
Abstract
Vocal process avulsion is a rare and often overlooked complication of laryngeal trauma, most commonly associated with endotracheal intubation. It involves detachment of the vocal process from the body of the arytenoid cartilage, leading to dysphonia, dysphagia, voice fatigue, and/or aspiration. While strobovideolaryngoscopy and laryngeal electromyography may suggest underlying structural disruption, diagnosis can be challenging when findings are subtle or imaging is inconclusive. Definitive diagnosis and management typically involves surgical evaluation and repair to restore vocal fold tension and glottic competence. We present the first documented case of bilateral vocal process avulsion following endotracheal intubation.
Introduction
Vocal process avulsion is a rare complication of laryngeal trauma characterized by the separation of the vocal process from the body of the arytenoid cartilage. It is caused by intrinsic or extrinsic trauma to the larynx, with reported cases often following endotracheal intubation or flexible or rigid endoscopy. 1 The resulting laxity of the vocal folds during phonation and respiration may lead to dyspnea, dysphonia, and/or dysphagia. In severe cases, acute edema and laryngeal hematoma may precipitate respiratory distress requiring urgent intervention. 2
Assessment of the larynx can be performed using strobovideolaryngoscopy, laryngeal electromyography (LEMG), and computed tomography, particularly in older patients with physiologic laryngeal calcification, when the avulsed vocal process may be visualized. 3 Diagnostic stroboscopic findings may include freely mobile vocal process during respiratory or phonation and thyroarytenoid muscle laxity, sometimes accompanied by a medial bulge within the vocal fold. However, palpation in office or under general anesthesia is the most definitive way to establish the diagnosis. 4
The differential diagnosis for posttraumatic dysphonia includes vocal fold paralysis or paresis, arytenoid subluxation or dislocation, vocal fold hematoma, vocal process avulsion, and thyroarytenoid muscle avulsion. While several case reports have documented unilateral vocal process avulsion, only 1 case of bilateral vocal fold avulsion has been reported in the literature, occurring secondary to external laryngeal trauma sustained in a trampoline accident. The vocal folds were avulsed from the intact vocal process, requiring surgical approximation. 5 However, bilateral vocal process avulsion specifically resulting from intrinsic laryngeal injury has yet to be described.
The first reported case of bilateral vocal process avulsion following endotracheal intubation that we present here is instructive because bilaterality makes the diagnosis more difficult because it eliminates the asymmetry, that is, helpful in recognizing unilateral vocal process avulsion.
Case Presentation
A 71 year-old male presented with persistent hoarseness, a weak and breathy voice, voice fatigue, and reduced voice projection following cervical foraminotomy performed 3 months prior to his initial evaluation. His symptoms were exacerbated by prolonged speaking, significantly impairing his ability to perform his professional duties as a public speaker. The voice changes were noted promptly after the surgery and were accompanied by marked throat pain, tongue ecchymosis, and oropharyngeal discomfort during the immediate postoperative period.
Since the operation, the patient also has had frequent episodes of coughing during ingestion of both liquids and solids. The patient previously sought evaluation elsewhere and was treated empirically for laryngopharyngeal reflux (LPR), without symptom resolution. He denied dysphagia, odynophagia, and reflux symptoms such as throat clearing or excess phlegm production.
On presentation, perceptual voice analysis revealed moderately breathy and hoarse voice with increased phonatory effort. Strobovideolaryngoscopy demonstrated mild bilateral arytenoid and interarytenoid edema, along with freely mobile and asymmetric vocal processes, resulting in glottic insufficiency (Figure 1). The vocal folds appeared foreshortened and lax bilaterally, contributing to a glottic gap during phonation. Moderate anterior posterior muscle tension and lateral supraglottic hyperfunction were observed as a compensatory mechanism for the glottic insufficiency. The patient was treated with voice therapy and high-dose pantoprazole for LPR without significant improvement in symptoms but with improvement in compensatory muscle tension.
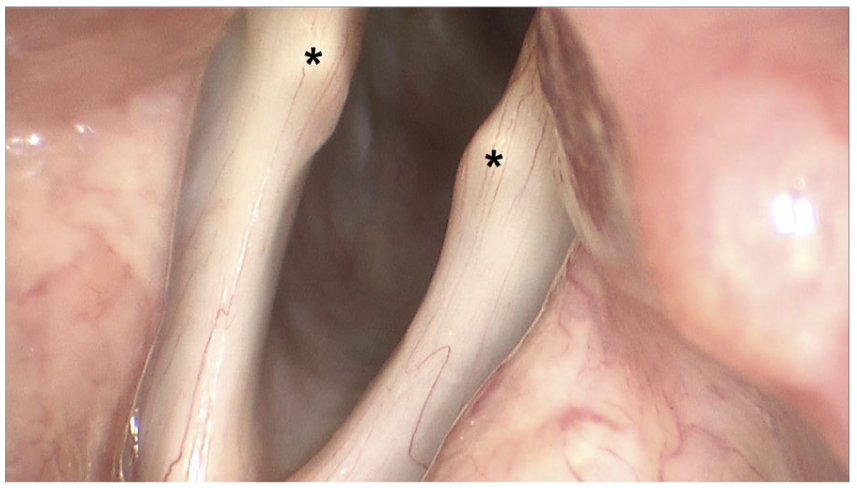
Stroboscopic view of the larynx during vocal fold abduction revealing asymmetric position of both vocal process (asterisks) with concave gaps between the vocal processes and arytenoid bodies.
LEMG revealed 60% decreased recruitment with synkinesis in both thyroarytenoid muscles, 70% decreased recruitment with mild synkinesis in the right posterior cricoarytenoid muscle, and 70% decreased recruitment with prominent synkinesis in the left posterior cricoarytenoid. Additionally, the right and left cricothyroid muscles demonstrated 30% to 40% and 40% decreased recruitment, respectively. A noncontrast computed tomography (CT) of the soft tissues of the neck was unremarkable, and vocal process avulsion was not visualized radiographically, as is the case often.
Although LEMG demonstrated reduced recruitment with synkinesis in multiple intrinsic laryngeal muscles, the pattern was not consistent with isolated recurrent laryngeal nerve injury. Bilateral recurrent laryngeal nerve injury would be expected to result in impaired arytenoid motion which was not present. The decision was made to proceed microdirect laryngoscopy for diagnosis and possible open reduction of vocal process avulsion. The patient underwent operation ~2 weeks following the initial evaluation.
In the operating room, arytenoid joint mobility was normal. Intraoperative palpation of the vocal processes bilaterally confirmed mechanical dissociation of both vocal process from the arytenoid bodies. Once diagnosis was confirmed, an incision was made along the superior surface of the posterior portion of the vocal fold on each side. The avulsed vocal process was found to be densely scarred to the overlying epithelium and could not be separated. Each fractured vocal process was secured to the corresponding arytenoid cartilage body with a figure-of-8 stitch using 4-0 chromic suture. Suture tightening led to visible improvement of vocal fold tension, with successful approximation of the vocal processes to the arytenoid bodies, restoring anatomic positions (Figure 2).
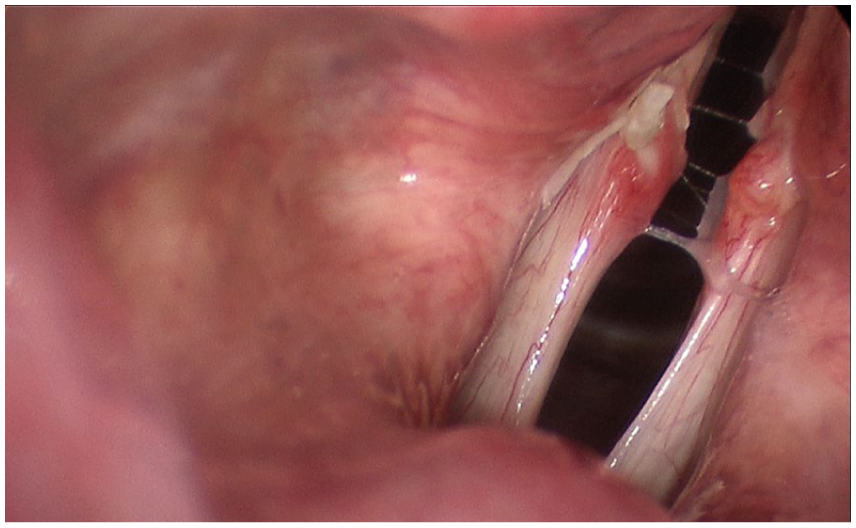
Stroboscopy view of the larynx on 1 week after reapproximation of both vocal fold processes. Chromic sutures are still present with appropriate postoperative erythema and edema of the vocal folds.
To reduce phonatory distraction forces during the healing process, 5 units of botulinum toxin were injected into each thyroarytenoid muscle. Strobovideolaryngoscopy 1 week after surgery revealed bilateral vocal process secured to each body of the arytenoid. There were normalization of vibratory symmetry and amplitude, and improved glottic closure. At 1 month follow-up, the patient reported substantial subjective improvement in voice quality perceived by the patient and voice care team. The Voice Handicap Index, maximum phonation time, and Grade (degree of hoarseness), Roughness, Breathiness, Asthenia (weakness), and Strain scale (GRBAS) were not repeated postoperatively.
Discussion
The current literature surrounding vocal process avulsion is limited, likely reflecting both the rarity and under recognition of this injury. The vocal process is vulnerable to trauma due to its delicate structure and the presence of an embryologic fusion plane between the vocal process and the arytenoid body. The arytenoid body consists of hyaline cartilage, whereas the vocal process originates from mesenchyme of the pharyngeal floor consisting of elastic cartilage. These distinct elements are joined by a fusion plane, that is, vulnerable to shearing forces. In setting of substantial mechanical stress, such as traumatic endotracheal intubation, can cause at this junction, resulting in vocal process avulsion rather than isolated mucosal injury or primary neural dysfunction.
Diagnosis is often challenging, as stroboscopic findings may be subtle, bilaterality may obscure asymmetry, and radiologic abnormalities frequently are absent. Therefore, direct palpation in the office or under general anesthesia often is necessary for definitive diagnosis. Following a brief trial of voice therapy to address compensatory hyperfunction, timely surgical repair, supplemented by adjunctive therapies such as botulinum toxin-mediated chemical tenotomy to reduce phonatory distraction forces, can result in meaningful functional voice improvement, even in cases of bilateral involvement.
Footnotes
Ethical Considerations
IRB was not required for this study as it was a case study of individual patient. The materials of this case study were not previously distributed or published.
Consent to Participate
Written informed consent was obtained from the patient.
Author Contributions
H.R.C. and R.T.S. contributed to writing the final manuscript. O.R. identified necessary case information and strobovideolaryngoscopy photos.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data can be accessed upon request to the corresponding author.