
Abstract
Widespread narratives frame mental illness as a sign of inherent personal weakness—an alleged weakness that would permanently undermine people’s ability to pursue goals in life. Do these narratives have self-fulfilling consequences? To test this hypothesis, and to attain a practical way to support people in realizing their strengths, we developed a brief (~20 min), highly scalable exercise that highlights the strengths people show when contending with depression. Three experiments (Ntotal = 748) show that this depression-reframing-exercise enhanced the confidence of people who had experienced depression to pursue their goals in life, 0.30≤ ds ≤0.68 (Ns = 158, 419, and 171); and, over 2 weeks, the progress they reported making towards a valued personal goal by 49% (from 43% reported completion to 64%), d = 0.47 (Experiment 3). While default inherent-weakness-narratives harm goal pursuit among people with depression, efforts to reframe depression can help people with depression recognize and access their strengths.
Introduction
Worldwide, roughly 1 in 10 people—800 million of the world’s population—will experience at least one depressive episode in their lives (Lim et al., 2018). These experiences are associated with a decreased chance to successfully pursue goals such as a career, hobbies, or important relationships (e.g., Dooley et al., 2000). Why?
Some decrements in goal pursuit are rooted in the experience of depression itself. Indeed, some of the defining symptoms of depression, such as decreased interest and activity, make it more difficult to pursue goals. Such goal pursuit impairments stem from a range of interconnected factors, including early childhood experiences and chemical imbalances (Beck & Alford, 2009).
Here, we investigate an additional socio-cultural barrier to goal pursuit: a simplistic and stigmatizing narrative that portrays depression as a sign of the person’s inherent personal weakness, not the consequence of an illness that is usually temporary. The insidious implication is that struggles with goal pursuit in the context of depression render one a “weak person.” We theorize that this narrative can impede goal pursuit, whether a person is currently experiencing depression or not.
To test the effect of the inherent-weakness-narrative, we counter it, applying social-psychological field-experimental methods to a clinical population. Specifically, extending recent advances in techniques to help people reclaim agentic representations of themselves from stigmatizing social-identity-based narratives (Bauer & Walton, 2023; Bauer et al., 2021; Hernandez et al., 2021), we develop an intervention that reframes the implications of an experience with depression as a sign of personal strength rather than inherent weakness (see Figure 1). We test the effect of this depression-reframing-intervention on goal pursuit in three randomized-controlled experiments, one a longitudinal intervention-experiment that tracks goal progress among individuals who have experienced depression over 2 weeks.
The depression-reframing approach: Reframing the implications of depression experiences.
Depression and Goal Pursuit: The Importance of Self-efficacy
Past research linking depression to decrements in goal pursuit implicates people’s general self-efficacy—the broad belief that one can succeed at achieving one’s goals. Self-efficacy is associated with greater goal commitment and successful goal pursuit in many populations and contexts, including school performance, health-related behaviors, and relationships (Fiori et al., 2006; Strachan & Brawley, 2009). Yet individuals with depression have repeatedly been shown to exhibit lower self-efficacy (Fiori et al., 2006). Prior research understands such decrements as arising only from depression as a mental disease, including the cognitive and affective biases associated with depression. Here, we test the impact of strength representations: We theorized that societal narratives that frame people with depression as inherently weak contribute to decrements in self-efficacy too, and test this hypothesis through an intervention that counters these narratives.
Inherent-Weakness-Narratives
Inherent-weakness-narratives portray entire groups of people as weak, casting all individuals with a certain characteristic (e.g., all people who have experienced depression) as lacking strength and agency in general (Cuddy et al., 2008). Such narratives can be applied to many groups in adverse circumstances; people who live in poverty, homeless people, or refugees are all sometimes portrayed as “passive,” “needy,” or “weaklings.”
Prior research illustrates the inherent-weakness narrative for people with depression. One analysis of social media posts documented a common narrative that framed depression as a “sign of personal weakness,” as illustrated by examples like this: “A woman with a strong heart will never suffer from depression!” (Li et al., 2018). This research has tended to examine inherent-weakness-narratives as one of several stigmatizing narratives (e.g., another is that depression is not a real illness), which are often collectively described as “mental health stigma” (Corrigan et al., 2016). In the present research, we focus specifically on countering the inherent-weakness-narrative. One contribution of the present work is to deepen our understanding of this particular narrative and its causal effects on goal pursuit.
In our theorizing, the inherence in the inherent-weakness-narrative implies that weakness is deeply rooted inside people who have experienced depression and permanent or hard to change. This inherence reflects the stickiness of mental illness stereotypes: the allegation is that a person who has experienced depression is a “weak person.” As such, inherent-weakness-narratives may apply to people with past experiences of depression, regardless of their current symptomology. Thus, we test the effect of our intervention countering weakness-narratives among people with prior experiences of depression broadly. Exploratory analyses examine the generalizability of effects across people with varying levels of current depression severity.
Consequences of Inherent-Weakness-Narratives
Past research shows that inherent-weakness-narratives regarding various social-identity groups can have self-fulfilling consequences, undermining goal pursuit by reducing individuals’ confidence in their ability to effectively pursue their goals (Bauer et al., 2021, 2025; Hernandez et al., 2021). One experiment manipulated inherent-weakness-narratives among low-income people receiving financial assistance in Kenya (Thomas et al., 2020). Small cash transfers were accompanied by a randomly assigned description of the aid program. One description framed recipients as passive and helpless, receiving aid to compensate for challenges (inherent-weakness-narrative), a common representation of aid programs. Others framed recipients as strong and agentic, using aid to pursue their goals (inherent-strength narratives). When aid recipients were exposed to the weakness (vs. strength) narrative, this undermined their confidence in their abilities, anticipated social mobility, and choice to learn business skills of value in the local economy.
Research exploring narratives that characterize people with depression as weak is limited mostly to correlational data, showing that people who contend with depression sometimes view themselves as weak and incapable. In turn, such self-views predict lower self-efficacy and worse mental health outcomes (Corrigan et al., 2016). Extending this research, we aim to manipulate and hence test the causal effect of narratives about the agency of individuals with depression experiences.
Countering Inherent-Weakness-Narratives Through Wise Interventions
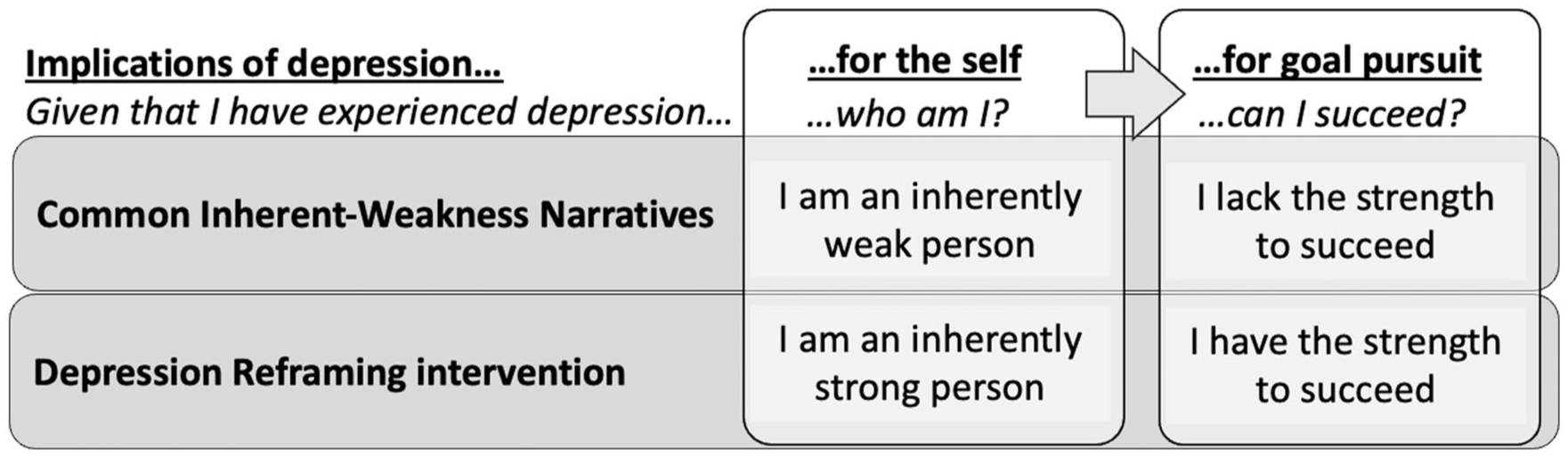
The depression-reframing-intervention represents the strength of people with depression as not in spite of but because of their experience with depression. It offers the idea that, in contending with symptoms of depression such as fatigue and reductions in motivation, people often show and develop important strengths, such as perseverance and the ability to deal with negative emotions. It then invites participants to consider how they have and can use these strengths to pursue goals in their lives. It thus reframes the implications of depression for the inherent qualities of the self and, connectedly, for one’s ability to pursue goals in the future (see Figure 1): experiences of depression are presented as a sign and a source of underlying strengths, not weaknesses, and hence as compatible, not incompatible, with successful goal pursuit.
In doing so, depression-reframing extends research on life stories as a central predictor of individuals’ behavior (McAdams, 1995, 2001): This research suggests that people commonly use life stories to integrate their past (e.g., experiences with depression), present (e.g., who am I now? what are my qualities?), and future (e.g., will I be able to succeed?) into a coherent story of their self across time (see Figure 1). In the present research, we test how depression-related strength-representations can shape key aspects of individuals’ life stories—including their perception of who they are based on their depression experience, and how likely they can succeed in the future—and subsequent goal pursuit.
In developing the depression-reframing-intervention, we were informed by field-experimental research on psychologically “wise” interventions broadly (Walton, 2014; Walton & Crum, 2020). This research provides intervention design processes (e.g., using interviews or focus groups; Bauer & Walton, 2023; Walton & Crum, 2020) to construct relatively brief (~10–40 min) exercises that target key meaning-making processes (here: who am I, given that I have experienced depression?). Exercises often use a common grammar, including (a) short parable-like stories from people in similar positions that illustrate the key intervention message (here: that people with depression have important strengths); and (b) “saying-is-believing” exercises that give people an opportunity to think through this way of thinking for themselves, including how it may apply to their own life, typically in an asset-based, honorific form (e.g., as advice for others; see Study 1 Methods).
The present work builds most specifically on prior identity-reframing-interventions: exercises used to invert inherent-weakness-narratives about marginalized student groups, including students with low socioeconomic status, racial-ethnic minority, or refugee backgrounds (Bauer & Walton, 2023; Bauer et al., 2021, 2025; see also Hernandez et al., 2021). Identity-reframing-interventions re-frame what it means to be a student with a marginalized identity: as strong, and capable of succeeding in a challenging academic setting, as evidenced by the strengths a person has shown and developed in contending with social-identity-based challenges. One randomized-controlled field-experiment implemented a refugee-identity-reframing-exercise in the onboarding-process at an online-university in Europe, reaching 533 refugee students. Refugees read stories from other refugee students and reflected on how their own experience as a refugee has been a source of strength for them, and how they have and can apply these strengths to schooling. This increased students’ engagement in the university’s learning environment over the next year (Bauer & Walton, 2023).
Contributions
The present research makes three main contributions.
First, it extends prior research on identity-reframing interventions, which has focused on marginalized demographic identities and academic goals (e.g., highlighting how the strengths refugees have shown can help them succeed at university). Here, we develop an intervention that reframes the experience of a mental illness (rather than a demographic identity) with regard to goal pursuit broadly (not just academic goals) and test its effects among people who have experienced depression and the broad array of personal goals they pursue in their adult lives.
Second, this research contributes to an understanding of psychological process, namely, in how stigma affects people contending with depression, by testing the specific causal effect of default depression-as-inherent-weakness-narratives on goal pursuit. This contribution extends prior clinical programs aimed at reducing mental health stigma (Mittal et al., 2012; Yanos et al., 2015). Such multi-week programs are usually implemented in a manner akin to group therapy. They involve repeated group sessions directed by a therapist/counselor to address stigma through multiple elements, including psycho-education (educating people about mental illness and stigma) and cognitive restructuring (helping people become aware of and then change stigmatizing thoughts). Results imply reductions in the endorsement of stigmatizing narratives and improvement in affective measures (e.g., reported hope). However, these studies are limited in that (a) they address mental health stigma broadly, limiting conclusions about the role of specific narratives; (b) they involve a bouquet of intervention elements that may contribute to benefits (e.g., a supportive group setting and a therapist/counselor). Our social-psychological methods allow us to assess the causal relationship between the strength versus weakness narrative on goal pursuit. Moreover, while prior research has focused on affective outcomes, we test effects on pursuit of personally important goals.
A third contribution is methodological. Traditionally, trials conducted with clinically relevant populations (e.g., trials testing mental health stigma programs) are broad, and resource-intensive, and therefore often have small sample-sizes (Ns < 100), lack active control conditions, and/or show relatively high dropout rates (Mittal et al., 2012). By contrast, extending advances in wise interventions, we show how researchers can use rapid, low-cost experimental methods to test important causal processes in clinical populations. Here we test the effect of depression-reframing among 748 people who have experienced depression in a series of three studies, each with an active control condition, one a longitudinal study with minimal dropout (<3%), at relatively low cost. These methods are valuable both for application, developing scalable solutions to a common problem, and enhancing the validity and accelerating the pace of science.
Present Research
We develop and test the depression-reframing-exercise in three experiments (Ntotal = 748 individuals who had experienced depression). Experiments 1 and 2 assess immediate effects on key processes in goal pursuit: whether the depression-reframing-exercise boosts individuals’ confidence to pursue their life goals and their commitment to these goals. In addition, Experiment 2 investigates a potential mechanism of intervention effects: the degree to which people perceived having experienced depression as being compatible or incompatible with successful goal pursuit. Finally, Experiment 3, a pre-registered longitudinal randomized-controlled experiment, tracks people’s success in pursuing a valued personal goal over 2 weeks, and tests whether the depression-reframing-exercise enhances this progress.
As outlined, we explore depression-reframing-effects among people who have experienced depression, regardless of their current symptoms; exploratory moderation analyses assess how well our effects generalize across individuals with varying experiences of current depression severity.
Transparency
Experiments 2 and 3 were pre-registered at https://aspredicted.org/RSG_DSC and https://aspredicted.org/BV4_DL3, respectively. All data, material, and code are accessible at https://osf.io/f9xrb/?view_only=0a8970be59ee45059bd9ad7b1500a9af. We report how we determined our sample size, all data exclusions, all manipulations, and all measures.
Experiment 1: Effect of Depression-Reframing on General Self-Efficacy to Achieve Life Goals
In Experiment 1, we developed the depression-reframing-exercise, examined how participants used this exercise to describe strengths they had shown in contending with depression, and tested causal effects on self-efficacy to pursue goals in general.
We designed our control condition so as to test the depression-reframing-intervention against baseline ways of thinking about depression, without framing depression in terms of strengths or weaknesses. Thus, control participants read factual information about depression obtained from the American Psychiatric Association (e.g., descriptions of depression definitions and treatment options in line with the DSM-5) and then openly reflected on their experiences with depression.
Method
Depression-Reframing-Exercise
Intervention Development
We developed the depression-reframing-exercise in a multi-step-process following established guidelines (Bauer & Walton, 2023). This process centered the experiences of people living with depression and the narratives of strength and agency they told. To characterize the specific challenges and strengths of people with depression experience, we reviewed the scientific literature, interviewed a psychotherapist trained in cognitive-behavioral therapy, and conducted a pilot study with participants who have experienced depression (N = 206), which led to further refinements of the materials (see Supplement).
Key Nuances
Three key nuances informed our design.
First, the exercise highlights the strengths that individuals have shown specifically in contending with negative experiences that come from depression. Hence, the materials do not downplay the very real negative experiences of depression, which could backfire. Instead, they recognize negative experiences, but reframe their implications: as implying personal strength rather than inherent weakness.
Second, in highlighting strengths, the materials do not deny or downplay possible weaknesses people may also have, which could also backfire (e.g., preventing people from addressing weaknesses). Overall, the intervention aimed to elevate representations of strengths, so people can see themselves as inherently strong even if they also have possible weaknesses—that is, even if they have specific weaknesses, they are not inherently weak people.
Third, the exercise was not presented as an effort to help participants, but as an opportunity to help others, following many “wise” social-psychological interventions (Walton & Crum, 2020). This approach reinforces the focus on empowerment and increases engagement and impact (Yeager et al., 2016).
Structure and Content
The exercise consists of three parts. First, the exercise was presented as sharing the results of previous research (e.g., Devendorf et al., 2022) finding “that many individuals . . . said that they have learned important things from their experiences dealing with depression [that helped] them pursue goals that are important to them in life.”
Second, this central idea was illustrated in three parable-like stories from people contending with depression. One story read:
“[My depression] has been extremely difficult. . . At the same time, [it] has also taught me some important things. . .I’ve learned to better deal with negative thoughts and feelings. When my wife died, I thought this was the end of the world – I just didn’t want to live without her. . .But I realized that life does go on and I should make the most of it – also for my wife who always tried to make everyone happy. . .Dealing with depression is a long journey, and surely not an easy one; but. . .it’s been making me stronger and better able to deal with other challenges.”
Last, we invited participants to reflect (a) on what “you [have] learned through your experiences as someone dealing with depression” and (b) “how these learning experiences help you successfully pursue your personal goals in life (i.e., any things that are important to you).” This reflection allows participants to apply the message to their own experience.
The exercise took 15 to 20 min to complete (total study-completion time: M = 19.28, SD = 10.56).
Active Control
Our control condition referenced depression but did not imply strengths or weaknesses. It used a similar format to the intervention (reading material, written reflection) and was also presented as an opportunity to help others. The material presented general information about depression and asked participants, “how [would] you describe your experiences dealing with depressive symptoms?”
Participants
Recruitment Procedure
To reach people who had experienced depression, we used Prolific, taking advantage of a screening question Prolific had posed: whether users had ever taken anti-depressants. We made our study available only to people who had reported to Prolific that they were fluent in English and that they had taken anti-depressants, indicating that a medical professional had judged their mental health symptoms as severe enough to warrant a prescription. As anti-depressants are sometimes prescribed for mental health conditions other than depression, we also excluded people who, in our survey, reported that they had never experienced depression (see below).
Sample
With a target of 80% statistical power and an estimated d = 0.40 (Bauer et al., 2021), we aimed to recruit 156 participants. Overall, 159 people completed our materials (three participants failed to flag their study-completion, making Prolific recruit three more). We excluded one person who reported that they may not have experienced depression (indicating “not at all agree” that they were someone “who has had to deal with depression”; in Experiments 2–3, we improved the clarity of this item). The final sample size was thus 158 (Mage = 32.01, SD = 10.97). Most participants (70%) reported living in the United Kingdom; the rest in other, mostly Western countries (see Table S1). Most were White (89% were, 4% Asian, 3% mixed, 1% Black, 2% Other, 1% missing data) and female (83%; 16% were men and 1% self-identified as other; in Experiments 2–3, we use a sampling-strategy allowing for gender balance).
Participants’ Experience of Depression
Table 1 summarizes participants’ experience of depression across studies. As can be seen, at the time of participation, most participants still took anti-depressants. Additionally, as reported in the Supplement, most said they still dealt with depression at least “a little” (across experiments, 90–97% did). Further, as Table 1 shows, participants’ symptoms varied, with similar proportions reporting minimal, mild, moderate, and heavy symptoms.
Participants’ anti-depressant use, depression severity, and psychotherapy participation.
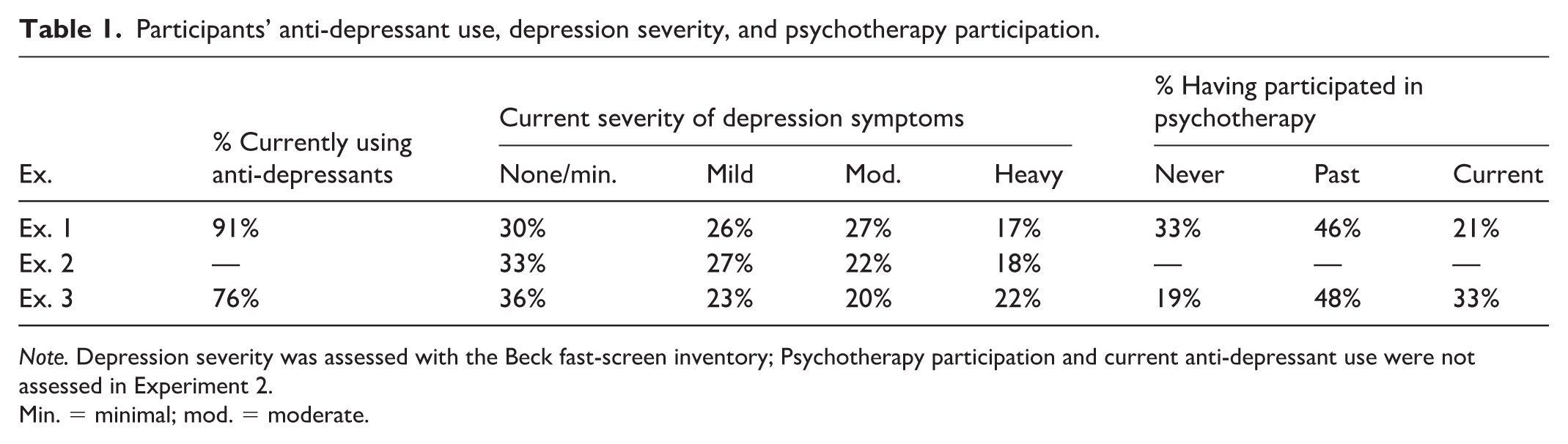
Note. Depression severity was assessed with the Beck fast-screen inventory; Psychotherapy participation and current anti-depressant use were not assessed in Experiment 2.
Min. = minimal; mod. = moderate.
Across experiments, experimental conditions did not vary in any of these baseline factors, all ps > .10, confirming the success of randomization.
Procedure and Measures
Participants were randomized to complete the depression-reframing or active control materials, followed by outcomes and demographics.
Primary Outcome: General Self-Efficacy
We assessed general self-efficacy with a widely-used eight-item-scale from Chen et al. (2001; e.g., “I will be able to achieve most of the goals that I have set for myself.”; 1 = strongly disagree, 6 = strongly agree, α =.92). This scale predicts both individuals’ task-specific self-efficacy (e.g., students’ academic self-efficacy) and goal attainment (e.g., grades) across a variety of domains (Chen et al., 2001).
Depression Severity
We used the 7-item Beck depression inventory fast-screen (α = .86; Beck et al., 2000). Each item lets participants rate their current thoughts and feelings (e.g., feelings of hopelessness) on a scale from 0 to 3 (e.g., 0 = I am not particularly discouraged about the future, 3 = I feel the future is hopeless and that things cannot improve). Scores range from 0 to 21 (established cut-offs: 0–3 = no or minimal depression, 4–6 = mild; 7–9 = moderate, 10–21 = severe).
Results
How Did Participants Use the Depression-Reframing-Exercise? We analyzed the most common themes in participants’ descriptions of the strengths they had shown and developed using ChatGPT (Version 5). Past research finds that ChatGPT can efficiently extract core themes from open-ended data (Morgan, 2023). We instructed ChatGPT to “Summarize the major 3-5 themes in the following texts from participants reflecting on their experiences with depression. Do not let our prior conversations influence how you complete the task,” providing it with anonymized intervention responses. We then asked ChatGPT to code each participant response—using both intervention responses as well as control responses, for comparison—as to whether the response included each respective theme. To validate the results, we also had a research assistant manually code all themes. Inter-rater agreement levels (between ChatGPT and research assistant codings) were generally acceptable, 0.43 ≤ ICC ≤ 0.75 (see Table 2).
Top Themes in Participants’ Responses to the Depression-Reframing Material in Experiment 1.
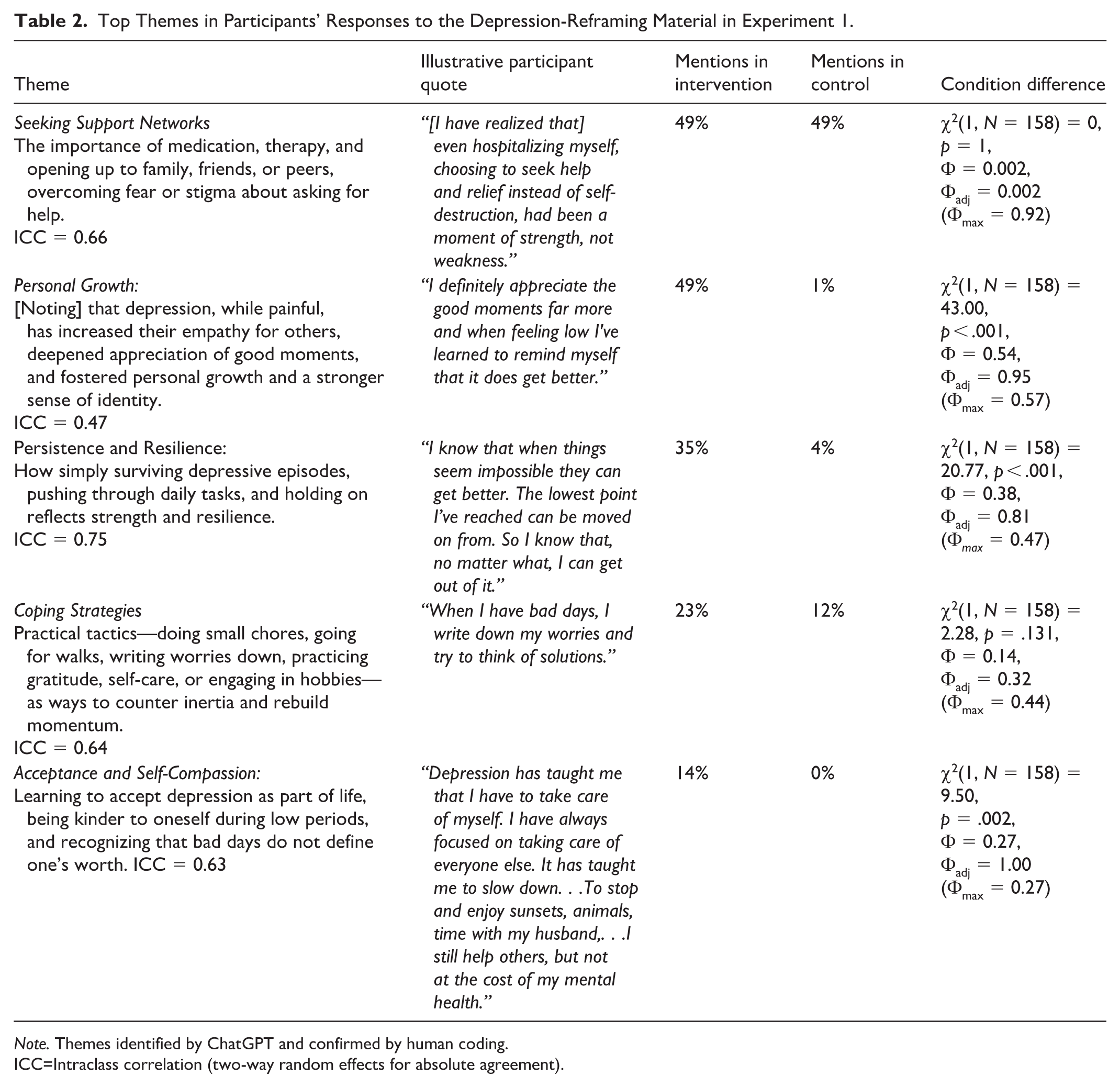
Note. Themes identified by ChatGPT and confirmed by human coding.
ICC=Intraclass correlation (two-way random effects for absolute agreement).
Table 2 shows the themes ChatGPT identified and illustrative participant responses. The results show that participants used the depression-reframing-exercise to articulate a strong and agentic representation of themselves, including in contending with depression. While participants in both conditions commonly referenced seeking support, participants in the depression-reframing condition were more likely to report (a) how they have shown “personal growth” (b) how “simply surviving depression reflects . . .strength” and (c) how they have learned to be self-compassionate, including “being kinder to oneself, . . . and recognizing that bad days do not define one’s worth.” There was also a descriptive tendency for intervention participants to reference developing coping skills more, but this difference was nonsignificant.
Overall, people in the depression-reframing condition articulated personal strengths they have shown, including in situations that are commonly seen as signs of inherent weakness, such as when people are simply “surviving depression,” or asking for help.
Depression-Reframing-Effects
The primary causal question was whether the depression-reframing-exercise increased participants’ self-efficacy to successfully pursue goals meaningful to them. It did. Participants expressed more confidence in their ability to pursue goals in their lives in the depression-reframing condition (M = 4.14; SD = 0.82) than in the control (M = 3.81; SD = 0.92), F(1,156) = 5.52, p = .020, d = 0.37, 95% CI [0.06, 0.69].
In a follow-up analysis, we tested whether the severity of the depression people currently experienced moderated this effect. It did not, F(1,154) = 0.80, p = .373. To maximize power for these moderation analyses, we re-run analyses using all data from Experiment 1 to 3 (see Results of Experiment 3).
Discussion
In Experiment 1, participants who were offered the depression-reframing-exercise used this exercise to articulate strengths they had shown in experiencing depression. In turn, as compared to participants in an active control condition, they expressed more confidence in their ability to pursue goals successfully in their lives.
Experiment 2: Self-Efficacy to Accomplish and Commitment to a Specific Personal Goal
Experiment 2 had two main goals. First, we provide a pre-registered replication of the causal depression-reframing effect on general self-efficacy. Second, we test whether depression-reframing also enhances individuals’ self-efficacy for, and commitment to, a specific goal personally important to participants (also pre-registered).
We also had three secondary goals.
First, we explored whether the depression-reframing-intervention affected goal selection. In theory, goal-specific effects could be driven by differences in goal selection: the depression-reframing-exercise could lead people to choose goals they find easier or more motivating, rather than to enhance self-efficacy for and commitment to a given goal. To rule out goal selection effects, we randomized participants to identify a goal before versus after completing experimental materials. We predicted that the depression-reframing exercise would enhance individuals’ self-efficacy and commitment even when participants had already selected their goal. We hence pre-registered to explore intervention × order effects to investigate this theorizing (as “secondary analyses” in our pre-registration).
Second, we tested effects on additional measures of motivation—individuals’ intrinsic motivation for and sense of control over the goal (pre-registered as “secondary analyses”). Both are linked to self-efficacy and goal commitment (Fan & Williams, 2010; Ste-Marie et al., 2016) and, we reasoned, may also exhibit positive effects.
Third, in non-pre-registered exploratory analyses, we also examined a potential mechanism of the depression-reframing-exercise: the perceived compatibility between having experienced depression and having the qualities necessary to pursue goals successfully. We tested whether the depression-reframing exercise enhanced this perceived compatibility and whether this improvement would statistically mediate gains in self-efficacy and goal commitment.
Method
Participants
To test a main effect with a target of 80% statistical power and an estimated d = 0.40 (Experiment 1) requires a sample of at least 156 participants. However, we also sought sufficient power to detect any order effects. Based on Monte Carlo simulations with a target of 80% power for an estimated condition × order interaction effect of η2 = .01 (see details in code on OSF), we pre-registered to recruit 440 participants. Overall, 442 participants completed our materials (two participants failed to flag their study completion, making Prolific recruit two more). Following pre-registration, we excluded 23 participants who indicated that they may not have experienced depression (indicating “no” or “I’m unsure” to the question “Have you ever had a depression? [sic]”). The final sample size was thus 419 (210 female, 200 male, 8 other, 1 missing; Mage = 35.18, SD = 12.78). A preponderance of participants lived in the United Kingdom (46% did). Most were White (80%, 9% Black, 5% Asian, 4% LatinX, 2% other, 1% Middle Eastern).
Procedure
Our study had three parts: (a) experimental materials (depression-reframing vs. active control), (b) the selection of a personal goal, and (c) the outcome and process measures. The order of the first two parts was randomized.
Experimental materials were identical to those in Experiment 1. To assess goal-specific beliefs, we asked participants to identify a personal goal they wanted to “achieve in the next two weeks.” This goal, we said, “could be big or small—just something that is meaningful to you.”
Measures
Primary Motivational Measures
General self-efficacy was assessed as in Study 1 (α = .94).
In addition, we assessed self-efficacy for and commitment to the personal goal participants specified. Goal-specific efficacy was assessed with the item “How likely do you think it is that you will successfully complete this goal?” (1 = very unlikely, 6 = very likely; Hofmann et al., 2015). Commitment was assessed with a four-item scale (e.g., “I fully identify myself with that goal”; 1 = strongly disagree, 6 = strongly agree; α = .81; Brunstein et al., 1998). Both scales have been validated in previous research, and reliably predict the progress individuals make towards their goals (Brunstein et al., 1998; Hofmann et al., 2015).
Depression-Goal Pursuit Compatibility
To assess the degree to which participants saw experiencing depression as compatible with successful goal pursuit, we adapted an identity-compatibility scale (Debrosse et al., 2020). We asked participants to list four characteristics “you think [you should] ideally have to successfully achieve your goal.” The most frequently listed strengths were determination (mentioned by 30% of participants), motivation (17%), patience (16%), positivity (14%), and discipline (11%). The kinds of strengths listed did not differ by condition, all ps > .10. Then we asked participants to rate “how much each of those characteristics can generally be used to describe individuals who are dealing with a depression” (1 = not at all, 6 = extremely much; α = .89).
Secondary Motivational Measures: Intrinsic Motivation and Perceived Control
Intrinsic motivation was assessed with the item, “I pursue this goal because it gives me pleasure and enjoyment” (1 = strongly disagree; 6 = strongly agree; Brunstein et al., 1998). Perceived control was assessed with the item “How much do you feel in control over this goal?” (1 = not at all, 6 = extremely; Hofmann et al., 2015).
Results
Personal Goals
Two research assistants coded the kinds of personal goals individuals identified. We used a master-coder approach in which one research assistant’s codings were used for analyses, and the second for determining reliability. Inter-observer reliability was high (0.69 ≤ ICC ≤ 0.93). As shown in Table 3, the most frequently mentioned goals involved physical self-care, work/study, and life management. Notably few participants (1%) mentioned depression or mental health in their goal descriptions. The types of goals mentioned did not differ by condition, all ps > .10.
Categories of Personal Goals Participants Wanted to Accomplish Over The Next 2 Weeks (Experiments 2 and 3).
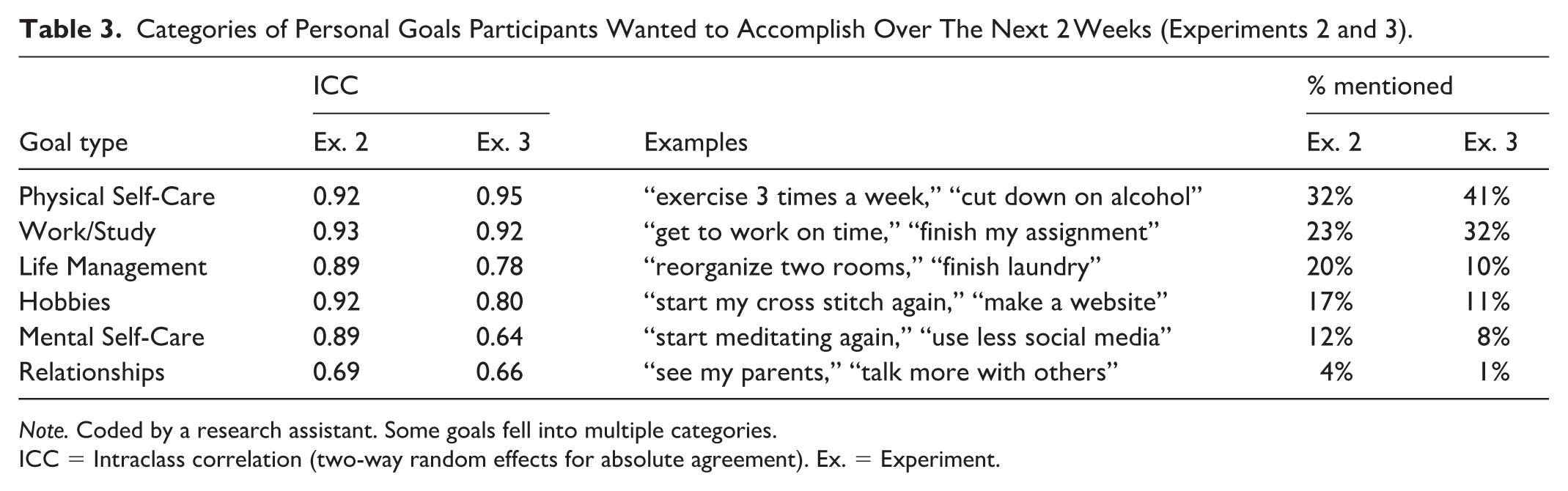
Note. Coded by a research assistant. Some goals fell into multiple categories.
ICC = Intraclass correlation (two-way random effects for absolute agreement). Ex. = Experiment.
Goal-Related Outcomes
Primary Motivational Measures: Self-efficacy and Goal Commitment
First, replicating Experiment 1, people were more confident in their ability to successfully pursue their goals in life in general in the depression-reframing condition (M = 4.17, SD =0.97) than in the control condition (M = 3.88, SD = 0.97), F(1,417) = 9.72, p = .002, d = 0.30, 95% CI [0.11, 0.50], see Figure 2.
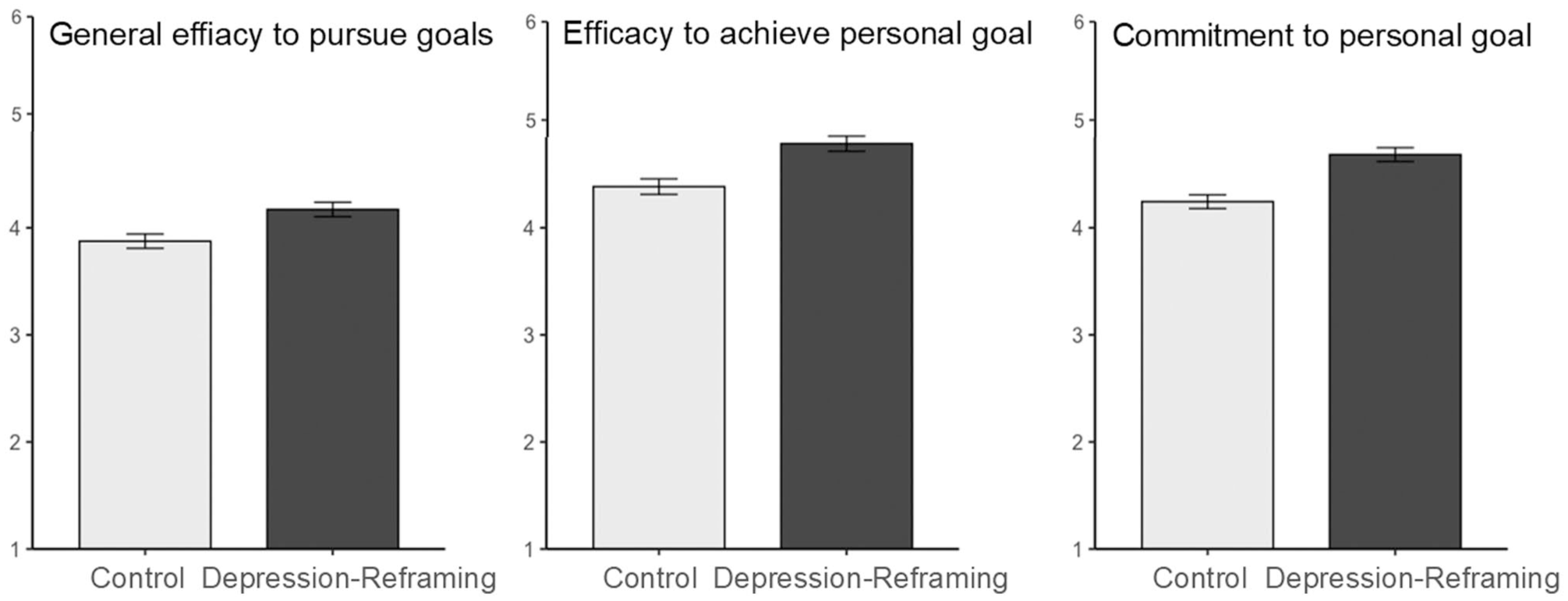
Participants’ general efficacy to pursue goals in life and their efficacy for and commitment to a specific personal goal (Experiment 2).
Second, this gain extended to a specific self-selected goal. People were more confident that they could complete their personal goal in the depression-reframing condition than in the control condition, F(1,417) = 15.60, p < .001, d = 0.39, 95% CI [0.19, 0.58], (M = 4.78, SD = 1.02 vs. M = 4.38, SD = 1.06). They were also more committed to this goal, F(1,417) = 23.40, p < .001, d = .47, [0.28, 0.67], (M = 4.68, SD = 0.93 vs. M = 4.24, SD = 0.93).
Secondary Pre-Registered Motivational Measures: Intrinsic Motivation and Perceived Control
These measures yielded similar gains. Participants in the depression-reframing (vs. control) condition reported that they pursued their goal more because they enjoyed it, F(1,417) = 14.49, p < .001, d = 0.37, 95% CI [0.18, 0.57], (M = 4.29, SD = 1.49 vs. M = 3.72, SD = 1.54), and that they felt more in control over their goal, F(1,417) = 7.72, p = .006, d = .27, [0.08, 0.46], (M = 4.36, SD = 1.14 vs. M = 4.05, SD = 1.16).
None of the five depression-reframing effects on the indices of goal pursuit varied with whether participants identified their goal before or after completing randomized exercise, all ps > .10. The gains thus reflect improvements in participants’ sense of efficacy and motivation toward a given goal, not a change in goal selection.
As in Experiment 1, the severity of current depressive symptoms did not moderate any effect, all ps > .10.
Perceived Compatibility of Depression With Successful Goal Pursuit
Last, we tested our theorizing about psychological process.
As predicted, the depression-reframing-exercise reduced the perceived incompatibility between the qualities of a person who has experienced depression and the strengths participants identified as necessary to successfully pursue their personal goal, F(1,415) = 20.47, p < .001, d = 0.44, 95% CI [0.25, 0.64], (M = 3.51, SD = 1.40 vs. M = 2.91, SD = 1.30). In the control condition, fully 71% of participants indicated that the strengths they thought necessary to pursue their goal (e.g., motivation, patience, positivity, and discipline, see section “Methods”) on average did not describe people dealing with depression well (scale response options: “not at all,” “very little,” or “rather little” vs. “rather much,” “very much,” or “totally”). The depression-reframing-exercise reduced this figure to 52%, χ2(1, N = 397) = 15.48, p < .001, OR = 2.28, [1.51, 3.45].
Mediation analyses are consistent with the hypothesis that this reduction in perceived incompatibility (using the linear measure to maximize statistical power) contributed to intervention effects on motivational outcomes. The indirect effect on general efficacy was: 95% CI [0.03, 0.14]; on goal-specific efficacy: [0.01, 0.11]; and on goal-specific commitment: [0.01, 0.12]. See Figure 3.
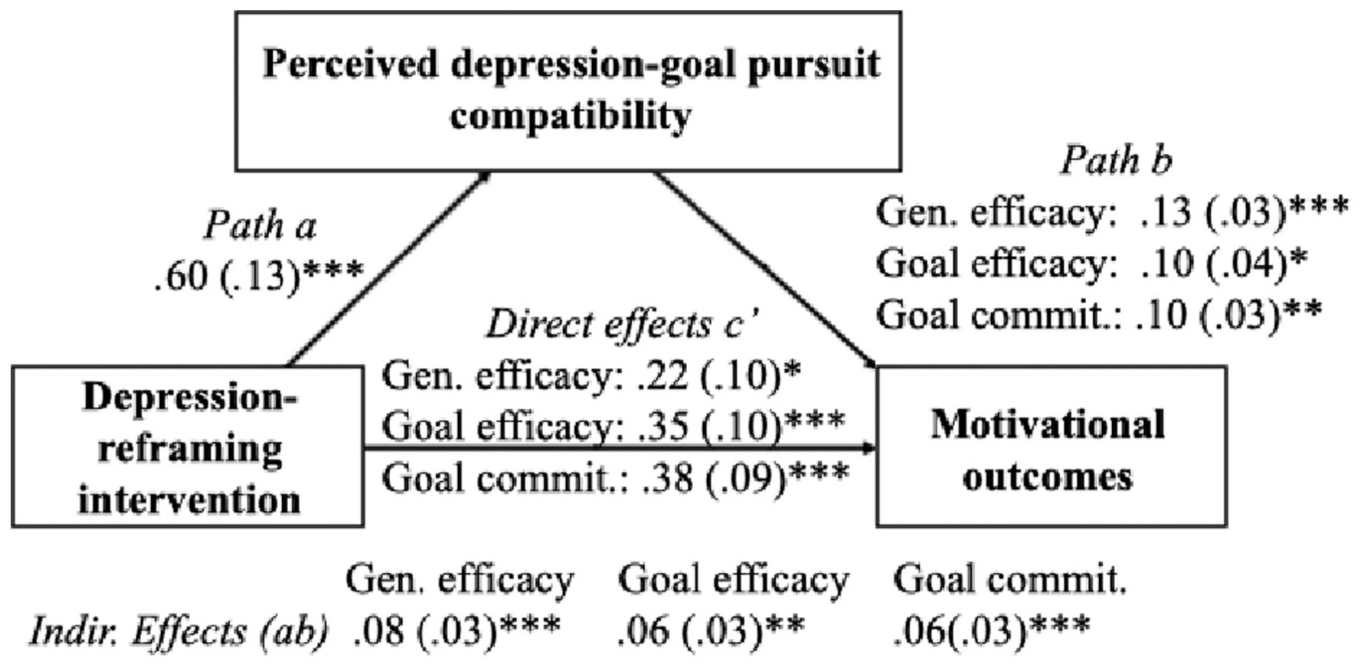
Perceived compatibility between depression and goal pursuit mediates gains in motivational outcomes (Experiment 2).
Discussion
Replicating Experiment 1, in Experiment 2 the depression-reframing-exercise again increased general self-efficacy among people who had experienced depression. It also enhanced their confidence in their ability to achieve, and their commitment to pursuing, a specific valued personal goal. The latter effects were not driven by change in the selection of personal goals. Instead, all three effects were mediated by a reduction in the degree to which people saw the experience of depression as incompatible with having the strengths needed to successfully pursue a valued goal.
Experiment 3: Successful Goal Pursuit Over 2 Weeks
We theorized that, even as worries like “Are people with depression weak?” can become self-confirming, targeted exercises that counter these worries might trigger cascades of self-reinforcing processes that improve goal pursuit over time. If people who have experienced depression see their experience as more compatible with pursuing goals successfully, and if they feel more confident and committed to their goals, they may make more progress, in turn reinforcing their confidence and motivation, and further increasing their progress. To test the potential of depression-reframing to support people who have experienced depression in making progress on their goals, we conducted a longitudinal randomized-controlled trial. As primary pre-registered outcomes, we assessed both whether the depression-reframing exercise boosted individuals’ general self-efficacy immediately and the amount of progress they reported having made toward a specific valued personal goal 2 weeks later.
Beyond our primary focus on goal pursuit, we also began to explore effects on functioning in the face of a relapse in non-preregistered analyses. First, if people view instances of depression at least in part as a sign of strength rather than weakness, they might anticipate being more compassionate with themselves in the event of a relapse. Second, they might also anticipate reaching out to others for support more. We examined these possibilities in exploratory analyses, with outcomes assessed immediately after the depression-reframing exercise.
We also pre-registered an additional measure. Since improvements in goal pursuit can improve well-being over time (Hofmann et al., 2015; Sheldon et al., 2010), we also examined effects on well-being. However, the measure we used assessed overall life satisfaction, which goes beyond well-being. While we report the results along this measure following our pre-registration, in retrospect, we suspect it is premature within the 2-week assessment frame.
Methods
Participants
With a target of 80% statistical power and an estimated effect size of d = 0.40 (Experiments 1 and 2), we aimed to retain 156 participants. Anticipating a 30% dropout rate, we pre-registered to recruit 230 individuals. A total of 232 people completed the first part of the study (two failed to flag their study completion, making Prolific recruit two more). Following pre-registration, we excluded participants who indicated that they may not have experienced depression. We asked participants specifically if they had experienced “depression in a clinical sense (i.e., a depressive disorder).” Sixty-one participants indicated “no” or “I’m unsure” to this question and were hence excluded.
The final sample size at T1 was thus 171 (86 female, 83 male, 2 other), mean age M = 32.58, SD = 10.81. Drop-out was low and balanced across conditions: Only five participants (three in the intervention group, two in the control group; less than 3% of participants) did not complete the 2-week follow-up survey (Nt2 = 166). Most participants were White (at T1: 82%; n = 140 White; n = 17 Black, n = 7 LatinX, n = 5 other, n = 1 Asian, n = 1 Middle Eastern).
Procedure
At T1, participants were randomized to complete the depression-reframing exercise or control materials. They then identified a valued personal goal and completed initial outcome variables. Two weeks later (T2), they completed longitudinal outcomes in a second online-survey.
Time 1 Outcome Measures
General Self-Efficacy
General self-efficacy was assessed as in Experiments 1 and 2, immediately after the randomized material.
Anticipated Self-Compassion in the Event of a Relapse
Next, we asked participants to imagine a relapse of depression: “Imagine you have not experienced depressive symptoms for several months, but then you experience quite severe depressive symptoms for five weeks in a row again—without any obvious reason.” We asked participants how they would respond to this situation, using two items adapted from a self-compassion scale (“I would be kind to myself,” “I would feel respect for myself”; 1 = totally disagree, 6 = totally agree; α = .71; Falconer et al., 2015).
Anticipated Support-Seeking in the Event of a Relapse
We assessed support seeking from (a) friends and family and (b) mental health professionals, again in the context of a relapse of depression, using two items from the General Help-Seeking Questionnaire (Wilson et al., 2005). We asked participants how likely they would be to reach out to “friends or family” and “a psychotherapist or other qualified professionals” (1 = extremely unlikely, 6 = extremely likely). These outcomes were only moderately correlated, r = .29, p < .001, so we examined them separately. It is possible that people are even more concerned about the consequences of being seen as weak by friends and family than a mental health professional; this would make a reframing-effect on the former especially plausible. If friends and family see oneself as weak, this could threaten relationship dynamics that are pillars of one’s daily life rather than therapeutic interactions that are narrow in scope and temporary by design. However, we explored effects on both outcomes.
Time 2 (2-Week) Outcome Measures
Goal Progress
As individuals identified a wide range of personal goals, we deferred to participants’ definition of goal progress. Accordingly, we used two validated self-report scales to assess goal progress. Both predict other measures of goal progress, including objective indices (Brunstein et al., 1998; Hofman et al., 2015).
First was a pre-registered descriptive scale (2-items; “I have made progress with regards to this goal” and “Many things have happened that made it difficult to realize the goal,” reverse-coded; 1 = strongly disagree, 6 = strongly agree; α = .47; Brunstein et al., 1998). To address the low reliability in this scale, we also conducted item-level analyses.
Second was a percent-completion scale (Hofmann et al., 2015; not preregistered). People described how close they were to completing the goal on a scale from 0% to 100% (“think about where you stand at the moment with regards to the completion of your goal: With 0% being at the very beginning of starting to work on your goal and 100% meaning full goal completion, how close are you to goal completion?”).
Life Satisfaction
Life satisfaction was assessed at T2 with a two-item scale developed for the national U.S. midlife survey (e.g., “At present, how satisfied are you with your life?,” 1 = not at all, 6 = extremely; α = .84; Brim et al., 2004).
Moderator: Depression Severity
Depression severity was again assessed with the Beck fast-screen, at the end of the T2 survey (α = .94; Beck et al., 2000), along with demographic information.
Results
Personal Goals
We again asked two research assistants to code the goals participants identified, using the same procedure as in Experiment 2. Inter-observer reliability was again high (0.64 ≤ ICC ≤ 0.95) and the contents were similar to the goals described in Experiment 2 (see Table 3).
Goal-Related Outcomes
General Self-Efficacy (Time 1)
Replicating Experiments 1 and 2 and confirming the pre-registered prediction, the depression-reframing exercise boosted participants’ self-efficacy to successfully pursue their goals in life in general immediately after the exercise (M = 4.25, SD = 0.85 vs. M = 3.60, SD = 1.03), F(1,169) = 19.93, p < .001, d = 0.68, 95% CI [0.37, 0.99], see Figure 4.
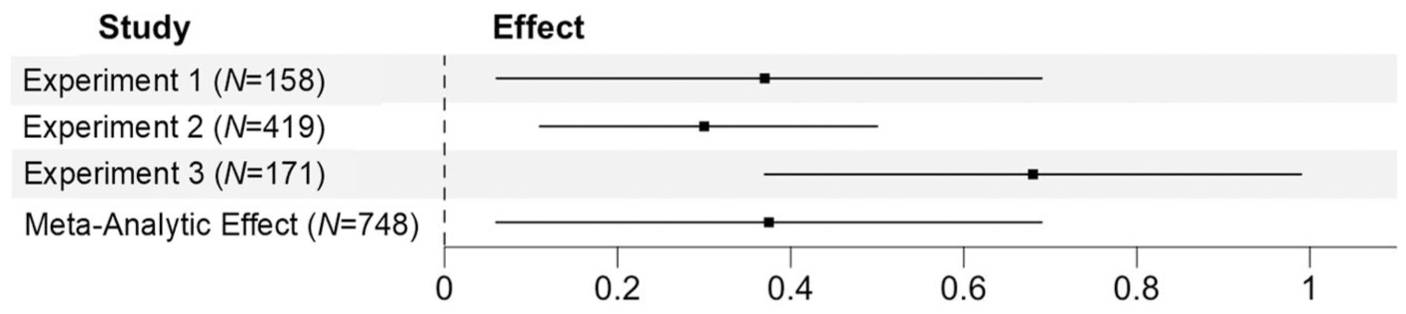
Effects of the depression-reframing-exercise on general efficacy across studies.
Progress Toward a Specific Personal Goal (Time 2)
The exercise also increased the progress individuals reported having made toward the valued goal they had specified at T1 at the 2-week assessment (see Figure 5).
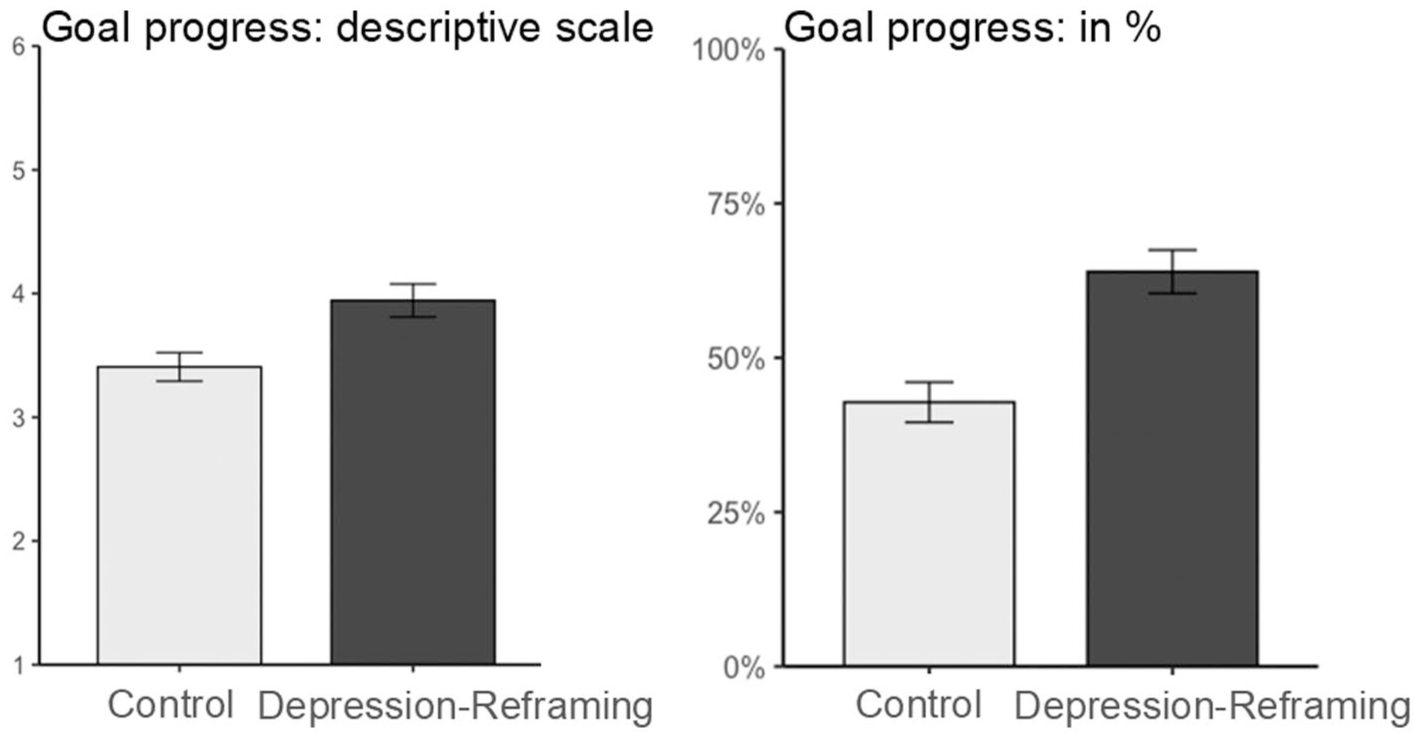
Self-reported progress on a personal goal over 2 weeks as assessed by two scales (Experiment 3).
Analysis of the descriptive scale yielded a positive effect of the depression-reframing exercise, F(1,164) = 9.10, p = .003, d = 0.47, 95% CI [0.16, 0.78], (M = 3.94, SD = 1.21 vs. M = 3.41, SD = 1.08), as predicted and pre-registered. Exploratory item-level analyses showed a robust effect on the item describing the progress individuals reported having made (“I have made progress with regards to this goal”), F(1,164) = 9.06, p = .003, d = 0.47, [0.16, 0.78], (M = 4.36, SD = 1.50 vs. M = 3.64, SD = 1.59), and a marginal effect on the item describing barriers to progress (“Many things have happened that made it difficult to realize the goal”), F(1,164) = 3.03, p = .084, d = 0.27, [−0.04, 0.58], (M = 3.52, SD = 1.32 vs. M = 3.17, SD = 1.28; reverse-scored, so higher values indicate fewer barriers).
The percent-completion scale also showed a significant increase, F(1,164 = 18.98, p < .001, d = 0.68, 95% CI [0.36, 0.99], (M = 63.98, SD = 32.05 vs. M = 42.79, SD = 30.49). While participants in the control condition reported being 43% done with their goal at the 2-week assessment, the depression-reframing exercise boosted this to 64%, a 49% increase.
Mediation Analysis
Exploratory analyses tested whether the T1-improvements in general self-efficacy mediated effects on goal progress. We found no significant mediation, indirect effects on the descriptive scale, 95% CI [−0.05, 0.18], and on the percentage scale, [−3.49, 3.14]. While the intervention improved general self-efficacy at T1, self-efficacy at T1 did not predict specific goal progress at T2, b = 0.10, SE = 0.10, p = .261, and b = −0.09, SE = 2.63, p = .973, respectively. As we will discuss, cascading processes (e.g., changes in behavior, longer-term changes in self-efficacy, and/or commitment) beyond immediate changes in efficacy may be key in carrying long-term benefits forward.
Self-Compassion, Help-Seeking, and Well-Being
Self-Compassion and Help-Seeking (T1)
When asked to imagine a relapse of depression, participants expressed greater compassion for themselves in the depression-reframing (vs. control) condition, F(1,169) = 10.22, p = .002, d = 0.49, 95% CI [0.18, 0.79], (M = 3.45, SD = 1.18 vs. M = 2.91, SD = 0.99).
On a marginal level, they were also more likely to report they would seek help from friends and family members in this circumstance, F(1,169) = 3.08, p = .081, d = 0.27, 95% CI [−0.003, 0.57], (M = 3.98, SD = 1.52 vs. M = 3.57, SD = 1.52). However, support-seeking from mental-health professionals was high in both conditions and did not differ by condition, F(1,169) = 0.006, p = .938, d = 0.01, [−0.29, 0.38], (M = 3.93, SD = 1.53 vs. M = 3.91, SD = 1.57).
Life Satisfaction (T2)
Life satisfaction did not yield a significant effect of condition, F(1,163) = 0.22, p = .644 (depression-reframing: M = 3.22, SD = 1.33; control: M = 3.13, SD = 1.11).
Moderation by Depressive Symptoms
We again tested whether depression severity moderated any depression-reframing effects, finding no significant effects, all ps > .10.
To maximize power, we repeated the moderation analysis on general self-efficacy combining all three samples (N = 748). Still, the moderation effect was not significant, F(1,736) = 2.51, p = .114. 1 While people with more severe symptoms reported lower self-efficacy to achieve their goals, F(1,736) = 212.98, p < .001, they were not less responsive to the depression-reframing-exercise. If anything, the pattern was such that they showed the largest increase in self-efficacy (see Figure 6; condition effects by subgroup are reported in the Supplement).
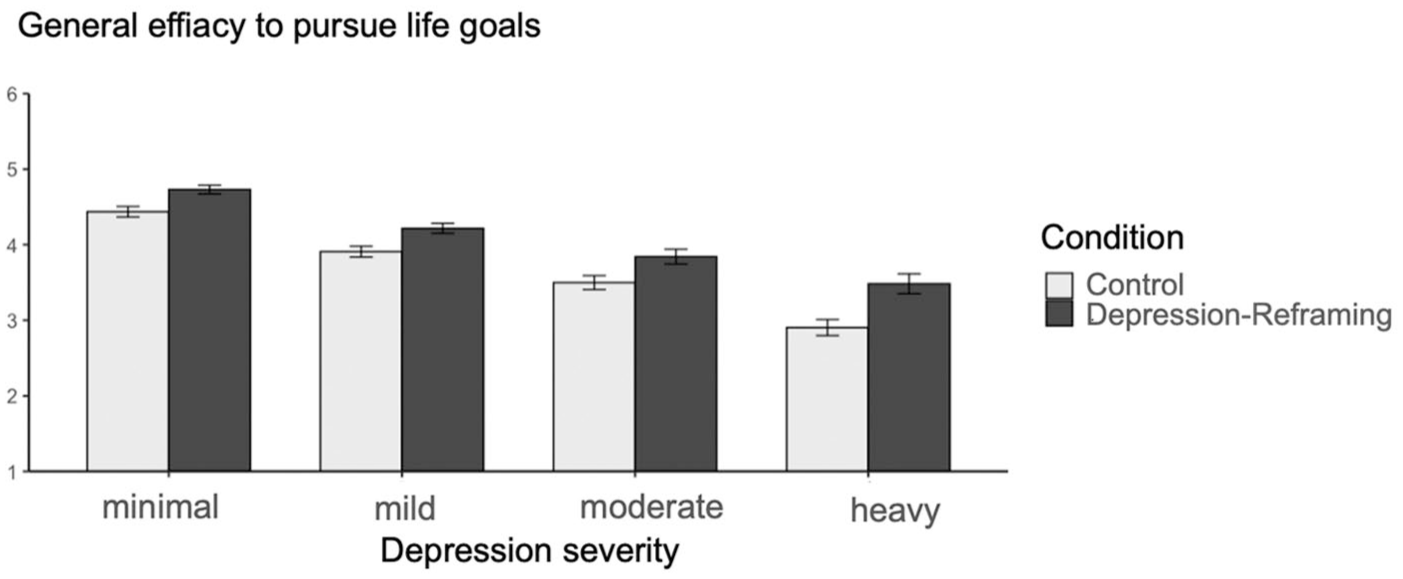
Effects of the depression-reframing-exercise on general efficacy by current depression severity.
Comparing the experimental effect with the effect of depression severity revealed that the average effect of the depression-reframing-intervention on general efficacy to accomplish goals, d = 0.40, 95% CI [0.26, 0.55], was 78% as large as the difference between people with a heavy and a moderate depression, d = 0.51, [0.28, 0.74].
Discussion
In Experiment 3, not only did the depression-reframing exercise again increase general efficacy among people who had experienced depression; it also boosted the degree to which people reported they had completed a valued personal goal 2 weeks later, from 43% complete in the control condition to 64% complete in the depression-reframing condition. Participants were not just more confident. They put their confidence to work. In addition, participants expressed greater compassion for themselves should they experience a relapse of depression and on a marginal level, greater intentions to seek help from family and friends in this circumstance. We did not find effects on individuals’ overall life satisfaction at the 2-week assessment point.
General Discussion
Societal narratives often frame people who have experienced depression as inherently weak, unable to pursue goals effectively. While depression can create barriers to goal pursuit, we provide causal evidence that this stigmatizing narrative itself contributes to self-confirming cycles. It makes people less confident in their abilities, holds them back from fully committing to their goals, and, over time, constrains the progress they make on goals they value.
We show the causal influence of the depression-as-inherent-weakness-narrative by countering it. We developed a brief (~20 min) exercise that reframes what it means to be a person who has contended with depression: As a resourceful person who has shown strengths in contending with an illness. Reflecting the predominant societal narrative, Experiment 2 revealed that 71% of participants in the active control condition indicated that the strengths necessary to pursue goals did not describe people dealing with depression well. The depression-reframing exercise reduced this perceived incompatibility to 52%.
In turn, this representation of personal strength boosted the confidence people expressed in their ability to pursue their goals as well as their commitment to these goals (Experiments 1–3). These gains are substantial. For instance, the increase in general self-efficacy caused by the intervention is similar in magnitude to the difference in efficacy observed between people with moderate versus heavy symptoms of depression. Most important, the depression-reframing exercise caused a 49% increase in the progress participants reported making toward completing a valued personal goal 2 weeks later (Experiment 3).
Our results extend several areas of research. First, prior research has shown the benefits of reframing the strengths of students whose social-identity groups are commonly represented as weak, including low-SES students and students with refugee backgrounds (Bauer & Walton, 2023; Bauer et al., 2021, 2025; Hernandez et al., 2021). Marginalized social-identity groups often face external challenges, which can make it easier for them to reframe their strengths in the face of adversity. In contrast, the challenges that come with depression and other mental illnesses (e.g., low energy levels) are often internal, and more readily conflated with inherent weaknesses. We demonstrate that it is possible to reframe internal challenges too, and that doing so can help individuals achieve their goals.
Second, our studies isolate the causal effects of a specific default narrative—depression-as-inherent-weakness—among people who have experienced depression. In so doing, they invite researchers to explore the causal effects of other specific narratives, both among people with depression and others. Further, they invite designers to consider how they can incorporate or adapt depression-reframing in ongoing programming for people with depression.
A third contribution is methodological. By adapting social-psychological intervention methods to a clinical population, we were able (a) to test the effect of a specific mechanism (inherent-weakness-narratives) on goal pursuit, (b) to do so in three randomized-controlled experiments with large samples of people who have experienced depression (Ntotal = 748), including a longitudinal trial with minimal dropout (3%), and (c) to develop a highly scalable, and hence practically useful tool that could reach many people at low marginal cost. These methods do not meet all needs. Yet, they have important advantages for cumulative science, complementing traditional resource-intensive methods used to study clinical populations.
Limitations and Future Directions
Measures of Goal Progress
To assess goal progress, Experiment 3 used subjective self-reported measures. This approach allowed us (a) to assess progress across a wide range of personally important goals and (b) to use individuals’ own standards of assessment. While subjective measures predict objective measures of goal progress (Brunstein et al., 1998; Hofmann et al., 2015), it is also valuable to assess objective measures to confirm this progress and understand how it comes about. To this end, future research may include behavioral goal pursuit measures, such as goals established in a therapeutic context (e.g., to increase exercise, as assessed by smartwatch data) or pursued in institutional settings (e.g., performance in school or at work), as in prior research on identity-reframing-interventions implemented in school contexts (Bauer et al., 2021, 2025).
Assessment Duration and Frequency
Another important direction for future research is to extend the assessment period beyond 2 weeks. Objective measures of goal progress, accompanied by daily-diary self-reports over a longer window, could provide more granular insights into the cascade of processes by which the depression-reframing intervention may cause improvements over time, as well as inform boundary conditions on longitudinal benefits. Extending the assessment period would also permit a closer examination of well-being and mental-health related outcomes. An important finding in Experiment 3 was that the depression-reframing exercise increased the compassion people anticipated feeling for themselves should they experience a relapse of depression. An extended assessment could examine this response in vivo, as well as follow up on the marginal pattern observed in Experiment 3 on support-seeking from friends and family in the event of a relapse. Such measures would inform whether depression-reframing can enhance the resilience of people to future experiences of depression. Additionally, while Experiment 3 yielded no effects on life satisfaction over 2 weeks, future studies could assess both day-to-day well-being and broader affective outcomes over time.
Role of Perceived Expectations of Others
Future research may also examine the role of participants’ perception that those providing the depression-reframing exercise want them to show strength in the effects of the depression-reframing intervention. While it seems unlikely that a pure demand process explains the goal pursuit effects reported 2 weeks after the intervention (Experiment 3), it is possible that demand processes could contribute to immediate self-report effects, for example, making people in the intervention (vs. control) more likely to reference strengths in the reflection exercises and to report high self-efficacy levels. Indeed, much past research identifies the importance of others’ views and expectations for intervention effects (e.g., Rosenthal & Jacobson, 1968): if an intervention changes how people think they are seen and what is expected of them, it can shift how people see themselves, and how they behave, contributing to self-fulfilling effects. That is, demand effects may contribute to intervention benefits (see Corneille & Lush, 2023; Silverman et al., 2025). Future research may test this theorizing by assessing, for example, beliefs about others’ expectations and whether these beliefs mediate increases in objective indices of goal progress (see Bauer et al., 2021).
Control Comparisons
Future research may also include additional control groups to better understand depression-reframing effects. In the present research, we designed the control condition to hold constant thoughts about depression (participants read factual information about depression and openly reflected on depression experiences) without manipulating representations of strengths or weaknesses. Our experimental comparison, hence, focused on the effect of depression narratives: how people think about depression, not whether they think about depression at all.
Yet, activating thoughts about depression may well have effects compared to not thinking about depression, too. While thinking about depression may often be productive and important (e.g., to monitor symptoms and consider treatment options), if depression is associated with default inherent-weakness-narratives, unguided reflections may also undermine individuals’ efficacy. It is also possible that, with no external structure to think about depression, people suppress negative thoughts in ways that are ultimately unproductive (Gross, 2002). Future studies may explore these possibilities by including a passive or no-treatment control group alongside our depression-reframing and active control conditions.
In addition, while we activated depression in both conditions, other elements differed. For example, we did not include first-person testimonials in the active control group. Although it seems unlikely that superficial differences could explain our effects, such as the mediating role of perceived compatibility between depression (Experiment 2), future research may explore additional control conditions, such as conditions that include personal testimonials and strength reflections in contexts irrelevant to depression.
Generalizability
Another important question for future research lies in the generalizability of our findings and identifying boundary conditions.
Our recruitment targeted people who had previously been prescribed anti-depressants, indicating that a medical professional had judged their mental health symptoms as warranting medical treatment. This strategy allowed us to examine the benefits of depression-reframing for individuals who had previously experienced depression but varied in their current symptoms. Although we found no moderation by current symptomology or current anti-depressant use, we do not know whether the benefits are contingent on past anti-depressant use, as all participants had been prescribed anti-depressants. An important question is whether depression-reframing can benefit goal pursuit among people with untreated depression, including people with less access to mental health services.
Additionally, our participants were recruited through online-services in Western, relatively rich countries. An open question is to what extent the intervention would be helpful in other contexts, including populations with less access to technology and populations in which interdependent representations of the self are more prominent. The depression-reframing exercise counters a narrative about the qualities of individuals—namely, that people with depression are weak. It may be most fitting in cultural contexts in which people have strong assumptions about the distinct qualities of individuals and less fitting in settings in which people understand the self in more interdependent terms (see McAdams, 1995). In such contexts, a more collective approach may be more effective (e.g., reframing the implications of depression for the strength of families; see Thomas et al., 2025).
Enhancing Strength-Based Narratives About Depression
How might strength-based narratives about depression be enhanced further?
One way is to consider timing, which is often an important variable in wise interventions (Walton & Wilson, 2018). Instead of implementing the depression-reframing exercise at a time of convenience to a research team, could it be implemented at a critical crossroads for participants, such as at the point of or soon after a diagnosis? Would this furth enhance efficacy?
A second way is to address the social context within which a person navigates depression (see Silverman et al., 2025). Gains from the depression-reframing exercise in the long-term may depend on whether the person’s social environment affords a strength-based narrative, one that allows them to freely express and act on this narrative (Walton & Yeager, 2020). If people find, instead, that family, friends, or medical professionals express an inherent-weakness-narrative, such as by treating them with pity, overprotecting them, or looking down on them, a strength-narrative may seem illegitimate or even false and therefore difficult to sustain. Future studies could test this prediction by measuring or manipulating features of the context; for example, by adapting the depression-reframing intervention to help others recognize and honor the strengths of people contending with depression.
Supplemental Material
sj-docx-1-psp-10.1177_01461672251412492 – Supplemental material for Depression-Reframing: Recognizing the Strength in Mental Illness Improves Goal Pursuit Among People Who Have Faced Depression
Supplemental material, sj-docx-1-psp-10.1177_01461672251412492 for Depression-Reframing: Recognizing the Strength in Mental Illness Improves Goal Pursuit Among People Who Have Faced Depression by Christina A. Bauer, Gregory M. Walton, Jürgen Hoyer and Veronika Job in Personality and Social Psychology Bulletin
Footnotes
Acknowledgements
We thank Patrick Corrigan for his feedback.
Ethical considerations
An IRB was obtained (IRB of the University of Vienna).
Consent to Participate
All participants in the present research gave their informed consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present research was supported by a grant of the Austrian Science Fund (ESP 67) awarded to Christina Anna Bauer.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available online with this article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.