
Abstract
Recurrent respiratory papillomatosis (RRP) is characterized by benign papillomatous lesions of the respiratory tract, most commonly involving the larynx. Cases of RRP originating solely from the nasopharynx are rarely reported in the literature. To our knowledge, this is the first reported case of nasopharyngeal RRP causing secondary Eustachian tube dysfunction (ETD) managed by office-based laser excision. We describe a 68-year-old male with a history of nasopharyngeal RRP. The papilloma’s location resulted in diminished hearing, tinnitus, and an intermittent ear-popping sensation, findings consistent with ETD. Flexible laryngoscopy revealed a papillomatous lesion on the right torus tubarius completely obstructing the Eustachian tube. Office-based flexible laryngoscopy with laser excision was performed without the need for sedation or operating room resources. Following excision, the patient experienced resolution of symptoms. This case demonstrates the feasibility of office-based laser excision for select cases of nasopharyngeal RRP involving the torus tubarius. Compared with operative management, this approach may offer potential advantages, including reduced healthcare costs, avoidance of general anesthesia, and the ability to perform real-time functional assessment. Further study is needed to evaluate the role of office-based techniques in the management of extralaryngeal RRP.
Keywords
Introduction
Recurrent respiratory papillomatosis (RRP) consists of benign exophytic lesions that arise along the respiratory tract, most commonly involving the larynx, and represents a rare manifestation of human papillomavirus infection.1,2 Symptoms usually include dysphonia, stridor, cough, and dyspnea. 3 At the moment, there is no curative treatment for RRP. For this reason, the management is often based on symptoms and revolves around surgical excision or ablation. 4 Extralaryngeal locations of RRP are rare. 1 However, patients can present with RRP in other areas of the respiratory tract, such as the nasopharynx or the lungs.5,6 Symptomatic RRP of the nasopharynx is often treated with surgical excision in the operating room, but this creates new patient expenses, requires additional resources, and introduces new potential for anesthesia-related complications. The following case describes a novel office-based approach to managing nasopharyngeal RRP at an anatomically challenging site that had contributed to the development of Eustachian tube dysfunction (ETD).
Case Summary
The patient was a 68-year-old male with a known history of RRP who presented to his otolaryngologist with progressive symptoms of exertional dyspnea, decreased hearing, tinnitus, and intermittent aural fullness. The patient endorsed an ongoing tobacco use history of approximately half a pack per day. In the clinic, a flexible nasolaryngoscopy was performed and revealed an expanding solid mass arising from the right torus tubarius, consistent with prior findings. Clinical examination further demonstrated new evidence of a right-sided otitis media with effusion.
During the past 10 years, the patient had developed multiple papillomatous lesions involving the right nasopharynx, torus tubarius, and soft palate, with no evidence of malignant transformation on pathology. In addition to the presenting symptoms, these prior lesions had contributed to a history of dysphagia with episodes of liquid aspiration and recurrent epistaxis provoked by coughing or sneezing. In this case, the proximity of the lesions to the orifice of the Eustachian tube would typically warrant management in the operating room due to the anatomical challenge of accessing the site in the clinic setting. However, an office intervention was proposed to the patient, as this would avoid the unnecessary risk associated with operative management under general anesthesia without compromising patient safety or symptomatic relief. With the patient agreeable to the plan, the patient was seated in the exam chair, and the nasopharynx was anesthetized with 4% lidocaine/Afrin/Cetacaine under laryngoscopic guidance. A TrueBlue laser, a blue light (BL) laser with a wavelength of 445 nm, was threaded through the side channel of the laryngoscope and placed 2 to 3 mm above the lesion. The laser was set to 10 watts and pulsating mode with 40 ms on and 300 ms off and directed at the vasculature of the papilloma to achieve angiolysis. Once the lesion appeared blanched with whitening of the epithelium, the laser was used in contact mode to induce coagulation necrosis;. then, the lesion was debulked with cup forceps. The nasopharyngeal orifice of the Eustachian tube was visually patent at the end of the laryngoscopic procedure (Figures 1 and 2). The patient tolerated the procedure well, with excellent hemostasis and no complications. The patient had immediate improvement in his symptoms and was able to return home following the in-office procedure. Histopathological analysis indicated an atypical papilloma with low-grade dysplasia. HPV subtyping and immunohistochemical analysis were not performed in this case.
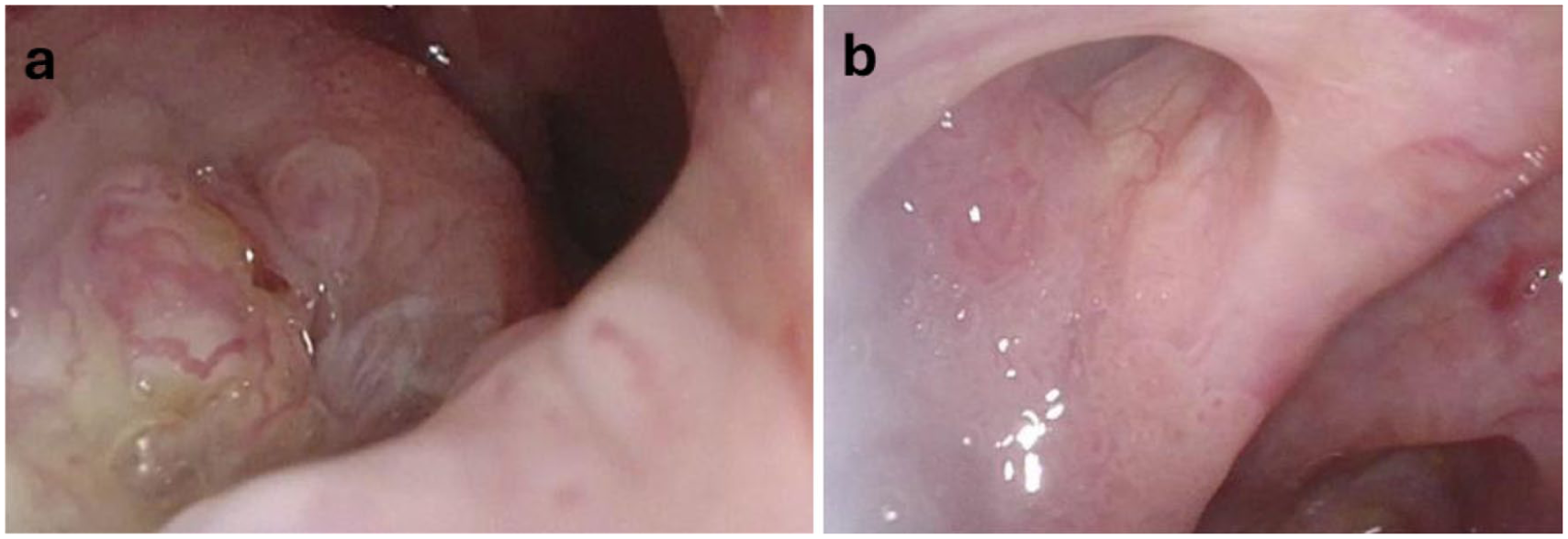
BL laser excision resulted in removal of the papilloma that blocked the right Eustachian tube and relieved the obstruction as seen. (a) Papilloma is visualized obstructing the right Eustachian tube through flexible laryngoscopy. (b) After BL laser therapy, the right Eustachian tube is patent when visualized by flexible laryngoscopy. BL, blue light.
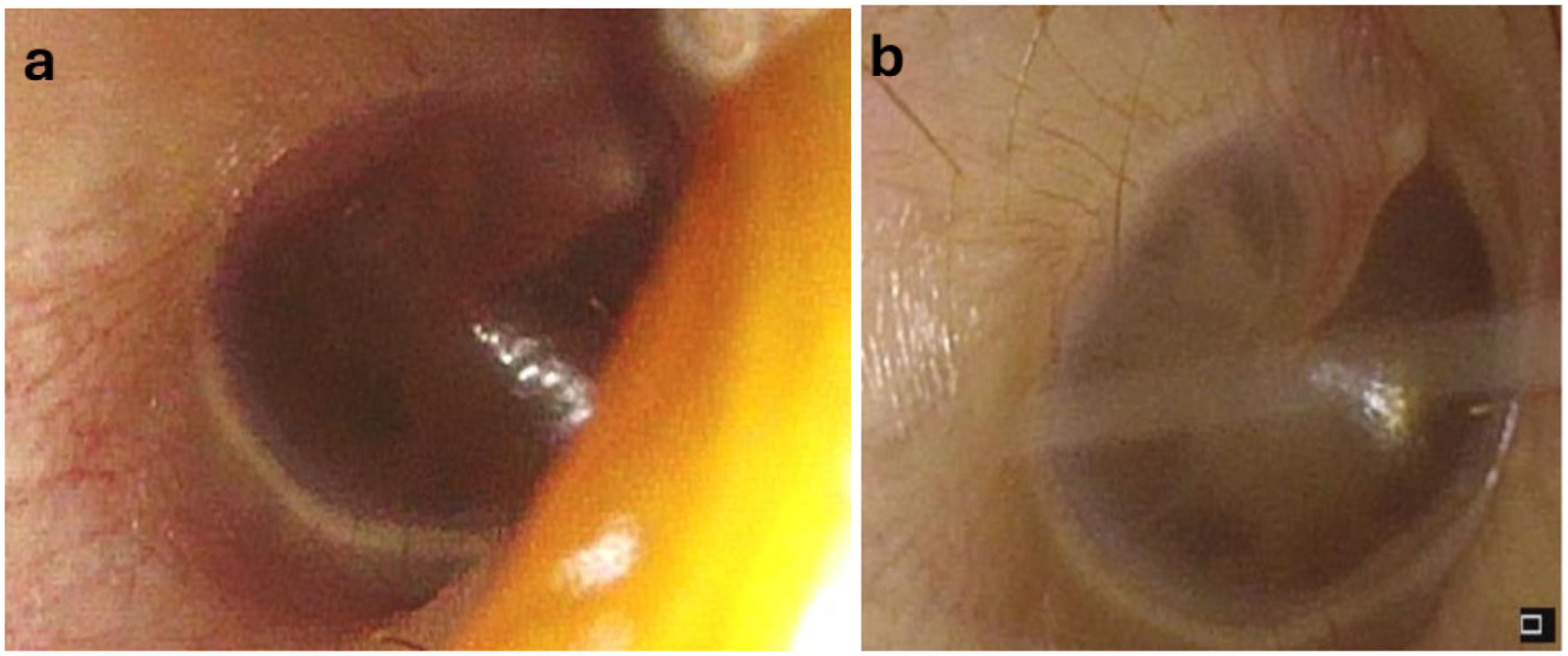
BL laser therapy led to the resolution of ETD. (a) Otoscopic exam demonstrated otitis media with effusion prior to the in-office procedure. (b) At the 3-week follow-up appointment, the patient had resolved otitis media with effusion. BL, blue light; ETD, Eustachian tube dysfunction.
At the 3-week follow-up appointment, the patient reported resolution of dyspnea, hearing loss, and aural fullness. Given the recurrent nature of RRP, ongoing surveillance with flexible nasolaryngoscopy every 3 months has been maintained. Over 4 years of follow-up, the patient has demonstrated sustained symptomatic improvement.
Conclusion
This case highlights the potential of office-based interventions for a rare and anatomically challenging presentation of nasopharyngeal RRP. In this patient, laryngoscopic excision of the nasopharyngeal papillomatous lesion was associated with resolution of symptoms of secondary ETD, including unilateral hearing loss, aural fullness, and ear popping. The lesion was excised in the clinic using a BL laser, a photoangiolytic laser with properties similar to the commonly used potassium-titanyl-phosphate (KTP) laser. 7 These findings align with prior work by Miller and Gardner, which demonstrated that office-based laser excision can offer symptomatic relief comparable to operative management. 8 Furthermore, in-office intervention bypasses the need for general anesthesia while allowing real-time patient feedback throughout the procedure.9,10
In addition to effectiveness and safety, office-based approaches may also offer potential cost advantages. Chen et al reported that RRP management in the operating room costs 3.6 to 3.7 times that of the equivalent in-office laser therapy procedure, supporting that laser therapy could serve as a more cost-conscious management option. 11 Additionally, this may be a practical alternative for nasopharyngeal RRP, as clinic-based interventions can be completed more quickly and with a shorter recovery period. 8
Although nasopharyngeal RRP has traditionally been managed in the operating room due to anatomical complexity, this case suggests that office-based BL laser excision may provide symptomatic improvement while feasibly mitigating procedural risks and costs in a time-effective manner. Together, these findings suggest that office-based BL laser excision may represent a safe, efficient, and patient-centered option in select cases of nasopharyngeal RRP involving the right torus tubarius. Further study with longer follow-up and larger patient cohorts is needed to better define the role of this approach in the management of nasopharyngeal RRP.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data relevant to this case report are included within the article.