
Abstract
Purpose
Head and neck unicentric Castleman disease (HN-UCD) often lacks specific clinical and laboratory markers, leading to frequent preoperative misdiagnoses. While surgical resection typically offers a favorable prognosis, the management of atypical postoperative outcomes, such as new regional lymphadenopathy or persistent systemic symptoms, remains poorly defined. This study aimed to identify the characteristic imaging features of HN-UCD and explore effective management strategies for these atypical postoperative scenarios.
Methods
A retrospective analysis was conducted on 24 patients diagnosed with HN-UCD at the Peking Union Medical College Hospital over the past 20 years. The preoperative imaging characteristics and postoperative clinical outcomes were systematically evaluated.
Results
Imaging confirmed significant hypervascularity as a hallmark of HN-UCD: 94.4% (17/18) of lesions exhibited abundant and disordered blood flow signals on ultrasound, and 71.4% (10/14) of lesions presented with prominent feeding vessels on CT. Postoperatively, 87.5% (21/24) of the patients achieved complete remission within the surgical field. For the two patients exhibiting atypical outcomes (new regional lymphadenopathy and persistent fever), a strategy of rigorous follow-up was adopted after multidisciplinary exclusion of malignancy and infection; both patients remained clinically stable.
Conclusion
Prominent feeding vessels and marked hypervascularity are characteristic preoperative imaging markers for HN-UCD. For patients with atypical postoperative outcomes, a management protocol based on multidisciplinary evaluation and close clinical observation is recommended.
Introduction
Unicentric Castleman Disease (UCD) is a rare and heterogeneous lymphoproliferative disorder characterized by the pathological enlargement of a single lymph node station. UCD can affect individuals of all ages (ranging from 2 to 84 years), with a median age of 34 years at diagnosis. 1 The estimated incidence of UCD in the United States is 16–19 per million. 2 Histologically, UCD is primarily classified into three variants: the hyaline-vascular (HV) variant (79.0%), the plasma cell (PC) variant (13.1%), and the mixed subtype (7.9%). 3 Topographically, UCD can occur in various anatomic regions. The mediastinum is the most common site of involvement (29%), followed by the neck (23%), abdomen (21%), and retroperitoneum (17%). 4 Although it predominantly affects lymph nodes, rare extranodal involvement of parenchymal organs and soft tissues can occur, most frequently in the pancreas, adrenal glands, and skeletal muscle. 5 Clinically, most UCD cases present as a painless mass; however, as the lesion expands, it may not only compress vital adjacent anatomical structures but also lead to complications such as autoimmune hemolytic anemia and autoimmune thrombocytopenia, which can severely impact the patient’s quality of life or even prove life-threatening. 6 Consequently, early and precise diagnosis and intervention are critical for patients with UCD. Nevertheless, misdiagnosis remains common due to its tumor-like radiological appearance and clinical symptoms that often mimic infection. 7 In this context, identifying characteristic preoperative imaging features is crucial for differential diagnosis and surgical planning.
Surgical resection remains the preferred therapeutic strategy for UCD and is generally associated with a favorable prognosis. A large-scale retrospective study involving 1,634 patients demonstrated a 3-year overall survival rate of 98.0%. 3 However, the favorable overall prognosis can obscure specific clinical challenges: a minority of patients may experience postoperative local recurrence, new-onset lesions, or even persistent systemic inflammatory symptoms resembling multicentric Castleman disease (MCD), such as fever, fatigue, and weight loss.8,9 Although some studies suggest that these symptoms often resolve spontaneously after surgery, a few patients exhibit refractory symptoms that necessitate medical intervention.9,10 Due to the scarcity of relevant case reports, there are currently no clear clinical guidelines for managing such complex postoperative outcomes.
As noted above, the head and neck is a common site for UCD, accounting for approximately 23% of all cases. 4 Specifically within this region, lesions typically arise in regional cervical lymph nodes but can also manifest in mucosal locations and major salivary glands.5,11 However, specialized research on head and neck UCD (HN-UCD) remains limited, particularly regarding in-depth discussions on imaging characteristics and atypical postoperative outcomes. This study retrospectively reviewed the clinical data of patients with HN-UCD at Peking Union Medical College Hospital (PUMCH) over the past 20 years, focusing on summarizing the imaging features and postoperative outcomes. We aim to provide clinical insights and the “Chinese experience” to support the preoperative diagnosis and postoperative management of HN-UCD.
Materials and Methods
Patient Selection
This study was approved by the Institutional Review Board of PUMCH (Ethics No. K25C3638), and informed consent was obtained from all participants. Clinical data of patients pathologically diagnosed with HN-UCD between 2005 and 2025 were retrospectively retrieved. The inclusion criteria were as follows: (1) histopathological confirmation of Castleman disease; (2) disease localization to a single anatomical region in the head and neck, with involvement of other lymph node stations ruled out by preoperative systemic imaging; (3) exclusion of lymphoma, IgG4-related disease, systemic lupus erythematosus, and other autoimmune or infectious lymphadenopathies; and (4) availability of complete clinical and imaging data.
Data Collection and Imaging Assessment
Patient demographics, clinical manifestations, laboratory findings, surgical records, and pathological subtypes were collected from the electronic medical record system. Preoperative imaging data, including ultrasound, CT, MRI, and PET/CT, were systematically re-evaluated for all patients. We recorded the lesion size, location, borders, density/signal characteristics, enhancement patterns, the presence of necrosis or calcification, and the relationship with adjacent vasculature. Follow-up data were obtained from outpatient review records or telephone interviews. The primary observation endpoints included postoperative symptom resolution, local recurrence, and survival status.
Statistical Analysis
Statistical analysis was performed using R software (version 4.4.3). The normality of continuous variables was determined using the Shapiro-Wilk test. Normally distributed continuous data were expressed as mean ± standard deviation (Mean ± SD). Non-normally distributed data were presented as median (interquartile range) [M (IQR)]. Categorical variables were reported as frequencies and percentages [n (%)].
Results
Baseline Characteristics and Clinical Features
Baseline Characteristics and Postoperative Outcomes of 24 Patients With HN-UCD

Note. Due to the retrospective nature of this study, baseline laboratory data were incomplete for certain variables. Specifically, serum albumin levels were available for 21 of the 24 patients, and hs-CRP levels were available for 15 patients.
Imaging Findings
Imaging Features of Patients With HN-UCD

On ultrasonography, 94.4% (17/18) of the enlarged lymph nodes appeared as hypoechoic masses with regular shapes, well-defined margins, and poorly defined corticomedullary junctions (Figure 1A). Among these, 27.8% (5/18) showed heterogeneous internal echogenicity, 16.7% (3/18) exhibited iso-to-hyperechoic or hyperechoic signals, and 22.2% (4/18) displayed linear or reticular echoes within the nodes. Color Doppler flow imaging (CDFI) revealed abundant and disorganized blood flow signals within the masses in 94.4% (17/18) of patients (Figure 1B). On CT, all lymph nodes appeared as round or oval soft-tissue density masses with clear margins; they exhibited relatively homogeneous density similar to surrounding muscles on plain scans and showed homogeneous or heterogeneous enhancement on contrast-enhanced scans. Rich vascular supply around the tumors was observed in 71.4% (10/14) of patients, with some showing tortuous and enlarged intra- or extranodal vessels (Figure 1C-E), while distinct internal calcification was noted in 7.1% (1/14). Neck soft tissue MRI showed well-defined tumor margins, with isointense or slightly prolonged T1 signals and long T2 signals; contrast-enhanced MRI demonstrated significant homogeneous enhancement in the arterial phase and slightly decreased enhancement in the venous phase. Flow-void signals were visible within or around the tumors in 30% (3/10) of patients (Figure 1F-H), and all three cases involving DWI sequences showed high signals. In the limited subset of patients who underwent PET/CT (n=4), imaging revealed mildly increased radioactivity uptake in the enlarged neck lymph nodes (Figure 1I-J), with a mean SUVmax of 4.03 ± 1.04 g/mL. Representative imaging findings of HN-UCD. (a-b) Ultrasound imaging revealed a hypoechoic lesion with abundant internal blood flow signals. (c-e) CT shows a soft tissue density mass with visible peripheral and internal vasculature. (f-h) MRI demonstrates isointense to slightly prolonged T1 signals and prolonged T2 signals with internal flow-void phenomena. (i-j) PET/CT shows mild metabolic activity within the lesion. Red arrows indicate external (extranodal) feeding vessels; blue arrows indicate internal (intranodal) feeding vessels
Treatment and Postoperative Outcomes
Detailed Anatomical Localizations and Surgical Procedures of the 24 HN-UCD Patients

Notes.
1 Lesion location refers to the primary site of the dominant disease focus identified preoperatively and intraoperatively.
2 Surgical procedure was determined based on the complete excision of the primary lesion and was further guided by intraoperative exploration to address any suspicious regional lymphadenopathy.
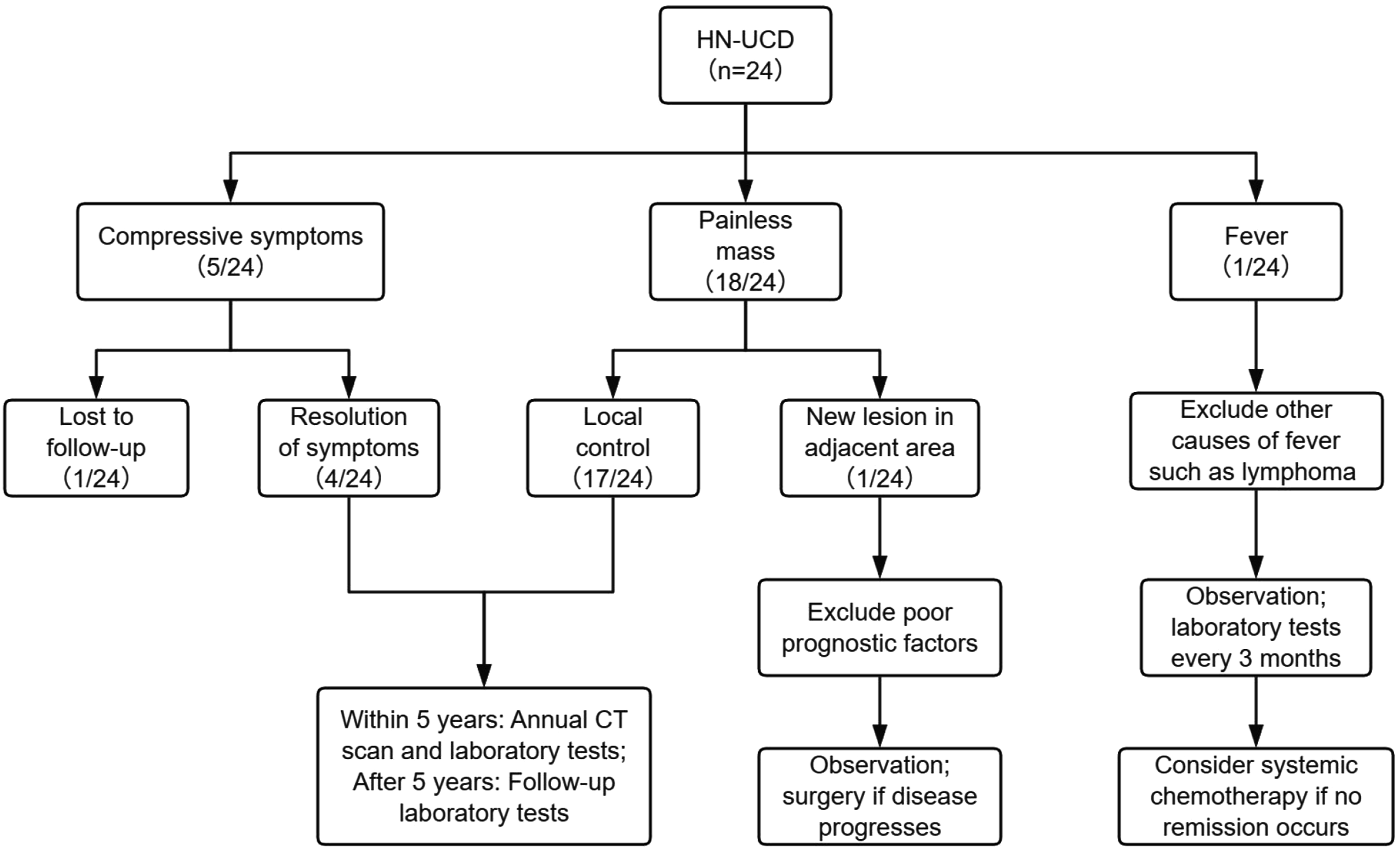
Postoperative outcomes and surveillance protocols for patients with HN-UCD
Case of New Regional Lymphadenopathy
One patient underwent resection of lesions in the right cervical Levels II and V. A follow-up examination seven months postoperatively revealed a new enlarged lymph node (2.2 × 1.2 cm) at the junction of the right cervical Levels III and IV. Laboratory investigations showed no abnormalities, and ultrasound and PET/CT revealed no evidence of lymphadenopathy in other regions. Given the absence of subjective discomfort and the exclusion of adverse high-risk prognostic factors, an active surveillance strategy was adopted following thorough patient-clinician communication, and the patient’s condition remained stable.
Case of Persistent Systemic Symptoms
One patient, who primarily presented with recurrent fever preoperatively, experienced a febrile relapse four months after surgery following a period of normal body temperature. The fever was periodic, with peak temperatures fluctuating between 37.0°C and 38.0°C, and resolved spontaneously. Following multidisciplinary consultations with the Departments of Hematology and Infectious Diseases, comprehensive evaluations, including inflammatory markers, a full immunological profile, and PET/CT, revealed no evidence of malignancy, active infection, or autoimmune disease. This patient is currently under close follow-up.
Additionally, among the patients presenting with preoperative local compression symptoms (n=5), symptoms resolved completely in four cases, while one patient was lost to follow-up.
Discussion
Although the exact etiology of HN-UCD remains elusive, it may involve clonal expansion of lymph node stromal cells.12,13 While preoperative laboratory tests in patients with HN-UCD often lack specificity, our study and existing literature confirm that characteristic imaging features are the primary clues for preoperative diagnosis, with the most prominent hallmark being extreme hypervascularity.14,15 Disorganized blood flow signals on Doppler ultrasound and coarse, prominent feeding vessels on CT or MRI are consistent with previous findings. 16 Furthermore, internal linear or reticular echoes and heterogeneous enhancement correspond pathologically to fibrous deposition, cystic degeneration, or necrosis. 15 Some studies suggest these features are more common in lesions with a diameter > 5 cm,17,18 aiding in the differentiation from lymphoma. Although lymphoma can also be hypervascular, it typically lacks coarse feeding vessels and often involves multiple or bilateral lymph node regions. In contrast, benign reactive lymph nodes usually exhibit absent or regular hilar blood flow.16,19 Regarding calcification, while some scholars consider it a characteristic of UCD, 20 we observed it in only one patient. This differs from the 22.4%–24.4% incidence reported in the literature,21-23 suggesting that calcification may not be a sensitive marker for HN-UCD.
Surgical resection remains the therapeutic cornerstone for HN-UCD.
12
While local mass excision is the standard approach for typical well-circumscribed nodal disease, the surgical strategy should be tailored to the disease extent and specific anatomical location. As demonstrated in our cohort, selective neck dissection may be warranted when lesions involve multiple adjacent lymph nodes. Furthermore, for complex anatomical sites, a recent report demonstrated that transoral robotic surgery (TORS) is a safe and effective minimally invasive option for debulking mucosal UCD lesions, such as those situated at the base of the tongue.
24
However, there is limited guidance in the literature regarding the management of regional recurrence or new postoperative lesions. In this study, one patient developed a new enlarged lymph node in an adjacent area postoperatively; due to its slow growth and the absence of systemic symptoms, an active surveillance strategy was chosen. This scenario may represent an intermediate state between UCD and MCD, termed “Oligocentric Castleman Disease” (OligoCD). OligoCD is defined by the involvement of more than one but a limited number of lymph node regions, with systemic inflammation less severe than that of idiopathic MCD.10,12,25 Current expert consensus tends to recommend surgery over systemic chemotherapy for these patients.
12
Talat
4
also noted in a 10-year retrospective study that lesions in some patients under observation remained stable over the long term without affecting their survival. Therefore, after excluding adverse prognostic factors, such as the plasma cell subtype, anemia (Hb ≤ 100 g/L), hypoalbuminemia (albumin
While surgery is typically curative, a very small number of patients still exhibit persistent postoperative systemic symptoms, posing a clinical challenge. One patient in our cohort experienced recurrent low-grade fever post-surgery, which, despite resolving spontaneously, underscores the clinical heterogeneity of HN-UCD. Such cases with hyperinflammatory manifestations clinically mimic MCD. Recent reports have emphasized that while most patients experience symptom resolution within several years after resection, symptoms such as fatigue and night sweats may persist in a minority.9,10 Rigorous follow-up is essential to exclude lymphoma transformation or occult infection. 28 If symptoms persist and affect the quality of life after such exclusions, immunomodulatory therapy may be considered. 10 For patients with favorable postoperative recovery, we recommend annual imaging (CT) and laboratory tests (including complete blood count, LDH, liver and kidney function, CRP, and immunoglobulin quantification). If there is no evidence of recurrence for five consecutive years, routine CT scans may be discontinued, maintaining only laboratory monitoring. 12
This study had several limitations. First, its retrospective single-center design and relatively small sample size may introduce selection bias; specifically, PET/CT data were available for only four patients, making our SUVmax findings preliminary. Second, the follow-up duration for some cases was short, which may be insufficient to capture long-term complications or late-onset recurrence. Future research should focus on multicenter collaborations and extended follow-up periods to establish more evidence-based diagnostic and therapeutic standards for HN-UCD.
Conclusion
In conclusion, HN-UCD is a rare hypervascular lymphoproliferative disorder. Its preoperative imaging features are highly suggestive, typically manifesting as well-circumscribed, intensely enhancing masses with characteristic coarse feeding vessels and internal fibrous septa, whereas necrosis or cystic degeneration is rare. While surgical resection remains the gold standard of treatment, this study underscores the necessity of long-term postoperative follow-up. Specifically, for atypical cases, such as the emergence of new regional lymphadenopathy or persistent systemic symptoms, individualized surveillance protocols established through multidisciplinary collaboration are essential to guide subsequent clinical decision-making.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to the staff of the Medical Records Department at PUMCH for their invaluable assistance and professional support in retrieving the historical clinical data spanning the 20-year study period.
Ethical Considerations
The study was conducted with the approval of the Peking Union Medical College Hospital Ethics Committee (approval no: K25C3638).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National High Level Hospital Clinical Research Funding (2022-PUMCH-B-094).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.