
Abstract
Objective:
To evaluate the association between the triglyceride-glucose (TyG) index and the hearing prognosis in patients with idiopathic sudden sensorineural hearing loss (ISSNHL).
Materials and Methods:
This retrospective study included 63 hospitalized patients with ISSNHL and 32 healthy controls. Clinical data, including audiological assessment, fasting triglyceride (TG), fasting plasma glucose (FPG), and TyG index, were analyzed. Treatment outcomes were classified as good (≥15 dB improvement) or poor (<15 dB). Univariate and multivariate logistic regression were performed, with age, degree of hearing loss, and TyG index included as covariates. Post hoc power analysis was applied to nonsignificant results.
Results:
Compared to the healthy group, ISSNHL patients had significantly higher FPG (110.46 mg/dL vs 84.96 mg/dL, P < .001) but lower TG levels (75.28 mg/dL vs 113.81 mg/dL, P = .036). The TyG index did not differ significantly (8.46 ± 0.78 vs 8.50 ± 0.54, P = .825). Within the ISSNHL cohort, only baseline hearing loss severity predicted prognosis (P = .038). TyG index showed a nonsignificant inverse trend (OR 0.52, 95% CI 0.22-1.19, P = .105). Post hoc analysis indicated limited statistical power (≈38%), suggesting potential Type II error.
Conclusions:
The TyG index was not independently associated with prognosis in ISSNHL, though metabolic alterations were evident. Initial hearing loss severity remained the strongest predictor of recovery. Larger prospective studies with extended follow-up and metabolic monitoring are needed to validate these findings and refine individualized management strategies.
Keywords
Introduction
Sudden sensorineural hearing loss (SSNHL) is a common otolaryngological emergency, defined as ≥30 dB sensorineural hearing impairment over at least 3 consecutive frequencies developing within 72 hours. Approximately 90% of SSNHL cases remain idiopathic (termed ISSNHL) despite comprehensive evaluation. 1 People with ISSNHL often experience accompanying symptoms such as tinnitus, vertigo, and difficulty in sound localization or speech comprehension in noisy environments, which may lead to anxiety, distress, and impact quality of life. 2 The exact pathophysiological mechanisms underlying ISSNHL are unknown. There are several hypotheses that include viral infection, vascular disorders, rupture of the labyrinthine window, and immune-mediated mechanisms. In recent years, attention has focused on interruption of the vascular supply to the cochlea. 3 Cardiovascular disease and metabolic syndrome have been identified as potential risk factors for ISSNHL. 4
The triglyceride-glucose (TyG) index, as a biomarker for the identification of insulin resistance (IR), could be a beneficial tool for the evaluation of diabetes mellitus, metabolic syndrome, and cardiovascular disease. 5 Previous researches show a close association between ISSNHL and diabetes, hypertension, higher total cholesterol, and a higher cardiovascular risk. 6 Recent studies suggest that the TyG index may also serve as a potential predictor of hearing recovery in patients with ISSNHL. 7 However, these studies were based on databases and have not been extensively validated in clinical settings. Our study aimed to evaluate the prognostic significance of the TyG index in hospitalized patients with ISSNHL based on real-world clinical data.
Materials and Methods
Study Population
This retrospective study included patients diagnosed with ISSNHL who were hospitalized in the Department of Otolaryngology, the Fourth Affiliated Hospital of Zhejiang University School of Medicine, between January 2024 and June 2025. Patients who had incomplete clinical or audiological data, who had a history of prior hearing loss in the affected ear or had identifiable causes, who had bilateral hearing loss, who had concurrent severe systemic illnesses, and who were unable to complete follow-up evaluations were excluded. A total of 63 patients who met the admission criteria were enrolled.
In addition, 32 healthy individuals who underwent routine physical examinations, with complete audiological tests, during the same period were enrolled as the healthy group. Notably, pure-tone audiometry (PTA) was added to the routine physical examination package of our hospital as an optional item in 2024, resulting in a relatively small number of eligible controls.
Clinical Data Collection
Clinical information was collected for all participants, including gender, affected ear, audiological assessment, and laboratory test results. Additional variables assessed in the ISSNHL group included tinnitus, vertigo, diabetes mellitus, hypertension, cardiovascular disease, and therapeutic medication.
All patients underwent a comprehensive audiological evaluation at diagnosis, including PTA, acoustic immittance testing, otoacoustic emissions (OAE), and auditory brainstem response (ABR). For post-treatment follow-up, PTA was the most consistently available assessment and therefore served as the primary representation of hearing outcomes in this study. Patients were categorized into 3 subgroups according to their worst hearing threshold before hospitalization: Moderate subgroup: PTA <65 dB; severe subgroup: 65 dB ≤ PTA < 95 dB; Profound subgroup: PTA ≥95 dB.
Laboratory tests included fasting triglyceride (TG) and fasting plasma glucose (FPG) levels obtained before treatment. The TyG index was calculated using the following formula: Ln [fasting TG (mg/dL) × FPG (mg/dL)/2].
Treatment Protocol
All patients received intravenous methylprednisolone, with the dose ranging from 40 to 80 mg/dL for 7 to 10 days. The exact dose and duration were individualized according to the degree of hearing loss, comorbidities, blood glucose control, and dynamic monitoring of hearing recovery. In addition, patients received batroxobin intravenously every other day if fibrinogen levels remained above 100 mg/dL. The total cumulative doses of methylprednisolone and batroxobin were recorded for each patient. Oral mecobalamin and Ginkgo biloba extract drops were also used. Blood glucose and blood pressure levels were closely monitored throughout treatment to avoid complications.
Efficacy Evaluation
The efficacy of treatment was evaluated based on the latest available PTA results obtained after completion of therapy. Among the 63 patients, 37 had audiograms performed at approximately 1 month after treatment, 9 patients did not return for outpatient follow-up and their discharge audiogram was used, 10 had follow-up at 2 months, 5 at 3 months, and 2 at 6 months. Patients with a hearing improvement of ≥15 dB were classified into the good outcome subgroup, while those with <15 dB were classified into the poor outcome subgroup.
Statistical Analysis
The study data were analyzed with SPSS version 27.0. Continuous variables with normal distribution were expressed as mean ± standard deviation (x– ± s). Independent-sample t-tests and 1-way ANOVA were used for comparisons between groups. Continuous variables with nonnormal distribution were expressed as median and interquartile range (M [P25, P75]). Mann–Whitney U test and Kruskal–Wallis test were used for comparisons between groups. Categorical variables were expressed as counts and percentages (n [%]) and compared using the chi-square test (χ² test). Binary logistic regression was performed for multivariate analysis to identify independent predictors of hearing prognosis. To minimize the risk of model overfitting given the limited number of outcome events, we restricted the multivariable logistic regression model to 3 covariates: age, degree of hearing loss, and TyG index. A P-value <.05 was considered statistically significant. Post hoc power analyses will be implemented in case of nonsignificant findings.
Results
Baseline Characteristics
A total of 95 participants were enrolled in this study, including 63 patients in the ISSNHL group (66.32%) and 32 individuals in the healthy group (33.68%). The mean age in the ISSNHL group was 49.27 ± 16.38 years, significantly higher than that of the healthy group (41.72 ± 13.81 years, t = 2.23, P = .028). The gender distribution did not show significant differences between the groups (χ² = .63, P = .427); the ISSNHL group included 34 males (53.97%) and 29 females (46.03%), while the healthy group included 20 males (62.50%) and 12 females (37.50%).
Regarding metabolic indicators, the median level of TG was significantly lower in the ISSNHL group (75.28 [48.27, 140.82] mg/dL) compared to the healthy group (113.81 [82.15, 139.05] mg/dL; Z = −2.09, P = .036). Conversely, the FPG level was significantly higher in the ISSNHL group (110.46 [93.52, 127.94] mg/dL) than in the healthy group (84.96 [81.09, 90.91] mg/dL; Z = −4.79, P < .001). The TyG index was 8.46 ± 0.78 in the ISSNHL group and 8.50 ± 0.54 in the healthy group, with no statistically significant difference (t = −0.22, P = .825).
Baseline analysis showed differences in age, TG and FPG between ISSNHL and healthy groups, but not in TyG index. Detailed results are presented in Table 1. The observed TyG difference was negligible (Cohen’s d ≈ −0.056), corresponding to a post hoc power ≈5.8%.
Baseline Characteristics of ISSNHL and Healthy Group.
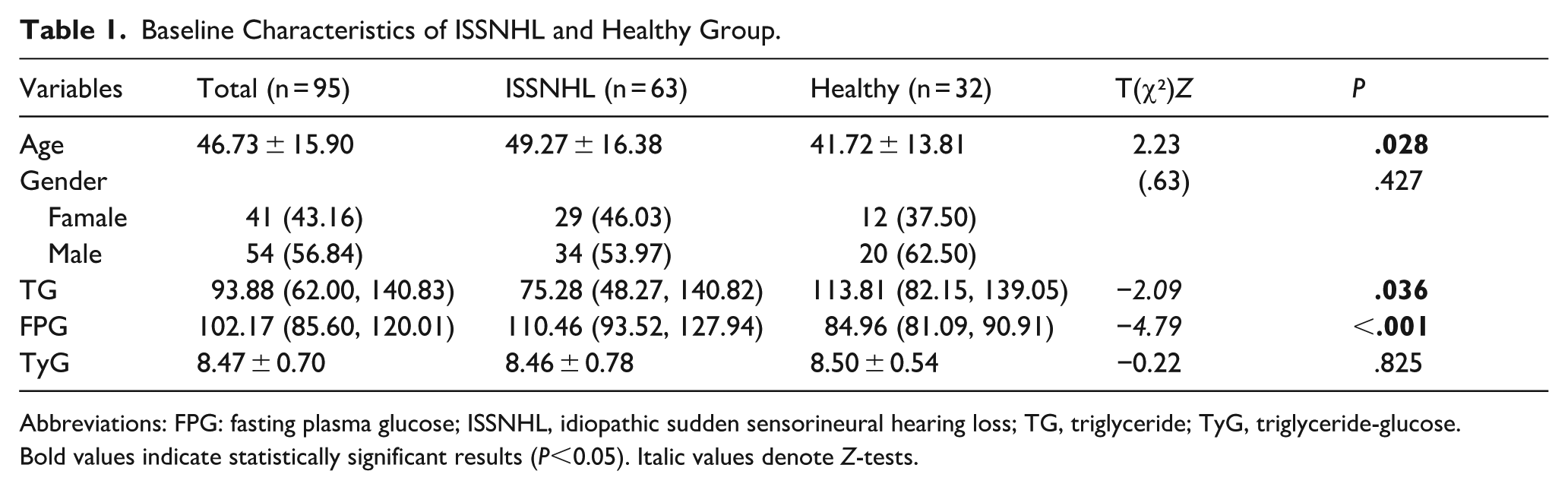
Abbreviations: FPG: fasting plasma glucose; ISSNHL, idiopathic sudden sensorineural hearing loss; TG, triglyceride; TyG, triglyceride-glucose. Bold values indicate statistically significant results (P<0.05). Italic values denote Z-tests.
Univariate Logistic Regression Analysis
In the univariate regression analysis, the 63 patients with ISSNHL were categorized into the good outcome subgroup (n = 32, 50.79%) and the poor outcome subgroup (n = 31, 49.21%).
It revealed that only the degree of hearing loss was significantly associated with prognosis (P = .038). No significant associations were found for age, gender, affected side, disease duration at treatment, presence of vertigo or tinnitus, comorbidities (diabetes, hypertension, cardiovascular diseases), TG, FPG, TyG index, total methylprednisolone or total batroxobin (all P > .05). Full results are summarized in Table 2.
Univariate Logistic Regression Analysis Results.
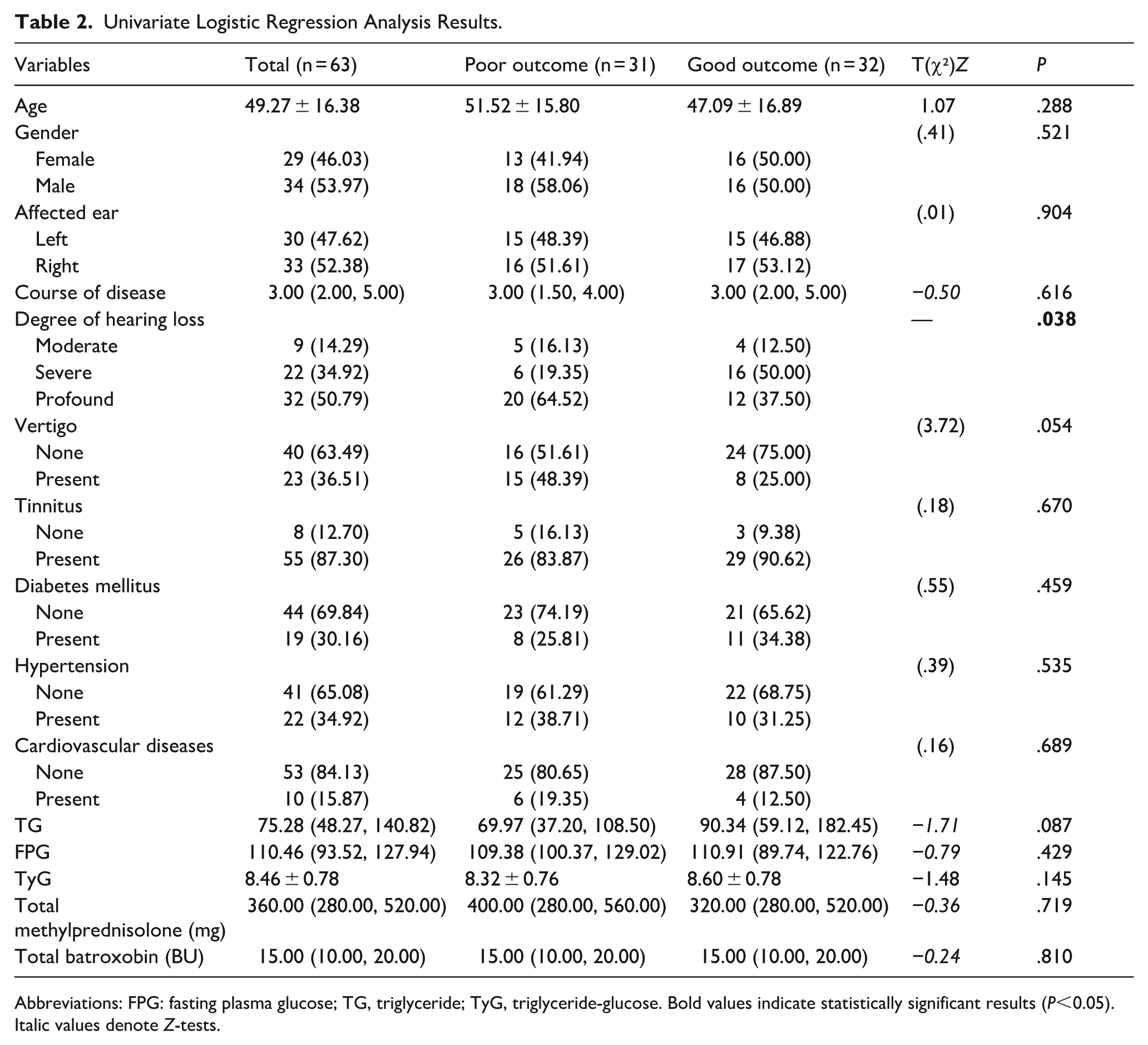
Abbreviations: FPG: fasting plasma glucose; TG, triglyceride; TyG, triglyceride-glucose. Bold values indicate statistically significant results (P<0.05). Italic values denote Z-tests.
Multivariate Logistic Regression Analysis
Variables identified as statistically significant in the univariate analysis (degree of hearing loss), along with age and TyG index.
None of the variables was independently associated with the outcome of treatment in the multivariate analysis (all P > .05). The TyG index demonstrated a borderline inverse association with poor prognosis (β = −.66, OR 0.52; 95% CI 0.22-1.19; P = .105), but this did not reach statistical significance (Table 3). The observed TyG effect corresponds approximately to Cohen’s d ≈ 0.36, with post hoc power ≈38% given the present outcome group sizes (31 vs 32).
Multivariate Logistic Regression Analysis Results.
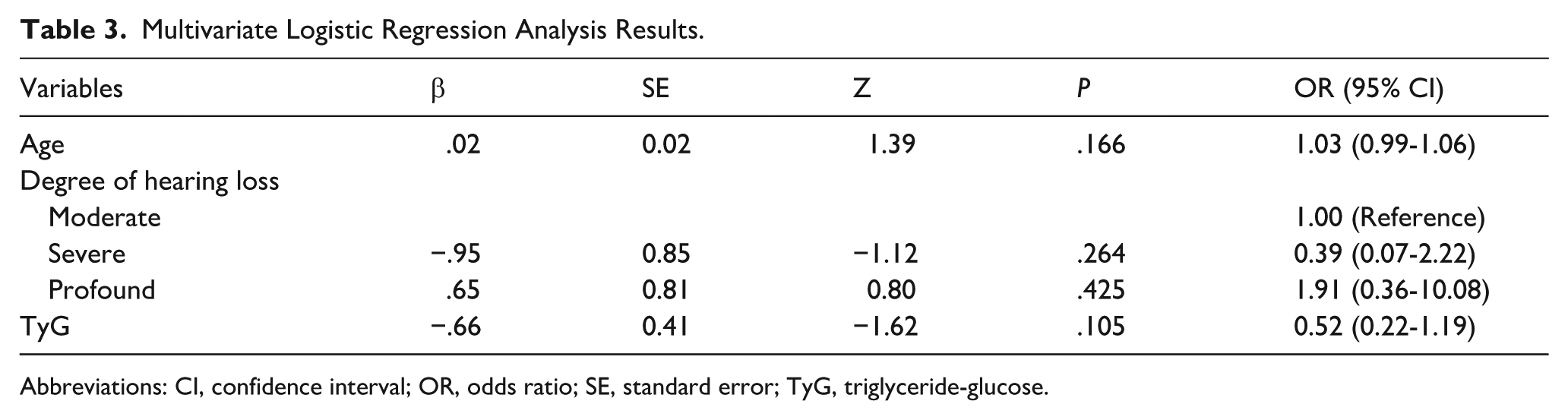
Abbreviations: CI, confidence interval; OR, odds ratio; SE, standard error; TyG, triglyceride-glucose.
Discussion
This study preliminarily explored the relationship between the TyG index and the hearing prognosis in patients with ISSNHL. To our knowledge, this is the first investigation utilizing real-time inpatient data to assess the potential predictive value of this index in clinical practice. We found significant differences in TG and FPG levels, whereas the TyG index itself showed no significant difference between the ISSNHL and healthy groups. Within the ISSNHL cohort, both univariate and multivariate logistic regression analyses failed to establish a statistically significant association between the TyG index and treatment outcomes. In contrast, the degree of hearing loss at onset was significantly related to prognosis, consistent with previous studies suggesting that milder initial hearing impairment predicts better recovery. 8 Other variables, including gender, age, presence of vertigo symptoms, metabolic comorbidities, and the use of corticosteroids and batroxobin, did not exert a significant influence in our cohort.
The TyG index, a composite marker derived from TG and FPG levels, has been widely adopted as a surrogate marker for IR since it was first proposed in 2008. As a key precursor to type 2 diabetes, IR can impair endothelial nitric oxide production and reduce microvascular dilation capacity, ultimately contributing to vascular endothelial dysfunction and inflammation, thereby elevating cardiovascular risk.9,10 The cochlea is a metabolically active organ highly sensitive to fluctuations in blood flow. It is supplied primarily by a terminal artery system without collateral circulation, making it particularly vulnerable to ischemia and hypoxia once perfusion is compromised. 11 Animal experiments have demonstrated that both hyperglycemia and hyperlipidemia can exacerbate microvascular damage in the inner ear, leading to hearing impairment. 12 Building on this pathophysiological rationale, recent hypotheses propose that IR may also compromise cochlear microcirculation, increasing the risk of ISSNHL. 13 However, in our cohort, no significant difference in the TyG index was observed between the ISSNHL group and the healthy group, and no direct statistical association with disease occurrence could be established. Importantly, post hoc power analysis revealed that the statistical power for this comparison was only approximately 5.8%, indicating a substantial risk of Type II error. Therefore, the negative result is more likely to reflect insufficient sample size and a minimal effect size, rather than definitive evidence against a potential link between the TyG index and ISSNHL. Based on this, the between-group comparison results should be regarded as an exploratory observation, which requires further validation in larger cohorts.
Interestingly, we observed significantly elevated FPG levels but unexpectedly lower TG levels in ISSNHL patients compared to the healthy group. One contributing factor may be the limitation in sample selection, as the 2 groups were not strictly age-matched, leading to a significant age difference that could have influenced FPG and TG levels. Beyond this, the findings may also point to a potentially more complex pattern of glucose and lipid metabolism. 14 A recent meta-analysis also indicated that patients with ISSNHL tend to have higher body mass index (BMI), elevated total cholesterol and low-density lipoprotein cholesterol levels, and a higher prevalence of diabetes, hypertension, and heart disease. 15 These findings reinforce the hypothesis that ISSNHL may be a manifestation of microvascular dysfunction, sharing pathophysiological features with cerebrovascular events such as stroke. 16 Therefore, a comprehensive metabolic and cardiovascular risk assessment should be incorporated into the clinical management of ISSNHL. 17 Notably, some studies have reported that ISSNHL patients with comorbid cardiovascular disease may exhibit better hearing recovery, possibly due to the chronic use of anti-inflammatory and lipid-lowering medications. 18 As representative agents, statins were confirmed in a retrospective study of type 2 diabetes mellitus patients to protect hearing and microvascular function. Their mechanisms extend beyond cholesterol reduction and may involve vascular protection, anti-inflammatory and antioxidative actions, as well as modulation of cellular signaling pathways. These effects may partly disrupt the pathological link between IR and the risk of ISSNHL in patients with type 2 diabetes. 19 Therefore, in ISSNHL patients with comorbid diabetes mellitus or cardiovascular diseases, personalized medication should comprehensively consider metabolic dysfunctions, rather than focusing solely on glycemic or lipid reduction. 20
In our cohort, most hospitalized ISSNHL patients presented with more severe conditions, such as flat-type audiograms or profound deafness. Consequently, the majority received defibrinogen therapy, which is recommended by the Chinese Guideline of Diagnosis and Treatment of Sudden Deafness (2015). 21 Batroxobin is a serine protease with fibrinogen-degrading and anticoagulant properties. To date, no evidence has suggested that it directly affects glucose or lipid metabolism. 22 Clinical studies have indicated that, in the treatment of ISSNHL, using batroxobin to maintain a low and safe level of plasma fibrinogen (<100 mg/dL) can improve inner-ear microcirculation and thereby increase the probability of hearing recovery. 23
As a simplified marker based solely on TG and FPG, the TyG index may have inherited limitations in reflecting the complex pathophysiology of ISSNHL. In our analysis, post hoc power calculation indicated that the statistical power of the multivariate logistic regression was only about 38%, suggesting a substantial risk of Type II error. Therefore, the lack of a significant association between the TyG index and prognosis in this study is more likely attributable to insufficient sample size rather than definitive evidence against a potential link. The etiology of ISSNHL is believed to be multifactorial, involving viral infections, microvascular impairment, and autoimmune responses. Metabolic dysfunction may be only one of several contributing factors. 24 Large-scale studies using data from the National Health and Nutrition Examination Survey (NHANES) have demonstrated strong correlations between the TyG index and mid-to-high frequency hearing thresholds, 7 supporting its relevance in hearing research. A recent Mendelian randomization study revealed that a TyG index >9.07 significantly increased the risk of ISSNHL, while the relationship between FPG and ISSNHL was L-shaped, with a notable risk increase when FPG exceeded 94 mg/dL. Interestingly, mildly elevated FPG levels within a certain range appeared to have a protective effect. 25 In our cohort, the average FPG level was 110.46 mg/dL in ISSNHL patients compared with 84.96 mg/dL in the healthy group, a pattern consistent with the L-shaped association described in that study. Another Mendelian randomization study suggested a causal relationship between elevated TG levels and increased risk of ISSNHL. It also proposed a potential bidirectional interaction in which ISSNHL itself may influence glucose metabolism. 26 These insights further highlight the complexity of ISSNHL pathogenesis and provide promising avenues for future research.
Limitations
This study has several limitations. First, it was a single-center retrospective study. Although all eligible cases were included, the overall sample size remained limited, which led to insufficient statistical power, potential selection bias, and limited generalizability. Second, follow-up durations were inconsistent and relatively short, with most patients reassessed at 1 month, which may have underestimated long-term recovery. Third, prognostic evaluation relied primarily on PTA, a subjective and relatively narrow measure, which may not fully reflect inner-ear function. Finally, post-treatment changes in the TyG index were not available, preventing evaluation of dynamic metabolic alterations and their influence on prognosis.
Future research should adopt multicenter, large-scale prospective cohorts to improve statistical power and external validity. Longer follow-up, dynamic monitoring of the TyG index and other metabolic markers, and incorporation of more comprehensive audiological assessments (such as OAE and ABR) are warranted. These approaches will provide more robust evidence to clarify metabolic contributions to ISSNHL and to guide individualized prognostic assessment and management.
Conclusion
This study evaluated the prognostic significance of the TyG index in ISSNHL. Although no significant association with hearing recovery was identified, post hoc analyses suggested that the null findings were largely attributable to insufficient statistical power. The degree of initial hearing loss emerged as the only independent prognostic factor. These results indicate that while the TyG index may not yet serve as a reliable predictor, further large-scale, prospective studies are warranted to clarify its clinical implications.
Footnotes
Acknowledgements
We thank the study staff and participants for their essential contributions to this research, including assistance with data collection.
Ethical Considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of the Fourth Affiliated Hospital, Zhejiang University School of Medicine (Approval No. K2025198) on Aug 13, 2025. Written informed consent was waived by the Ethics Committee due to the use of anonymized retrospective data.
Author Contributions
Yatian Liu and Jialian Feng designed and performed the clinical study; Yatian Liu analyzed the data and drew the tables; Yatian Liu drafted the original manuscript; Supervision: Yatian Liu and Jianguo He. All authors have read and approved the final work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.