
Abstract
Objectives:
This study aims to investigate the association between the perceived functional impact of hearing loss, assessed using the evaluation of the impact of hearing loss in adults (Évaluation du Retentissement de la Surdité chez l’Adulte; ERSA), and depressive symptoms quantified by the Beck Depression Inventory (BDI) in adults with hearing impairment.
Methods:
This cross-sectional study comprised adult individuals exhibiting hearing loss of at least 25 dB in 1 ear for a minimum period of 6 months. The ERSA scale assessed hearing-related quality of life (QOL) in functional and psychosocial domains, whereas depression symptoms were measured using the BDI. Demographic and clinical attributes were documented. Correlations between ERSA scores and BDI scores were analyzed in various aspects.
Results:
A total of 103 adults with hearing loss were included in this study. Higher BDI scores were significantly correlated with lower ERSA scores in the QOL, personal life, and social life domains. Strong negative correlations were observed between BDI scores and ERSA total scores (ERSA 150 and ERSA 200). Participants exhibiting more severe, bilateral, and mixed-type hearing loss showed higher depressive symptom scores and lower ERSA outcomes. Hearing aid users exhibited higher BDI scores and lower ERSA scores compared with non-users. A higher socioeconomic status correlated with reduced depression symptoms and improved hearing-related QOL.
Conclusions:
The perceived functional and psychosocial impact of hearing loss, as evaluated by ERSA, is strongly associated with the severity of depressive symptoms measured by the BDI. These findings highlight the necessity of incorporating patient-reported outcome measures and mental health screening into routine audiological assessment. A multidisciplinary, patient-centered approach addressing both auditory and psychological requirements may improve overall outcomes in adults with hearing loss.
Keywords
Introduction
Hearing loss and impairment are major public health concerns worldwide, affecting more than 20% of the global population, with prevalence increasing markedly with age. Currently, ~5% of the world’s population has disabling hearing loss requiring rehabilitation. 1 Beyond measurable declines in auditory thresholds, hearing impairment imposes substantial limitations on communication, participation in social activities, and engagement in professional and personal roles. These functional difficulties are frequently associated with social withdrawal, reduced self-efficacy, and diminished overall quality of life (QOL). Accordingly, hearing loss is increasingly recognized not only as a sensory deficit but also as a condition with broad psychosocial consequences.2 -4
Accumulating evidence indicates that hearing loss is associated with adverse mental health outcomes, including social isolation, depressive symptoms, anxiety, stress, and reduced cognitive function.3 -5 In addition to depression, individuals with hearing impairment have a higher prevalence of comorbid conditions such as arthritis, cancer, cardiovascular disease, diabetes, hypertension, stroke, and emphysema. 6 Several studies have demonstrated that adults with untreated or progressive hearing loss exhibit significantly higher rates of depressive disorders compared with individuals with normal hearing.4,5,7,8 Consequently, the assessment of depressive symptoms in individuals with hearing impairment has become an essential component of comprehensive clinical evaluation.
Evaluation of the impact of hearing loss in adults (Évaluation du Retentissement de la Surdité chez l’Adulte; ERSA) is a questionnaire developed by Ambert-Dahan et al to assess the functional and psychosocial burden of hearing loss. 9 This instrument evaluates perceived hearing-related difficulties across 4 domains: QOL, personal life, social life, and professional functioning. Unlike pure-tone audiometry, which primarily reflects auditory sensitivity, ERSA captures the individual’s subjective experience and the extent to which hearing difficulties interfere with daily functioning.
The Beck Depression Inventory (BDI), developed by Beck et al in the 1960s, remains one of the most widely used, practical, and well-validated self-report measures for assessing the severity of depressive symptoms. 10 The BDI encompasses cognitive, affective, and somatic components of depression, making it suitable for identifying psychological distress in populations with chronic health conditions, including sensory impairments. As hearing loss has been consistently associated with increased vulnerability to depression, examining depressive symptoms alongside functional hearing-related difficulties may provide a more comprehensive understanding of patient well-being.2,7
Although the association between hearing loss and depression has been well documented, relatively few studies have explored the relationship between ERSA scores—which reflect perceived functional and psychosocial impact—and BDI scores, which indicate depressive symptom severity. Understanding how perceived hearing-related handicap relates to emotional well-being may assist clinicians in identifying individuals who may benefit from further psychological evaluation and supportive interventions. Furthermore, clarifying the nature of this association may inform interdisciplinary management strategies integrating audiological and psychological assessment.
The aim of this study is to examine the correlation between ERSA scores and BDI scores in adults with hearing impairment. By evaluating the relationship between the perceived functional impact of hearing loss and depressive symptoms, this study seeks to contribute to the existing literature on the importance of mental health assessment in hearing-impaired populations and to support patient-centered approaches in clinical practice.
Materials and Methods
Measurement Tools
ERSA Scale
In this study, the ERSA scale was used to assess the impact of hearing loss on the daily lives of adult individuals. The ERSA scale is a self-report assessment tool developed by a multidisciplinary team consisting of 3 ENT physicians, 3 speech therapists, and 1 clinical psychologist, working at an adult cochlear implant reference center in France. 9
The ERSA scale evaluates the effects of hearing loss across 4 domains: general QOL, personal life, social life, and professional life. Each domain consists of 5 items. Participants score each item on a scale from 0 to 10, based on a system adapted from the Visual Analog Scale. A score of 0 represents the most negative condition, whereas 10 reflects a normal or ideal condition. Therefore, lower scores indicate a greater negative impact of hearing loss on daily functioning.
The ERSA scale includes 2 scoring formats: ERSA 150 and ERSA 200. ERSA 200 incorporates the professional functioning domain and is applicable only to employed participants, whereas ERSA 150 excludes this domain and can be calculated for all individuals. In the present study, both ERSA 150 and ERSA 200 scores were reported. ERSA 150 was used to ensure comparability across the full cohort, while ERSA 200 was analyzed separately within the subgroup of employed participants. This approach allowed us to present comprehensive results while minimizing analytic heterogeneity related to employment status.
The maximum score for each domain is 50 points.
For participants who were unemployed or retired, the total score was calculated based on 3 domains, with a maximum value of ERSA 150.
For participants who were professionally active, the professional life domain was also included, resulting in a maximum total score of ERSA 200.
The scale was administered to all participants in a face-to-face setting. Owing to the clarity and simplicity of the items, administration time was short, and completion was straightforward. Participants who were unable to read the questions or mark their responses were assisted by a family member. Prior to administration, all participants were informed about the study, and written informed consent was obtained.
Öztürk et al evaluated the validity and reliability of the ERSA questionnaire adapted into Turkish in 2023. 11
Beck Depression Inventory
In addition to the ERSA scale, the BDI was administered to evaluate the presence and severity of depressive symptoms among participants. The BDI is a widely used, validated self-report instrument developed by Beck et al, designed to measure cognitive, affective, and somatic components of depression. 10
The inventory consists of 21 items, each scored on a 0 to 3 scale, reflecting increasing levels of symptom severity. The total score ranges from 0 to 63, with higher scores indicating more severe depressive symptoms. Standard cut-off points were used to classify depression severity as follows:
0 to 9: minimal depression
10 to 18: mild depression
19 to 29: moderate depression
30 to 63: severe depression
Participants completed the inventory individually in a quiet environment to ensure privacy and optimal concentration. For participants who had difficulty reading or marking responses, assistance was provided by a relative without influencing the participants’ choices. Completion time for the BDI was ~5 to 10 minutes. Before administering the inventory, participants were informed about the purpose of the assessment, and written informed consent was obtained.
Hisli evaluated the validity and reliability of the BDI adapted into Turkish in 1989. 12
Participants
Participants were required to be 18 years of age or older, native Turkish speakers, and to have a median value of 25 dB or more hearing loss in at least 1 ear for a minimum duration of 6 months. Individuals with any previously diagnosed psychiatric disorder were excluded from the study. Only native Turkish speakers were included to ensure accurate comprehension and culturally valid administration of the Turkish versions of the ERSA and BDI scales. Only those with all the inclusion criteria were enrolled. Ethical approval for this study was obtained from the Ethics Committee of our own institution (no: 298/2025). Informed consent was signed by all patients. This study was conducted in accordance with the basic principles of the Declaration of Helsinki.
Demographic and clinical information was collected from all participants, including age, education level, economic status, use of hearing aids, duration of hearing-related complaints, and the presence of comorbid medical conditions.
The classification of hearing loss severity (slight: 16-25 dB HL, mild: 26-40 dB HL, moderate: 41-55 dB HL, moderately severe: 56-70 dB HL, severe: 71-90 dB HL, profound: ≥91 dB HL) followed the widely accepted framework described by Clark and adopted in current ASHA guidelines. 13
Statistical Analysis
Data were analyzed using R software version 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria). The normality of the data was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests. The Mann-Whitney U test was used to compare quantitative variables displaying non-normal distribution with 2-category independent variables. The Independent 2-Sample T-test was used to compare quantitative variables displaying normal distribution with 2-category independent variables. When comparing quantitative variables among 3 or more independent groups, the Kruskal-Wallis H test was used for non-normally distributed data, and multiple comparisons were analyzed with the Dunn test. For normally distributed data with 3 or more independent groups, 1-way analysis of variance was used. Post hoc multiple comparisons were conducted using the Bonferroni test when variances were homogeneous and the Tamhane T2 test when variances were not homogeneous. Associations between categorical variables were analyzed using Fisher’s exact test with Monte Carlo correction, and multiple comparisons were assessed using the z-test with Bonferroni correction. Correlations between non-normally distributed quantitative variables were examined using Spearman’s rho correlation coefficient. Descriptive statistics for quantitative variables were presented as mean ± standard deviation and median (minimum-maximum), while categorical variables were presented as frequency and percentage. A P < .05 was considered statistically significant.
Results
In this study, 43.7% of participants were male, and 56.3% were female, and the mean age was found to be 38.12 years. Among age groups, 68.9% were under 45 years, and 31.1% were 45 years or older. The median value for hearing loss was 43 dB (26-118). Most patients (76.7%) had mild and moderate hearing loss, a hearing loss level below 55 dB. Patients mostly presented with unilateral (69.9%) and mixed (56.3%) hearing loss. Most of the patients did not use a hearing aid (74.8%), were primary or high school graduates (61.1%), and had severe depression (39.8%). The median BDI score was 23 (0-48). The median ERSA 150 score was 94 (17-146), and the median ERSA 200 score was 105 (22-196). Descriptive statistics for quantitative and categorical variables of the study are shown in Tables 1 and 2.
Descriptive Statistics for Quantitative Variables.

Abbreviation: ERSA, Evaluation of the impact of hearing loss in adults (Évaluation du Retentissement de la Surdité chez l’Adulte).
Mean ± standard deviation; median (minimum-maximum).
Descriptive Statistics for Categorical Variables.
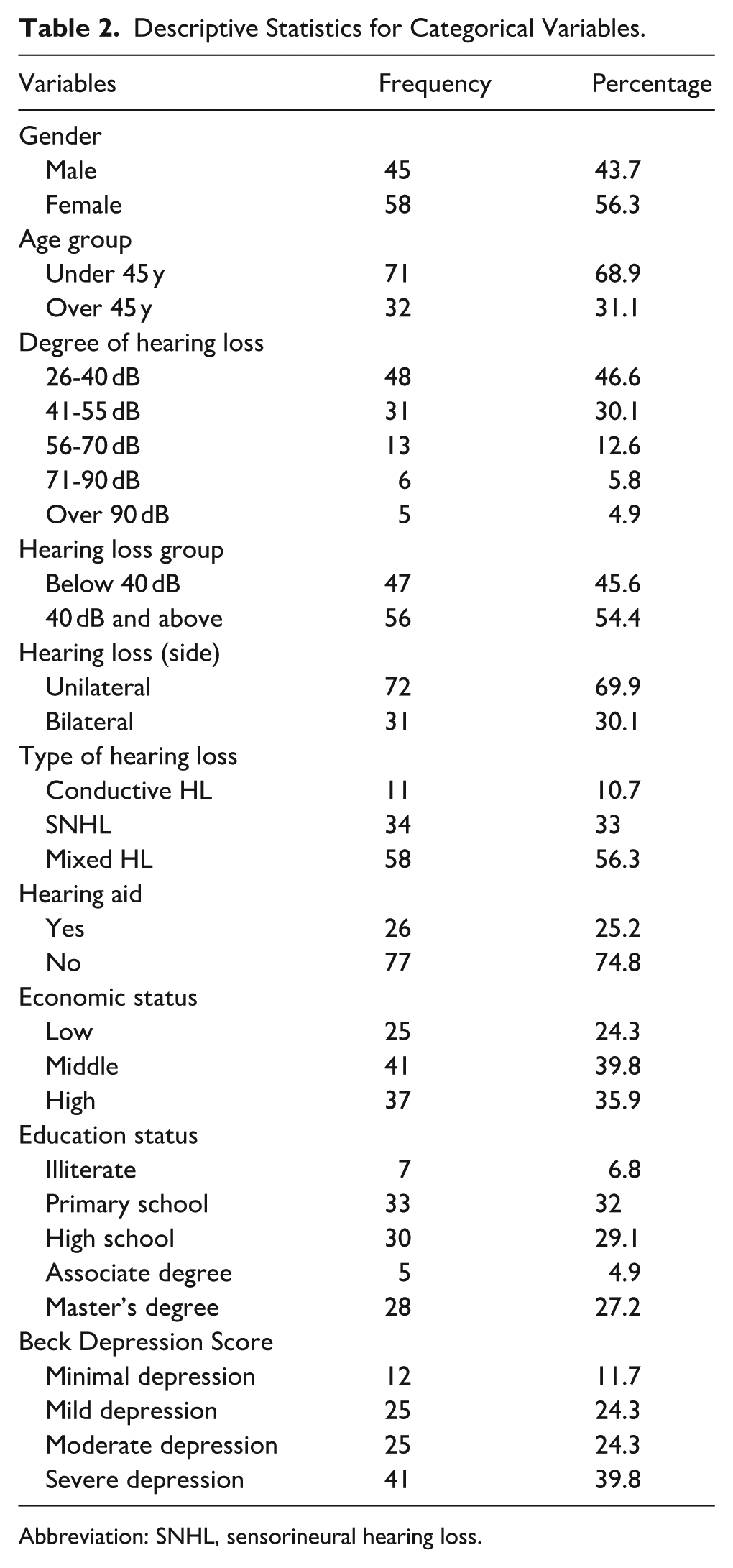
Abbreviation: SNHL, sensorineural hearing loss.
We compared Beck Depression Score (BDS), ERSA QOL score, ERSA Personal Life score, ERSA Social Life score, ERSA 150 score, professional life score, and ERSA 200 score in terms of gender, age groups, degree of hearing loss, HL groups, HL laterality, HL type, hearing aid usage, economic status, and educational status of the patients.
When we compared BDS and ERSA scores in terms of gender, there were no statistically significant differences between the gender groups except for the professional life score (median [min-max]: 30 [0-50] vs 18 [0-47]; Mann-Whitney U = 1764.0, r = 0.30, 95% confidence interval 0.12-0.47; P = .002). When we divided patients into 2 groups as under and over 45 years of age, BDS was statistically significantly higher in the over 45 years group and ERSA QOL, personal life, ERSA 150, and ERSA 200 scores were significantly higher in the under 45 years age group (P < .05; Tables 3 and 4).
Comparison of Scale Scores by Gender.

Abbreviations: CI, confidence interval; ERSA, Evaluation of the impact of hearing loss in adults (Évaluation du Retentissement de la Surdité chez l’Adulte); ES, effect size. Bold values indicate statistically significant results (P < 0.05).
Mean ± standard deviation; median (minimum-maximum); ES [95% CI]: Effect Size (Cohen’s d) [95% Confidence Interval].
Mann Whitney U test.
Independent samples t-test.
Comparison of Scale Scores by Age Groups.

Abbreviations: CI, confidence interval; ERSA, Evaluation of the impact of hearing loss in adults (Évaluation du Retentissement de la Surdité chez l’Adulte); ES, effect size. Bold values indicate statistically significant results (P < 0.05).
Median (minimum-maximum); ES [95% CI]: Effect Size (Cohen’s d) [95% Confidence Interval].
Mann-Whitney U test.
If we classified patients according to their HL degree into 5 categories, and compared them in terms of scale scores, there was a statistically significant difference between groups in every score category, and the mild HL group was mainly the group causing this difference (P < .05; Table 5).
Comparison of Scale Scores According to Degree of Hearing Loss.

Abbreviations: CI, confidence interval; ERSA, Evaluation of the impact of hearing loss in adults (Évaluation du Retentissement de la Surdité chez l’Adulte); ES, effect size. Bold values indicate statistically significant results (P < 0.05).
There is no difference between hearing loss degrees with the same letter (superscript A and B). ES [95% CI]: Effect Size (Eta Square) [95% Confidence Interval].
Kruskal-Wallis H test; median (minimum-maximum).
There was a statistically significant difference between unilateral and bilateral HL patient groups in terms of all scale scores except for ERSA QOL score (P < .05). Patients with bilateral HL had higher BDS and lower ERSA scores except for ERSA QOL (Table 6).
Comparison of Scale Scores According to Hearing Loss Laterality.
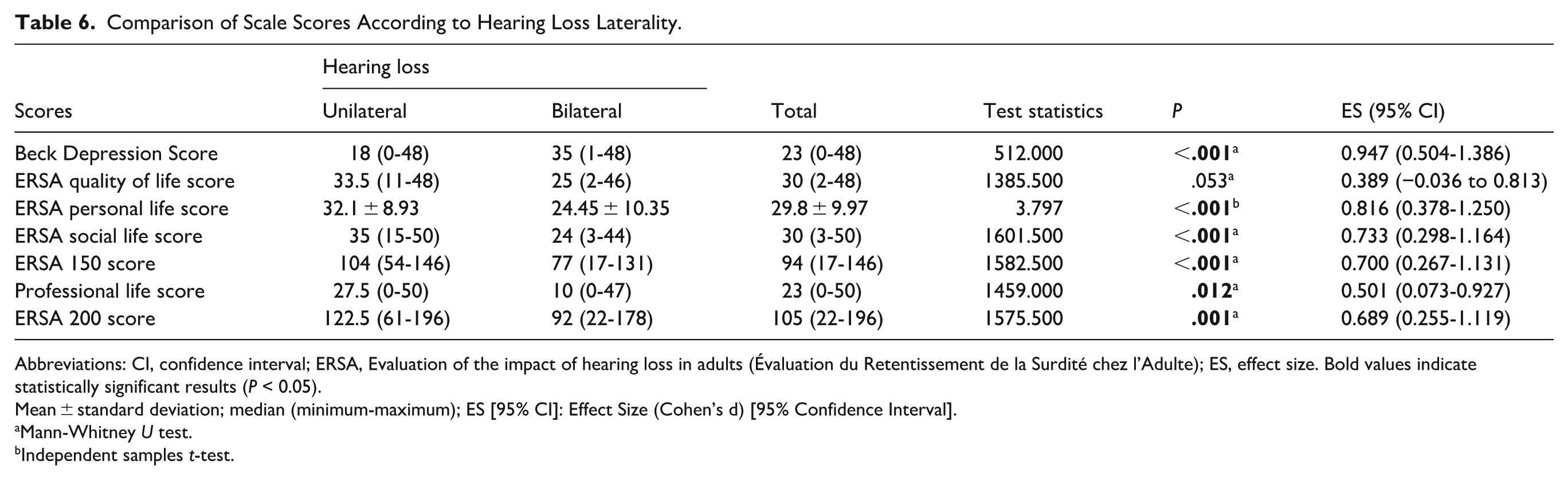
Abbreviations: CI, confidence interval; ERSA, Evaluation of the impact of hearing loss in adults (Évaluation du Retentissement de la Surdité chez l’Adulte); ES, effect size. Bold values indicate statistically significant results (P < 0.05).
Mean ± standard deviation; median (minimum-maximum); ES [95% CI]: Effect Size (Cohen’s d) [95% Confidence Interval].
Mann-Whitney U test.
Independent samples t-test.
When we classified patients according to their HL type, there was a statistically significant difference between the groups in terms of all scale scores (P < .05). Especially, patients with mixed HL had higher BDS and lower ERSA scores compared with the other 2 groups (Table 7).
Comparison of Hearing Loss Type Scores.

Abbreviations: CI, confidence interval; ERSA, Evaluation of the impact of hearing loss in adults (Évaluation du Retentissement de la Surdité chez l’Adulte); ES, effect size. Bold values indicate statistically significant results (P < 0.05).
Mean ± standard deviation; median (minimum-maximum); there is no difference between types of hearing loss that have the same letter (superscript letter A and B). ES [95% CI]: Effect Size (Eta Square) [95% Confidence Interval].
Kruskal-Wallis H test.
One-way analysis of variance.
There was a statistically significant difference between patients using and not using hearing aid and the patients with hearing aids had higher BDS and lower ERSA scores compared with patients who were not using hearing aids (P < .05; Table 8).
Comparison of Scale Scores According to Hearing Aid Presence.
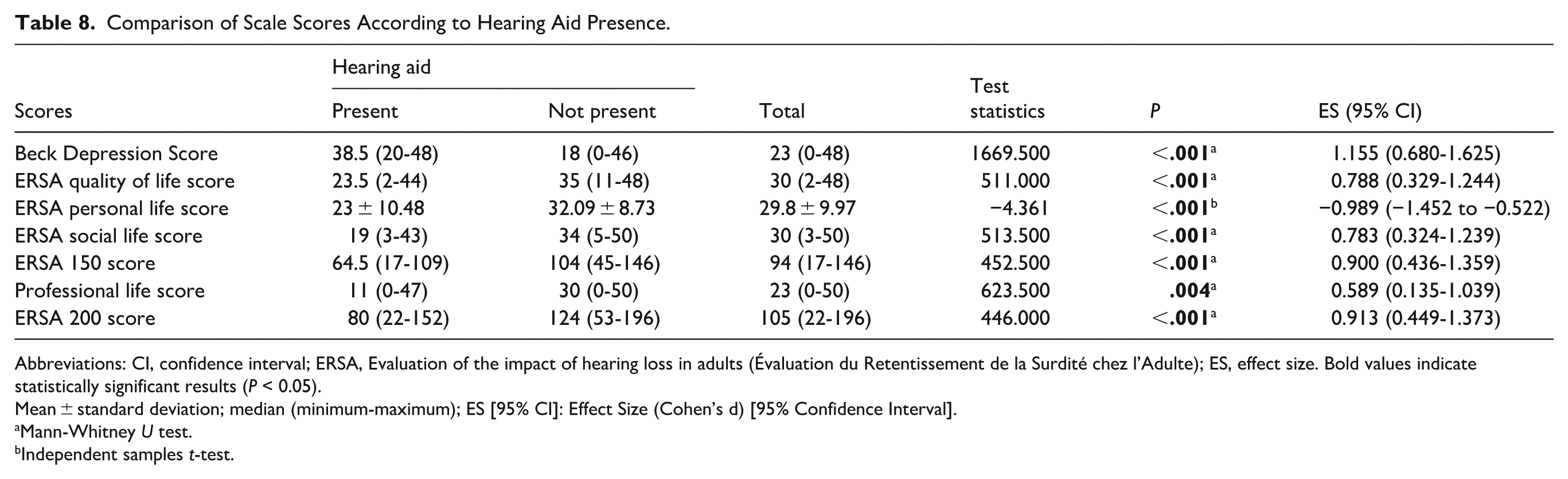
Abbreviations: CI, confidence interval; ERSA, Evaluation of the impact of hearing loss in adults (Évaluation du Retentissement de la Surdité chez l’Adulte); ES, effect size. Bold values indicate statistically significant results (P < 0.05).
Mean ± standard deviation; median (minimum-maximum); ES [95% CI]: Effect Size (Cohen’s d) [95% Confidence Interval].
Mann-Whitney U test.
Independent samples t-test.
When we classified patients according to their economic status, patients with high economic status had lower BDS and higher ERSA scores; there was a statistically significant difference between the economic status groups (P < .05; Table 9).
Comparison of Scale Scores According to Economic Status.

Abbreviations: CI, confidence interval; ERSA, Evaluation of the impact of hearing loss in adults (Évaluation du Retentissement de la Surdité chez l’Adulte); ES, effect size. Bold values indicate statistically significant results (P < 0.05).
Mean ± standard deviation; median (minimum-maximum). There is no difference between economic statuses with the same letter (superscript A and B). Effect Size (Eta Square) [95% Confidence Interval].
Kruskal-Wallis H test.
One-way analysis of variance.
The correlation between BDS and ERSA scores is demonstrated at Table 10. There was a statistically significant, strong negative correlation relationship between BDS and ERSA QOL, personal life, social life, ERSA 150, and the ERSA 200 scores (r = −0.654, P < .001, r = −0.648, P < .001, r = −0.659, P < .001, r = −0.731, P < .001, r = −0.682, P < .001, respectively). When the relationship between BDS and professional life score was examined using Spearman’s correlation, a statistically significant, weak negative correlation was observed (r = −0.393, P < .001).
Examining the Relationship Between Scale Scores.

Abbreviation: ERSA, Evaluation of the impact of hearing loss in adults (Évaluation du Retentissement de la Surdité chez l’Adulte). Bold values indicate statistically significant results (P < 0.05).
r, P: Spearman’s rho correlation.
Discussion
This study highlights a clinically relevant association between the perceived functional and psychosocial effects of hearing loss, which are significantly correlated with the severity of depression symptoms in people with hearing impairment. Our findings reveal substantial and consistent negative correlations between ERSA scores and BDI scores across various domains, thereby enhancing previous research by highlighting that subjective hearing-related handicap is strongly associated with mental health outcomes, independent of audiometric thresholds alone.
Although most of the previous studies demonstrating the correlation between hearing impairment and depressive symptoms have relied primarily on objective audiometric measures or categorical definitions of hearing loss, our findings indicate that an individual’s subjective assessment of hearing-related challenges—assessed using ERSA domains such as QOL, personal life, and social life—demonstrates a more clinically significant correlation with depressed symptoms. This supports emerging evidence demonstrating that perceived communication handicap and participation restriction may mediate the relationship between hearing loss and depression more powerfully than pure-tone averages alone.3,4,14 -16
While general patient-reported outcome measures capture overall psychological distress, the ERSA scale provides a hearing-specific, multidimensional assessment tailored to the functional and psychosocial challenges of individuals with hearing impairment, as it is specifically built by a multidisciplinary ENT and speech therapy team. By separating perceived burden into 4 distinct domains, ERSA allows for a more granular characterization of hearing-related difficulties and by pinpointing whether a patient’s highest burden is in “social life” versus “professional life,” which may help clinicians better contextualize hearing-related difficulties and consider individualized rehabilitation strategies beyond standard amplification. These findings underscore that perceived functional impact, rather than hearing level per se, may be relevant for recognizing individuals who could benefit from additional psychological assessment and supportive care.
The strong negative correlations between BDI scores and ERSA total scores (ERSA 150 and ERSA 200) align with previous research indicating that reduced hearing-related QOL is intricately associated with psychological distress. The study by Golub et al indicates that patients with subclinical hearing loss may exhibit depressive symptoms, the decrease in hearing independently correlates with clinically significant depressive symptoms, and the impact of hearing impairments on depression may commence earlier than previously acknowledged. 7 Jayakody et al’s study concluded that the severity of hearing impairment correlates positively with the severity of mental health symptoms, irrespective of whether speech or high-frequency losses were evaluated. Individuals with severe hearing impairment have higher probabilities of clinically relevant mental health symptoms compared to those with normal auditory function. 3 Our findings validate and enhance previous observations by demonstrating that deteriorating ERSA scores correlate with progressively higher depression severity. Given the cross-sectional design of the study, these findings should be interpreted as associations, and the directionality of the relationship between depressive symptoms and perceived hearing-related handicap cannot be determined.
Age-related differences observed in the present study further align with the existing literature. Participants aged 45 years and older exhibited significantly higher depressive symptom scores and lower ERSA scores in several domains. This finding is consistent with longitudinal studies indicating that older adults with hearing loss are particularly vulnerable to depression due to the cumulative effects of social role changes, reduced social engagement, and increased comorbidity burden.4,17
The identified observations between depression and severity, laterality, and type of hearing loss align with previous findings. Individuals with bilateral and mixed-type hearing loss exhibited markedly lower ERSA scores and elevated BDI scores in comparison to those with unilateral or conductive hearing loss. Bilateral and mixed hearing loss likely necessitate increased communicative demands and listening effort, which have been demonstrated to lead to weariness, frustration, and emotional discomfort. These findings strengthen the notion that increased auditory complexity and diminished compensating ability intensify psychosocial load.18,19
Notably, hearing aid users in our population demonstrated higher depressive symptom scores and lower ERSA outcomes compared with non-users. This finding should be interpreted with caution. Consistent with observations from prior cross-sectional studies, this association is more likely to reflect confounding by indication, whereby hearing aid use is correlated with greater baseline severity or bilateral involvement of hearing loss, rather than an effect of amplification itself. In our cohort, the majority of participants had mild-to-moderate hearing loss and did not use amplification, whereas hearing aid users were predominantly individuals with more advanced impairment—factors that were also associated with higher depressive symptom scores in our data. Given the absence of severity-adjusted or multivariable analyses, no conclusions can be drawn regarding the effectiveness of hearing aids on depressive symptoms. Instead, this observation should be regarded as descriptive and highlights the importance of considering psychosocial burden alongside audiological measures. 20 These findings support the integration of psychological assessment and counseling within hearing rehabilitation frameworks, rather than reliance on amplification alone.
Socioeconomic status emerged as a strong determinant of both depression and hearing-related QOL, with individuals of higher economic status demonstrating more favorable outcomes. This aligns with broader public health literature emphasizing the role of social determinants in shaping both mental health and access to rehabilitative services. Limited financial resources may restrict access to hearing aids, audiological follow-up, and psychosocial support, thereby amplifying the emotional burden of hearing loss.20 -22
From a clinical perspective, these findings underscore the necessity of a multidimensional, patient-centered approach to hearing loss management. The regular use of subjective functional assessments like ERSA, in conjunction with mental health evaluation instruments such as the BDI, may facilitate greater awareness of coexisting depressive symptoms in clinical practice. Interdisciplinary management options that incorporate audiologists, otolaryngologists, and mental health experts may enhance auditory and psychological outcomes.
This study has several limitations that should be considered when interpreting the findings. The study relied on self-report questionnaires, which may be affected by response bias, and its cross-sectional nature prevents the determination of causality. Although strong associations were observed between ERSA and BDI scores, the temporal or directional nature of this relationship cannot be determined. In addition, participants’ emotional state at the time of assessment may have influenced their responses. Furthermore, the BDI may not fully distinguish depressive symptoms from anxiety-related distress; therefore, the scores should be interpreted as reflecting general emotional distress rather than a specific depressive diagnosis. 23 Potential confounding factors such as comorbid medical conditions, social isolation, duration and characteristics of hearing aid use, and previous treatment for depression were not included in a multivariable model, which may have influenced the observed associations. The relatively modest sample size and single-center design may limit the generalizability of the results to broader populations. Future longitudinal and multicenter studies with larger samples and multivariate analyses are needed to confirm and extend these findings.
In conclusion, this study provides new evidence that the perceived functional effects of hearing loss are significantly and consistently linked to the severity of depression symptoms. Our findings support a more integrated approach to hearing assessment that incorporates patient-reported outcomes and mental health evaluation.
Footnotes
Ethical Considerations
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Consent to Participate
Informed consent was obtained from all patients included in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.