
Abstract
Orbital complications are the second most common complications of endoscopic sinus surgery (ESS), and orbital hematoma is the most frequent orbital complication. An orbital abscess is usually associated with rhinosinusitis, and a few cases of orbital abscesses occurring after orbital trauma have been reported. However, orbital abscess occurring after ESS is rare. Herein, we present a case of a right orbital abscess that developed after bilateral ESS, performed at an outside facility, and decreased vision in the right eye to light perception only. The visual loss persisted for 3 days, after which the patient was referred to our hospital for urgent management. The cause of abscess formation might have been an infected stagnant orbital venous hematoma that occurred as a complication of ESS. A defect in the right lamina papyracea and emphysema were confirmed on computed tomography. Orbital symptoms started immediately after ESS, and vision deteriorated to light perception only and lasted for 3 days, which was considered a high-grade risk factor for irreversible blindness by the ophthalmology team. Urgent endoscopic endonasal orbital decompression was performed to drain the orbital abscess, and maximal medical treatment was initiated, which included intravenous corticosteroids, intravenous broad-spectrum antibiotics, topical intranasal corticosteroids, irrigation, and topical antibiotic eye drops. Close follow-up assessments were performed by the infectious diseases team, and the ophthalmology team performed frequent orbital assessments. The patient recovered from blindness, which was an unexpected outcome.
Introduction
Orbital complications are the second most common complications of endoscopic sinus surgery (ESS), and orbital hematoma is the most frequent orbital complication.1,2 The overall risk of minor complications was found to be 5% and major complications was found to be 0.5% to 1%, and orbital hematoma was considered a major complication.3,4 Orbital hematomas can be arterial, which rapidly develops and appears intraoperatively or in the recovery room; the signs should be recognized immediately, or venous, which arises due to injury to vessels around the lamina papyracea and develops slowly; orbital signs appear within a few hours after surgery. 5 Growing orbital lesions, such as expanding hematomas, raise of intraocular pressure to a critical point, causing anterior eye globe displacement, optic nerve stretching, increased venous pooling, and decreased arterial flow until neuron degeneration occurs due to ischemia of the optic nerve, thus causing blindness. 5 In addition to the pressure effect of orbital hematoma on the optic nerve, a long-standing hematoma can transform into an abscess, most likely due to invasion by microorganisms from sinus mucosa through a bony defect of the orbital wall, causing further inflammation and edema and increasing the risk of cavernous sinus thrombosis. Orbital abscess occurring after orbital trauma and fracture has been mentioned in a few reports; however, its occurrence as a complication of ESS is considered rare. 6 Herein, we report a case of an iatrogenic orbital abscess that developed after ESS, decreasing vision to light perception only, with the successful restoration of vision after maximal medical treatment and urgent orbital decompression through an endonasal endoscopic approach after 3 days of visual loss.
Case Presentation
A 35-year-old woman who had undergone bilateral ESS to manage chronic rhinosinusitis 3 days ago at an outside facility visited our emergency department complaining of swelling of the right eye, severe right orbital pain, and visual loss in the right eye for 3 days. Orbital symptoms started to appear a few hours after ESS and progressed over time. The nasal packs were removed 1 day after ESS. On the third postoperative day, the orbital symptoms did not improve, and the surgeon consulted an ophthalmologist who advised urgent orbital decompression, for which she was immediately referred to our hospital. The patient had no other nasal symptoms such as nasal bleeding, discharge, or obstruction; neurological symptoms such as headache, loss of consciousness, seizures, or weakness; or constitutional symptoms. Past medical history was unremarkable for chronic illnesses, and no allergies were reported. The patient had no history of similar orbital complications. The patient was conscious and alert, and her vital signs were normal. Nasal examination revealed bilateral blood clots and dry crusts in the nasal cavity, with bilateral internal nasal splints but no discharge. The internal splints were removed. Oral examination results were normal. Orbital examination revealed proptosis of the right eye with periorbital swelling, ecchymosis, chemosis, tenderness, blood-tinged discharge at the medial canthus, and difficulty in opening the right eye. Examination by an ophthalmologist revealed normal vision, extraocular muscle (EOM) motility, fundus, and reactive pupil in the left eye, while the right eye had limited EOM motility in all directions, a semi-dilated nonreactive pupil, decreased vision corresponding to light perception only, and fundus examination could not be performed. The ophthalmologist documented that the patient had a high chance of developing permanent visual loss, even after surgical intervention. Blood tests revealed leukocytosis (white blood cell count: 25 × 109/L) and increased erythrocyte sedimentation rate (46 mm/h). The other parameters such as chemistry and coagulation profile were normal. Non-contrast computed tomography (CT) of paranasal sinuses (PNS) revealed increased attenuation of fat planes in the right periorbital area that extended to the extraconal intraorbital area along the medial rectus muscle and the orbital floor and was associated with multiple foci of air with a mass effect on the globe and mild proptosis. A bony defect in the right lamina papyracea was observed, and the right middle turbinate was absent. Bilateral partial opacification of all the sinuses was observed (Figure 1).
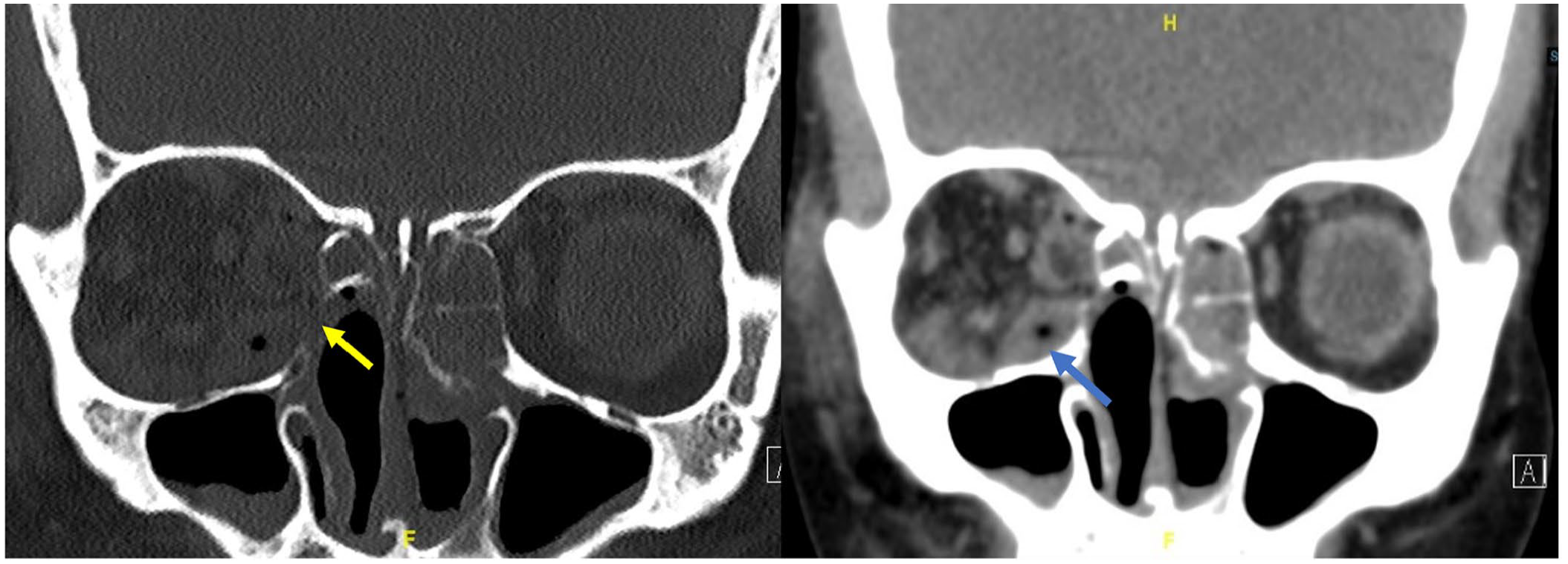
CT PNS coronal view, bone window image showing an iatrogenic defect in the lamina papyracea from previous ESS (yellow arrow). Coronal view soft tissue window showing inferomedial hypodense intraorbital lesion with surgical emphysema (blue arrow). CT, computed tomography; ESS, endoscopic sinus surgery; PNS, paranasal sinuses.
The patient was immediately admitted and started on intravenous dexamethasone (8 mg every 8 hours), ceftriaxone (1 g every 12 hours), metronidazole (500 mg every 8 hours), and paracetamol (1 g every 8 hours). In addition, saline nasal irrigation and intranasal steroid spraying were performed. Magnetic resonance imaging of PNS performed with gadolinium contrast revealed proptosis of the right eye associated with stretching and thinning of the right optic nerve, caused by the presence of inferior and medial orbital fluid collection, and periorbital fat edema, suggesting an orbital abscess (Figure 2). Urgent endoscopic endonasal orbital decompression was performed. Intraoperative nasal endoscopy revealed a disrupted anatomy, indicating an improperly performed ESS. The findings included an absent left inferior turbinate and right middle turbinate and a defect in the right lamina papyracea with exposed orbital fat. The nasal mucosa was inflamed and unhealthy with minimal purulent secretions. The surgery was initiated by performing a middle meatal antrostomy, anterior and posterior ethmoidectomy, and sphenoidotomy on the right side. The lamina papyracea was exposed along the medial orbital floor, and part of the medial orbital floor was drilled using an endoscopic cutting burr. A horizontal incision of the periorbita was made inferiorly and parallel to the medial rectus muscle, and a gush of frank pus was observed (Figure 3). The orbital abscess was drained by applying gentle eye pressure, and the pus was sent for culture. Proptosis of the right eye decreased; the orbital fat and muscles were preserved, and hemostasis was achieved. Intravenous vancomycin (1 g every 12 hours) was initiated after consultation with the infectious diseases team. The day after surgery, the orbital pain and swelling began to improve, but the headache persisted. Evaluation of the right eye revealed decreased proptosis and chemosis, a mid-dilated pupil, limited EOM motility in all directions, and improvement in vision to counting fingers. Gatifloxacin eye drops (3 drops every 4 hours) were administered. On the third postoperative day, right eye examination revealed 20/40+ visual acuity, a clear lens, minimal corneal edema, a flat retina and normal optic disc on fundus examination, limited motility in the upward gaze only, and mild conjunctival injection with subconjunctival hemorrhage. Gatifloxacin administration was discontinued, and treatment with maxitrol (neomycin/polymyxin/dexamethasone) eye drops (1 drop every 6 hours) was initiated. A pus culture revealed no bacterial growth, and the infectious diseases team discontinued vancomycin administration. Magnetic resonance venography of the brain performed 5 days after orbital decompression revealed no signs of cavernous sinus thrombosis. On the eighth postoperative day, the right visual acuity improved to 20/30+, with normal EOM motility in all directions, an intraocular pressure of 15 mmHg, a relative afferent pupillary defect +1, minimal subconjunctival hemorrhage, and no proptosis. On the 10th postoperative day, the patient improved clinically and discharged from the hospital with moxifloxacin eye drops (1 drop every 8 hours) for 1 week and oral Augmentin (amoxicillin/clavulanate) 625 mg every 8 hours for 10 days. After 2 weeks, the patient was following in the ophthalmology and the otorhinolaryngology clinics and showed no new symptoms or signs of orbital complications.
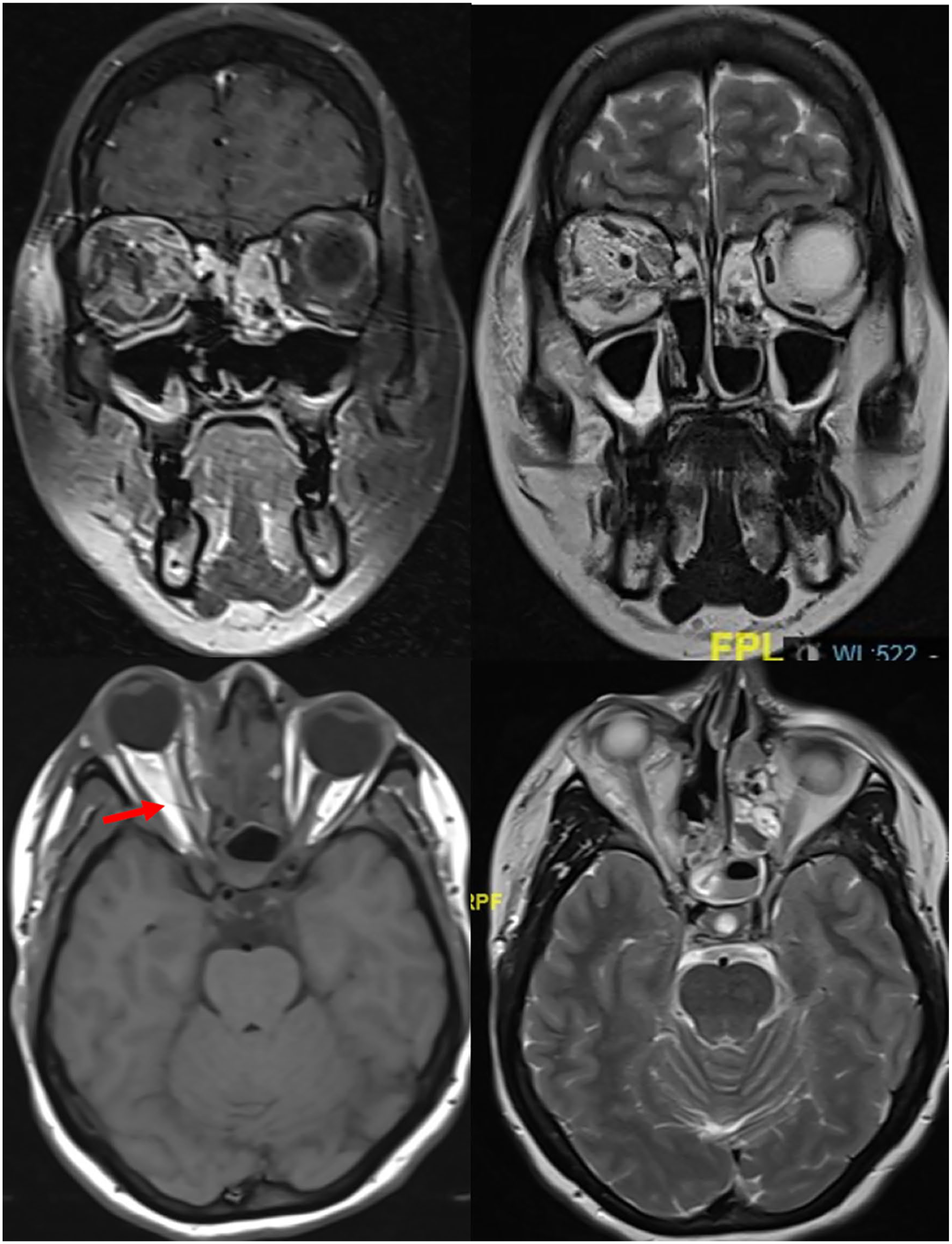
MRI PNS with contrast, coronal views showing a right inferomedial hyperintense collection in both T1 and T2 with rim enhancement on T1 with contrast. A right optic nerve thinning and stretching out in T1 and T2 axial views (red arrow). PNS, paranasal sinuses.
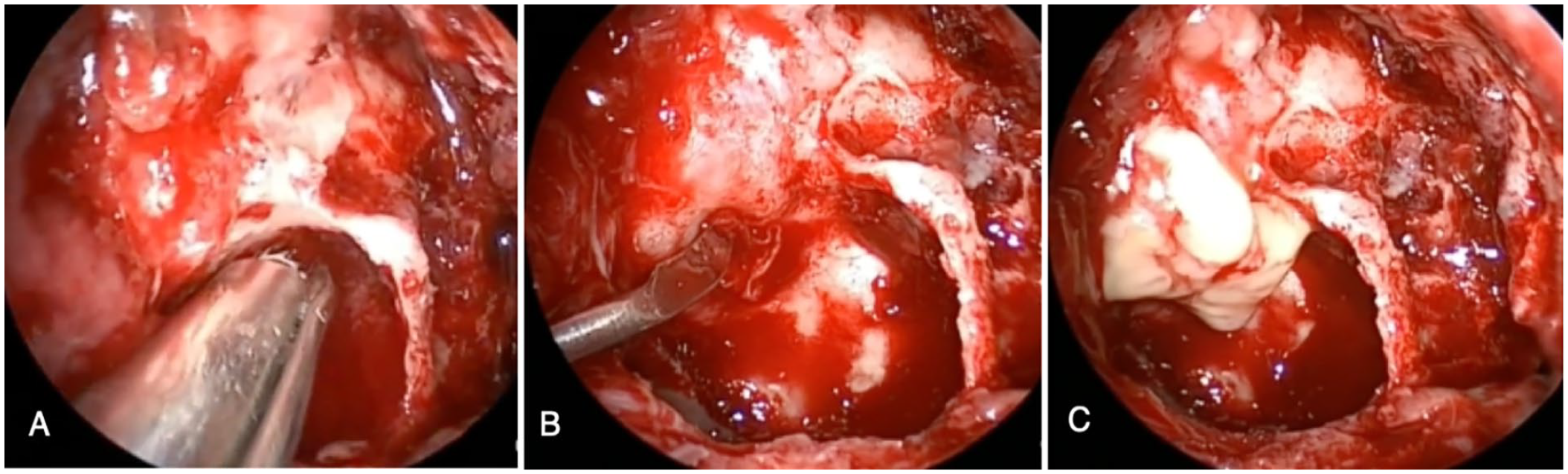
Showing pictures of intraoperative endoscopic endonasal orbital decompression. (A) Drilling of the medial orbital floor and the medial orbital wall and properly exposing the periorbita. (B) Incising the periorbita by a sickle knife to drain the orbital abscess. (C) Frank pus is seen coming out.
Discussion
Orbital complications are seen in 5% to 7% of patients with rhinosinusitis and are mostly related to acute rather than chronic rhinosinusitis and commonly present in the pediatric population. 7 According to one study, 81% of adult patients diagnosed with orbital complications secondary to chronic rhinosinusitis had a history of sinus surgery, and 61% had radiological evidence of lamina papyracea dehiscence associated with the previous surgery, a finding likely to be associated with orbital complications. 7 Few cases of orbital abscess development after facial trauma, either through infected external wounds or orbital bone fractures, and rarely after ESS, have been reported. 6 In the present case, the patient had an iatrogenic injury of the lamina papyracea, causing post-septal orbital hematoma that progressed to an orbital abscess within 3 days. Risk factors for orbital injury during ESS are varied and include poor surgical skills, revision surgery, extent and severity of the disease, and anatomical variations. 2
The most common organisms causing orbital cellulitis or abscesses are those causing acute and chronic sinusitis, including Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus, and anaerobic bacteria (Prevotella, Porphyromonas, Fusobacterium, and Peptostreptococcus spp.), and antibiotic treatment should be directed accordingly. In the present case, the pus culture was negative, and antibiotics were chosen by the infection diseases team. 8 Many studies have found no benefit of using prophylactic antibiotics in cases of uncomplicated sinusitis after uneventful ESS in medically free patients, as no difference in postoperative endoscopic scores or rates of infection in comparison to placebo was observed. However, the authors recommend using prophylactic antibiotics in pediatric cases and cases of cystic fibrosis, pregnancy, complicated sinusitis, active sinus infection, fungal ball, intraoperative complications, and nasal pack insertion.9,10 The present patient reported that her previous surgeon had prescribed prophylactic antibiotics after ESS. However, these antibiotics did not prevent orbital abscess transformation, suggesting that the abscess developed due to the direct spread of microorganisms from infected sinus mucosa through the medial orbital wall defect. Another mechanism hypothesized in a study on orbital cellulitis secondary to orbital floor fractures was that infections could develop secondary to trauma to the infraorbital vessels, affecting the blood supply of the inferior orbital fat and predisposing the area to anaerobic growth, facilitating cellulitis. 11
Early evaluation of orbital symptoms and signs after ESS is important to prevent the risk of blindness, especially in cases of arterial retrobulbar hematoma, which can increase intraocular pressure within minutes. Additionally, an experimental model study was conducted to test the tolerance of neurons in the retinal ganglion cell layer of the optic nerve according to different volumes and durations using a simulation model of an expanding retrobulbar lesion reaching a critical point. This study demonstrated that duration of more than 90 minutes increased the risk of neurodegenerative changes in the retinal ganglion cell layer and optic nerve by 48.3%. 12 Timing of surgical management of an orbital abscess is crucial to avoid the risk of irreversible blindness and the catastrophic outcome of cavernous sinus thrombosis. A study on the risk factors of irreversible blindness, which was defined as only light perception or no light perception in the affected eye, in patients with surgically treated orbital complications of PNS infection, has shown that the timing of surgical management is crucial and if the surgery is delayed by more than 2.5 days after the onset of orbital symptoms, irreversible blindness can occur. 13 They also investigated patient health status variables, such as immunosuppression, diabetes mellitus, chronic renal failure, cancer, and any other comorbidities affecting the immunological condition, which were regarded as additional risk factors. The results showed that surgically treated patients with orbital complications of rhinosinusitis and at least 1 additional risk factor had 1.683 times the risk of irreversible blindness compared with patients without any risk factors. 13 The duration of visual loss in the present patient exceeded this limit (3 days), and the ophthalmology team considered her to be at high risk of irreversible blindness. However, the vision recovered after maximal medical and surgical treatment, which was an unexpected outcome.
Conclusion
Iatrogenic orbital hematoma is considered a major complication of ESS and can be avoided by studying preoperative CT PNS images, respecting surgical landmarks during ESS, providing adequate training in ESS, and managing complications. Untreated orbital hematoma can transform into an orbital abscess, which is an uncommon complication of ESS. An orbital abscess is managed by urgent orbital decompression through an endonasal endoscopic approach and medical treatment, and the timing of management is very crucial to preventing permanent blindness.
Footnotes
Consent for publication
There are no identifiable data through the figures or research information in this article and informed consent is not applicable.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declare
We declare that this article is original, have never been published, or under the consideration for publication elsewhere (in part or in whole). We also declare that the corresponding author and all the coauthors have actively participated in this article. There is no Arabic abstract and Arabic article for this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.