yiin et al. (2017, 2018) found positive trends with uranium-specific dose to the kidneys, but with CIs that did not exclude the absence of a trend. (294) Among gaseous diffusion plant workers, there is a suggestion of an increase in the risk of various types of lymphatic and haematopoietic cancers, although not leukaemia, with uranium exposure. Yiin et al. (2009, 2017, 2018) found increased risk of multiple myeloma associated with the dose to RBM from exposure to uranium, after adjusting for external radiation resulting from occupational chest x rays and film badge records. Chan et al. (2010) reported an increased risk of non-Hodgkin’s lymphoma with exposure to uranium, but with no apparent trend with level of exposure. (295) Overall, epidemiological studies of uranium workers do not provide convincing evidence of increased risk of cancer that can be attributed to uranium exposure. Even studies of lung cancer following inhalation of insoluble compounds of uranium, which lead to the highest lung doses from uranium, have provided inconclusive evidence, and the results from studies of other sites of cancer do not provide a consistent pattern of findings. Further high-quality studies are required to improve this situation.
3.4.4.3. Complexity of exposure and dose reconstruction
(296) Differences in the solubility of uranium and methods used to measure uranium-specific doses complicate the interpretation of results with respect to internal uranium exposure. Studies have included workers employed in uranium processing and reprocessing operations, where the solubility of the uranium ranged from very soluble to insoluble. (297) In their case–control study of multiple myeloma, Yiin et al. (2009) assigned absorbed doses to the specific organ of interest, namely RBM; doses to RBM from photofluorographic chest x rays documented in the workers’ occupational medical records were included as a separate variable in analyses. Boice et al. (2006a,b) used ICRP biokinetic models from then-current or upcoming ICRP publications to estimate annual equivalent doses to 16 specific organs or tissues, taking into account time of exposure, type of radionuclide, and excretion patterns. Other studies included an estimate of internal radiation exposure but not the calculation of doses to target organs. Ritz et al. (2000) estimated lung dose based on uranium urinalysis results, and used this dose as a surrogate for all organs of interest. Guseva Canu et al. (2010) estimated exposure to uranium based on a job-exposure matrix where different uranium compounds were distinguished by their absorption type (F, M, or S) and their isotopic composition (natural uranium and reprocessed uranium-bearing compounds). Chan et al. (2010) also used uranium urinalysis results but reported cumulative excretion as microgram-years (µg.y). The use of µg.y as a measure of internal exposure is questionable as it depends on the frequency of monitoring. During recent years, more studies have provided estimates of organ-/tissue-specific doses from uranium. In the Alpha-Risk case–control study, Grellier et al. (2017) assigned best estimates of individual organ/tissue doses. In a study combining cohorts of gaseous diffusion plant workers (Yiin et al., 2017, 2018), organ/tissue doses were calculated using extensive uranium urinalysis data along with uranium gravimetric and radioactivity concentration data, and estimates of enrichment levels of uranium to which workers may have been exposed (Anderson et al., 2017). Ellis et al. (2018) described the methodology that was used to update the Mallinckrodt Chemical Works uranium processing workers cohort following the framework outlined by Bouville et al. (2015). (298) The calculations of external radiation exposure for the uranium worker studies were similar to those used for the plutonium worker studies in terms of the variability in the methods used. Most cohort studies limited external exposure to recorded exposure to gamma and x rays at the site. In addition to external radiation monitoring records from the site, Boice et al. (2006a,b, 2011), Golden et al. (2019), and Yiin et al. (2009) included these records from other sites and databases. Yiin et al. (2009) included gamma and x rays alone, while Richardson and Wing (2006) included tritium; all three imputed exposures for missing records.
3.4.4.4. Recommendations for future studies
(299) The information from current epidemiological studies of uranium exposure is insufficient to reliably quantify dose–response relationships in terms of organ-/tissue-specific doses from uranium. More studies are needed before any estimate of risk and detriment can be envisaged. (300) Work is already ongoing to enable future combined studies of uranium workers which will greatly improve the statistical power of the studies. The protocol of an international pooled analysis of uranium processing workers, including cohorts from the USA, Europe, and possibly other countries, is currently being developed. More than 15 cohorts including 100,000 uranium processing workers are potentially eligible for inclusion. As part of this project, a dosimetric protocol aiming to harmonise uranium exposure information and organ-/tissue-specific dose calculations across cohorts is being developed. The improved statistical power of this analysis will allow the proposed collaborative study to have greater ability to characterise potential risks associated with occupational uranium exposure. (301) In the USA, work is progressing on the Epidemiologic Study of One Million Persons. A component of this study includes Department of Energy nuclear workers who have been exposed to uranium (and plutonium) (Boice et al., 2018). Over 360,000 workers employed at 15 Department of Energy (and its predecessor) facilities have been identified. The goal of the pilot project is to characterise these workers with regard to vital status follow-up, external dose, and potential for internal intakes. The focus of the effort will be on those workers already included in a retrospective cohort mortality study. Vital status is being updated using a common protocol. Bioassay and external radiation monitoring data have been computerised, and the methodology that will be used to perform the organ-/tissue-specific dose estimations has been established (Bouville et al., 2015). A pooled analysis of approximately 13,000 North American workers involved in uranium milling and processing is currently underway. The methods being used are very similar to those used in the One Million Persons study.
4. Conclusion
(302) The risks of cancer following exposure to alpha-particle-emitting isotopes of plutonium and uranium have been evaluated in the present publication, which is complementary to Publication 115 (ICRP, 2010) focusing on exposure to radon and its decay products. The publication updates previous reviews published by national and international committees on exposure to plutonium and uranium, especially the IARC monograph on internal emitters in 2012 (IARC, 2012), Annex D of the UNSCEAR 2016 Report on the biological effects of exposure to uranium (UNSCEAR, 2017), and the BEIR IV Report (NRC, 1988). The close collaborative work between experts of ICRP Committee 1 and Committee 2 and other experts with competences in epidemiology or dosimetry was key for preparing this publication, which constitutes the first comprehensive review of health risks associated with plutonium exposure for over 30 years. (303) Compared with radon and its decay products, the epidemiological evidence on risks associated with exposure to plutonium is less extensive. Indeed, the first epidemiological results from underground hard-rock miner studies were published towards the end of the 1960s, whereas most of the results related to plutonium have been published since 1990. Further, the number of studies providing reliable results on plutonium-specific risks is limited to a few studies (essentially the MWC and SWC), whereas approximately 20 cohorts of miners have been studied, plus several tens of indoor radon studies in the general population. In addition, the assessment of doses due to plutonium exposure is complicated by the chemical nature of plutonium compounds, which plays a major role in determining lung solubility, and presents difficulties in the reconstruction of lung doses from bioassay measurements of plutonium concentrations in urine or faeces. These differences may partly explain the fact that results on plutonium-related risks are presently less consistent than those related to radon. The situation is more striking for uranium-specific risks, with the information currently available from epidemiological studies being insufficient to provide reliable estimates of risk, particularly due to limits in exposure reconstruction. Further studies with improved internal dosimetry are needed. (304) Most of the cohorts of workers studied had a long follow-up (over several decades). A good understanding of the dosimetric approaches used in the past, or of surrogates such as job-exposure matrix approaches, was necessary to evaluate the quality and reliability of the individual annual organ-/tissue-specific doses used in the epidemiological analyses. The number and quality of bioassay measurements per individual, the quality of environmental measurements, and the solubility of the inhaled radionuclide and its chemical compounds are some of the factors that influence the quality of estimates of organ-/tissue-specific dose over time. (305) Risk of cancer resulting from plutonium exposure has been examined through studies of Russian, American, and European workers, which include a wide range of exposure levels. The two most informative cohorts of plutonium workers are those employed at Mayak PA in the Russian Federation and at Sellafield in the UK. Assessments of intakes and resulting organ/tissue doses for workers arising from the inhalation of plutonium (principally 239Pu) have been based primarily on the interpretation of individual urine bioassay data, taking account of the workers’ occupational histories and the physicochemical forms of the inhaled plutonium aerosols. Results from autopsy data have also been used to determine model parameter values. Biokinetic and dosimetric models have been improved continuously over the last 20 years, but significant uncertainties remain in the assessed doses. The epidemiological studies of plutonium workers provide results that allow quantitative estimation of risk of lung cancer related to alpha-particle dose. Much of the evidence is based upon data for male smokers. For risk of cancers other than lung cancer, associations between plutonium exposure and risk of liver and bone cancers were also observed in the Mayak studies, as would be anticipated from the preferential deposition of plutonium in the liver and on bone surfaces, although data are limited and do not, as yet, permit detailed quantitative evaluation. There is no consistent evidence of a positive dose–response relationship between the risk of leukaemia and plutonium exposure. (306) Calculations have been conducted of the lifetime excess risk of lung cancer mortality associated with lung absorbed dose, based on scenarios of inhalation of a total plutonium intake of 1 Bq, assuming either acute intake or chronic intake, of either soluble plutonium nitrate or insoluble plutonium oxide. These unitary intake scenarios should be considered as examples to provide an order of magnitude of the risk, and to illustrate variations in the dose and risk for a unitary intake. (307) Comparing the lifetime excess risk of lung cancer mortality from exposure to external gamma radiation (based on the LSS of Japanese atomic bomb survivors) and from internal exposure to plutonium alpha particles (based on the Mayak workers study), it was found that, for the same lung absorbed dose, the risk from plutonium alpha-particle exposure is greater than the risk from external gamma-ray exposure by factors of approximately 15–16 and 19–22 when based on the LSS ERR model and EAR model, respectively, depending on the exposure scenario. Despite the very different dose distributions of plutonium and radon progeny within the lung, a similar calculation for radon progeny exposure produced factors based on the ERR model of approximately 14–15. These results suggest a biological effectiveness of alpha particles relative to high-energy photons equal to approximately 14–16 for lung cancer. (308) These values are compatible with the current wR of 20 used for the purposes of radiological protection by the Commission for alpha particles in the calculation of equivalent and effective doses (ICRP, 2007). Nevertheless, it should be noted that this comparison is based on lung absorbed dose and lifetime excess risk of lung cancer mortality, with application of a DDREF of 2 to the risk derived from the Japanese LSS. Not applying a DDREF would lead to RBE of approximately 7–8. Also, this comparison of the effects of plutonium exposure and external gamma exposure is based on the lifetime risk of lung cancer mortality, and not on radiation detriment. Meanwhile, wR is a judgement value for radiological protection purposes and applies to all stochastic effects of alpha radiation, including other types of cancer. Plutonium-related risks have been observed for the liver and bone for which different RBEs for alpha radiation may apply. (309) The review of recently published epidemiological studies of the risk of cancer from exposure to uranium updated the UNSCEAR 2016 Report (UNSCEAR, 2017). Most studies did not use uranium-specific doses to organs/tissues derived from monitoring results, and considered exposure through environmental indicators, job-exposure matrices, or expressed the risk in relation to external radiation exposure. A few studies published in recent years used improved organ-/tissue-specific uranium dose calculations, but they remain inconclusive because statistical power was limited or because some of the information needed to reconstruct doses was not recorded in the past. Relatively fast clearance of uranium from blood circulation, variability of exposure to uranium compounds, and differences in the methods used to monitor internal exposure to uranium complicate the dosimetry of workers employed in uranium processing, concentration, enrichment, and reprocessing operations. The solubility of the uranium compounds to which workers are exposed is an especially important parameter in determining lung doses from bioassay data. In summary, with the information from currently available epidemiological studies, there are insufficient data to reliably estimate the dose–response relationships between uranium exposure and any cancer site. (310) Uncertainties associated with plutonium and uranium exposure and dose reconstruction are important, and different chemical forms can lead to very different cumulative organ-/tissue-specific absorbed doses per Bq intake. Important concerted efforts have been made in recent years to improve organ-/tissue-specific dose assessment and to consider the potential impact of uncertainty on risk estimates. Continuation of such efforts and consideration of improved dosimetric approaches is recommended for future research, as the isotopes of these two elements continue to be of major importance for some groups of workers in the nuclear industry. Also, extension of existing cohorts and combined analyses of data are needed to increase power and allow a better estimation of the risks associated with plutonium and uranium exposures. Further research is needed to improve assessment of health risks associated with plutonium or uranium exposure in epidemiology, dosimetry, and risk modelling. Future research may better characterise the risks associated with alpha particles emitted by plutonium for cancer induction in organs other than the lung. For uranium, distinction of the different chemical forms of uranium compounds in future analyses is highly desirable. Future pooled analyses are expected to provide additional information on potential risks associated with uranium exposure.
REFERENCES
ANNEX A. RISK OF CIRCULATORY DISEASES FROM EXPOSURES TO PLUTONIUM AND URANIUM
(A1) In addition to the risk of cancer, several epidemiological studies of populations exposed to plutonium or uranium also considered other health effects, particularly diseases of the circulatory system. Being outside the scope of the present publication, these results are summarised in this annex.
A.1. Plutonium exposure and risk of circulatory diseases
(A2) The incidence and mortality risks from circulatory diseases have been analysed in the MWC. The first such study (Azizova et al., 2010a,b) considered a cohort of 12,210 Mayak workers first employed at one of the main facilities during the first 10 years of operation (1948–1958). This period corresponded with the first years of Mayak PA operation, when workers were exposed to high doses of both external gamma rays and internal alpha-particle radiation due to plutonium intake. This study showed a significant effect of external and internal plutonium exposures on the risk of circulatory diseases. Further analyses of both ischaemic heart disease (IHD) (Azizova et al., 2012) and cerebrovascular disease (CeVD) (Azizova et al., 2011) were performed on an expanded MWC with an additional 6553 workers first employed in 1959–1972. The cohort included 18,763 workers (25% females) first employed at one of the main facilities of Mayak PA (i.e. reactors, radiochemical, and plutonium plants) in 1948–1972. Workers employed at the radiochemical and plutonium production facilities could be exposed to both external gamma rays and internal alpha-particle radiation from incorporated plutonium. Liver absorbed doses were estimated using the respiratory tract model described by Khokhryakov et al. (2005), and the systemic model for plutonium of Leggett et al. (2005). Follow-up was extended to the end of 2005. The numbers of observed cases (deaths) were 6134 (2629) for IHD and 7326 (1495) for CeVD. Data on non-radiation circulatory disease risk factors such as smoking (available for 91.5% of workers), alcohol consumption (86.5%), blood pressure (95.2%), and body mass index (79.6%) were collected. (A3) A significant increasing trend was demonstrated for the incidence of CeVD with increasing total internal alpha-particle dose to the liver. Estimated ERR Gy−1 increased with increasing lag period. The relationship persisted after adjustment for body mass index, duration of employment, and external radiation exposure. The evidence for this trend related mainly to males rather than females (P-value for interaction <0.001), and to radiochemical facility workers rather than plutonium facility workers (P-value for interaction = 0.001). Notably, there was no significant trend in CeVD mortality (rather than incidence) in relation to internal alpha-particle liver dose. (A4) No significant trend was observed for the incidence of IHD with absorbed dose to the liver from internal alpha-particle radiation, either with or without adjustment for external gamma-ray dose. For IHD mortality, an increasing trend was observed with liver dose from internal alpha-particle exposure, but estimated ERR Gy−1 became lower and was non-significant after adjustment for external exposure. (A5) The SOLO project considered circulatory disease mortality in the MWC and SWC, and where appropriate (i.e. in the absence of significant heterogeneity between the two cohorts) in the combined cohort (Azizova et al., 2018). The study examined circulatory diseases as a whole, and also examined IHD and CeVD mortality separately. Doses used in the analyses were the cumulative external Hp(10) dose and the cumulative absorbed dose to the liver from alpha particles emitted by deposited plutonium. In respect of external dose, ERR Sv−1 estimates were significantly increased for both worker cohorts (marginally so for the MWC) for all circulatory diseases combined and IHD (but not for CeVD), but differed significantly between the two cohorts, with the estimate for the SWC being approximately 10 times greater than that for the MWC. In respect of the internal liver dose from plutonium, estimated ERR Gy−1 did not differ significantly from zero for either the MWC, the SWC, or the pooled plutonium worker cohort (PuWC) for mortality from circulatory diseases, IHD, or CeVD. For circulatory diseases, estimated ERR Gy−1 was 0.03 (95% CI −0.07 to 0.17) for the MWC, 1.06 (95% CI <0–3.49) for the SWC, and 0.04 (95% CI −0.06 to 0.18) for the PuWC; for IHD, estimated ERR Gy−1 was +0.00 (95% CI <0–0.20), 0.61 (95% CI <0–3.12), and 0.02 (95% CI <0–0.22), respectively; and for CeVD, estimated ERR Gy−1 was 0.07 (95% CI <0–0.37), 3.75 (95% CI <0–12.44), and 0.08 (95% CI <0–12.44), respectively.
A.2. Uranium exposure and risk of circulatory diseases
(A6) A significant association between circulatory disease mortality and external radiation dose was observed among male radiation workers of BNFL (McGeoghegan et al., 2008). Although part of this cohort consisted of uranium workers (37% of the cohort was employed at Springfields uranium processing installation and 6.8% at Capernhurst uranium enrichment installation) and plutonium workers (50.5% of the cohort was employed at the Sellafield reprocessing installation), no formal study of the effects of uranium or plutonium doses on the circulatory system has been performed to date. However, the circulatory disease mortality ERR Sv−1 associated with external exposure to gamma radiation was notably less for those monitored for exposure to internally deposited radionuclides compared with unmonitored workers. (A7) One cohort study suggested an increasing circulatory disease mortality risk related to insoluble uranium exposure in France (Guseva-Canu et al., 2012). The cohort considered 2897 workers employed at the AREVA NC Pierrelatte uranium processing plant between 1960 and 2006 (79,892 person-years). Cumulative exposure to different uranium compounds, classified by isotopic composition and solubility type, was assessed using a plant-specific job-exposure matrix. HR and associated 95% CIs were estimated using Cox regression models accounting for sex, calendar period, initial socio-economic status, and associated exposure. The number of circulatory disease deaths was 111, including 48 from IHD and 31 from CeVD. Circulatory disease mortality risk appeared increased among workers exposed to insoluble compounds of reprocessed uranium [HR = 2.07 (95% CI 0.99–4.99)], but this result was based on a limited number of workers (n = 9). (A8) A nested case–control study has been performed in French AREVA NC Pierrelatte nuclear workers employed between 1960 and 2005 to estimate circulatory disease risks, adjusting for major circulatory disease risk factors (smoking, blood pressure, body mass index, total cholesterol, and glycaemia) and external gamma-radiation dose (Zhivin et al., 2018). The study included 102 deaths from circulatory diseases and 416 controls individually matched on age, gender, birth cohort, and socioprofessional status. Information on circulatory disease risk factors was collected from occupational medical records. Organ-/tissue-specific absorbed doses were estimated using biomonitoring data, taking into account exposure regime and uranium physicochemical properties. External gamma radiation was measured by individual dosimeter badges. Workers were exposed to very low doses of radiation (mean gamma-radiation dose of 2 mGy and lung uranium dose of 1 mGy). A positive but imprecise association was observed [EOR mGy−1 0.2 (95% CI 0.004–0.5)]. Results obtained after adjustment suggested that uranium exposure might be an independent circulatory disease risk factor. The authors concluded that a positive association might exist between internal uranium exposure and circulatory disease mortality, not confounded by circulatory disease risk factors, but caution should be exercised in interpreting the results due to numerous uncertainties associated with internal uranium dose estimation.
A.3. Conclusion
(A9) Some results are suggestive of an association between plutonium or uranium exposure and increased risk of circulatory diseases. In particular, some results from the MWC suggest an association between plutonium exposure and risk of both CeVD and IHD. Nevertheless, the results are based on a small number of studies, and some discrepancies and inconsistencies persist, between and within cohorts, and between incidence and mortality data. Extension of these studies in the future is needed, as well as verification of the repetition of such results in other populations.