
Abstract
Background:
Depression is a mental health disease of growing public health concern because depressive mood affects the sufferer’s daily life and is also associated with productivity decline. Depression that is caused by other diseases or substances is referred to as secondary depression, which is an important distinction because curing the underlying cause could subsequently regulate depressive mood. Empty nose syndrome (ENS), also known as “paradoxical obstruction of the nose,” is a condition in which the major symptom is difficulty breathing, despite having sufficient breathing space in the nose. Empty nose syndrome has been increasing in prevalence in Korea. We found that patients with this ENS have a tendency toward depressive mood, which can escalate so far as to lead to suicide attempts. Thus, herein, we aimed to investigate the psychological burden on patients with ENS.
Methods:
We divided patients into 4 groups: ENS (group A), chronic rhinosinusitis with polyp (CRS c polyp, group B), chronic rhinosinusitis without polyp (CRS s polyp, group C), and allergic rhinitis (AR, group D). We estimated and compared Beck Depression Inventory (BDI) scores among the 4 groups, and we investigated the relationship between depression index and nasal cavity area in patients with ENS.
Results:
The ENS group (A) had depression prevalence of 71% with varying severity, which was much higher than group B (19%), group C (15%), and group D (27%). The correlation between nasal cavity volume and BDI score for the ENS group was not statistically significant.
Conclusion:
The degree and severity of depression in patients with ENS was higher than in patients with CRS or AR. Furthermore, there was no relationship between depression severity and nasal cavity volume in the patients with ENS. Thus, physicians should be careful not to dismiss the accompanying mental health problems of patients with ENS.
Introduction
Depression is mental health disease getting more interest in public health area in terms of substantial effects on the individual’s life and social productivity. 1 It is well known that there is tendency to be increased prevalence of major depression in the medically ill patients, which is called secondary depression, 2 refers to depression caused by physical illness. In otolaryngology area, several clinical studies have found that allergic rhinitis (AR) and empty nose syndrome (ENS) have something to do with depression. 3 -7
There are no consensual definition about ENS as yet. 5,8,9 Empty nose syndrome is caused by mainly turbinate reduction surgery, which include not only total turbinate resection but also even in conservative procedures. 7,9 Main symptom of the disease is paradoxical obstruction of nose, which means thatcomplaining of nasal congestion, even though there is enough space of nasal cavity. 5,7 -9 Other symptoms such as sensation of suffocation, headache, pain, a sensation of empty nose, and pharyngeal dryness are also often reported. 5,8,9 Symptom intensity varies, and mood change such as anxiety and depression can be manifested, that lead to declination in the productivity of the individual. 5,7 -9 Some patients attempt to suicide in extreme cases. 10 The true incidence of ENS is uncertain. Some authors estimated that the incidence of ENS may decrease over time as the trends of nasal surgery are toward advocation of conservative surgery.
The diagnosis of ENS is made empirically based on previous turbinate surgery history and related symptoms. The authors experienced patients with ENS complaining of depression, even with suicidal impulse. There is a study on the change in depression index between before and postsurgical treatment of repair of ENS. But there are few articles dealt with comparison of psychological burden of ENS to that of other sinonasal disease. The aim of this study is to compare the degree of depression between patients with ENS and patients with sinonasal disease.
Material and Methods
Patients
We analyzed data from patients (group A), who were diagnosed with ENS at Kosin University hospital from January 2015 to May 2017. The diagnosis of ENS was based on the following criteria: (1) history of previous nasal surgery to change the structure of the nose; (2) subjective symptoms including excessive nasal crusting or discharge, paradoxical nasal congestion, headache, hoarseness, excessive airflow, facial or nasal pain on inspiration, and depression; and (3) Cotton test (+). We set the rule in the process of collecting data to exclude patients who have already been diagnosed with depression before diagnosis of nasal disease. And patients with insufficient medical record are excluded from this study population. Finally, 24 patients were enrolled in group A. The comparison groups are consisted of group B (n = 16; chronic sinusitis with nasal polyp), group C (n = 20; chronic sinusitis without nasal polyp), and group D (n = 34; AR).
Measurements
Beck Depression Inventory
As a measure of depression, this study used Beck Depression Inventory (BDI) questionnaire. Beck Depression Inventory is regarded as useful tool for screening and detection of depression with sensitivity and reliability. The BDI included 21 items, each of which is rated between 0 and 3. Depression is rated by the total score, where the score of 0 to 13 indicates normal, 14 to 19 indicates mild depression, 20 to 28 indicates moderate depression, and 29 to 63 severe depression. The BDI can be subdivided into 2 scales: psychological (BDI items 1-13) and somatic (BDI items 14-21). The authors also get BDI scores for each group by dividing the BDI score into 2 categories (psychologic and somatic).
SNOT-22 (Sino Nasal Outcome Test-22)
For each patient, the symptom score was assessed using SNOT-22, which was conducted via questionnaire. SNOT-22 consists of 22 items that quantify the symptoms associated with nasal symptoms, and each item is rated on a score from 0 (no symptoms) to 5 (severe symptoms).
Endoscopic examination
We conducted endoscopic examination in all patients for evaluating abnormal nasal cavity structures (Figure 1).
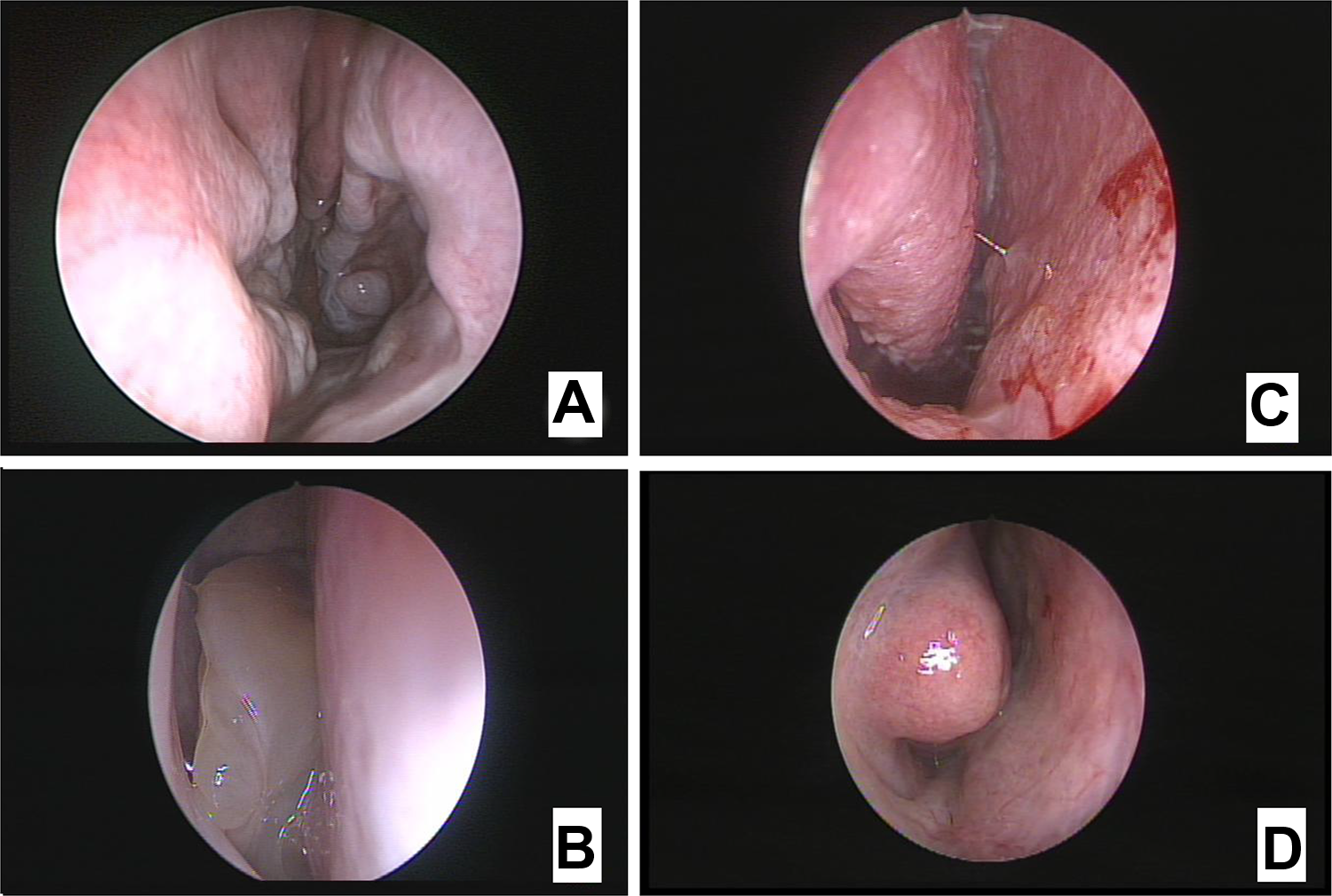
Representative findings of endoscopy for each group. A, Resected inferior turbinate due to previous surgery. B, Nasal polyp in nasal cavity. C, Chronic mucous drainage. D, Watery rhinorrhea and relatively pale mucosa.
Acoustic rhinometry
Using acoustic rhinometry, minimal cross-sectional area and total volume along the nasal cavity were measured.
Cotton test
For ENS group (group A), moistened cotton ball was applied into nasal cavity where previous endonasal surgery or procedures were performed. Then, the patient was asked after 10 minutes if he felt any relief of the ENS symptom or not.
Statistical Analysis
Statistical analysis was performed using SPSS software for Window (version 22.0, SPSS Inc). The Kolmogorov-Smirnov test was used in verifying normality. The Mann-Whitney U test was used for 2- and 3-nonparametric group comparisons. Spearman correlation test was used to clarify correlation 2 variables.
Results
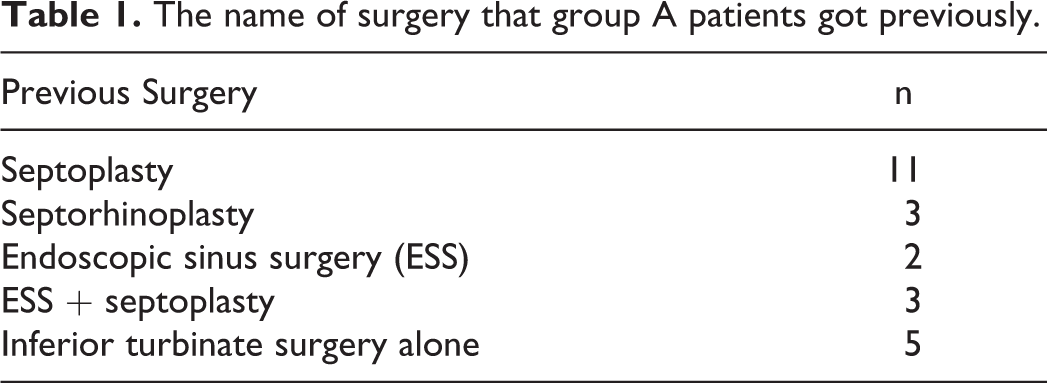
The characteristics of each patients group show no significant differences in age. The name of surgery group A patients got previously are presented in Table 1. There were 5 cases in which the inferior turbinate surgery was performed alone. In the case performed with other surgery, septoplasty was the most common with 11 cases, followed by septorhinoplasty, endoscopic sinus surgery plus septoplasty, and rhinoplasty in this order (Table 1).
The name of surgery that group A patients got previously.
We analyzed the relationship between the type of inferior turbinate surgery and BDI score (Table 2). Even patients who underwent conservative surgeries (n = 16; eg, microdebrider-assisted inferior turbinoplasty, coblator turbinoplasty) lead to ENS and it take up larger portion compared to radical turbinate surgeries (n = 8; eg, inferior turbinectomy, total or partial turbinectomy) in this study. There is no BDI score difference with statistical significance between conservative and radical group.
BDI score between Radical group and Conservative group.
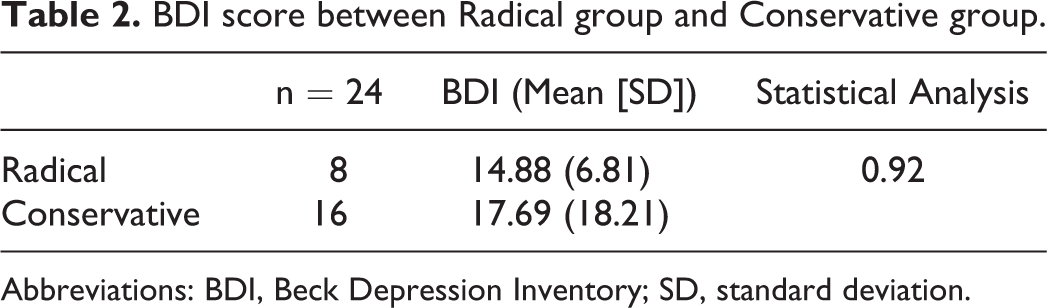
Abbreviations: BDI, Beck Depression Inventory; SD, standard deviation.
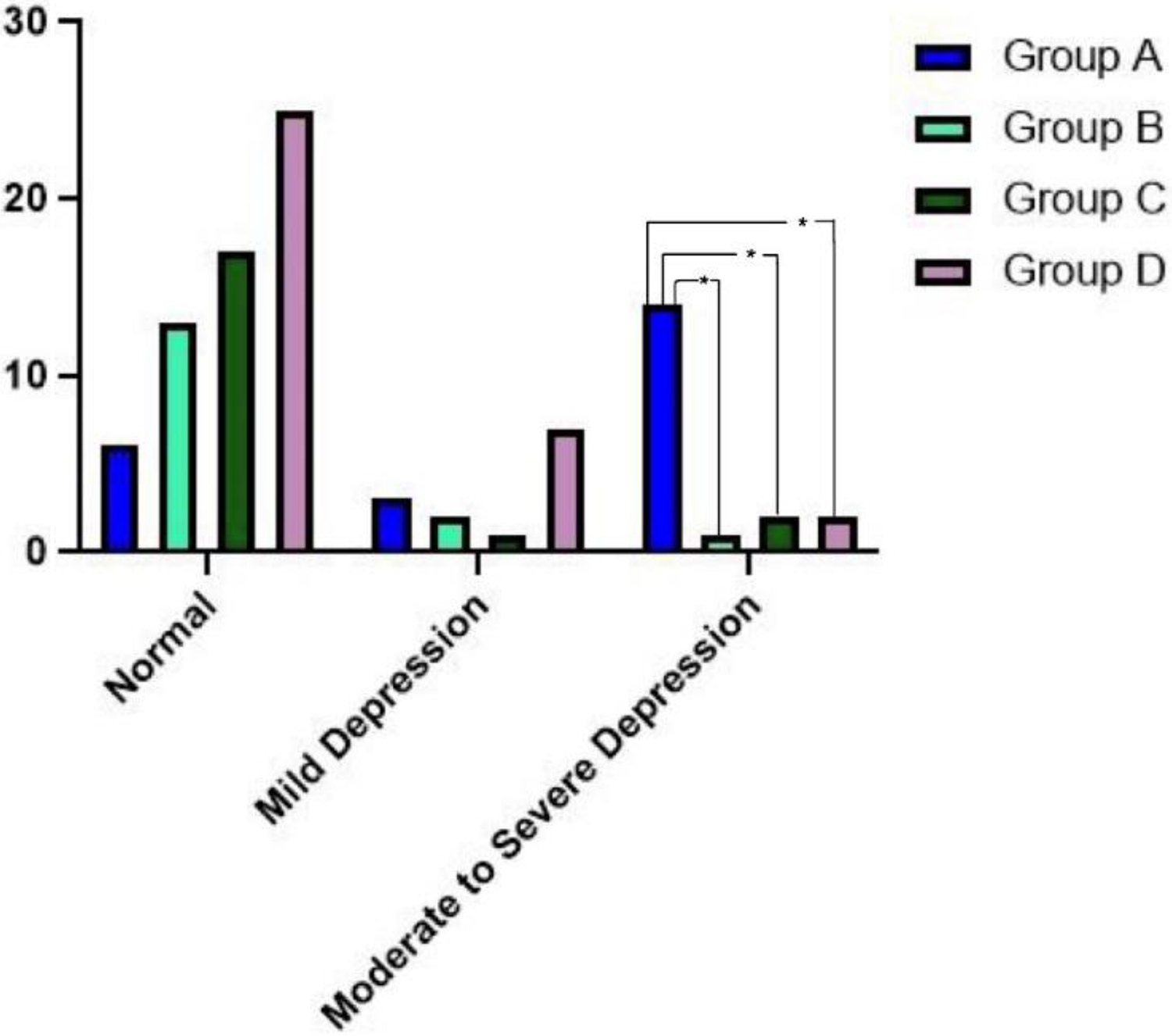
The severity of depression in the group A was as following: normal 7 (29%) patients, mild depression 3 (13%) patients, moderate depression 8 (33%) patients, and severe depression 6 (25%) patients. Seventy-one percent of patients with ENS showed various degree of depression. On the other hand, 3 (19%), 3 (15%), and 9 (27%) of patients in group B, C, and D, respectively, showed various degree of depression (Table 3). The number of moderate to severe depression in group A is greater than other groups with statistical significance (Figure 2).
BDI score between radical group and conservative group. Somatic score as well as psychologic score of Beck Depression Inventory (BDI) in empty nose syndrome (ENS) group was significantly higher than that of other groups. P < .05.
BDI score between each group.
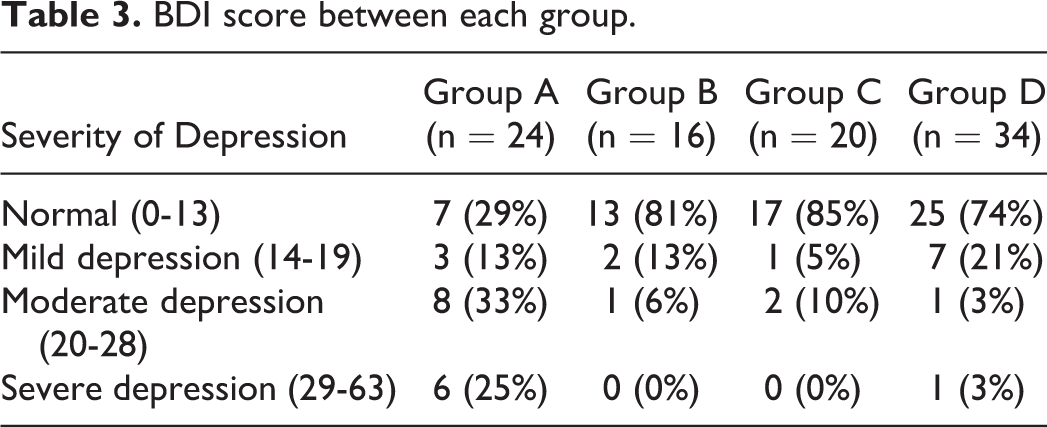
Psychological score is 12.6 (8.5), 5.31 (4.30), 4.45 (4.5), and 4.14 (4.36) for group A, B, C, and D, respectively. Somatic score is 9.04 (4.9), 2.06 (1.98), 2.1 (2.32), and 3.32 (3.30) for group A, B, C, and D, respectively. Somatic score as well as psychologic score of BDI in ENS group was significantly higher than that of other groups (Figure 3). However, there is no significant statistical differences among group B, C, and D.
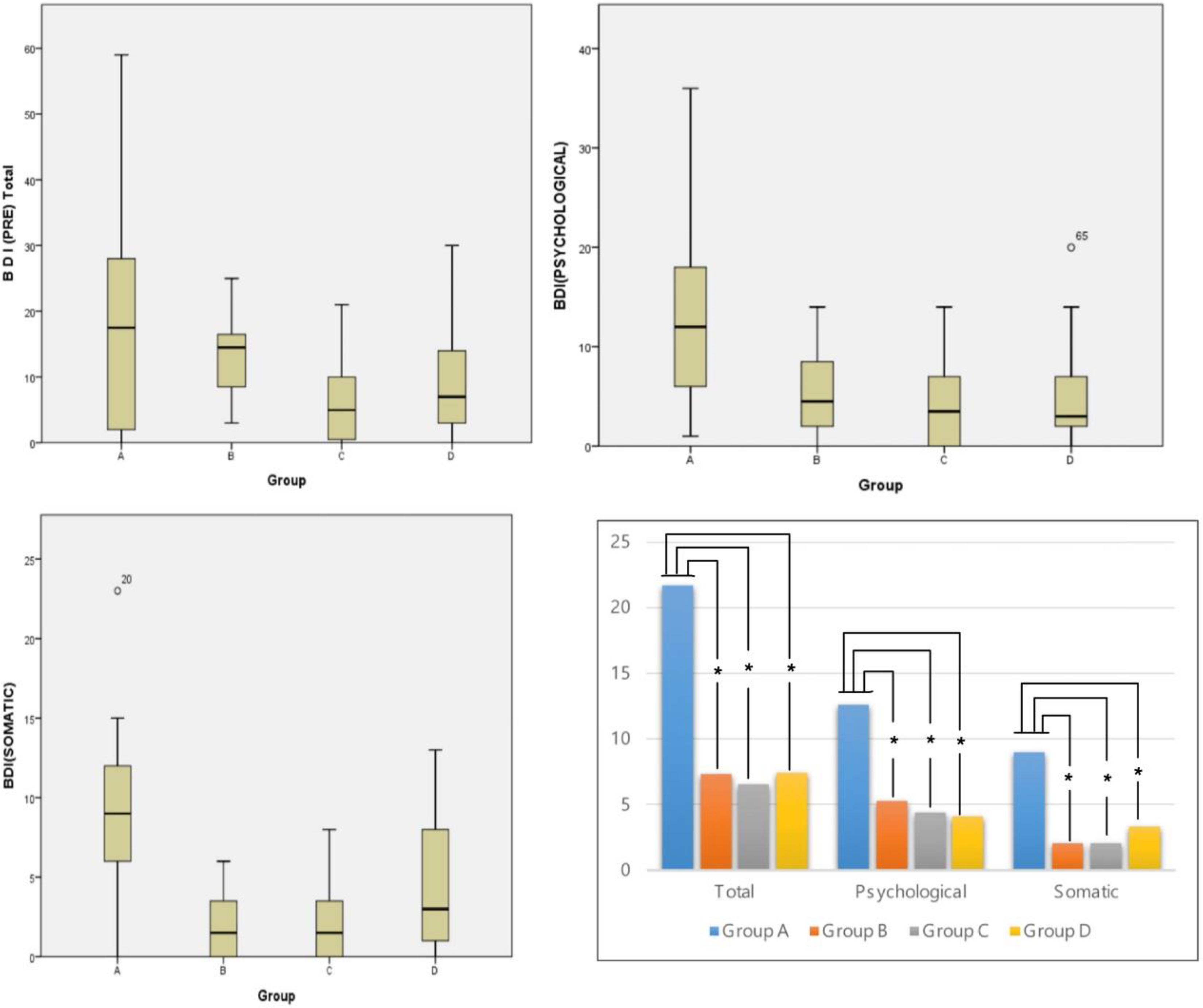
Somatic score as well as psychologic score of Beck Depression Inventory (BDI) in empty nose syndrome (ENS) group was significantly higher than that of other groups. *P < .05.
The correlation between nasal cavity volume measured by acoustic rhinometry and BDI score of group A showed no statistically significance (Figure 4). And no relationship between SNOT and BDI score (Figure 5).
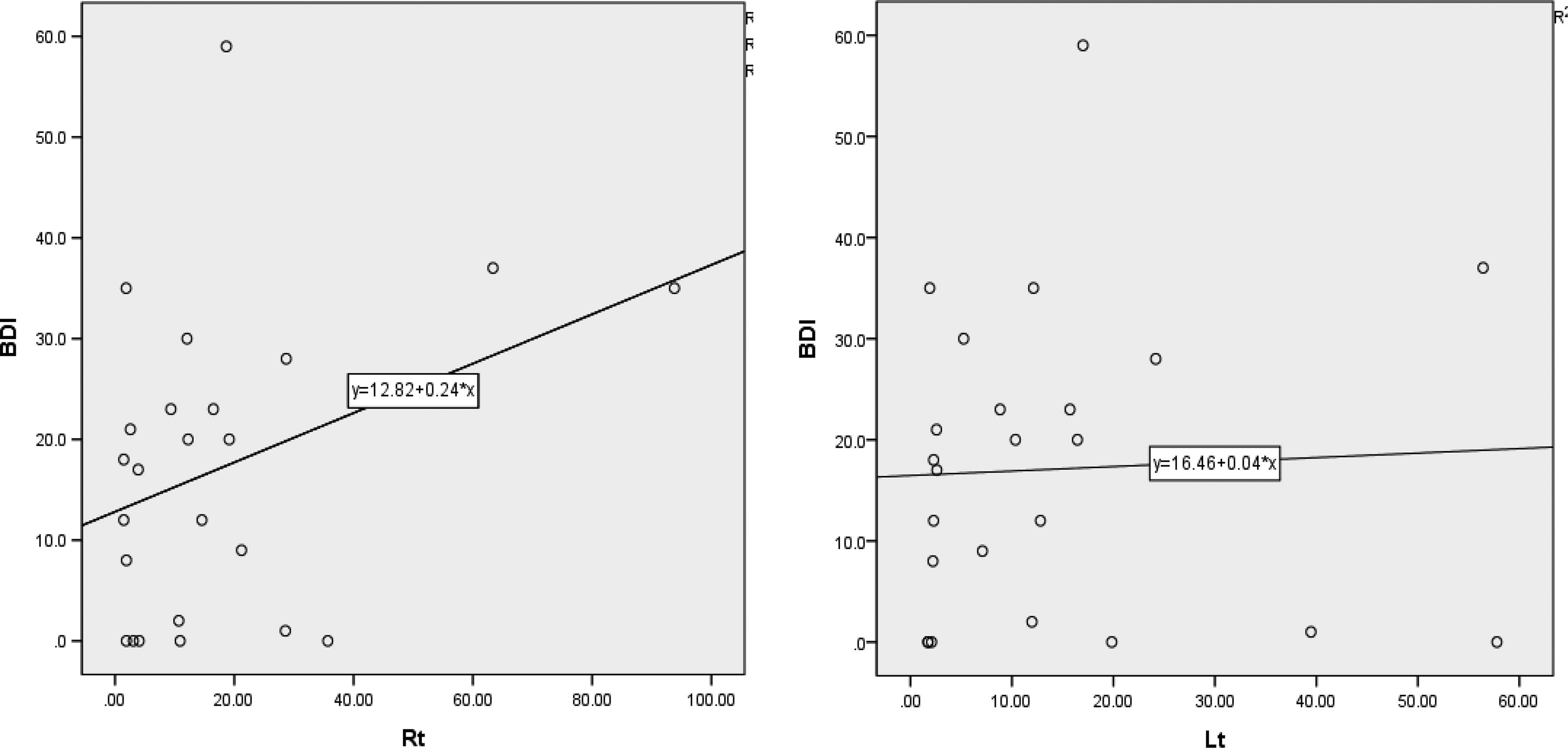
There is no significant relationship between nasal cavity volume and degree of depression. Rt: P = .95, r = 0.26. Lt: P = .828, r = 0.47.
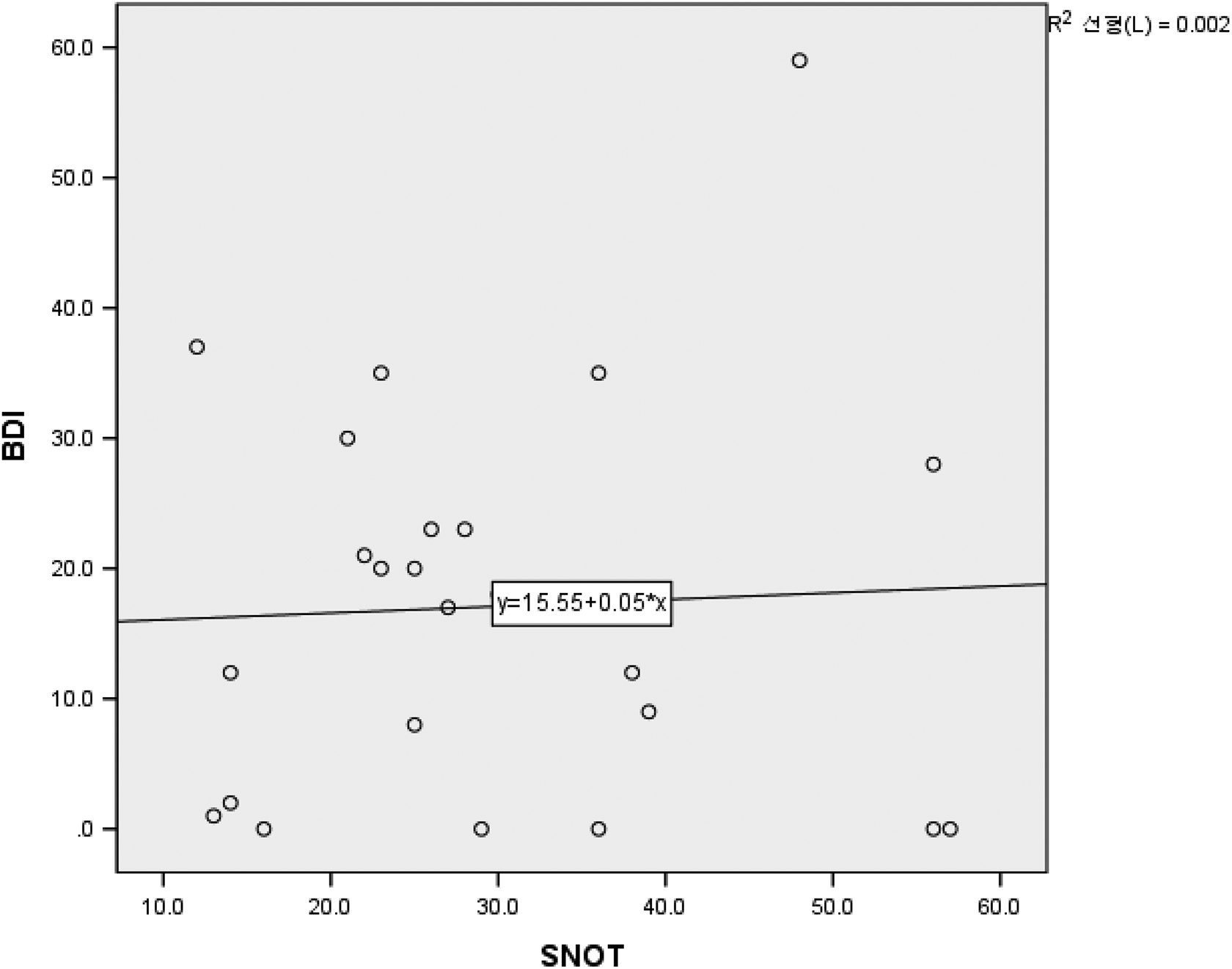
There is no significant relationship between sino-nasal outcome score (SNOT) and degree of depression. P = .62, r = 0.106.
Discussion
Empty nose syndrome, an iatrogenic disease mainly caused by turbinate surgery, is classified into 4 subtypes 8 : (1) ENS secondary to inferior turbinate resection (ENS-IT), (2) ENS secondary to middle turbinate resection, (3) ENS secondary to both inferior and middle turbinate, and (4) ENS after turbinate-sparing procedures (termed ENS-type; eg, turbinate reduction). 8,10 The overall frequency of each subtype is currently not certain, but the most common type in this study is ENS-IT.
Because there is no definite diagnosis criteria for this disease, diagnoses are clinically made based on subjective symptoms and previous surgery history. 10 The incidence of ENS following turbinate resection is unknown. Some reports have quoted a 20% ENS incidence after inferior turbinate surgery and have estimated that the incidence of ENS may decrease over time as the trends of nasal surgery move toward the advocation of conservative surgery. 9 Our results showed that patients with ENS is predominantly caused by conservative surgery, which somewhat contradicts results from earlier studies. Although surgeries on inferior turbinate are increasingly preservation surgery (eg, microdebrider-assisted inferior turbinoplasty), it is prudently thought that the prevalence rate of ENS may not be reduced, reflecting on the fact that those who undergo preservation surgery are also at risk of ENS.
There are several notable features of the pathophysiology of ENS: (1) a total turbinectomy of inferior turbinate does not always result in ENS, and (2) this disease can be caused by conservative procedures, even including bipolarization of inferior turbinate. 5,11 Two-thirds of patients in the ENS group in our study were diagnosed with ENS, even though they had undergone the conservative surgery of inferior turbinate.
Patients with ENS complain of nasal obstructions despite having enough space for breathing; this is called paradoxical nasal obstruction. The severity of paradoxical obstruction cannot solely be explained by a “wide” or “narrow” nasal space. Three plausible mechanisms for this symptom are (1) anatomic changes leading to changes in air pathways, (2) disruption of the mucosal homeostasis of nasal cavity, and (3) disruption of neurosensory fibers. 8 The most widely accepted theory is that there is disruption of the nasal mucosa area, which is necessary for nasal humidification, temperature control, and mucociliary clearance after turbinate surgery. 8
Treatment options for ENS are medical therapy such as mucosal humidification, saline irrigations, adequate fluid intake, and ointment application. 10 Surgical treatment narrows the nasal cavity volume by using rib or auricular cartilage. 12 Jung et al reported that the cartilage is superior to ear cartilage as an implant in the treatment of ENS. 13 Lee et al reported that surgical treatment for ENS is effective in improving depression and anxiety, and patients with worse preoperative BDI scores, as well as female patients, may be better candidates for surgical intervention. 6
Many studies have reported that chronic diseases and depression are closely associated with each other; the majority of patients with ENS have reportedly developed depression. 4,14 -16 The term “secondary depression” refers to depression that has been caused by physical illness. 2 It is well known that the mean depression score for those with a chronic disease status is significantly higher than that for control groups. 3,4,17,18
Overall, the prevalence of clinically important depression in ENS individuals has been shown to be approximately 68%. 17 In our study, the about 71% of patients in the ENS group had depression with varying severities of depression. Among them, 25% had severe depression, which is noticeably higher than the patients in groups B, C, and D. This emotional impact of ENS cannot be explained simply with anatomical changes; there have been some reports on the relationship between ENS and mental health. Freund et al studied the activation of the limbic system, which is normally involved in processing emotions, using functional magnetic resonance imaging in patients with ENS at a resting condition. 19 These scans suggested that limbic activation could lead to unsteady mental conditions for patients with ENS. 19
Patients with chronic rhinosinusitis (CRS) also have an increased prevalence of depression as compared to healthy controls. 14,15 Previous articles have reported that the general prevalence of previous physician-diagnosed depression in patients with CRS is 10%, 14 whereas in this study, the percentages of patients with depression were 19% (CRS s polyp) and 15% (CRS c polyp).
The depression index is known to be higher in patients with both CRS and ENS diseases, 3,14,17,20 but there is no study yet that has compared the severity of depression of patients with ENS to that of other patients with sinonasal disease. These results show that the degree of depression of patients with ENS is higher than that of patients with CRS and AR. Our study discovered mild depression (13%), moderate depression (33%), and severe depression (25%) in patients with ENS. The ENS group had a higher rate of moderate to severe depression than the other sinonasal disease group (Figure 2, Table 3).
The BDI scores were categorized into 2 groups, psychological and somatic score, which combined to give a total BDI score. A higher score for both somatic and physiologic scores leads to a higher total BDI score in patients with ENS (Figure 3).
There was no statistically significant relationship between BDI scores and SNOT scores. Although the symptoms of ENS are a nuisance to patients, it seems that they do not necessarily lead to a change in the depression index. This suggests the possibility of other factors, such as sensitivity to depression in individual patients, being related to the expression of depression.
We are hesitant to conclude that the cause of depression is ENS, and this study does not fully support the hypothesis there is a causal relationship between depression and ENS. This is one limitation of our study, in addition to the small sample size. Despite these limitations, we can at least maintain that depression is more prevalent and more severe in patients with ENS than any other sinonasal disease, regardless of whether that depression is secondary or comorbid. The psychological burden of ENS should not be overlooked; therefore, we would like to suggest that patients’ psychological status should be investigated as part of the workup in the treatment of ENS.
Conclusion
Our study demonstrates that the degree and severity of depression of patients with ENS is higher than that of patients with CRS and AR. We should be careful not to dismiss the mental health problems that accompany the medical and surgical treatment of ENS.
Footnotes
Authors’ Note
Jae Hwan Kwon has made substantial contributions to conception, supervision, design of study and editing. Chang Hoi Kim contributed to writing original draft, investigation. Jooyeon Kim contributed to conceptualization, data curation, and investigation. Song Ji Ah contributed to visualization. Choi Gil Soon contributed to data curation. This study has been approved by institutional review board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.