
Abstract
Objective:
Evaluation of the feasibility and surgical applicability of the ENDOFIXexo robotic endoscope holder (AKTORmed) in various ear, nose, and throat (ENT) procedures.
Methods:
This study was conducted as a prospective single-center feasibility study involving 26 patients who underwent endoscopic ENT surgery between September 2022 and May 2025. The ENDOFIXexo system was used as a passive robotic assistant. The study assessed surgical performance, intraoperative handling, system limitations, and safety outcomes.
Results:
The device provides stable endoscopic visualization and allows truly bimanual operation in multiple procedures. It is particularly beneficial for orbital decompression, dacryocystorhinostomy, eustachian tube balloon dilation, and endoscopic ear and laryngeal surgeries. Nonetheless, its application is limited to narrow nasal cavities and highly hemorrhagic procedures. No adverse events were observed, and the setup time remained below 10 minutes.
Conclusions:
The ENDOFIXexo is a safe and practical tool with the potential to enhance the quality of endoscopic ENT surgery by strongly facilitating bimanual techniques. Its utility is highly valuable in complex or assistant-limited procedures. However, further studies are necessary to strengthen these findings.
Keywords
Introduction
Over the last decade, robotic surgery has become increasingly important in head and neck surgery. One notable area is endoscopic surgery that applies robotic support in ear, nose, and throat (ENT) procedures. In particular, endoscopic techniques are considered the gold standard in sinus surgery. 1 Importantly, the scope of endoscopic surgery in ENT extends beyond paranasal sinus surgery to include skull base surgery,2,3 nasopharyngeal surgery, eye and tear duct surgery,4,5 and laryngeal and ear surgery.6 -9 Although it is the gold standard in sinus surgery, endoscopic surgery has a notable disadvantage. While holding the endoscope with one hand, the surgeon can use only the other hand to perform the surgery. A standard solution is the “four-hand technique,” where an assistant holds the endoscope while the surgeon operates. However, incorporating an assistant as a co-surgeon introduces challenges, particularly in the learning curve associated with coordinating an additional operator, which can be relatively flat. Moreover, the static nature of endoscope holding during long operations often leads to assistant fatigue and tremor, resulting in an unsteady image and, eventually, lens contamination from blood. 10 In addition, given the increasing staff shortages and the ongoing efforts to economize healthcare systems, a qualified assistant may not always be available.
To address this issue, various endoscopic guiding systems have been developed.6,11 -13 Over the past few decades, considerable effort has been spent developing mechanical endoscope holders that facilitate bimanual operation.11,14,15 These mechanical endoscope holders typically consist of passive multijointed arms with mechanical, pneumatic, or electromagnetic locking mechanisms. Recent innovations, such as the AESOP system (Medineering), are motorized and allow surgeons to control the endoscope hands-free using a foot pedal.11,16 However, existing systems have several limitations,11,15 including downward drift of the arm, high costs of advanced systems, risk of iatrogenic trauma due to rigid endonasal fixation, bulky construction, and restricted range of motion compared to free-hand techniques.
These persistent issues likely explain why no current endoscope holding system has achieved widespread acceptance in otolaryngology or neurosurgery.
In this report, we present the ENDOFIXexo, a computer-controlled robotic endoscope holder developed by AKTORmed, and initially designed for abdominal surgery and successfully adapted for sinus procedures.17,18 The endoscopic guidance system presented here (ENDOFIXexo® by Aktormed®) is approved for passive robotic assistance in all ENT procedures, including transoral endoscopic surgery and endoscopic ear surgery. It has been utilized not only for sinus surgery 12 but also for transoral pharyngeal surgery. 19 This study aims to evaluate the feasibility of ENDOFIXexo in ENT procedures, seeking to overcome the limitations of “single-hand” and “four-hand” surgery, as well as the downsides of existing endoscope holders. Our goal is to potentially enable truly “two-hand” surgery without the disadvantages currently faced in a wide range of ENT procedures.
Materials and Methods
This prospective single-center study included 26 patients and was conducted between September 2022 and May 2025. The study was approved by the local ethics committee of the University Medical Faculty Duisburg-Essen and was conducted in accordance with the Declaration of Helsinki.
Aktormed Endofix Exo Guiding System
The ENDOfixexo (AKTORmed) is a passive robotic endoscope holder designed to assist surgeons. The system features multiple joints with electronically regulated braking units; all arm positioning and adjustments are performed manually by the surgeon via a fingertip control panel at the last joint, near the end of the endoscope. The endoscope is securely attached to the robotic arm, enabling the surgeon to position it as required. The endoscope is securely attached to the robotic arm, enabling the surgeon to position it as required. Setting up the device takes approximately 5 to 10 minutes. Once the patient is positioned and under deep anesthesia, the robotic endoscope holder is typically attached to the side of the operating table opposite the surgeon. The surgical staff and the robotic arm configuration are shown in detail in Figure 1. The company previously provided staff training.
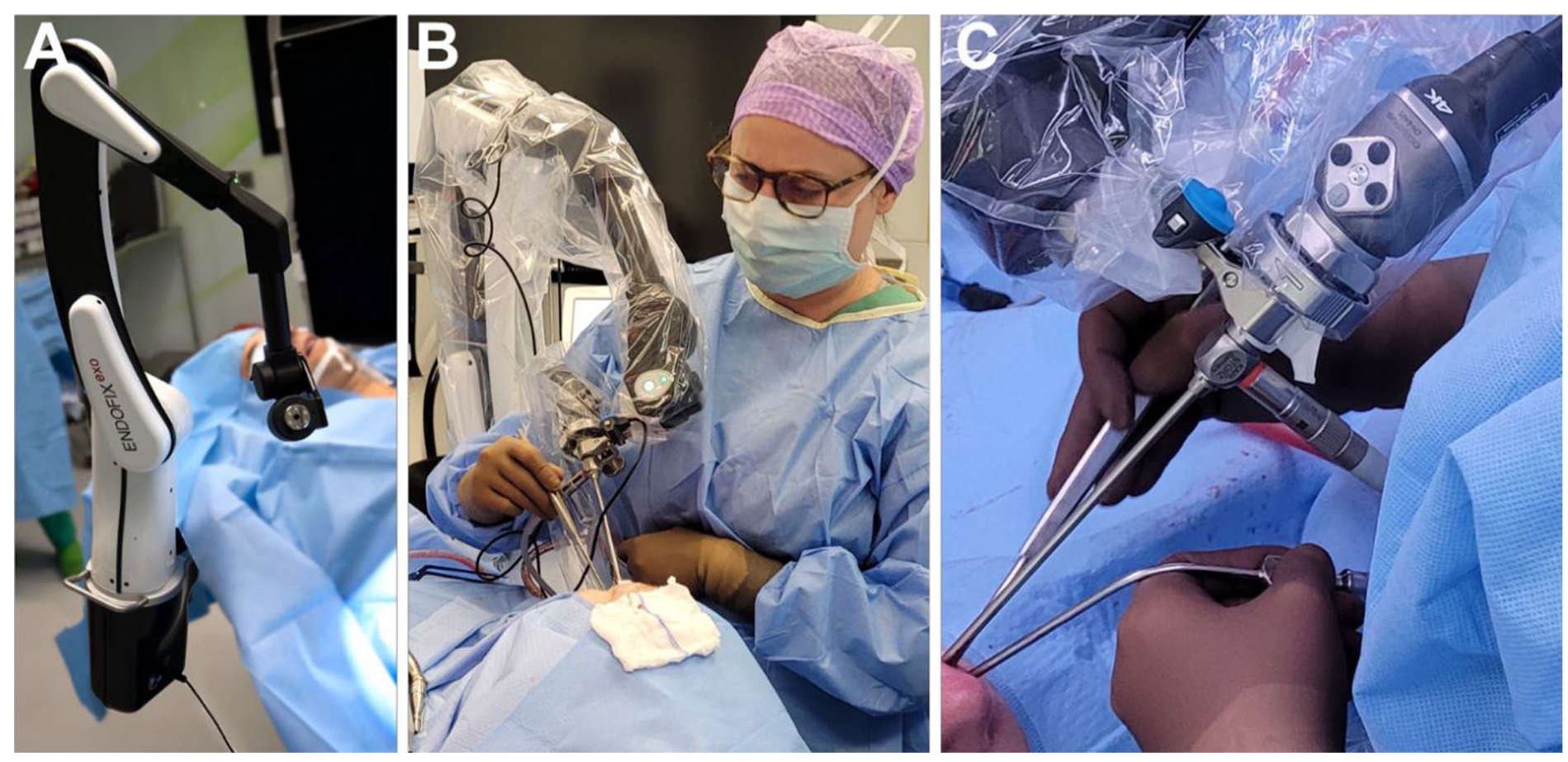
Shows the setup of the ENDOFIXexo endoscopic arm holder in the OR. (A) The ENDOFIXexo endoscopic arm holder is secured to the operating table. (B) This panel illustrates the positioning of the ENDOFIXexo endoscopic arm holder during an endonasal surgery. (C) Here, we demonstrate a true “two-hand” surgical technique while the ENDOFIXexo endoscopic arm holds the endoscope. OR, operating room.
Patients and Surgeries
We performed various endoscopic procedures on 26 patients with various diseases using the ENDOFIXexo (AKTORmed) robotic endoscope holder. Patients were selected based on their physical ability to undergo surgery and their need for various ENT procedures, aside from tumor dissection. The intentional inclusion of a diverse range of surgeries and the absence of additional criteria aimed to assess the feasibility of the device across different ENT surgeries with varying anatomical requirements, ensuring an unbiased evaluation.
Endoscopic paranasal sinus surgery has been developed in our department and described previously. In addition, we performed balanced orbital decompression and endoscopic ear surgery, which included creating a tympanal perforation using a transtympanal approach. Furthermore, the dacryocystorhinostomy was performed endoscopically. Tubal dilation and other masses were biopsied in the nasopharyngeal area. All operations, patients, and their data are listed in Table 1.
Presents Details of Individual Cases, Including Sex, Diagnosis, Surgery, and Approach.
The patient’s surgeries were conducted under general anesthesia. The robotic system was securely anchored to the operating table, and following sterile preparation, the endoscope was connected to the robotic guiding system. The endoscope was equipped with a 4K camera connected to a 55′ monitor (Olympus Visera 4k UHD CLV-5400 HD camera with LMD X55OS 4K display, Sony; Olympus).
Results
Handling of the Aktormed ENDOFIXexo Guiding System
The endoscope can be easily attached to the Aktormed ENDOFIXexo Guiding System, which facilitates straightforward placement of the endoscope on the operating room table. Positioning the system takes only 5 to 10 minutes. Tool movements and control can be performed comfortably and precisely using the fingertip. With the endoscope attached, the system allows for 2- to 4-hand techniques. Although the setup time is slightly longer (less than 10 minutes) than for surgeries without the endoscopic guide system, the overall operating time remains unaffected. Importantly, no adverse events (AE) or serious adverse events (SAE) were reported during the procedures.
Use of ENDOFIXexo in Various Surgical Procedures
Six surgeons conducted the procedures using the system, and all reported a consistently positive user experience characterized by intuitive operation and minimal technical complexity. Use of the system eliminated the need for an assistant during tubal dilatation, orbital decompression, dacryocystorhinostomy, and transcervical procedures, demonstrating its practical feasibility across various surgical contexts. The user experience included subjective assessments from the operating surgeons, focusing on perceived ease of use, image stability, overall handling, and physical strain. All 6 surgeons consistently reported that the system was easy to operate, with a uniform setup time of approximately 5 to 10 minutes for all procedures. Importantly, the device was utilized in surgical contexts where it had not been previously applied, yet its integration was straightforward and did not require additional technical expertise. However, its application does have certain limitations, depending on the specific procedure.
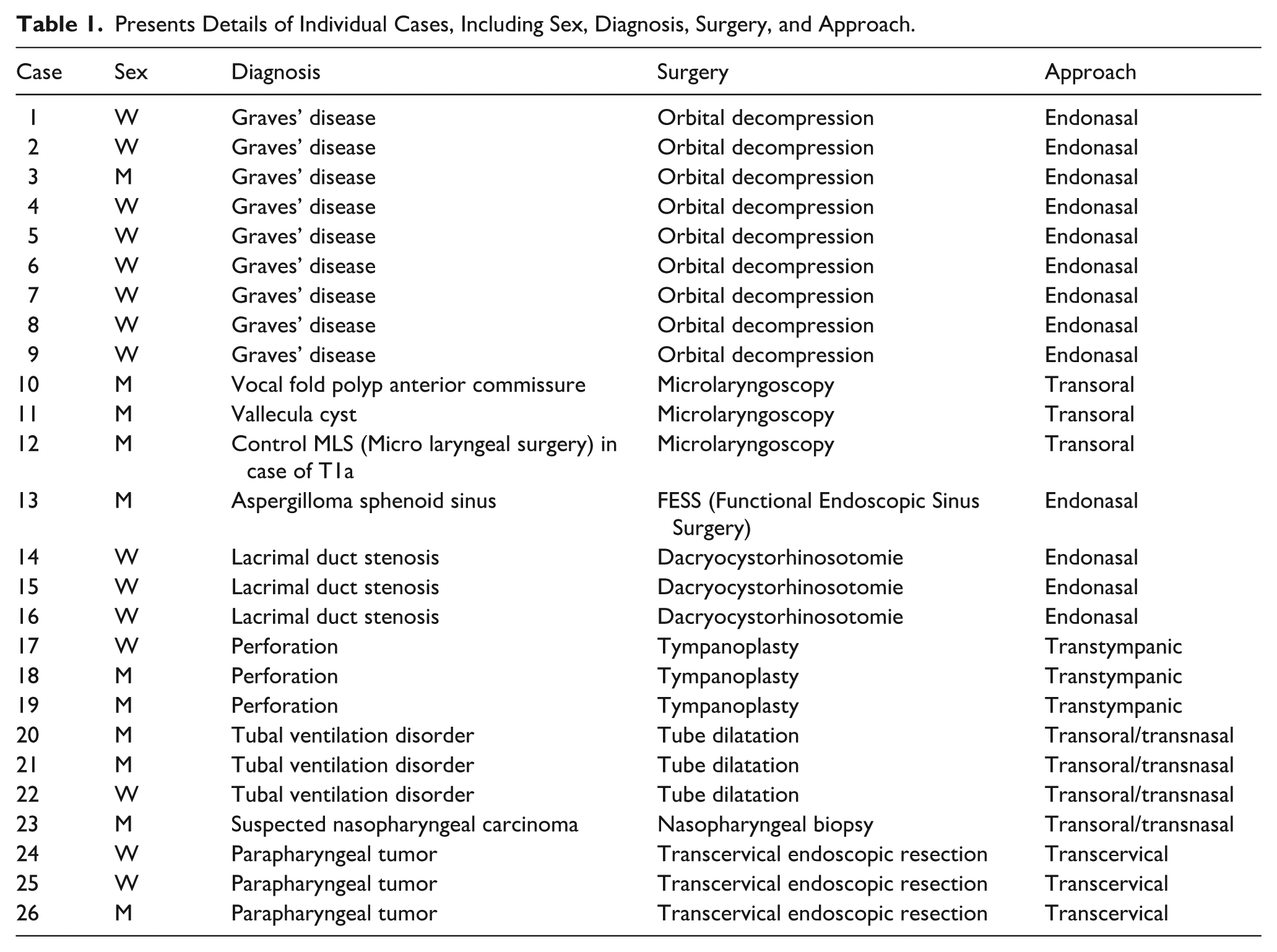
For orbital decompression (9/26 surgeries), the device was particularly beneficial. The removal of the lamina papyracea could be performed under excellent visual conditions, utilizing a truly bimanual technique (Figure 2), which provided a clear procedural advantage.
Depicts the surgical environment for orbital decompression using the ENDOFIXexo endoscopic arm holder. (A) This image shows the application of the ENDOFIXexo endoscopic arm holder and the view provided by the endoscope during the orbital decompression procedure. (B) Additionally, a true “two-hand” approach to orbital decompression surgery is illustrated.
A notable benefit was also observed during dacryocystorhinostomy procedures (3/26 surgeries). In this operation, the endoscope can be statically positioned to visualize the opened lacrimal sac from an endonasal perspective, while an Oggel probe can be introduced through the lacrimal punctum. This setup allowed the surgeon to operate with both hands while maintaining continuous visual control.
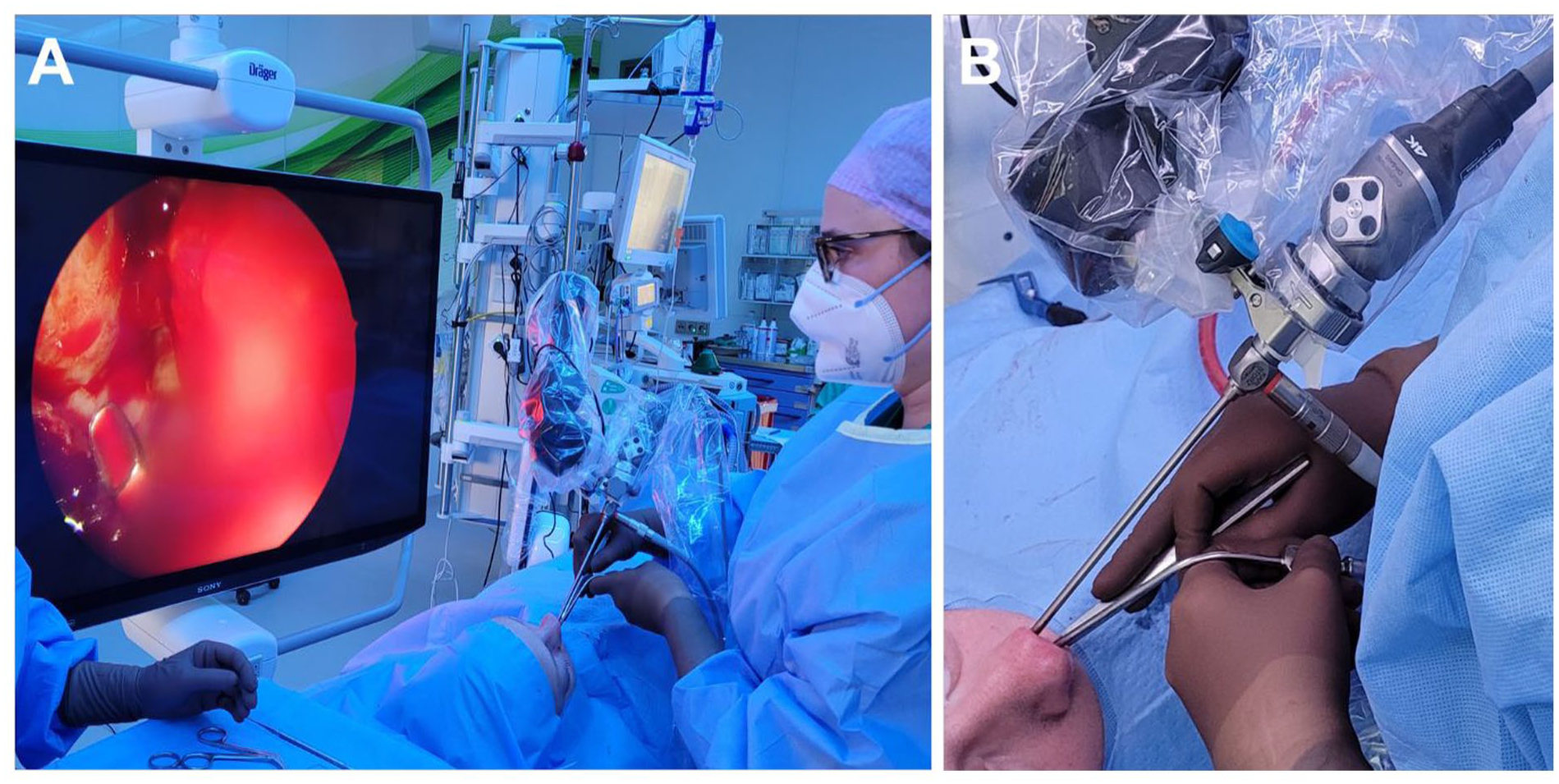
Also, the endoscopic balloon dilation of the eustachian tube (3/26 surgeries) and the nasopharyngeal surgery (1/26) benefited from the use of the robotic arm (Figure 3). The surgeon was able to insert the balloon catheter and simultaneously activate the inflation pump without losing visualization of the nasopharynx. Our team rated this application as highly effective and supportive.
Portrays the surgical environment for tube balloon dilation with the ENDOFIXexo endoscopic arm holder. (A) This image displays the use of the ENDOFIXexo endoscopic arm holder and the view from the endoscope during tube balloon dilation. (B) Furthermore, a genuine “two-hand” technique for tube balloon dilation surgery is demonstrated.
In endoscopic ear surgery (3/26 surgeries), the static passive robotic arm has proven to be a valuable tool, providing significant procedural support, especially in cases involving small tympanic membrane perforations that are suitable for transtympanic repair.
In endoscopic endonasal sinus surgery (1/26 surgeries), however, a static endoscope holder is impractical in scenarios involving significant intraoperative bleeding or anatomically narrow nasal cavities. Under such conditions, the surgeons rated the use of ENDOFIXexo as moderate.
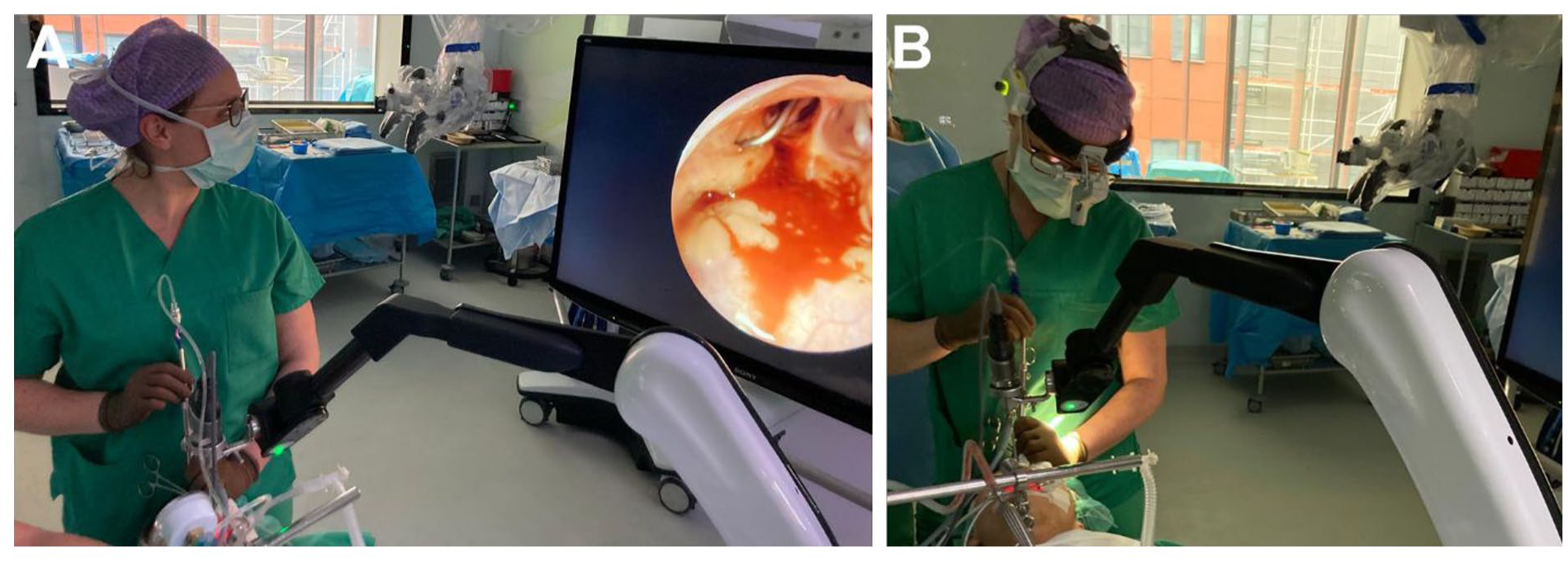
Even in surgical approaches, where endoscopes are generally used for diagnostic purposes, such as microlaryngoscopy (3/26 surgeries) or transcervical endoscopic resection (3/26), the use of ENDOFIXexo has been advantageous. Particularly when microscopic visualization is inadequate for identifying pathologies in the anterior commissure, endoscopic assistance becomes crucial. By incorporating ENDOFIXexo, we were able to resect pathologies using 2 instruments while maintaining complete visualization of the anterior commissure (Figure 4).
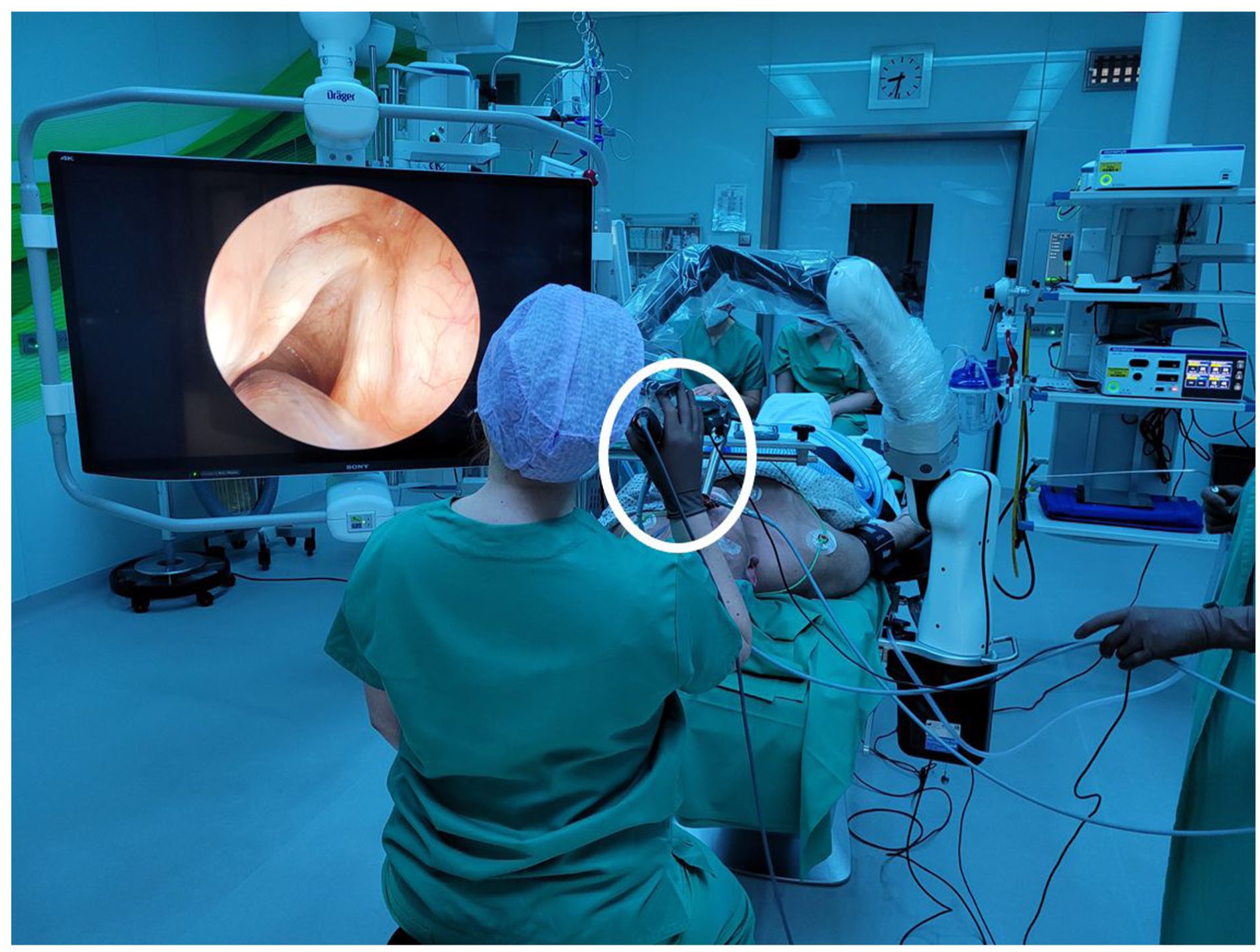
Illustrates the surgical setting for microlaryngoscopy utilizing the ENDOFIXexo endoscopic arm holder. It highlights the simple adjustment of the endoscope using one hand, as indicated by the white circle.
Discussion
In the last decade, robotic surgery has become increasingly important in head and neck surgery. Recent innovations, such as the AESOP system (Medineering), are motorized devices that enable surgeons to control the endoscope hands-free using a foot pedal.11,16 Nevertheless, existing systems present several limitations,11,15 including downward drift of the arm, high costs, the risk of iatrogenic trauma, bulky construction, and restricted range of motion. In particular, for sinus surgery, these systems are often suboptimal because the narrow surgical corridors and frequent, fine endoscope adjustments require a compact, highly responsive support system. The limited maneuverability and slow repositioning of motorized arms hinder the surgeon’s ability to quickly adapt the view, increasing operative time and compromising workflow efficiency. In addition, the bulkiness of robotic arms near the patient’s head restricts access for instrumentation, which may elevate the risk of collision or mucosal trauma in confined nasal spaces. These persistent issues likely account for the failure of any current endoscope holding system to gain widespread acceptance in otolaryngology or neurosurgery.
This feasibility study demonstrated that the ENDOFIXexo robotic endoscope holder can be effectively integrated into a wide range of endoscopic ENT procedures. The system offers a promising solution to the well-known limitations of single- and 4-handed endoscopic surgery, especially when a trained assistant is unavailable or prolonged interventions risk assistant fatigue and image instability.
For procedures such as orbital decompression and dacryocystorhinostomy, the use of ENDOFIXexo provided significant advantages. By maintaining a stable endoscopic view while enabling truly bimanual surgery, the system improved procedural efficiency and surgeon ergonomics. These findings align with previous reports that highlight the benefits of robotic support in precision-demanding interventions.11,14
Similarly, during eustachian tube balloon dilation and endoscopic tympanoplasty, the system proved to be a helpful adjunct, facilitating simultaneous instrument manipulation without compromising visualization. In addition to the newly evaluated feasibility for tube balloon dilation, we confirmed the effectiveness observed in tympanoplastic surgeries. 6 In microlaryngoscopy, where endoscopic assistance is occasionally needed to visualize anterior commissure lesions, ENDOFIXexo enables controlled and effective 2-handed resection, a task often limited by conventional microscopic techniques.
However, some limitations were also identified. In endoscopic sinus surgery, particularly in cases with significant intraoperative bleeding or anatomically narrow nasal passages, static endoscope positioning reduces the flexibility needed for optimal visualization. We rated the system’s effectiveness as only moderately helpful in such scenarios, highlighting the need for careful patient selection and potential refinement to the device’s adaptability. Moreover, to optimize visual clarity, we recommend the routine use of an endoscope with an irrigation channel, especially for longer procedures.
From a technical standpoint, the setup time was slightly longer than that of standard procedures. However, this was limited to less than 10 minutes and did not extend the overall operative duration.
Importantly, no intraoperative complications, AEs, or SAEs were observed, underscoring the system’s safety when used properly.
Despite these encouraging results, it is essential to note that this study was conducted in a single center with a limited number of cases, and the same surgeons performed all procedures. To strengthen our findings and evaluate broader applicability, learning curves, and long-term outcomes, multicenter studies with larger patient cohorts and diverse user and surgeon experiences are necessary.
This study added to the recent developments in minimally invasive techniques for accessing deep-neck spaces. For example, transoral robotic approaches for benign and malignant parapharyngeal space tumors: comparative analysis and systematic review by Chiari et al presents a comprehensive systematic review of transoral robotic surgery (TORS) in the PPS (parapharyngeal space), and highlights how TORS can enhance visualization, provide wristed instrumentation, and allow bimanual access in a challenging anatomical region. 20 Similarly, the multicentric case-series endoscopic-assisted transoral approach (EATA) for extracranial tumors: a multicentric case series by Motta et al demonstrates that endoscope-assisted transoral approaches can safely and effectively remove benign, encapsulated PPS and other deep-neck tumors, with short hospital stays and minimal complications. 21 These contributions illustrate a clear trend: regardless of the specific technology used (robotic platforms, endoscope-assisted approaches, or fixed endoscope holding systems such as ENDOFIXexo), the underlying goal remains the same. All these techniques aim to improve visual field exposure, maintain bimanual operative capability, and reduce the invasiveness. They are as effective as traditional open surgeries while prioritizing functionality and patient well-being.20,22,23 Our transcervical endoscopic approach similarly leveraged these principles—we obtained direct visual control, preserved the ability to use both hands during the procedure, and avoided more extensive external exposures. By placing our results within this broader context, we emphasize the feasibility of minimally invasive, deep-space neck surgery and highlight the incremental value of access systems that facilitate efficient resection in anatomically complex regions, not only for tumor surgeries.
Conclusion
The ENDOFIXexo robotic endoscope holder has proven to be a feasible and safe tool for various endoscopic ENT procedures. It offers significant ergonomic and practical advantages by enabling stable, bimanual surgical techniques without requiring constant manual control of the endoscope. However, its effectiveness can be limited in narrow areas or during procedures involving heavy bleeding. Despite these limitations, the endoscope holder has demonstrated clear benefits in surgeries such as orbital decompression, dacryocystorhinostomy, balloon dilation of the eustachian tube, and endoscopic procedures of the ear and larynx. In an era of increasing surgical complexity and personnel shortages, this system may provide a valuable solution. Future studies are necessary to evaluate long-term outcomes, surgeon learning curves, and cost-effectiveness in broader clinical settings.
Footnotes
Acknowledgements
The authors would like to thank AKTORmed for providing the ENDOFIXexo robotic endoscope holder. We acknowledge support by the Open Access Publication Fund of the University of Duisburg-Essen.
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the local ethics committee of the University Medical Faculty Duisburg-Essen (23-11637-BO 02/2024).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Author Contributions
The study was designed and conceptualized by Anke Daser and Stefan Mattheis. Methodology and Surgery was performed by Anke Daser, Kerstin Stähr, Friederike Kaster, Freya Dröge, Kazim Shiraliyev, and Stefan Mattheis. Data were collected by Anke Daser, Maren Buschmeier, Benedikt Höing, and Cornelius Kürten. Analysis was performed by Anke Daser, Kerstin Stähr, Friederike Kaster, Stefan Mattheis, and Katharina Klinger. Supervision and Resources came from Stefan Mattheis and Stephan Lang. The first draft of the manuscript was written by Anke Daser and Stefan Mattheis and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research and authorship of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research and authorship of this article.
Data Availability Statement
All data are included in this publication.