
Abstract
Objective:
Glucagon-like peptide 1 receptor agonists (GLP-1 RAs) are a rapidly proliferating class of drugs used for diabetes and obesity management. Their use poses several implications for ear, nose and throat (ENT) surgeons, including high-risk airway surgery considerations. This review highlights pharmacological mechanisms, ENT-specific side effects and perioperative challenges.
Methods:
A narrative review was performed with comprehensive literature search across PubMed and Google Scholar (2000-2025). International anaesthetic, surgical and endoscopic guidelines were reviewed and synthesised to compare management strategies.
Results:
GLP-1 RAs function to regulate glucose, reduce appetite and slow gastric emptying, increasing aspiration risk during airway surgery. ENT clinical implications include patulous eustachian tube dysfunction, nasopharyngitis and improvement in sleep apnoea and emerging sinus surgery outcomes. Pre-clinical data suggest a theoretical medullary thyroid cancer risk. Despite endoscopy data showing increased residual gastric content, no studies specifically address risks in airway surgery. Peri-operative guidelines vary, and this review reports the range of recommendations from major international anaesthetic organisations.
Conclusion:
ENT surgeons must recognise GLP-1 RA associated risks, especially during tubeless airway surgery. An individualised, team-based approach may be necessary for patients, as current guidelines do not reach consensus. ENT side effects of eustachian tube dysfunction, and theoretical risk of medullary thyroid cancer still needs further investigation.
Keywords
Introduction
Glucagon-like peptide 1 receptor agonists (GLP-1 RAs) are a relatively novel class of drugs used to treat type 2 diabetes mellitus (T2DM) and obesity. While available for T2DM since 2005, their 2014 approval for obesity and recent surge in public profile have led to a significant increase in the surgical patients presenting on these medications.1,2 Common prescriptions include semaglutide (Ozempic, Wegovy), liraglutde (Saxenda, Victoza) and tirzepatide (Mounjaro).
Although offering substantial metabolic and overall health benefits, they present significant perioperative implications. Significantly, GLP-1 RAs can cause increased risk of pulmonary aspiration during routine general anaesthesia due to delayed gastric emptying. 3 For ear, nose and throat (ENT) surgeons, this risk is compounded during procedures involving the shared airway, including tubeless airway surgery using trans-nasal humidified rapid-insufflation ventilatory exchange (THRIVE). At present, there are no studies assessing patients on GLP-1 RAs undergoing tubeless airway surgery, and the implications peri-operatively.
Beyond perioperative safety, a growing body of literature – currently limited to preclinical, case series and observational data – suggests several ENT-related issues associated with GLP-1 RA use. These effects range from therapeutic benefits in obstructive sleep apnoea (OSA) to potential adverse associations with medullary thyroid cancer, patulous eustachian tube dysfunction and chronic nasopharyngitis. For the ENT surgeon, recognising these associations is essential for patient counselling and diagnosis in the context of GLP-1 RA use.
This narrative review aims to consolidate current evidence regarding the ENT-specific side effects of GLP-1 RAs and provides a critical appraisal of perioperative management strategies to guide ENT surgeons in optimising patient safety and patient counselling on ENT-specific clinical implications and side effects.
Methods
A comprehensive search was performed using PubMed and Google Scholar to identify studies published between January 2000 and 2025. The search strategy employed specific keywords, including “GLP-1RA AND otolaryngology,” “GLP-1RA AND perioperative risk,” “GLP-1RA in Ear, Nose and Throat Surgery,” “GLP-1 RA and pulmonary aspiration,” “GLP-1 RA and airway surgery.”
Given the paucity of randomised controlled trials in this field, all studies and systematic reviews were included such as case reports, large retrospective cohort studies, and pre-clinical data if they reported clinical outcomes. Non-English articles were excluded. Additionally, current perioperative guidelines from major international anaesthetic and surgical organisations were also screened and compared. References from relevant articles and guidelines were manually reviewed and incorporated. The methodology followed and articles included have been summarised in Figure 1.

Narrative review flow diagram regarding perioperative risk management and clinical implications of GLP-1 RAs. GLP-1 RA, glucagon-like peptide 1 receptor agonist.
As a narrative review, the identified literature was summarised to highlight emerging clinical trends and practice considerations.
Results and Discussion
GLP-1 RA Mechanism of Action
Incretins are peptide hormones secreted under neural control by the gastrointestinal lumen in response to eating, especially carbohydrate-rich food. 4 The 2 primary incretins linked to glucose homeostasis and satiety are GLP-1 and glucose-dependent insulinotropic polypeptide (GIP).5,6
Incretins target GLP-1 receptors which are widely distributed throughout the body including gastrointestinal tract, cardiac, adipose and neural tissues. 5 Physiologically, they both stimulate insulin production, suppress glucagon secretion, reduce appetite and slow gastric emptying. 6 Physiological GLP-1 and GIP have a short half-life, undergoing rapid inactivation by the enzyme dipeptidyl peptidase-4 (DPP-4) within 2 minutes of secretion.4,5
GLP-1 RAs are engineered to resist DPP-4 degradation and have low renal clearance, resulting in a significantly prolonged duration of action. 7 The glucose lowering effects of GLP-1 RAs result from manipulation of gastric emptying, rather than the effect on pancreatic secretion. 7 Therefore, in the perioperative context, the risk of hypoglycaemia while on GLP-1 RAs during fasting is extremely low as GLP-1 only functions during a hyperglycaemic state. 8
By delaying gastric emptying and inhibiting gastric acid secretion, GLP-1 RAs increase postprandial gastric volumes.1,9 This inhibition is dose-dependent and varies based on the frequency and duration of drug exposure.7,10 Evidence suggests that gastric emptying tachyphylaxis may occur 8 to 12 weeks after commencing therapy, particularly with longer-acting formulations.11,12 This can result in normalisation of gastric emptying. Despite this potential adaptation, the persistence of delayed emptying remains a primary perioperative concern.
Indications
Currently, T2DM is a globally recognised indication for all GLP-1 RAs and the dual GLP-1/GIP agonist tirzepatide. As of late 2025, liraglutide and semaglutide are the specific agents approved for weight management in patients with a body mass index (BMI) >30, or a BMI >27 with weight-related comorbidities. 2 Table 1 presents a summary of available GLP-1 RAs and dual GLP-1/GIP agonist indications and pharmacology overview internationally.
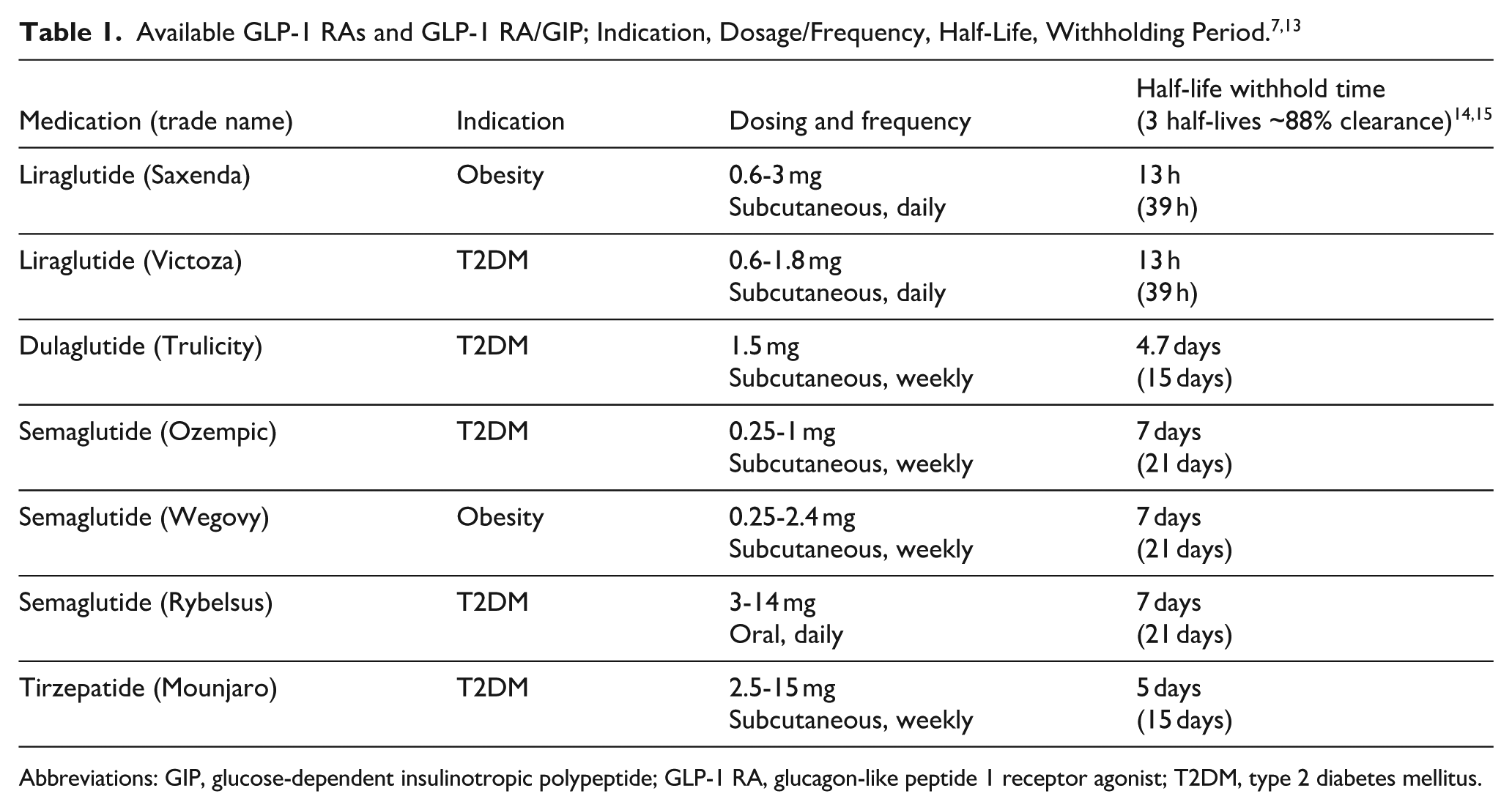
Abbreviations: GIP, glucose-dependent insulinotropic polypeptide; GLP-1 RA, glucagon-like peptide 1 receptor agonist; T2DM, type 2 diabetes mellitus.
ENT Clinical Implications and Side Effects of GLP-1 RAs
Obstructive Sleep Apnoea
GLP-1 RAs improve the apnoea-hypopnoea index (AHI) in patients with OSA for several reasons.16,17 Weight loss after commencing GLP-1 RAs improves OSA. GLP-1 receptors are also found in the central nervous system including in areas involving respiratory control and can influence respiratory patterns enhance respiratory drive and may have a direct action in altering tone of upper airway muscles. 17
A large, longitudinal double-blind randomised, multi-centre study phase 3 SURMOUNT-OSA compared tirzepatide to placebo in OSA. 18 This study of obese patients with moderate-to-severe OSA found that AHI decreased significantly in the GLP-1 RA group when compared with placebo. There is strong evidence supporting the safety and efficacy of GLP-1 RAs in OSA management, which may suggest reduced surgeries for OSA management is possible with increased GLP-1 RA use. 19
GLP-1 RAs are also being considered for use as neoadjuvant and adjuvant therapy prior to sleep surgery. 20 Cheong and Pang in their Viewpoint article have suggested that surgical interventions especially hypoglossal nerve stimulation have poorer perioperative outcomes for obese patients, and the use of GLP-1 RAs pre- and post-operatively may enhance surgical efficacy, reduce perioperative risks and improve patient outcomes, in which at this stage, remains conjecture as there are limited published clinical trials. 20
Thyroid Cancer
GLP-1 RAs should be avoided in patients with a family or personal history of multiple endocrine neoplasia type 2-associated medullary thyroid cancer. Although not observed in human studies, preclinical observations have linked sustained GLP-1 receptor agonism to development of C cell hyperplasia and medullary thyroid cancer in rats and mice.5,21 Khan et al, suggest that there is a high proportional reporting ratio for both medullary and papillary thyroid cancer in patients using all GLP-1 RAs; however, this cannot estimate incidence. 21 The rarity of the outcome and potential for stimulated reporting may inflate signal magnitude.
GLP-1 receptors are present on papillary thyroid cancer cells. 22 Brito et al retrospectively reviewed 41 110 patients on GLP-1 RAs from an American database and found an elevation of new thyroid cancer diagnoses within first year of GLP-1 RA initiation with a hazard ratio of 1.85. 23 However, this was attributed to detection bias as more people had thyroid ultrasounds when on GLP-1 RA therapy than those who were not on GLP-1 RA therapy.23,24 Although, there is established preliminary data showing no significant association of GLP-1 RAs with thyroid cancer in humans, it is limited to large database retrospective studies which are subject to biases.
Eustachian Tube Dysfunction
Rapid weight loss is associated with loss of Ostmann’s fat pad around the Eustachian tube opening, resulting in a patulous Eustachian tube and symptoms including autophony, aural fullness and tinnitus. 25 Sudhoff and Pak et al have reported several cases of patulous eustachian tubes within a few months of commencing GLP-1 RAs.25,26 The current evidence is limited to anecdotal reporting. ENT surgeons should incorporate questions about GLP-1 RA use when evaluating patients with unexplained autophony or aural fullness and can commence early conservative intervention with nasal emollients. 25
Rhinosinusitis
There is limited evidence regarding GLP-1 RAs causing sinusitis, but a common side effect of most GLP-1 RAs is nasopharyngitis. 27 This has not usually led to discontinuation of the drug, and is most significantly associated with exenatide (reporting odds ratio 1.47). 21 Hoying et al found in their high-powered retrospective study that GLP-1 RA users have significantly decreased rates of revision sinus surgery within the first year (risk ratio of 0.6) and decreased prescription of first-time biologics within 5 years (risk ratio 0.72). 28 The main mechanism proposed was likely due to weight loss, given weight loss has been shown to improve asthma, and asthma and sinusitis are closely related; however, another proposed mechanism was possibly through anti-inflammatory effects of interleukin-33. 28 However, larger controlled studies are lacking in this area; therefore, definitive causality cannot be determined.
Perioperative Risk of GLP-1 RAs
Delayed gastric emptying in patients using GLP-1 RAs is a major perioperative concern due to the increased risk of pulmonary aspiration during anaesthesia. Pulmonary aspiration is the most common cause of anaesthesia-related mortality, accounting for 1 in 3000 to 4000 elective procedures. 29 Complications following an aspiration event include acute respiratory failure, multi-organ failure, prolonged hospital stay, possible intensive care unit admission and death.3,30
Several factors increase the likelihood of aspiration including increased residual gastric volume, reduced lower oesophageal sphincter tone and suppressed upper airway reflexes. 31 As the lower oesophageal sphincter and upper airway reflexes are both suppressed during anaesthesia, any risk from residual stomach volume is usually mitigated by requiring patients to fast pre-operatively. 9 There are certain patient factors that increase the risk of aspiration including history of gastro-oesophageal reflux, hiatus hernia or meal-related factors.9,30,32 -34 The anaesthetic factors that affect aspiration include use of propofol, opioids, volatile agents, reduced depth of anaesthesia, supraglottic airways, positive pressure ventilation duration of surgery greater than 2 hours and difficult intubation.35,36
Delayed gastric emptying can result in residual gastric contents even after fasting according to standard fasting guidelines.35 -40 Patient factors can also compound delayed gastric emptying such as obesity, older age, gastroparesis associated with T2DM, or previous foregut surgery. Medications that further slow gastric emptying include opioids, beta blockers, calcium channel blockers, anticholinergics, antacids, neurological and psychiatric medications, progesterone, and octreotide.8 -10,30,41 -43 Thus, the above factors can further compound residual gastric content for patients taking GLP-1 RAs.
There is a well-established direct correlation between residual gastric content volume and risk of pulmonary aspiration. 9 A myriad of lower quality evidence studies, mainly case reports and retrospective chart reviews have explored the relationship of GLP-1 RAs to residual gastric content and risk of progression to pulmonary aspiration under anaesthesia.
Retained gastric content is significantly higher in patients taking GLP-1 RAs and is independent of other confounders that could slow gastric motility.40,42 Persistent digestive symptoms while taking GLP-1 RAs were also positively correlated with higher residual gastric content.1,9 Most GLP-1 RAs have a half-life between 5 and 7 days, meaning ~88% of clearance of the drug can take up to 3 weeks to achieve (Table 1).14,15 Therefore, to return the delay in gastric emptying to normal, GLP-1 RAs would theoretically have to be withheld for 3 to 5 weeks which may not be feasible, especially when prescribed for glycaemic control. 29
A high-powered retrospective database study by Yeo et al, examined 20099 GLP-1 RA user undergoing upper gastrointestinal oesophagoscopy (UGIE) and found a higher incidence rate of aspiration pneumonia. 44 In comparison, Chen et al and Dixit et al both performed high-power retrospective chart reviews on large patient cohorts comparing GLP-1 RAs users with non-users undergoing 1 of 14 common surgeries and emergency operations.45,46 Neither study found an association between GLP-1 RA use and post-operative respiratory complications.45,46 While there appears to be strong established and reproducible data to suggest that GLP-1 RAs are associated with increased retained gastric contents, there is mixed evidence from low-quality studies to suggest a reliable association with increased pulmonary aspiration.30,42 As such, some professional anaesthetic bodies are recommending against withholding GLP-1 RAs prior to surgery, even for higher aspiration-risk procedures such as UGIE and airway surgery with key studies outlined in Table 2. 39 Recent guidelines suggest use of other mitigating strategies.39,47 -49
Summary Table of Key Studies and Findings That Have Informed Current Peri-Operative Management Guidelines for GLP-1 RAs in Chronological Order.

Abbreviation: GLP-1 RA, glucagon-like peptide 1 receptor agonist.
Current Anaesthetic Guidelines for Perioperative Management of GLP-1 RAs
All international anaesthetic guidelines currently recommend individual assessment of patient risk factors prior to advising any patient about GLP-1 RA use prior to anaesthesia. Airway status has also been considered in a selection of guidelines, particularly in the context of the unprotected airway in endoscopic procedures.
The 2025 Australian and New Zealand College of Anaesthetists (ANZCA) guidelines for periprocedural use of GLP-1/GIP RAs recommend not withholding GLP-1/GIP RAs due to risk of hyperglycaemia in T2DM and compromising weight control. 39 This was a significant change from the 2024 guidelines in which the evidence base was considered insufficient to support withholding GLP-1 RAs. 50 Currently, the ANZCA recommendations are:
Clear fluid diet for 24 hours prior to procedure
6-hour fast pre-procedure
If a clear fluid diet is not followed, multiple risk mitigation strategies are recommended including gastric ultrasound, intravenous erythromycin, proceeding with rapid sequence induction, or deferring the procedure.
Similarly, the American Society of Anaesthesiologists (ASA) have similar guidelines and recommend patients without other risk factors for aspiration continue GLP-1 RAs in the perioperative period. 51 The ASA recommends that patients with an increased risk profile should use a liquid diet for at least 24 hours prior to procedure, or withhold medication on the day of surgery for daily formulations or a week before surgery for weekly formulations. 51
Anaesthetists of Great Britain and Ireland not only recommend continuation of GLP-1 RAs but also suggest use of peri-operative techniques to mitigate risk of pulmonary aspiration. 52
The European Journal of Anaesthesiology has suggested the importance of an individualised perioperative management plan. 53 However, they have not made any suggestions regarding withholding or continuing GLP-1 RAs pre-operatively.
In contrast, the Canadian Anaesthetics guidelines and Royal Australasian College of Surgery have suggested to withhold GLP-1 RAs for 3 half-lives prior to a procedure to allow for ~88% clearance and regain normal gastric emptying function.14,15 However, both recommendations have not been updated since early 2024.
Periprocedural Risk Mitigation Strategies for Patients Taking GLP-1 RAs
Gastric ultrasound has been suggested for pre-operative assessment of residual gastric contents as per systematic review completed by Van de Putte and Perlas. 54 The disadvantages are that it is user dependent and requires training. 55 Additionally, gastric ultrasound findings have only been validated in patients with normal gastric anatomy, and thus estimating gastric content in patients with structural abnormalities such as previous lower oesophageal or gastric surgery may not be reliable. 56
There is significant established evidence including systematic reviews and large retrospective studies regarding the ANZCA guidelines for a 24-hour clear fluid diet prior to surgery. Systematic reviews have shown that smaller retained gastric volumes are seen in patients with a combined UGIE and colonoscopy than UGIE alone for patients using GLP-1 RAs.42,43,47,49 This is attributed to the required longer fasting periods for solid food such as 24-hour liquid diet and the required bowel prep.
Erythromycin induces effective, propulsive antral motility in health and disease states and promotes emptying of non-digestible solids from the stomach. 57 Meier et al performed a study on 9 healthy males showing the efficacy of erythromycin in reversing the delayed gastric emptying of GLP-1 RAs. 58 This study, however, does not assess the efficacy of erythromycin in patients who have been prescribed GLP-1 RAs, who often have compounding factors for delayed gastric emptying such as T2DM. Support for erythromycin use to hasten gastric emptying for GLP-1 RA users as evaluated by gastric ultrasound, is limited to anecdotal evidence from a single case report by Sidhu. 59
Use of rapid sequence induction to mitigate aspiration risk during general anaesthetic for routine elective procedures is not always suitable during airway surgery which may require a tubeless field for access.
ENT Airway Surgery and Anaesthetic Considerations
The THRIVE anaesthetic technique introduced in 2015 is popular method for tubeless oxygenation and ventilation of a patient during airway surgery. 60 The technique involves intravenous anaesthesia and allows for either spontaneous breathing or prolonged apnoea supported by high flow nasal cannula. The humidified high flow of gas provides a low level of PEEP and reduces hypercapnia.60 -62 Using this technique, there is an uninterrupted surgical field, and reduced time from induction to laryngoscopic suspension, and decreased overall surgical time. 62
To date no studies have specifically addressed the impact of GLP-1 RAs on airway surgery with or without THRIVE. Additionally, the data discussed above is in relation to upper endoscopy/colonoscopy as most studies assessing GLP-1 RA aspiration risk has been undertaken in these patients to also quantify residual gastric content. As previously discussed, some of the risk mitigation strategies for GLP-1 RA users such as rapid sequence induction may not be possible for airway procedures, where an endotracheal tube limits surgical access and visibility. Additionally, upper endoscopies may be aborted due to direct visualisation of residual gastric content which is not possible in airway surgery, until regurgitation and aspiration of gastric contents have occurred. 42 Propofol sedation during upper endoscopy has been associated with an increased risk of aspiration due to impaired airway protection reflexes, which is important to note given its frequent use in THRIVE procedures. 44 Figure 2 describes recommended risk mitigation strategies for anaesthetists and ENT surgeons performing tubeless airway surgery based on this narrative review.

Recommended flow chart for GLP-1 RA patients undergoing tubeless airway surgery. This decision-making tool is based on the current narrative literature review. Authors recommend clinicians consult local professional and institutional guidelines as further updates become available. GLP-1 RA, glucagon-like peptide 1 receptor agonist; pre-op, pre-operatively; T2DM, type 2 diabetes mellitus.
Limitations
This review is limited by its narrative design and potential selection bias; however, the purpose of this review was to gain awareness and clarity of the current guidelines of GLP-1 RAs in ENT surgery, their effect specifically on tubeless airway surgery, and adverse effects causing clinical implications for ENT surgeons. Given the current literature is largely limited to preclinical data, case reports and large retrospective observational studies with minimal randomised controlled trials available, this narrative review serves as the best consolidated summary of evidence to date. Future higher-quality studies are necessary to help inform best practice.
Conclusion
GLP-1 RAs are increasingly popular, and ENT surgeons need to be aware of their significant perioperative implications. While beneficial for OSA management and improving rates of revision sinus surgery, the risk of medullary thyroid cancer and patulous eustachian tube dysfunction still need further investigation. An individualised approach may be necessary for patients who are taking GLP-1 RAs and undergoing tubeless airway surgery as the current evidence stems from observational studies for patients undergoing upper endoscopy. However, risk mitigation strategies with longer fasting times, gastric ultrasound and erythromycin use may provide options for proceeding with tubeless airway surgeries for GLP-1 RA users.
Footnotes
Ethical Consideration
Ethical approval was not required for this article as it is a review paper. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are embedded in manuscript as secondary research.