
Abstract
Objective:
This study aimed to examine the epidemiological characteristics of patients with sudden sensorineural hearing loss (SSNHL) to provide an evidence-based foundation for its prevention and treatment.
Methods:
A retrospective analysis was conducted on the clinical data of 2030 SSNHL patients admitted to our department between February 2001 and February 2025. Variables analyzed included sex, age, treatment duration, and prognosis.
Results:
The cohort comprised 957 males (47.14%) and 1073 females (52.86%), with a median age of 54 years. Incidence peaked in the 51 to 60 age group (22.41%). Seasonal peaks occurred in March, July, and November. The overall cure rate was 32.12%, with a total effective rate of 78.72%. Cure rates were significantly higher in younger patients (19-40 years) and lower in patients over 60. Univariate analysis showed a higher cure rate in females (35.32%) than in males (28.56%). However, multivariate logistic regression identified female gender (adjusted odds ratio [OR] = 0.712, 95% confidence interval: 0.586-0.865, P = .001), increased age (adjusted OR = 0.978 per year, P < .001), and longer treatment duration (adjusted OR = 0.942 per day, P < .001) as independent negative predictors of cure.
Conclusion:
This study delineates key epidemiological patterns of SSNHL, including a female predominance, peak incidence in middle age, and distinct seasonal variation. While younger age at presentation predicts better outcomes, female gender, advanced age, and prolonged hospitalization are independent risk factors for poorer prognosis. The findings underscore the need for prompt, targeted management and highlight the complex interplay of demographic and clinical variables in determining SSNHL recovery. As a single-center retrospective study, the generalizability of these findings may be limited to similar clinical settings.
Introduction
Sudden sensorineural hearing loss (SSNHL) is an otologic emergency characterized by rapid-onset hearing impairment of ≥20 dB across 2 contiguous frequencies within 72 hours. 1 As a condition with potentially-permanent consequences, SSNHL has evolved into a significant public health challenge due to its profound impact on communication, psychosocial well-being, and quality of life. 2 Recent epidemiological studies report a rising global incidence of SSNHL, with growing clinical concern about its heterogeneous etiology and variable recovery patterns.1 -3 Despite extensive research, evidence gaps persist regarding population-specific risk profiles, temporal trends, and demographic predictors of therapeutic outcomes. Current literature lacks large-scale analyses examining the interaction between age, gender, seasonality, and treatment timelines—particularly within the Chinese population over extended observation periods.
To address these knowledge gaps, this study retrospectively analyzed 2030 SSNHL cases treated at our institution between February 2001 and February 2025. Through multidimensional assessment of epidemiological characteristics (including age of onset, gender, seasonal patterns, treatment duration, and prognosis), we aimed to enhance the understanding of SSNHL, provide evidence-based insights to inform clinical decision-making, and improve treatment strategies.
Methods
Clinical Data Collection
A total of 2030 patients with SSNHL were admitted to the Department of Otorhinolaryngology at our hospital between February 2001 and February 2025.
Inclusion Criteria
Sudden onset of sensorineural hearing loss of unknown etiology within 72 hours, with hearing loss ≥20 dB HL at least at 2 adjacent frequencies. 1
Exclusion Criteria
Hearing loss due to identifiable causes, such as congenital deafness, drug-induced hearing loss, or noise-induced hearing loss;
Presence of other inflammatory conditions affecting the ear, nose, or throat, or other ear-related diseases (eg, otitis media);
Inner ear malformations or space-occupying lesions in the internal auditory canal.
Treatment Protocol
Patients initially received intravenous methylprednisolone (40 mg/day) or dexamethasone (10 mg/day), combined with vasodilators and neurotrophic agents. Following the release of updated clinical guidelines in 2015, hyperbaric oxygen therapy and thrombolytic therapy were added to the treatment regimen. 1
Efficacy Criteria
Cured: Complete restoration of hearing and resolution of symptoms such as dizziness and nausea.
Markedly effective: Significant hearing improvement (≥30 dB), with resolution of symptoms like tinnitus, vertigo, and nausea.
Effective: Hearing improvement of at least 15 dB, with occasional mild symptoms.
Ineffective: No significant improvement in hearing or symptoms compared to the pretreatment status.
Research Methods
This study is a single-center retrospective observational study. All SSNHL cases were managed and stored via the hospital’s electronic medical record system. Clinical data were retrospectively retrieved and verified by 2 independent researchers using a standardized data extraction form to minimize information bias. Data collected included demographic information (age and gender), treatment duration, and prognosis. Missing data for continuous variables were minimal (<1.5% for any given variable) and were assumed to be missing completely at random. Given the very low missing rate, missing values were imputed using the series mean method, a conservative approach that provides stability without introducing complex assumptions. While this method may slightly reduce estimated variance, its impact is negligible at the observed missing data level.
Statistical Methods
Data were recorded in Microsoft Excel and analyzed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA, 2013).
Measurement data conforming to a normal distribution are presented as mean ± standard deviation, and group comparisons were made using the independent samples t-test.
Data not conforming to a normal distribution are expressed as median (interquartile range) and compared using the nonparametric rank-sum test.
Categorical variables are presented as percentages, and comparisons were conducted using the chi-squared (χ2) test.
Definitions
Total effective cases = cured + markedly effective + effective
Total effective rate = (cured + markedly effective + effective)/total number of patients × 100%
Cure rate = cured/total number of patients × 100%
Results
Gender and Age Distribution
Between 2001 and 2025, a total of 2030 patients diagnosed with SSNHL were admitted to our center. Of these, 957 patients (47.14%) were male and 1073 patients (52.86%) were female, resulting in a male-to-female ratio of approximately 1:1.12.
A detailed breakdown of age distribution by gender is presented in Table 1.
Gender-Age Grouping.
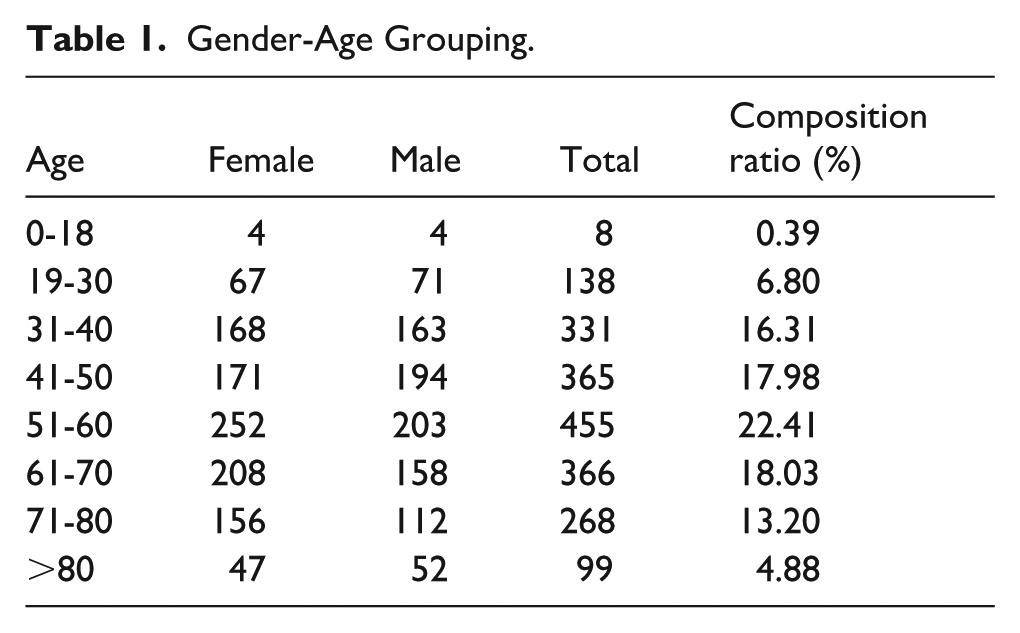
The patients’ ages ranged from 11 to 103 years, with a median age of 54 years. Cases were most frequent in the 51 to 60 year age group (constituting 22.41% of all cases), followed by the 61 to 70 (18.03%), 41 to 50 (17.98%), 31 to 40 (16.31%), and 71 to 80 year groups (13.20%). The number of patients under 30 and over 80 was relatively small. The differences in case distribution across age groups were statistically significant (χ2 = 337.959, P < .001).
Among individuals aged 19 to 50, the distribution of cases between males and females was approximately equal. However, among those aged 51 and above, the proportion of cases was significantly higher in females than in males (χ2 = 10.009, P = .002).
Time of Onset
Seasonal Distribution
The onset of SSNHL exhibited seasonal variation. Monthly peaks in incidence were observed in March (199 cases), July (190 cases), and November (188 cases). The lowest incidence occurred in January (134 cases) and February (128 cases). See Figure 1 for a visual representation of the monthly distribution.
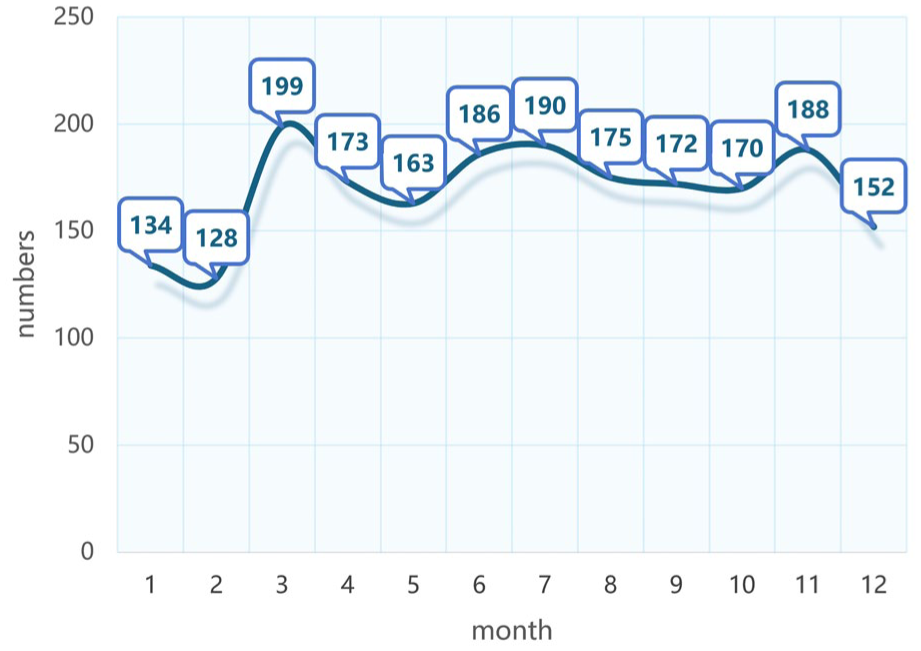
Number of cases in January to December.
There is an increasing trend in incidence year on year from 2001 to 2025, with a trough in 2020 to 2022 (see Figure 2).
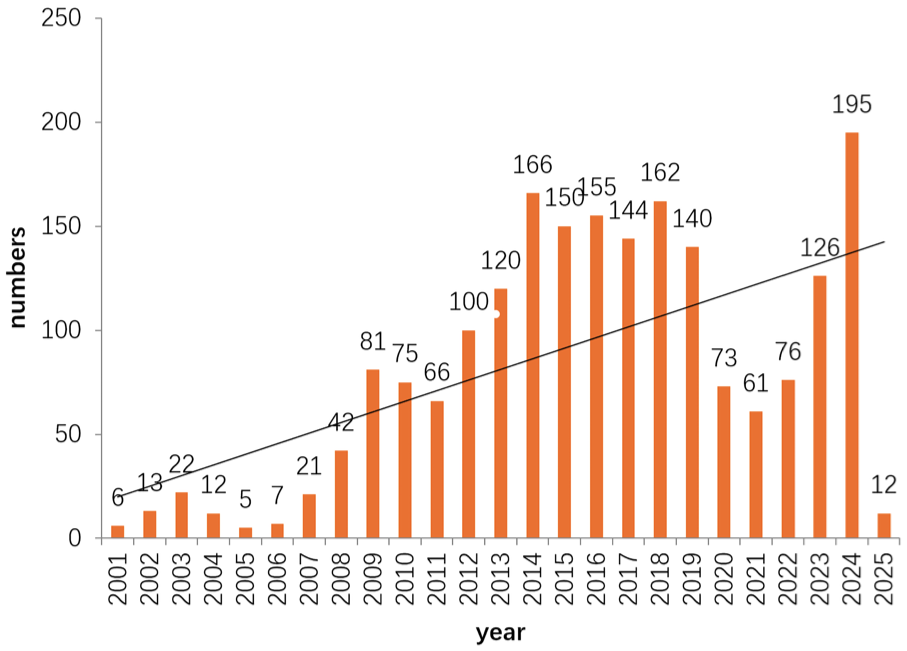
Number of cases 2001 to 2025.
Age and Cure Rate
The cure rates by age group are as follows: 0 to 18 years: 25.00%, 19 to 30 years: 43.48%, 31 to 40 years: 45.02%, 41 to 50 years: 41.37%, 51 to 60 years: 27.09%, 61 to 70 years: 23.77%, 71 to 80 years: 23.51%, and over 80 years: 17.17%. The data indicate that younger patients, particularly those aged 19 to 40 years, had significantly-higher cure rates, while patients aged over 61 years exhibited notably-lower cure rates. A chi-squared test confirmed that the differences in cure rate distribution across age groups were statistically significant (χ2 = 84.129, P < .001).
Gender and Cure Rate
The composition ratio among male patients was 47.12% with a cure rate of 28.56%. In comparison, female patients had a composition ratio of 52.88% and a cure rate of 35.32%. The cure rate for females was statistically-significantly higher than that for males (χ2 = 10.610, P = .001).
Hospitalization Time and Efficacy
The length of hospitalization of total effective (cured, efficacious) patients was counted according to age as shown in Table 2.
Duration of Treatment for the Total Effective Cases in Different Ages.
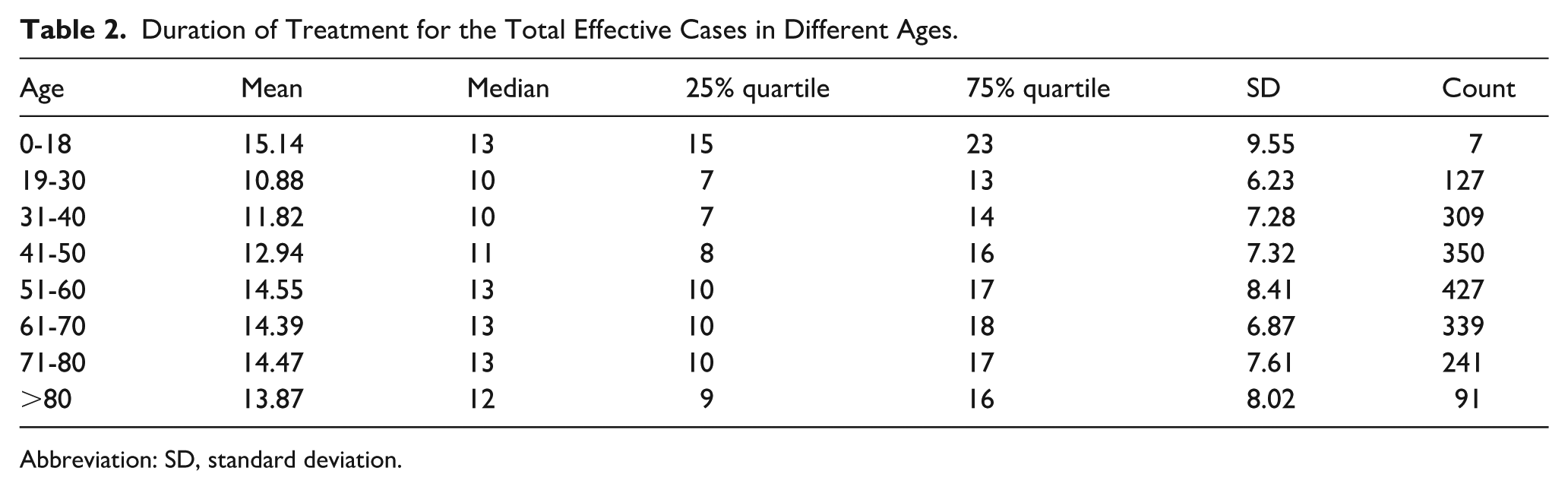
Abbreviation: SD, standard deviation.
It showed that the treatment time of most effective cases was concentrated between 8 and 14 days, with a prolongation in the higher age groups.
Multivariate Logistic Regression Analysis of Factors Associated with Cure Rate
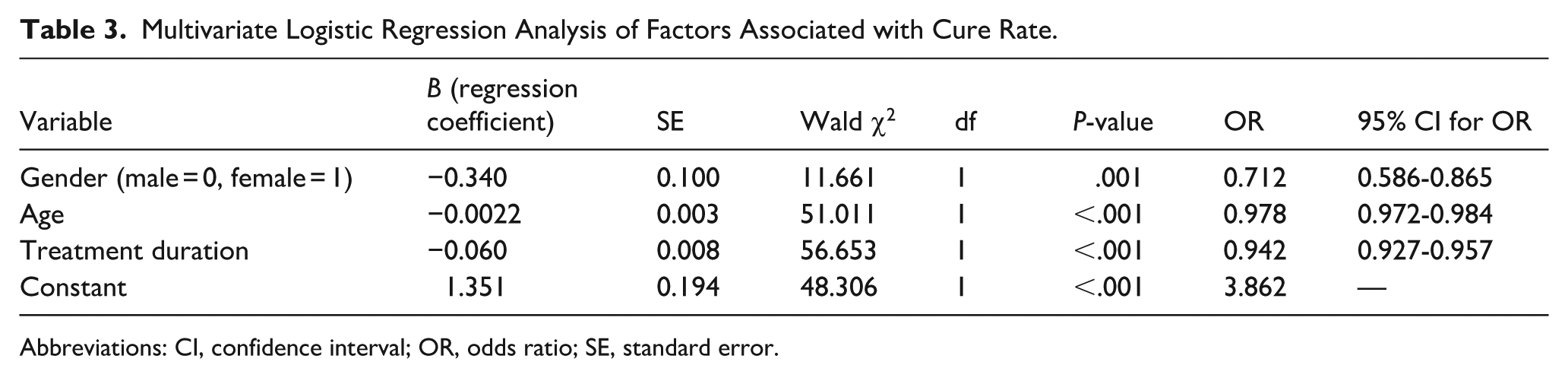
To identify the independent factors influencing the cure rate (dependent variable: cured = 1, not cured = 0), a binary logistic regression analysis was performed, with gender (male = 0, female = 1), age (continuous variable, years), and treatment duration (continuous variable, days) as independent variables. The results are presented as follows:
Independent Effects of Variables
After adjusting for confounding among variables, the regression results were derived, which are shown in Table 3.
Multivariate Logistic Regression Analysis of Factors Associated with Cure Rate.
Abbreviations: CI, confidence interval; OR, odds ratio; SE, standard error.
Result Interpretation
Gender: Female patients had a significantly-lower cure rate than male patients (adjusted odds ratio [OR] = 0.712, 95% confidence interval [95% CI]: 0.586-0.865, P = .001), indicating that female gender was an independent risk factor for non-cure.
Age: Age was negatively associated with cure rate (adjusted OR = 0.978, 95% CI: 0.972-0.984, P < .001), meaning that for each 1 year increase in age, the odds of being cured decreased by (1 − 0.978) × 100% = 2.2%.Treatment duration: Prolongation of treatment duration was negatively correlated with cure rate (adjusted OR = 0.942, 95% CI: 0.927-0.957, P < .001), suggesting that extending treatment duration was associated with a reduced likelihood of cure.
Discussion
Demographic Characteristics
According to the 2015 Chinese guidelines, SSNHL is defined as unexplained sensorineural hearing loss with ≥20 dB of hearing loss at 2 adjacent frequencies occurring within 72 hours. 1 The US diagnostic criteria, which require ≥30 dB of hearing loss at 3 consecutive frequencies, are comparatively-more stringent. 3 This divergence in diagnostic thresholds has 2 important implications for interpreting our findings within the global context. First, it directly influences the reported incidence rate. A less stringent criterion inherently casts a wider diagnostic net, likely leading to the inclusion of a larger number of patients, particularly those with milder or more focal hearing loss. Consequently, our reported incidence and absolute case numbers may not be directly comparable to studies adhering to the stricter US criteria. Comparative analyses of disease burden across regions must account for this fundamental definitional difference. Second, it affects the baseline characteristics and clinical spectrum of the included cohort. By including patients with potentially-milder deficits, our cohort’s average baseline hearing loss might be less severe than that of cohorts defined by stricter criteria. This has a direct bearing on prognostic assessment. Patients with milder initial loss are known to have a higher rate of spontaneous recovery and generally-better prognosis. Therefore, the overall cure and total effective rates reported in our study might appear comparatively higher than those from studies using stricter inclusion criteria, reflecting differences in case mix rather than in solely-therapeutic efficacy. Data from our department show that the incidence of SSNHL spans a wide age range, with a median onset age of 54 years. Most cases are concentrated between the ages of 30 and 70, accounting for 73.78% of all cases. The highest incidence was observed in the 51 to 60 age group, which also corresponds to the age range with the highest prevalence of atherosclerosis, hypertension, diabetes, and other comorbidities.4 -8 Notably, the 30 to 40 age group also accounted for a considerable proportion (16.28%) of cases, suggesting a trend toward younger onset. This shift may be related to factors such as population aging, an accelerated pace of life, and increased psychological stress.9,10
A multicenter study in China reported a median age of onset of 41 years, with no significant difference in the male-to-female ratio. 11 In our study findings, the higher median age may be attributed to our hospital primarily admitting adult patients with more severe conditions. As a single-center retrospective analysis, our findings are subject to selection bias. Our hospital serves as a tertiary referral center, which tends to admit patients with more severe or complex conditions. This likely explains the higher median age (54 years) in our cohort than in multicenter studies that encompass a broader patient spectrum. In terms of gender distribution, our data show a male-to-female ratio of 1:1.12. Among individuals over 50 years old, the incidence was slightly higher in women than in men, which may be associated with greater levels of anxiety or a stronger inclination to seek medical attention. Previous studies have shown that women at this age are more susceptible to anxiety and depression, potentially linked to declining estrogen levels. 12
Health care providers should take a proactive role in enhancing public education and awareness regarding SSNHL. This includes disseminating accessible information about its symptoms—such as abrupt hearing loss, tinnitus, and dizziness—and emphasizing the critical importance of seeking immediate medical attention. Public health campaigns, multimedia resources, and community workshops can be effective tools to increase recognition and reduce delays in diagnosis.
Simultaneously, it is essential to integrate mental health support into the standard care framework for SSNHL patients. 13 The sudden onset of the condition often leads to significant psychological distress, including anxiety and depression, which can adversely affect recovery.14,15 Health care systems should provide timely-psychological counseling, stress management strategies, and peer support groups to address these challenges. Furthermore, early intervention for underlying health issues, particularly cardiovascular diseases such as hypertension and diabetes, should be prioritized.8,16 These conditions are known to contribute to the risk and progression of SSNHL. Regular screening and coordinated management of comorbid diseases can improve overall outcomes.
By adopting a comprehensive approach that combines public education, mental health support, and early-medical intervention, health care providers can help alleviate the emotional burden on patients, promote faster functional recovery, and enhance long-term quality of life for those affected by SSNHL.
Temporal Patterns and Etiological Correlations
Seasonal Variation
Several studies have identified seasonal variation in SSNHL onset, particularly during spring and the transitional period between winter and spring—an observation consistent with our findings. Although the etiology of SSNHL remains unclear, a substantial body of literature suggests associations with vascular conditions (eg, vasospasm or thrombosis of the inner ear), viral infections, autoimmune disorders, membranous labyrinth hydrops, and hair cell damage. March, a common peak month for influenza, and November, a high-risk period for respiratory and cardiovascular diseases in older adults, support the hypothesis that infections and vascular events are key triggers for SSNHL.
The hospital where we are located is situated in a southern city of the Northern Hemisphere, which consistently experiences a pronounced peak in patient admissions during July—the hottest month of the year. This seasonal surge is likely associated with a range of heat-related health issues, including sleep disturbances, reduced appetite, and increased irritability.17,18 High temperatures can disrupt normal sleep patterns, leading to insufficient rest and subsequent declines in immune function and neuroregulatory balance. 19 Additionally, heat often suppresses digestive secretions and peristalsis, contributing to poor nutritional intake and weakened overall resilience. Psychological stress, such as heightened anxiety and agitation in response to prolonged heat, may further exacerbate physiological instability through neuroendocrine pathways. 20
Other studies have suggested that elevated ambient temperatures may contribute to the onset of SSNHL by influencing various metabolic and circulatory pathways. In high-temperature environments, the body undergoes thermoregulatory changes such as peripheral vasodilation, which can divert blood flow away from critical regions including the inner ear, resulting in transient hypoperfusion. 21 Concurrently, excessive heat places sustained strain on the autonomic nervous system, potentially triggering dysfunction that manifests as vasospasm, microthrombosis, and impaired cochlear blood flow. 22 The resulting tissue hypoxia and oxidative stress can damage highly-sensitive hair cells, leading to metabolic impairment, ischemic injury, and ultimately hearing loss. Clinical observations further support this correlation, noting increased reporting of tinnitus, vertigo, and sudden hearing impairment during extreme heat events, consistent with mechanisms of thermal-induced microvascular compromise and ischemia-reperfusion injury in the inner ear.
Data from our center also reveal a gradual year-on-year increase in SSNHL incidence. However, a decline was observed between 2020 and 2022, likely due to the COVID-19 pandemic, during which outpatient visits and home-based treatments predominated and were not captured in the inpatient information system. Other studies have similarly reported a rise in SSNHL cases during the pandemic. 23 National multicenter studies suggest that increasing life stress, irregular sleep patterns, and noise exposure contribute to the rising incidence. 24 In the United States, SSNHL affects 5 to 27 individuals per 100 000 annually, with approximately an estimated 66 000 new cases each year. 25 In Japan, the incidence rose from 3.9 per 100 000 in 1972 to 27.5 per 100 000 in 2001. 26 Similarly, during the period from 2011 to 2012, the hospitalization rate for sudden deafness in Germany was 11.23 per 100 000. 27 These findings support the conclusion that the global incidence of SSNHL is steadily increasing, likely due to modern lifestyle and environmental factors.
Our data indicate that treatment outcomes are more favorable in patients aged 19 to 50, while efficacy tends to decline with advancing age. We hypothesize that younger patients may have a higher likelihood of viral infections as the primary cause, coupled with stronger regenerative capacity, which enhances recovery potential. In contrast, older patients often have coexisting vascular pathologies, which may hinder short-term recovery and negatively affect outcomes.28 -30
In the present study, univariate analysis showed that female patients had a significantly-higher cure rate (35.32%) than male patients (28.56%), a finding consistent with some previous reports and suggesting that gender may play a role in the prognosis of SSNHL. 31 However, when age and treatment duration were further included in a multivariate logistic regression analysis, female gender emerged as an independent unfavorable factor for cure (adjusted OR = 0.712, P = .001). This superficially-contradictory result actually reveals the potential complex interactions and confounding effects among factors such as age, gender, and treatment duration.
We posit that the observed female advantage in cure rate in the univariate analysis was likely confounded by other prognostic factors. For instance, the female patient cohort in this study might have been relatively younger or might have initiated treatment earlier—factors inherently associated with better outcomes. When both age (continuous variable) and treatment duration (continuous variable) were adjusted for in the multivariate model, the independent effect of gender itself became apparent, indicating that among patients of the same age and with the same treatment length, females had a lower likelihood of cure than males. The underlying biological mechanisms may involve gender differences in hormonal levels, immune responses, or microvascular function, warranting further investigation.
Limitations
This study was a single-center retrospective analysis without long-term follow-up, which limits the generalizability of the findings. Several factors may have influenced treatment outcomes, including the type of hearing loss, age distribution of enrolled patients, and the presence of comorbid conditions. Therefore, future research should include multicenter, prospective studies to enhance the quality of evidence and provide more robust data for guiding the treatment and prognostic evaluation of patients with SSNHL.
Regarding the modification of the treatment protocol in 2015. The updated Chinese guideline released that year recommended the addition of hyperbaric oxygen therapy and thrombolytic therapy, primarily for patients with total hearing loss or for those who showed no improvement after initial steroid treatment. However, a key limitation of our retrospective data set is the lack of subclassification of SSNHL types (eg, low frequency, high frequency, flat, or total deafness). Because the application of the new therapies was targeted at specific subtypes rather than to the entire cohort, we cannot reliably identify which patients in the post-2015 era actually received these adjunctive treatments based on guideline recommendations. Consequently, a direct and meaningful stratified prognostic analysis comparing the pre-2015 and post-2015 eras is not feasible with our current data. The potential confounding effect of this protocol change on the overall prognostic trends, while likely limited to a subset of patients, cannot be fully assessed or adjusted for in this study.
By analyzing the epidemiological characteristics of SSNHL, this study highlights the need for comprehensive preventive strategies to effectively reduce its incidence. These measures include promoting healthier lifestyle habits, managing chronic conditions, and strengthening awareness of ear health. For individuals already affected by SSNHL, timely-medical intervention remains critical to alleviating symptoms and maximizing the likelihood of hearing recovery.
Footnotes
Acknowledgements
This study complied with medical ethics standards and was approved by the Ethics Committee of Western Theater Air Force Hospital of PLA (approval number: 2025008). Given the retrospective nature of the study and the use of fully-anonymized data, the requirement for informed consent was waived by the ethics committee.
Author Contributions
Y.F.: Data collection, organization, statistics, writing of the results section, translation and polishing of the full text. L.F.: Visualization. Y.D.: Design, data interpretation, drafting, revision, writing – review and editing. J.Z.: Revision, writing – review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies.