
Abstract
Introduction
Orbital involvement is a serious complication of ethmoiditis in children, often occurring because the ethmoid sinuses are very close to the orbit. Our work aimed to report the clinical presentation, treatment modalities and the outcome of orbital complications of acute ethmoiditis to identify common indicators for surgery.
Methods
Retrospective observational study to review cases that were hospitalized in pediatrics and otorhinolaryngology departments of the Farhat Hached Hospital in Sousse, Tunisia, during the period from January 2013 to December 2023.
Results
We collected 79 cases. The mean age was 4,55±3,64 years old. Five of our patients had anemia, six had allergic rhinitis, and one had asthma. Two other patients had undergone recent dental care. Palpebral edema and fever were the most frequently reported symptoms. A palpebral abscess was present in five cases, while nineteen cases exhibited exophthalmos. Seven children had limited occulomotricity, and one child had ophthalmoplegia.In addition, reduced visual acuity was reported in 3 cases. Referring to Chandler’s stratification, we report 37 cases of preseptal cellulitis, 10 cases of orbital cellulitis and, 31 cases of subperiosteal abscess. Eleven patients required surgical treatment consisting of orbitotomy. Age equal to or above 5 years old was more associated with surgical treatment (p<0.001). The outcome was generally favorable.
Conclusion
Orbital complications of acute ethmoiditis are a low-prevalence high risk disease. Most patients are successfully treated without long-term complications. Younger children (<5 years) are less likely to undergo surgery.
Introduction
Acute ethmoiditis is a potentially severe inflammatory condition of the ethmoid sinus complex. In the pediatric population, the clinical presentation often follows a progressive course, traditionally categorized into two stages: the pre-septal (periorbital) stage, characterized by localized edema of the inner canthus and low-grade fever; and the orbital stage, marked by systemic distress, high fever, and alarming local signs including proptosis, ophthalmoplegia, and visual impairment. Children are inherently more vulnerable than adults due to their immature immune systems and the anatomical specificities of the developing ethmoid bone, notably the thinness and porosity of the lamina papyracea. This anatomical proximity facilitates the rapid spread of infection from the paranasal sinuses to the orbit and, potentially, the intracranial compartment. 1
While orbital involvement occurs in 3–4% of pediatric acute rhinosinusitis cases, 2 it remains a diagnostic and therapeutic challenge requiring multidisciplinary management. Although the prognosis has improved significantly since the introduction of targeted antibiotic therapy, orbital complications remain a leading cause of preventable blindness, with permanent vision loss still reported in 3% to 11% of cases. 2 While medical therapy remains the cornerstone of treatment, surgical intervention remains indicated in specific refractory or advanced cases.
In recent years, an increasing incidence of orbital cellulitis has been observed within our department. Given the paucity of recent regional data regarding the clinical patterns and prognostic factors of this condition, we conducted this retrospective observational study to evaluate the clinical spectrum, management strategies, and outcomes of orbital complications secondary to acute ethmoiditis in children.
Methods
This retrospective observational study included 79 patients identified as having orbital complications of acute ethmoiditis in the database in the Departments of Paediatric and otorhinolaryngology of Farhat Hached University Hospital in Sousse. We reviewed medical records identified through the hospital database using the following keywords: “ethmoiditis,” “orbital cellulitis,” “orbitotomy,” and “subperiosteal abscess.”
The study period spanned 11 years, from January 2013 to December 2023. We included in this study children who were aged 16 years old or younger diagnosed with unequivocal evidence of acute exteriorized ethmoiditis during the study period (Ethmoid sinus filling in the computed tomography (CT) scan and/or the magnetic resonance imaging (MRI) with an orbital complication) and who required an inpatient treatment (medical treatment with or without surgical treatment). We excluded from this study patients who had an orbital infection caused by conditions other than acute ethmoiditis (insect bite, wound, dacryocystitis, etc ..) or had non exteriorized ethmoiditis. Clinical, epidemiological, and therapeutic data were extracted and recorded using a standardized data collection sheet. To assess the severity of orbital complications, we utilized the Chandler classification, which categorizes the progression of the disease into five distinct clinical stages: Stage I (Preseptal Cellulitis): Inflammatory edema of the eyelids without orbital involvement; Stage II (Orbital Cellulitis): Diffuse inflammation of the orbital contents with chemosis and proptosis, but without a discrete abscess; Stage III (Subperiosteal Abscess (SPOA)): A collection of purulent material between the periorbital and the bony orbital wall, often resulting in globe displacement; Stage IV (Orbital Abscess): A discrete collection of pus within the orbital fat or extraocular muscles, typically associated with ophthalmoplegia and decreased visual acuity; Stage V (Cavernous Sinus Thrombosis): Bilateral symptoms, cranial nerve palsies, and potential intracranial spread, representing the most life-threatening stage.”
Statistical analysis was performed using SPSS IBM version 23.0 to identify factors associated with the requirement for surgical intervention. A univariate analysis was conducted to compare clinical and epidemiological variables (e.g., age, gender) between patients managed with exclusive medical therapy and those requiring surgical drainage. Categorical variables were compared using the Chi-square test or Fisher’s exact test as appropriate. All statistical tests were two-tailed, with a significance level set at p <0.05.
Ethical Consideration
Due to the retrospective nature of the study and the use of de-identified data, the requirement for informed consent was waived, in accordance with institutional ethical guidelines.
Results
A total of 79 patients were included in the study. The cohort’s age ranged from 5 months to 14 years, with a mean age of 4.55 ± 3.64 years. Notably, more than three-quarters of the patients (75.9%) were under 5 years of age. A male predominance was observed, with a sex ratio of 1.72.
The mean annual incidence was 2.57 cases per year, with a marked seasonal distribution; the majority of admissions occurred during the winter and spring months.
Regarding the chronological trend, a gradual increase in the number of cases was observed over the study period. However, a significant decline was recorded in 2020 and 2021, coinciding with the COVID-19 pandemic and associated public health measures. Following this period, a subsequent rise in the annual case count was noted, as illustrated in Figure 1. Distribution of ethmoiditis cases in children by year
The mean delay between symptom onset and consultation was 3.01 ± 2.3 days (range: 0–14 days). Evaluation of medical history revealed potential predisposing factors, including anemia (n=5), allergic rhinitis (n=6), and asthma (n=1). Dental involvement was noted in two cases: one patient had undergone dental procedures three days prior to admission, and another presented with untreated dental caries. No history of cystic fibrosis, primary ciliary dyskinesia, nasal polyposis, or craniofacial trauma was reported in our cohort.
Prior to emergency department presentation, 17 patients (21%) had initiated antibiotic therapy, primarily amoxicillin-clavulanic acid, for a mean duration of 2,78 ± 0,83 days. Symptomatic treatment was administered to 25% (n=20) of the children, consisting of paracetamol (n=12) or NSAIDs (n=8).
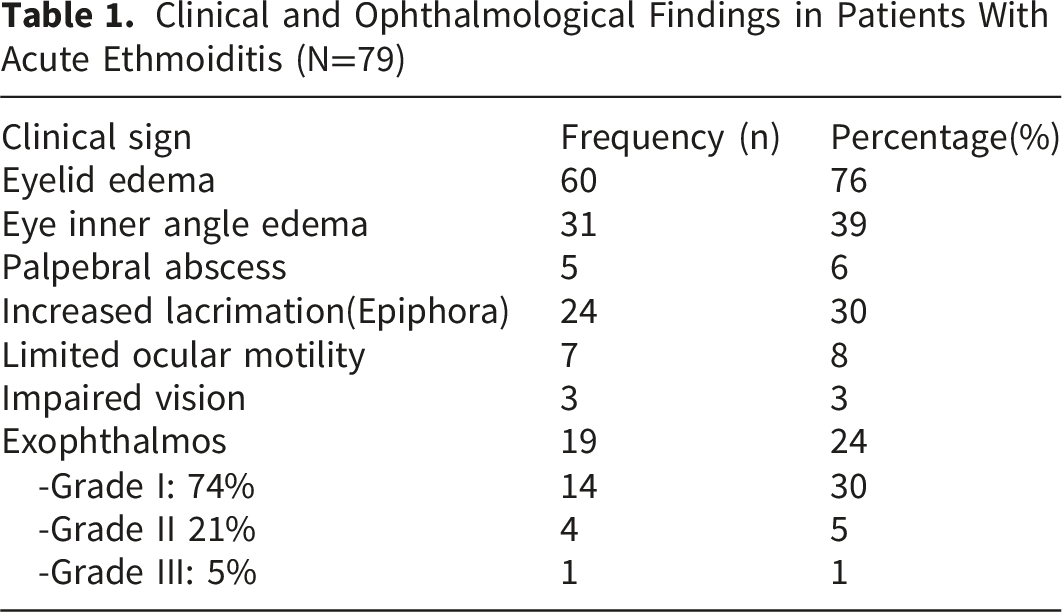
At the time of admission, fever was present in 59% (n=47) of the patients. The most common physical finding was palpebral edema (n=60, 76%), which was bilateral in 4.2% of cases. The right and left sides were affected almost equally (48,6%, n=38 and 47,2%, n=37, respectively). In 39% (n=31) of cases, the edema was localized strictly to the inner canthus.
Advanced orbital signs included exophthalmos in 19 patients (24%) and limited ocular motility in seven patients (8%), one of whom presented with complete ophthalmoplegia. Specific motility deficits included impaired adduction and abduction (n=5) and restricted elevation (n=2). Additionally, five children (6%) presented with a palpable palpebral abscess upon admission, and three children reported blurred vision. Rhinorrhea was observed in 22 cases (unilateral in 14), characterized as serous (n=13) or purulent (n=9). Headaches were reported by nine patients. Funduscopic examination was performed in seven cases, all of which yielded normal results.
Physical examination revealed a normal nasal pyramid in all patients, with no observed deformities. Anterior rhinoscopy demonstrated mucosal congestion in 36 children (45%) and the presence of purulent discharge in the middle meatus in 46 patients (58%). Structural abnormalities, specifically nasal septal deviation, were noted in two patients (2.5%).
Clinical and Ophthalmological Findings in Patients With Acute Ethmoiditis (N=79)
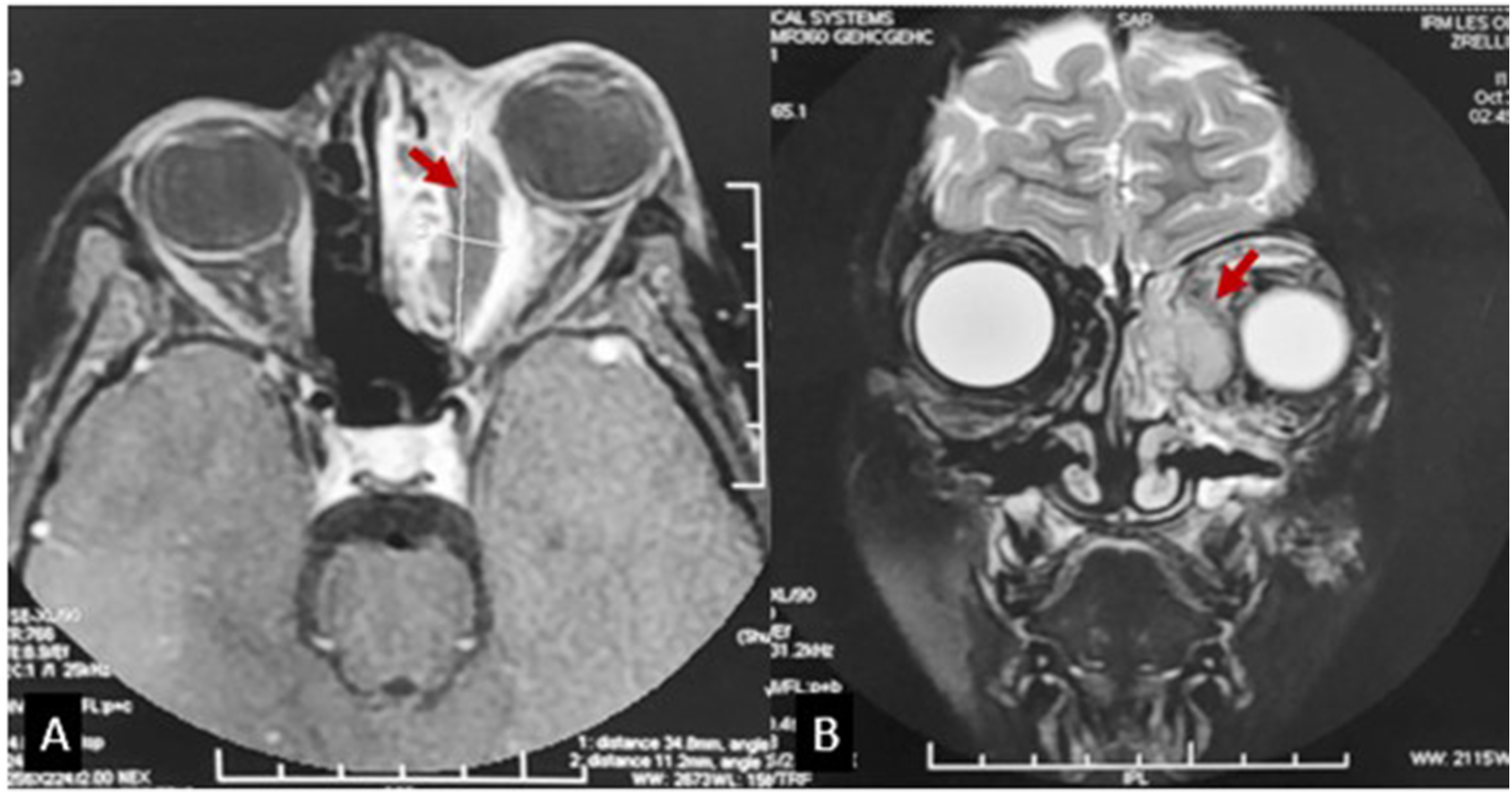
Regarding imaging modalities, orbital ultrasonography was performed in only one patient, confirming orbital cellulitis. Computed Tomography (CT) of the sinuses and orbits was the primary imaging tool, conducted in 77 cases (97%) to confirm the diagnosis, stage the orbital complications according to Chandler’s classification, and identify anatomical variants (Figure 2). The remaining two patients underwent magnetic resonance imaging (MRI) as their initial assessment (Figure 3). CT scan of the facial skeleton showing lamina papyracea lysis Complete opacification of the left ethmoidal sinus is associated with marked lysis of the lamina papyracea (black arrow). There is concurrent infiltration of palpebral fat and temporal soft tissues (red arrow) T1-weighted axial MRI section (A) and T2-weighted fat-saturated coronal section ( B) of the facial mass: Demonstration of a large left subperiosteal abscess ( red arrow) with mass effect on the left orbit resulting in grade 2 exophthalmos
Analysis of the ethmoid sinuses revealed total opacification in 49 children and partial opacification in 30. This involvement was unilateral in 47 cases and bilateral in 32. Associated sinus involvement was frequent: maxillary sinus opacification: 64%, n=51, sphenoid sinus opacification: 20%, n=16 and frontal sinus opacification: 16%, n=13. Pansinusitis was identified in 4 patients within our cohort.
According to Chandler’s classification, the distribution of orbital complications was as follows: Stage I (Pre-septal cellulitis): Identified in 37 patients (48%), five of whom (13%) presented with an associated palpebral abscess; Stage II (Orbital cellulitis): Diagnosed in 10 patients (13%); Stage III (SPOA): was observed in 29 patients (37%). Notably, one patient presented with bilateral SPOA. The mean maximum dimension of the abscesses was 17.28 ± 10.62 mm; Stage IV (Orbital abscess): no cases were observed. No cases of cavernous sinus thrombosis (Stage V) were identified in this series. Furthermore, no radiological evidence of intracranial complications, such as meningitis or intracranial abscess, was observed.
Isolated Pathogens and Associated Antibiotic Susceptibility and Management (N=8)
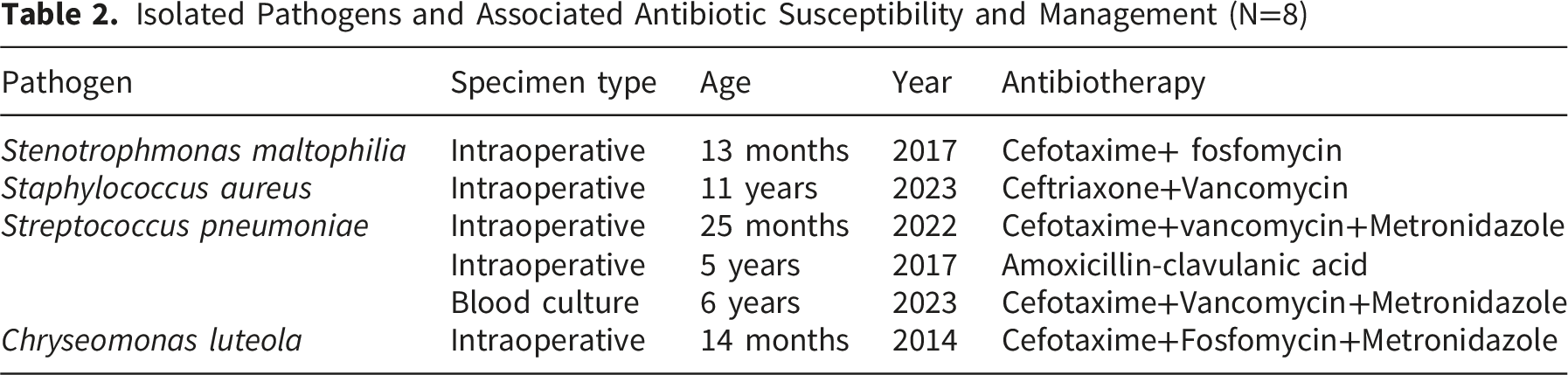
The isolated microorganisms included Streptococcus pneumoniae (n=3), Stenotrophomonas maltophilia (n=1), and Chryseomonas luteola (n=1). Additionally, one case of methicillin-resistant Staphylococcus aureus (MRSA) was identified. No pathogens were isolated from the remaining 2 samples.
All patients received intravenous (IV) empirical broad-spectrum antibiotic therapy, occasionally supplemented by adjuvant symptomatic treatment. The mean duration of IV therapy was 7,18 ± 4.07 days (range: 2–21 days). Treatment modification was required in 8 cases: 5 patients showed no clinical improvement after 48 hours of empirical therapy, and three experienced hypersensitivity reactions. Following clinical stabilization, patients were transitioned to oral antibiotics to complete a mean total treatment course of 15.87 ± 5.08 days (range: 7_30 days).
Surgical intervention was required in 11 patients (13.9%). All surgical cases underwent orbitotomy for the evacuation of purulent collections or SPOA. Regarding the five patients with palpebral abscesses, four showed complete resolution with medical therapy alone, while one required intervention following skin fistulization.
A univariate analysis was performed to identify clinical and biological predictors of the need for surgical management. The variables tested included age, sex, fever upon admission, C-reactive protein (CRP) levels, white blood cell count (WBC), and prior use of NSAIDs.
Age ≥ 5 years was the only factor significantly associated with a higher requirement for surgical intervention (p < 0.001). Patients requiring surgery were significantly older, with a mean age of 8.25 ± 3.7 years, compared to 3.36 ± 3.13 years for those managed exclusively with medical therapy. No statistically significant associations were found for the remaining parameters.
A favorable clinical outcome was achieved in all patients managed exclusively with medical therapy. The mean hospital stay for the entire cohort was 7.18 ± 4.07 days (range: 2_21 days).
Among the patients who underwent surgical intervention, corrugated drain (wavy blade) was typically removed within 48 to 72 hours postoperatively. One patient required revision surgery due to persistent symptoms following the initial procedure. Notably, there were no significant differences in the choice of antibiotic agents or the total duration of therapy between the surgical and non-surgical groups.
One patient experienced a delayed recovery postoperatively; further investigation revealed a concomitant odontogenic infection. Following targeted dental management, significant clinical improvement was observed.
The mean follow-up period was 16 months. Complete resolution without sequelae was achieved in the majority of surgically treated patients, with the exception of one case of persistent blepharoptosis.
Discussion
Orbital complications occur in 5% to 7% of acute rhinosinusitis cases, with the ethmoid sinus being the primary source in 43% to 100% of pediatric orbital cellulitis.1,3 In our series, we observed a marked reduction in admissions during the COVID-19 pandemic, a trend consistent with global reports. This decline likely mirrored the broader decrease in community-acquired respiratory infections, such as influenza and pneumonia, secondary to social distancing and enhanced hygiene measures.
Pediatric populations are significantly more affected than adults, with an incidence nearly 16 times higher (1.6 vs. 0.1 per 100,000). 4 Eviatar et al attribute this susceptibility to the immature bone structure and increased vascularization of the developing ethmoid, which facilitates bacterial colonization of the bony structures. 5 Furthermore, the thinness and natural dehiscences (such as the Zuckerkandl dehiscence) of the lamina papyracea provide a low-resistance pathway for the spread of infection into the orbital compartment.
Viral upper respiratory infections remain the most frequent precursor to acute ethmoiditis. 6 However, odontogenic sources must not be overlooked; Martinez et al reported that approximately half of the patients with odontogenic maxillary sinusitis also present with concomitant anterior ethmoiditis, 7 as seen in one of our patients who required dental intervention for clinical recovery. Structural factors, including nasal septal deviation, also contribute to impaired sinus drainage.
The role of NSAIDs remains a subject of debate. While Hsairi et al identified prior NSAID use as a potential risk factor for complications 8 evidence remains insufficient to definitively link them to a worsened prognosis in pediatric ear nose and throat infections. Nonetheless, the French Society of Otorhinolaryngology advises caution or avoidance of NSAIDs in acute ethmoiditis due to the 0.7% incidence of severe orbital or intracranial complications. 9
Acute ethmoiditis is often diagnosed only once it has “exteriorized” into the orbit, 10 making ophthalmological signs the most prominent clinical features. In our cohort, eyelid edema and erythema were the most frequent findings, mirroring the results of Anosike et al, who reported these signs in 95.9% and 77.7% of cases, respectively. 11
As emphasized by Rashed et al, the clinician must systematically screen for “red flag” symptoms, including painful or restricted ocular motility, proptosis, chemosis, impaired color vision, and relative afferent pupillary defects. 12 The severity of these signs typically correlates with the stage of progression. Notably, SPOA most frequently involves the medial orbital wall. It has been hypothesized that lamina papyracea osteitis during the acute phase plays a critical etiological role in the transition from cellulitis to a formal subperiosteal collection. 2
Orbital ultrasound is strongly recommended as firs-line imaging for its safety, especially for the pediatric population as it avoids the harms of ionizing radiation and for its low cost. 13 Others consider CT as the gold standard for children with ocular signs. In fact, CT is the key exam to confirm orbital involvement in ethmoiditis, to assess its severity especially to determine the volume SPOA and the involvement of the other sinuses and ultimately to help with differential diagnosis. 14 CT is recommended when ocular inflammatory signs persist for more than 24 to 48 hours after initial conservative management. 15 Identifying the causative pathogen is crucial for tailoring antibiotic therapy. It has been deduced that the samples taken during surgery are the most relevant and valuable. 16 The review of the literature showed that the pathogen most frequently identified was different from country to country. Streptococcus species were at the top of the list for the French, while Staphylococcus aureus was found most frequently by the Americans. 17 The old literature has recommended empirical antibiotherapy according to the most common pathogens given the relatively high mortality rates and sequelae at the time. 18 However, currently, and considering the increase of antibiotic resistance, it would be better to identify the pathogen and assess its antimicrobial resistance.
Orbital ultrasonography is strongly recommended as a first-line imaging modality due to its safety profile, particularly in the pediatric population, as it avoids exposure to ionizing radiation and remains cost-effective. 13 However, CT is frequently considered the gold standard for children presenting with ocular signs. CT remains the definitive examination to confirm orbital involvement in ethmoiditis and to assess disease severity, specifically in quantifying SPOA volume, evaluating multi-sinus involvement, and facilitating differential diagnosis. 14 Current guidelines recommend CT imaging when ocular inflammatory signs persist beyond 24 to 48 hours of conservative management. 15
In parallel, identifying the causative pathogen is essential to guide targeted antibiotic therapy. Evidence suggests that specimens obtained intraoperatively yield the most clinically relevant diagnostic value. 16 Literature reviews highlight significant geographical variations in microbial prevalence: Streptococcus species predominate in French cohorts, whereas Staphylococcus aureus is more frequently identified in American studies. 17 While historical literature advocated for broad-spectrum empirical antibiotherapy due to previously high mortality and morbidity rates, 18 the modern escalation of antimicrobial resistance necessitates a shift toward precise pathogen identification and susceptibility testing to optimize clinical outcomes.
The study by Coudert et al’s study involved intravenous treatment for 4 days followed by amoxicillin-clavulanate for approximately 8,5 days and the result was positive in all cases. 19
The study by Coudert et al. 19 reported successful outcomes in all cases using a protocol of four days of intravenous treatment followed by approximately 8.5 days of oral amoxicillin-clavulanate. For isolated preseptal involvement, the recommended duration of antibiotic therapy is seven days of amoxicillin-clavulanate, unless clinical findings or patient history dictate a more prolonged course. 20 Ideally, the transition to oral therapy should be guided by antimicrobial susceptibility testing. In the absence of an antibiogram, Bedwell et al. 21 recommend a 14-day course of either amoxicillin-clavulanate or clindamycin for post-septal cellulitis.
Regarding surgical management, a review of retrospective and observational studies by Cantone et al. 22 identified several key indicators for intervention: age over 9 years, visual impairment, ophthalmoplegia, proptosis, significantly elevated C-reactive protein (CRP), or hemodynamic instability. Furthermore, surgery is indicated for cases classified as stage III or higher according to the Chandler classification, or when there is a lack of clinical improvement after 48 to 72 hours of medical management.
To synthesize these surgical indications, Najarian et al. 23 emphasized that surgical drainage should be prioritized in patients older than nine years due to the higher prevalence of polymicrobial infections. Additional indications include frontal sinus involvement, which carries a substantial risk of intracranial dissemination, 23 and the presence of SPOA. Unlike medial collections, superior SPOAs are typically associated with more severe ophthalmological complications and larger abscess volumes 24
Conclusions
Orbital complications arising from acute ethmoiditis remain a significant concern in pediatric practice, particularly among children under five years of age. Our findings confirm that upper respiratory tract infections are the primary predisposing factor, with ophthalmological signs typically dominating the clinical presentation. Overall, clinical outcomes remain favorable when managed appropriately.
The most significant finding of this study highlights the efficacy of a conservative approach: initial medical management with broad-spectrum intravenous antibiotics is successful in the majority of cases, provided there is no immediate indication for surgery. Younger children (<5 years) are less likely to undergo surgery.
Tailoring treatment, from exclusive medical therapy for medial collections to prompt surgical drainage for complex cases, is essential to prevent permanent vision loss and life-threatening intracranial sequelae.
Footnotes
Acknowledgements
The authors have no acknowledgements to declare.
Ethical Considerations
Given the retrospective nature of the study and the absence of any data revealing the identity of the patients, approval from the ethics committee was not mandatory.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data available upon reasonable request from the corresponding author.