
Abstract
Objective:
Allergic rhinitis (AR) and chronic sinusitis (CRS) are prevalent upper airway inflammatory diseases with growing public health burdens. Sedentary behavior (SB) has emerged as an independent risk factor for multiple chronic conditions, yet its association with AR and CRS remains unclear.
Methods:
A cross-sectional analysis was conducted using data from the Korea National Health and Nutrition Examination Survey (2017-2018). AR and CRS were defined based on self-reported physician diagnoses. SB was assessed via self-reported daily sedentary time (ST) and categorized as <6, 6 to 8, and ≥ 8 hours/day. Multivariable logistic regression was performed to examine associations, adjusting for demographic, lifestyle, and clinical covariates. Subgroup analyses were conducted to assess potential heterogeneity across population subgroups.
Results:
Among 14 748 participants, the weighted prevalence of AR and CRS was 15.8% and 6.5%, respectively. Individuals with prolonged ST exhibited prominently higher prevalence rates of AR and CRS compared to those with low ST. Multivariable analysis indicated high ST (≥ 8 hours/day) was associated with increased odds of AR (OR = 1.161, 95% CI: 1.013, 1.329) and CRS (OR = 1.282, 95% CI: 1.038, 1.584). The association between SB and AR was more pronounced in individuals aged <40 years, alcohol users, those with a high school education, and white-collar workers.
Conclusion:
Prolonged ST was associated with a higher prevalence of AR and CRS in Korean adults. These findings highlight the potential public health relevance of SB in relation to upper airway inflammatory diseases; however, longitudinal studies are required to clarify causality and inform preventive strategies.
Introduction
Allergic rhinitis (AR) and chronic sinusitis (CRS) are 2 major chronic inflammatory diseases of the upper respiratory tract that significantly impair patients’ quality of life and impose a substantial socioeconomic burden.1,2 AR, in particular, has emerged as a global health concern. Over the past decades, the global prevalence of AR has steadily increased. In Denmark, repeated population-based surveys have demonstrated a marked rise in the prevalence of AR and allergic sensitization among adults, 3 while in China, the prevalence of adult AR has increased by 6.5% over the past 6 years. 4 Similarly, CRS is one of the most common chronic diseases, affecting an estimated 10% to 12% of the adult population worldwide. 5
In parallel, sedentary behavior (SB) has been identified as the fourth leading risk factor for global premature mortality. 6 The World Health Organization currently recommends at least 150 minutes of moderate-intensity aerobic physical activity, or 75 minutes of vigorous-intensity activity per week, to maintain health. 7 However, it is important to note that sedentary behavior is conceptually distinct from insufficient physical activity. SB refers to prolonged sitting or reclining with low energy expenditure and may exert adverse health effects independent of whether an individual meets recommended physical activity guidelines. Nevertheless, data from the Chinese National Center for Cardiovascular Diseases and the American Heart Association suggest that more than half of adults do not meet these minimum guidelines. 8 Consequently, SB, characterized by prolonged sitting with low energy expenditure, has drawn increasing attention as an independent health risk factor. This is especially relevant for individuals who remain sedentary for most of their waking hours and do not achieve recommended levels of physical activity.
The relationship between SB and allergic diseases remains controversial. Several epidemiological studies have reported a positive association between sedentary time (ST) and AR, 9 while others have found no significant link.10,11 Furthermore, the potential association between SB and CRS has not yet been systematically explored. Therefore, we conducted a cross-sectional study using nationally representative data from the Korea National Health and Nutrition Examination Survey (KNHANES) to explore the association between SB and the prevalence of AR and CRS. Our findings aimed to enhance understanding of the potential impact of SB on upper airway inflammatory diseases and provide insight into modifiable risk factors and preventive strategies for AR and CRS in adults.
Materials and Methods
Study Population and Data Source
In line with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines, 12 this cross-sectional study utilized data from the KNHANES (2017-2018) conducted by the Korea Centers for Disease Control and Prevention (KCDC). 13 KNHANES is designed to comprehensively assess health behaviors, medical conditions, and nutritional status among the Korean population using a stratified, multistage, probability-cluster sampling method. For the current analysis, individuals with missing data on ST (n = 780) and those without CRS/AR assessments (n = 591) were excluded. After these exclusions, a total of 14 748 participants were included in the final analytical cohort (Figure 1). Written informed consent was obtained from all participants, and the study protocol was approved by the Institutional Review Board of the KCDC. The study complied with institutional and national ethical regulations and followed the updated principles of the Declaration of Helsinki (2024). Since the analysis was based on de-identified, publicly available data from KNHANES, individual participants could not be traced or identified in any form.
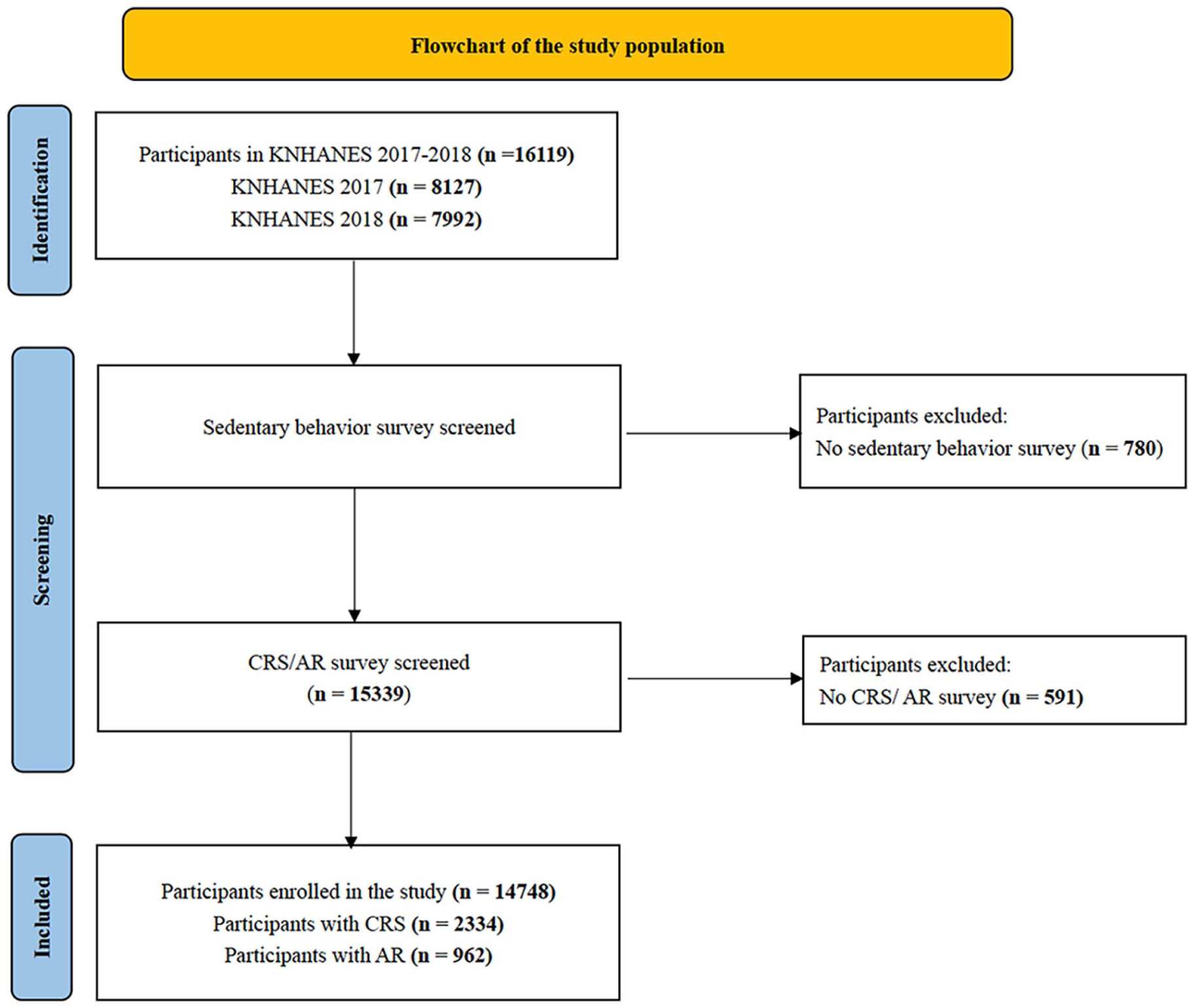
Flowchart of the study population.
Definition and Classification of AR and CRS
In this study, both CRS and AR were identified using responses from the standardized health interview questionnaire within the KNHANES survey. CRS was defined as a self-reported physician diagnosis based on an affirmative response to the question, “Have you ever been diagnosed with chronic rhinosinusitis by a doctor?” Participants were accordingly categorized into CRS and non-CRS groups. The definition and classification of AR followed the same approach. This method ensured consistent and clinically relevant case identification across the study population.
Definition and Classification of SB
SB was assessed using a self-reported questionnaire item that asked, “On average, how many hours per day do you spend sitting or lying down while awake?” Based on participants’ responses, sedentary time was categorized into 3 groups: <6 hours, 6 to 8 hours, and ≥8 hours per day. These cut-off points were informed by prior epidemiological evidence, particularly a dose-response meta-analysis identifying increased health risks beyond approximately 6 to 8 hours of daily sedentary time. 14
Assessment of Potential Confounding Variables
To account for potential confounders, multivariable models were adjusted for a range of demographic, behavioral, and health-related covariates. Sociodemographic characteristics: sex, age, education level (below high school, high school, and college or above), household income (quartiles), residential area (urban/rural), and occupational category. Lifestyle factors: alcohol consumption was classified based on frequency as <2 times/week or ≥ 2 times/week. Smoking status was categorized as < 5 pack-years or ≥5 pack-years. Health status indicators: body mass index (BMI) was included as a primary measure of obesity, dichotomized using the Asian population cut-off at 25 kg/m2 (<25 vs ≥ 25 kg/m2). Additionally, a self-reported history of physician-diagnosed asthma was included as a key comorbid condition for adjustment.
Statistical Analysis
All statistical analyses were conducted using IBM SPSS Statistics (Mac, version 27.0), following the official guidelines of the Korea Disease Control and Prevention Agency. A two-sided P value < .05 was considered statistically significant. Continuous variables were reported as weighted means ± standard deviations, and categorical variables as weighted frequencies and percentages. Multivariable logistic regression was used to evaluate the association between SB and the prevalence of AR and CRS, with results expressed as odds ratios (ORs) and 95% confidence intervals (CIs). Confounders were systematically adjusted in the final models. To assess potential multicollinearity among independent variables, variance inflation factors (VIFs) were calculated, with values <5 indicating no evidence of multicollinearity. Furthermore, to examine the consistency of associations across different strata, subgroup analyses were conducted based on key demographic and lifestyle variables. All inferences were drawn with consideration of the complex survey design to ensure robustness and generalizability of the findings.
Results
Baseline Characteristics and Disease Prevalence
A total of 14 748 participants were included in the weighted analysis, with a mean age of 43.22 ± 22.78 years. The sample comprised 54.6% females and 45.4% males. Key baseline characteristics were as follows: 62.4% had a smoking history of <5 pack-years, 75.3% consumed alcohol fewer than twice per week, 70.7% had a BMI <25 kg/m², 82.9% resided in urban areas, and 96.8% reported no history of asthma (Table 1).
Characteristics of the Study Population.
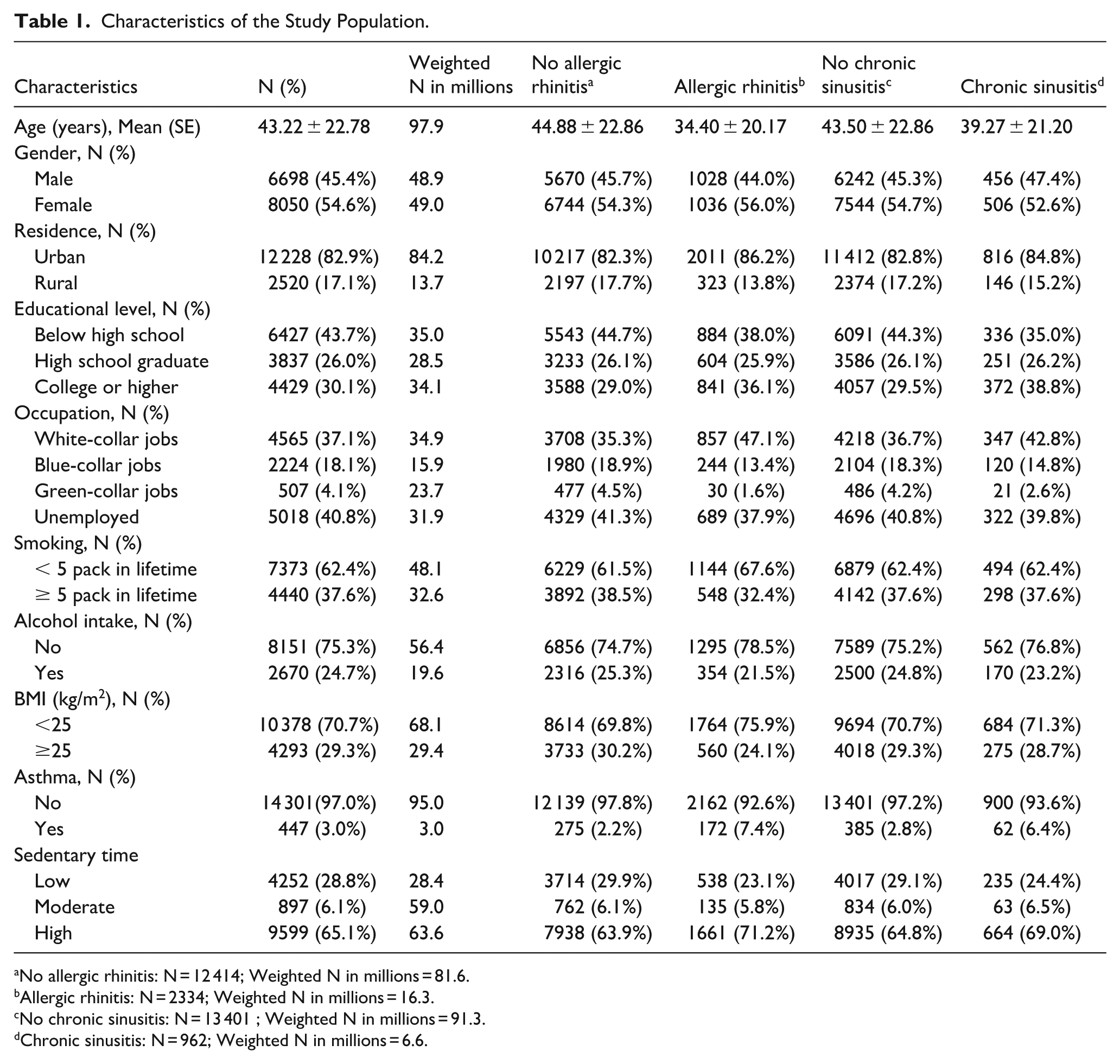
No allergic rhinitis: N = 12 414; Weighted N in millions = 81.6.
Allergic rhinitis: N = 2334; Weighted N in millions = 16.3.
No chronic sinusitis: N = 13 401 ; Weighted N in millions = 91.3.
Chronic sinusitis: N = 962; Weighted N in millions = 6.6.
Weighted prevalence estimates showed that 15.8% of participants had AR and 6.5% had CRS, corresponding to approximately 16.3 million and 6.6 million individuals nationwide in Korea, respectively. Additionally, 65.1% of participants reported prolonged SB, suggesting an estimated national burden affecting over 63.6 million individuals.
Stratified Analysis by SB
To explore the association between SB and nasal disease, we conducted stratified analyses by sedentary time. The prevalence of AR was substantially higher in the high sedentary group than in the low sedentary group (17.3% vs 12.7%, χ² = 47.728, P < .001). Similarly, CRS prevalence was higher among highly sedentary individuals (6.9% vs 5.5%, χ² = 9.388, P = .002) (Table 2).
Prevalence of AR and CRS according to ST categories.

Abbreviations: AR, allergic rhinitis; CRS, chronic sinusitis; ST, sedentary time.
Multivariate Analysis
After adjusting for multiple potential confounders, multivariable logistic regression revealed a threshold-like relationship between SB and the risk of AR and CRS. Notably, only high levels of ST were markedly associated with increased nasal disease risk. Compared with participants in the low sedentary group, those in the high sedentary group had a notably higher odds of AR (OR = 1.161, 95% CI: 1.013, 1.329) and CRS (OR = 1.282, 95% CI: 1.038, 1.584). In contrast, moderate sedentary time showed no statistically substantial association with either condition (Figure 2).
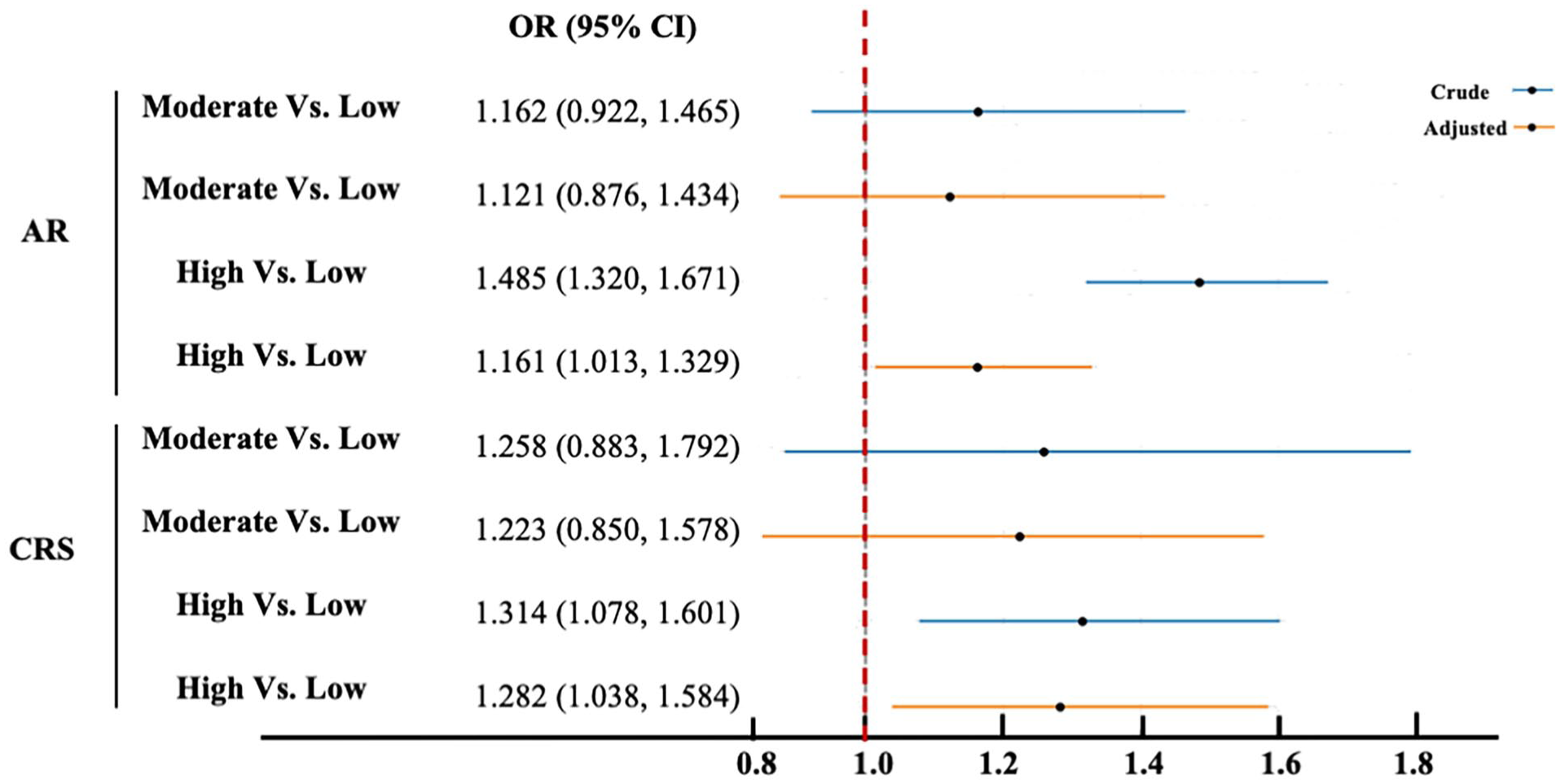
Association between sedentary time and the risk of AR and CRS based on multivariable logistic regression models.
Subgroup Analysis by Population Characteristics
To investigate potential effect modifiers in the association between ST and AR, we conducted subgroup analyses based on confounders identified in multivariable regression models (P < .05; Supplemental Table S1). The results indicated that prolonged ST was associated with an increased risk of AR, with varying risk levels across different subpopulations. Specifically, the association was more pronounced in individuals aged <40 years (OR = 1.276, 95% CI: 1.011, 1.611), those consuming alcohol ≥ 2 times weekly (OR = 1.186, 95% CI: 1.013, 1.388), individuals with a high school education (OR = 1.186, 95% CI: 1.013, 1.388), and white-collar workers (OR = 1.186, 95% CI: 1.013, 1.388). These findings highlighted an amplified effect of high sedentary time on AR risk within specific subgroups (Table 3).
Subgroup Analysis for the Association Between AR and ST in Patients With Different Characteristics.
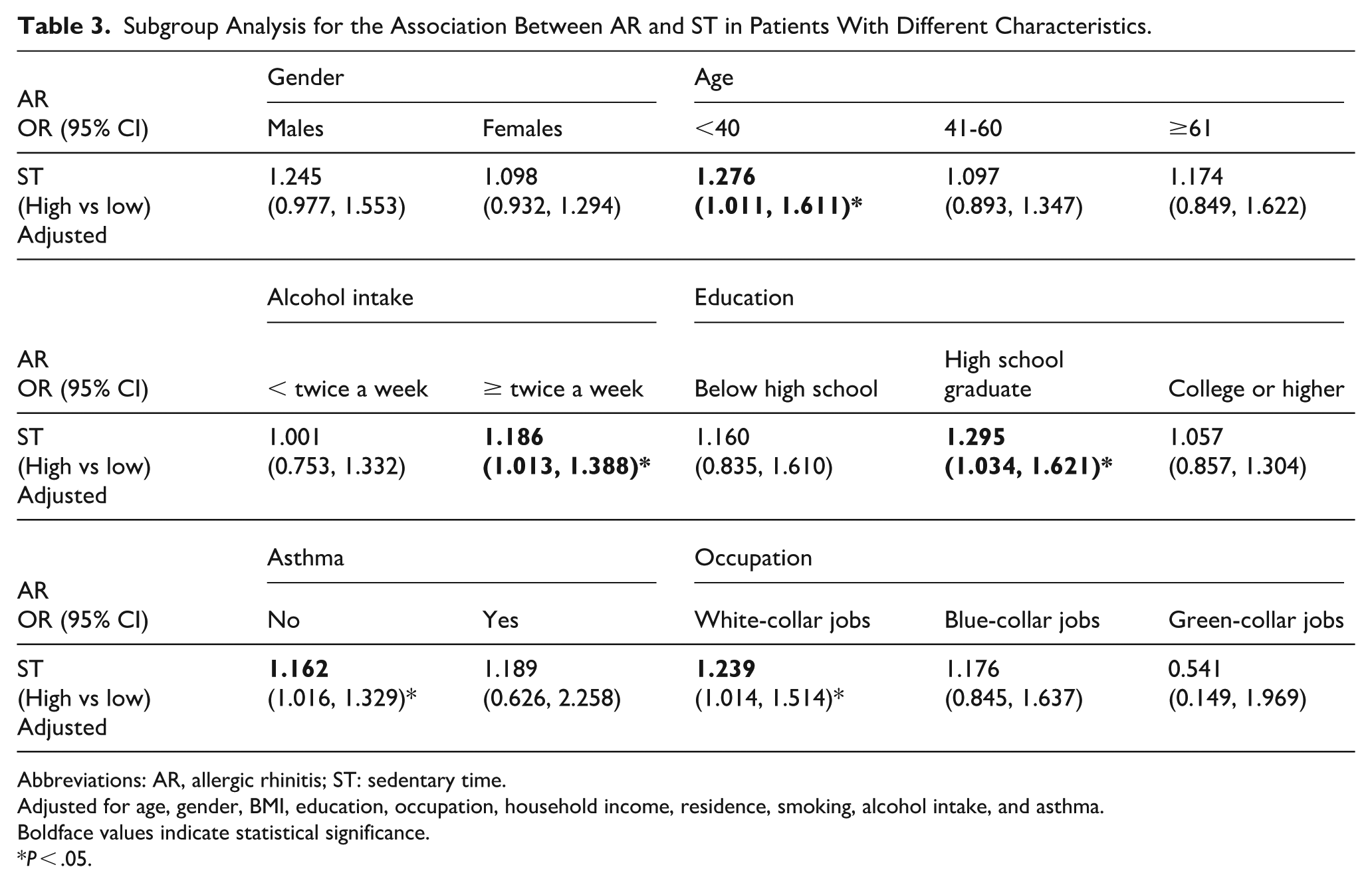
Abbreviations: AR, allergic rhinitis; ST: sedentary time.
Adjusted for age, gender, BMI, education, occupation, household income, residence, smoking, alcohol intake, and asthma.
Boldface values indicate statistical significance.
P < .05.
In BMI-stratified analyses, high ST was associated with increased odds of AR in both BMI <25 kg/m2 and BMI ≥25 kg/m2 groups; however, these associations did not reach statistical significance. Similar nonsignificant patterns were observed for CRS. No statistically significant interaction between ST and BMI was detected (all P > .05) (Supplemental Table S2).
Discussion
In this study, based on data from a nationwide cross-sectional survey, we revealed that individuals with prolonged ST exhibited prominently higher prevalence rates of AR and CRS compared to those with low ST. Multivariable analysis indicated that high levels of SB may be associated with an increased risk of AR and CRS, with this association being particularly pronounced among individuals <40 years old, those who consume alcohol ≥ twice weekly, individuals with a high school education, and white-collar workers. In contrast, moderate ST was not notably correlated with the risk of developing AR or CRS. To our knowledge, this study provides new population-based evidence on the relationship between SB and the prevalence of AR and CRS in a large-scale cross-sectional population.
Previous studies on SB have primarily focused on its associations with metabolic and cardiovascular diseases,15,16 while evidence regarding respiratory conditions remains relatively scarce. Vancampfort et al 17 reported that individuals with high levels of SB exhibited markedly increased risks of asthma and chronic pulmonary diseases. Similarly, Cao et al 18 revealed a positive linear relationship between prolonged SB and the risk of chronic obstructive pulmonary disease and asthma. In clinical settings, many asthma patients tend to avoid physical activity due to concerns about symptom exacerbation or exercise-induced bronchoconstriction, which may inadvertently lead to increased ST. 19 However, emerging research suggested that replacing SB with light-intensity physical activity may contribute to better asthma control, improved quality of life, and even reduced disease onset. 20 While existing literature has largely centered on lower airway diseases, our study extended the investigation to common chronic upper airway disorders, including AR and CRS. We observed that prolonged ST was substantially associated with increased risks of both AR and CRS. These findings underscore sedentary behavior as a potentially relevant behavioral correlate of upper airway diseases and suggest that its health implications warrant further investigation.
Notably, the observed associations were primarily driven by individuals with high levels of sedentary time, rather than showing a clear linear gradient across categories. The absence of a clear linear dose-response pattern across sedentary time categories warrants further consideration. One possible explanation is the presence of a threshold effect, whereby adverse upper airway inflammatory outcomes become apparent only after sedentary time exceeds a certain duration. This interpretation is consistent with prior epidemiological evidence suggesting that health risks associated with sedentary behavior may increase disproportionately beyond higher exposure levels. 14 Alternatively, the lack of significance in the moderate sedentary group may reflect limitations inherent to the cross-sectional and self-reported nature of the data. Self-reported sedentary time may be subject to nondifferential misclassification, which could attenuate associations at lower exposure levels. In addition, physician-diagnosed AR and CRS captured in large population surveys may be less sensitive to milder or subclinical disease, potentially obscuring associations in individuals with moderate sedentary exposure. These considerations highlight the need for longitudinal studies with objective exposure assessment and refined outcome characterization to better elucidate potential dose-response relationships.
Although the biological mechanisms underlying the association between prolonged SB and the increased risk of AR and CRS remain incompletely understood, several plausible pathways involving immune and stromal cell dysregulation have been proposed. First, SB exerts adverse effects on immune homeostasis. It promotes a pro-inflammatory gut microbiome, 21 elevates circulating cytokines such as IL-6 and CRP, 22 and impairs the production of anti-inflammatory myokines. 23 Notably, the link between sedentary time and low-grade systemic inflammation persists even after adjusting for confounding factors such as BMI, glycemic control, obesity, and intermittent physical activity. 24 Second, sedentariness may alter macrophage polarization, favoring the pro-inflammatory M1 phenotype while suppressing the anti-inflammatory M2 subtype. 25 This imbalance can trigger excessive production of transforming growth factor-β, disrupt fibroblast regulation, and promote tissue remodeling and fibrosis. 26 Such maladaptive immune-stromal interactions may foster a chronic inflammatory environment in the upper airways, contributing to the pathogenesis and persistence of both AR and CRS.
Subgroup analyses revealed that the association between SB and AR was more pronounced among individuals aged <40 years, those consuming alcohol ≥2 times per week, individuals with a high school education, and white-collar workers. These findings are consistent with previous research. Hong et al 27 reported that the prevalence of AR peaks between the ages of 20 and 29 and gradually declines with advancing age. He et al 28 further demonstrated that frequent alcohol consumption is associated with an increased risk of AR and elevated serum total immunoglobulin E levels, a key biomarker in allergic responses. Notably, the association between SB and AR was stronger in individuals with a high school education. This population may engage in relatively sedentary occupations while lacking sufficient health literacy or awareness to adopt protective behaviors, leading to greater exposure without adequate mitigation. 29 Similarly, the amplified effect of SB among white-collar workers is particularly noteworthy. Park et al 30 observed a higher prevalence of AR among white-collar workers, potentially due to prolonged indoor and sedentary work, often in enclosed, air-conditioned office environments. Such settings may facilitate sustained exposure to indoor allergens, including dust mites and molds, which are known contributors to allergic sensitization and upper airway inflammation. Together, these subgroup findings indirectly support the hypothesis that work-related indoor environmental exposures may modify the association between sedentary behavior and AR. Although detailed environmental and climatic variables could not be directly assessed in the present study, the observed heterogeneity across subgroups underscores the potential importance of occupational and environmental contexts in shaping the health effects of prolonged sedentary time.
Given the relatively low prevalence of overweight and obesity in the study population, we further examined whether BMI modified the association between ST and upper airway inflammatory diseases. In BMI-stratified analyses, higher ST was associated with increased odds of AR and CRS in both BMI <25 kg/m² and BMI ≥25 kg/m² groups; however, these associations did not reach statistical significance, and no statistically significant interaction between sedentary time and BMI was detected. The directionally consistent but nonsignificant findings across BMI strata suggest that the potential adverse associations of prolonged sedentary behavior with upper airway inflammatory diseases may not be exclusively driven by adiposity. Nevertheless, the lack of statistical significance should be interpreted with caution. Stratified analyses inevitably reduce statistical power, particularly for less prevalent outcomes such as CRS, which may have limited the ability to detect modest associations. In addition, nondifferential misclassification of self-reported sedentary time and reliance on physician-diagnosed outcomes may have further attenuated associations within BMI subgroups. Future longitudinal studies with larger sample sizes and objective exposure assessment are needed to further elucidate the interplay between sedentary behavior, adiposity, and upper airway inflammatory diseases.
Several limitations of this study should be acknowledged. First, due to the cross-sectional design, causal relationships between SB and nasal inflammatory diseases could not be established. Second, both sedentary time and physician-diagnosed AR/CRS were obtained through self-reported questionnaires, which may be subject to recall bias and potential misclassification. Third, residual confounding cannot be entirely excluded, as certain unmeasured factors, such as detailed occupational characteristics, indoor environmental exposures, regional climatic conditions, proximity to water bodies, air pollution exposure, or genetic predisposition, were not captured in KNHANES. Despite these limitations, the study benefits from a nationally representative sample, standardized data collection, and comprehensive adjustment for major covariates, supporting the robustness of the observed associations.
Conclusions
In conclusion, this nationally representative study found that prolonged SB was substantially associated with increased risks of AR and CRS. This association followed a threshold-like pattern and was particularly evident among younger adults, frequent alcohol consumers, individuals with a high school education, and white-collar workers. These findings highlight sedentary behavior as a potentially relevant behavioral correlate of upper airway inflammatory conditions and provide epidemiological evidence that may inform future preventive research. Further longitudinal studies are needed to establish causality and to determine whether reducing sedentary time can effectively contribute to prevention or management strategies.
Supplemental Material
sj-docx-1-ear-10.1177_01455613261421037 – Supplemental material for Sedentary Behavior as a Risk Factor for Nasal Inflammatory Diseases: A Cross-Sectional Study
Supplemental material, sj-docx-1-ear-10.1177_01455613261421037 for Sedentary Behavior as a Risk Factor for Nasal Inflammatory Diseases: A Cross-Sectional Study by Yue Liu, Min Li and Han Chen in Ear, Nose & Throat Journal
Supplemental Material
sj-docx-2-ear-10.1177_01455613261421037 – Supplemental material for Sedentary Behavior as a Risk Factor for Nasal Inflammatory Diseases: A Cross-Sectional Study
Supplemental material, sj-docx-2-ear-10.1177_01455613261421037 for Sedentary Behavior as a Risk Factor for Nasal Inflammatory Diseases: A Cross-Sectional Study by Yue Liu, Min Li and Han Chen in Ear, Nose & Throat Journal
Supplemental Material
sj-docx-3-ear-10.1177_01455613261421037 – Supplemental material for Sedentary Behavior as a Risk Factor for Nasal Inflammatory Diseases: A Cross-Sectional Study
Supplemental material, sj-docx-3-ear-10.1177_01455613261421037 for Sedentary Behavior as a Risk Factor for Nasal Inflammatory Diseases: A Cross-Sectional Study by Yue Liu, Min Li and Han Chen in Ear, Nose & Throat Journal
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board of the Korea Centers for Disease Control and Prevention (No. 2018-01-03-P-A).
Consent to Participate
All participants in the KNHANES provided written informed consent and voluntarily took part in the survey.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Breeding Program of Fujian Children’s Hospital (Grant number: YP202404) and the Guiding Science and Technology Program of Fujian Province (2025Y0045).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.