
Abstract
At the request of the Main Commission of the International Commission on Radiological Protection (ICRP), Task Group 107 (TG107) was set up to consider the issue of radiological protection of the patient in veterinary medicine. TG107, who authored this article, brought together information relating to the use of diagnostic imaging and radiation oncology in veterinary medicine. A number of specific areas were identified that appeared to be appropriate for attention by ICRP. These included the use of dose quantities and units, the need for re-evaluation of stochastic and deterministic risks from ionising radiation in animals, and the growing use of imaging and therapeutic equipment for animals that is little different from that available to humans. TG107 unanimously recommended that it was both appropriate and timely for ICRP to consider and advise on these issues, and the Main Commission agreed. This paper summarises the findings of TG107.
Keywords
1. INTRODUCTION
Concerns about radiological protection of the animal as the patient in veterinary medicine were first raised by Pentreath (2016), and the International Commission on Radiological Protection (ICRP) quickly responded by announcing the establishment of Task Group 107 (TG107) to advise the Main Commission on the subject (Clement, 2018). The issues to be addressed by TG107 were: the extent to which ionising radiation is used in veterinary medicine; the international setting in which any specific advice on the radiological protection of the animal as the patient is already being provided; the areas that it would be most useful for ICRP, together with the veterinary profession, to pursue in order to provide further advice; and the broader implications for ICRP and, indeed, for the radiological protection community as a whole, should it become involved in this subject. TG107, chaired by Jan Pentreath, completed its task and presented its findings to ICRP in October 2018. This article is a brief summary of the findings.
2. USE OF RADIATION IN VETERINARY MEDICINE
Radiation is now widely used in veterinary medicine, and its rapid growth parallels that in human medicine. Most clinics in Europe and North America have access to x-ray machines, and increasing use, at specialist centres, is made of computed tomography (CT), fluoroscopy, gamma camera imaging, positron emission tomography (PET), and combined single-photon emission computed tomography (SPECT)/CT and PET/CT scanners. Radiotherapy may include superficial or orthovoltage (keV) units; cobalt-60 units; intensity-modulated radiation therapy; brachytherapy; the use of radioiodine, technetium, or linear accelerators; and multi-leaf collimators. The basic equipment used is essentially the same as that for humans, but procedures can take place in a variety of non-dedicated facilities that may pose unique problems and necessitate specific education and training for veterinary practitioners. The handling of animals in many situations may involve the presence of specialised personnel (animal handlers), which may also result in the need to take specific protective measures.
Not all radiographic examinations are undertaken because the animals are unwell. One of the most frequent uses of radiography seems to be the examination of horses prior to their purchase, or for breeding, as a result of which they may be examined many times throughout their lives. Dogs are also radiographed as part of selective breeding programmes. Sheep, pigs, and other animals may be CT scanned simply to assess their fat and meat content.
By and large, the majority of animals examined, and treated, are essentially ‘valuable’ in one sense or another, but the list of those known to be examined or treated includes small and large animal pets (also referred to as ‘companion animals’), exotic pets such as reptiles, and those in zoological gardens and wildlife parks. Radiation therapy primarily relates to cats, dogs, and horses, and may involve brachytherapy and the application of radionuclides.
It is presumed that the use of these techniques around the world will increase as facilities become more available, the costs of examination and treatment reduce, and the demand from animal owners increases (Baker, 2017). There are already tele-imaging, for-profit, veterinary companies that provide certified veterinary radiologists, but the lack of published literature to demonstrate standardisation, guidelines, and protocols suggests that there are opportunities for ICRP to collaborate in this area of radiological protection. There is also a growing awareness within the veterinary profession that there is a greater need for guidance and the establishment of best practice, although this need has been primarily in the context of the radiological protection of veterinarians, their staff, and the owners of the animals, rather than of the animals themselves. The number of facilities used for diagnostic or therapeutic veterinary medicine worldwide is not known, but there are over 100 radiation oncology treatment sites registered in the USA alone. There are more than 20 centres across Europe that provide megavoltage, brachytherapy, and orthovoltage therapies, and there are probably many more centres that provide radioiodine treatment (predominantly for hyperthyroid cats) and a few centres that provide other radionuclide therapies. There are currently eight small veterinary teaching hospitals and three private referral hospitals using megavoltage facilities in Japan. There are even more diagnostic radiology facilities within the USA, Europe, and Japan. Many private practices and most veterinary colleges now have CT scanners. Some of these scanners may be ‘second hand’.
3. CURRENT RADIOLOGICAL PROTECTION ADVICE FOR VETERINARIANS
Specific advice on the subject of radiation protection in veterinary medicine has been produced in some countries, aimed at the veterinary practitioners and, to a limited extent, the owners of the animals, but not the animals themselves. Such examples are those issued by the Radiological Protection Institute of Ireland (RPII, 2002), the National Council on Radiation Protection and Measurements (NCRP, 2004), and the Australian Radiation Protection and Nuclear Safety Agency (ARPANSA, 2009), and in a leaflet by the Heads of the European Radiological Protection Competent Authorities (HERCA, 2020). In the USA, the American College of Veterinary Radiology and the American Veterinary Medical Association provide their members with advice on radiation safety and treatment protocols. In addition, the American Hospital Association provides accreditation and some radiation safety training, and the Veterinary Interventional Radiology and Interventional Endoscopy Society aims to advance the art and science of veterinary interventional radiology, interventional endoscopy, and other image-guided procedures. Also of relevance is the Veterinary Cancer Society, which has members beyond the USA. Elsewhere, there are national organisations, such as the Australasian Association of Veterinary Diagnostic Imaging which covers both Australia and New Zealand, the Japanese Veterinary Medical Association which provides information concerning radiation safety and the handling of animals, and the Japanese Society of Veterinary Science which has an advisory board for providing radiation safety and related guidelines. Within Europe, there is the European College of Veterinary Diagnostic Imaging which consists of specialists in both diagnostic imaging and radiotherapy, and the European Association of Veterinary Diagnostic Imaging. There is also the International Veterinary Radiology Association. There are no formal connections between any of these bodies and ICRP, and no known connections between these bodies and the International Commission on Radiation Units and Measurements (ICRU), the International Radiation Protection Association (IRPA), the International Atomic Energy Agency (IAEA), and any other international body with radiological protection responsibilities or interests.
Notwithstanding the above professional bodies, it seems that there is still considerable opportunity for radiation protection guidance and collaboration within the veterinary profession. A recent survey of veterinary specialists in the USA (Gregorich et al., 2018) concluded that: ‘Radiation safety training, although more common in academia, was not universally available and may not meet radiography equipment license requirements for some institutions. Most radiologists, internal medicine clinicians, and EEC clinicians had a poor understanding of the amount of ionising radiation associated with medical imaging procedures and the potential hazards to their patients’. Apparently, 34% of those asked did not know what ‘ALARA’ (as low as reasonably achievable) stood for.
It is therefore of interest that IAEA, under the umbrella of its Fundamental Safety Principles, has drafted a safety report on ‘Radiation Protection and Safety in Veterinary Medicine’ to provide guidance with respect to veterinary uses of ionising radiation. This report, because of the limitations of the Basic Safety Standards to human radiation protection, does not mention any issues or guidance in relation to the protection of the animal as the patient.
4. SPECIFIC ISSUES
4.1. Dose quantities and units
Radiotherapy doses in veterinary medicine always appear to be expressed in Gy, but doses received by animals undergoing CT examination are usually expressed in terms of mSv (it is not always clear whether it is the equivalent dose or the effective dose that is implied in its use, although the latter is often specified). However, CT scanners estimate ‘dose’ based on the scan factors selected and on measurements made in the factory on cylindrical phantoms for human use. The quantities that the machines produce are volume CT dose index (CTDI volume), in mGy, and dose length product, which is the CTDI volume multiplied by the scan length, in mGy cm. This is the case for all CT scanners with respect to DICOM (Digital Imaging and Communications in Medicine) which is the international standard for transmitting, storing, retrieving, printing, processing, and displaying medical imaging information. These measured quantities may be converted to effective dose or organ dose estimates by third parties in order to arrive at ‘risk’ estimates depending on the organ irradiated. The results are then expressed as mSv. Scanners also produce a ‘patient protocol’ after a CT examination is completed, giving a breakdown of doses for each scan phase performed during the examination, and the cumulative dose. The ICRP guidance for medical imaging dose tracking is to use measured quantities rather than effective dose (ICRP, 2007a). It therefore appears that no CT scanner interpretation in veterinary medicine is based on any animal (non-human) data, but this fundamental point does not seem to be made explicit in the relevant veterinary publications. There also seems to be no acknowledgement that the quantities of equivalent and effective dose are related specifically to human beings, and that they are not, strictly speaking, scientific quantities but practical quantities created by ICRP for use in the calculation of reference doses for the purposes of human radiological protection. Neither is measurable, although both can be calculated.
4.2. Diagnostic procedures
A wide range of imaging modalities is now used in veterinary medicine for animals of all shapes and sizes (Fig. 1), including PET scans (Fig. 2). Such techniques are of value, but optimisation and an understanding of risks relating to all of these diagnostic procedures are not well documented. There are also concerns about the number of radiographs and, particularly, CT scans taken of the same animal; for example, by different potential buyers of a horse. Concerns have also been raised about the failure to determine, or even to consider, whether or not the animal is pregnant, and the failure to screen gonads in such procedures regardless of the reproductive state or age of the animal. Specific concerns have been raised about the lack of draped shielding in the radiography of dogs (Nemanic et al., 2015), and it is recommended that protective shielding should be used on all veterinary patients, drawing particular attention to the risks related to breeding animals, those receiving multiple radiographs over their lifetimes, and in breeds known to have increased susceptibility to cancer. In general, therefore, there appears to be nothing that is equivalent to the human medical imaging guidelines set out in Publication 121 (ICRP, 2013), and no equivalent approach to that of the use of diagnostic reference levels as advocated for human medical imaging in Publication 135 (ICRP, 2017).
A computer tomography scan of a 12-year-old cow (source: J. Gambino, Mississippi State University, USA). A portable positron emission tomography scanner being used for diagnosis of the left hind leg of a horse (source: Dr Spriet, UC Davis Veterinary Medicine, USA).

There is clearly scope to increase awareness of the basic principles of radiation protection in this field with respect to justification, optimisation, and dose limits. The overall problem with respect to diagnostic procedures is perhaps exemplified by a recent survey in the USA (Gregorich et al., 2018), which found that over 60% of veterinary radiologists and associated staff did not believe that the doses of ionising radiation used in veterinary CT scanning carried any increased risk of potentially fatal cancer to their patients. Indeed, the majority (74%) of those surveyed, even if they were aware of the risks, did not warn veterinary clinicians or animal owners that the use of ionising radiation in imaging procedures may carry an increased risk of cancer to the patient. The same study also concluded that there was probably a general belief that dogs and cats do not live long enough to develop cancer as a result of exposure to ionising radiation. This appears to be a common belief, notwithstanding the experiments with thousands of dogs, in particular, relating to cancer induction, from both internal and external sources, including exposures during the fetal and neonatal periods (Benjamin et al., 1975, 1978; Gillette, 1990). Analogous to human diagnostic imaging systems, there is therefore an opportunity to develop reporting databases, especially for CT imaging, and practice learning and improvement programmes for such situations.
4.3. Therapeutic procedures
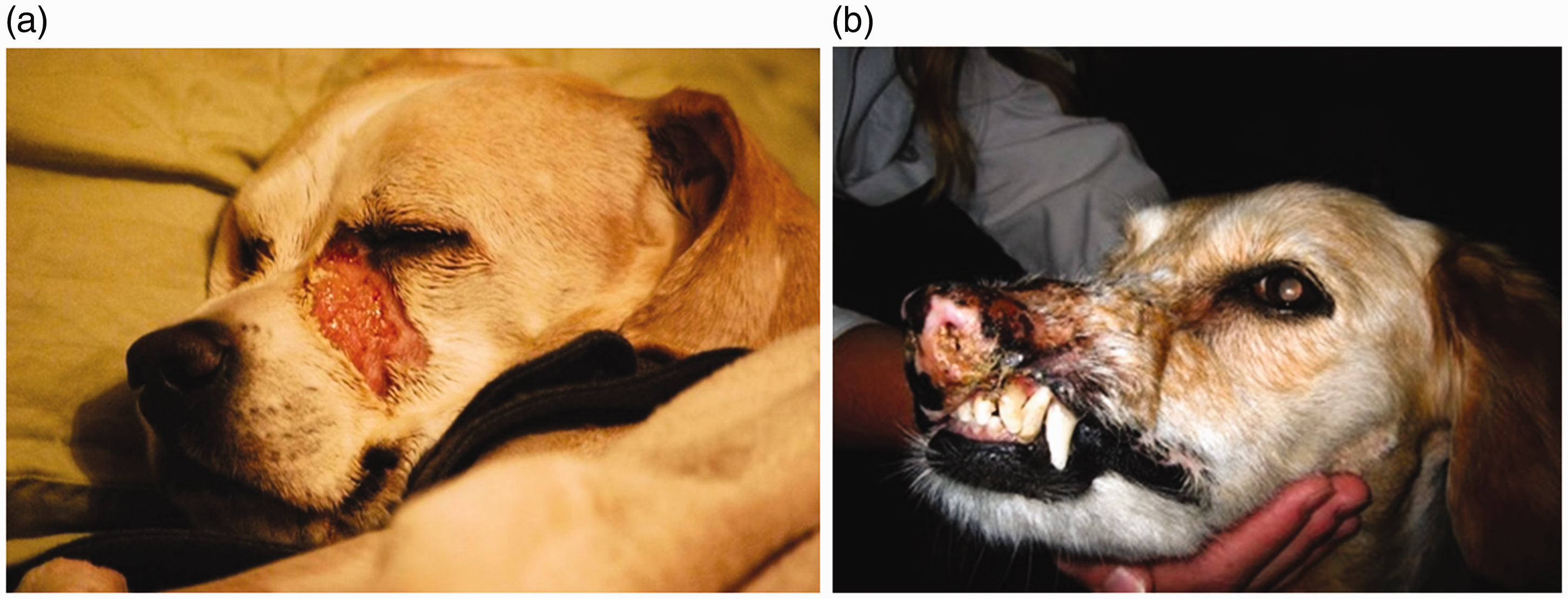
Veterinary radiation oncology is relatively new compared with that for humans (McEntee, 2006). However, linear accelerators are now used routinely to provide therapeutic treatment, although some use is still made of brachytherapy (Fig. 3), proton therapy, and carbon ion therapy in some centres. Doses delivered can be up to 70 Gy (to dogs) (Coomer et al., 2009), and there is already some concern about the knowledge upon which such treatment is based. There are not many published scientific reviews of the damage incurred to healthy tissues, and very few of the consequences of errors in therapeutic treatment, although examples are not difficult to find (Fig. 4a,b). In one example, Arkans et al. (2015) reported a specific case of misadministration of radiation therapy to a dog, where mistakes led to application of the wrong treatment plan, notwithstanding the use of a ‘record and verify’ system. Late effects (Fig. 5) are also known but not well recorded, although a review of acute and chronic effects published over 20 years ago stated that severe reactions occurred in less than 5% of treated animals (Harris et al., 1997).
Brachytherapy of a horse being treated for sarcoid (source: J. Benoit). (a) Radiation treatment burns 1 week after tomotherapy for nasal carcinoma (source: T. Loughlin). (b) Fibrosis in a dog 3 years after hypofractionated radiotherapy for mast cell tumour of the lip (source: J. Benoit). Osteosarcoma in a dog 5 years after treatment for mast cell tumour (source: J. Benoit).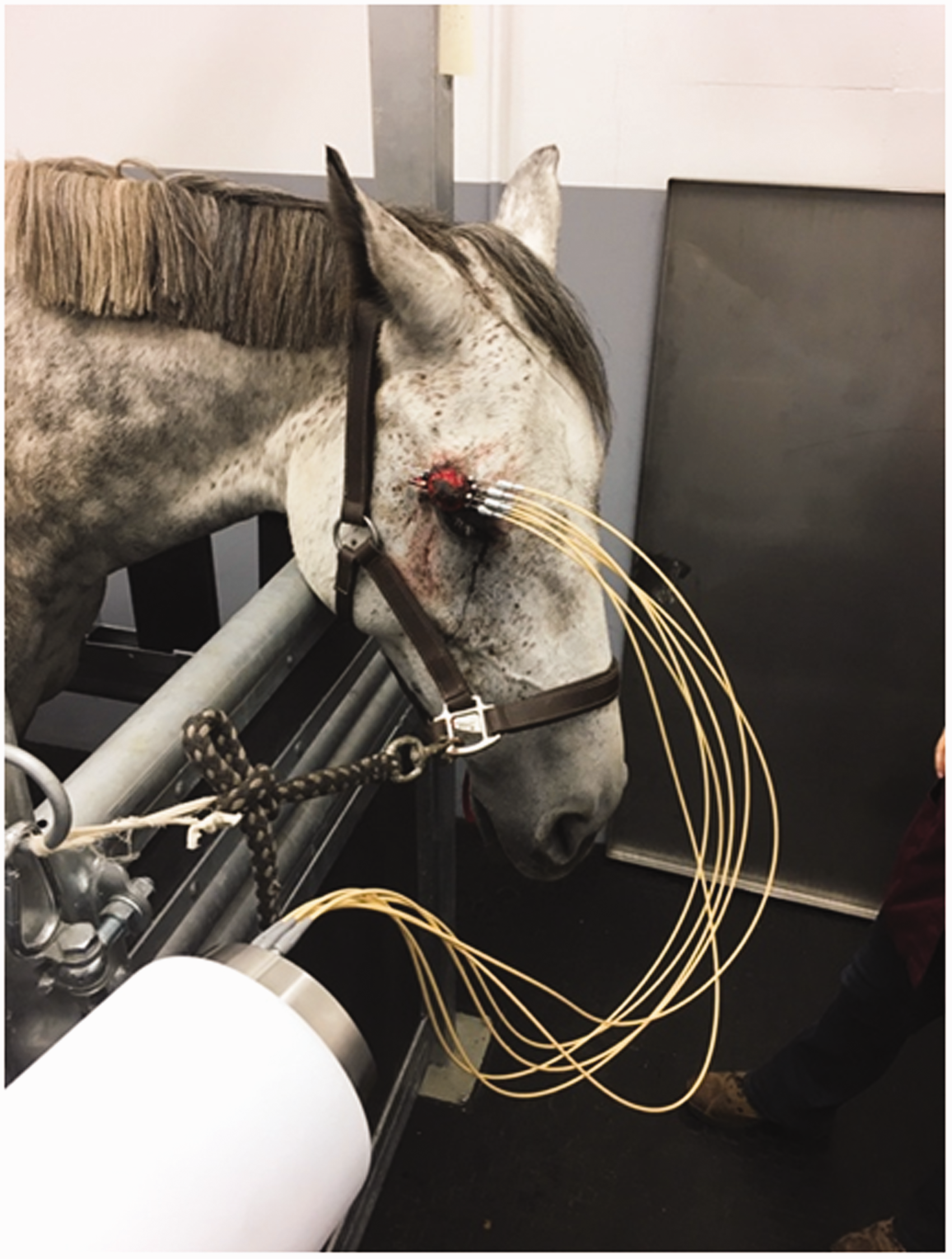

Considering the subject as a whole, in another review of practices in the USA, Keyerleber et al. (2012) looked at the completeness of reporting (in published studies) of treatment planning, radiation dose, treatment delivery, quality assurance, and adjunctive therapies. They found that in the vast majority of published manuscripts, the information provided was lacking or insufficient to allow complete interpretation of the results, or the reproduction of how treatments were planned or delivered. None of the studies provided a level of completeness consistent with the ICRU guidelines (ICRU, 2010), and only 24% reported more than 50% of the items evaluated. (ICRU emphasises the importance of standardisation in reporting for optimal interpretation of clinical results and for repeatability of treatments.) It was therefore concluded that there was a clear need for the adoption of standards for the reporting of clinical studies, as well as for the reporting of details of radiotherapy planning and delivery, and that such developments were essential for the progress of this area of veterinary practice.
A serious concern was that of inconsistencies in the definition of target volumes during the treatment planning process. This is particularly true for ‘conformal’ radiotherapy, where the expected therapeutic benefit, as well as the increased risk of missing part of the cancer cell population, is heavily dependent on tumour delineation. The accurate reporting of margins around a target is obviously necessary for any useful exchange of information between centres, and to ensure repeatability of results. Thus, Christensen et al. (2016) have shown that, even within a single institution, the routine evaluation of contouring nasal tumours, which should be reasonably straightforward, resulted in variabilities of gross tumour volume, clinical target volume, and planning target volume that constituted a significant barrier to the accurate reporting of the results of radiation therapy.
As in human radiotherapy, fractionation has been a mainstay in veterinary practice, but protocols differ considerably, even for the curative intent of the same condition; for example, two, three, or four fractionation protocols for osteosarcoma in dogs (Coomer et al., 2009). However, with the advent of intensity-modulated radiation therapy and stereotactic techniques, there has been a shift towards hypofractionation, although it is considered that more clinical experience is needed, and that biological models to test different fractionation schemes for both tumour control probability and normal tissue complication probabilities are necessary to determine, at least theoretically, the feasibility of such protocols. Thus, for example, Rohrer Bley et al. (2017) modelled two protocols using different fractionation schemes for brain tumours in dogs, and determined that they could safely increase the dose per fraction and decrease the number of fractions without incurring a large risk of late complications for selected brain tumours. In general, therefore, there are many areas of interest, such as the uncertainties over the reconstruction of dose and how this relates to the risks of late effects in different types of animals, which are essentially similar to those arising from the treatment of human patients (Vu Bezin et al., 2017).
Clinical trials are also imperative to progress veterinary radiation oncology, but there appears to be an over-reliance on retrospective studies (considered to be a poor basis for evidence) to assess clinical outcomes. One important limitation is the issue of incomplete or missing data. A recent review (Kent et al., 2018) referred to various studies relating to intracranial tumours in dogs, and concluded that prospective clinical trials are needed to answer lingering questions about efficacy outcomes, such as survival. Case selection to identify patients best suited for different procedures is also seen as an area requiring more attention with regard to the adoption of newer approaches (Kubicek et al., 2016).
Arkans et al. (2015) discussed the common issue of the risk of potential sources of error arising, and thus of potential harm to the patient, simply because of the increasing complexity of the treatments that may now be used. Useful comparisons were drawn between the roles of medical personnel in human and veterinarian radiation oncology (at least in the USA) and of quality assurance issues, even in the presence of ‘record and verify’ systems. Other matters arising were those relating to the certification of radiation therapists with respect to veterinary medicine, licensing, error reporting (or the lack of error reporting), the need for more guidelines to be drawn up, and so on. There has also been an increase in the use of radiation for palliative care, particularly for cats and dogs, but there appears to be a lack of agreed protocols with respect to such use, such as for nasal tumours in dogs (Tan-Coleman et al., 2013), in order to do so.
5. PROVISION OF RADIOLOGICAL PROTECTION ADVICE IN VETERINARY MEDICINE AND ITS IMPLICATIONS FOR THE DISCIPLINE OF RADIOLOGICAL PROTECTION AS A WHOLE
It is evident from these and other reviews that, as well as scope, there is a clear necessity for the provision of guidance specifically relating to the protection of the individual animal as the patient in veterinary medicine. This applies across all of the modalities being used and, although many of them are only currently available in a limited number of treatment centres, their availability is expected to increase rapidly in the near future. The necessary guidance needs to cover all of the issues identified above, including diagnostic and therapeutic imaging protocols, treatment planning and delivery, education and ongoing training [e.g. by drawing upon Publication 113 (ICRP, 2009)], and quality assurance. There is also scope for mutually beneficial biomedical research opportunities that include biological models, animal dose, and the dose quantities used, and all against a deeper understanding of the ethics of radiological protection in a veterinary context, which has yet to be developed.
Given time, there is also much more that could be done by the radiological community to improve the current situation. There are large databases relating to dogs, in particular (NCRP, 2004), that have been obtained in order to inform radiological protection of humans, and these could now be used to provide better guidance in veterinary medicine for thousands of dogs themselves, although it might take a determined effort to consider such databases in this way. Although guidance specifically for protection of the animal as the patient is needed, it would appear opportune that the radiological protection community and the veterinary imaging communities in particular are ready to collaborate and learn from each other. Adding specific advice on the protection of the patient to that of advice with regard to the veterinarians and their assistants would provide a more valuable holistic approach to the profession as a whole. As NCRP Report 148 (NCRP, 2004) noted: ‘To the extent that the animal patient exposure is reduced, there is usually a proportionate decrease in the exposure to personnel’. This argument also applies to human medical radiation protection, and is often cited (ICRP, 2013, 2017).
6. CONCLUSIONS, OUTCOME, AND NEXT STEPS
The Main Commission of ICRP accepted the findings of TG107, and has now created a new task group (TG110) to take these matters forward. In doing so, it is important to recognise that the provision of advice by ICRP has evolved continually over its 90-year history. Initially, it was aimed at the use of radiation in medicine, but it then expanded to include protection of those who were occupationally exposed, and protection of the general public who were exposed to man-made sources including the testing of nuclear weapons, discharges from the nuclear industries, accidental releases, and from natural (but variable) radiation sources. It then evolved from the aim of protecting people and
Many of the principles and guidelines needed for protection of the animal as the patient are, however, not dissimilar from those set out in Publication 121 (ICRP, 2013), which provides guidance in paediatric diagnostic and interventional radiology. Consideration of the lack of patient cooperation, wide ranges in size and disease conditions, and the need to provide guidance for patient comforters and holders are all similar to paediatric medical care. A more suitable starting point would be the production of an over-arching document as a parallel to that of Publication 105 (ICRP, 2007b), which considers all of the issues with respect to radiological protection in medicine for humans. In accepting the contents of the report by TG107, TG110 will provide such a document that will consider veterinary medicine as a whole, veterinarians, staff, their patients, and the public, whilst acknowledging that additional work will be needed in the future.